Embed Size (px)
DESCRIPTION
understanding deep vein thrombosis
Citation preview

March/April 2008 Nursing made Incredibly Easy! 29
In too deepUnderstanding deep vein thrombosis
Two million people will experience someform of deep vein thrombosis, or DVT,this year, so it’s easy to see why DVT issuch an important topic. We’ll give youthe tools you need to understand DVTfrom how it happens and who’s at riskto what you can do to help thesepatients. JAMES STOCKMAN, RN, CCRN, BSNStaff Nurse • Trinity Mother Frances HealthSystem • Tyler, Tex.The author has disclosed that he has no significant relation-ships with or financial interest in any commercial companiesthat pertain to this educational activity.
2.5ANCC/AACN
CONTACT HOURS
DEEP VEIN THROMBOSIS(DVT) is a clot that forms mostcommonly within the deepveins of the legs, but it can alsooccur in the pelvis or arms.DVT has been increasingly inthe spotlight for the last 15years due to three factors: therising cost of health care, an in-crease in preventive medicine,and our aging population.
In this article, I’ll fill you in onDVT, including what you needto know about taking care of a
patient who already has it andhow to prevent at-risk patientsfrom developing it.
But first, let’s review thepathophysiology of DVT.
You’re so veinThe veins of the body consist ofthe superficial veins that runnear the surface of the skin, andthe deep veins, such as the greatsaphenous and popliteal veins,that are located underneath themuscles and run parallel to the

30 Nursing made Incredibly Easy! March/April 2008
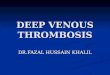
Lower limb veins arteries (see Lower limb veins). Smaller veinsconnect the superficial and deep veins andhelp move blood from the skin to the deepveins. Blood is then moved back to theheart with the aid of valves in the superfi-cial and deep veins that allow unidirec-tional flow. Various factors influence bloodflow through the legs: Valves in the veinsprevent backflow, while walking and mus-cle movement in the legs aid blood flowback to the heart. Since blood flow is al-ready slowed as it’s squeezed from the con-necting veins into the deep veins, there’s ahigh risk of clot (thrombus) formation ifany further slowing of the flow occurs. Anytime blood slows or is stationary, as instanding or sitting for long periods, there’sthe potential for a thrombus to form.
Let’s now take a look at blood flow to bet-ter understand thrombus formation.
Don’t slow the flow!Anything that alters the strength of theblood vessel wall can slow blood flow andcause DVT. Think of the vascular system asan intertwining water hose. Normally, wa-ter flows through the hose without any dif-ficulty but if you kink the hose, you reducethe flow of water. Over time, dirt and otherimpurities build up within the hose andadd to the reduced flow. The same princi-ples apply to the vascular system. So everytime you sit down, curl your legs, or crossyour arms, you reduce blood flow, whichcan cause small clots to form. Normally, thebody immediately breaks down these clots.However, when stasis of blood (venous sta-sis), vessel wall injury, and hypercoagulabil-ity—the three factors known as Virchow’striad—are present, an abnormal thrombuswill most likely form (see A closer look atVirchow’s triad).
How does the thrombus form? Let’s take alook at that next.
A thrombus among usMechanical or physiologic damage to thevessel wall leads to platelet activation. Ex-
Vena cava
Common iliac vein
Internal iliac vein
External iliac vein
Great saphenous vein
Femoral vein
Deep veins of the knee
Superficial veins of the knee
Popliteal vein
Small saphenous vein
Fibular vein
Posterior tibial vein
Great saphenous vein
Deep veins of the foot
Superficial veins of the foot

March/April 2008 Nursing made Incredibly Easy! 31
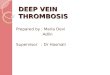
amples of mechanical damage include highvelocity trauma in which bones are brokenand surgery, especially orthopedic or ab-dominal surgery. Examples of physiologicdamage include hypertension, in which thevessel wall weakens over time, and phle-bitis, in which a vein is inflamed. The plate-lets adhere to one another and clump to-gether, forming a thrombus (see Picturingvenous thrombosis). After a thrombus forms,it flows in the body and is either dissolvedover time or grows and becomes largeenough to occlude a vessel. If the thrombusoccludes a vessel, it’s known as an embolus.
After an embolus forms, the blood behindthe blockage slows and the veins expand toaccommodate an increase in volume. Thisleads to a general pooling of blood thatslows the blood further and causes moreclots to form. Ultimately, the drainage of thelymphatic system slows, leading to edema ofthe affected extremity.
So who’s at risk for developing DVT?That’s up next.
Risks, risks everywhere…Patients who are most at risk for DVT arethose undergoing major surgery, especiallyorthopedic surgery. Other at-risk patientsinclude those who smoke or have lung dis-ease, diabetes, blood disorders, and periph-
eral vascular disease. But remember, anyhospitalized patient is at risk for DVT, espe-cially those who’ll be immobile for an ex-tended period of time or are of advancingage. If your patient has any one of the threefactors in Virchow’s triad, there’s the poten-tial for DVT.
See Which surgical patients are at risk forDVT? for more information.
A closer look at Virchow’s triadRisk factors Common causes
Changes in blood flow • Stasis related to prolonged immobility, paralysis, varicose veins, or heart failure
• Increased blood viscosity
Changes in the vessel wall • Atherosclerosis leading to rupture of plaque on the vessel wall exposes thrombogenic material, activating platelets and the coagulation cascade
Changes in blood coagulability • Traumatic, burn, and surgical injuries because of tissue damage, release of tissue factors, and activation of the extrinsic pathwayof coagulation
• Cancer (fibrinolytic activity may be reduced and malignant tissue may promote coagulation)
Picturing venous thrombosis
Tunica intima
Tunica media
Tunica adventitia
Thrombus
Valve
Endothelium
Internal elasticmembrane
Smooth muscle
External elasticmembrane

32 Nursing made Incredibly Easy! March/April 2008
It’s a signHow do you know if your patient hasDVT? And if he does, is he at risk for morecomplications? Let’s now review signs andsymptoms to be alert for and then we’lltake a look at potential complications.
DVT may be difficult to recognize imme-diately because many patients don’t exhibit
signs and symptoms or their symptomsare nonspecific. Signs and symptomsinclude: n edema or swelling of the affected ex-tremityn rednessn pain or tendernessn an increase in the temperature of theaffected extremity compared with therest of the bodyn cyanosis and mottling of the skin due
to stagnant blood flow. Although Homans’ sign (pain with dorsi-
flexion of the foot) has historically been usedto assess DVT, it’s not a reliable or valid sign;in fact, the literature suggests that up to 50%of patients with DVT don’t have a positiveHomans’ sign.
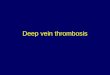
It can get complicatedThe most serious complication of DVT ispulmonary embolism (PE), in which the dis-
lodged thrombus obstructs the pulmonaryartery bed (see Picturing pulmonary emboli).PE can be life-threatening and may requiremechanical ventilation. If your patient com-plains of any of these signs and symptoms,notify the health care provider immediately:n severe dyspnean tachypnean chest painn coughn hemoptysis (coughing up blood).
Another complication occurring in 40% to60% of patients with DVT is postthromboticsyndrome. Caused by a combination of fac-tors, such as back flow of blood related tofaulty valves and blockage that remains inthe vessel, signs and symptoms of this syn-drome include pain, increased swelling, skinulcers, and hyperpigmentation. How longpostthrombotic syndrome persists dependson the patient’s ability to form collateral cir-culation around any remaining embolus.Treatment for this condition is palliative,including anticoagulation therapy and ele-vating the affected extremity to help de-crease swelling and pain.
Assessment = early detectionLet’s say you’re worried that your over-weight patient with diabetes who doesn’t
want to get out ofhis bed to ambulateis developing DVT.What do you do?Careful assessmentwill help detectearly signs of a ve-nous disorder of thelegs. Assess for: n limb painn a feeling of heavi-nessn functional im-pairmentn ankle engorge-mentn edeman differences in leg
Which surgical patients are at risk for DVT?
Risk level Patient populationHighest • Patients undergoing hip or knee surgery
• Patients with multiple risk factors undergoing surgery• Patients with major trauma
High • Patients greater than age 60 undergoing surgery• Patients age 40 to 60 with additional risk factors undergoing surgery
Moderate • Patients with additional risk factors undergoing minor surgery • Patients age 40 to 60 with no additional risk factors undergoing surgery
Low • Patients less than age 40 with no additional risk factors undergoing minor surgery
He’s really asuperficial vein. He
just thinks if hereads enough
literature, peoplewill start to think
he’s deep.

March/April 2008 Nursing made Incredibly Easy! 33
circumferences bilaterally from thigh toanklen an increase in the surface temperature ofthe leg, particularly the calf or anklen areas of tenderness or superficial throm-bosis.
One of the most reliable physical indica-tions of DVT is unilateral edema of theextremity. Measure the extremity and com-pare your findings with baseline measure-ments to detect an increase in circumfer-ence. Changes should be reported and docu-mented.
Diagnosis: DVTBecause DVT is often difficult to detect clin-ically, diagnostic studies may be indicated.If the health care provider suspects DVT, hemay order a venous ultrasound of the pa-tient’s legs, magnetic resonance imaging
(MRI), a venogram, or a D-dimer test.
Let’s take a closer look atthese tests.
Duplex venous ultra-sonography, which may beperformed at the bedside, isone of the simplest diagnos-tic tests for DVT. Ultrasoundimagery can reveal a throm-bus in a deep vein; theDoppler ultrasound mea-sures the blood flow velocityin veins and can detect flow abnormalities.Although a duplex study is noninvasive andrelatively simple to perform, its accuracydepends on the technician’s skill. If the ultra-sound is negative for DVT and the healthcare team still suspects that the patient hasDVT, a venogram may be indicated to make
Picturing pulmonary emboliMultiple emboli insmall branches ofleft pulmonary artery
Infarcted area
Large, solid embolus
I spy a thrombus. Webetter head for shore.

34 Nursing made Incredibly Easy! March/April 2008
a definitive diagnosis.MRI is another noninvasive study
that can be used to detect DVT in theproximal deep veins. Whether to use
this test or a venogram depends on thepatient’s clinical findings; MRI is more
useful than venography in patients with sus-pected DVT of the inferior vena cava orpelvic veins.
Although it’s being replaced by ultra-sound, the venogram is still considered bymany health care providers to be the goldstandard for diagnosing DVT. During thisinvasive test, the patient is placed on afluoroscopic table that’s usually tilted 45degrees, and a contrast medium is injectedinto a superficial foot vein. A clinician
observes the flow of contrast medium by
fluoroscopy and takes X-rays; if the con-trast medium doesn’t fill the veins normal-ly, acute DVT is confirmed. Complicationsof venography include hypersensitivityreactions to the contrast medium, acuterenal failure because of the volume of con-trast medium used, and extravasation ofthe contrast medium (especially in patientswith a history of arterial insufficiencybecause of tissue necrosis and ulceration).The risk of acute renal failure is higher inelderly patients and in patients with dia-betes, hyperuricemia, or multiple mye-loma.
A D-dimer test is a blood test to measurefibrin degradation fragments generated byfibrinolysis. An elevated D-dimer level indi-cates a thrombotic process but isn’t specificto DVT. This test is useful as an adjunct tononinvasive testing. If the patient has a lowclinical probability of DVT and a negative D-dimer test, DVT can be ruled out without anultrasound.
It turns out your suspicions were cor-rect—your patient has DVT. What’s the nextstep? Let’s look at treatment options next.
Anticoagulation is A-OK The treatment goals for DVT are to pre-vent the thrombus from growing and frag-menting, which increases the risk of PE; toprevent recurring thrombi; and to let thebody’s own fibrinolytic system work. An-ticoagulant therapy, with unfractionatedheparin, low-molecular-weight heparin(LMWH), or oral anticoagulants such aswarfarin (Coumadin), is the first-line treat-ment. Thrombolytic therapy or the factorXA inhibitor fondaparinux (Arixtra) mayalso be used. Depending on the patient’srisk factors, anticoagulant therapy maylast from 6 months to 1 year if he has idio-pathic DVT or indefinitely if he continuesto have recurring thrombi. Let’s take acloser look.
Unfractionated heparin is administeredby intravenous (I.V.) infusion for 5 to 7days to prevent the growth of a thrombus
sheet
cheat
Superficial veins liejust beneath theskin; they drain
through perforatorveins into deep
veins.
Superficial veins
Perforator veins connect superficial
to deep veins.
Perforator veins
Deep veins receivevenous blood from
perforator veins andreturn it to the heart.
Deep veins
The superficialvein’s connected tothe perforator vein,
the perforatorvein’s connected tothe deep vein...I love
this song!

March/April 2008 Nursing made Incredibly Easy! 35
and the development of new thrombi. Anelectronic infusion device is used to pre-vent the inadvertent infusion of large vol-umes, which can cause hemorrhage.Unfractionated heparin can also be givensubcutaneously to prevent the develop-ment of DVT. The dosage of unfractionatedheparin depends on the patient’s activatedpartial thromboplastin time, internationalnormalized ratio (INR), and platelet count.Heparin is at an effective (therapeutic) levelwhen the patient’s partial thromboplastintime is 1.5 times normal. Patients receivingunfractionated heparin for a long period oftime (several days to weeks) are at risk fora sudden decrease in platelet count (30%)known as heparin-induced thrombocytope-nia (HIT). If HIT develops, heparin must bediscontinued.
Associated with fewer bleeding complica-tions and a lower risk of HIT than unfrac-tionated heparin, LMWH, such as enoxa-parin (Lovenox), may be used instead toprevent thrombus growth and new thrombiformation. Given in one or two subcuta-neous injections per day, doses are adjustedaccording to the patient’s weight and arebased on the specific product and facilityprotocol. LMWH is more expensive thanunfractionated heparin, but it can be usedsafely in pregnant women and patients whotake it may be more mobile.
An oral anticoagulant, such as warfarin(a vitamin K antagonist), is typically admin-istered with heparin therapy. Once the ther-apeutic level is reached, heparin can be dis-continued. If the patient requires long-termtherapy, warfarin is frequently used. Thedosage of warfarin depends on the patient’sprothrombin time and INR; the therapeuticlevel is reached when the patient’s pro-thrombin time is 1.5 to 2 times normal orthe INR is 2 to 3. For more information onwarfarin, prothrombin time, and INR, see“Going with the flow: Warfarin” from ourJuly/ August 2004 issue and “Is this on thelevel?” from our July/August 2006 issue.
Thrombolytic therapy dissolves thrombi
in 50% of patients. A thrombolytic, such asactivase (Alteplase) or reteplase (Retavase),is given within the first 3 days after acutethrombosis. Thrombolytics cause less long-term damage to the venous valves andreduce the incidence of postthrombotic syn-drome; however, they have a higher risk ofbleeding than heparin. If bleeding can’t bestopped, thrombolytic therapy must be dis-continued.
Unlike LMWH, which acts on thrombinand factor Xa, fondaparinux only inhibitsfactor Xa. Because it doesn’t affect platelets,fondaparinux doesn’t cause HIT. Fondapari-nux is given subcutaneously at a fixed doseonce a day and is excreted unchanged by thekidneys; therefore, it must be used with cau-tion in patients with renal insufficiency andit’s contraindicated in patients with renalfailure.
Surgery may be necessary if anticoagulantor thrombolytic therapy is contraindicated,the patient is at high risk for PE, or hisvenous drainage is so compromised that per-manent damage is likely (see When anticoagu-lant therapy is a no-no). Thrombectomy, orremoval of the thrombus, is the procedure of
When anticoagulanttherapy is a no-noAnticoagulant therapy is contraindicated if yourpatient has:• bleeding from the gastrointestinal, genitouri-nary, respiratory, or reproductive systems• hemorrhagic blood dyscrasias• an aneurysm• severe trauma• alcoholism• recent or impending surgery of the eye,spinal cord, or brain• severe liver or kidney disease• recent cerebrovascular hemorrhage• an infection• an open ulcerative wound• an occupation that involves a significant riskfor injury• recently delivered a baby.
Surgerymay bea lastresort.

36 Nursing made Incredibly Easy! March/April 2008
choice under these circumstances. Duringthis procedure, a catheter is used to deliver athrombolytic directly into the clot to dissolve
it. A vena cava filter may also be placedthrough the catheter into the
groin, just below the junctionof the inferior vena cava and
the lowest renal veins, to trap largeemboli and prevent PE. About the
size of a quarter, this filter made ofwire mesh catches any clots that
break off the DVT and head for thelungs via the inferior vena cava. A
vena cava filter for short-term use hasrecently been introduced, designed to beremoved once the increased risk of PEsubsides.
So what can you do to help your patientwho’s receiving anticoagulant therapy?Let’s delve into the care of a patient with
DVT next.
Take care When caring for a patient with DVT, youmust:n monitor for potential complications,such as bleeding or HIT. Spontaneousbleeding anywhere in your patient’s bodyis the most common complication of anti-coagulant therapy. Bleeding from the kid-neys, bruises, nosebleeds, and bleeding
gums are earlysigns of excessiveheparin dosage. Toimmediately re-verse the effects ofheparin, the healthcare provider mayorder I.V. prota-mine sulfate. Prota-mine sulfate ismost effective in re-versing the effectsof unfractionatedheparin, but it mayalso be used in pa-tients receivingLMWH. If your pa-
tient receiving warfarin experiences bleed-ing, the health care provider may orderoral or low-dose I.V. vitamin K or an in-fusion of fresh frozen plasma or pro-thrombin concentrate. HIT is anothercomplication you must watch out for.Early signs and symptoms of HIT includea decreasing platelet count, the need forincreasing doses of heparin to maintainthe therapeutic level, and hemorrhagiccomplications (skin necrosis at the injec-tion site or sites distal to the thrombus,skin discoloration, hematomas, purpura,and blistering). If your patient developsHIT, the health care provider may order adirect thrombin inhibitor, such as I.V. lep-irudin (Refludan) or argatroban. n monitor for drug interactions. If your pa-tient is taking an oral anticoagulant, youmust monitor his medication schedule be-cause many medications and supplementsaccelerate or inhibit the effects of warfarin(see What affects warfarin?). n provide pain relief. Depending on theextent and location of the thrombus, yourpatient may be on bed rest for 5 to 7 days.To promote circulation and increase com-fort, periodically elevate his feet and lowerlegs above his heart. Help him perform ac-tive and passive leg exercises, particularlywith the calf muscles, to increase venousflow. Apply warm, moist packs to the af-fected leg, as ordered, to reduce the dis-comfort of the thrombus. An analgesicmay also be ordered to control pain.n encourage early ambulation. Once he’sambulatory, instruct your patient to avoidsitting for more than 2 hours at a time. Heshould walk at least 10 minutes every 1 to 2hours if possible to help prevent venousstasis.n perform discharge teaching. Educateyour patient about the signs and symp-toms of DVT to report, such as newswelling or increased swelling of the af-fected limb, skin breakdown, pain, andweak or absent pulses. Also teach himthe signs and symptoms of PE, such as
What affects warfarin?
Warfarin to therescue—that’s
Mr. SuperWarfarin to
you!
Increased anticoagulation• Angelica• Celery• Chamomile• Cinchona• Garlic• Ginger• Ginkgo biloba• Grapefruit juice• Horse chestnut• Licorice• Quinine• Sweet clover
Decreased anticoagulation• Broccoli• Cabbage• Collard leaves• Ginseng• Lettuce• Spinach• Stinging nettle• Turnip leaves

March/April 2008 Nursing made Incredibly Easy! 37
shortness of breath,chest pain, bluenail beds, andtachypnea. Instructhim to go to theemergency depart-ment immediatelyif he experiencesany of these symp-toms. Inform yourpatient about therisk of bleeding as-sociated with anti-coagulant therapyand the signs andsymptoms to bealert for, such aschanges in mentalstatus, a racingpulse, and ex-tremely pale skin (see Patient teaching foranticoagulants). If your patient is goinghome on warfarin, tell him to avoid foodshigh in vitamin K, such as avocados,broccoli, brussel sprouts, cabbage, greenonions, liver, and green leafy vegetables.And make sure he understands that he’llneed regular blood draws to monitor hisprothrombin time and INR. If he’s goinghome on unfrac-tionated heparin,he’ll need his par-tial prothrombintime monitored ona monthly basis aswell. If your pa-tient is going homeon LMWH or fon-daparinux, teachhim the propertechnique for sub-cutaneous injec-tions into the ab-domen (2 inchesfrom the umbili-cus) and make surehe knows to rotatethe injection sites.
Have him demonstrate the techniqueback to you. Let him know that it’s com-mon to experience some bruising aroundthe injection sites but to contact his healthcare provider if the bruises begin tospread. Finally, assist your patient withsetting up follow-up appointments, whichmay include a computed axial tomogra-phy scan of his chest to check for PE andmagnetic resonance venography or a ve-nous Doppler scan to monitor the statusof the thrombus.
But how about steps you can take to pre-vent your at-risk patients from developingDVT? Let’s take a minute to review preven-tion strategies.
did youknow?Want to beef upyour practice whenit comes to DVTprevention? Checkout the AmericanAssociation ofCritical-CareNurses’ PracticeAlert for Deep VeinThrombosisPrevention athttp://www.aacn.org/AACN/practiceAlert.nsf/Files/dvt/$file/DVT%20Prevention%2012-2005.pdf.
With treatment, yourpatient’s blood will
flow as free as me inthe sea!
Patient teaching for anticoagulantsTeach your patient who has been prescribed an anticoagulant the following:• Take the anticoagulant at the same time each day, usually between 8 a.m. and 9 a.m.• Because other medications affect the action of anticoagulants, don’t take vitamins, cold medicines,antibiotics, aspirin, mineral oil, or anti-inflammatory drugs without consulting your health care pro-vider.• Avoid alcohol because it may change your body’s response to the anticoagulant.• Avoid food fads, crash diets, or marked changes in eating habits.• Avoid injury that can cause bleeding.• If you experience faintness, dizziness, increased weakness, severe headaches or abdominal pain,reddish or brown urine, red or black stool, any unusual bleeding, nosebleeds, bruises that enlarge, orrash, contact your health care provider immediately.• Contact your health care provider before having dental work or elective surgery and inform the den-tist or surgeon that you’re taking an anticoagulant.• For women, contact your health care provider if you suspect you’re pregnant.• Wear or carry identification indicating the anticoagulant you’re taking.• Keep all appointments for blood tests.

38 Nursing made Incredibly Easy! March/April 2008
Your role in preventionElastic compression stockings, which exertsustained, evenly distributed pressureover the calves to help increase blood flowin the deep veins, are usually ordered forpatients with venous insufficiency to pre-vent DVT. They may be knee-high, thigh-high, or like pantyhose. The health careprovider may order short-stretch elasticwraps instead, which are applied from thetoes to the knee in an overlapping spiralpattern using a one- or two-layer system.Intermittent pneumatic compression de-vices may also be used with elastic com-pression stockings to prevent DVT. Thesedevices consist of plastic knee- or thigh-high leg sleeves attached to air hoses andan electric controller. The leg sleeves fillwith air to apply pressure to the ankle,calf, and thigh.
If your patient is receiving compressiontherapy, inspect his skin for signs of irrita-tion and his calves for tenderness wheneveryou remove the stockings or wraps. Report
any skin changes or tenderness to the healthcare provider immediately.
The moral of the story:PreventionDVT is a serious, but preventable, condi-tion. With diligent care, your patient withDVT will not only recover, but avoid recur-rence as well. And with an eye on preven-tion, your at-risk patients will be less likelyto develop DVT. Now that’s good news! n
Learn more about it Day MW. Recognizing and managing deep vein thrombo-sis. Nursing2003. 33(5):36-42, May 2003. Pathophysiology Made Incredibly Visual! Philadelphia, Pa.,Lippincott Williams & Wilkins, 2008:66-67. Smeltzer SC, et al. Brunner and Suddarth’s Textbook ofMedical-Surgical Nursing, 11th edition. Philadelphia, Pa.,Lippincott Williams & Wilkins, 2007:1004-1010. Surgical Care Made Incredibly Visual! Philadelphia, Pa.,Lippincott Williams & Wilkins, 2007:185. Turka J. Is this on the level? Nursing Made Incredibly Easy!4(4):7-9, July/August 2006. Wound Care Made Incredibly Visual! Philadelphia, Pa.,Lippincott Williams & Wilkins, 2008:107. Zajac PM. Going with the flow: Warfarin. Nursing MadeIncredibly Easy! 2(4):52-57, July/August 2004.
INSTRUCTIONS
In too deep: Understanding deep vein thrombosisDISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any nursing journal published by Lippincott Williams& Wilkins together and deduct $0.95 from the price of each test.• We also offer CE accounts for hospitals and other health care facilities onnursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATIONLippincott Williams & Wilkins, publisher of Nursing made Incredibly Easy!, willaward 2.5 contact hours for this continuing nursing education activity.
LWW is accredited as a provider of continuing nursing education by theAmerican Nurses Credentialing Center’s Commission on Accreditation.
LWW is also an approved provider of continuing nursing education by theAmerican Association of Critical-Care Nurses #00012278 (CERP Category A),District of Columbia, Florida #FBN2454, and Iowa #75. LWW home study activi-ties are classified for Texas nursing continuing education requirements as Type1. This activity is also provider approved by the California Board of RegisteredNursing, Provider Number CEP 11749, for 2.5 contact hours. Your certificate isvalid in all states.
Earn CE credit online: Go to http://www.nursingcenter.com/CE/nmie and receive a certificate within minutes.
TEST INSTRUCTIONS• To take the test online, go to our secure Web site atwww.nursingcenter.com/ce/nmie.• On the print form, record your answers in the test answersection of the CE enrollment form on page 54. Each ques-tion has only one correct answer. You may make copies ofthese forms.• Complete the registration information and course evalu-ation. Mail the completed form and registration fee of$24.95 to: Lippincott Williams & Wilkins, CE Group,2710 Yorktowne Blvd., Brick, NJ 08723. We will mail yourcertificate in 4 to 6 weeks. For faster service, include a faxnumber and we will fax your certificate within 2 businessdays of receiving your enrollment form. Deadline is April 30, 2010.• You will receive your CE certificate of earned contacthours and an answer key to review your results. There is nominimum passing grade.

March/April 2008 Nursing made Incredibly Easy! 39
1. Which of the following is a component of Virchow’striad?a. increased blood flowb. venous stasisc. decreased coagulability
2. A clot that occludes a vessel is calleda. an embolus.b. a thrombus.c. postthrombotic syndrome.
3. Which of the following patients is at highest risk forDVT?a. a nonsmoker undergoing outpatient arthroscopyb. a smoker undergoing knee replacementc. a smoker who’s ambulatory following appendectomy
4. The most reliable physical sign of DVT isa. unilateral pain.b. positive Homans’ sign.c. unilateral edema.
5. Which symptoms are commonly associated withpulmonary embolism (PE)?a. dyspnea and coughb. edema and chest painc. tachycardia and hyperpigmentation
6. Which noninvasive test is useful in diagnosing DVT ofthe inferior vena cava?a. venogramb. Doppler ultrasoundc. magnetic resonance imaging
7. Which statement about the D-dimer test is correct?a. The D-dimer level is checked only after ultrasound confir-
mation of DVT.b. A negative D-dimer and low clinical probability rule out
DVT.c. An elevated D-dimer level is only seen with DVT.
8. A therapeutic partial thromboplastin time (PTT) shouldbea. 3 times normal.b. 2 times normal.c. 1.5 times normal.
9. Heparin-induced thrombocytopenia (HIT) isn’t a concernwhen the patient is anticoagulated usinga. unfractionated heparin.b. enoxaparin.c. fondaparinux.
10. Which statement about the use of enoxaparin iscorrect?a. Enoxaparin is associated with a higher risk of bleeding than
unfractionated heparin.
b. Patients receiving enoxaparin must be on bed rest.c. Enoxaparin is safe for pregnant women.
11. Thrombectomy is most likely to be performed on thepatient whoa. has hemorrhagic blood dyscrasias.b. has a normal D-dimer and low risk for PE.c. has an international normalized ratio of 2.5 on heparin
therapy.
12. Which statement about vena cava filter placement iscorrect?a. It’s placed by a catheter inserted into the subclavian vein. b. It’s a device placed in the inferior vena cava above the
renal veins.c. It’s purpose is to trap emboli headed for the lungs.
13. The most common complication of anticoagulanttherapy isa. drug interactions.b. spontaneous bleeding.c. renal failure.
14. Which of the following can be used to reverse theeffects of heparin?a. I.V. protamine sulfateb. I.V. vitamin Kc. fresh frozen plasma
15. Which isn’t a sign of HIT?a. a 30% drop in platelet countb. the need for smaller doses of heparin to maintain a thera-
peutic PTTc. hematomas and blistering
16. To prevent venous stasis, you instruct your patient toambulate for 10 minutesa. once a day.b. every 8 hours.c. every 1 to 2 hours.
17. Which food should the patient on warfarin avoid?a. broccolib. milkc. red meat
18. Explain to your patient that wearing compressionstockings after discharge will help bya. slowing bleeding from superficial veins.b. increasing blood flow in deep veins.c. mobilizing residual clots in the legs.
In too deep: Understanding deep vein thrombosisGENERAL PURPOSE: To provide the professional nurse with an overview of the pathophysiology, treatment, and prevention of deepvein thrombosis (DVT). LEARNING OBJECTIVES: After reading this article and taking this test, you should be able to: 1. Discuss thepathophysiology, risk factors, and symptoms associated with DVT. 2. List diagnostic tests and treatment options for DVT. 3. Identifynursing interventions for care of the patient with DVT and its complications.
2.5 ANCC/AACN CONTACT HOURS
Turn to page 54 for the CE Enrollment Form.