Embed Size (px)
Citation preview

JCN 2016, Vol 30, No 5 25
A chronic wound is defined as one that does not heal in an orderly sequence or
predictable timeframe and fails to progress along the wound-healing continuum. In the UK alone, there were recently estimated to be 1.3 million chronic wounds, of which 153,000 were pressure ulcers, 253,000 dehisced surgical wounds, 169,000 diabetic foot ulcers and 730,000 leg ulcers (Guest et al, 2015). A leg ulcer is defined as a wound between the knee and the ankle that takes more than two weeks to heal (National Institute for Health and Care Excellence [NICE], 2016).
The cost of wound management to healthcare providers in the UK is estimated to be between £4.5–5.1 billion per year, two-thirds of which is incurred in the community setting. In hospitals it is estimated that between 25–40% of beds are occupied by
Devising a treatment programme to address the challenges of excess exudate
patients with wounds (Posnett et al, 2009). This financial burden can only have a negative impact on the already over-stretched NHS budget, particularly as NHS England’s Five Year Forward View (NHS England, 2014) outlined plans to introduce cost savings to close a funding gap of £30 billion by 2020/21.
The burden of chronic wound management can also put enormous pressure on clinicians, particularly community nurses. Chronic wounds are associated with increased exudate levels, which if not managed properly can lead to a greater risk of wound infection, skin maceration and delayed healing (Tickle, 2016). For the community nurse, wound chronicity leads to more patient appointments and an increased use of resources and wound dressings, with 61-64% of the cost associated with the management of venous leg ulcers, for example, related to community nursing visits (Guest et al, 2015).
Joy Tickle,tissue viability nurse specialist; clinical lead, Shropshire Community NHS Trust
A chronic heavily exuding wound can have a devastating impact on a patient’s quality of life, often resulting in symptoms such as increased pain, depression, anxiety and stress, as well as a loss of independence and social isolation. For community nurses, wounds with high levels of exudate can incur increasing costs, both in time and resources. It is imperative to heal these wounds as quickly as possible and the community nurse should undertake a robust and holistic assessment before implementing a clear and evidence-based management plan, potentially including wound debridement and the use of an effective absorbent dressing in combination with compression therapy, where appropriate, to manage exudate. This article examines the development of chronic wounds and the problem of excess exudate production specifically, before going onto look at the benefits of one particular superabsorbent dressing (Flivasorb®; Activa Healthcare/L&R). The author uses extensive evidence as well as clinical expertise to provide an overview of the dressing, and presents a case study to demonstrate its benefits in practice.
KEYWORDS: Chronic wounds Exudate Superabsorbent dressings
Joy TickleThe biggest burden of chronic
wounds, however, falls on patients and families. As mentioned above, increases in exudate production and bacterial burden can lead to pain, discomfort and anxiety due to increased dressing changes (Edwards, 2013).
Similarly, patients often experience psychosocial problems such as embarrassment and a loss of dignity when a chronic wound leaks exudate and becomes malodorous (Faucher et al, 2012). As well as the emotional impact, a chronic wound will also frequently involve the patient having to wear oversized clothes/footwear to accommodate wound dressings and disguise any exudate leakage, which can impact on mobility (Persoon et al, 2004). Leakage may also impact upon the patient’s everyday household duties as it can increase the amount of laundry and personal hygiene needs, which may be physically challenging for some patients (Tickle, 2016).
CLINICAL CHALLENGES.
It is important that community nurses remember that wound exudate is a natural and vital component of the wound-healing process, which is generated as a part of the natural wound inflammatory response and proliferative phase and, in the author’s experience, is essential for the reparative process. When a wound becomes chronic, however, this can involve changes in the volume and viscosity of wound exudate, resulting in significant clinical challenges for the patient and the community nurse.
Bacterial loadIncreased exudate is associated with the presence of biofilms, surface-attached communities of microorganisms that are encased in a
INSIGHT
Wounds-Activa Insight-read by pic .indd 25 19/10/2016 10:37

26 JCN 2016, Vol 30, No 5
impaired venous return/ lymphatic drainage. This, in turn, can lead to non-healing ulceration, ‘weeping’ oedema, skin excoriation/maceration and increased risk of wound/skin infection (NICE, 2016).
Compression therapy is the ‘gold standard’ treatment for venous leg ulceration and is also effective in the management of lower limb oedema. It is therefore imperative that community nurses implement an effective wound assessment and management plan alongside compression therapy.
WOUND MANAGEMENT
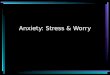
To effectively assess and manage wounds it is essential that community nurses first address all the factors that might act as a barrier to wound healing. The TIME acronym may assist clinicians when considering these barriers (Figure 1), including the presence of non-viable tissue; inflammation and infection;
WOUND CARE
CASE STUDY
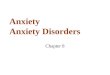
Ms L is a 70-year-old woman with chronic leukaemia who presented to the tissue viability service with a 12-month history of chronic lower limb ulceration. On presentation the wound bed consisted of a combination of sloughy and necrotic tissue with high levels of exudate and malodour, while the limb itself was distorted in shape. Debridement of the wound was difficult due to pain and discomfort experienced by the patient (Figure A). Following assessment, a treatment plan was implemented using a Monofilament Fibre debridement pad (Debrisoft®; Activa Healthcare/L&R) to debride the wound bed with minimal discomfort to the patient. This allowed speedy removal of the devitalised tissue and assisted in reducing bacterial burden.
The author decided to use a superabsorbent dressing (Flivasorb®; Activa Healthcare/L&R), mainly to allow the effective management of the high levels of exudate being produced by the wound and to reduce the amount of dressing
Figure A
strikethrough, which would contribute to improving the patient’s quality of life. The author also began to apply inelastic compression bandaging (Actico®; Activa Healthcare/L&R) to help manage the exudate levels. The conformable properties of the Flivasorb dressing ensured that it it was comfortable underneath the compression therapy and did not affect the sub-bandage pressures exerted by the compression.
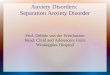
Within two weeks, the wound showed reduced exudate levels, increased granulation tissue and improved periwound skin condition,
while the patient commented that the dressing increased her comfort levels (Figure B). The reduction in exudate levels and management of the patient’s distorted limb shape meant that the compression bandaging could then be changed to a compression hosiery kit (Leg Ulcer Hosiery Kit®; Activa Healthcare/L&R).
This case shows that a reduction in exudate levels when managing leg ulcers can trigger a review not only of the type of dressing selected, but also the type of compression. This can bring about reductions in clinicians’ time and improve quality of life for the patient.
Figure B
strong extracellular matrix formed of carbohydrates, proteins and/or DNA. Biofilms form an extremely effective protective barrier against antibodies, antibiotics and antimicrobial agents (Schultz and Dowsett, 2012), and mature biofilm colonies can form in 2–4 days, perpetuating the inflammatory response and resulting in increased exudate and slough (masses of dead cells that collect in the exudate) and wound degeneration.
This increased exudate and slough escalates the bacterial burden, which increases the risk of critical colonisation and or wound infection (Vowden et al, 2015).
Another consequence of increased exudate and slough is more frequent dressing changes due to exudate strikethrough and leakage, as well as subsequent periwound maceration caused by the enzymes contained within the exudate. Frequent dressing changes can lead to skin stripping (Drewery, 2015), and these types of periwound skin damage can increase pain and discomfort for the patient (Vowden et al, 2015).
Leg ulcerationThe location of the wound may also influence the level of exudate, for example, venous leg ulcers and lower limb oedema involve high fluid volumes due to underlying
Figure 1.The TIME acronym indicates potential barriers to wound healing.
Tissue non-viableInflammation and/or infection
Moisture balanceEpithelial edge advance
T I M E
Wounds-Activa Insight-read by pic .indd 26 19/10/2016 10:37
WOUND CARE
28 JCN 2016, Vol 30, No 5
In cases of lower limb oedema, particularly where exudate or leaking is a challenge, cohesive inelastic bandages are recommended as they reduce oedema more quickly than elastic bandages, therefore having a positive impact on exudate reduction (Atkin and Tickle, 2016). This is due to the higher standing and working pressure and lower resting pressure of inelastic systems (e.g. Actico®, Activa Healthcare/L&R), which improves patient comfort at the same time as increasing the effectiveness of the calf muscle pump (where the muscles in the calf help to return blood to the heart during walking) (Wounds UK, 2014).
Hosiery kitsWhen limb distortion and exudate volumes have been successfully reduced with compression bandaging, the patient can be stepped across to an effective alternative such as a leg ulcer hosiery kit. The use of hosiery kits has been endorsed by a recent randomised control trail, the Venus IV trial, which highlighted that the use of active compression hosiery kits are a viable and cost-effective alternative to graduated compression bandages, with the added benefit of reducing recurrence rates, an effect believed to be related to the promotion of patient self-care (Ashby et al, 2014).
Dressing selectionMoist wound healing is essential and requires a balance between excessive moisture and the wound bed becoming too dry (White and Cutting, 2006). Effective dressing selection is an important component in achieving this balance.
It is essential that the community nurse fully understands that dressing selection should be tailored to the condition of the wound and the type and amount of exudate being produced (Dowsett, 2012); furthermore, they should understand the composition and mode of action of dressings that have been designed to manage exudate so that they can select the most appropriate dressing and apply it effectively and efficiently. For example, while foam dressings are commonly used to control exudate, their fluid-handling capacity may be inadequate, which can mean the
biofilm disruption (Vowden and Vowden, 2011).
In a recent survey of 475 clinicians, 87% reported that exudate production reduced in a very short period of time when following a two-week biofilm pathway incorporating Debrisoft. This is most likely because the biofilm had been managed (Morris et al, 2016).
Skin careMaintaining healthy skin is also extremely important. Patients with lower limb conditions such as oedema, or underlying venous or lymphatic complications may present with skin changes such as hyperkeratosis (dry scaly areas of skin), dermatitis and cellulitis, which, if not managed effectively can lead to leaking ‘weepy’ limbs and chronic ulceration. These symptoms can be managed with regular cleansing and debridement, lower limb elevation, and compression therapy (Scottish Intercollegiate Guidelines Network [SIGN], 2010).
Compression therapyCompression therapy using either bandages or hosiery is designed to support the veins in the lower limb and increase circulation in the legs. Compression is fundamental to controlling lower limb oedema, managing venous ulceration and skin changes, and reducing exudate. Compression also improves limb shape and reduces wound size.
Before beginning compression, however, it is imperative that the community nurse undertakes a robust assessment of the patient and their wound/skin, as well as performing a vascular assessment to make sure there are no contraindications, such as arterial disease.
The choice of compression therapy will depend upon the outcomes of the assessment, the clinician’s knowledge and skills, the available resources and patient choice. For example, assessment may indicate that a patient with a heavily exuding wound initially requires compression bandaging; whereas lower exudate levels may be more suited to a hosiery kit.
uncontrolled moisture balance (too much or too little moisture in the wound); and any changes in the wound edges or surrounding skin.
DebridementDevitalised tissue must be effectively debrided to assist tissue repair (Strohal et al, 2013); not only does this optimise wound healing, but it also allows the clinician to have a clearer picture of the wound and surrounding skin (Stephen-Haynes and Callaghan, 2012). Devitalised tissue (including necrosis and slough) may lead to increased bacterial bioburden/infection, malodour and increased pain and distress for patients, all of which impede wound healing.
Once the wound has been successfully debrided, the community nurse is able to: Assess the tissue type(s) within
the wound Record the wound size and depth Assess the condition of the
periwound skin/tissue.
By obtaining a clearer picture of the wound’s status, an appropriate and timely treatment regimen can be implemented. When considering which method of debridement to use, e.g. mechanical, sharp or autolytic, it is important that the community nurse chooses one that is effective, safe, and acceptable to the patient.
Newer mechanical debridement tools use Monofilament Fibre Technology TM (Debrisoft®; Debrisoft® Lolly; Activa Healthcare/L&R) to effectively remove dead tissue, slough and hyperkeratosis, facilitating gentle debridement within minutes. From the author’s clinical experience, all staff (and carers/patients) can successfully debride wounds/skin using monofilament fibre pads due to their simplicity. As well as the clinical benefits, using monofilament fibre pads can reduce nursing time and promote increased skill-mix within the clinical team as different levels of staff are able to use them (NICE, 2014; Tickle, 2016).
Early and regular wound debridement is likely to accelerate wound healing and is associated with reductions in odour, bacterial burden, slough and exudate as a result of
Wounds-Activa Insight-read by pic .indd 28 19/10/2016 10:37
30 JCN 2016, Vol 30, No 5
WOUND CARE
nurse needs to perform more frequent dressing changes; also, foam dressings may struggle to contain fluid under pressure, eg under compression bandaging (Jones, 2016).
Wound dressings vary in the way they absorb and retain exudate, for example, simple absorptive dressing materials take up fluid into spaces in their structure by wicking the exudate laterally, across the dressing (or in
some cases vertically into the dressing) and are aided by moisture vapour transmission (a type of evaporation). However, to help solve the problem of fluid retention within the dressing, other products form a gel or use fibres/particles to trap or ‘lock-in’ exudate and its components (e.g. bacteria and proteases), helping to influence the composition of exudate in the wound (World Union of Wound Healing Societies [WUWHS], 2007).
Often, dressing products combine different materials, and techniques resulting in a wide range of products that vary considerably in their fluid-handling characteristics and abilities (Romanelli et al, 2010). It is particularly important that community nurses consider a dressing that retains fluid effectively when it is used under compression. If not, the pressure may cause fluid to leak from any dressing used, causing the harmful exudate to make contact with the wound/skin.
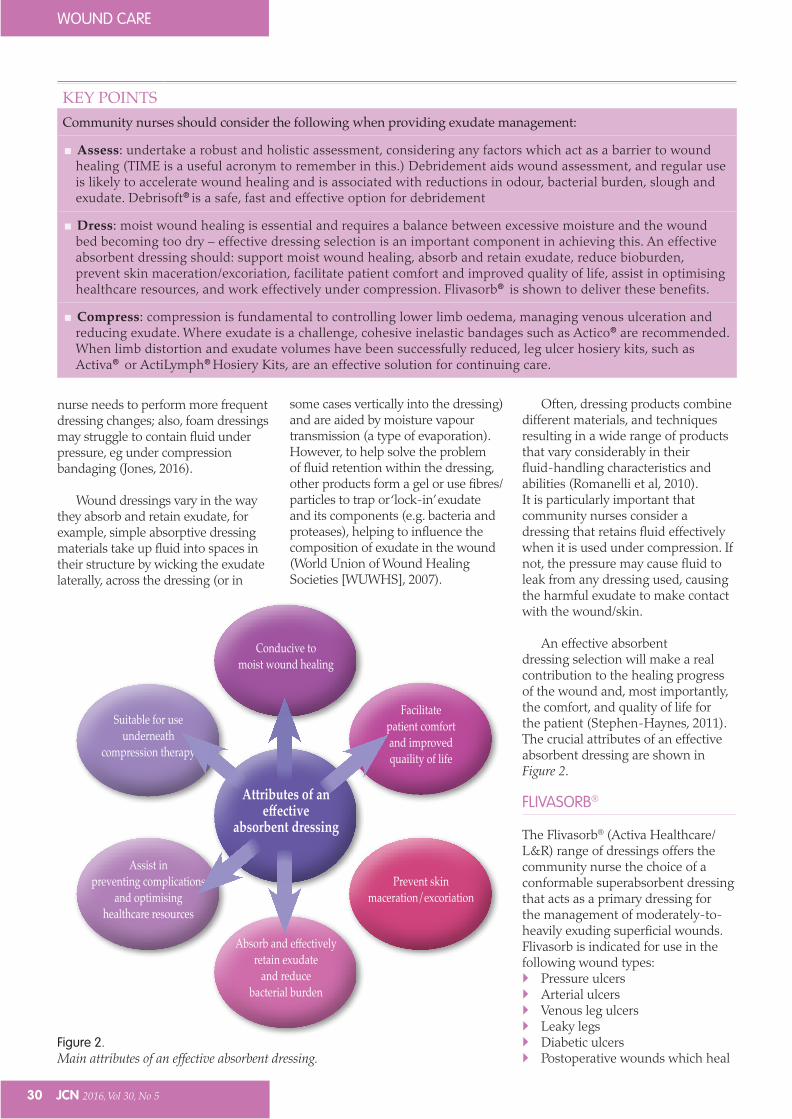
An effective absorbent dressing selection will make a real contribution to the healing progress of the wound and, most importantly, the comfort, and quality of life for the patient (Stephen-Haynes, 2011). The crucial attributes of an effective absorbent dressing are shown in Figure 2.
FLIVASORB®
The Flivasorb® (Activa Healthcare/L&R) range of dressings offers the community nurse the choice of a conformable superabsorbent dressing that acts as a primary dressing for the management of moderately-to-heavily exuding superficial wounds. Flivasorb is indicated for use in the following wound types: Pressure ulcers Arterial ulcers Venous leg ulcers Leaky legs Diabetic ulcers Postoperative wounds which heal
Figure 2.Main attributes of an effective absorbent dressing.
Conducive to moist wound healing
Attributes of an effective
absorbent dressing
Absorb and effectively retain exudate
and reduce bacterial burden
Facilitate patient comfort and improved quaility of life
Prevent skin maceration/excoriation
Assist in preventing complications
and optimising healthcare resources
Suitable for use underneath
compression therapy
KEY POINTSCommunity nurses should consider the following when providing exudate management:
Assess: undertake a robust and holistic assessment, considering any factors which act as a barrier to wound healing (TIME is a useful acronym to remember in this.) Debridement aids wound assessment, and regular use is likely to accelerate wound healing and is associated with reductions in odour, bacterial burden, slough and exudate. Debrisoft® is a safe, fast and effective option for debridement
Dress: moist wound healing is essential and requires a balance between excessive moisture and the wound bed becoming too dry – effective dressing selection is an important component in achieving this. An effective absorbent dressing should: support moist wound healing, absorb and retain exudate, reduce bioburden, prevent skin maceration/excoriation, facilitate patient comfort and improved quality of life, assist in optimising healthcare resources, and work effectively under compression. Flivasorb® is shown to deliver these benefits.
Compress: compression is fundamental to controlling lower limb oedema, managing venous ulceration and reducing exudate. Where exudate is a challenge, cohesive inelastic bandages such as Actico® are recommended. When limb distortion and exudate volumes have been successfully reduced, leg ulcer hosiery kits, such as Activa® or ActiLymph® Hosiery Kits, are an effective solution for continuing care.
Wounds-Activa Insight-read by pic .indd 30 19/10/2016 10:37
JCN 2016, Vol 30, No 5 31
WOUND CARE
by secondary intention Fistula exit sites.
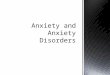
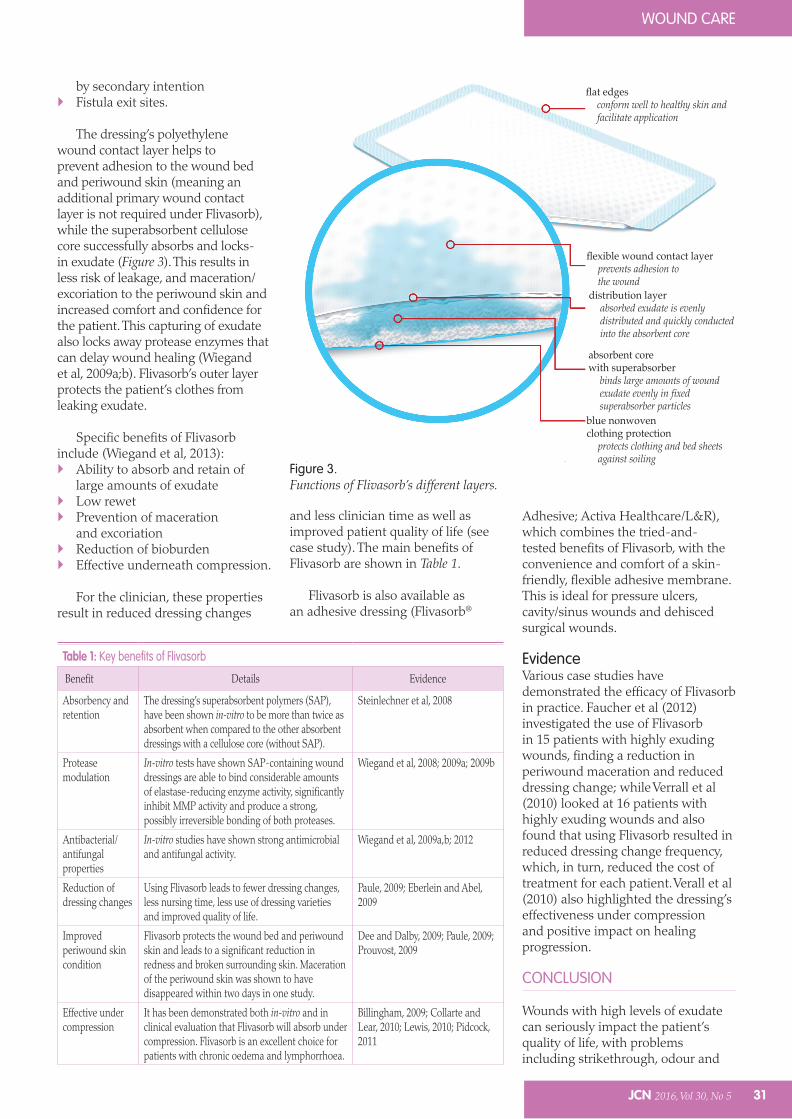
The dressing’s polyethylene wound contact layer helps to prevent adhesion to the wound bed and periwound skin (meaning an additional primary wound contact layer is not required under Flivasorb), while the superabsorbent cellulose core successfully absorbs and locks-in exudate (Figure 3). This results in less risk of leakage, and maceration/excoriation to the periwound skin and increased comfort and confidence for the patient. This capturing of exudate also locks away protease enzymes that can delay wound healing (Wiegand et al, 2009a;b). Flivasorb’s outer layer protects the patient’s clothes from leaking exudate.
Specific benefits of Flivasorb include (Wiegand et al, 2013): Ability to absorb and retain of
large amounts of exudate Low rewet Prevention of maceration
and excoriation Reduction of bioburden Effective underneath compression.
For the clinician, these properties result in reduced dressing changes
and less clinician time as well as improved patient quality of life (see case study). The main benefits of Flivasorb are shown in Table 1.
Flivasorb is also available as an adhesive dressing (Flivasorb®
Adhesive; Activa Healthcare/L&R), which combines the tried-and-tested benefits of Flivasorb, with the convenience and comfort of a skin-friendly, flexible adhesive membrane. This is ideal for pressure ulcers, cavity/sinus wounds and dehisced surgical wounds.
EvidenceVarious case studies have demonstrated the efficacy of Flivasorb in practice. Faucher et al (2012) investigated the use of Flivasorb in 15 patients with highly exuding wounds, finding a reduction in periwound maceration and reduced dressing change; while Verrall et al (2010) looked at 16 patients with highly exuding wounds and also found that using Flivasorb resulted in reduced dressing change frequency, which, in turn, reduced the cost of treatment for each patient. Verall et al (2010) also highlighted the dressing’s effectiveness under compression and positive impact on healing progression.
CONCLUSION
Wounds with high levels of exudate can seriously impact the patient’s quality of life, with problems including strikethrough, odour and
Table 1: Key benefits of Flivasorb
Benefit Details Evidence
Absorbency and retention
The dressing’s superabsorbent polymers (SAP), have been shown in-vitro to be more than twice as absorbent when compared to the other absorbent dressings with a cellulose core (without SAP).
Steinlechner et al, 2008
Protease modulation
In-vitro tests have shown SAP-containing wound dressings are able to bind considerable amounts of elastase-reducing enzyme activity, significantly inhibit MMP activity and produce a strong, possibly irreversible bonding of both proteases.
Wiegand et al, 2008; 2009a; 2009b
Antibacterial/antifungal properties
In-vitro studies have shown strong antimicrobial and antifungal activity.
Wiegand et al, 2009a,b; 2012
Reduction of dressing changes
Using Flivasorb leads to fewer dressing changes, less nursing time, less use of dressing varieties and improved quality of life.
Paule, 2009; Eberlein and Abel, 2009
Improved periwound skin condition
Flivasorb protects the wound bed and periwound skin and leads to a significant reduction in redness and broken surrounding skin. Maceration of the periwound skin was shown to have disappeared within two days in one study.
Dee and Dalby, 2009; Paule, 2009; Prouvost, 2009
Effective under compression
It has been demonstrated both in-vitro and in clinical evaluation that Flivasorb will absorb under compression. Flivasorb is an excellent choice for patients with chronic oedema and lymphorrhoea.
Billingham, 2009; Collarte and Lear, 2010; Lewis, 2010; Pidcock, 2011
Figure 3.Functions of Flivasorb’s different layers.
flat edgesconform well to healthy skin and facilitate application
flexible wound contact layerprevents adhesion to the wound
distribution layerabsorbed exudate is evenly distributed and quickly conducted into the absorbent core
absorbent core with superabsorber
binds large amounts of wound exudate evenly in fixed superabsorber particles
blue nonwoven clothing protection
protects clothing and bed sheets against soiling
Wounds-Activa Insight-read by pic .indd 31 19/10/2016 10:37

32 JCN 2016, Vol 30, No 5
WOUND CARE
periwound skin maceration. This also involves increasing costs for community nurses, both in terms of their own clinical time and wider healthcare resources.
It is important to heal these wounds as quickly as possible and the community nurse needs to understand how to perform an holistic wound assessment before implementing an evidence-based management plan, including wound debridement and the the use of an effective absorbent dressing and, where appropriate, compression therapy to manage exudate (see key points box).
This author has examined the development of chronic wounds and the problem of excess exudate production specifically, before looking at the benefits of the superabsorbent dressing Flivasorb, which has been shown to demonstrate enhanced exudate control, reduced nursing time and periwound skin maintenance. JCN
The Assess Dress Compress concept has been developed by Activa Healthcare/L&R.
REFERENCES
Ashby RL, Gabe R, Ali S, et al (2014)
VenUS IV (Venous leg Ulcer Study IV)
- compression hosiery compared with
compression bandaging in the treatment
of venous leg ulcers: a randomised
controlled trial, mixed-treatment
comparison and decision-analytic model.
Health Technol Assess 18(57): 1–293
Atkin L, Tickle J (2016) A new pathway for
lower limb ulceration. Wounds UK 12(2): 32–6
Billingham R (2009) The management
of Lymphorrhoea with Flivasorb®
and Actico®. Available online: www.
activahealthcare.co.uk/casestudies-files/
FS009-R-Billingham-The-management-
of-Lymphorrhoea-with-F.pdf
Collarte and Lear, 2010 http://www.
activahealthcare.co.uk/casestudies-files/
FS018-Collarte-and-Lear-Use-of-
superabsorbent-and-antimicrob.pdf
Dee and Dalby, 2009 http://www.
activahealthcare.co.uk/casestudies-files/
FS010-A-Dee-The-use-of-Flivasorb-in-
a-highly-exuding-wou.pdf .
Drewery K (2015) Is Kliniderm foam silicone
a suitable, cost-saving alternative to
other silicone foam dressings? Wounds
UK 11(2): 98
Dowsett C (2012) Management of wound
exudate. Independent Nurse Available
online: www.independentnurse.co.uk
(accessed October 7, 2016)
Edwards J (2013) Dealing with wound-
related pain at dressing change. J Comm
Nurs 27(4): 36–42
Faucher N, Safar H, Baret M, et al (2012)
Superabsorbent dressings for copiously
exuding wounds. Br J Nurs 21(Suppl 12): S22–8
Guest JF, Ayoub N, McIlwraith T, Uchegbu
I, Gerrish A, Weidlich D, Vowden K,
Vowden P (2015) Health economic
burden that different wound types
impose on the UK’s National Health
Service. Available online: http://bmjopen.
bmj.com (accessed 7 October, 2016)
Eberlein T, Abel M (2009) Superabsorbent
wound dressings in clinical practice:
problem solving in heavy exuding
wounds. Available online: www.
activahealthcare.co.uk/casestudies-files/
FS012-Eberlein_-Abel-Superabsorbent-
wound-dressings-in-c.pdf
Jones J (2012) Flivasorb & Flivasorb Adhesive:
how to guide. Wound Essentials Available
online: www.wounds-uk.com (accessed 7
October, 2016)
Lewis M (2010) Chronic oedema — a
patient’s perpetual journey for treatment.
Available online: www.activahealthcare.
co.uk/casestudies-files/A062-M-Lewis-
Chronic-Oedema-A-patients-perpetual-
jour.pdf
Lurton Y (2011) Superabsorbent dressings for
exudate control. Available online: www.
activahealthcare.co.uk/casestudies-files/
FS022-Superabsorbent_dress.pdf
Morris C, Timmons J, Sykes R (2016) The
management of chronic wound biofilm
with a monofilament fibre debridement
biofilm pathway: results of an audit.
Poster presented at The World Union of
Wound Healing Societies - Florence, Italy
NICE (2014) The Debrisoft monofilament
debridement pad for use in acute or
chronic wounds. Available online: www.
nice.org.uk (accessed 7 October, 2016)
NICE (2016) Leg ulcer — venous. Available
online: http://cks.nice.org.uk/leg-ulcer-
venous#!topicsummary (accessed 7
October, 2016)
NHS England (2014) Five Year Forward View.
Available online: www.england.nhs.uk
(accessed 7 October, 2016)
Paule A (2009) The Management of Maceration
in a Nursing Home Environment. Available
online: www.activahealthcare.co.uk/
casestudies-files/SXP021-A-Paule-
The-management-of-maceration-in-a-
Nursing.pdf
Persoon A, Heinen MM, van der Vleuten
CJM, et al (2004) Leg ulcers: a review
of their impact on daily life. J Clin Nurs
13(3): 341–54
Pidcock (2011) Lymphovenous disease: a
condition for life...not suffering for life.
Available online: www.activahealthcare.
co.uk/casestudies-files/A069-L-Pidcock-
Lymphovenous-disease-A-condition-
for-li.pdf
Prouvost L (2009) The performance of
a superabsorbent dressing in the
management of exudate and maceration.
Available online: www.activahealthcare.
INSIGHT...for individual e-learning and
CPD time
Why not go online and take your individual learning further by testing your knowledge of this topic in the INSIGHT section of the new, FREE JCN e-learning zone (www.jcn.co.uk/learning-zone)?
If you answer the accompanying online questions correctly, you can download a certificate to show that you have completed this JCN e-learning unit on excess exudate.
Then, add the article and certificate to your free JCN revalidation e-portfolio, as evidence of your continued learning — safely, securely and all in one place: www.jcn.co.uk/revalidation
Also, for further e-learning opportunities, why not check out our online Products in Practice learning modules on Flivasorb® and Debrisoft® by visiting: www.jcn.co.uk/learning-zone
Wounds-Activa Insight-read by pic .indd 32 19/10/2016 10:37

34 JCN 2016, Vol 30, No 5
WOUND CARE
co.uk/casestudies-files/FS017-L-
Prouvost-The-performance-of-a-
superabs_dressing-.pdf
Posnett J, Gottrup F, Lundgren H, Saal G
(2009) The resource impact of wounds on
healthcare providers in Europe. J Wound
Care 18(4): 154-61
Romanelli M, Vowden K, Weir D (2010)
Exudate Management Made Easy. Available
online: www.woundsinternational.com
(accessed 7 October, 2016)
Schultz G Dowsett, C (2012) Wound
Bed Preparartion revisited.Wounds
International 391: 27–9
SIGN (2010) Management of chronic venous
leg ulcers: a national clinical guideline.
Available online: www.sign.ac.uk
(accessed 7 October, 2016)
Stephen-Haynes J (2011) Managing exudate
and the key requirements of absorbent
dressings. Br J Community Nurs 16(3 Suppl): S44–9
Stephen-Haynes J, Callaghan R (2012) The
role of an active debridement system
in assisting the experienced clinician to
undertake an assessment and determine
appropriate wound management
objectives. Clinical poster presented at
EWMA, 2012.
Steinlechner E, Rohrer C, Abel M (2008)
Absorbent dressings with superabsorbent
polymers: a new generation of wound
dressings. Available online: www.
activahealthcare.co.uk/casestudies-files/
FS001-Steinlechner-et-al-Absorbent-
dressings-with-supera.pdf
Tickle J (2016) A new pathway for lower
limb ulceration. Wounds UK Available
online: www.wounds-uk.com (accessed 7
October, 2016)
Verrall D, Coulbourn A, Bree-Aslan C (2010)
Evaluating a super-absorbent dressing
(Flivasorb) in heavily exuding wounds. Br
J Nurs 19(7): 449–53
Vowden K, Vowden P (2011) Debridement
Made Easy. Available online: www.
wounds-uk.com (accessed 7 October,
2016)
Vowden P, Bond E, Meuleneire F (2015)
Managing high viscosity exudate. Wounds
International Available online: http://
www.woundsinternational.com (accessed
October 7, 2016)
White R, Cutting K (2006) Modern exudate
management: a review of wound
treatments. World Wide Wounds Available
online: www.worldwidewounds.com
(accessed October 7, 2016)
Wiegand C, Abel M, Ruth P, Hipler UC (2008)
The superabsorber Vliwasorb® irreversibly
absorbs proteases, which delay the
healing process (elastase, MMP-2).
Available online: www.activahealthcare.
co.uk/casestudies-files/FS002-
Wiegand C, Abel M, Ruth P, Hipler UC
(2009a) Polyacrylate-superabsorber binds
inflammatory proteases in vitro Available
online: www.activahealthcare.co.uk/
casestudies-files/FS003-Wiegand-et-al-
Polyacrylate-superabsorbers-bind-inf.pdf
Wiegand C, Abel M, Ruth P, Hipler UC
(2009b) A polyacrylate-superabsorber
inhibits the formation of ROS/RNS
in-vitro. Available online: www.
activahealthcare.co.uk/casestudies-files/
FS013-Wiegand-A-polyacrealate-
superabsorber.pdf
Wiegand C, Abel M, Muldoon J, et al (2013)
SAP-containing dressings exhibit
sustained antimicrobial effects over 7
days in vitro. J Wound Care 22(3): 120–7
Wounds UK (2014) Two-component
compression: Concordance, evidence and
clinical use. Wounds UK Available online:
www.activahealthcare.co.uk (accessed
October 11, 2016)
WUWHS (2007) Wound exudate and the role of
dressings: a consensus document. Available
online: www.woundsinternational.com
(accessed October 11, 2016)
Call our customer care line: 08450 606707 (International enquiries: +44 1283 576800)or visit our website at: www.activahealthcare.co.ukActiva Healthcare Ltd, 1 Wellington Court, Newborough Road, Needwood, Burton-upon-Trent, Staffordshire DE13 9PS.Activa® is the registered trademark of Activa Healthcare Ltd. ADV119 V1.3
Flivasorb®
superabsorbentwound dressing
Same SuperDressing at itsLowest Price
Ever!
Ideal for wet conditions
Helping you manageexudate and your budget
Flivasorb half page advert (JCN) ADV119 V1.3.qxp_Flivasorb half page advert (JCN) ADV119 V1.3 06/10/2016 12:55 Page 1
Wounds-Activa Insight-read by pic .indd 34 19/10/2016 10:37