Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1990;53:244-246
Disappearing brain lesions, psychosis andepilepsy: a report of two cases
Anthony Feinstein, Maria Ron, Simon Wessely
AbstractThe association between disappearingbrain lesions, psychosis and epilepsy intwo patients is reported for the first time.Mechanisms to explain the underlyingpathogenesis are postulated.
In primary generalised epilepsy, imagingprocedures seldom detect structural ab-normalities that correlate with areas of alteredcerebral function. Thus Gastaut and Gastaut,'reporting on 401 computed tomography (CT)scans in a sample of 500 consecutive patientswith epilepsy, found 900o of their 73 patientswith primary generalised epilepsy (idiopathic)to have normal brain scans. The percentage ofpositive scans, however, rose to 61 00 and 630ofor secondary generalised and partial seizuresrespectively, the CT abnormalities reflectingthe presence of demonstrable brain pathology,such as atrophy or space occupying lesions.More unusual is the presence of well demar-cated, often contrast enhancing, lesions thatappear during various types of ictal activity anddisappear either spontaneously, or in responseto the control of seizure activity brought aboutby anticonvulsant drugs alone,2-5 or with theaddition of steroids.6
In the reports no mention has been made ofany psychiatric symptomatology occurring inthese patients. We report two such cases ofdisappearing lesions on CT, who in addition totheir seizures, presented with grossly abnormalmental states. To our knowledge, this is thefirst report linking psychosis, epilepsy and thedisappearing lesions on CT.
Institute of Neurology,Queen Square,LondonA FeinsteinThe National Hospitalfor Nervous Diseases,and Institute ofNeurology, QueenSquare, LondonM RonThe Institute ofPsychiatry, DeCrespigny Park,LondonS Wessely
Correspondence to:Dr Anthony Feinstein,Institute of Neurology,Queen Square House,Queen Square, LondonWC1N 3BC, UnitedKingdom.Received 27 June 1989.Accepted 6 September 1989
Case 1
A previously healthy 50 year old bus conduc-tress with no past psychiatric history, graduallydeveloped paranoid ideas with associated de-pressive features (anorexia, weight loss anddisturbed sleep with early morning waking).She described voices commenting about hercritically in the third person, and felt guiltyabout the allegations the voices made, namelythat she was "dirty" and had had an extramarital affair. Her husband reported that dur-ing the previous two years she had becomeincreasingly tense and withdrawn.The patient's mother died giving birth but
the patient herself did not suffer any obstetriccomplications. There was no documented his-tory of mental illness in the family. Her up-bringing and work record were uneventful.
She responded well to a period of inpatientpsychiatric care during which perphenazine
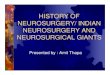
and a tricyclic antidepressant were prescribed.Full insight into her condition returned. Aweek after her discharge from hospital sheagain became deluded, while being treated foran upper respiratory tract infection. Ten daysafter this, she had two generalised convulsions.Neurological examination revealed no localis-ing signs, but CT showed a contrast enhancingleft fronto-temporal mass initially thought tobe a tumour (fig 1A). She was given dexa-methasone and phenytoin 100 mgm three timesa day and had no further epileptic attacks. Fourweeks after the initial scan a repeat scan was
normal (fig IB), the dexamethasone was dis-continued and her mental state returned tonormal. However, four months later paranoiddelusions returned. The patient believed herpremises were bugged and that she was beingpersecuted. She was readmitted to hospital.On examination, the only positive findings
were a fine rotatory nystagmus on lateral gaze,
more pronounced when looking to the right,and a mild gait ataxia. She appeared suspiciousand tense but cooperative. Her speech was
rapid with occasional loosening of associationsand her mood was normal. Paranoid delusionsof a persecutory nature, and auditory halluci-nations in the third person were elicited. APresent State Examination (PSE)7 carried outretrospectively, gave a Catego subclass of"nuclear schizophrenia".The results of the investigations were as
follows: FBC, ESR, urea and electrolytes,LFT's, VDRL, serum phenytoin, T4, andTSH were all normal. A baseline prolactin was2465 mU/ml (normal range = 118-500 mU/ml). Repeat CT showed no recurrence of theoriginal lesion. An EEG showed a left temporalslow wave abnormality but no epileptiformactivity. Psychometric testing revealed no sig-nificant change compared to 10 months earlierwhen she first became ill. She was functioningat the lower level of the normal IQ range andthere was no evidence to suggest that thisrepresented any intellectual decline.She responded well to pimozide 20 mg daily
and her mental state again returned to normal.She has remained seizure free over the pasteight years, and although mild paranoid symp-toms have occasionally returned, these have notwarranted admission. She has not taken medi-cation for the past four years.
Case 2A previously well, 22 year old unmarried hotelreceptionist suddenly developed Jacksoniantype seizures affecting the right side of herbody. As the attacks increased in frequency,
244
on April 5, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.3.244 on 1 M
arch 1990. Dow
nloaded from
Disappearing brain lesions, psychosis and epilepsy: a report of two cases
a-"
Fig IA Ring enhancinglesion in the left fronto-temporal area seen oninitial CT (within 48hours of seizure onset).
Fig IB Repeat CTcarried out one monthafter thefirst, showingresolution of the lesion.
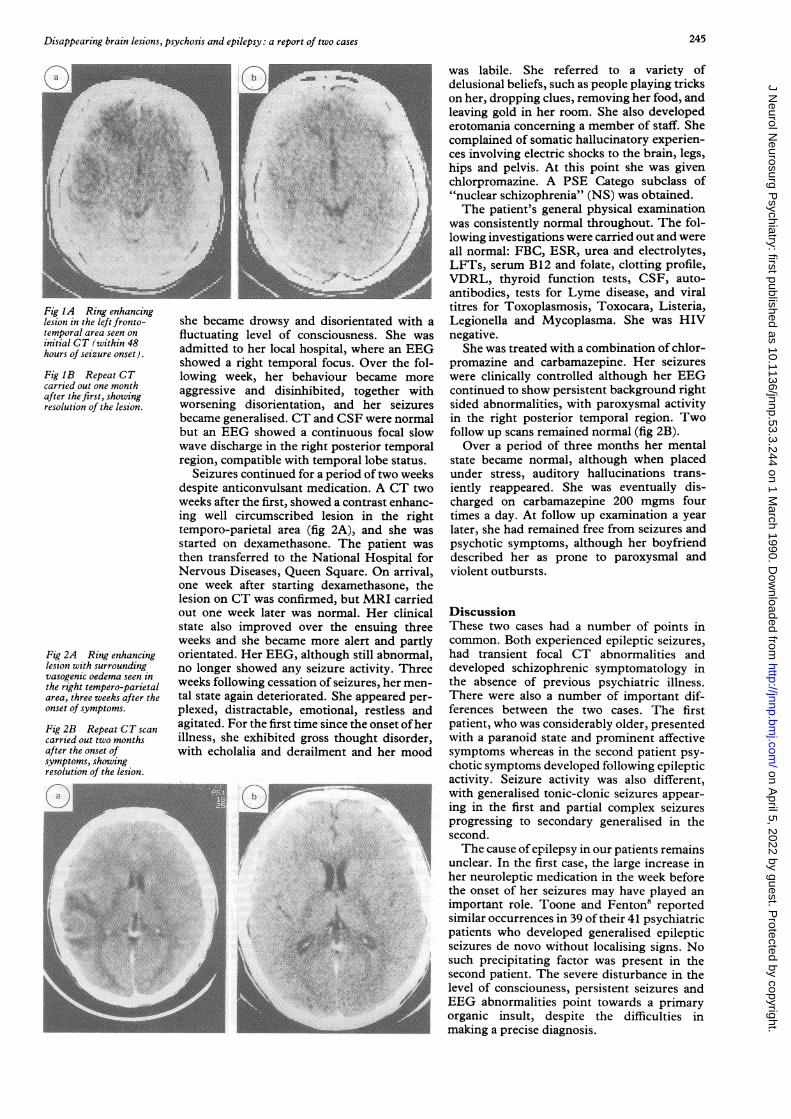
Fig 2A Ring enhancinglesion with surroundingvasogenlc oedema seen inthe right tempero-parietalarea, three weeks after theonset of symptoms.
Fig 2B Repeat CT scancarried out two monthsafter the onset ofsymptoms, showingresolution of the lesion.
/
i;
she became drowsy and disorientated with a
fluctuating level of consciousness. She was
admitted to her local hospital, where an EEGshowed a right temporal focus. Over the fol-lowing week, her behaviour became more
aggressive and disinhibited, together withworsening disorientation, and her seizuresbecame generalised. CT and CSF were normalbut an EEG showed a continuous focal slowwave discharge in the right posterior temporalregion, compatible with temporal lobe status.
Seizures continued for a period of two weeksdespite anticonvulsant medication. A CT twoweeks after the first, showed a contrast enhanc-ing well circumscribed lesion in the righttemporo-parietal area (fig 2A), and she wasstarted on dexamethasone. The patient was
then transferred to the National Hospital forNervous Diseases, Queen Square. On arrival,one week after starting dexamethasone, thelesion on CT was confirmed, but MRI carriedout one week later was normal. Her clinicalstate also improved over the ensuing threeweeks and she became more alert and partlyorientated. Her EEG, although still abnormal,no longer showed any seizure activity. Threeweeks following cessation of seizures, her men-tal state again deteriorated. She appeared per-
plexed, distractable, emotional, restless andagitated. For the first time since the onset ofherillness, she exhibited gross thought disorder,with echolalia and derailment and her mood,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
.9
.IIL.
...,...,X5t g.o !/,,: 1F t ..~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...6g ....
was labile. She referred to a variety ofdelusional beliefs, such as people playing trickson her, dropping clues, removing her food, andleaving gold in her room. She also developederotomania concerning a member of staff. Shecomplained of somatic hallucinatory experien-ces involving electric shocks to the brain, legs,hips and pelvis. At this point she was givenchlorpromazine. A PSE Catego subclass of"nuclear schizophrenia" (NS) was obtained.The patient's general physical examination
was consistently normal throughout. The fol-lowing investigations were carried out and wereall normal: FBC, ESR, urea and electrolytes,LFTs, serum B12 and folate, clotting profile,VDRL, thyroid function tests, CSF, auto-antibodies, tests for Lyme disease, and viraltitres for Toxoplasmosis, Toxocara, Listeria,Legionella and Mycoplasma. She was HIVnegative.
She was treated with a combination of chlor-promazine and carbamazepine. Her seizureswere clinically controlled although her EEGcontinued to show persistent background rightsided abnormalities, with paroxysmal activityin the right posterior temporal region. Twofollow up scans remained normal (fig 2B).Over a period of three months her mental
state became normal, although when placedunder stress, auditory hallucinations trans-iently reappeared. She was eventually dis-charged on carbamazepine 200 mgms fourtimes a day. At follow- up examination a yearlater, she had remained free from seizures andpsychotic symptoms, although her boyfrienddescribed her as prone to paroxysmal andviolent outbursts.
DiscussionThese two cases had a number of points incommon. Both experienced epileptic seizures,had transient focal CT abnormalities anddeveloped schizophrenic symptomatology inthe absence of previous psychiatric illness.There were also a number of important dif-ferences between the two cases. The firstpatient, who was considerably older, presentedwith a paranoid state and prominent affectivesymptoms whereas in the second patient psy-chotic symptoms developed following epilepticactivity. Seizure activity was also different,with generalised tonic-clonic seizures appear-ing in the first and partial complex seizuresprogressing to secondary generalised in thesecond.The cause ofepilepsy in our patients remains
unclear. In the first case, the large increase inher neuroleptic miedication in the week beforethe onset of her seizures may have played animportant role. Toone and Fenton8 reportedsimilar occurrences in 39 of their 41 psychiatricpatients who developed generalised epilepticseizures de novo without localising signs. Nosuch precipitating factor was present in thesecond patient. The severe disturbance in thelevel of consciouness, persistent seizures andEEG abnormalities point towards a primaryorganic insult, despite the difficulties inmaking a precise diagnosis.
245
IN -7 .7.N, ..!M(-u-, .)
-Y.
". ..:.
on April 5, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.3.244 on 1 M
arch 1990. Dow
nloaded from

Feinstein, Ron, Wessely
Although it is uncommon for schizophreniato begin at the age of 50, it seems likely that inour first patient this was the primary diagnosis.The fact that she has had no subsequentseizures, and that she has been intermittentlypsychotic over the years, would support thisassumption. In our second patient, however,the psychosis began two months after the onsetof epilepsy and a month after the lesion on CThad disappeared. By this time, although herEEG remained grossly abnormal epilepticattacks had ceased. The course of her illnesswould suggest that the primary brain insult wasresponsible both for the epilepsy and psy-chosis, in a way similar to suggestions by Slateret al9 explaining the association betweenepilepsy and schizophrenia. The possibility ofasteroid induced psychosis in our two patientswas considered most unlikely, as the necessarytemporal relationship between the psychosisand treatment was not present.
In neither of the two cases could an obviouscause be found to explain these disappearinglesions. In the first case, the aetiology wasinitially thought to be either vascular (forexample, microvascular malformations, rup-ture of a small angioma), or the result of focalencephalitis, but the absence of any relevantclinical or laboratory findings and the rapidresolution of the lesion makes this unlikely. Anencephalitic process was also considererd as apossibility in the second case, but thoughtunlikely to explain the well circumscribed CTlesion.There remains the possibility that these
transient CT findings could be the result,rather than the cause of the focal seizureactivity. Similar conclusions have been reachedby a number of previous studies which havereported disappearing CT"6 and MRI5 lesionsin patients with complex partial and general-ised seizures in different age groups. In thelargest series of cases reported,4 completeresolution ofthe lesion was observed in 37 of46patients, corresponding to seizure control, andtaking place in most patients within 16 weeks.A number of theories have been postulated to
explain the transient nature of these disappear-ing lesions. Lesion enhancement probablyrepresents a break in the blood-brain barrier(BBB) with the observed hypodensity accoun-ted for by oedema. Local changes secondary toictal activity would include a relative hypoxiawith increased C02 and lactate concentrationsleading to a loss of autoregulation and vaso-dilatation. 10 Systemic changes such as in-creased blood pressure and decreased bloodpHfurther inhibit autoregulation and increaseCBF." With control of seizure activity, theBBB is restored and enhancement subsides.CT abnormalities are not associated withseverity ofseizure activity2 and it is unclear whythis phenomenon should occur in only aminority of epileptics.
Changes in the BBB as detected on Gadolin-ium enhanced MRI can also account for thefluctuating appearance of new lesions in mul-tiple sclerosis.'2 However, Thompson et al13advocate caution when interpreting the phen-omenon of disappearing lesions in MS, citingthe limitations imposed by MRI (shared byCT), such as repositioning errors and in-adequate spatial resolution. They emphasisethat in MS, despite the disappearance of grossMRI lesions, more subtle abnormalities inmagnetisation parameters usually persist.An alternative explanation is that pre-exist-
ing focal cerebral pathology, such as gliosis,only becomes apparent on CT when oedemaassociated with ictal activity is present.4 Thisagrees with the PET findings of Kuhl et al,4who have shown decreased local cerebralglucose utilisation in the interictal period inareas that appeared normal on CT. The gliosistheory, however, appears unlikely in our twopatients as there was no history of previousbrain insults.
In summary, two cases ofepilepsy, psychosisand disappearing lesions on CT are presented.While at present the exact nature of the patho-genesis is unclear, future improvements inimaging techniques may explain more fully themechanisms underlying this rare triad.
The authors thanks to Dr Trimble for drawingour attention to one of the patients and forallowing us to report the case.
1 Gastaut H, Gastaut JL. Computerised transverse axialtomography in epilepsy. Epilepsia 1976;17:325-36.
2 Jayakumar PN, Taly AB, Mohan PK. Transient computer-ised tomographic (CT) abnormalities following partialseizures. Acta Neurol Scand 1985;72:26-9.
3 Zegers de Beyl D, Hermanus N, Colle H, Goldman S. Focalseizures with reversible hypodensity on the CT scan.J Neurol Neurosurg Psychiatry 1985;48:187-8.
4 Goulatia RK, Verma A, Mishra NK, Ahuja GK. Disappear-ing CT lesions in Epilepsy. Epilepsia 1987;28:523-7.
5 Kramer RE, Luders H, Lesser RP, Weinstein MR, DinnerDS, Morris HH, Wyllie E. Transient Focal Abnormalitiesof Neuroimaging Studies During Focal Status Epilep-ticus. Epilepsia 1987;28:528-32.
6 Sethi PK, Kumar BR, Madan VS, Mohan V. Appearing anddisappearing CT scan abnormalities and seizures.J Neurol Neurosurg Psychiatry 1985;48:866-9.
7 Wing JK, Cooper JE, Sartorious N. The measurement andclassification of psychiatric symptoms. Cambridge:Cambridge University Press, 1974:93-126.
8 Toone BK, Fenton GW. Epileptic seizures induced bypsychotropic drugs. Psychological Medicine 1977;7:265-70.
9 Slater E, Beard AW, Glithero E. The Schizophrenia-likePsychoses of Epilepsy. Br J Psychiatry 1963;109:95-150.
10 Lee JC, Goldberg HI. Hypervascular pattern associatedwith idiopathic focal status epilepticus. Radiology 1977;125:159-63.
11 Plum F, Posner JB, Troy B. Cerebral metabolic andcirculatory responses to induced convulsions in animals.Arch Neurol 1968;18:1-13.
12 Miller DH, Rudge P, Johnson G, et al. Serial gadoliniumenhanced magnetic resonance imaging in multiplesclerosis. Brain 1988;111:927-39.
13 Thompson AJ, Kermode AG. Personal communication.14 Kuhl DE, Engel J, Phelps ME, Selin C. Epileptic Patterns of
Local Cerebral Metabolism and Perfusion in HumansDetermined by Emission Computed Tomography of"FDG and "NH3. Ann Neurology 1980;8:348-60.
246
on April 5, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.3.244 on 1 M
arch 1990. Dow
nloaded from