Embed Size (px)
Citation preview

Taibah University
Journal of Taibah University Medical Sciences (2015) 10(2), 123e131
Journal of Taibah University Medical Sciences
www.sciencedirect.com
Review Article
Methodologies used in quality assessment of root canal preparation
techniques: Review of the literature
Adnan Asaad Habib, PhD *, Mazen Ibrahim Taha, MS and Elias Michel Farah, MS
Department of Conservative Dentistry, Aleppo University, Syria
Received 20 July 2014; revised 4 November 2014; accepted 8 November 2014; Available online 9 January 2015
صخلملا
ةمدختسملاريياعملاوةيثحبلاقرطلامهألمييقتوةعجارمءارجإ:ثحبلافادهأ.ةيرذجلاةينقألاريضحتيفةمدختسملاتاودألاوتاينقتللءادألامييقتيف
-م١٩٥٠ماعنمةقباسلاتاساردللةفثكموةلماشةعجارمءارجإ:ثحبلاقرطريياعمبقيقدتلاعمةضيرعةيبطتانايبةدعاقلالخنمتاغللالكبم٢٠١٤
لالخنمو،ةيرذجلاةينقألاريضحتمييقتلةمدختسملاصاوخلاداعبتساوءاوتحاهذهيفتمدختسايتلاريياعملاوةيثحبلاقرطلاىلعزيكرتلامتةعجارملاهذه.ةيرذجلاةانقلافيظنتولكشمييقتلتاساردلا
تزجنأيتلاتاساردلاوتالاقملانمريثكلادوجوجئاتنلاترهظأ:ثحبلاجئاتنبلغأو.حساملاينورتكلإلابوكسوركيملامادختسابعوضوملااذهلوحتاساردلانمريبكءزجو.ليكشتلاىلعةردقلاتميق)٪٧١.٩(تاساردلاامك،ةعولقملانانسألاىلعيعاعشلاليلحتللةيربخملاتاقيبطتلانعةروشنملادقعلايفيعطقملاريوصتلابليلحتلامادختسانعةروشنملاتاساردلاددعدادزأ.ريخألا
دعبثدحتيتلاةيلكشلاتاريغتلامييقتلريياعملانمددعمادختسا:تاجاتنتسالادعبةانقلاليكشتىلعتاودألاةردقمييقتنأظحولدقو،ةيرذجلاةينقألاريضحت،ةينقألافيظنتمييقتتاساردعمةنراقمتاساردلامظعمىلعذوحتسااهريضحتيعاعشلايعطقملاريوصتلاةينقتبةريخألاتاونسلايفمامتهالاةدايزظحولامك.قيقدلا
;فيظنتلاةردق;ةانقللةيزكرملاةبسن;ةانقلالقن;ةانقلاةقطنم:ةيحاتفملاتاملكلاليكشتةردق;يجنتارلابلاقلاةينقت;قيقدلايعاعشلايعطقملاريوصتلا;ريضنتلاةانقلا
* Corresponding address: Department of Conservative Dentistry,
Aleppo University, Aleppo, Syria.
E-mail: [email protected] (A.A. Habib)
Peer review under responsibility of Taibah University.
Production and hosting by Elsevier
1658-3612 � 2015 The Authors.
Production and hosting by Elsevier Ltd on behalf of Taibah University. T
(http://creativecommons.org/licenses/by-nc-nd/4.0/). http://dx.doi.org/10.10
Abstract
Objectives: To review the dentistry literature regarding
methodologies and parameters used to evaluate the
quality of performance of root canal debridement tech-
niques and instruments.
Methods: An extensive literature search with pre-defined
inclusion and exclusion criteria was undertaken to iden-
tify studies that assessed root canal debridement, meth-
odologies and parameters used to assess shaping and
cleaning ability of root canal debridement and in-
struments. The relevant literature in the field of end-
odontics published from November 1950 to February
2014 was reviewed using PubMed and MEDLINE da-
tabases in all languages.
Results: A large number of studies have assessed the
quality of root canal instrumentation through the eval-
uation of cleaning ability (debris, smear layer) using
histological sections and Scanning Electron Microscopy
(SEM). The majority (71.9%) of studies evaluated the
shaping ability. A body of literature has illustrated in-
vitro applications of extracted teeth in muffle system
and radiographic analysis. Additionally, the majority of
studies have used Schneider angle technique as a random
criterion. Micro-CT analysis has been increasingly used
in the last decade.
Conclusion: Several parameters are employed in the
assessment of the post-operative shape or changes in the
root canal morphology. Shaping ability of the root canal
instrumentation techniques has been more extensively
investigated than the cleaning ability. Additional care
needs to be taken regarding entire angular changes by
combining both Schneider and Canal Access Angel
(CAA) methods and their variants. Finally, more concern
his is an open access article under the CC BY-NC-ND license
16/j.jtumed.2014.11.002

A.A. Habib et al.124
regarding micro-computed tomography technique has
been expressed.
Keywords: Canal area; Canal transportation; Centering ratio;
Debridement; Micro-CT; Muffle system
� 2015 The Authors.
Production and hosting by Elsevier Ltd on behalf of Taibah
University. This is an open access article under the CC BY-
NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).
Introduction
The goal of root canal therapy is to eliminate microor-ganisms and necrotic pulp tissue debris, and to shape the rootcanal system to facilitate irrigation and placement of medi-
caments and obturation materials.1
Successful root canal treatments depend on multiplefactors such as adequate cleaning, shaping and filling of the
root canal system. However, root canal instrumentation isone of the most essential therapeutic procedures in anytreatment since it determines the efficacy of all subsequent
procedures, in addition to the fact that it includes me-chanical debridement, creation of space for medicamentdelivery, and optimized canal geometries for adequateobturation.2
The literature is replete with studies on various aspectsof instruments performance such as: cleanliness of root ca-nals after preparation, shaping ability of instruments, and
fracture properties. Several methodologies have beendescribed to evaluate the performance of root canalinstrumentation.
When analyzing the quality of root canal instrumenta-tion created by instruments and techniques, several pa-rameters can be considered, including the cleaning and
shaping ability.
Cleaning ability of instruments and techniques
Cleaning ability of endodontic instruments and prepara-tion techniques is based on the evaluation of the percentageof debris and un-instrumented root canal walls. It was
assessed in many studies by histological sections of humanroot canals (usually curved canals in maxillary andmandibular molars).3,4
This includes histological preparation of specimens,
obtainment of serial cross-sections (mm) and assessment ofremaining pulp tissue using a morphometric approach.4
Other studies have investigated cleaning ability using the
scanning electron microscope.5,6 SEM evaluation includessplitting the specimen into two halves and preparing themost visible section for SEM examination, different
parameters evaluated; smear layer, pulpal debris, inorganicdebris, surface profile.7 The studies demonstrated that evenwith most sophisticated instruments, there might be some
area that cannot be reached, cleaned or instrumented byinstruments or techniques, suggesting that all techniques ofroot canal instrumentation are unable to completelyremove pulpal debris from irregularities such as dentin
grooves and depressions.4,7,8
Shaping ability of instruments and techniques
The aim of root canal instrumentation is to form a
continuously tapered shape with the smallest diameter at theapical foramen and the largest at the orifice to allow effec-tive irrigation and filling.1 This procedure is carried outwithout any deviations from the original trajectory, in
curved and thin canals,9 using techniques and instrumentswhich have the greatest precision and the shortest workingtime.10
The purpose of studies analyzing post-operative root ca-nal shape is to evaluate the conicity, taper and flow of theprepared root canal, and maintenance of the original canal
shape. The ability of an instrument or a technique to allowthe prepared canal to stay centered is seen as a positiveaspect. Conversely, canal transportation and preparation
errors are seen as a negative aspect.11
Canal transportation is defined according to the Glossaryof Endodontic Terms of the American Association of End-odontists as: “Removal of canal wall structure on the outside
curve in the apical half of the canal due to the tendency offiles to restore themselves to their original linear shape duringcanal preparation; may lead to ledge formation and possible
perforation”.12
Various undesirable apical preparation outcomes such asdamage to the apical foramen,13 elbow formation,14 and zip
formation and perforation,11 have been described as possibleresults of canal transportation.
Many methodologies were mentioned to assess thechanges after instrumentation of root canal; these include
silicone impressions of instrumented canals which assessflow, taper, and smoothness of the walls,15,16 superimposingradiographs before and after shaping17,18 and computer
manipulation for comparative analysis19,20 via using specialsoftware programs like AutoCad21 or Photoshop.22
One of the most popular methods of in-vitro evaluation is
the “muffle system”. Bramante et al. were the first to developthis method to evaluate changes in canal diameter.23 TheMuffle system provides a plaster block around a resin-
indexed experimental tooth. The block can be custom-machined and sectioned in various planes to allow exactrepositioning of the complete block or sectioned parts of thetooth. Simultaneous evaluation and measurement of
numerous parameters are possible such as canal area, shapedform, and centering ability. Furthermore, Data can begathered both pre- and post-operatively, and can be
compared and statistically contrasted.24
The quantification of post-instrumentation root canaldeviation can be measured by “centering ratio” method,25,26
modified formulas to calculate transportation or centeringratio26,27 or by measuring pre- and post-instrumentationdentine thickness.24,28 Alternatively, it can be directlycalculated by Pythagorean theorem.19,29
Superimposing radiographs before and after shaping,17,18
Digital subtraction radiography images, and computermanipulation19,20 are useful methods to evaluate centering
ratio. Centering ratio can be calculated using the followingformula: (X1-X2/Y), X1 represents the maximum extent ofcanal movement in one direction, X2 is movement in the
opposite direction and Y is the diameter of final canalpreparation.25

Parameters used to evaluate root canal preparation 125
Other parameters, such as root-canal diameter, workingsafety (instrument fractures, perforations, apical blockages,
loss of working length -WL-), and working time, wereconsidered when investigating the performance of root canalinstrumentation created by instruments and techniques.30e32
Many of the parameters mentioned above (canal trans-portation, centering ratio, postoperative root-canal diam-eter, loss of working length, and measurements of dentine
thickness pre- and post-instrumentation) could be assessedby a non-destructive technology such as micro-computedtomography (micro-CT).
In 1995, Nielsen et al.33 found that micro-CT accurately
reproduced internal and external tooth morphology withouttooth destruction and demonstrated surface and volumechanges after instrumentation and obturation in extracted
maxillary molars. Thus, this technology has been advocatedfor the comparison of pre- and post-instrumentation images.Micro computed tomography can render cross-sectional
(cutplane) and 3D images that are highly accurate andquantifiable.2,24,34,35
Recently, Micro computed tomography technique hasbeen used in assessing accumulated hard-tissue debris after
preparation procedures specifically in fins, isthmus, irregu-larities, and ramifications-using free software for imageprocessing and analysis.36
It is well known that when curvatures are present, end-odontic preparation becomes more difficult, and there is atendency for all preparation techniques to divert the pre-
pared canal away from the original axis.37
The morphology of a curved root canal is of greatimportance to the outcome of root canal instrumentation,
with several studies being conducted to describe thecurvature.38
In 1971, Schneider et al.39 performed pioneering work onmeasuring canal angulation. Subsequently, Weine40
developed an alternative method for determining canalangulation. A third method known as the long-axis (LA)technique was first described by Hankins et al.41 In contrast,
Kyomen et al. introduced a linear parameter described as themaximum curvature height, which differs from the angularmeasurement techniques.42 Likewise, Pruett et al.
introduced a new parameter described as the “curvatureradius” for measuring root canal curvature.43
In 2005, Gunday et al. introduced the term CAA and two
new curvature parameters pertaining to the coronal zone ofcurved root canals: the curvature starting distance (y) and thecurvature height (x). They compared the new technique withSchneider method and reported that CAA evaluates the root
canal curvature more effectively.38
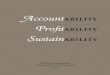
The Schneider method involves first drawing a line par-allel to the long axis of the canal, in the coronal third; a
second line is then drawn from the apical foramen to inter-sect the point where the first line left the long axis of thecanal. The Schneider angle is the intersection of these lines.38
In the Weine technique, a straight line is drawn from theorifice through the coronal portion of the curve, and a secondline is drawn from the apex through the apical portion of thecurve. Weine angle is the intersection of these lines. The LA
technique involves drawing a line passing through the apicalone-third of the canal, the angle formed by the intersection ofthat line with the long axis of the tooth is known as the LA
angle (Figure 1a).38
Canal access angle (CAA) was described and comparedwith Schneider angle technique. The canal orifice (A) and apex
(B) points were connected with a line. The angle formed by theintersection between this line (AB) and one drawn parallel tothe long axis of the canal from the coronal part (AC) (used in
the Schneider method), is defined as the CAA (Figure 1b). Atthe point (C) where the parallel line described in the Schneidermethod leaves the root canal a perpendicular linewas drawn to
AB. The point that the perpendicular line intersects AB is D.CD gives the curvature height (x), and the distance from Ato point D is the curvature distance (AD/y).38
Most studies that evaluated the quality of canal prepa-
ration techniques have been conducted in-vitro. The Prepa-ration of root canals may be evaluated using extractedteeth2,4,44 or simulated root canals in resin blocks.45,46
The aim of this study is to highlight the most importantmethodologies and parameters for assessing the quality of in-struments and techniques used in root canal instrumentation.
Materials and Methods
A literature search for relevant published articles onmethodologies used in the assessment of the quality of root
canal instrumentation in the context of endodontics betweenNovember 195047 and February 201436 in all languages usingPubMed and MEDLINE database searches.
The search was performed using different keywords
(‘preparation of root canal’, ‘root canal instrumentation’,‘root canal debridement’, ‘cleaning ability of instruments andtechniques’, ‘shaping ability of instruments and techniques‘,
‘changes in root canal diameters’, ‘canal transportation‘ or‘centering ratio of root canal’).
Peer-reviewed studies of the quality of preparation and
endodontic instruments have been identified throughPubMed. Articles in which keywords do not match the subjectof the search and case reports and non-English language
studies have been excluded. After removing duplicates, theremaining papers were retrieved, and their reference listschecked to identify any other articles/textbooks relevant tothe topic, which might have provided additional information.
The data have been analyzed, and weighted averages havebeen determined for each of the following: shaping ability,root canal debridement, simulated canals and extracted teeth.
Results
The search through PubMed has shown primarily a hugenumber of articles (3855). After exclusion of duplicates, ar-
ticles in which key words do not match the subject of thesearch, case reports and non-English language studies 528published papers relevant on instrumentation of root canals
were checked.380 (71.9%) studies evaluated shaping abilityand 148 (28.1%) studies assessed cleaning ability.
- The majority of studies/492 (95.2%)/used extracted teethwhile/36 (6.8%)/studies used simulated root canals in resinblocks.
In addition to the studies that have been retrieved,there are several methodologies and parameters used
to evaluate the performance of root canal instrumentation.

Figure 1: Techniques to measure the angulation of root canals. a. Schnieder(S), canal access angle (CAA), Weine(W), and Long Axsis
(LA) angles. b. CAA variables, (x) height and (y) starting distance of the root canal curvature. c.&d. Root canal curvature can have same
(S) and different CAA.
A.A. Habib et al.126
- The methodologies used to evaluate the performance ofroot canal instrumentation in most studies are:
� For cleaning ability: histological sections, scanningelectron microscope, and micro computed tomographytechnique.
� For shaping ability: silicone impressions. Radiographs
and images and computer analysis, muffle system,
modified formulas, and micro-computed tomographytechnique and its breakthroughs.
- The parameters used to evaluate the performance of rootcanal instrumentation in most studies are:� For cleaning ability: percentage of debris (pulpal debris,inorganic debris,), un-instrumented root canal walls,
smear layer, surface profile, and apically extruded debris.

Table 1: In vitro studies evaluating the cleaning ability of instrumentation using extracted teeth.
Reference
(chronologic order)
Type of study
in-vitro, ex-vivo, clinical
Samples Methodology/parameters
Walton 19763 in-vitro extracted teeth histological sections (debris)
Moodnik et al. 19765 in-vitro extracted teeth SEM (debris)
Conningham et al. 198248 in-vitro extracted teeth histological sections (debris)
Mandel et al. 199049 in-vitro extracted teeth SEM (debris)
Myers and ontgomery 199150 in-vitro extracted teeth assessment of apically extruded debris
Hulsmann et al.199751 in-vitro extracted teeth SEM (debris)
Prati et al. 20047 in-vitro extracted teeth SEM (debris, smeer layer)
Zmener et al. 200552 in-vitro extracted teeth SEM (debris)
Liu et al. 200653 in-vitro extracted teeth SEM (debris)
De-Deus et al. 201054 in-vitro extracted teeth assessment of apically
extruded debris
Taha et al. 201055 in-vitro extracted teeth histological sections (debris)
Fornari et al. 201056 in-vitro extracted teeth histological sections (debris)
Arya et al. 201157 in-vitro extracted teeth histological sections (debris)
Burklein and Schafer 201258 in-vitro extracted teeth assessment of apically extruded debris
Chandra et al. 201359 in-vitro extracted teeth SEM (debris)
De-Deus et al. 201436 in-vitro extracted teeth micro-CT (debris)
Parameters used to evaluate root canal preparation 127
� For shaping ability: flow, taper, smoothness of the walls,original canal shape, changes in curvature angulation,
apical transportation, canal area, centering ratio, thick-ness of remaining root structure, working time, fracturedinstruments, aberrations and working length.
Table 1 shows in-vitro studies evaluating the cleaning
ability of instrumentation using extracted teeth:Table 2 shows studies evaluating the shaping ability of
instrumentation:
Discussion
The understanding of endodontic therapy concepts leadsto great advance in instruments and techniques, which is the
reason why, many studies to assess the performance andquality of these instruments and techniques have beenundertaken.
It has been noted that studies using extracted teeth toevaluate the quality of root canal instrumentation were morethan their counterparts using simulated canals in resin blocks.
The major advantage of extracted human teeth is toreproduce the clinical situation. However, it is difficult tostandardize some variables such as root canal length andwidth, dentine hardness, calcification and pulp stones, loca-
tion and nature of canal curvatures.13
On the other hand, simulated resin root canals allowstandardization of degree, location and radius of root canal
curvature in three dimensions as well as the tissue hardnessand the width of the root canals.
Superimposition techniques of pre- and post-operative
root canal outlines can be easily applied to these models,thus facilitating measurement of deviations at any point ofthe root canals using PC-based measurement (comparison
among parameters recorded as data in computer) or sub-traction radiography. This model guarantees a high degree ofreproducibility and standardization of the experimentaldesign.77 It has been suggested that the results of such studies
may be transferred to human teeth.77
Nevertheless, some concern has been expressed regardingthe differences in hardness between dentine and resin.Microhardness of dentine has been measured as 35e40 kg/mm2 near the pulp space, while the hardness of resin mate-
rials used for simulated root canals is estimated to rangefrom 20 to 22 kg/mm2 depending on the material used.78,79
For the removal of natural dentine, double the force had
to be applied than that for resin.77 Additionally, criticsreported that the size of resin chips and natural dentinechips may not be identical, resulting in frequent blockages
of the apical root canal space and difficulties to remove thedebris in resin canals.77 In consequence, data on workingtime and working safety from studies using resin blocks
may not be transferable to the clinical situation.13
Most studies on post-operative root canal shape orchanges in root canal morphology, have been performed inmesial root canals of mandibular molars,24,30,32,67,73,74 as
these teeth in most cases show a curvature at least in themesioedistal plane.80 On the other hand, other studiesused mandibular premolars,52,55,57,66 mandibularincisors,18
maxillary incisors50 or maxillary molars.81,82
The studies on root canal curvature have shown thatseveral techniques were conducted to describe canal curva-
tures. Schneider angle was routinely used. Schneider tech-nique mainly emphasizes the canal curvature in the apicalregion, and Weine technique considers the apical region, andthe LA technique considers only the apical curvature of the
canal and does not evaluate the overall root canal curvature.CAA together with height and distance of curvature providemore information about the coronal geometry of root canal
curvatures.38 Few studies have used Schneider angle incombination with the radius of curvature.83e85 Othersclaimed that the shape of root canal curve is more
accurately described using Schneider in combination withCAA and the related parameters including radius, length,distance and height of curvature. This combination
provides more accurate guidelines for both coronal andapical parts of canal curvature.86
Lately, many investigators have been more concernedwith micro-computed tomography technique and its

Table 2: Studies evaluating the shaping ability of instrumentation.
Reference
(chronologic order)
Type of study
in-vitro, ex-vivo,
clinical
Samples Methodology/parameters
Schneider 197139 in-vitro extracted teeth cross sections (shaped form)
Jungmann et al. 197560 in-vitro extracted teeth cross sections (shaped form)
Abou-Rass et al. 198261 in-vitro extracted teeth silicone impressions (apical design, aberration removal, flow, taper,
uniformity, and smoothness of preparation)
Stadler et al. 198662 clinical patients radiographic analysis (breakage, lateral deviation, overfilling, root
perforation, Loss in working length).
Southard et al. 198763 in-vitro extracted teeth drawings and projected radiographic images (original canal shape)
Luiten et al. 199517 in-vitro extracted teeth Radiographs and computer analysis (Canal enlargement, apical
transportation)
Deplazes et al. 200126 in-vitro extracted teeth muffle system (canal area, centering ratio)
Gluskin et al. (2001)24 in-vitro extracted teeth CT scans Image analysis (canal area, canal transportation thickness
of remaining root structure, working time)
Schafer &
Lohmann 200264in-vitro simulated canals images and computer analysis (working time, canal transportation,
fractured instruments)
Song et al. 200465 in-vitro extracted teeth muffle system, modified formulas (centering ratio)
Guelzow et al. 200566 in-vitro extracted teeth muffle system, computer analysis (degree of curvature, working
length, straightening of curved root canals, working time, time for
changing the instruments)
Veltri et al. 200567 in-vitro extracted teeth radiographic analysis/Wiene, angle (shaping ability, working time,
canal form, working safety)
Mahran &
AboEl-Fotouh 20082in-vitro extracted teeth micro-CT (cervical dentin thickness, Canal volume)
Cheung & Cheung 200835 in-vitro extracted teeth micro-CT (canal diameter, remaining thickness of the dentin wall)
Vahid et al. 200968 ex-vitro extracted teeth radiographic analysis/Schneider’s angle (working time, canal
curvature, working length)
Moore et al. 200969 in-vitro extracted teeth micro-CT (amount of dentine removed, canal roundness,
transportation correlation between prepared apical root canal and
final instrument used)
Unal et al. 200970 in-vitro extracted teeth muffle system, images and radiographic analysis/Schneider’s angle,
formulas (dentine removed, transportation, working time, amount
of dentin removed, working length)
Ersev et al. 201022 in-vitro simulated canals images and computer analysis (amount of material removal, canal
transportation, centering ratio, aberrations)
Plotino et al. 201071 in-vitro simulated canals images analysis (angle and radius of the curvature, position of the
center of the curvature)
Hartmann et al. 201172 in-vitro extracted teeth micro-CT (canal transportation)
Alves Vde 201273 in-vitro extracted teeth Radiographs and computer analysis (canal aberration, apical
transportation)
Hashem et al. 201274 in-vitro extracted teeth CT scans Image analysis (canal transportation, centering ratio)
Ba-Hattab et al. 201375 in-vitro simulated canals images and computer analysis (working time canal transportation,
amount of removal resin)
Celik et al. 201376 in-vitro extracted teeth Radiographs and computer analysis (working length, canal
transportation)
A.A. Habib et al.128
breakthroughs (multislice computed tomography, cone-
beam computed tomography). A major factor for thisconcern is that the radiographs are two-dimensional repre-sentations for three-dimensional structures causing certainanatomical features not to be reflected in radiographic
changes. In the late 1980s, radiographs were digitized toprovide control over the quality of the film and reduce theradiation dosage. These digitized radiographs have an
advantage of controlling contrast and brightness by theoperator,87 although they still provide a 2-dimentional pic-ture. Conversely, micro-CT provides a 3-dimentional pic-
ture. It allows pre-instrumentation and post-instrumentationmeasuring of several parameters to evaluate the quality ofroot canal instrumentation techniques without using
complicated procedures, destructive sectioning of the speci-
mens, or loss of the root material during sectioning. Thereare no instrumentation problems passing through sections oraround curvatures that could affect the instrumentationoutcomes. Also, CT scans allow easy measurement of canal
changes, because each image has an accurate scale,decreasing the potential of a radiographic orphotographictransfer error.88 However, a cone-beam computed tomog-
raphy scan can expose the patient to two to eight times moreradiation than that of a panoramic radiograph and aboutone third of a full mouth radiographic series.89 It should also
be noted that cone-beam computed tomography scanningneeds complex devices,90 and is more expensive thanperiapical and panoramic radiography.

Parameters used to evaluate root canal preparation 129
Conclusion
1) Deep understanding of the phase of root canal instru-mentation leads to the use of several parameters to assess
post-operative shape or changes in root canalmorphology.
2) Shaping ability of the root canal instrumentation tech-niques has captured more researches compared with
cleaning ability.3) More attention must betaken regarding entire angular
changes by combining both Schneider and CAA methods
and their variabilities.4) More concern regarding micro-computed tomography
technique has been expressed as, this non-destructive
technique provides a 3-dimentional picture, and allowspre- and post-instrumentation measuring of several pa-rameters. We, therefore, conclude that, currently, themicro-computed tomography technique is a superior
methodology to evaluate the quality of root canalinstrumentation techniques.
Authors’ contributions
All authors contributed in collecting and classficating
papers. Dr. Adnan Asaad Habib wrote the text of the paperand was the corresponding author. Dr. Mazen Ibrahim Tahadesigned the figures.
Conflict of interest
The authors have no conflict of interest to declare.
Acknowledgment
The staff of Aleppo University, faculty of dentistry.
References
1. Schilder H. Cleaning and shaping the root canal. J Dent Clin
North Am 1974; 18: 269.
2. Mahran AH, AboEl-Fotouh MM. Comparison of effects
of ProTaper, HeroShaper, and Gates Glidden Burs on
cervical dentin thickness and root canal volume by using
multislice computed tomography. J Endod 2008; 34(10):
1219e1222.
3. Walton R. Histological evaluation of different methods of
enlarging the pulp canal space. J Endod 1976; 2: 304e311.
4. De-Deus D, Paulo Garcia-Filho P. Influence of the NiTi rotary
system on the debridement quality of the root canal space. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 108(4):
e71ee76.5. Moodnik RM, Dorn SO, Feldman MJ, Levey M, Borden BG.
Efficacy of biomechanical instrumentation: a scanning electron
microscopic study. J Endod 1976; 2(9): 261e266.
6. Cymerman JJ, Jerome LA, Moodnik RM. A scanning electron
microscope study comparing the efficacy of hand instrumenta-
tion with ultrasonic instrumentation of the root canal. J Endod
1983; 9(8): 327e331.
7. Prati C, Foschi F, Nucci C, Montebugnoli L, Marchionni S.
Appearance of the root canal walls after preparation with NiTi
rotary instruments: a comparative SEM investigation. Clin Oral
Investig 2004; 8(2): 102e110.
8. Klyn SL, Kirkpatrick TC, Rutledge RE. In vitro comparisons
of debris removal of the EndoActivatorTM System, the F Fil-
eTM, ultrasonic irrigation, and NaOCl irrigation alone after
hand-rotary instrumentation in human mandibular molars.
J Endod 2010; 36: 1367e1371.
9. Hata GI, Uemura M, Kato AS, Imura N, Novo NF, Toda T.
A comparison of shaping ability using ProFile, GT File and
Flex-R endodontic instruments in simulated canals. J Endod
2002; 28: 316e321.
10. Iqbal MK, Maggiore F, Suh B, Edwards KR, Kang J, Kim S.
Comparison of apical transportation in four Ni-Ti rotary
instrumentation techniques. J Endod 2003; 29: 587e591.
11. Peters OA. Current challenges and concepts in the preparation
of root canal systems: a review. J Endod 2004; 30(8): 559e567.
12. American Association of Endodontists. Glossary of endodontic
terms. 7th ed. Chicago: AAE; 2003.
13. Hulsmann M, Peters OA, Dummer PM. Mechanical prepara-
tion of root canals: shaping goals, techniques and means. Endod
Top 2005; 10: 30e76.
14. Weine F, Kelly R, Lio P. The effect of preparation procedures
on original canal shape and on apical foramen shape. J Endod
1975; 1(8): 255e262.15. Barthel CR, Gruber S, Roulet JF. A new method to assess the
results of instrumentation techniques in the root canal. J Endod
1999; 25(8): 535e538.16. Nagaratna PJ, Shashikiran ND, Subbareddy VV. In vitro
comparison of NiTi rotary instruments and stainless steel hand
instruments in root canal instrumentations of primary and
permanent molar. J Indian Soc Pedod Prev Dent 2006; 24(4):
186e191.
17. Luiten DJ, Morgan LA, Baumgartner JC, Marshall JG.
A comparison of four instrumentation techniques on apical
canal transportation. J Endod 1995; 21(1): 26e32.
18. Mikrogeorgis G, Molyvdas I, Lyroudia K, Nikolaidis N,
Pitas I. A new methodology for the comparative study of the
root canal instrumentation techniques based on digital radio-
graphic image processing and analysis. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 2006; 101(6): e125ee131.
19. Coleman CL, Svec TA. Analysis of Ni-Ti versus stainless steel
instrumentation in resin simulated canals. J Endod 1997; 23(4):
232e235.
20. Porto Carvalho LA, Bonetti I, Gagliardi Borges MA.
A comparison of molar root canal instrumentation using
stainless-steel and nickel-titanium instruments. J Endod 1999;
25(12): 807e810.
21. Lopez FU, Travessas JAC, Fachin E, Fontanella V, Grecca F.
Apical transportation: two assessment methods. Aust Endod J
2009; 35(2): 85e88.
22. Ersev H, Yılmaz B, Ciftcio�glu E, Ozkarsl SF. A comparison of
the shaping effects of 5 nickel-titanium rotary instruments in
simulated S-shaped canals. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2010; 109(5): e86e93.
23. Bramante CM, Berbert A, Borges RP. A methodology for
evaluation of root canal instrumentation. J Endod 1987; 13(5):
243e245.24. Gluskin AH, Brown DC, Buchanan LS. A reconstructed
computerized tomographic comparison of Ni-Ti rotary GT files
versus traditional instruments in canals shaped by novice op-
erators. Int Endod J 2001; 34(6): 476e484.25. Calhoun C, Montgomery S. The effects of four instrumenta-
tion techniques on root canal shape. J Endod 1988; 14(6):
273e277.
26. Deplazes P, Peters O, Barbakow F. Comparing apical prepa-
rations of root canals shaped by nickel-titanium rotary in-
struments and nickel-titanium hand instruments. J Endod 2001;
27(3): 196e202.
27. Gergi R, Rjeily JA, Sader J, Naaman A. Comparison of canal
transportation and centering ability of twisted files, Pathfile-

A.A. Habib et al.130
ProTaper system, and stainless steel hand K-files by using
computed tomography. J Endod 2010; 36(5): 904e907.
28. McCann JT, Keller DL, Labounty GL. Remaining dentine/
cementum thickness after hand or ultrasonic instrumentation.
J Endod 1999; 16: 109e113.
29. Short JA, Morgan LA, Baumgartner JC. A comparison of canal
centering ability of four instrumentation techniques. J Endod
1997; 23(8): 503e507.
30. Hulsmann M, Gressmann G, Schafers F. A comparative study
of root canal instrumentation using FlexMaster and HERO 642
rotary Ni-Ti instruments. Int Endod J 2003; 36(5): 358e366.
31. Hulsmann M, Gressmann G, Schafers F. Comparative study of
root-canal preparation using Lightspeed and Quantec SC ro-
tary NiTi instruments. Int Endod J 2003; 36(11): 748e756.32. Hulsmann M, Schade M, Schafers F. A comparative study of
root canal instrumentation with HERO 642 and Quantec SC
rotary Ni-Ti instruments. Int Endod J 2001; 34(7): 538e546.
33. Nielsen RB, Alyassin AM, Peters DD, Carnes DL, Lancaster J.
Microcomputed tomography: an advanced system for detailed
endodontic research. J Endod 1995; 21(11): 561e568.
34. Rhodes JS, Pitt Ford TR, Lynch JA, Liepins PJ, Curtis RV.
Micro-computed tomography: a new tool for experimental
endodontology. Int Endod J 1999; 32(3): 165e170.
35. Cheung LHM, Cheung GSP. Evaluation of a rotary instru-
mentation method for C-shaped canals with micro-computed
tomography. J Endod 2008; 34(10): 1233e1238.
36. De-Deus G, Marins J, de Almeida Neves A, Reis C, Fidel S,
Versiani MA, et al. Assessing accumulated hard-tissue debris
using micro-computed tomography and free software for image
processing and analysis. J Endod 2014; 40(2): 271e276.
37. Javaberi HH, Javaberi HG. A comparison of three Ni-Ti ro-
tary instruments in apical transportation. J Endod 2007; 33(3):
284e286.38. Gunday M, Sazak H, Garip Y. A comparative study of three
different root canal curvature measurement techniques and
measuring the canal access angle in curved canals. J Endod
2005; 31(11): 796e798.
39. Schneider SW. A comparison of canal preparations in straight
and curved root canals. Oral Surg Oral Med Oral Pathol 1971;
32(2): 271e275.
40. Weine FS. Endodontic therapy. 3rd ed. St. Louis: CV Mosby;
1982. pp. 288e306.
41. Hankins PJ, ElDeeb ME. An evaluation of the Canal Master,
balanced force, and step-back techniques. J Endod 1996; 22(3):
123e130.
42. Kyomen SM, Caputo AA, White SN. Critical analysis of the
balanced force technique in endodontics. J Endod 1994; 20(7):
332e337.
43. Pruett JP, Clement DJ, Carnes DL. Cyclic fatigue testing of
nickel-titanium endodontic instruments. J Endod 1997; 23(2):
77e85.44. Bryant ST, Dummer PM, Pitony C, Bourba M, Moghal S.
Shaping ability of .04 and .06 taper ProFile rotary nickel-
titanium instruments in simulated root canals. Int Endod J
1999; 32(3): 155e164.45. Dummer PM, al-omari MA, Bryant ST. Comparison of the
performance of four files with rounded tips during shaping of
simulated root canals. J Endod 1998; 24(5): 364e371.
46. Aydin C, Inan U, Yasar S, Bulucu B, Tunka YM. Comparison
of shaping ability of RaCe and Hero Shaper instruments in
simulated curved canals. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2008; 105(3): e92ee97.
47. Maeglin B, Muller O. Preparation of the infected root canal.
SSO Schweiz Monatsschr Zahnheilkd 1950 Nov; 60(11): 1142e
1143.
48. Conningham WT, Martin H, Forrest WR. Evaluation of root
canal debridement by the endosonic ultrasonic synergistic sys-
tem. Oral Surg Oral Med Oral Pathol 1982; 53(4): 401e404.
49. Mandel E, Matchou P, Friedman S. Scanning electron micro-
scope observation of canal cleanliness. J Endod 1990; 16(6):
279e283.50. Myers GL, Montgomery S. A comparison of weights of debris
extruded apically by conventional filing and Canal Master
techniques. J Endod 1991; 17(6): 275e279.
51. Hulsmann M, Rummelin C, Scha fers F. Root canal cleanliness
after preparation with different endodontic handpieces and
hand instruments: a comparative SEM investigation. J Endod
1997; 23(5): 301e306.52. Zmener O, Pameijer CH, Banegas G. Effectiveness in
cleaning oval-shaped root canals using anatomic endodontic
technology, ProFile and manual instrumentation: a scan-
ning electron microscopic study. Int Endod J 2005; 38(6):
356e363.
53. Liu SB, Fan B, Cheung GS, Peng B, Fan MW, Gutmann JL,
et al. Cleaning effectiveness and shaping ability of rotary Pro-
Taper compared with rotary GT and manual K-Flexofile. Am J
Dent 2006; 19(6): 353e358.
54. De-Deus G, Brandao MC, Barino B, Giorgi KD, Fidel RAS,
Luna AS. Assessment of apically extruded debris produced by
the single-file ProTaper F2 technique under reciprocating
movement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2010; 110(3): 390e394.
55. Taha N, Ozawa T, Messer HH. Comparison of three techniques
for preparing oval-shaped root canals. J Endod 2010; 36(3):
532e535.
56. Fornari VJ, Silva-Sousa YT, Vanni JR, Pecora JD,
Versiani MA, Sousa-Neto MD. Histological evaluation of
the effectiveness of increased apical enlargement for cleaning
the apical third of curved canals. Int Endod J 2010; 43(11):
988e994.
57. Arya A, Bali D, Grewal M. Histological analysis of cleaning
efficacy of hand and rotary instruments in the apical third of the
root canal: a comparative study. J Conserv Dent 2011; 14(3):
237e240.58. Burklein S, Schafer E. Apically extruded debris with recipro-
cating single-file and full-sequence rotary instrumentation sys-
tems. J Endod 2012; 38(6): 850e852.
59. Chandra V, Gandi P, Shivanna AK, Srinivas S, Himgiri S,
Nischith KG. A scanning electron microscopic study to eval-
uate the efficacy of NaviTip FX in removing the canal debris
during root canal instrumentation: an in vitro study. J Contemp
Dent Pract 2013; 14(4): 653e656.
60. Jungmann CL, Uchin RA, Bucher JF. Effect of instrumentation
on the shape of the root canal. J Endod 1975; 1(2): 66e69.
61. AboueRass M, Jastrab RJ. The use of rotary instruments as
auxiliary aids to root canal instrumentation of molars. J Endod
1982; 8: 78e82.
62. Stadler LE, Wennberg A, Olgart L. Instrumentation of the
curved root canal using filing or reaming techniqueea clinical
study of technical complications. Swed Dent J 1986; 10(1e2):
37e43.
63. Southard DW, Oswald RJ, Natkin E. Instrumentation of
curved molar root canals with the Roane technique. J Endod
1987; 13(10): 479e489.
64. Schafer E, Lohmann D. Comparison of the shaping ability of
GT� Series X, twisted files and AlphaKite rotary nickel-
titanium systems in simulated canals. Int Endod J 2002; 35(6):
505e513.
65. Song YL, Bian Z, Fan B, Fan MW, Gutman GL, Peng B.
A comparison of instrument-centering ability within the root
canal for three contemporary instrumentation techniques. Int
Endod J 2004; 37(4): 265e271.
66. Guelzow A, Stamm O, Martus P, Kielbassa MA. Comparative
study of six rotary nickel-titanium systems and hand instru-
mentation for root canal instrumentation. Int Endod J 2005;
38(10): 743e752.

Parameters used to evaluate root canal preparation 131
67. Veltri M, Mollo A, Mantovani L, Pini P, Balleri P, Grandini S.
A comparative study of Endoflare-Hero Shaper and Mtwo NiTi
instruments in the preparation of curved root canals. Int Endod
J 2005; 38(9): 610e616.
68. Vahid A, Roohi N, Zayeri F. A comparative study of four
rotary NiTi instruments in preserving canal curvature, prepa-
ration time and change of working length. Aust Endod J 2009;
35(2): 93e97.
69. Moore J, Fitz-Walter P, Parashos P. A micro-computed
tomographic evaluation of apical root canal instrumentation
using three instrumentation techniques. Int Endod J 2009;
42(12): 1057e1064.
70. Unal GC, Maden M, Savgat A, Orhan EO. Comparative
investigation of 2 rotary nickel-titanium instruments: protaper
universal versus protaper. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2009; 107(6): 886e892.
71. Plotino G, Grande NM, Mazza C, Petrovic R, Testarelli L,
Gambarini G. Influence of size and taper of artificial canals on
the trajectory of NiTi rotary instruments in cyclic fatigue
studies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2010; 109(1): e60ee66.
72. Hartmann MS, Fontanella VR, Vanni JR, Fornari VJ,
Barletta FB. CT evaluation of apical canal transportation
associated with stainless steel hand files, oscillatory technique
and pro taper rotary system. Braz Dent J 2011; 22(4): 288e293.
73. Alves Vde O, Bueno CE, Cunha RS, Pinheiro SL, Fontana CE,
de Martin AS. Comparison among manual instruments and
PathFile and Mtwo rotary instruments to create a glide path in
the root canal instrumentation of curved canals. J Endod 2012;
38(1): 117e120.
74. Hashem AA, Ghoneim AG, Lutfy RA, Foda MY, Omar GA.
Geometric analysis of root canals prepared by four rotary NiTi
shaping systems. J Endod 2012; 38(7): 996e1000.
75. Ba-Hattab R, Prohl AK, Lang H, Pahncke D. Comparison of
the shaping ability of GT(R) Series X, twisted files and
AlphaKite rotary nickel-titanium systems in simulated canals.
BMC Oral Health 2013; 13: 72.
76. Celik D, Tasdemir T, Er K. Comparative study of 6 rotary
nickel-titanium systems and hand instrumentation for root ca-
nal instrumentation in severely curved root canals of extracted
teeth. J Endod 2013; 39(2): 278e282.
77. Lim KC, Webber J. The validity of simulated root canals for the
investigation of the prepared root canal shape. Int Endod J
1985; 18(4): 240e246.78. Eldeeb ME, Boraas JC. The effect of different files on the
preparation shape of severely curved canals. Int Endod J 1985;
18(1): 1e7.
79. Miserendino LJ, Miserendino CA, Moser JB, Heuer MA,
Osetek EM. Cutting efficiency of endodontic instruments. Part
III. Comparison of sonic and ultrasonic instrument systems.
J Endod 1988; 14(1): 24e30.
80. Cunningham C, Senia S. A three-dimensional study of canal
curvatures in the mesial roots of mandibular molars. J Endod
1992; 18(6): 294e300.81. Kfir A, Rosenberg E, Zuckerman O, Tamse A, Fuss Z. Com-
parison of procedural errors resulting during root canal in-
strumentations completed by senior dental students in patients
using an ‘8-step method’ versus ‘serial step-back technique’.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 97(6):
745e748.
82. Kunert GG, Fontanella VRC, de Moura AAM, Barletta FB.
Analysis of apical root transportation associated with ProTaper
universal F3 and F4 instruments by using digital subtraction
radiography. J Endod 2010; 36(6): 1052e1055.
83. Schafer E, Diez C, Hoppe W, Tepel J. Roentgenographic
investigation of frequency and degree of canal curvatures in
human permanent teeth. J Endod 2002; 28(3): 211e216.
84. Schafer E, Erler M, Dammaschke T. Comparative study on the
shaping ability and cleaning efficiency of rotary Mtwo in-
struments. Part 1. Shaping ability in simulated curved canals.
Int Endod J 2006; 39(3): 196e202.
85. Schafer E, Erler M, Dammaschke T. Comparative study on the
shaping ability and cleaning efficiency of rotary Mtwo in-
struments. Part 2. Cleaning effectiveness and shaping ability in
severely curved root canals of extracted teeth. Int Endod J 2006;
39(3): 203e212.
86. Sadeghi S, Poryousef V. A novel approach in assessment of root
canal curvature. Iran Endod J 2009; 4(4): 131e134.
87. Mouyen F, Benz C, Sonnabend E, Lodter J. Presentation and
physical evaluation of RadioVisioGraphy. Oral Surg Oral Med
Oral Pathol 1989; 68(2): 238e242.
88. Uyanik OM, Cehreli CZ, Mocan OB, Dagli TF. Comparative
evaluation of three nickel-titanium instrumentation systems in
human teeth using computed tomography. J Endod 2006; 32(7):
668e671.
89. Okano T, Harata Y, Sugihara Y, Sakaino R, Tsuchida R,
Iwai K, et al. Absorbed and effective doses from cone beam
volumetric imaging for implant planning. Dentomaxillofac
Radiol 2009; 38: 79e85.
90. Low KM, Dula K, Burgin W, von Arx T. Comparison of
periapical radiography and cone beam tomography in posterior
maxillary teeth referred for apical surgery. J Endod 2008; 34:
557e562.