Embed Size (px)
Citation preview

a S c i T e c h n o l j o u r n a lResearch Article
Journal of Spine & Neurosurgery
All articles published in Journal of Spine & Neurosurgery are the property of SciTechnol, and is protected by copyright laws. Copyright © 2017 SciTechnol, All Rights Reserved.
Kongwad et al., J Spine Neurosurg 2017, 6:2DOI: 10.4172/2325-9701.1000263
International Publisher of Science, Technology and Medicine
Solitary Plasmacytoma of the Axial Spine and Dorsal Spine: Treatment Dilemmas and Review of LiteratureKongwad LI1, Nair RP1*, Nayal B2 and Nagaraj A2
Abstract
Background: Solitary plasmacytoma of the spine accounts for 5% of plasmacytomas and is a rare entity [1]. More than 25-60% of these lesions are localized in the dorsal spine and cause myelopathy in 42-71% of the patients. Diagnosis and treatment protocols have been established, however the final decision of whether to stabilize and irradiate locally versus direct irradiation is controversial. Many centers advocate different treatment protocols based on their institutional experience and patient outcomes.
Clinical presentation: We present, herewith, our experience with a 63 year-old patient with upper dorsal solitary lesion, who presented with upper back pain and was diagnosed to have a D3-4 solitary plasmacytoma and another 44 year old patient who presented with spastic quadriparesis progressing to quadriplegia over the last 6 months, who had a C2 lytic lesion with instability.
Conclusion: In the presence of solitary spinal lesions, despite the location, solitary plasmacytoma of the bone should be considered as one of the differential diagnosis. Abnormal proteinemia or proteinuria may often be absent, yet this entity is commonly encountered in clinical practice. Patients show clinical and neurological improvement with surgical decompression with/without stabilization. Postoperatively, radiotherapy is advocated since it reduces the recurrence rates. Often confused with spinal tuberculosis, starting ATT can be detrimental to the patient since it delays the standard line of treatment.
KeywordsCervical plasmacytoma; Dorsal plasmacytoma; Solitary plasmacytoma; Lytic lesion; Instrumentation and spinal irradiation
*Corresponding author: Dr. Rajesh P Nair, MS, MCh, Senior Registrar, Department of Neurosurgery, Kasturba Medical College, Manipal University, India, E-mail: [email protected]
Received: December 12, 2016 Accepted: January 20, 2017 Published: April 20, 2017
Neurological examination revealed an increase in the lower limb tone [Grade 1 Modified Ashworth]. Power seemed to be Grade 5/5 in all four limbs. Sensory [pin prick] seemed to be decreased below D3 on left and below L1 on right. Lower limb reflexes were brisk and plantars were upgoing. A clinical diagnosis of a D1 level lesion with myelomalacia [UMN signs] was made and investigations were done for localizing the lesion.
MRI Dorsal spine [done at an outside hospital] showed a D3 vertebral body destruction with epidural collection between D2-D4 level with myelomalacic changes with involvement of the posterior element of D3 (Figure 1 a,b).
CT Dorsal spine showed a lystic lesion involving D2-D4 vertebrae with extension into the posterior elements of D3, with collapse of D3 body and significant paravertebral and epidural collection (Figure 2).
Patient underwent D2 to D4 laminectomy with transpedicular decompression of tumour and D2 and D5 transpedicular screw stabilization (Figure 2, far right colour plate). Postoperatively he was
Case ReportCase 1
A 63 year-old gentleman presented to the outpatient department with the history of upper back pain radiating to bilateral shoulders since 2 years. He had been seen at various local hospitals and was started on analgesics to relieve his symptoms, but to no avail. The pain was radiating to the shoulder girdle [L>R], which aggravated on movement, however there were no motor deficits. On general examination he had a D3-D4 level gibbus with no spinal tenderness.
Figure 1a: MRI D-L spine (sagittal section, T2W) showing a destruction of D3 vertebrae with wedging and significant ventral compression of the thecal sac with obliteration of the ventral epidural space with cord intensity changes.
Figure 1b: Preoperative MRI Axial T2W showing a lesion within the spinal canal, compressing the thecal sac and destroying the posterior elements on the left side invasion into the vertebral body at the level of D3, Lower images showing the involvement (T2W) of the vertebral body and ventral compression of the thecal sac at the level of D4.
Citation: Kongwad LI, Nair RP, Nayal B, Nagaraj A (2017) Solitary Plasmacytoma of the Axial Spine and Dorsal Spine: Treatment Dilemmas and Review of Literature. J Spine Neurosurg 6:2.
• Page 2 of 5 •
doi: 10.4172/2325-9701.1000263
Volume 6 • Issue 2 • 1000263
ambulated with a Taylor’s brace and discharged within a fortnight. Pathology rendered a diagnosis of Solitary plasmacytoma of the spine (Figure 7a) and he was subjected to adjuvant radiotherapy. Prior to irradiation, peripheral smear along with Bence jones proteins [in urine] were done, to rule out multiple myeloma. He underwent irradiation of the spine (C6 to D5 level). He received a total of 30Gy in 10 fractions over 2 weeks. Followup MRI showed insignificant residual lesion with no evidence of bone marrow changes and serum electrophoresis showed NO M bands (Figure 3).
Case 2
A 44 year-old gentleman, presented to the outpatient department, with the history of neck pain since 8 months. It was the first time that he was being evaluated for the same. The pain was non-radiating in nature and localized to the posterior aspect of the nape of the neck. He also complained of progressive weakness in all four limbs since the last 2 months. The progression of the weakness followed an Elsberg pattern, starting from the right lower limb. He had been bed bound since the last 3 weeks, requiring assistance for all daily activities. There was no history of cough or valsalva headache and no history of trauma.
On general examination, he was moderately built and nourished with severe, painful restriction of neck movements. Neurological examination revealed spastic quadriparesis (Modified Ashworth Grade 2A). His single breath count was grossly reduced with restricted chest expansion. He had no CVJ markers and no evidence of Horners syndrome or hearing loss. There were no obvious cranial nerve deficits including trigeminal nerve. On Motor examination, he had a flicker of movement in bilateral upper limbs (Grade 1/5) and Grade1/5 and Grade 2/5 in the right and left lower limbs respectively. Sensation (Crude touch and pin prick) was diminished below C3-4 segments with exaggerated deep tendon reflexes in all four limbs. Superficial reflexes were absent and plantars were upgoing. A clinical diagnosis of upper cervical myelopathy secondary to cranio-vertebral junction pathology was considered and further investigations were done.
Cervical spine x ray showed a well-defined expansile lytic lesion involving the anterior and posterior elements of the C2 vertebra with associated cortical thinning (Figure 5). A corroborative computed tomographic (CT) scan of the cervical spine showed a well-defined
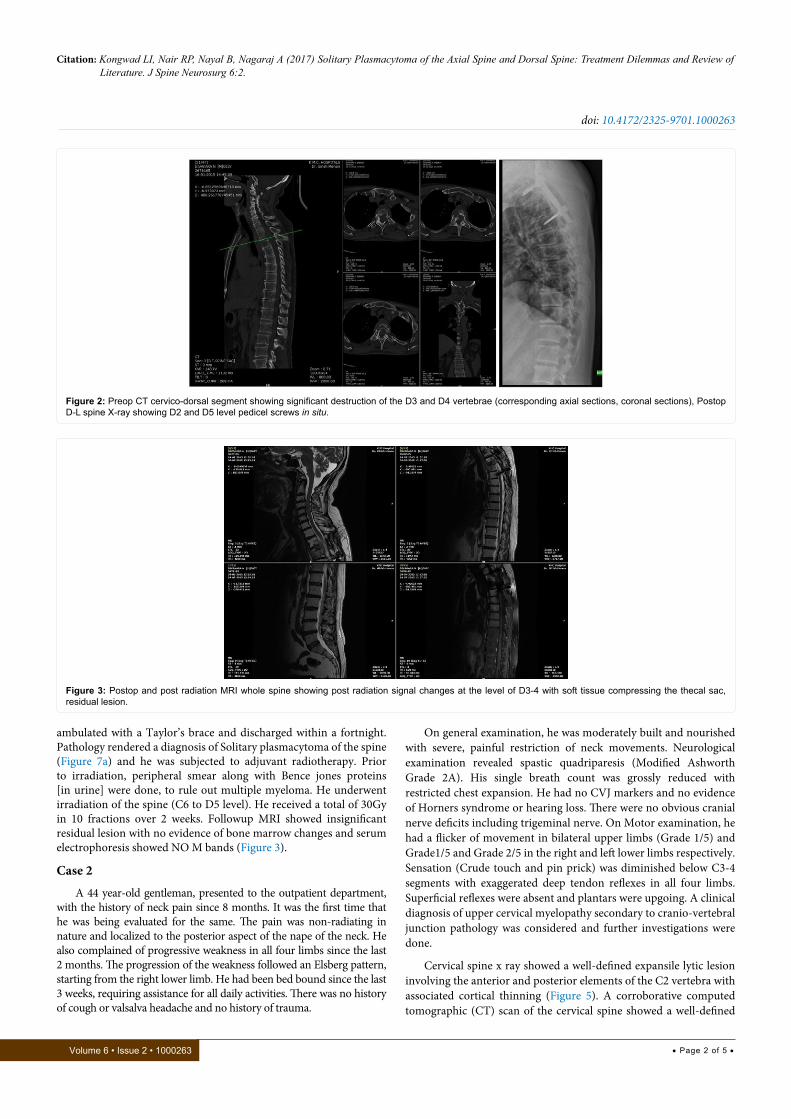
Figure 2: Preop CT cervico-dorsal segment showing significant destruction of the D3 and D4 vertebrae (corresponding axial sections, coronal sections), Postop D-L spine X-ray showing D2 and D5 level pedicel screws in situ.
Figure 3: Postop and post radiation MRI whole spine showing post radiation signal changes at the level of D3-4 with soft tissue compressing the thecal sac, residual lesion.

Citation: Kongwad LI, Nair RP, Nayal B, Nagaraj A (2017) Solitary Plasmacytoma of the Axial Spine and Dorsal Spine: Treatment Dilemmas and Review of Literature. J Spine Neurosurg 6:2.
• Page 3 of 5 •
doi: 10.4172/2325-9701.1000263
Volume 6 • Issue 2 • 1000263
lytic lesion involving the entire C2 vertebra with thinning of the cortex. There was no evidence of basilar invagination (Figure 4).
Magnetic resonance imaging of the cervical spine showed an expansile, lytic lesion, involving the entire C2 body [anterior and posterior elements], hypointense on T1W and hyperintense on STIR with restriction on DWI with post contrast enhancement (Figure 4). There seemed to be a soft tissue component, with possible collection, around the C2 vertebral body, tracking along the para-spinal muscles [more in the left side], extending from the superior end plate of C4 vertebra to the base of the skull. Anteriorly the collection seemed to involve the retropharyngeal space with scabbard appearance of the nasopharynx and oropharynx with maintenance of flow voids within the vessels.
Patient underwent an occipito-cervical fusion with tumour decompression (Figure 6). Post operatively, he was started on aggressive physiotherapy and he showed significant neurological improvement. His power improved to Grade 2/5 on right side and Grade 3/5 on the left.
Histopathological examination proferred a diagnosis of plasmacytoma with CD 138 positivity and he was subjected to adjuvant radiotherapy (Figure 7b).
DiscussionThe optimal treatment for solitary plasmacytoma of the bone
[SPB] is still controversial. Local radiation therapy without surgery is often employed [2,4], but no randomized study has confirmed its superiority over surgery alone. Often encountered in patients in the sixth decade of life, more than 80% of plasmacytoma occur in D6 - L4 region, of these, 50% are seen within D11 - L1 segments, due to biomechanical factors acting on the dorso-lumbar transition zone. It is often difficult to differentiate between potts’ spine, pyogenic and fungal vertebral osteomyelitis from primary and metastatic spinal deposits based on clinical and radiographic findings alone.
Since tuberculosis is almost ubiquitous in the Asian continent, it is often considered as the first diagnosis in young patients with an epidural collection with vertebral body destruction, in the dorsal and dorso-lumbar region, usually without significant neurological deficits. These patients are erroneously started on ATT (Anti-Tubercular treatment) without any confirmatory tests in lieu with the Middle pathway regimen as described by Tuli et al. [6]. This usually is associated with progression of symptoms and subsequent spinal instability. Taneichi et al. established a criteria [7] for vertebral collapse as a result of osteolytic metastatic lesions, they were based on:
Figure 4: Preoperative MRI C-spine axial and sagittal sections showing a C2 lesion with extension to the paraspinal muscles on the left and extending posteriorly, CT shows a lytic lesion involving the C2 body in sagittal, coronal and axial sections. Cervical spine X-ray, lateral view, showing the occipito-cervical rod with C3 and C4 lateral mass screws in situ.
Figure 5: Dynamic X-ray showing no evidence of any cervical listhesis.

Citation: Kongwad LI, Nair RP, Nayal B, Nagaraj A (2017) Solitary Plasmacytoma of the Axial Spine and Dorsal Spine: Treatment Dilemmas and Review of Literature. J Spine Neurosurg 6:2.
• Page 4 of 5 •
doi: 10.4172/2325-9701.1000263
Volume 6 • Issue 2 • 1000263
(a) Morphology of the vertebral destruction at initial diagnosis
(b) Compromised area of vertebral body
(c) Destruction of posterior elements and costovertebral joints (in dorsal spine)
Various diagnostic criteria have been described for diagnosing plasmacytomas, however we have adhered to the IMWG diagnostic criteria [3] (Table 1). Harrington et al. had established that patients who had more than 50% of the vertebral body destroyed required
posterior stabilization along with decompression of the lesion [8]. With our experience in 2 patients, one with an upper dorsal lesion and the other with a C2 lesion, we recommend that all patients with an extradural compression, in the presence of neurological deficits, should undergo surgical decompression in the form of transpedicular decompression of the tumour with posterior stabilization. These patients [once biopsy proven] were also advised to undergo subsequent radiotherapy after 6 to 8 weeks.
In general about 75% of patients, with apparent solitary
Figure 6: Intraoperative image showing occpito-cervical fixation (occiput to C3 and C4 lateral mass screws).
Figure 7a: Photomicrograph showing sheets of plasma cells (H&E, x200).
Figure 7b: Photomicrograph showing immunoreactivity of plasma cells to CD138 (x200).

Citation: Kongwad LI, Nair RP, Nayal B, Nagaraj A (2017) Solitary Plasmacytoma of the Axial Spine and Dorsal Spine: Treatment Dilemmas and Review of Literature. J Spine Neurosurg 6:2.
• Page 5 of 5 •
doi: 10.4172/2325-9701.1000263
Volume 6 • Issue 2 • 1000263
plasmacytomas, progress to develop Multiple Myeloma. Most of these patients may have a positive monoclonal protein in blood or urine (<10 g/l) [5]. The largest series of solitary plasmacytoma, published in 2006 [4] predicted that more than one half of the patients with SPB develop multiple myeloma with a median time to development of 21 months (range 2-135 months). 5 and 10 year probability rates of developing multiple myeloma were 51% (95% CI, 43-59%) and 72% (95% CI, 62-82%), average disease free interval, after diagnosis of solitary plasmacytoma, was 81 months and the 10-year survival rate was 85%. Age more than 60 years was the only independent predictor of development of multiple myeloma [4]. Thus patients with solitary plasmacytoma can expect a benign course and a prolonged progressive free survival, unless the lesion progresses and manifests as a more moribund multiple myeloma.
ConclusionWe strongly recommend that patients with spinal compressive
lesions should undergo decompression with or without stabilization and adjuvant radiation in lieu of diagnosis and to reduce the conversion to multiple myeloma. Radiation alone is advocated in patients who may not withstand surgery; however they have a bad prognosis and bleak survival rates. Surgical decompression offers improved progression free survival rates with a relatively benign course.
References
1. Kim DH, Yoo SD, Kim SM, Im SJ, Hong DW (2012) Atypical Thoracic Solitary Plasmacytoma. Ann Rehabil Med 36: 739-743.
2. British Committee for Standards in Haematology (2004) Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. British Journal of Haematology124: 717-726.
3. The International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group (2003). British Journal of Haematology 121: 749-757
4. Knobel D, Zouhair A (2006) Prognostic factors in solitary plasmacytoma of bone: a multicenter rare cancer network study. BMC Cancer 6: 118.
5. Wilder RB, Ha CS, Cox JD, Weber D, Delasalle K, et al. (2002) Persistence of myeloma protein for more than one year after radiotherapy is an adverse prognostic factor in solitary plasmacytoma of bone. Cancer 94: 1532-1537
6. Tuli SM (1975) Results of treatment of spinal tuberculosis by “middle-path” regime. Bone & Joint Journal 57: 13-23.
7. Taneichi H, Kaneda K, Takeda N, Abumi K, Satoh S (1997) Risk Factors and Probability of Vertebral Body Collapse in Metastases of the Thoracic and Lumbar Spine. Spine 22: 239-245.
8. Harrington KD (1993) Metastatic tumors of the spine: Diagnosis and treatment. Jour. A.A.O.S. 1: 76-86.
Diagnosis Criteria
Solitary plasmacytoma of the bone
No M-protein in serum and/ or urineSingle area of bone destruction due to clonal plasma cellsBone marrow not consistent with multiple myeloma (plasma cells <5%)Normal skeletal survey (and MRI of spine and pelvis if done)No related organ or tissue impairment
Extramedullary plasmacytoma
No M-protein in serum and/ or urineExtramedullary tumor of clonal plasma cellsNormal bone marrowNormal skeletal surveyNo related organ or tissue impairment
Multiple solitary plasmacytomas (+/- recurrent)No M-protein in serum and/ or urineMore than one localized area of bone destruction or extramedullary tumor of clonal plasma cells which may be recurrent
Table 1: International Myeloma Working Group diagnostic criteria of solitary plasmacytoma of bone, extramedullary plasmacytoma and multiple solitary plasmacytomas (+/- recuurent).
Author Affiliation Top1Department of Neurosurgery, KMC, Manipal University, Manipal, India2Department of Pathology, KMC, Manipal University, Manipal, India
Submit your next manuscript and get advantages of SciTechnol submissions
� 80 Journals � 21 Day rapid review process � 3000 Editorial team � 5 Million readers � More than 5000
� Quality and quick review processing through Editorial Manager System
Submit your next manuscript at ● www.scitechnol.com/submission











![Journal of Spine Neurosurgery - SciTechnol Lumbar Spine: A review of One Surgeon’s Experience with Over 10,000 Cases Since 1991 Yeung AT* Abstract ... [TFE] surgery [3,4]. This has](https://img.pdfslide.us/doc/110x75/5e9976d10da73f4be4436166/journal-of-spine-neurosurgery-scitechnol-lumbar-spine-a-review-of-one-surgeonas.jpg)

















