Embed Size (px)
Citation preview
S
O
pen Access
Journal of Neurology and Neuro Toxicology
J Neurol Neuro Toxicol Volume 1(1): 20171
Case RepoRt
MS Stands for Mimicking StrokeMishaal Al khaldi, Farah Al Eisa, Abdulnasser Aboud, Eman Nasim, Khaled Darawil
King Fahad Specialist Hospital, Dammam, Eastern Province, Saudi Arabia
AbstractStroke, Multiple sclerosis and vasculitis may share the same symptoms and sometimes also the radiological findings.
The similarity between these conditions make it difficult to diagnose and it is even more complicated when these conditions coexist and the patient presents with an acute attack. It becomes challenging for physicians to decide which of these diagnoses is behind the flared up symptoms.
All the above diseases can cause broad symptoms which may lead to disability, and making an early diagnosis will limit the burden of the disease and improve the patient’s quality of life; we illustrated this in our case report.
We are presenting a case of a young lady with a Sudden-onset pseudo stroke form of Multiple Sclerosis resulting in a left side hemiplegia; this patient with the bizarre presentation had extensive investigations before a diagnosis was confirmed.
After the right diagnosis was reached, patient was put on an early intensive program rehabilitation using new assistive technology, and within two months time our patient improved magnificently from being totally dependent in bed mobility to be able to walk without assistance.
IntroductionMultiple Sclerosis (M.S) is the most common inflammatory demyelinating disease of the central nervous system (1); it is known to cause scarring in multifocal areas. A cross sectional study conducted in Saudi Arabia in 2016 stated that the largest prevalence of M.S in Saudi Arabia found to be in the Eastern Province (34.4%) (2).
M.S usually has certain clinical features, but it may come with many atypical forms which might be a reason for M.S diagnosis challenge (1). However, with the development of technology many diagnosing equipment have been used to confirm the clinical examinations like Magnetic Resonance Imaging (MRI) or brain CT scan (1).
Once a diagnosis is made, an early rehabilitation along with medications should be offered. Physical therapy is a main element in the M.S rehabilitation program; it is vital in managing gait problems, and in deciding the best assistive devices to assist the movement and ankle foot orthosis (AFO)(1).
Usually the gait disturbance happens due to fatigue, spasticity and weakness which might happen as a result of lesions in the descending motor tracts of the brain and spinal cord, and the disturbed balance can be caused by lesions in the cerebellar pathways (1).
In this case report, a description of a rare M.S presentation will be discussed, used methods for diagnosis, the rehabilitation program applied for this patient and the progress made in the
patient’s functional status upon discharge after four weeks of admission.
Case ScenarioA 20 year old female came to the Emergency unit complaining of three days left side weakness associated with a difficulty in swallowing. The weakness started with paresthesia on the left thigh then it involved the entire left side including the face.
The muscle weakness of the left side reached maximum the day she came the emergency when she was not able to move the left upper and lower extremities.
The patient had no past medical history of note. However, the patient described a bilateral blurred vision one month prior to her admission. This was associated with pain during eye movements for a course of a week then it was resolved without taking any prescribed medications. Her mother had a positive history of Scleroderma.
On clinical examination, there is evidence of nystagmus, left side face drop, flaccidity, hyper-reflexia , un-sustained clonus, positive left Babinski sign, impaired left sensation, Coordination and balance assessment could not be done as the muscle power on the left side was grossly graded as 1/5 with
Correspondence to: Mishaal Al khaldi, Senior Physical therapist, King Fahad Specialist Hospital, Dammam, Eastern Province, Saudi Arabia, Tel: 00966555404862; E-mail: Mishaal[DOT]Alkhaldi1[AT]hotmail[DOT]co[DOT]uk
Received: Sep 12, 2017; Accepted: Sep 15, 2017; Published: Sep 18, 2017
Khaldi MA (2017) MS Stands for Mimicking Stroke
J Neurol Neuro Toxicol Volume 1(1): 20172
sensory impairment. Her swallowing was impaired but her speech, cognition and memory were not affected.
Investigations
Based on the history and clinical assessment patient was likely to have one of the following diagnoses i.e. vasculitis, Behçet’s disease, multiple sclerosis, cardio embolic stroke.
Upon the patient’s arrival to the Emergency Unit, she had a Brain CT Scan, which showed Brain hypodensed areas bringing up a possibility for a stroke. Blood investigations showed negative vasculitis screen, negative Hyper coagulant state screen, negative specific typing for Behçet’s disease, her Echocardiography ruled out cardiac source for thrombosis. The patient declined Lumbar puncture.
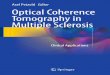
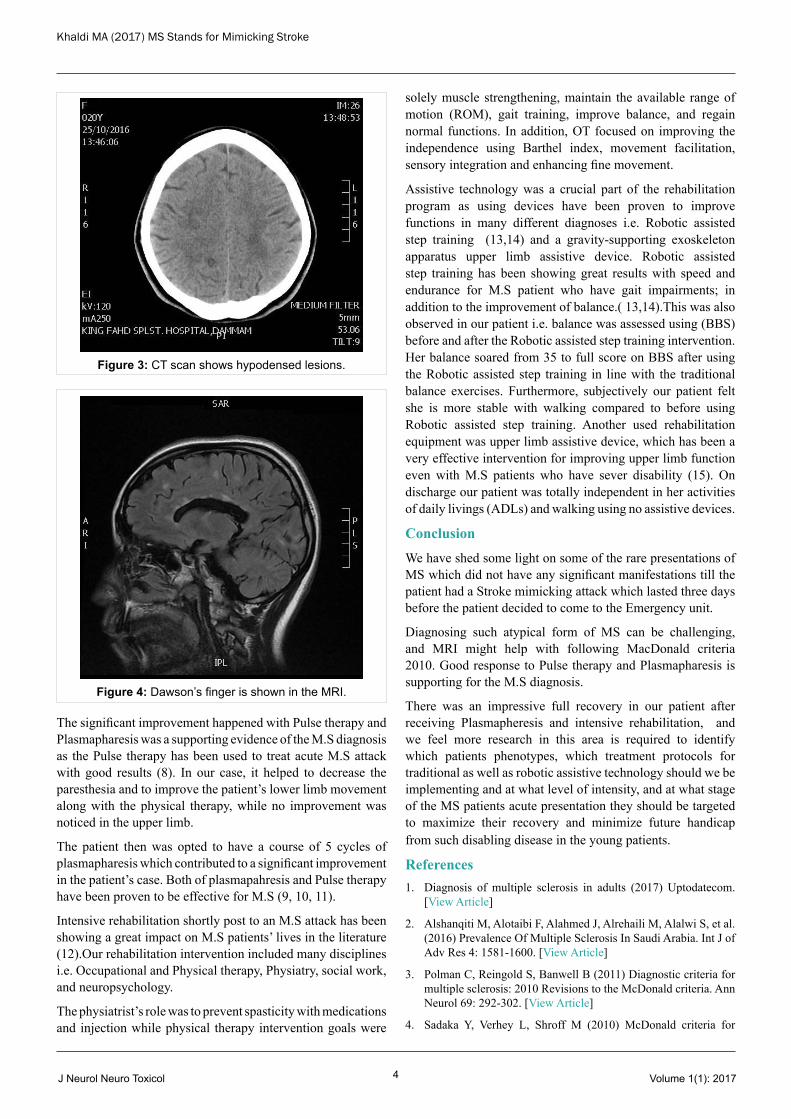
Magnetic resonance imagining (MRI) showed multiple demyelinating lesions on both hemispheres with Dowson’s finger; also non enhancing lesions were found on the cervical and thoracic spine. (Figure: 1, 2, 3, 4)
Management
Rehabilitation intervention started on the second day of admission with physical and occupational therapy; the muscle strength on the left side of the upper and lower extremity was graded as 1/5 except for ankle dorisflexors, hand grip and wrist extensors which were graded as 0/5.
Using Barthel index her Functional independence score was 45/100, and Berg balance scale (BBS) was not implemented as the patient was immobile.
She was started on pulse steroid therapy along with rehabilitation. Within 5 days her paresthesia disappeared, and there was a mild improvement in muscle power in the lower limb which graded as 2/5 except for hip flexors 3/5. However, no improvement in the upper limb muscle strength was observed at that stage. For that reason Plasmapharesis was prescribed and the patient was put on an intensive rehabilitation program.
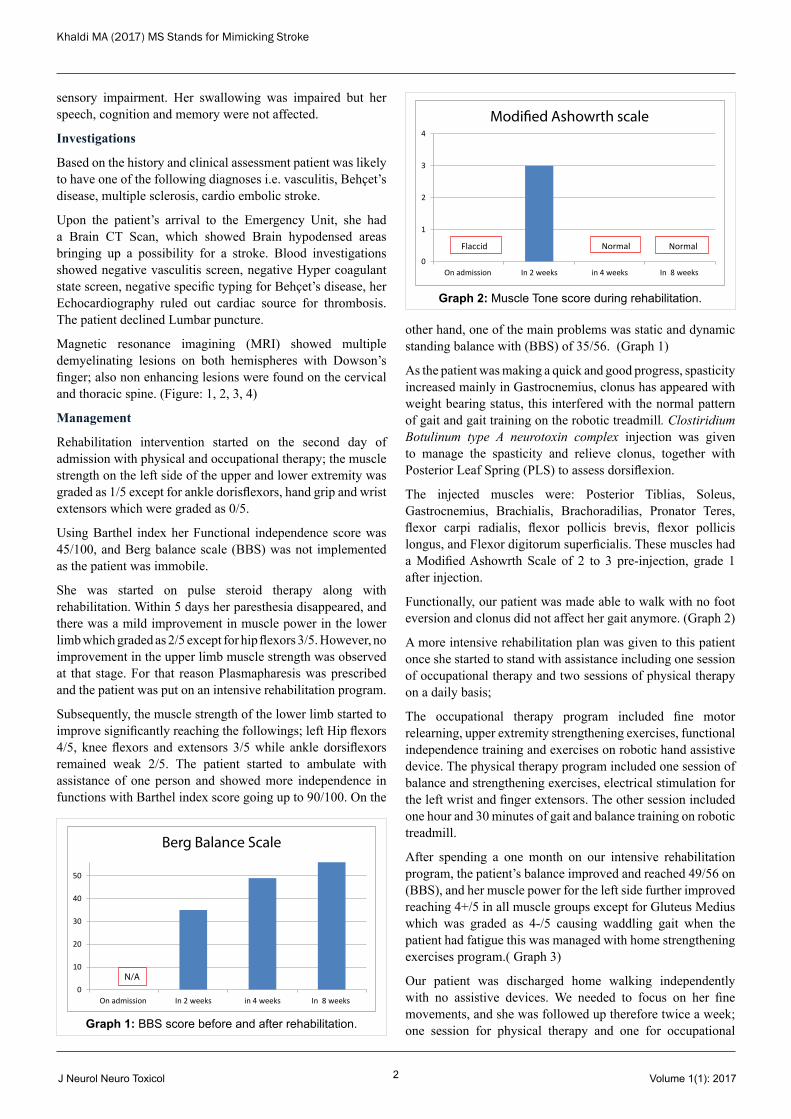
Subsequently, the muscle strength of the lower limb started to improve significantly reaching the followings; left Hip flexors 4/5, knee flexors and extensors 3/5 while ankle dorsiflexors remained weak 2/5. The patient started to ambulate with assistance of one person and showed more independence in functions with Barthel index score going up to 90/100. On the
other hand, one of the main problems was static and dynamic standing balance with (BBS) of 35/56. (Graph 1)
As the patient was making a quick and good progress, spasticity increased mainly in Gastrocnemius, clonus has appeared with weight bearing status, this interfered with the normal pattern of gait and gait training on the robotic treadmill. Clostiridium Botulinum type A neurotoxin complex injection was given to manage the spasticity and relieve clonus, together with Posterior Leaf Spring (PLS) to assess dorsiflexion.
The injected muscles were: Posterior Tiblias, Soleus, Gastrocnemius, Brachialis, Brachoradilias, Pronator Teres, flexor carpi radialis, flexor pollicis brevis, flexor pollicis longus, and Flexor digitorum superficialis. These muscles had a Modified Ashowrth Scale of 2 to 3 pre-injection, grade 1 after injection.
Functionally, our patient was made able to walk with no foot eversion and clonus did not affect her gait anymore. (Graph 2)
A more intensive rehabilitation plan was given to this patient once she started to stand with assistance including one session of occupational therapy and two sessions of physical therapy on a daily basis;
The occupational therapy program included fine motor relearning, upper extremity strengthening exercises, functional independence training and exercises on robotic hand assistive device. The physical therapy program included one session of balance and strengthening exercises, electrical stimulation for the left wrist and finger extensors. The other session included one hour and 30 minutes of gait and balance training on robotic treadmill.
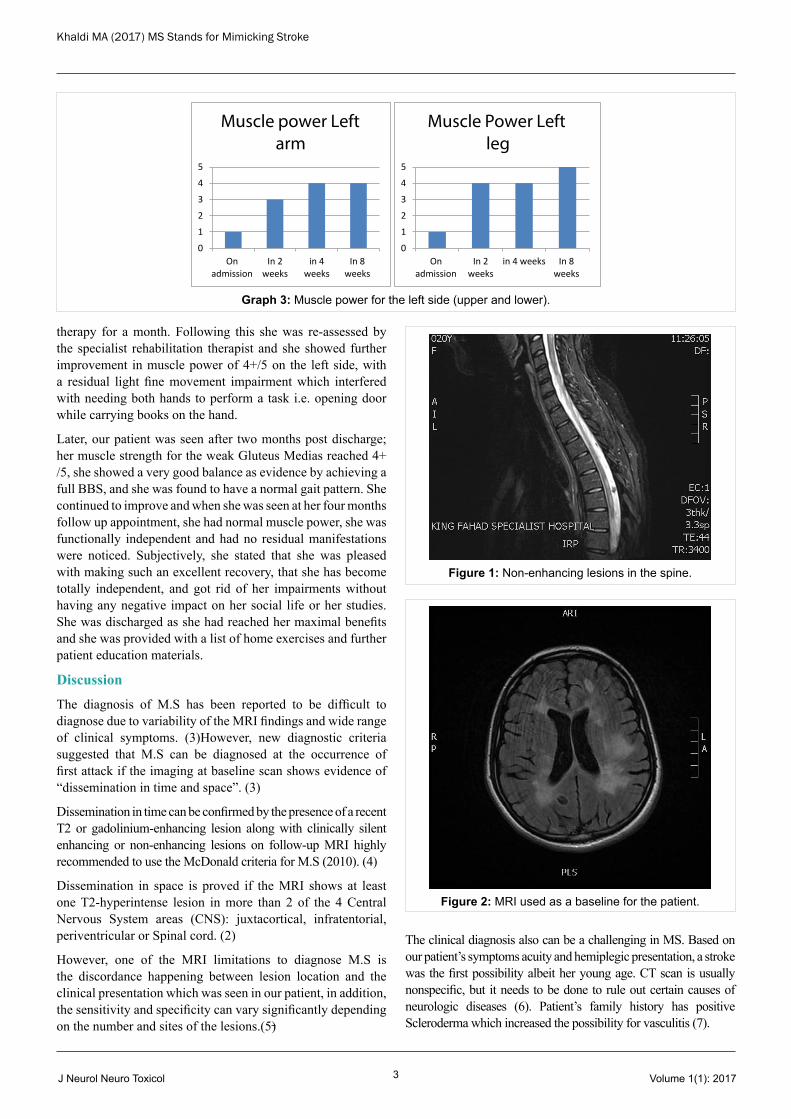
After spending a one month on our intensive rehabilitation program, the patient’s balance improved and reached 49/56 on (BBS), and her muscle power for the left side further improved reaching 4+/5 in all muscle groups except for Gluteus Medius which was graded as 4-/5 causing waddling gait when the patient had fatigue this was managed with home strengthening exercises program.( Graph 3)
Our patient was discharged home walking independently with no assistive devices. We needed to focus on her fine movements, and she was followed up therefore twice a week; one session for physical therapy and one for occupational
0
10
20
30
40
50
On admission In 2 weeks in 4 weeks In 8 weeks
Berg Balance Scale
N/A
Graph 1: BBS score before and after rehabilitation.
0
1
2
3
4
On admission In 2 weeks in 4 weeks In 8 weeks
Modi�ed Ashowrth scale
Normal Normal Flaccid
Graph 2: Muscle Tone score during rehabilitation.
Khaldi MA (2017) MS Stands for Mimicking Stroke
J Neurol Neuro Toxicol Volume 1(1): 20173
therapy for a month. Following this she was re-assessed by the specialist rehabilitation therapist and she showed further improvement in muscle power of 4+/5 on the left side, with a residual light fine movement impairment which interfered with needing both hands to perform a task i.e. opening door while carrying books on the hand.
Later, our patient was seen after two months post discharge; her muscle strength for the weak Gluteus Medias reached 4+ /5, she showed a very good balance as evidence by achieving a full BBS, and she was found to have a normal gait pattern. She continued to improve and when she was seen at her four months follow up appointment, she had normal muscle power, she was functionally independent and had no residual manifestations were noticed. Subjectively, she stated that she was pleased with making such an excellent recovery, that she has become totally independent, and got rid of her impairments without having any negative impact on her social life or her studies. She was discharged as she had reached her maximal benefits and she was provided with a list of home exercises and further patient education materials.
DiscussionThe diagnosis of M.S has been reported to be difficult to diagnose due to variability of the MRI findings and wide range of clinical symptoms. (3)However, new diagnostic criteria suggested that M.S can be diagnosed at the occurrence of first attack if the imaging at baseline scan shows evidence of “dissemination in time and space”. (3)
Dissemination in time can be confirmed by the presence of a recent T2 or gadolinium-enhancing lesion along with clinically silent enhancing or non-enhancing lesions on follow-up MRI highly recommended to use the McDonald criteria for M.S (2010). (4)
Dissemination in space is proved if the MRI shows at least one T2-hyperintense lesion in more than 2 of the 4 Central Nervous System areas (CNS): juxtacortical, infratentorial, periventricular or Spinal cord. (2)
However, one of the MRI limitations to diagnose M.S is the discordance happening between lesion location and the clinical presentation which was seen in our patient, in addition, the sensitivity and specificity can vary significantly depending on the number and sites of the lesions.(5)
The clinical diagnosis also can be a challenging in MS. Based on our patient’s symptoms acuity and hemiplegic presentation, a stroke was the first possibility albeit her young age. CT scan is usually nonspecific, but it needs to be done to rule out certain causes of neurologic diseases (6). Patient’s family history has positive Scleroderma which increased the possibility for vasculitis (7).
0
1
2
3
4
5
On admission
In 2 weeks
in 4 weeks
In 8 weeks
Muscle power Left arm
0
1
2
3
4
5
On admission
In 2 weeks
in 4 weeks In 8 weeks
Muscle Power Left leg
Graph 3: Muscle power for the left side (upper and lower).
Figure 1: Non-enhancing lesions in the spine.
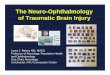
Figure 2: MRI used as a baseline for the patient.
Khaldi MA (2017) MS Stands for Mimicking Stroke
J Neurol Neuro Toxicol Volume 1(1): 20174
The significant improvement happened with Pulse therapy and Plasmapharesis was a supporting evidence of the M.S diagnosis as the Pulse therapy has been used to treat acute M.S attack with good results (8). In our case, it helped to decrease the paresthesia and to improve the patient’s lower limb movement along with the physical therapy, while no improvement was noticed in the upper limb.
The patient then was opted to have a course of 5 cycles of plasmapharesis which contributed to a significant improvement in the patient’s case. Both of plasmapahresis and Pulse therapy have been proven to be effective for M.S (9, 10, 11).
Intensive rehabilitation shortly post to an M.S attack has been showing a great impact on M.S patients’ lives in the literature (12).Our rehabilitation intervention included many disciplines i.e. Occupational and Physical therapy, Physiatry, social work, and neuropsychology.
The physiatrist’s role was to prevent spasticity with medications and injection while physical therapy intervention goals were
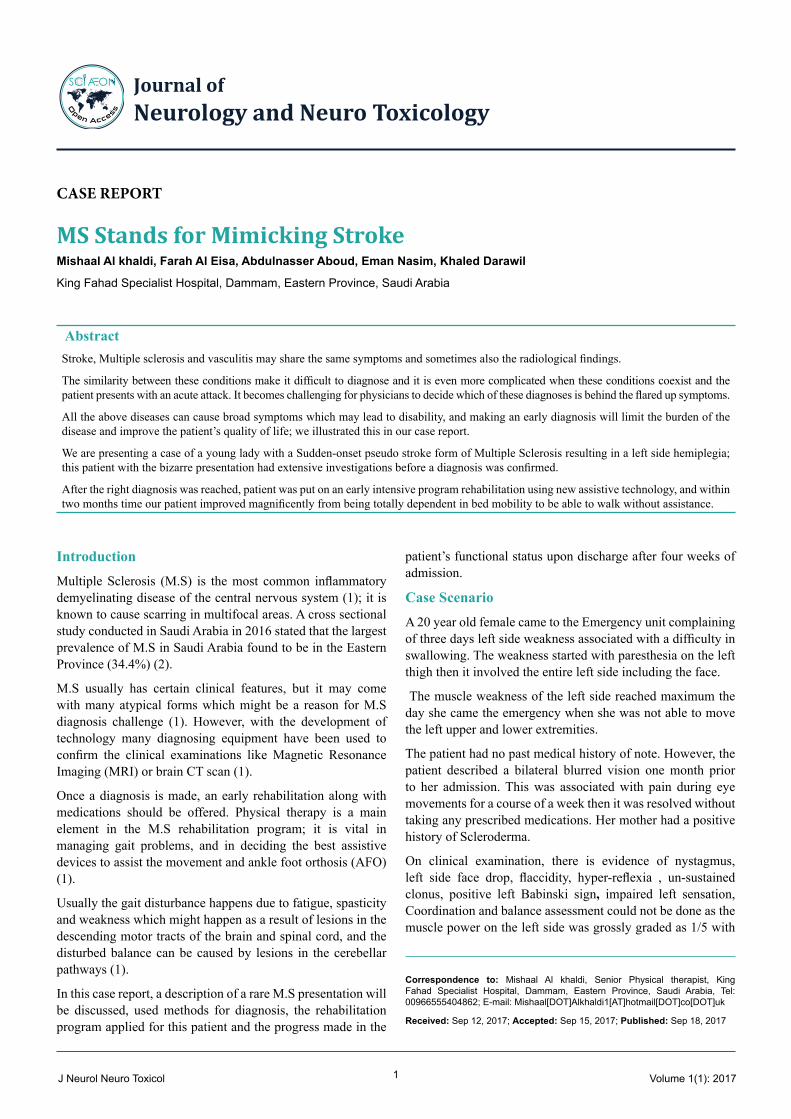
Figure 3: CT scan shows hypodensed lesions.
Figure 4: Dawson’s finger is shown in the MRI.
solely muscle strengthening, maintain the available range of motion (ROM), gait training, improve balance, and regain normal functions. In addition, OT focused on improving the independence using Barthel index, movement facilitation, sensory integration and enhancing fine movement.
Assistive technology was a crucial part of the rehabilitation program as using devices have been proven to improve functions in many different diagnoses i.e. Robotic assisted step training (13,14) and a gravity-supporting exoskeleton apparatus upper limb assistive device. Robotic assisted step training has been showing great results with speed and endurance for M.S patient who have gait impairments; in addition to the improvement of balance.( 13,14).This was also observed in our patient i.e. balance was assessed using (BBS) before and after the Robotic assisted step training intervention. Her balance soared from 35 to full score on BBS after using the Robotic assisted step training in line with the traditional balance exercises. Furthermore, subjectively our patient felt she is more stable with walking compared to before using Robotic assisted step training. Another used rehabilitation equipment was upper limb assistive device, which has been a very effective intervention for improving upper limb function even with M.S patients who have sever disability (15). On discharge our patient was totally independent in her activities of daily livings (ADLs) and walking using no assistive devices.
ConclusionWe have shed some light on some of the rare presentations of MS which did not have any significant manifestations till the patient had a Stroke mimicking attack which lasted three days before the patient decided to come to the Emergency unit.
Diagnosing such atypical form of MS can be challenging, and MRI might help with following MacDonald criteria 2010. Good response to Pulse therapy and Plasmapharesis is supporting for the M.S diagnosis.
There was an impressive full recovery in our patient after receiving Plasmapheresis and intensive rehabilitation, and we feel more research in this area is required to identify which patients phenotypes, which treatment protocols for traditional as well as robotic assistive technology should we be implementing and at what level of intensity, and at what stage of the MS patients acute presentation they should be targeted to maximize their recovery and minimize future handicap from such disabling disease in the young patients.
References1. Diagnosis of multiple sclerosis in adults (2017) Uptodatecom.
[View Article]
2. Alshanqiti M, Alotaibi F, Alahmed J, Alrehaili M, Alalwi S, et al. (2016) Prevalence Of Multiple Sclerosis In Saudi Arabia. Int J of Adv Res 4: 1581-1600. [View Article]
3. Polman C, Reingold S, Banwell B (2011) Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann Neurol 69: 292-302. [View Article]
4. Sadaka Y, Verhey L, Shroff M (2010) McDonald criteria for

Khaldi MA (2017) MS Stands for Mimicking Stroke
J Neurol Neuro Toxicol Volume 1(1): 20175
diagnosing pediatric multiple sclerosis. Ann Neurol 72: 211-223. [View Article]
5. Amy T Waldman (2017) Acute disseminated encephalomyelitis in adults. Uptodatecom. [View Article]
6. Pelidou SH (2007) Multiple sclerosis associated with systemic sclerosis. Rheumatol Int 27: 771-773. [View Article]
7. Waldman A, Gorman M, Rensel M, Austin T, Hertz D, et al. (2011) Management of Pediatric Central Nervous System Demyelinating Disorders: Consensus of United States Neurologists. J Child Neurol 26: 675-682. [View Article]
8. Michael J Olek (2016) Treatment of acute exacerbations of multiple sclerosis in adults. Uptodatecom. [View Article]
9. Weinshenker B, O’Brien P, Petterson T (1999) A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann Neurol 46: 878-886. [View Article]
10. Keegan M, Konig F, McClelland R (2005) Relation between humoral pathological changes in multiple sclerosis and response to therapeutic plasma exchange. Lancet 366: 579-582. [View Article]
11. Rietberg MB (2017) Exercise therapy for multiple sclerosis. Cochrane Database Syst Rev 25. [View Article]
12. Beer S, Aschbacher B, Manoglou D, Gamper E, Kool J, et al. (2007) Robot-assisted gait training in multiple sclerosis: a pilot randomized trial. Mult Scler 14: 231-236. [View Article]
13. Freeman J, Gear M, Pauli A (2010) The effect of core stability training on balance and mobility in ambulant individuals with multiple sclerosis: A multi-centre series of single case studies. Mult Scler 16: 1377-1384. [View Article]
14. Gijbels D, Lamers I, Kerkhofs L, Alders G, Knippenberg E, et al. (2011) The Armeo Spring as training tool to improve upper limb functionality in multiple sclerosis: a pilot study. J Neuroeng Rehabil 8: 5. [View Article]
Citation: Khaldi MA, Eisa FA, Aboud A, Nasim E, Darawil K (2017) MS Stands for Mimicking Stroke. J Neurol Neuro Toxicol 1: 001-005.
Copyright: © 2017 Mishaal Al khaldi et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.