Embed Size (px)
Citation preview

Manuscript Accepted Early View Article
Page 1 of 19
Early View Article: Online published version of an accepted article before publication in the final form.
Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD)
Type of Article: ORIGINAL ARTICLE
Title: Head coring for chronic calcific pancreatitis (CCP) without head mass - Short term outcome analysis
Authors: Rajamahendran Rajendran, Anbalagan Amudhan, Prabhakaran R, Benet
Duraisamy, Rajendran Vellaisamy, Kannan D, Chandramohan SM
doi: To be assigned
Received: 11th August 2014
Accepted: 10th September 2014
How to cite the article: Rajendran R, Amudhan A, Prabhakaran R, Duraisamy B, Vellaisamy R, Kannan D, Chandramohan SM. Head coring for chronic calcific pancreatitis (CCP) without head mass - Short term outcome analysis. International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD). Forthcoming 2014.
Disclaimer: This manuscript has been accepted for publication. This is a pdf file of the Early View Article. The Early View Article is an online published version of an accepted article before publication in the final form. The proof of this manuscript will be sent to the authors for corrections after which this manuscript will undergo content check, copyediting/proofreading and content formatting to conform to journal’s requirements. Please note that during the above publication processes errors in content or presentation may be discovered which will be rectified during manuscript processing. These errors may affect the contents of this manuscript and final published version of this manuscript may be extensively different in content and layout than this Early View Article.

Manuscript Accepted Early View Article
Page 2 of 19
TYPE OF ARTICLE: ORIGINAL ARTICLE 1
2
TITLE: Head coring for chronic calcific pancreatitis (CCP) without head mass - Short 3
term outcome analysis 4
5
AUTHORS: 6
Rajamahendran Rajendran1, Anbalagan Amudhan2, Prabhakaran R3, Benet 7
Duraisamy4, Rajendran Vellaisamy5, Kannan D6, Chandramohan SM7 8
9
AFFILIATIONS: 10
1Post Graduate in Surgical Gastroenterology, Institute of Surgical Gastroenterology, 11
Rajiv Gandhi Government General Hospital, Chennai, Tamil Nadu, INDIA. Email ID: 12
2Assistant Professor in Surgical Gastroenterology, Institute of Surgical 14
Gastroenterology, Rajiv Gandhi Government General Hospital, Chennai, Tamil 15
Nadu, INDIA. Email ID: [email protected] 16
3Assistant Professor in Surgical Gastroenterology, Institute of Surgical 17
Gastroenterology, Rajiv Gandhi Government General Hospital, Chennai, Tamil 18
Nadu, INDIA. Email ID: [email protected] 19
4Assistant Professor in Surgical Gastroenterology, Institute of Surgical 20
Gastroenterology, Rajiv Gandhi Government General Hospital, Chennai, Tamil 21
Nadu, INDIA. Email ID: [email protected] 22
5Post graduate in Surgical Gastroenterology, Institute of Surgical Gastroenterology, 23
Rajiv Gandhi Government General hospital, Chennai, Tamil Nadu, INDIA. Email ID: 24
6Professor of Surgical Gastroenterology, Institute of Surgical Gastroenterology, Rajiv 26
Gandhi Government General Hospital, Chennai, Tamil Nadu, INDIA. Email ID: 27
7Director of Surgical Gastroenterology, Institute of Surgical Gastroenterology, Rajiv 29
Gandhi Government General Hospital, Chennai, Tamil Nadu, INDIA. Email ID: 30
32

Manuscript Accepted Early View Article
Page 3 of 19
CORRESPONDING AUTHOR DETAILS 33
Dr. Rajamahendran Rajendran, 34
Madras Medical College, Institute of Surgical Gastroenterology, Rajiv Gandhi 35
Government General Hospital, Chennai, Tamil Nadu, INDIA. 36
Phone No: 09787387183/094444878183 37
Email ID: [email protected] 38
39
Short Running Title: Head coring for Chronic Calcific Pancreatitis without head 40
mass- Short term outcome analysis. 41
42
Guarantor of Submission: The corresponding author is the guarantor of 43
submission. 44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63

Manuscript Accepted Early View Article
Page 4 of 19
TITLE: Head coring for chronic calcific pancreatitis (CCP) without head mass - Short 64
term outcome analysis 65
66
ABSTRACT 67
Aims: 68
Intolerable abdominal pain is the main cause which brings the patients with Chronic 69
Calcific Pancreatitis to the surgeon. As head is the pacemaker of pain in chronic 70
pancreatitis coring out the head even in the absence of inflammatory head mass 71
provides better pain relief. 72
73
Materials and Methods: 74
This retrospective cum prospective study analyzed the outcome of Frey procedure in 75
Chronic Calcific Pancreatitis patients without inflammatory head mass. Methods. For 76
the period between 2010 and 2013, 140 patients with chronic pancreatitis underwent 77
Frey procedure for intractable abdominal pain. Of them 80 patients without head 78
mass were included in the study. The mean follow-up was 6 months. Using Visual 79
analogue scale score pain was analyzed both preoperatively and postoperatively. 80
Endocrine and exocrine insufficiencies are also analyzed. 81
82
Results: 83
There was no 30-day mortality. Statistical analysis showed significant improvement 84
of Pain score. The improvement of Pain score in the patients without head mass is 85
comparable to the patients with head mass for whom Frey procedure was done. 86
Though there is improvement in Endocrine and exocrine insufficiency they are not 87
statistically significant as per Chi- Square test. 88
89
Conclusion: 90
This study shows that even in the patients with no head mass, the head coring 91
Pancreatico jejunostomy procedure described by Frey provides a better quality of life 92
and better pain relief with acceptable morbidity and nil mortality. Head coring 93
procedure can be therefore strongly recommended for pain relief even in pancreatitis 94
without head mass. 95

Manuscript Accepted Early View Article
Page 5 of 19
Keywords: Chronic calcific pancreatitis, Non-head mass CCP, Head coring, Pain 96
score, Pancreatico Jejunostomy, Frey procedure. 97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126

Manuscript Accepted Early View Article
Page 6 of 19
TITLE: Head coring for chronic calcific pancreatitis (CCP) without head mass - Short 127
term outcome analysis 128
129
INTRODUCTION 130
Intolerable abdominal pain is the main cause which brings the patients with Chronic 131
Calcific Pancreatitis to the surgeon .There are many causes for the pain in Chronic 132
Pancreatitis which includes ductal hypertension [1], increased parenchymal 133
pressure, perineural inflammation [2] or as a complication of the disease. There are 134
various interventions available to relieve the pain in Chronic Calcific Pancreatitis like 135
conservative [3, 4] and surgical management [5]. Based on the morphology of the 136
gland resection [6] and drainage [7] are the two types of surgeries that are available. 137
Of the Chronic Pancreatitis cases, 18-50% of patients present with an inflammatory 138
head mass [6] and its resection was considered very essential to relieve the pain by 139
removing the ‘‘pacemaker of pain’’ [8]. In 1987, Frey et al. reported a novel technique 140
for patients with inflammatory head mass commonly known as Frey Procedure in 141
which local resection of the head of pancreas combined with longitudinal 142
pancreatico-jejunostomy (LR-LPJ) was done. It was found that this Frey procedure 143
provided excellent pain control in 90% of the patients with low mortality and morbidity 144
[9]. There are a sub group of patients who present with Chronic Calcific Pancreatitis 145
without head mass with or without a dilated duct. Routine practice in those patients is 146
to do Lateral Pancreatico jejunostomy known as Modified Puestow’s procedure. 147
Aim and Background: 148
Pancreatitis induced pain can be relieved adequately by removing the pacemaker, 149
draining the major and branch ducts sufficiently, removing the stones in the duct and 150
parenchyma around the head. The cored out tissue will be also available to rule out 151
malignancy in pancreas. This study enlightens that since the head is the “Pacemaker 152
of Pain” [10a,b] if we apply the same procedure of Head coring for the patients 153
without head mass there will be good pain control without added morbidity or 154
mortality. Frey Procedure was done in 80 patients who presented to us without 155
pancreatic head mass. Short term outcome analysis was done and results are 156
analyzed by the statistical variables. 157
158

Manuscript Accepted Early View Article
Page 7 of 19
MATERIALS AND METHODS 159
Patients and Methods: 160
This is a combined prospective and retrospective study was done at Rajiv Gandhi 161
Government General Hospital by the Department of Surgical gastroenterology 162
between 2010 and 2013, 140 patients with chronic Calcific Pancreatitis underwent 163
Frey procedure for intractable abdominal pain. All patients had a detailed history and 164
clinical examination. The diagnostic workup includes measuring the Serum amylase, 165
Lipase, CA-19-9 and ultrasonography (USG), Upper GI endoscopy, Portal vein 166
Doppler, Computed tomographic scanning (CT), and magnetic resonance cholangio 167
pancreatography (MRCP). These patients presented to us with a typical history of 168
abdominal pain that is present in the epigastrium and radiating to the back. We 169
further evaluated and confirmed the diagnosis by looking at the pancreatic 170
calcification or dilatation of main pancreatic duct on imaging (US, CT scan, MRCP). 171
Head mass is defined by the presence of the mass in the head of pancreas with a 172
Antero posterior head diameter was more than 35 mm in CECT abdomen [11a,11b]. 173
Small or non-dilated duct is the name given if it measured 5 mm or less at neck [12]. 174
Main duct was considered as dilated if it measured greater than 7 mm in its maximal 175
diameter. Exocrine function of the pancreas was assessed by the presence or 176
absence of steatorrhea. Steatorrhea is defined as frequency of more than three 177
stools per day with nauseating smell and greasy consistency [13]. Pain was 178
assessed using Visual Analogue Scale (VAS) and frequency of pain attacks along 179
with analgesic requirement16. Surgery was offered to those patients who had Visual 180
analogue scale pain score more than 8. 181
Patient Exclusions: 182
Of the 140 cases of Chronic calcific pancreatitis those patients with head mass and 183
pseudocyst in the head are eliminated from the study. We also eliminated the 184
patients who failed to show alcohol abstinence. Patients who have completed at 185
least six months follow-up alone were included in the study. 186
In that way we selected only 80 patients who presented to us with Chronic Calcific 187
pancreatitis without head mass (CECT abdomen showing head of pancreas Antero 188
posterior diameter less than 35 mm) and had regular follow up for 6 months. 189
Surgical Procedure: 190

Manuscript Accepted Early View Article
Page 8 of 19
The head coring procedure was performed exactly as described by Frey and Smith 191
[14]. The coring was done at the head of pancreas after lay opening the major duct. 192
The coring was continued without breaching the posterior pancreatic capsule. In 193
most cases we could identify the duct by aspiration method. Using Diathermy and 194
Harmonic scalpel the head and uncinate process of pancreas were cored out. The 195
amount of tissue cored was measured in grams. After perfect hemostasis, a loop of 196
jejunum brought in Roux En Y fashion to Pancreas and pancreatico jejunostomy 197
using a continuous 3’0 polyglactin in a single continuous layer. All the cored out 198
pancreatic tissue was sent for histopathological examination. Most patients were 199
discharged by 10th postoperative day after suture removal. 200
201
RESULTS 202
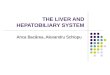
A total of 80 patients were analyzed. Of them 60 were male and 20 were female. The 203
age of the patients varies between 13 to 58 yrs. The mean age and SD is 37 +10.4 204
years (Figure 1). Regarding the etiology of chronic calcific pancreatitis, alcohol was 205
associated in 58 patients and 22 patients were considered to be tropical Calcific 206
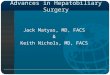
pancreatitis. (Table 1). Of the various complications in this group (Figure 2): 10 207
presented with diabetes mellitus, 6 presented with exocrine insufficiency, Splenic 208
vein thrombosis with fundal varices was seen in 3 patients. Pseudocyst in the tail of 209
the pancreas was seen in 7 patients. Pancreatic ascites was present in 3 patients 210
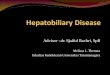
and only two of them without head mass presented with jaundice. All the patients 211
underwent Contrast enhanced CECT to look for calcifications and head mass (Figure 212
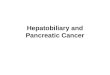
3). MRCP was done in 2 patients who presented with jaundice (Wadsworth 213
syndrome) both of them had a tapering end of the distal CBD in the absence of head 214
mass( figure 4) . Upper GI scopy and portal venous Doppler was done for all 215
patients. Only three patients who has splenic vein thrombosis on portal vein doppler 216
had fundal varices on endoscopy and diagnosed as Sinistral Portal hypertension. All 217
the patients underwent Frey procedure as already described, amount of tissue cored 218
was measured in grams (Figure 5e) Average tissue coring done in the 80 patients is 219
3.8 grams. (Figures 5a,b,c,d,e) 220
Additional procedures like Distal pancreatectomy with splenectomy was done in 10 221
patients – 3 patients who had Sinistral portal hypertension, 7 patients who had 222

Manuscript Accepted Early View Article
Page 9 of 19
pseudocyst in tail of pancreas. 6 patients who had small duct disease underwent 223
Izbikis ‘V’ shaped opening of the duct along with head coring. For the 2 patients who 224
had jaundice choledocho jejunostomy was done in 1 patient and the other patient 225
had relief of jaundice after coring (Table 2). All the other patients underwent single 226
layered Mucosa to mucosa Pancreatico jejunostomy using 3’0 Polypropylene 227
continuous sutures. (Figure 5.c and d) 228
No patient had major intra op complications. Mean blood loss is 150 ml. Mean 229
duration of surgery is 3 and half hours. There was no 30-day mortality. In this series 230
significant complications occurred in 10 patients. It included 3 with pulmonary 231
complications, 5 with wound infection, one had gastric outlet obstruction due to 232
Jejuno jejunal intussusception which was managed by laparotomy and one had 233
pancreatic leak which settled after 2 months by conservative management (Table 3). 234
The pulmonary complications that were mentioned include two patients with left lung 235
basal atelectasis and one patient with aspiration pneumonia. Atelectasis was treated 236
with Intravenous deriphylline, nebulization with bronchodilators and chest 237
physiotherapy. Aspiration pneumonitis was treated with Antibiotics and 238
bronchodilators. Wound Infection cases underwent Pus Culture and sensitivity and 239
appropriate antibiotics were added based on the antibiotic sensitivity. 4 cases had 240
Staphylococcus aureus positive in the culture test and one patient had E.Coli and 241
Kliebsiella grown in culture. One patient had jejuno jejunal intussusception at the 242
Jejuno jejunostomy site of anastomosis. The jejuno jejunostomy was done in that 243
case in an end to side fashion. The patient presented to us with history of pain 244
abdomen and vomiting after 2 months of surgery. When we did Gastrograffin study 245
we found that there is cut off at the level of upper jejunum with distension of 246
stomach. CECT abdomen showed the presence of intussusception. For that patient 247
we did relaparotomy and did disconnection of Jejuno jejunostomy. A new 248
anastomosis was done in a side to side fashion between the pancreatic limb of the 249
jejunum and afferent limb of jejunum. Biopsy of the cored tissue obtained in all cases 250
– Biopsy report came as chronic pancreatitis with only one patient showed evidence 251
of malignancy and she was referred to medical oncology for Gemcitabine based 252
Chemotherapy. The patient was under follow up with us for 6 months. He didn’t 253
develop any metastasis until 6 months. His CA 19-9 level after 6 months was 10. All 254

Manuscript Accepted Early View Article
Page 10 of 19
patients were followed up for 6 months regularly in OP and register was maintained 255
about the pain score based on Visual Analogue Scale ( VAS )score, Diabetic control 256
(in terms of reduction in Hba1c and reduction in dose of insulin/OHA) or new onset 257
diabetes, weight gain and about exocrine insufficiency. 258
On follow up for 6 months period, 72 (90%) had complete pain relief and 8(10%) 259
patients on follow up found to have VAS score of 8. Coeliac plexus blockade was 260
given in the follow up period if they do not respond for analgesics for a period of two 261
months. Only those patients who had retractable pain after 2 months of analgesics 262
were selected for CECT guided Coeliac Plexus blockade. Of the 8 patients, only 6 263
needed coeliac plexus blockade and 2 patients were comfortable with analgesics. Of 264
the 10 patients with diabetes 4 (40%) of them improved in glycemic control with 265
reduction of Insulin dose and reduction in HBa1c after 3 months. Of the 6 patients 266
with steatorrhea 4 (66%) had improvement of symptoms. No patient developed new 267
diabetes or steatorrhea in the 6 month follow up period. About 54 patients (67.5%) 268
developed a weight gain of more than 5 kilograms in 6 months (Table 4) 269
Using Chi square test, the variables analyzed showed statistically significant p value 270
for pain relief and there is no statistical significance in the glycemic control and 271
steatorrhea( table 4) With the data obtained the mean and SD for pain score before 272
is 8.33+ 0.66 and the mean score and SD after surgery 1.14 + 0.47. Using paired t 273
test p value <0.0001, significant as per statisticians analysis (Table 5). 274
275
DISCUSSION 276
Surgical intervention for chronic pancreatitis is the most effective therapeutic option 277
for pain control and management of complications as per all studies. The main aim of 278
the surgical treatment of CP is to alleviate severe pancreatic pain and to manage 279
pancreatitis-related loco regional complications. Although lateral pancreatico 280
jejunostomy (Partingtons Rochalle) which had been practised over 3 decades, it is 281
clear that this is not a technique that solves all problems for patients with Chronic 282
pancreatitis. 283
Many of the patients who underwent LPJ had recurrence of pain, which was often 284
attributed to persistence or relapse of the disease in the pancreatic head. So the 285
symptomatic relief which was the demand by most of the patients were not met. It is 286

Manuscript Accepted Early View Article
Page 11 of 19
only the symptomatic relief that we are aiming to achieve. The principle of Frey's 287
procedure is to decompress the branch ducts in the head of the pancreas, which is 288
considered to be the pacemaker of the disease ("controller of inflammation,") [20]. 289
The pancreatic head region is excised almost in its entirety, leaving behind a bridge of 290
pancreatic tissue about 1cm wide, while a rim of pancreas (5 to 10 mm) remains 291
beside the duodenum and on the upper margin of the pancreatic head [21,22]. The 292
pancreatic neck above the portal vein and superior mesenteric vein are left intact. 293
Regarding the post operative quality of life in terms of pain relief Frey procedure gives 294
much better life. Frey procedure is accepted as a ‘‘patient friendly’’ procedure with 295
zero mortality and a low morbidity rates [15].. Our mortality and morbidity is well 296
within the acceptable range as that of Frey procedure for Head mass Chronic 297
Calcific Pancreatitis (Table 6) 298
By doing surgery for chronic pancreatitis we aim at achieving the complete pain relief 299
and at the same time preserving the endocrine and exocrine function as much as 300
possible. As per the data, 70-80% of the patients with varying follow-up after this 301
procedure had good pain control [16,17]. A few patients having poor pain outcome 302
after surgery are multifactorial and may include inadequate drainage of head, 303
neuropathic changes and unrecognized cancer [18]. An incidence of 10-20% of 304
persistent recurrent symptoms has been reported following Frey procedure. A 305
significant improvement in diabetes and exocrine function is seen following the 306
decompression of the ductal system [19]. In our series we had improvement in both 307
endocrine and exocrine insufficiency though they are statistically not significant. 308
309
CONCLUSION 310
This study shows that the head coring Pancreatico jejunostomy procedure described 311
by Frey provides a better quality of life and better pain relief with acceptable 312
morbidity and nil mortality even in the patients with no head mass. Head coring 313
procedure can be therefore strongly recommended for pain relief even in pancreatitis 314
without head mass. Large scale RCTs must be done comparing the outcomes of LR-315
LPJ and LPJ alone for non-head mass Chronic Calcific Pancreatitis in future. 316
317
318

Manuscript Accepted Early View Article
Page 12 of 19
CONFLICT OF INTEREST 319
Authors declare no conflict of interest 320
321
REFERENCES 322
1. Ebbehoj N, Svendsen LB, Madsen P. Pancreatic tissue pressure in chronic 323
obstructive pancreatitis. Scand J Gastroenterol 1984;19:1066-8. 324
2. Bockmann DE, Buchler M, Malfertheiner P, Beger HG. Analysis of nerves in 325
chronic pancreatitis. Gastroenterology 1988;94:1459-69. 326
3. Buechler MW, Binder M, Friess H. Role of somatostatin and its analogues in the 327
treatment of acute and chronic pancreatitis. Gut 1994;3:515-9. 328
4. Carr-Locke DL. Endoscopic procedures in the treatment of pancreatic pain. Acta 329
Chir Scand 1990;156:293-8. 330
5. Warshaw AL, Banks PA, Fernandez-del Castillo C. AGA technical review: 331
Treatment of pain in chronic pancreatitis. Gastroentrology 1998;115:765-76. 332
6. Traverso LW, Kozarek RA. Pancreaticoduodenectomy for chronic pancreatitis. 333
Ann surg 1999;236:429-36. 334
7. Bradley EL. Long-term results of pancreatojejunostomy in patients with chronic 335
pancreatitis. Am J Surg 1987;153:207-13. 336
8. Traverso LW. The surgical management of chronic pancreatitis: the Whipple 337
procedure. Adv Surg 1999;32:23-39. 338
9. Pessaux P, Kianmanesh R, Regimbeau JM. Frey procedure in the treatment of 339
chronic pancreatitis: short-term results. Pancreas 2006;33(4):354-8. 340
10a. Fischer Mastery of surgery 6th edition.page1401 Keith D.Lilemoe and Chad 341
G.Ball.(b) Shackelford’s Surgery of Alimentary tract- 7th Edition- Page 1138. Table 342
89-5 343
11a. Strate T, Taherpour Z, Bloechle C. Long term follow-up of a randomized trial 344
comparing the Beger and Frey procedures for patients suffering from chronic 345
pancreatitis. Ann Surg 2005;241:591-8. 346
11b. Factors affecting outcome after Frey procedure for chronic pancreatitis 347
:Anbalagan amudhan, tirupporur govindaswamy balachandar, Devy gounder 348
kannan, govindhasamy rajarathinam, Vellayudham vimalraj, shanmugasundaram 349
rajendran, 350

Manuscript Accepted Early View Article
Page 13 of 19
Palanisamy ravichandran, satyanesan jeswanth & Rajagopal surendran, hpb 2008 351
12. Shrikande SV, Kleeff J, Friess H. Management of pain in small duct chronic 352
pancreatitis. J Gastrointest Surg 2006;10:227-33. 353
13. Rault A, Sacunha A, Klopfenstein D. Pancreaticojejunal anastomosis is 354
preferable to pancreaticogastrostomy after pancreaticoduodenectomy for long term 355
outcomes of pancreatic exocrine function. J Am Coll Surg 2005;201:239-44. 356
14. Frey CF, Smith GJ. Description and rationale of a new operation for chronic 357
pancreatitis. Pancreas 1987;2:701-7. 358
15. Izbicki JR, Bloeche C. Drainage operation as therapeutic principle of surgical 359
organ saving treatment of chronic pancreatitis. Chirurug 1997;68(9):865-73. 360
16. Frey CF, Amikura K. Local resection of the head of the pancreas combined with 361
longitudinal pancreaticojejunostomy in the management of patients with chronic 362
pancreatitis. Ann Surg 1994;220:492-507. 363
17. Keus E, van Laarhoven CJ, Eddes EH. Size of the pancreatic head as a 364
prognostic factor for the outcome of Beger’s procedure for painful chronic 365
pancreatitis. Br J Surg 2003;90(3):320-4. 366
18. Markowitz JS, Rattner DW, Warshaw AL. Failure of symptomatic relief after 367
pancreaticojejunal decompression for chronic pancreatitis. Strategies for salvage. 368
Arch surg 1994;129(4):374-9. 369
19. Nealon WH, Thompson JC. Progressive loss of pancreatic function in chronic 370
pancreatitis is delayed by main pancreatic duct decompression: a longitudinal 371
prospective analysis of the modified Puestow procedure. Ann Surg 1993;217:458-68. 372
20. Egawa S, Motoi F, Sakata N, et al. Assessment of Frey procedures : Japanese 373
experience. J Hepatobiliary Pancreat Sci 2010;17:745-751. 374
21. Frey CF, Smith GJ. Description and rationale of a new operation for chronic 375
pancreatitis. Pancreas 1987;2:701-707. 376
22. Frey CF, Amikura K. Local resection of the head of the pancreas combined with 377
longitudinal pancreaticojejunostomy in the management of patients with chronic 378
pancreatitis. Ann Surg 1994;220:492-504. 379
380
381
382

Manuscript Accepted Early View Article
Page 14 of 19
TABLES 383
Table: 1: Etiology of Chronic Calcific Pancreatitis without Head mass. 384
Cause Number Percentage
Alcohol 58 72.5%
Tropical and others 22 27.5%
385
Table 2: Additional procedures performed. 386
Features Procedure Number of cases
(%)
Pseudocysts in tail of
pancreas
Frey+ Distal pancreatectomy and
splenectomy
7 (8.75%)
Sinistral portal hypertension Frey+ Distal Pancreatectomy and
splenectomy
3 (3.75%)
Wadsworth syndrome Choledocho jejunostomy 1 (1.25%)
Small Duct disease Izbikis with Head coring 6 (7.5%)
387
388
Table 3: Post operative complications. 389
Complications Number of patients (%)
Wound infection 5 (6.25%)
Pulmonary complication 3 (3.75%)
Jejuno jejunal intussusception 1 ( 1.25%)
Pancreatic fistula 1 (1.25%)
390
391
392
393
394
395
396
397

Manuscript Accepted Early View Article
Page 15 of 19
Table 4: Follow Up. 398
S:No Variable Preop Post op Improvement
(%)
P value
1 Pain score ( >8) 80 (100%) 8(10%) 90% <0.00001
2 Diabetes mellitus
( reduction in Hba1c and
Insulin/OHA agents dose)
10 (100%) 6 (60%) 40% 0.29
3 Steatorrhea ( Increased stool
frequency >3 with oily nature)
6 (100%) 2 (44%) 66% 0.14
4 Weight gain >5 kg after 6
months
- 52 67.5% -
399
400
Table 5: Analysis of Pre op and Post op variables. 401
S:No Variables Pre op score Post op values P Value
1 Pain score 8.33+ 0.66 1.14 + 0.47 <0.00001
(significant)
402
403
Table 6: Various studies showing the outcome of Frey procedure. 404
Pain remission at end
of follow up (%)
Average follow
up( Months)
N
Frey and Amikura ( 1994) 86.7 37 50
Izbicki et al (1995) 89 17 22
Ho and Frey (2001) 88 38.4 75
Falconi et al (2006) 88.8 60 40
Pessaux et al ( 2006) 88 15 34
Egawa et al (2009) 100 46
Keck et al (2010) 62 43 50
Negi et al ( 2010) 75 76.8 60
405

Manuscript Accepted Early View Article
Page 16 of 19
FIGURE LEGENDS 406
Figure 1: Age distribution of Chronic Calcific Pancreatitis without Head mass. 407
Figure 2: Complications of CCP without head mass. 408
Figure 3: CECT abdomen showing diffuse parenchymal calcification in head and 409
body. 410
Figure 4: MRCP showing Biliary stricture (Wadsworth syndrome). 411
Figure 5: Intraoperative pictures: (a) Removal of stones. (b) Head coring & opening of 412
duct. (c) Anastomosing the jejunum with pancreas. (d) Completed LR-LPJ. (e) 413
Removed stones and cored tissue being weighed. 414
415
FIGURES 416
417
Figure 1: Age distribution of Chronic Calcific Pancreatitis without Head mass. 418
419

Manuscript Accepted Early View Article
Page 17 of 19
420
Figure 2: Complications of CCP without head mass. 421
422
423
Figure 3: CECT abdomen showing diffuse calcification in head and body. 424
425

Manuscript Accepted Early View Article
Page 18 of 19
426
Figure 4: MRCP showing Biliary stricture (Wadsworth Syndrome). 427
428

Manuscript Accepted Early View Article
Page 19 of 19
429
Figure 5: Intraoperative pictures: (a) Removal of stones. (b) Head coring & opening of 430
duct. (c) Anastomosing the jejunum with pancreas. (d) Completed LR-LPJ. (e) 431
Removed stones and cored tissue being weighed. 432