5. 158 Bangladesh J Cardiol, 2009; 1(2): 158-60Rahman M,
Chakraborty B, Ali E et al. Abstract The authors report a case of
acute pulmonary embolism (PE) in a young man who was treated with
thrombolytic agent. The diagnosis was suggested by echo-Doppler
study which showed dilated right ventricle (RV) and right atrium
(RA) and calculated pulmonary artery (PA) pressure 90 mm of Hg. The
diagnosis of PE was confirmed by pulmonary angiogram and he was
treated with streptokinase for 24 hours with excellent clinical out
come. He continues to remain in stable state at last follow up 5
weeks after discharge. Introduction PE, most commonly originating
from deep venous thrombosis of the legs, ranges from asymptomatic,
incidentally discovered emboli to massive embolism causing
immediate death.1 Although thrombolytic agents have been studied as
a treatment of acute PE, to date there have been only 11 randomized
controlled trials comparing thrombolytic therapy to conventional
anticoagulation.2 Many studies confirm that thrombolytic therapy
leads to rapid improvement in haemodynamic aberrations associated
with PE, and this approach to massive PE with cardiogenic shock is
guide-based practice.2-4 It is widely accepted that acute PE
without associated RV dysfunction or haemodynamic instability can
be readily managed with standard anticoagulation.1,2,5,6,7 Here we
report case of a massive PE who responded well to thrombolyic
therapy. Case Report A young man of 38 years of age was admitted in
a hospital with complaints of progressive shortness of breath and
cough for 10 days. His previous medical history was unremarkable.
He did not give any history of hypertension, diabetes mellitus or
bronchial asthma and he was non smoker. On admission his systemic
clinical examination revealed tachycardia and tachypnoea along with
raised jugular venous pressure (JVP). Auscultation of heart and
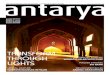
lung did not reveal any abnormality. 12 lead electrocardiogram
(ECG) showed partial right bundle branch block with wide spread T
wave inversion in chest leads (Fig-1). Bed side echo-Doppler study
revealed dilated right ventricle (RV) and right atrium (RA) with
severe tricuspid regurgitation (TR) with calculated pulmonary
artery (PA) pressure 90 mm of Hg (Fig 2,3). Thrombolytic Therapy
for Acute Pulmonary Embolism -A Case Report M Rahman, B
Chakraborty, E Ali, M Rahman, A MonsurM Rahman, B Chakraborty, E
Ali, M Rahman, A Monsur Labaid Cardiac Hospital, Dhaka, Bangladesh
Dr Matiur Rahman, FRCP, Head of the Department of Cardiology Dr
Baren Chakraborty, FRCP, Chief, Continuing Medical Education and
Research Dr Md. Elias Ali, MD, Consultant Dr. Mahbubor Rahman,
FACC, Senior Consultant Dr. A H M Abul Monsur, D. Card, Consultant
Cardiologist Correspondence : Dr. Matiur Rahman, Head of the
department of Cardiology, Labaid Cardiac Hospital, House 1, Road 4,
Dhanmondi, Dhaka 1205, Bangladesh Tel: +880-2-8610793, 9670210-3,
E-mail : [email protected] FIGURE- 1 12 lead electrocardiogram
(ECG) showed partial right bundle branch block with wide spread T
wave inversion in chest leads. FIGURE- 2 Bed side echo-Doppler
study revealed dilated right ventricle (RV) and right atrium
(RA).