Embed Size (px)
Citation preview

Volume 26 • 2011S U P P L E M E N T
The International Journal of
ORAL & MAXILLOFACIAL IMPLANTS
JOMI
The Academy of Osseointegration Silver Anniversary SummitImpact of Biological & Technological Advances on Implant DentistryThe Academy of Osseointegration Silver Anniversary Summit
20102010SUMMITS I L V E R A N N I V E R S A R Y
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The Academy of Osseointegration Silver Anniversary SummitImpact of Biological & Technological Advances on Implant DentistryAugust 5–8, 2010 • Oak Brook, IL
Planning Committee
Co-Chairs Peter K. Moy, DMDVincent J. Iacono, DMD
Committee membersTara L. Aghaloo, DDS, MD, PhD
Neel Bhatavadekar, BDS, MS, MPH
David L. Cochran, DDS, PhD
Steven E. Eckert, DDS, MS
Brian L. Mealey, DDS, MS
Thomas W. Oates, DMD, PhD
Clark M. Stanford, DDS, PhD
Ulf M. E. Wikesjo, DDS, DMD, PhD
ConsultantFrancine Berkey, PhD
Staff liaisonKevin P. Smith, MA, MBA
2010SUMMITS I L V E R A N N I V E R S A R Y
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal ofORAL & MAXILLOFACIAL IMPLANTSTable of Contents
Volume 26 • SuPPLeMeNT • 2011ISSN 0882-2786 (print) • ISSN 1942-4434 (online)
7 IntroductIon
BIoengIneerIng
11 Bioengineering in the oral cavity: Insights from Articular cartilage tissue engineering
Grayson DuRaine, PhD/Jerry Hu, PhD/Kyriacos Athanasiou, PhD, Pe
20 group Members 21 group report
nAnotechnology
25 nanotechnology Approaches to Improve dental Implants Antoni P. Tomsia, PhD/Maximilien e. Launey, PhD/Janice S. Lee, DDS, MD/
Mahesh H. Mankani, MD/ulrike G. K. Wegst, PhD/eduardo Saiz, PhD
45 group Members 46 group report
SteM cell therApy
50 role of Adult Stem/progenitor cells in osseointegration and Implant loosening
Rocky S. Tuan, PhD
63 group Members 64 group report
growth And dIfferentIAtIon
70 the use of Soluble Signals to harness the power of the Bone Microenvironment for Implant therapeutics
erica L. Scheller, BS/Paul H. Krebsbach, DDS, PhD
80 group Members 81 group report
outcoMeS
85 capturing patient Benefits of treatment Alan Carr, DMD, MS/John Wolfaardt, BDS, MDent, PhD/Neal Garrett, PhD
93 health technology Assessment in oral health Shahrokh esfandiari, BSc, DMD, MSc, PhD/Jocelyne Feine, DDS, MS, HDR
101 group Members102 group report
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

103 AudIence reSponSe reSultS
cAll to ActIon
107 oral and Maxillofacial Surgery Michael S. Block, DMD
109 periodontics Myron Nevins, DDS
110 prosthodontics Thomas D. Taylor, DDS, MSD
113 SuMMIt AttendeeS
While the information in this issue of JOMI is believed to be true and accurate, neither the Editors nor Publisher accept legal responsibility for any errors or omissions that may have been made. JOMI also makes no warranty, expressed or implied, that the material contained in this publication was peer reviewed. JOMI, its Editors, and the Publisher accept no liability for the reader’s use or misuse of the information contained herein, nor for any resultant property damage, other economic loss, or bodily injury arising out of the reader’s reliance on any claim, product, or procedure contained herein. This disclaimer also includes the content of websites of other organizations, companies, or individuals to which the published material may be linked.
For advertising and subscription information contact:Quintessence Publishing Co, Inc, 4350 Chandler Drive, Hanover Park, Illinois 60133 • Telephone: (630) 736-3600Toll Free: (800) 621-0387 • Fax: (630) 736-3633Email: [email protected] • Web site: www.quintpub.com.
Copyright © 2011 by Quintessence Publishing Co, Inc. All rights reserved. No part of this journal may be reproduced or transmitted in any form or by any means, electronic or mechan-ical, including photocopying, recording, or any information and retrieval system, without permission in writing from the pub-lisher. The views expressed herein are those of the individual authors and are not necessarily those of the publisher or the Academy of Osseointegration (AO). Information included herein is not professional advice and is not intended to replace the judgment of a practitioner with respect to particular patients, procedures, or practices. To the extent permissible under ap-plicable laws, the publisher and AO disclaim responsibility for any injury and/or damage to persons or property as a result of any actual or alleged libelous statements, infringement of intel-lectual property or other proprietary or privacy rights, or from the use or operation of any ideas, instructions, procedures, products, or methods contained in the material therein.
Permission to photocopy items solely for internal or personal use, and for the internal or personal use of specific clients, is granted by Quintessence Publishing Co, Inc, for librar-ies and other users registered with the Copyright Clearance Center (CCC) Transaction Reporting Service, provided that the base fee of $5 per article plus $.10 per page is paid di-rectly to the CCC, 222 Rosewood Drive, Danvers, MA 01923 (www.copyright.com). Identify this publication by including with your payment the fee code: 0882-2786/11 $5 + $.10.
The International Journal of Oral & Maxillofacial Implants is indexed and/or abstracted in Index Medicus, Science Citation Index, Current Contents/Clinical Medicine, MEDLINE, Index to the Dental Literature, and CINAHL database.
The International Journal of Oral & Maxillofacial Implants (ISSN 0882-2786 [print]; ISSN 1942-4434 [online]) is pub-lished bimonthly by Quintessence Publishing Co, Inc, 4350 Chandler Drive, Hanover Park, Illinois 60133, to disseminate current information related to the management of patients uti-lizing implant modalities and to report the results of basic and clinical research by investigators whose studies embrace the implant concept. Printed in USA.
Postmaster: Send address changes to Quintessence Publishing Co, Inc, 4350 Chandler Drive, Hanover Park, Illinois 60133.
PublisherH. W. Haase
Executive Vice PresidentWilliam G. Hartman
Director, Journal PublicationsLori A. Bateman
Managing EditorAimée M. Newth
Production ManagerDiane Curran
Director, Advertising SalesWilliam G. Hartman
The Academy of Osseointegration Silver Anniversary SummitImpact of Biological & Technological Advances on Implant Dentistry
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

AcAdemy of osseointegrAtion BoArd of directors
Peter K. Moy, DMDPresidentLos Angeles, California
Kenneth F. Hinds, DDSPresident-ElectLaguna Niguel, California
David L. Cochran, DDS, PhDVice PresidentSan Antonio, Texas
Joseph E. Gian-Grasso, DMDTreasurerPhiladelphia, Pennsylvania
Stephen L. Wheeler, DDSSecretaryEncinitas, California
Vincent J. Iacono, DMDPast PresidentStony Brook, New York
directors
Jay P. Malmquist, DMDPortland, Oregon
Russell D. Nishimura, DDSWestlake Village, California
Michael R. Norton, BDS, FDS, RCS(Ed)London, United Kingdom
Alan S. Pollack, DDSNew York, New York
Steven J. Rosenstein, DMDAventura, Florida
Clark M. Stanford, DDS, PhDIowa City, Iowa
James C. Taylor, DMD, MAOttawa, Ontario, Canada
osseointegrAtion foundAtion BoArd of directors
James H. Doundoulakis, DMD, MSPresidentNew York, New York
Edward M. Amet, DDS, BS, MSDVice PresidentOverland Park, Kansas
Jonathan H. Orenstein, DMDSecretary/TreasurerMarlton, New Jersey
Richard K. Rounsavelle, DDSPast PresidentTorrance, California
directors
Luis J. Fujimoto, DMDNew York, New York
Vincent J. Iacono, DMDStony Brook, New York
Clarence C. Lindquist, DDSWashington, DC
Kevin T. McNally, DDSCulver City, California
Mollie A. Winston, DDSAtlanta, Georgia
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 7
The Academy of Osseointegration (AO) is a multi-disciplinary, international dental implant orga-
nization that exists to bring together individuals of different backgrounds in order to share experience and knowledge regarding dental implants. Academy members share the common goal of moving the field of osseointegrated implants forward through clinical and evidence-based research and education. The AO mission is to enhance oral health globally by advanc-ing the science, practice, and ethics of implant den-tistry and tissue engineering. The mission is achieved, in part, through annual meetings, publication of The International Journal of Oral & Maxillofacial Implants, and periodic workshops and conferences.
2010 marked the 25-year silver anniversary of the formation of the AO. As a way to recognize this mile-stone and to honor the AO’s dedication to research and education, the AO Board organized and convened the AO Silver Anniversary Summit: Impact of Biologi-cal and Technological Advances on Implant Dentistry. The Summit was almost 2 years in the making and involved extensive planning and resources to accom-plish. This could not have been achieved without the dedication of the AO Summit Planning Committee.
With the input of the Planning Committee, the co-chairs invited six experts and 100 participants to the Summit. In addition to the AO Board and the AO Foun-dation Board, other experts in implant dentistry were asked to participate, including scientists, academicians, and clinicians. Industry representatives, who, along with the AO Foundation funded the Summit, and pro-fessional partners, including the American Academy of Periodontology (AAP), the American Association of Oral and Maxillofacial Surgeons (AAOMS), and the American College of Prosthodontists (ACP) were also invited to participate.
The goal of the Summit was to gain an under-standing of how certain biotechnologies might im-pact the future of implant dentistry. The Summit was not a consensus conference but was instead intended to educate participants and AO members in general about the nature of these biotechnologies and to pro-vide the opportunity to envision how each of them could play a part in the future of implant dentistry.
The Summit also included a discussion of the out-comes of implant dentistry. The goal with the out-comes element of the Summit was to assess these new technologies, not just against scientific merit or their potential to improve clinical outcomes, but also to in-sure that improving patient outcomes (ie, answering the “So what?” question for patients) is included as well. The objective was to educate the participants in the Summit as well as the AO membership in general about this issue through the publication of the proceedings
of the Summit. The Summit also afforded those who are experts in the outcomes area, or interested in the topic as it relates to dental implants, to have a chance to interact about the issue and make recommenda-tions to their colleagues about moving the outcomes discussion forward in the future. Clinical and patient-centered outcomes were discussed to assist in the development of definitive success criteria for implant therapy that must be adopted by the profession.
Experts were identified and asked to present a lecture on their area of expertise as well as prepare a manuscript to be included in this publication. The quality of the content for the Summit was influenced in large part by the knowledge, expertise, and dedica-tion of these experts.
INTRODUCTION
AO Summit PlAnning COmmitteeCO-ChAirS
Peter K. Moy, DMD UCLA School of Dentistry, Los Angeles, CA
Vincent J. Iacono, DMD School of Dental Medicine, Stony Brook University, Stony Brook, NY
COmmittee memberS
Tara L. Aghaloo, DDS, MD, PhD UCLA School of Dentistry, Los Angeles, CA
Neel Bhatavadekar, BDS, MZS, MPH B-6 Yak 8 Yeti Society, Pune, India
David L. Cochran, DDS, PhD University of Texas Health Science Center, San Antonio, TX
Steven E. Eckert, DDS, MS Mayo Clinic, Rochester, MN
Brian L. Mealey, DDS, MS University of Texas Health Science Center, San Antonio, TX
Thomas W. Oates, DMD, PhD University of Texas Health Science Center, San Antonio, TX
Clark M. Stanford, DDS, PhD University of Iowa, Iowa City, IA
Ulf M. E. Wikesjo, DDS, DMD, PhD Medical College of Georgia, Martinez, GA
COnSultAnt
Francine Berkey, PhD The Avenues Company, Flagstaff, AZ
StAff liAiSOn
Kevin P. Smith, MA, MBA Academy of Osseointegration, Arlington Heights, IL
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Introduction
8 Volume 26, Supplement, 2011
The Summit began with the six presentations from the experts. After the presentations, each expert had time to answer questions and hear discussion from the participants relative to their topic. The manu-scripts included in this publication reflect the content for each of these presentations.
The participants were then assigned to one of four breakout groups focused on each of the biotechnolo-gies. These breakout groups were given the task of answering a set of common questions relative to their biotechnology area. Each group had a chair and a secretary to facilitate the discussion and document it. The breakout groups also included the expert for that biotechnology.
The questions that each biotechnology breakout group was asked to address were:
1. What is the primary rationale for the development of the technology?
2. What is the potential for the technology to im-prove clinical outcomes (eg, enhanced predictabil-ity of clinical results with hard and soft tissues) in dental implant therapy?
3. Improved kinetics (ie, faster osseointegration and/or improved wound healing)
4. Fewer complications (ie, infections, peri-implantitis, etc)
5. Better-quality clinical outcomes overall (ie, im-proved osseointegration and/or wound healing, better long-term survival/success rates, etc)
6. What kinds of patients are most likely to need, want, or be candidates for the treatment/technology? Please be as specific as possible about potential patient selection criteria for the technology.
7. What is the potential for the technology to improve a patient's physical health (oral and systemic) and quality of life (ie, psychosocial, functional)?
8. Is the current evidence sufficient to warrant fur-ther research and resources being directed toward the technology relative to dental implant therapy? If so, why?
The breakout group sessions were followed by the first plenary session in which each chair presented to all participants their respective group’s answers to the common questions. In this plenary session, the break-out group representatives also had an opportunity to provide any additional clarification or input they thought was important. Each presentation was also followed by questions and answers as well as discus-sion. The group reports reflecting the answers each group had for the questions is included in this publi-cation. The names of the members of each group are also provided.
COntent AreA/exPertS
bioengineeringKyriacos Athanasiou, BS, MS, PhM, PhD Department of Biomedical Engineering University of California Davis, Davis, CA
nanotechnologyAntoni Tomsia, PhD Materials Sciences Division Lawrence Berkeley National Lab, Berkeley, CA
Stem Cell therapyRocky S. Tuan, PhD Center for Cellular and Molecular Engineering Department of Orthopaedic Surgery, School of Medicine University of Pittsburgh, Pittsburgh, PA
growth and Differentiation/ Signaling molecules
Paul Krebsbach, DDS, PhD Department of Biologic and Materials Sciences University of Michigan, Ann Arbor, MI
OutcomesJocelyn Feine, DDS, MS, HDR Oral Health and Society Research Unit McGill University, Montreal, QC’
Neal Garrett, PhD Weintraub Center for Reconstructive Biotechnology UCLA School of Dentistry, Los Angeles, CA
breAkOut grOuPS
bioengineeringChair: David L. Cochran, DDS, PhDSecretary: German O. Gallucci, DMS
nanotechnologyChair: Brian L. Mealey DDS, MSSecretary: Wayne A. Aldredge, DMD
Stem Cell therapyChair: Tara L. Aghaloo, DDS, MD, PhDSecretary: John P. Schmitz, DDS, MS, PhD
growth and DifferentiationChair: Clark M. Stanford, DDS, PhDSecretary: Joseph P. Fiorellini, DMD, DMSc
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Introduction
The International Journal of Oral & Maxillofacial Implants 9
The format for the next set of breakout sessions was altered at this point in the Summit to allow for in-clusion of the outcomes discussion. Representatives were taken from the biotechnology breakout groups to comprise a separate breakout group focused on discussing outcomes and, more specifically, how out-come domains for implant dentistry might be iden-tified and measured in future research. The report that reflects the results of the outcomes discussion is included in this publication, as are the names of the members of the group.
The agenda addressed by the outcomes breakout group included:
1. Overview of the outcomes discussion from each of the technology groups by a targeted outcomes representative for each group
2. Identification of common critical outcome needs and any unique to specific technologies
3. Discussion of the following topics:• The need for/value of a core set of outcomes for
clinical studies in dental implant therapy• Desired domains for the outcome measures to
represent (following the HTA model)• Ways to create consensus for a broad range of
outcome measures along with a recommenda-tion for a preferred method
At this point, the biotechnology breakout groups reconvened, minus the outcomes participants, to ad-dress another set of common questions. Those ques-tions were:
1. What additional evidence should be gathered to enhance development and enable transfer of the new technology?a. Technical propertiesb. Safetyc. Efficacy and effectiveness (physiologic, clinical,
functional, patient perspectives, etc)d. Economic factorse. Legal/ethical issues
A final plenary session was then convened for each group to again present the results of their discussions to the entire group. In this plenary session, a wireless system called the Audience Response Technology (ART) was used to poll participants on their opinions regarding the Summit content. The ART questions for the biotechnology areas were a common set and the outcomes segment had a separate set of questions on which to poll the participants. The results of the polling are included in this publication.
The ART statements used to poll participants on each of the biotechnologies were:
1. There is a significant dental implant patient pop-ulation that could benefit from this technology. [Strongly Disagree to Strongly Agree]
2. This technology has the potential to significantly improve clinical outcomes with dental implants. [Strongly Disagree to Strongly Agree]
3. This technology has the potential to significantly improve physical health outcomes for dental im-plant patients. [Strongly Disagree to Strongly Agree]
4. This technology has the potential to significantly improve quality of life outcomes (eg, function) for dental implant patients. [Strongly Disagree to Strongly Agree]
5. The potential benefit of this technology will justify its estimated cost. [Strongly Disagree to Strongly Agree]
6. This technology has the potential to have a sig-nificant impact on dental implant therapy in: [Less than 5 to more than 20 years]
ART questions for outcomes were:
1. When assessing a technology for implant therapy, it is important to include more than just the stan-dard clinical measures of implant survival/success (ie, implant in function, no mobility, no pain, no in-fection, and minimal bone loss). [Strongly Disagree to Strongly Agree]
2. It is essential to identify and measure technol-ogy assessment outcomes that include life quality, function (as rated by the patient), cost, and prefer-ence. [Strongly Disagree to Strongly Agree]
3. A consensus on the appropriate outcomes for implant technology assessment should be devel-oped. [Strongly Disagree to Strongly Agree]
4. An essential aim in the assessment of an implant technology includes the prediction (or modeling) of individual therapeutic benefits. [Strongly Dis-agree to Strongly Agree]
5. It is fundamental to maximize resource allocation for the selection and development of implant technology. [Strongly Disagree to Strongly Agree]
For future planning purposes, the participants were also asked which areas of implant dentistry would be the priority for the AO to focus on in future meetings. The results of that polling indicated that treatment of peri-implantitis and vertical ridge aug-mentation were the two that ranked the highest. This polling was considered in the development of the AO’s strategic plan to convene annual focused work-shops on critical topics in implant dentistry.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Introduction
10 Volume 26, Supplement, 2011
The Summit concluded with summary and call to action presentations by respected representatives of the three major implant dentistry specialties:
The Summit successfully provided the profession with a better understanding about how the clini-cal application of nanotechnology, biologics, and genomic medicine research will enhance the regen-eration of lost soft and hard tissue for the optimal placement and restoration of dental implants to en-hance function, oral health, and patient well being.
In addition, there was very high interest among the participants to create core focus groups to concen-trate on specific areas of research correlating the four fields of biotechnologies to specific areas of need in implant dentistry, as well as establishing registries to document true survival and/or success rates for den-tal implants. In developing the registries, researchers and clinicians may, in the future, alter the course of patient treatment to improve treatment outcomes for patients, thus improving their quality of life.
The Academy is proud to have held this Summit to commemorate the Silver Anniversary of the Academy of Osseointegration. It has reinforced the AO’s leader-ship position in implantology education by providing its members with the latest information on current and future applications in their practices.
Peter K. Moy, DMDVincent J. Iacono, DMDCo-Chairs
SPeCiAlty CAll tO ACtiOn SPeAkerS
Oral and maxillofacial Surgery Michael S. Block, DMD
Periodontics Myron Nevins, DDS
Prosthodontics Thomas D. Taylor, DDS, MSD
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 11
Tissue engineering is defined as an interdisciplin-ary research field devoted to the repair or replace-
ment of tissues or organs through the application of engineering methods, material science, chemistry, cells and other biologic materials, and externally ap-plied stimuli. To properly place into context the need to engineer articular cartilage, the clinical need for replacement cartilages and their desired functional properties will be reviewed first.
The CliniCal issue
The Centers for Disease Control and Prevention esti-mate that osteoarthritis affects 27 million Americans,
and this number is expected to grow as the popula-tion ages. While osteoarthritis can affect younger populations, many more older persons are stricken, with estimates of almost one-fifth of the population over 45 years of age developing this debilitating dis-ease.1 Damage to the joints and articular cartilage from blunt or accumulated trauma represents a com-mon event during aging and results in severe pain and reduction in the quality of life.
Articular cartilage is recalcitrant to repair because of its low cellularity and aneural and avascular nature. While traumatic disruption of the joint is understood to result in cartilage degeneration, the initial etiology of osteoarthritis in many cases remains unknown. However, degradation of the matrix by multiple meth-ods, including wear and tear, overloading, and inflam-matory/catabolic destruction, results in loss of joint function. During the progression of osteoarthritis, cartilage typically decreases in collagen and proteo-glycan content and increases in water content,2 with subsequent changes in biomechanical characteristics. Fibrillation and fissures may develop and extend to the subchondral bone.3 Regardless of cause, defects within articular cartilage can be divided into two groups based on depth: partial defects and full-thick-ness defects. Although of less apparent severity, par-tial-thickness defects penetrate only to the articular cartilage matrix, resulting in a defect that is isolated from the underlying blood supply and bone marrow
1 Postdoctoral Fellow, Department of Biomedical Engineering, University of California, Davis, California.
2 Principal Development Engineer, Department of Biomedical Engineering, University of California, Davis, California.
3 Distinguished Professor and Chair, Department of Biomedi-cal Engineering, University of California, Davis, California.
None of the authors reported a conflict of interest.
Correspondence to: Dr Kyriacos A. Athanasiou, Department of Biomedical Engineering, University of California, Davis, One Shields Avenue, Davis, CA 95616. Fax: +530-754-5739. Email: [email protected]
Bioengineering in the Oral Cavity: Insights from Articular Cartilage Tissue Engineering
Grayson DuRaine, PhD1/Jerry Hu, PhD2/Kyriacos Athanasiou, PhD, PE3
Cartilage failure in diarthrodial joints results in pain and a reduction in quality of life. The goal of cartilage tissue engineering is to replace or regenerate these mechanically loaded tissues to restore function to the joint. Recent advances in the authors’ laboratory have resulted in the production of cartilage and fibrocartilage with clinically relevant properties. A review of salient results will constitute the bulk of this manuscript. After providing a brief background of the clinical problem, this review will highlight several specific tissue engineering tools. The approaches used to produce mechanically functional cartilage through tissue engineering have several parallels to the problems faced in osseointegration, eg, the need for mechanically appropriate tissues at the implantation site. The discussion that follows will focus on how approaches developed in identifying alternative cell sources and various exogenous stimuli for producing new cartilage may be applicable to osseointegration. Int J Oral Maxillofac Implants 2011;26(suppl):11–19
Key words: articular cartilage, regenerative medicine, self-assembly, stem cells, tissue engineering
Bioengineering
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering
12 Volume 26, Supplement, 2011
progenitor cells within the subchondral bone. There-fore, repair activities of the defect only originate from the adjacent, metabolically quiescent chondrocytes, which are incapable of more than a few days of in-creased matrix synthesis, resulting in a lasting defect that can affect the surrounding tissue mechanics and initiate further tissue degradation.4 Full-thickness de-fects (also known as osteochondral defects) penetrate into the subchondral bone, allowing for access to blood and mesenchymal progenitor cells to initiate a more robust healing response.5 However, the repaired tissue that fills this defect does not last because of its more fibrous and mechanically inferior nature. Current treatment options that successfully replace cartilage are inconsistent,6 and many treatment options deal with management of pain symptoms.7 The gold stan-dard of care remains the total joint replacement, which, while successful, has a usable life of approximately 10 to 15 years before revision is needed. This is inad-equate, especially for young patients. The widespread occurrence and harmful nature of cartilage degenera-tion have established a strong need for the develop-ment of replacement tissue-engineered cartilage.
naTive CarTilage ProPerTies
Replication of the structure and function of the native cartilage is desired; to this end, an understanding of the properties of the native tissue is needed. Articu-lar cartilage exists as a thin, smooth tissue covering the ends of the bones, with liquid and solid fractions. The interactions of these two phases are described by the biphasic model, which describes the viscoelastic nature of the tissue.8 The biochemical composition of the tissue allows for its unique mechanical properties. In adult humans, 70% to 80% of the matrix wet weight is water, while the remaining solid fraction is primarily type II collagen (50% to 75%) and proteoglycans (15% to 30%).9
The cells in cartilage, chondrocytes, occupy less than 5% of the tissue volume in humans but are es-sential for maintaining the extracellular matrix (ECM). Isolated within the dense ECM, the chondrocyte re-ceives nutrients primarily through diffusion from the synovial fluid, assisted by joint movement. The articu-lar chondrocyte phenotype varies by zonal depth, but all differentiate from mesenchymal progenitor cells and, in healthy adult tissues, have little to no prolif-eration. Immediately surrounding the chondrocytes is the pericellular matrix, which differs in composi-tion from the bulk ECM. Within the pericellular matrix, higher levels of decorin and aggrecan and a network of type VI collagen are found.10 The chondrocytes are anchored to this matrix through the CD44 receptor to hyaluronan-proteoglycan aggregates and by inte-grins. These integrins can serve as receptors for ECM proteins, such as types II and IV collagen, laminin, fi-bronectin, and vitronectin.11
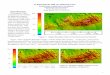
Three identifiable zones exist within articular carti-lage, based on ECM content and cell phenotype, and are termed superficial, middle, and deep (Fig 1). The su-perficial zone of articular cartilage contains flattened discoid cells that secrete superficial zone protein and collagen fibers oriented parallel to the surface in the direction of shear that provide tensile strength and control fluid permeability.12 The middle zone consists of spherical cells arranged in perpendicular columns, the highest aggrecan (proteoglycan) content,13,14 and cartilage intermediate layer protein.15 The deep zone includes the calcified area of cartilage; the tidemark distinguishes between the noncalcified and calcified areas. This characteristic zonal architecture, which is intimately linked to the biology, mechanical function, and changing composition, results in zone-specific mechanical properties of articular cartilage. The or-ganization of the cartilage varies by depth as a result of differences in the forces experienced throughout the tissue. Tensile forces within cartilage result primar-ily from load redistribution to the surrounding tissue
Super�cial zone 10%–20%
Middle zone 40%–60%
Deep zone 20%–50%
Subchondral bone
Collagen �brils
Chondrocytes
Hyaluronan
Aggrecan macromolecule
Chondroitin sulfate
Link proteinKeratan sulfate
Fig 1 Zones and macromolecules in ar-ticular cartilage.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Duraine et al
The International Journal of Oral & Maxillofacial Implants 13
during compressive loading and from the sliding motion of articulating surfaces upon each other. The mechanical properties of articular cartilage are depen-dent on the molecules composing the ECM and their organization; these properties are determined primar-ily by the interactions of collagen and aggrecan.
Collagen anD Tensile ProPerTies
Although type II collagen makes up the bulk of the collagens within cartilage, types VI, IX, X, and XI are also present. Collagens IX and XI can cross-link with collagen II to produce larger fibrils, which can form an interconnected mesh network surrounding the aggrecan.16 The collagen network encapsulating the aggrecan provides tensile strength to resist the expansion of the proteoglycans.17 On a microscopic scale, the water and collagen content in the tissue decreases with depth from the articulating surface, while the collagen fibril size increases. Collagen fibers are oriented tangential to the surface to resist shear and tension, while the organization of collagen fibrils in the middle of the tissue is more random. Fibers near the tidemark are arranged perpendicular to the surface, interfacing with the underlying bone.
ProTeoglyCans anD ComPressive ProPerTies
The bulk of the proteoglycans within cartilage are found in aggregates composed of aggrecan linked to hyaluronic acid via link protein. Aggrecan exists as a large highly glycosylated proteoglycan with long lin-ear glycosaminoglycan (GAG) chains of chondroitin sulfate and keratan sulfate molecules radiating from a central protein core, resulting in a bottle brush struc-ture. The carboxyl (COO−) and sulfate (SO3
−) groups present on these GAGs produce a strong negative charge, allowing it to absorb water and swell, creating an osmotic pressure that resists compressive mechani-cal forces.12 Smaller proteoglycans (eg, biglycan, fibro-modulin, and decorin) occur in lower concentrations and contribute to the organization of the matrix and ligand sequestering.18,19 Compressive loading is one of the main forces encountered by cartilage. The move-ment of the interstitial fluid trapped by the aggrecan through the matrix dissipates the compressive load as a result of frictional drag, which is dependent on the hydraulic permeability of the tissue. Because the permeability of healthy cartilage is low, this results in high interstitial fluid pressures during load. Over time, the interstitial fluid pressure decreases as a function of permeability, resulting in the load being transferred to
the solid portion of the extracellular matrix, contribut-ing to the viscoelastic nature of cartilage. As this fluid is exuded from the joint during loading, it also serves as a hydrodynamic lubricant to reduce friction.20
TeChniques For arTiCular CarTilage Tissue engineering
Approaches to engineering articular cartilage can be broadly divided into in vivo and in vitro methods. The former stems from the belief that the in vivo en-vironment contains all the necessary stimuli to direct tissue formation if a suitable cell source or scaffold is provided. A variety of polymer or biologic scaffold materials for the filling of articular cartilage defects has been studied, often in combination with various growth factors and cell sources.21 Clinically, this has resulted in the autologous chondrocyte implantation technique, wherein chondrocytes are isolated from non–load-bearing regions, expanded in vitro, and re-implanted under a periosteal flap22 or in a bilayer col-lagen scaffold.23 Although this results in defect filling and short-term pain relief,24 the implanted material may not regain the mechanical properties of native tissue. This review focuses on in vitro tissue engi-neering, which seeks to complete the bulk of matrix production and organization before implantation to deliver a new tissue of sufficient properties to func-tion, integrate, and remodel (Fig 2). The in vitro en-vironment is defined by the bioengineer. This allows for the controlled examination and fine-tuning of rel-evant tissue engineering parameters to stimulate the formation of functional tissue; the classic paradigm of tissue engineering has involved the triad of cells, sig-nals, and scaffolds. Because scaffolds can have many disadvantages, including stress shielding, cell-cell contact inhibition, and biodegradability issues, a scaf-foldless approach utilizing a self-assembling process has been developed.25 The self-assembling process is based on the differential adhesion hypothesis,26,27 and many encouraging results have been obtained using this method with different combinations of cells and signals, as will be described in the following.
scaffoldless self-assembling ProcessThe self-assembling process employs high-density seeding of native chondrocytes in agarose molds, which allows for control of construct size and shape. Cartilage constructs with clinically relevant dimensions (~15-mm diameter and 1-mm thick) and properties ap-proaching those of native cartilage have been created using this scaffoldless approach.25 The self-assembly of chondrocytes has been shown to closely resemble normal development and maturation (Fig 3). Abundant
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering
14 Volume 26, Supplement, 2011
cadherin activity, when the cells are first seeded, levels off after the cells have coalesced to initiate matrix pro-duction, which consists of GAGs and collagen VI. At 4 weeks, tensile properties reach a maximum and com-pressive properties level off, while biochemically the tissue matures with collagen VI localized pericellularly, increased amounts of collagen II in the interterritorial space, and an increased chondroitin 4-sulfate/chon-droitin 6-sulfate ratio.26
Cell sources Autologous chondrocytes are source limited, and the harvest of healthy cartilage tissue results in site morbid-ity and mortality, as is common with most autologous sourced cells. Chondrocytes have low natural prolifera-tion, and expansion techniques result in phenotypic changes.28 Therefore, for the numbers of chondrocytes needed for tissue engineering, the use of autologous chondrocytes is impractical clinically.29 This has led to the investigation of other cell sources, such as hu-man embryonic stem cells (hESC) and dermis-isolated aggrecan-sensitive cells (DIAS). To employ these cells in
tissue engineering, methods need to be determined to (1) isolate, (2) differentiate, and (3) purify them. These steps are being investigated in parallel using a modular approach to accelerate the pace of discovery. For exam-ple, as protocols for stem cell differentiation are refined to reach higher efficiencies, purification protocols are also under development to enrich the percentage of relevant cells for self-assembly.
Embryonic stem cells (ESCs) are pluripotent, as de-fined by their ability to indefinitely proliferate and differentiate into any of the three germ layers. Employ-ing the modular approach, the authors have induced chondrogenic differentiation of both BG01V and H9 hESC lines, followed by tissue engineering of these cells. This was performed by differentiating hESCs in chondrogenic media in embryoid bodies for up to 6 weeks, followed by enzymatic disassociation. These differentiated disassociated cells were self-assembled and cultured an additional 4 weeks. With both hESC lines, fibrocartilage constructs were produced.30 To improve chondrogenic differentiation, combinations of transforming growth factor β3 (TGF-β3) and bone
Fig 2 The paradigm of in vitro tissue engineering. hESC = human embryonic stem cells; DIAS = dermis-isolated aggrecan-sensitive cells.
NeotissueConstruct
NeotissueConstruct
Stem cellsheSC, DIAS Differentiation Differentiated cells
Cell harvest and expansion Native cells
Construct formationScaffold or scaffoldless cell sedding techniques
Scaffolds Scaffoldless
Construct validationBiochemistry
HistolotyBiomechanicsImplantology
Neotissueconstruct
Exogenous stimuliGrowth factors
Catabolic enzymesMechanical forces
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Duraine et al
The International Journal of Oral & Maxillofacial Implants 15
morphogenetic protein-4 (BMP-4) were used in embry-oid bodies. This growth factor combination increased cell surface marker CD44 and also increased GAG and total collagen by 6.7-fold and 4.8-fold, respectively. An alternative method of culturing embryoid bodies in the vicinity of fibrochondrocytes increased type II collagen production 9.8-fold.31 With these various techniques, hESC lines can be differentiated toward the chondrocyte phenotype.
Because of its relative abundance and ease of ac-cess, dermis is considered one of the best autologous source organs to isolate stem/progenitor cells for fu-ture therapeutic applications. A dermis-derived sub-population, the DIAS cells, can be chondro-induced using aggrecan. Protocols have been developed to isolate, purify, expand, and chondro-induce DIAS cells in vitro. Specifically, exposing DIAS cells to aggrecan for 24 hours produced dense cell aggregates that contained higher levels of type II collagen than fibro-blast controls for up to 14 days. Using self-assembly, these chondro-induced DIAS cells have shown prom-ise in producing three-dimensional constructs with cartilaginous properties.32
signals to generate Functional Properties in vitroIn vivo, cartilage is exposed to a milieu of mechani-cal and biochemical signals. The duration, magnitude, and combination of these stimuli are not well defined, but nonetheless they regulate the ECM components
that chondrocytes secrete. To better delineate how these stimuli contribute to improving the mechanical properties of neotissues, several stimuli have been examined in vitro, including growth factors, hydro-static pressure, and catabolic enzymes.
Using self-assembly, growth factors such as TGF-β, BMPs, and insulinlike growth factors (IGFs) have been shown to improve neotissue mechanical properties. Combined treatment with BMP-2 and IGF-I resulted in increases in GAG production and a greater than 1-fold increase in aggregate modulus. In contrast, TGF-β1 treatment increased both GAG and collagen content and yielded 1-fold increases in both aggre-gate and tensile modulus.33 For cartilage tissue engi-neering, TGF-β1 demonstrated the most potency, as it increased collagen content and tensile modulus and outperformed a combination of growth factors.
Mechanical stimulation, such as hydrostatic pres-sure or direct compression, has repeatedly been shown to have positive effects on the mechanical properties of native and newly formed tissue. In gen-eral, these stimuli have been chosen to have magni-tudes at or below the physiologic range. For instance, the application of 10 MPa of static hydrostatic pres-sure, applied for 1 hour a day for 5 days, significantly increased the collagen content by more than 2-fold, the aggregate modulus by 1.4-fold, and the tensile modulus by 1.9-fold.34 These increases in construct properties are similar to those obtained by using growth factors.
Fig 3 Phases in the self-assembly of dif-ferentiated articular chondrocytes mimics those of development. ECM = extracellular matrix; Col = collagen; PCM = pericellular matrix. (From Ofek et al26; used under the Creative Commons Attribution License.)
Varying intercellular adhesion results in a zonal architecture (by adjusting
expression levels of N-cadherin; less adhesive population envelops population
with higher intercellular adhesion)
Intense Col VI staining after
24 h of self-assembly
PCM localization of
Col VI at 6 wk of development
High-density cell suspension
seeded in agarose molds
Differential adhesion hypothesis suggests cadherin-mediated
cell interactions
Chondrocytes migrate apart
and secrete ECM, mainly ColVI
Matrix divisions become apparent, with a distinct PCM
Phase 1:Seeding
Phase 2:Cell
recognition
Phase 3:Construct formation
Phase 4:Matrix
maturation
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering
16 Volume 26, Supplement, 2011
Combinations of these two different classes of stim-uli—TGF-β1 and hydrostatic pressure—resulted in ad-ditive effects on mechanical properties, increasing the aggregate modulus by more than 1.6-fold and the ten-sile modulus by more than 2.3-fold. Furthermore, the combination treatment had a greater than additive effect; a synergistic increase in collagen content was observed.35 This combination of biochemical and me-chanical stimuli resulted in constructs with mechanical properties that resembled those of native tissue.
Classically, most tissue engineering studies (cartilage and other tissues) have been driven by the addition of anabolic factors to increase the production of extra-cellular matrix and tissue strength. Counterintuitively, catabolic factors, such as enzymes that digest the car-tilage matrix, may improve mechanical properties by assisting in matrix turnover. For example, application of chondroitinase ABC (C-ABC), which digests GAGs, has resulted in increased tensile mechanical properties in self-assembled cartilage constructs. Although a single 4-hour C-ABC treatment depleted GAGs and reduced the construct’s compressive properties, both of these recovered after 2 weeks. Furthermore, the treatment had resulted in an 80% increase in tensile modulus.36 Likely, the application of C-ABC mirrors that of native tissue matrix remodeling and suggests further uses of catabolic factors in tissue engineering.
assaying Tissue mechanical PropertiesTo determine whether engineered tissues can repli-cate native tissue function, assays capable of deter-mining mechanical properties are required. Because the compressive and tensile properties of articular car-tilage are necessary for its function, the authors have defined testing parameters that measure both com-pressive aggregate modulus and tensile modulus. To measure values for compressive properties, a form of creep indentation testing is used. A platen of known dimension and size is used to indent the sample un-der constant stress, and deformation is measured over time. A porous platen is used to allow fluid to exude from the sample at the platen contact site. Data are collected until the sample reaches deformational equi-librium. Following testing, a numeric algorithm fits the data to the biphasic theory to compute three indepen-dent variables that describe the construct’s material properties, the aggregate modulus, permeability, and Poisson ratio.37 To measure tensile modulus, a set of grips is fixed upon the tissue, and a constant strain rate of 1% is used to pull the sample apart until failure. The tensile modulus can then be calculated from the linear region of the stress-strain curve. These assays allow for identification of native tissue properties that need to be replicated, and they can also be used as quality con-trol for the tissue-engineered materials.
summaryWhile the self-assembly process was initially developed based on the use of articular chondrocytes, the encour-aging results have led it to be applied to a spectrum of cartilage tissues.38 By varying the cell source, the biochemical stimuli applied, and the mold geometry, the engineering of a range of fibrocartilage tissues has been accomplished (eg, meniscus, temporomandibular joint). For example, circumferential collagen fibril align-ment could be observed in meniscus constructs grown in ring-shaped molds, resulting in a threefold increase in circumferential tensile properties compared to radial tensile properties.39 While this technique shows prom-ise, current studies focus on continuing to improve the mechanical properties of the neotissues produced by optimization of biochemical and mechanical stimuli. Because of its versatility and capacity to increase func-tional (biochemical and biomechanical) characteristics, the self-assembly process has recently been combined with DIAS cells and chondro-differentiated hESCs to produce constructs with cartilage-specific ECM. This fur-ther demonstrates the ability to use this technique over multiple cell sources. Because no one signal controls the development and maintenance of articular cartilage, op-timization of stimuli combinations and a greater under-standing of the mechanisms of gene regulation at work remain areas of current research. The objective of the authors’ research remains the engineering of cartilage with clinically relevant biochemical and biomechanical properties that resemble those of native tissue.
insighTs relaTeD To DenTal imPlanT osseoinTegraTion
As previously discussed, articular cartilage tissue en-gineering can be approached using in vivo or in vitro methods employing a combination of cells, signals, and scaffolds. Insights gained from these approaches can similarly be applied to osseointegration. For instance, failure to osseointegrate can be attributed to lack of nec-essary tissue at the implantation site; placing implants in patients with inadequate bone support (either of sufficient quality or quantity) remains a major obstacle. Increasing the available bone for implantation using autologous sourced grafts requires multiple surgeries, which is undesirable. Autografts are also scarce, and their harvest can lead to donor site morbidity and pain. Engi-neered tissues may meet this need for autologous tissue. In articular cartilage tissue engineering, the quality and quantity of the neotissue have been increased through the use of growth factors, mechanical stimuli, and cata-bolic enzymes. Examples of how these stimuli may be or are used in in vivo and in vitro tissue engineering, as re-lated to osseointegration, are discussed in the following.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Duraine et al
The International Journal of Oral & Maxillofacial Implants 17
The in vivo approach to improving Bone quality and quantitySimilar to in vivo cartilage tissue engineering to fill defects, scaffolds, cells, and signals can be considered for osseointegration. With regard to scaffolds, various formulations of demineralized freeze-dried bone al-lograft putty or matrix have been used to fill intraos-seous defects40 to improve bone quality. As described earlier, one of the clinical strategies for in vivo articu-lar cartilage engineering has been the implantation of autologous cells in concert with scaffolds for defect filling. In applying this strategy to osseointegration, one may want to consider the previously described issues surrounding this approach (eg, cost, cell sourc-ing, multiple surgeries, and no immediate load bear-ing). Finally, the signals currently employed in vivo for bone formation have consisted of growth factors. For example, platelet-derived growth factor in com-bination with an osteoconductive material (GEM 21S, Osteohealth) has shown clinical efficacy in dental practice.41 Also, BMP-2 in conjunction with a colla-gen sponge (INFUSE, Medtronic), as well as BMP-7 in conjunction with a type I bone collagen carrier (OP-1, Stryker), are related products that are clinically avail-able for bone formation.
However, the use of anabolic growth factors alone may not be the complete answer. As described earlier, one of the insights gained from engineering articu-lar cartilage has been the use of catabolic enzymes to improve the quality (mechanical properties) of the tissue produced42 and to enhance cartilage-to-car-tilage integration.43 The in vivo use of appropriately selected catabolic agents in concert with growth fac-tors may similarly allow for increased functionality and/or implant integration.
The in vitro approach to improving Bone quality and quantityWhile growth factor–enhanced biomaterials are effec-tive, the use of these products requires time for both healing and growth of the new bone in vivo before an implant can be placed, which can be several months. To augment an implantation site, in vitro growth of a neotissue using a combination of scaffoldless self-as-sembly, various cell sources, and signals may result in a construct that provides a starting point for further bone incorporation, thereby reducing healing time. The in vitro approach offers other advantages in this regard. As previously described, the self-assembly process produces engineered tissues of controllable sizes and shapes. For cells, the in vitro setting also al-lows for the careful control of appropriate signals to differentiate or purify multiple cell sources. Although the cell sources identified in cartilage tissue engineer-ing have been differentiated toward a chondrogenic
potential, related technologies can be developed for identifying cells applicable to bony defect filling or for regenerating the periodontal ligament and gin-giva. With regard to signals, stimuli that are impracti-cal in the in vivo setting can be used and applied in a well-controlled manner, for example, certain types of mechanical loading (eg, hydrostatic pressure). Ad-ditionally, stimuli (growth factors) can be applied repeatedly without the need for complex sustained-release materials. This allows for the use of dosing regimens involving combinations of growth factors and/or mechanical loading. Finally, an in vitro tissue engineering approach prevents the patient from di-rect exposure to these growth factors, and the bulk of tissue growth can occur in an aseptic environment.
In addition to supplying implantable engineered tissues, one can also envision the enhancement of osseointegration in vitro. For instance, an implant may be integrated with engineered bone and asso-ciated mucosal tissue in vitro, prior to implantation. This would potentially have several benefits, includ-ing optimization of implant-tissue integration, higher mechanical stability, and the ability to treat areas of highly resorbed bone. The quality of osseointegra-tion and tissue formation could then be verified using noninvasive optical monitoring,44 an approach that the present authors are currently applying to tissue-engineered cartilage. Furthermore, bone-to-bone in-tegration is a more favorable condition than implant osseointegration that results in increased resistance to load bearing during the early critical period of im-plantation when the implant can be overloaded.
The role oF Tissue engineering BeyonD osseoinTegraTion
Currently available implants have a useful life expec-tancy that is less than that of natural teeth, which can last several decades. Therefore, a long-term solution may be the regeneration of native tissues, possibly via the implantation of adult stem cells differentiated to form a tooth bud that grows to the correct size, ge-ometry, and mechanical strength. The principal issue in tooth regeneration is similar to that faced in car-tilage tissue engineering, ie, the need to reproduce a specific spatial and temporal series of events to achieve mechanically functional tissues.
Regeneration of the tooth is complicated by the need to form four distinct tissues with functional in-terfaces (pulp, dentin, cementum, and enamel), in-cluding a root supported by the periodontal ligament and anchored into the alveolar bone. Current work on autologous cell sources (eg, stem cells from ad-jacent tissues such as the root apical papilla and the
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering
18 Volume 26, Supplement, 2011
periodontal ligament) has demonstrated promise in regenerating integrated living roots capable of sup-porting a crown in a pig model.45 However, control of tissue shape (necessary for correct function) and isola-tion of sufficient autologous cells remain elusive goals. The techniques outlined here for cartilage tissue engi-neering may help to elucidate the necessary steps to tissue engineer a functional tooth. The self-assembly technique can potentially be employed to create the complex shapes needed for dental function. The abil-ity to differentiate skin (DIAS) cells toward a chon-drogenic phenotype serves as an example of how nondental tissue sources might yield cell sources that would be useful in producing the various dental lin-eages required to engineer a tooth. While the exoge-nous stimuli identified for cartilage tissue engineering are unlikely to directly transfer to engineering other tissues, they nonetheless can serve as starting points for improving the mechanical properties of tissue.
ConClusion
Tissue engineering in implant dentistry necessarily focuses on the guided regeneration of bone. Some tissue-engineered products have already reached the market that combine biologic signals with osteocon-ductive scaffolds. The engineering of more complex dental structures can employ insights learned in re-generating cartilage. Further advancements in osseo-integration will require continued dialogue between clinicians and tissue engineers to reap the benefits of cooperative feedback between these two groups.
aCKnowleDgmenT
The authors would like to acknowledge the support of the Na-tional Institutes of Health (grant R01AR053286) for this work.
reFerenCes
1. Spector TD, Hart DJ, Doyle DV. Incidence and progression of osteoarthritis in women with unilateral knee disease in the general population: The effect of obesity. Ann Rheum Dis 1994;53:565–568.
2. Setton LA, Elliott DM, Mow VC. Altered mechanics of carti-lage with osteoarthritis: Human osteoarthritis and an experi-mental model of joint degeneration. Osteoarthritis Cartilage 1999;7:2–14.
3. Aluisio FV, Christansen CP, Urbaniak JR. Orthopaedics. Balti-more: Williams & Wilkins, 1998.
4. Hunziker EB. Articular cartilage repair: Are the intrinsic biological constraints undermining this process insuperable? Osteoarthritis Cartilage 1999;7:15–28.
5. Shapiro F, Koide S, Glimcher MJ. Cell origin and differentia-tion in the repair of full-thickness defects of articular carti-lage. J Bone Joint Surg Am 1993;75:532–553.
6. Revell CM, Athanasiou KA. Success rates and immunologic responses of autogenic, allogenic, and xenogenic treatments to repair articular cartilage defects [review]. Tissue Eng Part B Rev 2009;15:1–15.
7. Samuels J, Krasnokutsky S, Abramson SB. Osteoarthritis: A tale of three tissues. Bull NYU Hosp Jt Dis 2008;66:244–250.
8. Mow VC, Kuei SC, Lai WM, Armstrong CG. Biphasic creep and stress relaxation of articular cartilage in compression? Theory and experiments. J Biomech Eng 1980;102:73–84.
9. Poole AR, Kojima T, Yasuda T, Mwale F, Kobayashi M, Laverty S. Composition and structure of articular cartilage: A tem-plate for tissue repair. Clin Orthop Relat Res 2001:S26–S33.
10. Johnston SA. Osteoarthritis. Joint anatomy, physiology, and pathobiology. Vet Clin North Am Small Anim Pract 1997;27:699–723.
11. Knudson W, Loeser RF. CD44 and integrin matrix receptors participate in cartilage homeostasis. Cell Mol Life Sci 2002; 59:36–44.
12. Little K, Pimm LH, Trueta J. Osteoarthritis of the hip: An elec-tron microscope study. J Bone Joint Surg Br 1958;40-B:123–131.
13. Maroudas NG. On the low adhesiveness of fluid phospholipid substrata. J Theor Biol 1979;79:101–116.
14. Gu WY, Lai WM, Mow VC. Transport of fluid and ions through a porous-permeable charged-hydrated tissue, and streaming potential data on normal bovine articular cartilage. J Biomech 1993;26:709–723.
15. Lorenzo P, Bayliss MT, Heinegard D. A novel cartilage protein (CILP) present in the mid-zone of human articular cartilage increases with age. J Biol Chem 1998;273:23463–23468.
16. Responte DJ, Natoli RM, Athanasiou KA. Collagens of articu-lar cartilage: Structure, function, and importance in tissue engineering. Crit Rev Biomed Eng 2007;35:363–411.
17. Stockwell RA. Cartilage failure in osteoarthritis: Relevance of normal structure and function. A review. Clin Anat 1990;4: 161–191.
18. Hildebrand A, Romaris M, Rasmussen LM, et al. Interaction of the small interstitial proteoglycans biglycan, decorin and fi-bromodulin with transforming growth factor beta. Biochem J 1994;302(pt 2):527–534.
19. Iozzo RV. The biology of the small leucine-rich proteogly-cans. Functional network of interactive proteins. J Biol Chem 1999;274:18843–18846.
20. Ateshian GA. The role of interstitial fluid pressurization in articular cartilage lubrication. J Biomech 2009;42:1163–1176.
21. Frenkel SR, Di Cesare PE. Scaffolds for articular cartilage repair. Ann Biomed Eng 2004;32:26–34.
22. Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889–895.
23. Bartlett W, Skinner JA, Gooding CR, et al. Autologous chon-drocyte implantation versus matrix-induced autologous chondrocyte implantation for osteochondral defects of the knee: A prospective, randomised study. J Bone Joint Surg Br 2005;87:640–645.
24. Knutsen G, Drogset JO, Engebretsen L, et al. A randomized trial comparing autologous chondrocyte implantation with microfracture. Findings at five years. J Bone Joint Surg Am 2007;89:2105–2112.
25. Hu JC, Athanasiou KA. A self-assembling process in articular cartilage tissue engineering. Tissue Eng 2006;12:969–979.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Duraine et al
The International Journal of Oral & Maxillofacial Implants 19
26. Ofek G, Revell CM, Hu JC, Allison DD, Grande-Allen KJ, Atha-nasiou KA. Matrix development in self-assembly of articular cartilage. PLoS One 2008;3:e2795.
27. Steinberg MS. Mechanism of tissue reconstruction by dissoci-ated cells. II. Time-course of events. Science 1962;137:762–763.
28. Darling EM, Athanasiou KA. Rapid phenotypic changes in passaged articular chondrocyte subpopulations. J Orthop Res 2005;23:425–432.
29. Heng BC, Cao T, Lee EH. Directing stem cell differentiation into the chondrogenic lineage in vitro. Stem Cells 2004;22: 1152–1167.
30. Koay EJ, Hoben G, Athanasiou KA. Tissue engineering with chondrogenically differentiated human embryonic stem cells. Stem Cells 2007;25:2183–2190.
31. Hoben GM, Willard VP, Athanasiou KA. Fibrochondrogenesis of hESCs: Growth factor combinations and co-cultures. Stem Cells Dev 2008;18:283–292.
32. Deng Y, Hu JC, Athanasiou KA. Isolation and chondroinduction of a dermis-isolated, aggrecan-sensitive subpopulation with high chondrogenic potential. Arthritis Rheum 2007;56:168–176.
33. Elder BD, Athanasiou KA. Systematic assessment of growth factor treatment on biochemical and biomechanical proper-ties of engineered articular cartilage constructs. Osteoarthri-tis Cartilage 2009;17:114–123.
34. Elder BD, Athanasiou KA. Effects of temporal hydrostatic pressure on tissue-engineered bovine articular cartilage constructs. Tissue Eng 2009;15:1151–1158.
35. Elder BD, Athanasiou KA. Synergistic and additive effects of hydrostatic pressure and growth factors on tissue formation. PLoS ONE 2008;3:e2341.
36. Natoli RM, Revell CM, Athanasiou KA. Chondroitinase ABC treatment results in greater tensile properties of self-assem-bled tissue-engineered articular cartilage. Tissue Eng Part A 2009;15:3119–3128.
37. Mow VC, Gibbs MC, Lai WM, Zhu WB, Athanasiou KA. Biphasic indentation of articular cartilage—II. A numerical algorithm and an experimental study. J Biomech 1989;22:853–861.
38. Hoben GM, Athanasiou KA. Creating a spectrum of fibrocarti-lages through different cell sources and biochemical stimuli. Biotechnol Bioeng 2008;100:587–598.
39. Aufderheide AC, Athanasiou KA. Assessment of a bovine co-culture, scaffold-free method for growing meniscus-shaped constructs. Tissue Eng 2007;13:2195–2205.
40. Bender SA, Rogalski JB, Mills MP, Arnold RM, Cochran DL, Mellonig JT. Evaluation of demineralized bone matrix paste and putty in periodontal intraosseous defects. J Periodontol 2005;76:768–777.
41. Pellegrini G, Seol YJ, Gruber R, Giannobile WV. Pre-clinical models for oral and periodontal reconstructive therapies. J Dent Res 2009;88:1065–1076.
42. Natoli RM, Responte DJ, Lu BY, Athanasiou KA. Effects of mul-tiple chondroitinase ABC applications on tissue engineered articular cartilage. J Orthop Res 2009;27:949–956.
43. van de Breevaart Bravenboer J, In der Maur CD, Bos PK, et al. Improved cartilage integration and interfacial strength after enzymatic treatment in a cartilage transplantation model. Arthritis Res Ther 2004;6:R469–R476.
44. Sun Y, Phipps J, Elson DS, et al. Fluorescence lifetime imaging microscopy: In vivo application to diagnosis of oral carci-noma. Opt Lett 2009;34:2081–2083.
45. Sonoyama W, Liu Y, Fang D, et al. Mesenchymal stem cell-mediated functional tooth regeneration in swine. PLoS One 2006;1:e79.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

20 Volume 26, Supplement, 2011
Bioengineering Group Members
Group ChairDavid Cochran, DDS, PhD
Group ExpertKyriacos Athanasiou, BS, MS, PhM, PhD
Group SecretaryGerman Gallucci, DMD
Group ParticipantsJoel Berger, MD, DDS
Neel Bhatavadekar, BDS, MS, MPH
Daniel Cullum, DDS
Kenneth Hinds, DDS
Edwin McGlumphy, DDS, MS
Regina Mericske-Stern, DDS, PhD
Joerg Neugebauer, DDS, PhD
Michael Norton, BDS, FDS, RCS (Ed)
Steven Rosenstein, DMD
James Taylor, DMD, MA
Maurizio Tonetti, DMD, PhD
Stephen Wallace, DDS
Mollie Winston, DDS
Mark Wong, DDS
Jeremy Curtis (Silent Participant, Zimmer)
Christopher Damien, PhD (DENTSPLY)
Alice DeForest (Silent Participant, AAP)
Jim Kenealy (Biomet 3i)
Scott Root (Silent Participant, AstraTech)
Alex R. Schaer, PhD (Camlog)
Richard Sullivan, DDS (Nobel Biocare)
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 21
The bioengineering group met to discuss the article presented by the group’s expert entitled: “Bioen-
gineering in the Oral Cavity: Insights from Articular Cartilage Tissue Engineering.” The group expert be-gan the discussion by explaining that cartilage tissue engineering and tissue engineering in the oral cav-ity shared some similarities which, when examined, might be useful for future directions of research. These include the need for mechanically appropriate tissues at the implantation site, as well as the develop-ment of such tissues from multiple cell types using a series of biochemical and mechanical external stimuli.
The group expert went on to explain that, in car-tilage development, a scaffoldless self-assembly process of varying cell populations had been helpful including the use of human embryonic stem cells and dermis isolated sensitive cells, since autologous car-tilage cells are difficult to obtain. In vivo cartilage is typically exposed to a wide range of both mechani-cal and biochemical signals which can control the particular extracellular matrix components that the cartilage cells secrete. These stimuli have provided research tools that have been helpful in understand-ing cartilage tissue engineering and include growth factors, hydrostatic pressure, and catabolic enzymes. Thus, by manipulating the cell source (including the use of co-cultures which can function as feeder cells), the applied biochemical and mechanical stimuli, and the mold geometry, various fibrocartilage tissues have been successfully produced.
A general discussion took place regarding the topic assigned to this group and the fact that “bio-engineering” encompasses an extremely broad area involving the science of biology and engineering. For the purpose of this summit, the consensus of the breakout group was to limit the discussion to tissue engineering in the oral cavity.
Several very interesting ideas and concepts were considered during the general discussion of apply-ing tissue engineering in the oral cavity relative to implant dentistry today and where bioengineer-ing might lead in the future. One idea discussed was the concept of growing a periodontal ligament (consisting of cementum, periodontal ligament, and bone) on the current metallic dental implants. Buser et al1 first described this in the literature in 1990; when metallic implants were placed adjacent to broken root tips and cementum, periodontal ligament and bone were formed along the implant surface. Since then, a couple of other papers have also described such a phenomenon. A second con-cept discussed was the idea of growing bone on
the dental implant ex vivo and then placing the implant into a bony site such that osseointegration is created outside the mouth and a bone-to-bone interface is created at the time of placement in the oral cavity. Also discussed was another area where bioengineering might be particularly helpful, a situ-ation where the implant and bone can move so that dental implants could be placed in a population that today is largely excluded, ie, growing (younger) pa-tients. The last area discussed was the application of bioengineering so as to prevent the loss of ridge form after tooth removal. In all these discussions, the group realized that many of these situations would require significant costs in terms of time, money, and resources and that the outcome of such an effort may or may not be an advantage. In general, the group felt that two overall approaches to bioengineering would likely take place. The first would be to modify exist-ing dental implant structures. This was envisioned to either grow specific tissues on the surface of the implant or to add specific stimulating substances to the implant surface, both performed prior to place-ment in the oral cavity. It was also discussed that many efforts have been considered based on this di-rection already. The second overall approach would involve bioengineering the recipient dental implant site. This could involve enhancing the existing bone for the bone-to-implant interface or to enhance a bone-to-ligament transition area if that proved to be a desirable goal in the future. In either case, it was rec-ognized that biomechanical forces play a critical role and must be taken into account. For example, hydro-static pressure and compression are critical compo-nents in cartilage development and it is known that high-frequency vibration or ultrasonic forces can pro-mote the differentiation and synthesis of new bone. The group also acknowledged that, in all cases, an-giogenesis and new blood vessel formation are cru-cial to any tissue engineering effort.
The group then began a discussion of the prepared questions for the breakout session and the results of those discussions are provided and summarized be-low. In all cases, there was unanimous consensus on the answers.
What is the primary rationale for the development of bioengineering solutions?
The primary rationale has multiple motivations, includ-ing: (1) to improve the short- and long-term outcome of tooth replacement and craniofacial structure tissue
Bioengineering Group Report
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering Group
22 Volume 26, Supplement, 2011
engineering; (2) to expand the patient population receiving dental implants; (3) to reduce the techni-cal demands for tissue regeneration and limit pa-tient morbidity; and (4) to augment the beneficial aspects of healing responses and to minimize patho-physiological effects.
What is the potential for bioengineering to improve clinical outcomes (eg, enhanced predictability of clinical results with hard and soft tissues) in dental implant therapy?
The potential is extremely high. Discussion at the im-plant level included alteration of the implant surface, construction of periodontal ligament, creation of bone construct with preintegrated implants, and incorpora-tion of anabolic moieties. Discussion of the host site included quantity and quality of tissues in the context of prevention and reconstruction. Discussion also cov-ered the tissue engineered tooth and tooth hybrids.
What kinds of patients are most likely to need, want, or be candidates for bioengineering?
All patients at risk of losing dentoalveolar structures or diseased implants. All patients requiring reconstruction of craniofacial structures, including acquired and con-genital deformities, and skeletally immature patients. Bioengineering will also benefit compromised patients (systemically and locally), including iatrogenically in-duced patients (eg, previously operated patients and those with a history of radiation therapy).
What is the potential for bioengineering to improve a patient’s physical health (oral and systemic) and quality of life (ie, psychological, functional)?
At the implant level the potential is medium; at the host site the potential is high; and in tissue engi-neered tooth and tooth hybrids, the potential is low.
Is the current evidence sufficient to warrant further research and resources being directed toward bio-engineering relative to dental implant therapy?
At the implant level, the evidence is low/medium due to low need and past experience. At the host site, the evidence is high due to current experience, potential value, and low risk stratification. At the tissue engi-neered tooth and tooth hybrids level, the evidence is low due to the experimental nature.
These questions and the results of the group dis-cussion were presented in the plenary session. A few comments were made; however, none had a signifi-cant impact on the group’s answers to the questions. The group’s attention was then directed to the ques-tion posed by the organizing committee for the after-noon breakout session. The afternoon question to be discussed by the breakout group follows.
What additional evidence should be gathered to enhance development and enable transfer of bio-engineering as a new technology in regards to tech-nical properties, safety, efficacy and effectiveness, economic factor, and legal/ethical issues?
This discussion led to the recognition of bioengineer-ing as the convergence of three components: cells, factors, and scaffolds (Fig 1).
The group then discussed that, in the bioengineer-ing field, many of the technologies that were being explored were at very different points in the devel-opment process. Therefore, some technologies were closer to clinical application than others and as such would require less investment in regards to time, manpower, resources, innovation, and development. During the first plenary session, someone in the au-dience mentioned a scale that is used to evaluate technologies in relation to their development pro-cess, ranging from a basic idea and research all the way to its launch and application. This scale is called the “technology readiness level” or TRL, and is defined and shown in Fig 2.
Finally, the breakout group was asked to consider the afternoon question in regards to the clinical ap-plicability of the bioengineering technologies. As
Bioengineering
Cells Factors
Scaffolds
Bioengineering
Cells Factors
Scaffolds
Fig 1
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering Group
The International Journal of Oral & Maxillofacial Implants 23
noted above, since these technologies encompass a broad range of approaches, the breakout group con-sidered various day-to-day clinical indications and what technologies might be applied to help achieve a predictable and successful outcome. These tech-nologies ranged from existing technologies to single or multiple components involved in tissue engineer-ing, as noted above, to more complex bioengineering solutions envisioned to arrive in the future. The after-noon breakout group felt strongly that a major com-ponent of any tissue engineering effort in the oral cavity must include the growth of new blood vessels, such as through the process of angiogenesis. This was highlighted as a need for vascularity in order to
introduce nutrients, remove waste, and overall allow the development of new tissue formation. Finally, the technology was evaluated based on the TRL scale, not as specifically as TRL 1-9 but in more general terms as low, medium, or highly ready for application. Along with such an evaluation, an estimate was made by the group in terms of the risk of the technology and its benefit as well as its required investment. These last three areas were evaluated in terms of low, medium, or high. The breakout group’s discussion could be summarized in Table 1 that the group arranged from those clinical indications that might require less effort to those that would require greater effort.
Fig 2
TRL 9
TRL 8
TRL 7
TRL 6
TRL 5
TRL 4
TRL 3
TRL 2
TRL 1
Technology Readiness Level (TRL) is a measure used by some United States government agencies and many of the world’s major companies (and agencies) to assess the maturity of evolving technologies (materials, components, devices, etc) prior to incorporating that technology into a system or subsystem. Generally speaking, when a new technology is first invented or conceptualized, it is not suitable for immediate application. Instead, new technologies are usually subjected to experimentation, refinement, and increasingly realistic testing. Once the technology is sufficiently proven, it can be incorporated into a system/subsystem.
System test, launch& operations
System/subsystem development
Technology demonstration
Technology development
Research to prove feasability
Basic technology research
Table 1
Less effort Challenge Technology TRL Risk/benefit Investment
Horizontal bone growth Existing, factors, scaffolds (cells) High Low/low Low
Site preservation Existing, factors, scaffolds Medium/high Low/low Low
Peri-implantitis Existing, factors, scaffolds Medium Medium/high Medium
Vertical bone growth Existing?, factors, scaffolds (cells) Low/medium Low/high Medium
Soft tissues Existing?, factors, scaffolds (cells) Low Low/high High
Combination tissues Bioengineering Low Medium/high High
Large defects Bioengineering vascularity Low High/high High
Hybrid Bioengineering Low/medium High/medium High
More effort Bioengineered tooth Bioengineering Low High/medium Very high
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Bioengineering Group
24 Volume 26, Supplement, 2011
CLosInG CoMMenTaRy
As a final discussion, the group chair asked the bio-engineering expert to summarize his thoughts in regards to his experience in cartilage bioengineer-ing and how he saw that technology being applied to dental implants. He had eight areas for the summit participants to consider:
1. Surface modification of dental implants will likely yield significant results in regards to tissue integra-tion.
2. Varying substances, including catabolic enzymes, being added to the implant surface will likely be an area of future direction.
3. Attempts to accelerate osseointegration will likely take place, including in situ technologies, tech-niques that will begin in vitro to accelerate the tis-sue engineering process, tissue engineering of the dental implant–bone complex, and bioengineering of a soft tissue transition such as a dental implant–periodontal ligament.
4. Other materials will also be considered for implant compositions, such as ceramics.
5. Bioengineering will likely go beyond osseointegra-tion and include tooth bud tissue engineering.
6. Standards for success of bioengineering technolo-gies will need to be developed and might include some form of registry to help monitor outcome.
7. Future directions of research will likely also include optical or imaging methodologies to monitor bone healing and/or osseointegration.
8. All bioengineering efforts will need to be aware of pertinent regulatory pathways, as these can have a major influence on the clinical development and applicability of the technology.
ReFeRenCe
1. Buser D, Warrer K, Karring T, Stich H. Titanium implants with a true periodontal ligament: An alternative to osseointegrated implants? Int J Oral Maxillofac Implants 1990;5:113–116.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 25
NANOTECHNOLOGY
The replacement of teeth and bone with metal im-plants and plates is one of the most frequently
used and successful surgical procedures. The intro-duction of modern implants started with the work of
Brånemark et al, who in 1969 observed that a piece of titanium embedded in rabbit bone became firmly at-tached and difficult to remove.1 This led to Brånemark’s careful characterization of interfacial bone formation at titanium implant surfaces and demonstration of excellent osseointegration.2,3 Dental implants based on the work of Brånemark and colleagues were intro-duced in 1971.4 The total hip replacement was first de-veloped by Charnley in 1962, with stainless steel used for the stem and the attached ball.5,6 Charnley’s main contribution was to adapt polymethylmethacrylate cement from dentistry to fix the femoral stem and ac-etabular cup.7 After decades of subsequent research in industry and academia, implants have evolved and now show high survival rates and good longevity. Re-search has resulted in better designs, better materi-als, and more extensive clinical experience compared with the early years of implant development. One can argue, however, that the progress has been slow and incremental. Today’s clinicians are still using almost the same alloys described in the works of Brånemark and Charnley, many of which were originally devel-oped by the aerospace industry. Scientific evidence to determine the success (or failure) of dental implants in
1 Senior Scientist, Materials Sciences Division, Lawrence Berkeley National Laboratory, Berkeley, California.
2 Staff Engineer, Cordis Corporation, a Johnson & Johnson Company, Fremont, California.
3 Assistant Professor, Department of Oral Maxillofacial Surgery, University of California at San Francisco.
4 Associate Professor, Department of Surgery, University of California at San Francisco. Drexel University, Philadelphia, Pennsylvania.
5 Ann Stevens Associate Professor, Department of Materials Science and Engineering, Drexel University, Philadelphia, Pennsylvania.
6 Professor, Centre for Advanced Structural Ceramics, Department of Materials, Imperial College London, Exhibition Road, London, United Kingdom.
None of the authors reported a conflict of interest.
Correspondence to: Dr Antoni P. Tomsia, Materials Sciences Division, Lawrence Berkeley National Lab, One Cyclotron Road, MSD Building 62R0203, Berkeley, CA 94720. Email: [email protected]
Nanotechnology Approaches to Improve Dental Implants
Antoni P. Tomsia, PhD1/Maximilien E. Launey, PhD2/Janice S. Lee, DDS, MD3/ Mahesh H. Mankani, MD4/Ulrike G. K. Wegst, PhD5/Eduardo Saiz, PhD6
The requirements imposed by the enormous scale and overall complexity of designing new implants or complete organ regeneration are well beyond the reach of present technology in many dimensions, including nanoscale, as researchers do not yet have the basic knowledge required to achieve these goals. The need for a synthetic implant to address multiple physical and biologic factors imposes tremendous constraints on the choice of suitable materials. There is a strong belief that nanoscale materials will produce a new generation of implant materials with high efficiency, low cost, and high volume. The nanoscale in materials processing is truly a new frontier. Metallic dental implants have been used successfully for decades, but they have serious shortcomings related to their osseointegration and the fact that their mechanical properties do not match those of bone. This paper reviews recent advances in the fabrication of novel coatings and nanopatterning of dental implants. It also provides a general summary of the state of the art in dental implant science and describes possible advantages of nanotechnology for future improvements. The ultimate goal is to produce materials and therapies that will bring state-of-the-art technology to the bedside and improve quality of life and current standards of care. Int J Oral Maxillofac Implants 2011;26(suppl):25–44
Key words: coatings, dental implants, mechanical properties, nanotechnology, osseointegration, surface engineering
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
26 Volume 26, Supplement, 2011
the United States is almost nonexistent, as the coun-try lacks a national registry describing the rate and causes of failures. There are, of course, other avenues to alert clinicians about implant failures: the peer-re-viewed literature, other national registries (the Ameri-can Academy of Orthopaedic Surgeons is sponsoring one in the United States for hip and knee implants), US Food and Drug Administration alerts, manufactur-ing recalls, implant-retrieval labs across the country and worldwide, implant-retrieval studies in collabora-tion with clinical follow-up investigations, class-action lawsuits, and society presentations. The development of retrievable information relevant to medical devices is necessary to understand the overall performance of a particular implant and to improve the next genera-tion of medical implants. For improvements in implant design, implant-retrieval programs should be coor-dinated with clinical-outcome studies that include a patient’s history and medical records. Implant failure analysis not only helps manufacturers design better products but also provides a better understanding for clinicians of how the implant interacts with the body and which implants are best for a patient’s particular situation. In 2003, more than 700,000 dental implant procedures were performed in the United States and more than 1. 3 million procedures were performed in Europe.8 Approximately 1 million artificial hips and knees are implanted each year in the United States, as reported in 2006.9 Hip and knee replacements have a success rate of more than 90%, and dental implants fare better, at 90% to 95%.10
Dental implants have a long and successful history. The percentage of failure is very low, approximately 5%, mostly as the result of infection, rejection, acceler-ated bone loss, and poor osseointegration, with loos-ening of the implant.10 The most frequent cause of failure is insufficient bone formation around the bio-material immediately after implantation.11 Therefore, improvements are needed in this area. This is becom-ing even more important as clinicians and patients are pushing for faster healing times. Consequently, most of the recent modifications in implant designs have been geared toward reducing the time needed to wait before loading. It is here that the implant surface and implant-tissue interface are critical.12 Current surface chemistries and morphologies are controlled, at best, on the micron level, but tissue response is mainly dic-tated by processes controlled on the nanoscale level (Fig 1). Understanding and controlling interfacial reac-tions at the nano level are vital to developing new im-plant surfaces that will prevent rejection and promote adhesion and integration to the surrounding tissue.
Here, the first promising avenue is through sur-face engineering that would include nanoscale to-pography and/or coatings for better and faster os-seointegration of implants designed to function for the lifetime of the individual. However, the literature describing and comparing the different approaches is often confusing. Worldwide, there are 80 com-panies producing 220 various dental implants, so comparisons are often difficult.10 Likewise, there are few controlled studies that simultaneously compare
Impl
ant
Impl
ant
Impl
ant
Ti oxide
Immersed into bioliquid
Cell membrane with membrane proteinsHydrated cation
Hydratedanion–
+
Fibrous connective tissue
Water molecules
GlycolipidsIntegral proteinwith channel
Hydrophobictails
Peripheralproteins
Hydrophilicheads
Integralglycoproteins
Cytoplasm
Extracellular �uid
Fig 1 Successive events following implantation of a Ti-based material. Upon exposure to oxygen in air or water, Ti and its alloys spontaneously form a stable and strongly adherent oxide film (nanosecond timescale). Water molecules are adsorbed on the Ti oxide surface. The next sequence of events is not very well understood. Immediately after implantation, implants are coated with a fibrous connective tissue, which degrades and is replaced ideally by bone (adapted from Boyan et al13). The thickness of fibrous connec-tive tissue depends on the success of osseointegration. Once the cells reach the surface, their interaction takes place through the protein coatings (adapted from Kasemo14 and McMurry and Castellion1).
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 27
different implants, especially in the clinical setting. Manufacturers often do not find it in their best inter-est to participate in head-to-head competitions with their rivals, and clinicians often do not have sufficient patient numbers or motivation to initiate these stud-ies on their own. Additionally, variations in the patient population may influence the success of the implant. There are no commonly accepted guidelines for the design of surface topographies or the deposition of coatings, and the clinical evidence is often conflict-ing. As described later, this may be a result of the poor control of factors associated with fabrication tech-niques, rather than problems with the design itself. One critical problem is how to translate the results of in vitro cell-culture studies performed on model sur-faces in pristine conditions to the design and fabrica-tion of three-dimensional (3D) implant materials with complex shapes that will work in the harsh human oral environment.
The second scientific challenge is to develop a new generation of implant materials that will combine the advantages of ceramics, in particular their inertness, with a mechanical response comparable to those of dental implant alloys. The unique properties of ce-ramic materials, including their outstanding corro-sion resistance and excellent esthetics, make them appealing candidates for many dental applications. However, their inferior mechanical properties, partic-ularly their poor fracture resistance, have hampered their commercial use, especially in load-bearing situ-ations. This is a particular problem when designing porous implants or implants with rough and porous surfaces for better osseointegration. While the poros-ity will improve osseointegration, increased porosity can easily result in diminished strength and fracture at relatively low loads. Through new fabrication tech-nologies, these limitations may be overcome. Their potential has not yet been realized.
Solutions to these scientific challenges have a ben-efit that extends beyond the construction of implants. They can offer clinicians a path toward the resolution of a much more challenging goal: the construction of a true biologic tooth. The technical foundation for a neo-tooth will likely include surfaces that bind quick-ly to bone and occlusal surfaces that offer toughness during mastication. In the meantime, dentists need strategies to improve currently available metallic dental implants through surface modifications of the implant, which can be accomplished either by apply-ing novel ceramic coatings or by patterning the im-plant’s surfaces. These approaches are described in the following.
SurFACE mOdiFiCATiONS OF dENTAL impLANTS
Ceramic CoatingsVarious coatings have been developed to improve an implant’s ability to bond to living tissues, particularly bone. The idea is to apply a thin ceramic layer that will bond both to the implant and to the surrounding tissue while promoting bone apposition. Candidate coating materials are bioactive compounds able to promote cell attachment, differentiation, and bone formation. The most prevalent bioactive materials are calcium phosphates (CP), such as hydroxyapatite (HA) or tricalcium phosphate (TCP), and bioactive glasses. When implanted, these bioactive ceramics form a car-bonated apatite layer on their surfaces through dis-solution and precipitation. This phase is equivalent in composition and structure to the mineral phase of osseous tissue. At the same time, collagen fibrils can be incorporated into the apatite agglomerates. The sequence of events is poorly understood but appears to be: adsorption of biologic moieties and action of macrophages, attachment of stem cells and differ-entiation, formation of matrix, and, finally, complete mineralization.13–18
Animal studies have shown that, compared with uncoated implants, implants with a thin layer of CP show markedly enhanced interfacial attachment of bone tissue over a period of several months.19–26 Also, numerous histologic studies provide evidence that coated implants yield a more reliable interface with bone than pure titanium (Ti).27–36 Coating implant al-loys with CPs, therefore, is advantageous; it facilitates joining between a prosthesis and osseous tissue and consequently increases long-term integrity. Benefits arise during healing and subsequent bone-remod-eling processes,30,37 including faster healing time,38 enhanced bone formation,39,40 firmer implant-bone attachment,39,41 and a reduction of metallic ion re-lease.42,43 However, coating dental implants is not without controversy. Recent clinical orthopedic stud-ies44–46 indicate that there is no clear advantage to HA coatings on the femoral component of hip implants. The situation with dental implants is no different; there are contradictory reports on the effectiveness of HA coatings, as it is difficult to compare coatings applied using different methods.47 Thus, the issue of coating usefulness has not been fully resolved.
Ideally, implant coatings should be tailored to ex-hibit prescribed biologic attributes for each specific application. They should have strong adhesion to the implant and good fixation to bone. Their micro-structure and dissolution rates must be programmed to match the in vivo healing process, and they could serve as templates for the in situ delivery of drugs and
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
28 Volume 26, Supplement, 2011
growth factors at the required times. Requirements for the new family of coatings include: (1) good adher-ence to the implant, (2) fixation to the bone, (3) fine gradient and thickness control with a programmed dissolution rate in body fluids, and (4) therapeutic ca-pabilities. These are discussed in the following.
Coating/Implant Adherence. Most reports in-dicate that currently available coating techniques provide inadequate adherence of CP coatings to Ti alloys; the cited bond strengths of 15 to 30 MPa are very low.48–51 Systematic studies of the chemical and microstructural factors that control the interfacial strength and toughness are needed to optimize the mechanical stability of the coatings. Key principles for bonding ceramics to metals, elucidated over the past decade,52–63 can guide such an investigation, but researchers still need to develop standard procedures to test adhesion, and a clear understanding of the mechanisms of interfacial failure in the body environ-ment is required.
Fixation to Bone. Knowledge of the biologic pro-cesses occurring at the biomaterial-tissue interface is of utmost importance in predicting implant integra-tion and host response.64 Two primary modes of at-tachment are: (1) mechanical, in which the implant has a rough, porous surface into which bone grows (often supplemented by the use of a bone cement); and (2) chemical, in which bone “bonds” to the im-plant material. Here it is difficult to decouple the ef-fects of coating chemistry and topography. It has
been observed that differences in the nature of the implant-bone interface depend upon the specific coating. However, there is little agreement regarding which is the ideal coating chemistry. Dissolution of calcium and phosphorus from the coating may pro-mote mineralization and bone formation, but it is not clear to what degree coating solubility contributes to the best fixation, and excessive resorption can limit the lifetime of an implant.65,66
Programmed Dissolution Rates. A critical goal in the design of novel coatings is the programming of their dissolution (bioresorption) rates. The role of sol-ubility of coatings in the body is poorly understood.67 The presence of highly soluble phases markedly de-creases the mechanical stability of the coating in vivo, but some solubility of coating material expedites fixa-tion.68,69 These findings suggest that graded coatings, designed with a soluble surface to facilitate bonding to bone and an insoluble layer in contact with the metal to provide adhesion, corrosion resistance, and long-term mechanical stability, could offer a signifi-cant improvement over current materials. Both the composition and thickness of the graded coating lay-ers can be controlled to manipulate resorption rates. Their resorption can be programmed to match heal-ing rates and to expose different microarchitectures, chemical patterns, and porosities at different times to optimize the biomaterial coating surface for differ-ent periods of the healing phase. Possible designs of graded coatings are depicted in Fig 2.
Substrate
Fully resorbableRobocastingDip-coating
Substrate
Inert glassDip-coating
EPD
Substrate
Inert glassDip-coating
EPD
Substrate
Inert glassDip-coating
EPD
Soluble polymerfor drug delivery
Substrate
Inert glassDip-coating
EPD
TexturedRobocasting
PorousRobocasting
Porogen
PatternRobocasting
Fill poresRobocastingIn�ltration
Bioactive or bioresorbable layerglass or glass/HA
Fig 2 Possible designs for graded coat-ings. The layer in contact with the sub-strate could be formulated to provide good adhesion and long-term stability. The top layer can vary in thickness and porosity, can be a mixture of an inorganic and an organic component, and, if need-ed, be encapsulated in a bioresorbable material as either a glass (fabricated by pulsed laser deposition) or a polymer (by robocasting or dip-coating). EPD = electro-phoretic deposition.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 29
Drug Delivery. Inflammatory responses to im-plants are a significant problem in the health-care industry. Typically, medications are given to a patient following surgery to suppress inflammation and to facilitate the intended performance of the implanted medical device. Although generally helpful, in many cases this approach is insufficient or entirely inef-fective.70–72 A different approach is to provide a local dose of anti-inflammatory agents that is gradually re-leased from a coating on the surface of the implant-ed device.73,74 The main advantage of this approach over traditional means of administering the drug is that the drug can be released directly at the implant site without having to go through the bloodstream. This lowers the amount of drug needed, reducing the overall toxicity and side effects. In addition, growth factors that are known to encourage tissue-implant integration, such as transforming growth factor-beta (TGF-β),75,76 may be delivered locally using this plat-form. These chemicals could be incorporated into the porosity of microporous and nanoporous coatings, or they could be dispersed in biodegradable polymers, and combined with the bioactive glass/CP coatings. Developing the right platform to control the release rate is the key and is closely related to the control of the degradation rates.
Perhaps the most popular coating method is plas-ma spraying of HA.77–82 However, plasma spraying of HA offers only rudimentary control of the coating thickness and composition. The thickness of plasma-sprayed coatings typically exceeds 50 µm. The high processing temperatures cause partial thermal decom-position of HA, leading to the formation of other CPs, including 22% to 62% of highly soluble amorphous calcium phosphate,83–87 alpha tricalcium phosphate (α-TCP), β-TCP, tetracalcium phosphate, and calcium oxide.49,88–90 This results in coatings with unacceptable heterogeneous properties. Long-term in vivo studies demonstrate that some of the major causes of failure of HA-coated metal orthopedic and dental implants reside in the coating.47,91 Severe problems include: (1) unreliable adhesion, ie, the coatings can detach, yielding floating fragments92–99; (2) continued disso-lution of the coating, leading to catastrophic failure of the implant at the coating-substrate interface,100 and with any attempts to increase crystallinity and reduce solubility by postcoating thermal annealing markedly degrading the coating adherence88,91,101–104; (3) vari-ability during processing in terms of resulting phases, stresses, and cracking37,84,105–108; (4) partial crystalliza-tion of the deposited coating, leading to the presence of more soluble CP compounds48,109–111; (5) signifi-cant degradation in the fatigue resistance and endur-ance strength of the implant alloy112; (6) very irregular morphology of the coatings; (7) poor control of the
coating thickness, with greater risk of fracture, with a thicker coating; and (8) poor control of physicochemi-cal properties and hence poor biologic stability of the coating.113,114
Several other techniques have been used to apply CP coatings on metallic alloys, including sol-gel, radio-frequency magnetron sputtering, and others.106,114–132 These techniques may offer a more accurate composi-tional control and the possibility of fabricating much thinner layers (of the order of 1 µm or less). This could be advantageous for coating stability, as the driving force for cracking and delamination decreases with decreasing coating thickness. The nature of the coat-ing and the process might be adjusted to modify the interfacial strength. However, these approaches have yet to be translated into commercial designs. Some are line-of-sight techniques not suitable for coat-ing implants with complex shapes and result in in-complete coverage of the implant. Also, cost is a key variable that must be taken into account, and highly dense coatings produced by sputtering are probably the most desirable but are very expensive to fabricate.
There is increasing interest in the use of bioactive glasses in the fabrication of coatings. The potential of bioactive glass coatings has been recognized since the discovery of the original Bioglass composition by Hench.90 Bioglass has excellent bioactivity and could be used to enhance the adhesion of the implant to the bone. Furthermore, the glass properties can be easily adjusted from bioactive to bioresorbable or bioinert by controlling the composition.90 This cre-ates the possibility of fabricating layers with finely tuned properties. However, initial attempts to coat metallic implants with the original Bioglass were marred by the generation of large thermal expansion stresses and high reactivity between the metal and the glass.16 Subsequently, several techniques have been investigated for the preparation of glass coat-ings, such as enameling, plasma spray, radiofrequen-cy sputtering, sol-gel, pulsed laser deposition (Fig 3), and others.47,133–141 Although it has been possible to deposit glass layers that retain bioactivity, recurrent problems are the control of the glass-metal reactions to achieve good coating adhesion and the genera-tion of large thermal stresses during processing that can cause cracking and/or delamination of the coat-ing. The solution to the problem requires the devel-opment of coating procedures and novel bioactive glasses and glass-ceramics with adequate thermal expansion coefficients and softening points.
Lopez-Esteban et al have demonstrated that a new family of bioactive glasses, in the system Si-Ca-Mg-Na-K-P-O, exhibits thermal expansion coefficients that are similar to those of the metallic alloys used in dental and orthopedic implants.142 This is achieved through
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
30 Volume 26, Supplement, 2011
the partial substitution of calcium by magnesium and of sodium by potassium. These glasses have adequate softening points to be used in the fabrication of coat-ings by a simple enameling technique. Strong glass/metal adhesion is achieved through the formation of thin interfacial layers. The procedure can be extend-ed to the fabrication of graded coatings through the sequential deposition of different glass and glass-ce-ramic layers. For example, graded coatings have been fabricated on Ti and cobalt-chromium alloys consist-ing of a high-silica glass in contact with the metal and a composite surface layer that consists of a mixture of a low-silica glass and synthetic HA particles. The high-silica layer is very resistant to corrosion in body fluids; it provides good coating adhesion and long-term sta-bility, while the surface layer is designed to enhance coating attachment to the tissue (Fig 4).
The interaction of glass coatings with tissue can be further manipulated by designing appropriate surface textures. Furthermore, in vitro analysis in cell cultures has shown that bioactive glasses and coatings can indirectly affect osteoblast gene expression through their dissolution products.143–147 Quantitative real-time reverse-transcriptase polymerase chain reaction analysis showed that the silicate glass coating extract
induced a twofold expression of Runx-2, a key marker of osteoblast differentiation, compared with titanium alloy (Ti-6Al-4V) and tissue-culture polystyrenes.148 Future research should address the identification of specific chemical cues behind the induction of gene expression and the tailoring of layer compositions to control such effects.
Another technique worth further exploration is an-odic oxidation, which has been used as a means to en-gineer the surface of Ti-based implants.149,150 This tech-nique can be used to create an adherent oxide coating on the implant surface. Through the selection of differ-ent electrolytes and manipulation of the conditions, it is possible to create oxide layers with a wide range of stoichiometries as well as microporosities and nano-porosities. It is also possible to incorporate Ca and P ions into the layers. This is a relatively simple and eco-nomical technique that can be easily adapted to fabri-cation, and anodized implants are commercially avail-able. Several in vivo and clinical studies have shown that anodization enhances integration at early stages, and anodized surfaces have been considered as plat-forms for drug delivery because of their characteristic micropore/nanopore distribution. However, as for many other treatments, it is difficult here to separate
Focusinglens
Laser beamTarget
HeaterSubstrate
Vacuum
As prepared5 µm
Annealed700°C 5 µm
Si
CaKPN
aM
gAlO
Ti
VCou
nts
(a.u
.)
Energy (keV)0 2 4 6
Focusinglens
Laser beamTarget
HeaterSubstrate
Vacuum
As prepared5 µm
Annealed700°C 5 µm
Si
CaKPN
aM
gAlO
Ti
VCou
nts
(a.u
.)
Energy (keV)0 2 4 6
Focusinglens
Laser beamTarget
HeaterSubstrate
Vacuum
As prepared5 µm
Annealed700°C 5 µm
Si
CaKPN
aM
gAlO
Ti
VCou
nts
(a.u
.)
Energy (keV)0 2 4 6
Fig 3 Pulsed laser deposition (PLD) can be used to prepare thin coatings of highly bioactive glasses that cannot be fabri-cated by other methods. (a) Schematic of the PLD process. A la-ser beam is used to evaporate the glass into the substrate and form a film. Afterward, thermal treatment is needed to promote adhesion. The coatings are bioactive and retain the complex glass stoichiometry. The substrate can be moved and rotated during deposition to coat 3D pieces with complex shapes. (b) Surface of a thin glass coating deposited on Ti-6Al-4V by PLD. Thin coatings are more resistant to cracking and delamination. Because the coating has submicron thickness, the substrate peaks are visible in the electron dispersive spectroscopic anal-ysis. (c) Quantitative analysis indicates that the stoichiometry of the layer is in ± 5% by weight of the original glass target.
a
c
b
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 31
the effects of surface chemistry and morphology. In ad-dition, as with other implant technologies, systematic studies of the factors that control adhesion of the oxide layer to the alloy are still lacking.
Most likely an ideal coating will not be fabricated using a single procedure or material but by combin-ing several of them to fabricate layers that blend or-ganic and inorganic phases, with thicknesses rang-ing from hundreds of microns to the nanometer level, and chemically and topographically textured surfaces. Each technique has specific advantages and limitations, yet no single procedure can fabricate lay-ers combining organic and inorganic materials and generate textured surfaces. New coating techniques should be flexible enough to use glasses and CP phases with a wide range of compositions and should generate chemically and topographically textured surfaces while integrating organic and inorganic components. To accomplish this, colloidal techniques
(dip-coating, electrophoretic deposition, or robocast-ing) able to prepare thick layers (> 10 µm) can be com-bined with thin-film formation using techniques such as pulsed laser deposition (Fig 3).151,152 The translation of rapid prototyping techniques to the fabrication of coatings could prove very useful. For example, robo-casting, a 3D technique that can print different mate-rials at the same time and produce porous surfaces for infiltration of organic materials, can also be employed. These techniques can also be used to integrate organ-ic materials into coatings to serve as templates for the delivery of drugs and growth factors.
Surface FunctionalizationAn alternative or complementary strategy to the use of coatings for dental implants is the molecular grafting or chemical treatment of implant or coating surfaces to enhance cell adhesion and promote mineraliza-tion and the production of matrix and marker proteins.
Fig 4 (a) Environmental scanning electron microscope im-age showing a cross section of a graded glass coating after a 6-month in vivo test in a pig model. The coating survived, main-taining excellent adhesion to the implant. A corroded layer can be observed on the coating surface, providing adhesion to the bone, but the high-silica layer in contact with the alloy remains intact, maintaining good adhesion to the metal. Preliminary tests indicate that after 6 months, the bone matrix in the vicinity of the bone-implant interface of coated implants had remodeled itself into lamellar-type bone, while the uncoated implant–bone inter-face still showed woven-type bone. It is reasonable to assume that the coated device had less micromovement, such that the biomechanical integration of the device to the surrounding bone tissues was achieved earlier during the experimental period, facilitating the transformation of the woven bone matrix into a lamellar type over a 2- to 6-month period. (b and c) During inden-tation tests, the cracks do not propagate at the glass/metal in-terface, indicating good coating adhesion achieved through the formation of a thin (100- to 150-nm) Ti5Si3 layer that can be ob-served using high-resolution transmission electron microscopy.
Glass
Ti5Si3
Ti-6Al-4V
50 nm
50 µm
Ti-6Al-4V
Glasscoating
Silicahydrogel
Bone
Ti-6Al-4V Glass
Acrylic resin
40 µm
Glass
Ti5Si3
Ti-6Al-4V
50 nm
50 µm
Ti-6Al-4V
Glasscoating
Silicahydrogel
Bone
Ti-6Al-4V Glass
Acrylic resin
40 µm
Glass
Ti5Si3
Ti-6Al-4V
50 nm
50 µm
Ti-6Al-4V
Glasscoating
Silicahydrogel
Bone
Ti-6Al-4V Glass
Acrylic resin
40 µm
a
c
b
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
32 Volume 26, Supplement, 2011
Different treatments have been used to create hydro-philic implant surfaces (eg, through chemical etching) to promote protein adhesion and subsequent cell at-tachment (Fig 5). However, the native oxide layer usu-ally present on the surface of metallic implants exhibits relatively low contact angles with water without any particular treatment. Overall, several in vivo studies suggest that implants with increased hydrophilicity exhibit faster integration with greater bone-to-implant contact, but key questions remain: Is hydrophilicity the key variable? If so, what degree of hydrophilicity is needed to make a difference? Are there additional benefits derived from the surface treatment?
The logical candidates for molecular grafting are pro-teins present in the extracellular matrix (ECM), and im-plant surfaces have been functionalized with fibronec-tin, vitronectin, or laminin, to name a few.153 Recently, the focus has shifted to the use of signalling domains, composed of several amino acids. These domains are present along the chain of the ECM proteins and are the ones that interact with cell membrane receptors. Perhaps the best-known example is Arg-Gly-Asp (RGD), the signalling domain derived from fibronectin and laminin. However, other sequences such as Tyr-Ile-Gly-Ser-Arg (YIGSR) or Arg-Glu-Asp-Val (REDV) have also been used.154–156 The use of a short peptide is more convenient because the long molecules can be folded, and, as a result, the binding domains may not be avail-able. Two important aspects are the development of techniques to bind the molecules to the surface and the control of their spatial distribution.
Several approaches have been used to functionalize the Ti surface with different molecules, from adsorption (physical or chemical) to the use of covalent bonding or self-organized layers.157–159 The simplest procedures in-volve immersion of the material in a solution containing the desired molecules to promote adsorption on the surface. This approach has disadvantages because it can
result in relatively poor adhesion. Covalent bonding us-ing, for example, linker molecules can promote stronger adhesion to the implant, and it has been used to attach proteins, signalling domains,157–159 antibiotics,160 and growth factors such as human epidermal growth factor or recombinant human bone morphogenetic protein-2 to Ti and TiO2 surfaces.161,162 However, it may impose a spatial orientation on the grafted domains or proteins, limiting their effectiveness.154 Diverse molecules can also be incorporated into CP coatings or on Ti surfaces prepared by anodic polarization.157–159 The surface density is also important. It has been shown that the function of the osteoblastic cell lines can be enhanced by matching the surface density of the selected mole-cules to the distribution of the corresponding receptor in the cell membrane. This can be achieved, for exam-ple, by using functionalized gold nanoparticles whose density on the surface can be manipulated.163,164 Al-though most research on this subject supports the idea that functionalization can enhance and accelerate os-seointegration, the key is to adapt the functionalization techniques to the surfaces of specific dental alloys—each with different surface chemistries—and to be able to create surfaces that will display different molecules with controlled spatial distribution and the required degree of adhesion. Furthermore, the in vivo data needed to select optimum attachment methods and surface densities are still lacking.
Surface Topography of dental implantsIt has long been recognized that the chemical and morphologic characteristics of implant surfaces affect the behavior of the surrounding tissues. Numerous studies have shown marked differences in the in vitro and in vivo responses of textured implant surfaces, demonstrating that the ability of the implants to sup-port bone formation can be enhanced by modifying surface topography.165–168 This is critically important
Nanorods on the dental implant surface after etching
Fig 5 By coating dental implants with thin films of CP glass-ceramics and then using controlled crystallization, nanofeatures and microfeatures can be obtained on the scaffold surfaces after etching.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 33
in the case of dental implants, which are built using bioinert materials and where optimal and fast osseo-integration is needed to achieve long-term function-ality. It is generally accepted that rough surfaces will favor mechanical interlocking with the surrounding tissue, which will help implant stability. At a more fundamental level, surface topography may affect cell differentiation (perhaps by influencing cell shapes or by inducing specific signals)169–171 and consequently promote the formation of ECM and bone apposition. Although hundreds of papers have investigated sur-face engineering, decoupling and understanding these different effects is still an open scientific chal-lenge, and the answer could prove extremely useful to rationally design implant surfaces.
The topography of the implant surfaces can now be manipulated along a wide range of scales, down to the nanolevel. Several implant designs use sur-faces with large pores to promote bone ingrowth and favorable anchorage. Previous analysis indicated that these pores have to be on the order of 100 µm and larger to allow for bone ingrowth. These can be fabricated using partial sintering of metal particles or spheres on the surface. However, there is still some controversy regarding the benefit of this approach with respect to screw geometries. A recent study sup-ports the idea that screw implants perform better in long lengths and denser bone, while porous surfaces are more adequate at short lengths and in cancellous bone.172 In addition, excessive roughness can have the disadvantage of making the implant harder to remove (if necessary) and may be detrimental for im-plant strength.172
Texturing of the implant surface at the micro-level has been proposed as a feasible alternative to promote bone apposition. This work is based on the abundance of in vitro studies indicating that some degree of roughening at the microscopic scale favors cell attachment and differentiation.173,174 Several pa-pers and patents have described different techniques to increase surface roughness, including sandblast-ing, grinding, Ti plasma spraying, and laser textur-ing.28,149,175 The in vivo results are mixed. While many reports indicate an improvement in bone apposition using rougher surfaces, others suggest either no significant benefit or that the result will depend on the implant design. For example, Walboomers and Jansen compared the tissue reaction to smooth and microgrooved implants (width of grooves 2 or 10 µm, depth 1 µm), at different implantation sites.176 They were unable to prove the existence of an effect of implant surface topography on in vivo soft tissue response. Other recent studies reached similar con-clusions.177 It could be argued that the main advan-tage of microtextured surfaces is their contribution to
mechanical interlocking and tissue attachment of the implant. It should also be noted that implants with surfaces that are too rough have a high possibility of peri-implantitis, and the roughness will affect the de-gree of hydrophilicity. This effect could be described using the Wentzel equation: cosθr = rcosθ (where θr is the macroscopic contact angle on the rough sur-face, θ is the true contact angle, and r is a ratio be-tween actual and apparent area, r ≥ 1).178 Notice that according to this equation, for θ < 90 degrees, as can be expected for Ti alloy surfaces, roughness tends to decrease the contact angle (increase hydrophilicity). This simple model shows how roughness can have an effect at multiple levels.179
Unfortunately, few studies have systematically compared the performance of implants with surfaces treated using various methods. In particular, similar roughness (average peak-to-valley distances) can be obtained using diverse technologies, but the char-acteristic of the surface (random versus oriented fea-tures, sharp versus smooth) can vary greatly from one implant to another and there is no standard approach to fully quantify implant topography and compare it with in vitro and in vivo results. Furthermore, the sur-face chemistry can also be altered in different ways by roughening treatments. Ti alloys are covered by a native oxide layer whose characteristics can change according to treatment. For example, some studies suggest that sandblasting with TiO2 particles elicits more beneficial results than blasting with other ce-ramics.149,180 This is perhaps a result of the presence of ceramic particles that are left embedded in the metal after the sandblasting process. Finally, differ-ent treatments often result in a hierarchical surface structure where nanoscale features are also present. These features are often ill characterized but, as will be discussed later, can have a profound impact on the biologic response.
The arrival of nanotechnology has opened up new opportunities for the manipulation of implant surfaces. It is believed that implant surfaces could be improved by mimicking the surface topography formed by the ECM components of natural tissue. These ECM compo-nents are on the nanometer scale, with typical dimen-sions of 10 to 100 nm. Many in vitro studies have shown how cell attachment, proliferation, and differentiation are responsive to nanoscale features such as pillars or grooves prepared, for example, using nanolithography. In this respect, not only the size of the feature but also its distribution (ordered versus random) can play a role. Nanopatterned surfaces may also provide better adhe-sion of the fibrin clot that forms right after implantation, facilitating the migration of osteogenic cells to the ma-terial surface.181 At a more basic level, it is still not com-pletely clear that nanopatterning will be substantially
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
34 Volume 26, Supplement, 2011
better than patterning on the micron scale or what the interplay between surface topography and chemistry is. It is well known that a high density of nanopillars will create a super-hydrophobic surface that can be detri-mental,182 an d many of the basic studies have only been performed on flat surfaces and using model ma-terials (eg, silicon or polymethylmethacrylate).183,184 Extrapolation of these techniques to the fabrication of dental implants guarantees that these features will be robust enough to survive implantation, and reliable testing of in vivo effects of nanoscale manipulation is a technological challenge yet to be met.
NANOCOmpOSiTES FOr bONE rEGENErATiON
Because of their strength and toughness, metal im-plants have been used in orthopedic and dental surgeries for many years. Ti and its alloys have had considerable advantages over other metals because of their inertness, which yields excellent biocompat-ibility and nonsensitization of tissues. However, issues remain concerning the release of Ti and alloyed ele-ments from implants and the formation of Ti debris following wear during implantation. Metal and metal alloys (ie, Ti, Al, V, Ni) in implants and dentures have the potential to provoke allergic reactions and cause vague constitutional symptoms.185,186 Ceramic mate-rials are known to have excellent esthetics, corrosion resistance, and biocompatibility, and several ceramic implants have already been commercialized. The con-tinuing interest in the use of modern ceramics for the fabrication of dental implants has been emphasized by several presentations during recent meetings of the International Association of Dental Research and by recent research efforts by several European and Japanese companies (Kyocera, Dentsply, Metoxit, etc). Unfortunately, in contrast to metallic materials, most ceramics suffer from a nearly complete lack of plastic deformation; this is a result of the absence of mobile dislocation activity, although other modes of inelastic deformation, such as microcracking and in situ phase transformation, can provide limited alternative defor-mation mechanisms. The implications of this are that ceramics are inherently brittle, with an extreme sen-sitivity to flaws. As a result, fracture almost invariably occurs catastrophically (with crack initiation concomi-tant with instability) by cohesive bond breaking at the crack tip, with a resulting very low (intrinsic) tough-ness of roughly 1 to 3 MPa.m0.5. This problem is aggra-vated when designing porous implants or implants with rough and porous surfaces for better osseointe-gration. In this case, the porosity can easily result in diminished fracture strength at relatively low loads.
This dependence of strength on the distribution of preexisting flaws has several important implica-tions for brittle materials. In particular, large speci-mens tend to have lower strengths than smaller ones, and specimens tested in tension tend to have lower strengths than identically sized specimens tested in bending because the volume (and surface area) of material subjected to peak stresses is much larger; in both cases, the lower fracture strength is associ-ated with a higher probability of finding a larger flaw. Toughening ceramics, as with virtually all brittle ma-terials, must be achieved extrinsically, ie, through the use of microstructures that can promote crack-tip shielding mechanisms such as crack deflection, in situ phase transformations, constrained microcrack-ing (although this mechanism is generally not too po-tent), and, most importantly, crack bridging. Extrinsic mechanisms result in resistance-curve (R-curve) be-havior (where the crack-driving force to sustain crack-ing increases with crack extension), as they operate primarily behind the crack tip to lessen the effective crack-driving force; they are therefore mechanisms of crack-growth toughening. The incorporation of rein-forcements in the form of fibers, whiskers, or particles can also toughen ceramics, although the motivation may be rather to increase strength and/or stiffness. For toughening, crack bridging is the most prominent mechanism, particularly in ceramic-matrix compos-ites; through the use of fibers with weak fiber/matrix bonding, the fibers are left intact when the matrix fails, spanning the crack wake and acting as bridges to inhibit crack opening.187
The key question is: Can a new family of ceramic-based materials be created that will equal or improve the mechanical performance—particularly the com-bination of strength and toughness—of metallic al-loys? In ductile materials such as metals and polymers, strength is a measure of the resistance to permanent (plastic) deformation. It is defined invariably in uni-axial tension, compression, or bending, either at first yield (yield strength) or at maximum load (ultimate strength). The general rule with metals and alloys is that the toughness is inversely proportional to the strength. In brittle materials such as ceramics, where at low homologous temperatures macroscopic plastic deformation is essentially absent, the strength mea-sured in uniaxial tension or bending is governed by when the sample fractures. Strength, however, does not necessarily provide a sound assessment of tough-ness, as it cannot define the relative contribution of flaws and defects from which fracture invariably en-sues. For this reason, strength and toughness can also be inversely related in ceramics. By way of example, refining the grain size can limit the size of preexisting microcracks, which is beneficial for strength, yet for
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 35
fracture-mechanics–based toughness measurements, where the test samples already contain a worst-case crack, the smaller grain size provides less resistance to crack extension, generally by reducing the potency of any grain bridging, which lowers the toughness.
In recent years, the development of nanostruc-tured ceramic materials as a path to achieve enhanced strength and toughness has attracted a great deal of interest in the ceramics community. However, a controversial question in composite toughening is whether the use of nanoscale reinforcements favors strength to the detriment of fracture toughness. Al-though strength and toughness may seem to be simi-lar, changes in a material’s microstructure often affect the strength and toughness in very different ways, and they tend to be mutually exclusive.188 It has been claimed that composites made with such nanoscale reinforcing materials as nanotubes, platelets, and nanofibers would have exceptional properties; how-ever, results to date have been disappointing.189–191 A good example here is the excitement generated by the discovery of carbon nanotubes, which have excep-tionally high strengths (better than ε/10; ε is Young’s modulus).192 However, it is still uncertain whether such nanotubes can be harnessed into bulk structural mate-rials that can utilize their high strength (and stiffness) without compromising toughness. If the composite material is to be used for a small-volume structure with high strength, clearly the reinforcements must also be small; moreover, as there is a lessened probability of finding defects, small-volume reinforcements tend to be much stronger, as has been known since the early days of research on whiskers.193 However, from the perspective of toughening, a strong argument could be made that prime (extrinsic) toughening mecha-nisms such as crack deflection and particularly crack bridging are promoted by increasing, not decreasing, reinforcement dimensions.187
Recently, it has been shown that a possible path to combining high strength and toughness in a ceramic material is to take advantage of the transformation toughening mechanisms in nanozirconia-alumina materials.194,195 These materials consist of a disper-sion of a small amount of tetragonal zirconium oxide (ZrO2) particles (typically around 200 nm in size) in an aluminum oxide (Al2O3) matrix. The stress-induced phase transformation of metastable tetragonal grains toward monoclinic symmetry ahead of a propagat-ing crack leads to a significant increase of the work of fracture. For the same preexisting defects, these composites can work at loads two times higher than the pure materials without delayed failure. Hardness and stability are of prime interest in the dental field. Alumina-zirconia nanocomposites with relatively low zirconia content (below the percolation limit, ~16%
by volume) exhibit similar hardness values to alumina and are not susceptible to the hydrothermal instabil-ity observed in the case of zirconia bioceramics that caused the in vivo degradation of zirconia femoral heads and has resulted in the almost complete aban-donment of ZrO2 as an orthopedic biomaterial.194–196
The stabilization of the tetragonal zirconia phase in the nanocomposites is thought to arise from a com-bination of surface energy effects, constraints of the rigid matrix, and stabilizing oxide additions, eg, yttria, such that transformation can occur locally once the constraints are removed, in this case when the crack propagates.197–200 It is then necessary to develop processing methods that will allow the fabrication of materials in which the zirconia grains have controlled submicronic size and are homogenously dispersed in the ceramic matrix. Colloidal procedures in which a liquid precursor of the zirconia phase is mixed with the powders of the matrix ceramic phase present great potential. The use of a liquid precursor allows a more intimate mixing and a more homogenous distri-bution of nanoparticles, preventing the formation of aggregates after the heat treatment.201
Alumina/zirconia nanocomposites offer an ex-ample of how nanotechnology offers an attractive path to the development of new implant materials, but ceramics, even nanocomposite ceramics, will not replicate the unique combinations of mechanical properties of tooth tissues, as they are, for example, much stiffer and more wear-resistant. A possibility is to develop new hybrid organic/inorganic materials with properties that will closely match those of the tissue for which they substitute. However, the use of synthetic composite materials as permanent replace-ments for bone, which generated much excitement 30 to 40 years ago,202 has not become commonplace, largely as a result of significant challenges related to fabrication, performance, and cost. Current hybrid organic/inorganic composites have significant prob-lems related mostly to their mechanical performance and their degradation in vivo.203,204 As a result, the use of synthetic composite materials as permanent replacements for bone is nearly nonexistent.202 To achieve dramatic improvements in the in vivo perfor-mance of composites for dental implants and skeletal tissue repair, new ways of approaching composite design and fabrication are needed. Ideally, these ma-terials would be capable of self-healing, as is the case for many biologic materials. In addition, teeth have a complex structure in which several tissues (enam-el, dentin, cementum, and pulp) with very different properties and structures are arranged. An ideal ar-tificial tooth requires the combination of several syn-thetic materials with prescribed properties. Will nano-technology alone be enough to achieve this goal?
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
36 Volume 26, Supplement, 2011
The tissues in teeth have very specific and sophis-ticated hierarchic architectures, with strength and toughening mechanisms built into almost every di-mension. The nanodimension is only one of them, but new technologies for the fabrication of materials need to be developed, with architectures designed on multiple scales that, from the mechanical point of view, will exhibit extrinsic toughening mechanisms similar to those observed in natural composites. Re-cent advances in the processing of bioinspired ma-terials may provide new possibilities. For example, a new technique, freezecasting, has been developed that can be used to fabricate ceramic-based compos-ites with complex architectures to assemble novel hi-erarchic structures modeled after natural composites such as bone or nacre that strike a balance between mechanical and functional responses205–210 (Fig 6).
This technique uses the controlled freezing of ceram-ic suspensions to generate porous ceramic scaffolds whose architecture is given a template by the ice crys-tals. By controlling the composition of the suspension and the freezing conditions, it is possible to generate materials with complex hierarchic architectures that mimic those of the inorganic component of nacre on multiple scales, from the nano to the macro level. Subsequently, these scaffolds can be infiltrated with a second “soft” phase (eg, polymer) to prepare com-posites that exhibit unique combinations of strength and toughness. In particular, it is possible to achieve fracture resistance that is up to 300 times greater (in terms of energy) than that of their main ceramic con-stituents. As with natural materials, these values are much higher than what could be expected using a simple mixture of their components.
IceIce
Ice
Entrapped ceramic particles
Temperaturegradient
Freezing direction
Colder
Cold[0001]
40 50 60 70 800
40
80
120
160
Literaturevalues
Com
pres
sive
str
engt
h (M
Pa)
Porosity (% by vol)
Freeze-castedlamellar HA
100 µm
250 µm
Ice front
Ice front
IceIce
Ice
Entrapped ceramic particles
Temperaturegradient
Freezing direction
Colder
Cold[0001]
40 50 60 70 800
40
80
120
160
Literaturevalues
Com
pres
sive
str
engt
h (M
Pa)
Porosity (% by vol)
Freeze-castedlamellar HA
100 µm
250 µm
Ice front
Ice front
IceIce
Ice
Entrapped ceramic particles
Temperaturegradient
Freezing direction
Colder
Cold[0001]
40 50 60 70 800
40
80
120
160
Literaturevalues
Com
pres
sive
str
engt
h (M
Pa)
Porosity (% by vol)
Freeze-castedlamellar HA
100 µm
250 µm
Ice front
Ice front
IceIce
Ice
Entrapped ceramic particles
Temperaturegradient
Freezing direction
Colder
Cold[0001]
40 50 60 70 800
40
80
120
160
Literaturevalues
Com
pres
sive
str
engt
h (M
Pa)
Porosity (% by vol)
Freeze-castedlamellar HA
100 µm
250 µm
Ice front
Ice front
Fig 6 Freezecasting, a technique that uses the microstructure of ice as a template for the architecture of ceramic scaffolds, can be used to produce porous lamellar materials that replicate the structure of the inorganic component of nacre on multiple scales.205,207,208,214 These materials can be much stronger than others with similar porosity described in the literature.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 37
One of the problems for the dental application of modern technical ceramics is the difficulty associat-ed with the fabrication of ceramic pieces with com-plex shapes while maintaining accurate dimensional control of features from the macro to the micro level and good material properties. For example, when fabricating porous alumina dental implants to favor bone ingrowth, it has been observed that the resid-ual unwanted surface microporosity adjacent to the gingival cuff results in an inflammatory reaction that prevents formation of an effective biologic seal and leads to clinical failure.211 The advent of the so-called solid free-form fabrication technologies or rapid pro-totyping technologies has provided the opportunity to produce custom-designed ceramic parts directly from a computer model with determined shapes and porosities (Fig 7).212–224 These techniques produce 3D objects with the assistance of computer-aided design data, as well as digital data produced by an imaging source such as computed tomography or magnetic resonance imaging, opening the door for the fabrica-tion of custom-designed implants or crowns. Other novel processing techniques such as injection mold-ing or gel-casting could provide similar degrees of control.
ASSESSiNG impLANT OSSEOiNTEGrATiON
A critical feature of implants intended for dental appli-cations is their ability to promote bone formation along their surfaces. By definition, these implants need to be embedded in bone to function. That function includes support for either single- or multiple-unit prostheses. The bone-implant interface then becomes critical in various ways—it must secure the implant while distrib-uting loads on the implant in such a way as to mini-mize osteolysis and implant loosening. Additionally, the interface should secure the implant quickly.
In vitro tests in simulated body fluid (SBF) are often used to assess the bioactivity of coatings and materi-als.225 SBF is a solution with an ionic content similar to that of human plasma. Materials that can precipitate apatite crystals on their surface during immersion in SBF are often considered bioactive and expected to bond to bone in vivo. However, more recent research has criticized the significance of this test and the pro-cedures used, as they seem to generate false-positive and false-negative results.226 In any case, in vitro tests in SBF seem to provide useful information on the chemi-cal reactions that can be expected at the biomaterial
V
x
250 µm
HA structure printedthrough a 200 µmnozzle
Ceramicink
Gelation of highly concentratedcolloidal suspensions (~45% to 50% by vol)
Dispersant Gelling agent PAA PEIpH~9
Fig 7 Solid free-form fabrication techniques that are precise and reproducible, such as direct inkjet printing, robotic-assisted deposition or robocasting (shown), and hot-melt printing—which usually involve “building” structures layer by layer following a com-puter design or data from sources such as magnetic resonance imaging—can be used to fabricate custom-designed scaffolds with complex architectures.212,215–224 PAA = ammonium polyacrylate; PEI = polyethylenimine.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
38 Volume 26, Supplement, 2011
surface in vivo and can be used in combination with mechanical testing to understand the mechanisms of failure. Tests in cell cultures are also routinely used to assess cytotoxicity and biocompatibility as well as the effect of the materials on cell differentiation, which will be determined by examining the expression of important osteoblastic markers. However, a lack of guidelines to correlate in vitro results with in vivo per-formance makes the use of animal models a require-ment to truly assess implant performance.227
Two in vivo models are commonly available for as-sessing osseointegration via osteoconduction, and each offers both advantages and disadvantages. The easier model to use is the calvarial onlay.228–230 It mini-mally traumatizes the animal; can be set up quickly; can be used in animals of many different sizes, from mice to dogs; and offers standardized data on osteo-conductive bone growth into the implant. The model typically involves operatively exposing the skull, re-moving or elevating the periosteum, and laying the implant directly on the bone surface. The implant can be secured to the bone, but this is usually unnecessary, since the pressure of the overlying skin helps prevent implant migration. The implant-bone interface can be analyzed fairly easily using histology. The procedure and the implant do not weaken the skull. Mechanical testing of the implant can be challenging, however, since it focuses on shear of inconveniently shaped structures. The main disadvantage of this model re-lates to cost: the limited size of the calvarium limits the number of implants that can be tested simultaneously.
The second model involves embedding plug-shaped implants into same-sized holes created in ei-ther the mandible or the long bones.231 Each plug is gently press-fitted into the newly created hole. As new bone grows at the interface with the implant, it binds the implant into place. The implant-bone interface can then be examined via histology and mechanical testing. Multiple implants can be placed in the same animal, although too many implants will weaken the bone and make fractures likely. This model more closely reproduces the typical clinical situation of placing implants directly into bone. However, the pro-cedure is more invasive than the onlay and requires greater technical skill for proper implant placement.
FuTurE TrENdS FOr dENTAL impLANTS
Despite conflicting reports regarding the effect of ce-ramic coatings, microtopography, and/or nanotopog-raphy on the osseointegration of dental implants, the prevailing philosophy is that these techniques may significantly enhance bone growth and attachment to
implant surfaces and ultimately improve the success of dental implants, allowing a rapid return to function (ie, mastication). There is an urgent need for more fun-damental research in this area that would combine both in vitro and in vivo studies and ultimately lead to appropriate clinical application. In the desire to create the perfect implant designed with nanomaterials and bioinspired approaches, key gaps in basic knowledge must be closed, and a series of prototype dental im-plants with increasing functionality must be created. This process should start with a recognition of the specific gaps in the present knowledge and then look broadly for advances that will enable bridging them. Specifically, researchers should seek to uncover the relationships linking composition and materials archi-tecture at scales of multiple lengths with macroscopic mechanical behavior and the capability for osteo-genesis. Eventually, these relationships must be test-ed and evaluated systematically in vivo and finally in clinical studies that maintain the same stringent anal-yses and outcome measures. Although fundamental interactions between biomaterials and surrounding tissues may be determined, a systematic approach must be established to confirm the relevance and consequence of these biologic responses. Once basic strategies are defined, the knowledge could be used to design new implant systems capable of manipulat-ing chemistry and cellular responses down to the mo-lecular level. With this powerful capability, implant designs can be patient-specific and customized to the biology of the patient. To reach this goal, several sci-entific questions must be answered:
• What is the optimum coating composition and thickness? Does it depend on a specific location and can it be manipulated based on the patient’s needs?
• What are the biodegradation rates of different coat-ing materials? Are they appropriate for their respec-tive applications based on load-bearing?
• Is it possible to design coatings with hierarchic archi-tectures that combine good mechanical behavior with an optimal biologic response?
• How do the surface topography and chemistry of dental implants control the cell response, particu-larly the differentiation of stem cells toward osteo-blastic lineages? Is there an ideal number or type of topographic features of dental implants that would provide optimal osseointegration?
• What are the best routes for the design, fabrication, and assembly of new synthetic materials that will mimic the properties of tooth tissue?
• Can a reliable protocol be developed to test the osseointegration and in vitro performance of artifi-cial teeth? How can results from in vitro and in vivo analyses of materials be correlated?
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 39
The answers to these questions will provide the information needed to design and engineer a variety of dental implants for treating a diverse population of patients. This will require the integration of inter-disciplinary principles drawn from materials science, biology, computational and quantitative science, and tissue engineering, coupled with surgical insight and implant-product data gathering through comprehen-sive data registries. This review has summarized some of the aspects in which nanotechnology can inter-vene in the design and fabrication of new scaffolds. Nanotechnology offers a new spectrum of possibili-ties by providing new tools for the manipulation and characterization of matter at very small dimensions. The goal is to build “active” implants and structures that will interact with their surroundings, respond to environmental changes, deliver appropriate mol-ecules or drugs, and actively direct cellular events. The vision for the future is to move beyond the re-placement of diseased tissues to in vivo repair and regeneration. The strategies thus developed should be amenable to translation into clinical therapies and treatments. To this end, the goal is to produce materi-als and therapies that will bring state-of-the-art tech-nology to the bedside, improve quality of life, and adapt to a patient’s specific needs.
ACKNOwLEdGmENT
This work was supported by the National Institutes of Health (NIH/NIDCR) under grant No. 5R01 DE015633.
rEFErENCES
1. Worthington P. Introduction: History of implants. In: Worthing-ton P, Lang BR, Rubenstein JE (eds). Osseointegration in Dentistry: An Overview. Chicago: Quintessence, 2003: 2.
2. Branemark PI, Adell R, Breine U, Hansson BO, Lindstrom J, Ohlsson A. Intraosseous anchorage of dental prostheses. I. Ex-perimental studies. Scand J Plast Reconstr Surg 1969;3:81 –100.
3. Linder L, Albrektsson T, Branemark PI, et al. Electron-micro-scopic analysis of the bone titanium interface. Acta Orthop Scand 1983;54:45–52.
4. Hobo S, Ichida E, Garcia L. Osseointegration Implant Systems. In: Hobo S, Icida E, Garcia L (eds). Osseointegration and Oc-clusal Rehabilitation. Tokyo: Quintessence, 1990:3–4.
5. Schulte KR, Callaghan JJ, Kelley SS, Johnston RC. The outcome of charnley total hip-arthroplasty with cement after a minimum 20-year follow-up. J Bone Joint Surg [Am] 1993;75:961–975.
6. Ratner BD. Biomaterials Science: An Introduction to Materials in Medicine, ed 2. Amsterdam: Elsevier, 2004:xii, 851.
7. Shackelford JF. Bioceramics. Abingdon, UK: Taylor & Francis, 1999:82.
8. Schein H. Henry Schein enters growing dental implant cat-egory through strategic partnership with Camlog. Business Wire. July 6, 2004.
9. Meier B. Absence of warranties for implants costs health system. The New York Times. April 2, 2010.
10. Pye AD, Lockhart DE, Dawson MP, Murray CA, Smith AJ. A review of dental implants and infection. J Hosp Infect 2009; 72:104–110.
11. Christenson EM, Anseth KS, van den Beucken LJ, et al. Nano-biomaterial applications in orthopedics. J Orthop Res 2007; 25:11–22.
12. Coelho PG, Granjeiro JM, Romanos GE, et al. Basic research methods and current trends of dental implant surfaces. J Biomed Mater Res B Appl Biomater 2009;88:579–596.
13. Boyan BD, Lohmann CH, Dean DD, Sylvia VL, Cochran DL, Schwartz Z. Mechanisms involved in osteoblast response to im-plant surface morphology. Ann Rev Mater Res 2001;31:357–371.
14. Kasemo B. Biological surface science. Surf Sci 2002;500:656–677.15. Hench LL. Bioceramics [review]. J Am Ceram Soc 1998;81:
1705–1728.16. Hench LL, Andersson Ö. Bioactive glasses. In: Hench LL, Wilson
J (eds). An Introduction to Bioceramics. Singapore: World Scientific, 1993:41–62.
17. Hench LL, Xynos ID, Polak JM. Bioactive glasses for in situ tis-sue regeneration [review]. J Biomat Sci 2004;15:543 –562.
18. McMurry J, Castellion ME. Fundamentals of general, organic and biological chemistry, ed 3. Upper Saddle River, New Jersey: Prentice Hall, 1999:786.
19. Geesink RG. Osteoconductive coatings for total joint arthro-plasty. Clin Orthop Relat Res 2002(395):53–65.
20. Cook SD, Thomas KA, Kay JF, Jarcho M. Hydroxyapatite-coated titanium for orthopedic implant applications. Clin Orthop Relat Res 1988;140:225–243.
21. Hayashi K, Matsuguchi N, Uenoyama K, Kanemaru T, Sugioka Y. Evaluation of metal implants coated with several types of ce-ramics as biomaterials. J Biomed Mater Res 1989;23:1247–1259.
22. Søballe K, Hansen ES, Brockstedt-Rasmussen H, Pedersen CM, Bünger C. Hydroxyapatite coating enhances fixation of porous coated implants. A comparison in dogs between press fit and noninterference fit. Acta Orthop Scand 1990;61:299–306.
23. Dhert WJ, Klein CP, Wolke JG, van der Velde EA, de Groot K, Rozing PM. A mechanical investigation of fluorapatite, magnesiumwhitlockite, and hydroxylapatite plasma-sprayed coatings in goats. J Biomed Mater Res 1991;25:1183–1200.
24. Klein CP, Patka P, van der Lubbe HB, Wolke JG, de Groot K. Plasma-sprayed coatings of tetracalciumphosphate, hydroxyl-apatite, and alpha-TCP on titanium alloy: An interface study. J Biomed Mater Res 1991;25:53–65.
25. Wang BC, Lee TM, Chang E, Yang CY. The shear strength and the failure mode of plasma-sprayed hydroxyapatite coating to bone: The effect of coating thickness. J Biomed Mater Res 1993;27:1315–1327.
26. Yang CY, Wang BC, Chang WJ, Chang E, Wu JD. Mechanical and histological evaluations of cobalt-chromium alloy and hydroxyapatite plasma-sprayed coatings in bone. J Mater Sci 1996;7:167–174.
27. Wheeler DL, Montfort MJ, McLoughlin SW. Differential healing response of bone adjacent to porous implants coated with hydroxyapatite and 45S5 bioactive glass. J Biomed Mater Res 2001;55:603–612.
28. Buser D, Schenk RK, Steinemann S, Fiorellini JP, Fox CH, Stich H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs [see comments]. J Biomed Mater Res 1991;25:889–902.
29. Caulier H, van der Waerden JP, Wolke JG, Kalk W, Naert I, Jansen JA. A histological and histomorphometrical evalua-tion of the application of screw-designed calciumphosphate (Ca-P)-coated implants in the cancellous maxillary bone of the goat. J Biomed Mater Res 1997;35:19–30.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
40 Volume 26, Supplement, 2011
30. Dalcusi G, LeGeros RZ, Deudon C. Scanning and transmis-sion electron microscopy and electron probe analysis of the interface between implants and host bone. Scanning Microsc 1990;4:309–314.
31. Denissen HW, Klein CP, Visch LL, Vandenhooff A. Behavior of calcium phosphate coatings with different chemistries in bone. Int J Prosthodont 1996;9:142–148.
32. Dhert WJ, Klein CP, Jansen JA, et al. A histological and histo-morphometrical investigation of fluorapatite, magnesium-whitlockite, and hydroxylapatite plasma-sprayed coatings in goats. J Biomed Mater Res 1993;27:127–138.
33. Gottlander M, Johansson CB, Albrektsson T. Short- and long-term animal studies with a plasma-sprayed calcium phos-phate-coated implant. Clin Oral Implants Res 1997;8:345–351.
34. Jansen JA, van der Waerden JP, Wolke JG. Histologic investiga-tion of the biologic behavior of different hydroxyapatite plasma-sprayed coatings in rabbits. J Biomed Mater Res 1993; 27:603–610.
35. Spivak JM, Blumenthal NC, Ricci JL, Alexander H. A new canine model to evaluate the biological effects of implant materi-als and surface coatings on intramedullary bone ingrowth. Biomaterials 1990;11:79–82.
36. Vercaigne S, Wolke JG, Naert I, Jansen JA. Histomorphometri-cal and mechanical evaluation of titanium plasma-spray-coated implants placed in the cortical bone of goats. J Biomed Mater Res 1998;41:41–48.
37. Radin SR, Ducheyne P. Plasma spraying changes of calcium phosphate ceramic characteristics and the effect on in vitro stability. J Mater Sci Mater Med 1992;3:33–42.
38. Ducheyne P, Beight J, Cuckler J, Evans B, Radin S. Effect of calcium phosphate coating characteristics on early post-operative bone tissue ingrowth. Biomaterials 1990;11:531–540.
39. Cook SD, Thomas KA, Dalton JE, Volkman TK, Whitecloud TS 3rd, Kay JF. Hydroxylapatite coating of porous implants improves bone ingrowth and interface attachment strength. J Biomed Mater Res 1992;26:989–1001.
40. Ducheyne P, Hench LL, Kagan AD, Martens M, Bursens A, Mulier JC. Effect of hydroxyapatite impregnation on skeletal bonding of porous coated implants. J Biomed Mater Res 1980; 14:225–237.
41. Ducheyne P, Cuckler JM. Bioactive ceramic prosthetic coat-ings. Clin Orthop Relat Res 1992;39:102–114.
42. Ducheyne P, Healy KE. The effect of plasma-sprayed calcium phosphate ceramic coatings on the metal ion release from porous titanium and cobalt-chromium alloys. J Biomed Mater Res 1988;22:1137–1163.
43. Sousa SR, Barbosa MA. Effect of hydroxyapatite thickness on metal ion release from Ti6Al4V substrates. Biomaterials 1996;17:397–404.
44. Camazzola D, Hammond T, Gandhi R, Davey JR. A randomized trial of hydroxyapatite-coated femoral stems in total hip ar-throplasty. A 13-year follow-up. J Arthroplasty 2009;24:33–37.
45. Gandhi R, Davey JR, Mahomed NN. Hydroxyapatite coated femoral stems in primary total hip arthroplasty. A meta-analy-sis. J Arthroplasty 2009;24:38–42.
46. Stilling M, Rahbek O, Soballe K. Inferior survival of hydroxy-apatite versus titanium-coated cups at 15 years. Clin Orthop Relat Res 2009;467:2872–2879.
47. Yang Y, Bessho K, Kim K-H, Park S-W, Ong JL. Hydroxyapa-tite coatings In: Wnek GE, Bowlin GL (eds). Encyclopedia of Biomaterials and Biomedical Engineering. New York: Informa Healthcare USA, 2008:1464–1469.
48. de Groot K. Medical applications of calciumphosphate bio-ceramics. The Centennial Memorial Issue. Ceram Soc Jpn 1991; 99:943–953.
49. Filiaggi M, Pilliar R, Coombs N. Post-plasma spraying heat treat-ment of the HA coating/Ti-6Al-4V implant system. J Biomed Mater Res, 1993;27:191–198.
50. Whitehead RY, Lacefield WR, Lucas LC. Structure and integrity of a plasma sprayed hydroxylapatite coating on titanium. J Biomed Mater Res 1993;27:1501–1507.
51. Whitehead RY, Lucas LC, Lacefield WR. The effect of dissolu-tion on plasma sprayed hydroxylapatite coatings on titanium. Clin Mater 1993;12:31–39.
52. Beltz GE, Rice JR, Shih CF, Xia L. A self-consistent model for cleavage in the presence of plastic flow. Acta Materialia 1996; 44:3943–3954.
53. Duffy DM, Harding JH, Stoneham AM. A calculation of the structure and energy of the Nb/Al/sub 2/O/sub 3/ interface. Acta Materialia 1996;44:3293–3298.
54. Finnis MW. The theory of metal-ceramic interfaces. J Physics Condensed Matter 1996;8:5811–5836.
55. Gutekunst G, Mayer J, Ruhle M. Atomic structure of epitaxial Nb-Al2O3 interfaces I. Coherent regions. Philosoph Mag A Physics Condensed Matter Struct Defects Mech Prop 1997;75: 1329–1355.
56. Hong T, Smith JR, Srolovitz DJ. Theory of metal-ceramic adhe-sion. Acta Metallurgica Mater 1995;43:2721–2730.
57. Hutchinson JW, Suo Z. Mixed mode cracking in layered mate-rials. Adv Appl Mechan 1992;29:63–191.
58. Saiz E, Cannon RM, Tomsia AP. Energetics and atomic trans-port at liquid metal/Al2O3 interfaces. Acta Mater 1999;47: 4209–4220.
59. Suo Z, Hutchinson JW. Sandwich test specimens for measur-ing interface crack toughness. Mater Sci Eng 1989;107:135–143.
60. Suresh S, Mortensen A. Functionally graded metals and metal-ceramic composites. 2. Thermomechanical behaviour. Int Mater Rev 1997;42:85–116.
61. Tomsia AP, Pask JA, Loehman RE. Glass/metal and glass-ceramic/metal seals. In: Engineered Materials Handbook. Materials Park, OH: ASM International, 1991:493–501.
62. Tomsia A, Saiz E, Foppiano S, Cannon R. Reactive wetting: Ridging, adsorption and compound formation. In: Eustatho-poulos N, Sobczak N (eds). High Temperature Capillarity. Kracow, Poland: Foundry Research Institute, 1988:59–80.
63. Tvergaard V, Hutchinson JW. Toughness of an interface along a thin ductile layer joining elastic solids. Philosop Mag A 1994; 70:641–656.
64. Hosseini M, Sodek J, Franke R-P, Davies J. The structure and composition of the bone-implant interface. In: Davies JE (ed). Bone Engineering. Toronto: Em Squared Incorporated, 2000:295–304.
65. Porter AE, Botelho CM, Lopes MA, Santos JD, Best SM, Bonfield W. Ultrastructural comparison of dissolution and apatite pre-cipitation on hydroxyapatite and silicon-substituted hydroxy-apatite in vitro and in vivo. J Biomed Mater Res A 2004;69: 670–679.
66. Porter AE, Hobbs LW, Rosen VB, Spector M. The ultrastructure of the plasma-sprayed hydroxyapatite-bone interface predis-posing to bone bonding. Biomaterials 2002;23:725–733.
67. Hench LL. Biomaterials: A forecast for the future. Biomaterials 1998;19:1419–1423.
68. Bagambisa F, Joos U, Schilli W. Mechanisms and structure of the bond between bone and hydroxyapatite ceramics. J Biomed Mater Res 1993;27:1047–1055.
69. Klein CP, Wolke JG, de Groot K. Stability of calcium phosphate ceramics and plasma spray coating. In: Hench LL, Wilson J (eds). An Introduction to Bioceramics. Singapore: World Scien-tific, 1998:199–221.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 41
70. Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lap-pinscott HM. Microbial biofilms [review]. Ann Rev Microbiol 1995;49:711–745.
71. Lincoff AM, Topol EJ, Ellis SG. Local drug delivery for the prevention of restenosis: Fact, fancy, and future [review]. Circulation 1994;90:2070–2084.
72. Riessen R, Isner JM. Prospects for site-specific delivery of phar-macologic and molecular therapies [review]. J Am Coll Cardiol 1994;23: 1234–1244.
73. Camenzind E, Bakker WH, Reijs A, et al. Site-specific intravas-cular administration of drugs. History of a method applicable in humans. Cathet Cardiovasc Diagn 1997;41:342–347.
74. Lambert CR, Camenzind E, Robinson K. Local drug delivery. Cathet Cardiovasc Diagn 1997;41:231.
75. Frenkel SR, Simon J, Alexander H, Dennis M, Ricci JL. Osseo-integration on metallic implant surfaces: Effects of microge-ometry and growth factor treatment. J Biomed Mater Res 2002;63:706–713.
76. Hunziker EB, Rosenberg LC. Repair of partial-thickness defects in articular cartilage: Cell recruitment from the synovial mem-brane. J Bone Joint Surg [Am] 1996; 78:721–733.
77. Tisdel CL, Goldberg VM, Parr JA, Bensusan JS, Staikoff LS, Ste-venson S. The influence of a hydroxyapatite and tricalcium-phosphate coating on bone growth into titanium fiber-metal implants. J Bone Joint Surg [Am] 1994;76:159–171.
78. Ducheyne P, Healy K. Bioceramics. In: Bioceramics: Proceed-ings of the First International Bioceramics Symposium. Kyoto, Japan: Ishiyaku EuroAmerica, 1988.
79. Chae JC, Collier JP, Mayor MB, Surprenant VA, Dauphinais LA. Enhanced ingrowth of porous-coated CoCr implants plasma-sprayed with tricalcium phosphate. J Biomed Mater Res 1992; 26:93–102.
80. Soballe K, Overgaard S, Hansen ES, Brokstedt-Rasmussen H, Lind M, Bunger C. A review of ceramic coatings for implant fixation. J Long-Term Effects Med Implants 1999;9:131–151.
81. Wheeler DL, Campbell AA, Graff GL, Miller GJ. Histological and biomechanical evaluation of calcium phosphate coatings applied through surface-induced mineralization to porous titanium implants. J Biomed Mater Res 1997;34:539 –543.
82. Willmann G. Coating of implants with hydroxyapatite material connections between bone and metal [review]. Adv Eng Mat 1999;1:95–105.
83. Knowles JC, Gross K, Berndt CC, Bonfield W. Structural changes of thermally sprayed hydroxyapatite investigated by Rietveld analysis. Biomaterials 1996;17:639–645.
84. McPherson R, Gane N, Bastow TJ. Structural characterization of plasma sprayed hydroxylapatite coatings. J Mater Sci Mater Med 1995;6:327–334.
85. Frayssinet P, Tourenne F, Primout I, et al. A study of structure and degradation of nonpolymeric biomaterials implanted in bone using reflected and transmitted light microscopy. Biotech Histochem 1993;68:333 –341.
86. Huaxia J, Ponton C, Marquis P. Microstructural characteriza-tion of hydroxyapatite coating on titanium. J Mater Sci Mater Med 1992;3:283–287.
87. Weinlaender M, Beumer J, Kenney EB, Moy PK, Adar F. Raman microprobe investigation of the calcium phosphate phases of three commercially available plasma-flame-sprayed hydroxyapatite-coated dental implants. J Mater Sci Mater Med 1992;3:397–340.
88. Zyman Z, Weng J, Liu X, Li X, Zhang X. Phase and structural changes in hydroxyapatite coatings under heat treatment. Biomaterials 1994;15:151–155.
89. Gross KA, Berndt CC, Goldschlag DD, Iacono VJ. In vitro changes of hydroxyapatite coatings. Int J Oral Maxillofac Implants 1997;12:589–597.
90. Hench LL. Bioceramics: From concept to clinic. J Am Ceram Soc 1991;74:1487–1510.
91. Lacefield W. Hydroxylapatite coatings. In: Hench LL, Wilson J (ed). An Introduction to Bioceramics. Singapore: World Scien-tific, 1993:223–238.
92. Bloebaum RD, Beeks D, Dorr LD, Savory CG, DuPont JA, Hofmann AA. Complications with hydroxyapatite particulate separation in total hip arthroplasty. Clin Orthop Relat Res 1994;15:19 –26.
93. Gross KA, Babovic M. Influence of abrasion on the surface characteristics of thermally sprayed hydroxyapatite coatings. Biomaterials 2002;23:4731–4737.
94. Gross KA, Berndt CC, Iacono VJ. Variability of hydroxyapatite-coated dental implants. Int J Oral Maxillofac Implants 1998;13: 601–610.
95. Jarcho M. Retrospective analysis of hydroxyapatite develop-ment for oral implant applications. Dental Clin North Am 1992;36:19–26.
96. Lewandowski JA, Johnson CM. Structural failure of osseointe-grated implants at the time of restoration. A clinical report. J Prosthet Dent 1989;62:127–129.
97. Overgaard S, Lind M, Josephsen K, Maunsbach AB, Bünger C, Søballe K. Resorption of hydroxyapatite and fluorapatite ceramic coatings on weight-bearing implants: A quantita-tive and morphological study in dogs. J Biomed Mater Res 1998;39:141–152.
98. Park E, Condrate RA, Hoelzer DT, Fishman GS. Interfacial char-acterization of plasma-sprayed coated calcium phosphate on Ti-6Al-4V. J Mater Sci Mater Med 1998;9:643–649.
99. Yamamuro T, Hench LL, Wilson J. Calcium phosphate and hydroxylapatite ceramics. In: Yamamuro T, Hench LL, Wilson J (eds). Handbook of Bioactive Ceramics, vol II. Boca Raton, FL: CRC Press, 1990.
100. Koeneman J, Lemons J, Ducheyne P, et al. Workshop on char-acterization of calcium phosphate materials. J Appl Biomateri-als 1990;1:79–90.
101. Gross KA, Gross V, Berndt CC. Thermal analysis of amorphous phases in hydroxyapatite coating. J Am Ceram Soc 1998;81: 106–112.
102. Suk-Woo H, Reber R, Eckert KL, et al. Chemical and morpho-logical changes of vacuum-plasma-sprayed hydroxyapatite coatings during immersion in simulated physiological solu-tions. J Am Ceram Soc 1998;81:81–88.
103. Chen TS, Lacefield WR. Crystallization of ion beam deposited calcium phosphate coatings. J Mater Res 1994;9:1284–1290.
104. Wang BC, Chang E, Lee TM, Yang CY. Changes in phases and crystallinity of plasma-sprayed hydroxyapatite coatings under heat treatment: A quantitative study. J Biomed Mater Res 1995;29:1483–1492.
105. Chen J, Tong W, Cao Y, Feng J, Zhang X. Effect of atmosphere on phase transformation in plasma-sprayed hydroxyapatite coatings during heat treatment. J Biomed Mater Res 1997; 34:15–20.
106. Shirkhanzadeh M, Azadegan M, Stack V, Schreyer S. Fabrica-tion of pure hydroxyapatite and fluoridated-hydroxyapatite coatings by electrocrystallisation. Mater Lett 1994;18:211–214.
107. Tong W, Chen J, Cao Y, Lu L, Feng J, Zhang X. Effect of water vapor pressure and temperature on the amorphous-to-crys-talline HA conversion during heat treatment of HA coatings. J Biomed Mater Res 1997;36:242–245.
108. Wen HB, de Wijn JR, Cui FZ, de Groot K. Preparation of calcium phosphate coatings on titanium implant materials by simple chemistry. J Biomed Mater Res 1998;41:227–236.
109. Koch B, Wolke JG, de Groot K. X-ray diffraction studies on plasma-sprayed calcium phosphate-coated implants. J Biomed Mater Res 1990;24:655–667.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
42 Volume 26, Supplement, 2011
110. Ogiso M, Yamashita Y, Matsumoto T. Differences in microstruc-tural characteristics of dense HA and HA coating. J Biomed Mater Res 1998;41:296–303.
111. Radin S, Ducheyne P, Falaize S, Hammond A. In vitro transfor-mation of bioactive glass granules into Ca-P shells. J Biomed Mater Res 2000;49:264–272.
112. Evans SL, Gregson PJ. The effect of a plasma-sprayed hydroxy-apatite coating on the fatigue properties of Ti-6Al-4V. Mater Lett 1993;16:270–274.
113. Lusquinos F, De Carlos A, Pou J, et al. Calcium phosphate coat-ings obtained by Nd : YAG laser cladding: Physicochemical and biologic properties. J Biomedi Mater Res A 2003;64:630–637.
114. Lusquinos F, Pou J, Arias JL, et al. Production of calcium phosphate coatings on Ti6Al4V obtained by Nd : yttrium-alu-minum-garnet laser cladding. J Appl Phys 2001;90:4231–4236.
115. Antonov EN, Bagratashvili VN, Popov VK, et al. Biocompatibili-ty of laser-deposited hydroxyapatite coatings on titanium and polymer implant materials. J Biomed Optics 1998;3:423–428.
116. Bibby JK, Mummery PM, Bubb N, Wood DJ. Novel bioactive coatings for biomedical applications deposited by electro-phoretic deposition. Glass Technol 2004;45:80–83.
117. Bouyer E, Gitzhofer F, Boulos MI. The suspension plasma spraying of bioceramics by induction plasma. J Miner Metals Mater Soc 1997;49:58–62.
118. Chai CS, Gross KA, Ben-Nissan B. Critical ageing of hydroxy-apatite sol-gel solutions. Biomaterials 1998;19:2291–2296.
119. Cheng XL, Filiaggi M, Roscoe SG. Electrochemically assisted co-precipitation of protein with calcium phosphate coatings on titanium alloy. Biomaterials 2004;25:5395–5403.
120. Cleries L, Fernandezpradas JM, Sardin G, Morenza JL. Dissolu-tion behaviour of calcium phosphate coatings obtained by laser ablation. Biomaterials 1998;19:1483–1487.
121. Guipont V, Espanol M, Borit F, et al. High-pressure plasma spraying of hydroxyapatite powders. Mater Sci Eng A Struct Mater Prop Microstruct Process 2002;325:9–18.
122. Habibovic P, Barrere F, van Blitterswijk CA, de Groot K, Layrolle P. Biomimetic hydroxyapatite coating on metal implants. J Am Ceram Soc 2002;85:517–522.
123. Haddow DB, James PF, Van Noort R. Sol-gel derived calcium phosphate coatings for biomedical applications. J Sol-Gel Sci Technol 1998;13:261–265.
124. Hamdi M, Ide-Ektessabi A. Preparation of hydroxyapatite layer by ion beam assisted simultaneous vapor deposition. Surf Coatings Technol 2003;163:362–367.
125. Li H, Khor KA, Kumar R, Cheang P. Characterization of hydroxy-apatite/nano-zirconia composite coatings deposited by high velocity oxy-fuel (HVOF) spray process. Surf Coatings Technol 2004;182:227–236.
126. Lin SJ, LeGeros RZ, LeGeros JP. Adherent octacalciumphos-phate coating on titanium alloy using modulated electro-chemical deposition method. J Biomed Mater Res A 2003;66: 819–828.
127. Lucas LC, Lacefield WR, Ong JL, Whitehead RY. Calcium phos-phate coatings for medical and dental implants. Colloids Surf A Physicochem Eng Aspects 1993;77:141–147.
128. Mondragon-Cortez P, Vargas-Gutierrez G. Electrophoretic deposition of hydroxyapatite submicron particles at high volt-ages. Mater Lett 2004;58:1336–1339.
129. Redepenning J, Venkataraman G, Chen J, Stafford N. Electro-chemical preparation of chitosan/hydroxyapatite composite coatings on titanium substrates. J Biomed Mater Res A 2003; 66:411–416.
130. Song CL, Weng WJ, Cheng K, et al. Sol-gel preparation and preliminary in vitro evaluation of fluorapatite/hydroxyapatite solid solution films. J Mater Sci Technol 2003;19:495 –498.
131. Zhitomirsky I. Electrophoretic hydroxyapatite coatings and fibers. Mater Lett 2000;42:262–271.
132. Lotfibakhshaiesh N, Brauer DS, Hill RG. Bioactive glass engi-neered coatings for Ti6Al4V alloys: Influence of strontium sub-stitution for calcium on sintering behaviour. J Non-Crystalline Solids 2010;356:2583–2590.
133. Liste S, Gonzalez P, Serra J, et al. Study of the stoichiometry transfer in pulsed laser deposition of bioactive silica-based glasses. Thin Solid Films 2004;453–454:219–223.
134. Mardare CC, Mardare AI, Fernandes JRF, et al. Deposition of bioactive glass-ceramic thin-films by RF magnetron sputter-ing. J Eur Ceram Soc 2003;23:1027–1030.
135. Galliano P, De Damborenea JJ, Pascual MJ, Duran A. Sol-gel coatings on 316L steel for clinical applications. J Sol-Gel Sci Technol 1998;13:723–727.
136. Gomez-Vega JM, Saiz E, Tomsia AP, Marshall GW, Marshall SJ (eds). A multilayer approach to fabricate bioactive glass coatings on Ti alloys. In: Valentini R (ed). Biomedical Materials for Drug Delivery, Medical Implants and Tissue Engineering, MRS Proceedings, vol 550. Pittsburg, PA: Materials Research Society, 1999.
137. Lopez-Esteban S, Gutierrez-Gonzalez CF, Gremillard L, Saiz E, Tomsia AP. Interfaces in graded coatings on titanium-based implants. J Biomed Mater Res A 2009;88:1010–1021.
138. Saiz E, Goldman M, Gomez-Vega JM, Tomsia AP, Marshall GW, Marshall SJ. In vitro behavior of silicate glass coatings on Ti6Al4V. Biomaterials 2002;23:3749–3756.
139. Schausten MC, Meng DC, Telle R, Boccaccini AR. Electropho-retic deposition of carbon nanotubes and bioactive glass particles for bioactive composite coatings. Ceram Int 2010;36: 307–312.
140. Zhitomirsky D, Roether JA, Boccaccini AR, Zhitomirsky I. Electro-phoretic deposition of bioactive glass/polymer composite coat-ings with and without HA nanoparticle inclusions for biomedical applications. J Mater Process Technol 2009;209:1853–1860.
141. Tomsia AP, Saiz E, Song J, Bertozzi CR. Biomimetic bonelike composites and novel bioactive glass coatings. Adv Eng Mater 2005;7:999–1004.
142. Lopez-Esteban S, Saiz E, Fujino S, Oku T, Suganuma K, Tomsia AP. Bioactive glass coatings for orthopedic metallic implants. J Eur Ceram Soc 2003;23:2921–2930.
143. Varanasi VG, Saiz E, Loomer PM, et al. Enhanced osteocalcin expression by osteoblast-like cells (MC3T3-E1) exposed to bio-active coating glass (SiO2-CaO-P2O5-MgO-K2O-Na2O system) ions. Acta Biomater 2009;5:3536–3547.
144. Hench LL. Genetic design of bioactive glass. J Eur Ceram Soc 2009;29:1257–1265.
145. Christodoulou I, Buttery LDK, Saravanapavan P, Tai GP, Hench LL, Polak JM. Dose- and time-dependent effect of bioac-tive gel-glass ionic-dissolution products on human fetal osteoblast-specific gene expression. J Biomed Mater Res B Appl Biomater 2005;74:529–537.
146. Xynos ID, Edgar AJ, Buttery LDK, Hench LL, Polak JM. Gene-expression profiling of human osteoblasts following treat-ment with the ionic products of Bioglass (R) 45S5 dissolution. J Biomed Mater Res 2001;55:151–157.
147. Sepulveda P, Jones JR, Hench LL. Bioactive sol-gel foams for tissue repair. J Biomed Mater Res 2002;59:340–348.
148. Foppiano S, Marshall SJ, Marshall GW, Saiz E, Tomsia AP. Bioac-tive glass coatings affect the behavior of osteoblast-like cells. Acta Biomater 2007;3:765–771.
149. Le Guehennec L, Soueidan A, Layrolle P, Amouriq Y. Surface treatments of titanium dental implants for rapid osseointegra-tion. Dent Mater 2007;23:844–854.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Tomsia et al
The International Journal of Oral & Maxillofacial Implants 43
150. Frauchiger VM, Schlottig F, Gasser B, Textor M. Anodic plasma-chemical treatment of CP titanium surfaces for biomedical applications. Biomaterials 2004;25:593–606.
151. Boyd IW. Thin film growth by pulsed laser deposition [review]. Ceram Inter 1996;22:429–434.
152. Chrisey DB, Pique A, McGill RA, J.S. et al. Laser deposition of polymer and biomaterial films [review]. Chem Rev 2003;103: 553–576.
153. Shin H, Jo S, Mikos AG. Biomimetic materials for tissue engi-neering. Biomaterials 2003;24:4353–4364.
154. Shin HY, Bizios R, Gerritsen ME. Cyclic pressure modulates endothelial barrier function. Endothelium 2003;10:179–187.
155. Davis DH, Giannoulis CS, Johnson RW, Desai TA. Immobiliza-tion of RGD to < 111 > silicon surfaces for enhanced cell adhe-sion and proliferation. Biomaterials 2002;23:4019–4027.
156. Massia SP, Hubbell JA. Covalent surface immobilization of Arg-Gly-Asp-containing and Tyr-Ile-Gly-Ser-Arg-containing peptides to obtain well-defined cell-adhesive substrates. Anal Biochem 1990;187:292–301.
157. Beutner R, Michael J, Schwenzer B, Scharnweber D. Biologi-cal nano-functionalization of titanium-based biomaterial surfaces: A flexible toolbox. J R Soc Interface 2010;7:S93–S105.
158. Schliephake H, Scharnweber D. Chemical and biological func-tionalization of titanium for dental implants. J Mater Chem 2008;18:2404–2414.
159. Schliephake H, Scharnweber D, Dard M, Sewing A, Aref A, Roessler S. Functionalization of dental implant surfaces using adhesion molecules. J Biomed Mater Res B-Appl Biomater 2005;73:88 –96.
160. Jose B, Antoci V, Zeiger AR, Wickstrom E, Hickok NJ. Vancomy-cin covalently bonded to titanium beads kills Staphylococcus aureus. Chem Biol 2005;12:1041–1048.
161. Lange K, Herold M, Scheideler L, Geis-Gerstorfer J, Wendel HP, Gauglitz G. Investigation of initial pellicle formation on modified titanium dioxide (TiO2) surfaces by reflectometric interference spectroscopy (RIfS) in a model system. Dent Mater 2004;20:814–822.
162. Becker J, Kirsch A, Schwarz F, et al. Bone apposition to titanium implants biocoated with recombinant human bone morphogenetic protein 2 (rhBMP-2). A pilot study in dogs. Clin Oral Investig 2006;10:225–225.
163. Arnold M, Cavalcanti-Adam EA, Glass R, et al. Activation of integrin function by nanopatterned adhesive interfaces. Chemphyschem 2004;5:383 –388.
164. Cavalcanti-Adam EA, Micoulet A, Blummel J, Auernheimer J, Kessler H, Spatz JP. Lateral spacing of integrin ligands influ-ences cell spreading and focal adhesion assembly. Eur J Cell Biol 2006;85:219–224.
165. Healy K, Harbers G, Barber T, Sumner D. Osteoblast inter-actions with engineered surfaces. In: Davies JE (ed). Bone Engineering. Toronto: Em Squared, 2000:268–281.
166. Boyan B, Schwartz Z. Modulation of osteogenesis via implant surface design. In: Davies JE (ed). Bone Engineering. Toronto: Em Squared, 2000:232–239.
167. Lemons J. Structure of bone adjacent to different dental implants. In: Davies JE (ed). Bone Engineering. Toronto: Em Squared, 2000:313–320.
168. Ricci JL, Charvet J, Frenkel SR, et al. Bone response to laser microtextured surfaces. In: Davies JE (ed). Bone Engineering. Toronto: Em Squared, 2000:282–294.
169. Kieswetter K, Schwartz Z, Hummert TW, et al. Surface rough-ness modulates the local production of growth factors and cytokines by osteoblast-like MG-63 cells. J Biomed Mater Res 1996;32:55–63.
170. Schwartz Z, Martin JY, Dean DD, Simpson J, Cochran DL, Boyan BD. Effect of titanium surface roughness on chondrocyte prolif-eration, matrix production, and differentiation depends on the state of cell maturation. J Biomed Mater Res 1996;30:145–155.
171. Zinger O, Zhao G, Schwartz Z, et al. Differential regulation of osteoblasts by substrate microstructural features. Biomaterials 2005;26:1837–1847.
172. Deporter D. Dental implant design and optimal treatment out-comes. Int J Periodontics Restorative Dent 2009;29:625–633.
173. Jayaraman M, Meyer U, Buhner M, Joos U, Wiesmann HP. Influ-ence of titanium surfaces on attachment of osteoblast-like cells in vitro. Biomaterials 2004;25:625–631.
174. Kunzler TP, Drobek T, Schuler M, Spencer ND. Systematic study of osteoblast and fibroblast response to roughness by means of surface-morphology gradients. Biomaterials 2007;28:2175–2182.
175. Simmons CA, Valiquette N, Pilliar RM. Osseointegration of sintered porous-surfaced and plasma spray-coated implants: An animal model study of early postimplantation healing response and mechanical stability. J Biomed Mater Res 1999; 47:127–138.
176. Walboomers XF, Jansen JA. Cell and tissue behavior on micro-grooved surfaces. Odontology 2001;89:2–11.
177. Gahlert M, Rohling S, Wieland M, Sprecher CM, Kniha H, Milz S. Osseointegration of zirconia and titanium dental implants: A histological and histomorphometrical study in the maxilla of pigs. Clin Oral Implant Res 2009;20:1247–1253.
178. Wenzel RN. Surface roughness and contact angle. J Phys Chem 1949;53:1466–1467.
179. Elias CN, Oshida Y, Lima JHC, Muller CA. Relationship between surface properties (roughness, wettability and morphology) of titanium and dental implant removal torque. J Mech Behav Biomed Mater 2008;1:234–242.
180. Ivanoff CJ, Hallgren C, Widmark G, Sennerby L, Wennerberg A. Histologic evaluation of the bone integration of TiO2 blasted and turned titanium microimplants in humans. Clin Oral Implant Res 2001;12:128–134.
181. Albrektsson T, Johansson C. Osteoinduction, osteoconduction and osseointegration. Eur Spine J 2001;10:S96–S101.
182. Quere D. Surface chemistry: Fakir droplets. Nat Mater 2002;1: 14–15.
183. Dalby MJ, Gadegaard N, Tare R, et al. The control of human mesenchymal cell differentiation using nanoscale symmetry and disorder. Nat Mater 2007;6:997–1003.
184. Yang JY, Ting YC, Lai JY, Liu HL, Fang HW, Tsai WB. Quantitative analysis of osteoblast-like cells (MG63) morphology on nano-grooved substrata with various groove and ridge dimensions. J Biomed Mater Res A 2009;90:629–640.
185. Li Y, Wong C, Xiong J, Hodgson P, Wen C. Cytotoxicity of titanium and titanium alloying elements. J Dent Res 2010;89:493–497.
186. Costa MT, Lenza MA, Gosch CS, Costa I, Ribeiro-Dias F. In vitro evaluation of corrosion and cytotoxicity of orthodontic brack-ets. J Dent Res 2007;86:441–445.
187. Evans AG. Perspective on the development of high-toughness ceramics. J Am Ceram Soc 1990;72:187–206.
188. Launey ME, Ritchie RO. On the fracture toughness of ad-vanced materials. Adv Mater 2009;21:2103–2110.
189. Dzenis Y. The quest for stronger, tougher materials: Response. Science 2008;320:448.
190. Dzenis Y. Materials science: Structural nanocomposites. Sci-ence 2008;319:419–420.
191. Ritchie RO. The quest for stronger, tougher materials. Science 2008;320(5875):448.
192. Liu J, Rinzler AG, Dai HJ, et al. Fullerene pipes. Science 1998; 280:1253–1256.
193. Kelly A. Strong Solids. Oxford, UK: Clarendon Press, 1966.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology
44 Volume 26, Supplement, 2011
194. Deville S, Chevalier J, Fantozzi G, et al. Low-temperature ageing of zirconia-toughened alumina ceramics and its impli-cation in biomedical implants. J Eur Ceram Soc 2003;23: 2975–2982.
195. Pecharroman C, Bartolome JF, Requena J, et al. Percolative mechanism of aging in zirconia-containing ceramics for medi-cal applications. Adv Mat 2003;15:507–511.
196. Chevalier J, Gremillard L, Deville S. Low-temperature degrada-tion of zirconia and implications for biomedical implants. Ann Rev Mater Res 2007;37:1–32.
197. De Aza AH, Chevalier J, Fantozzi G, Schehl M, Torrecillas R. Crack growth resistance of alumina, zirconia and zirconia toughened alumina ceramics for joint prostheses. Biomateri-als 2002;23:937–945.
198. Ruhle M, Claussen N, Heuer AH. Transformation and micro-crack toughening as complementary processes in Zro2-toughened Al2o3. J Am Ceram Soc 1986;69:195–197.
199. Heuer AH, Claussen N, Kriven WM, Ruhle M. Stability of tetragonal Zro2 particles in ceramic matrices. J Am Ceram Soc 1982;65:642–650.
200. Kibbel B, Heuer AH, Ruhle M. Transformation zones in zirconia-toughened alumina. Am Ceram Soc Bull 1982;61:812.
201. Schehl M, Diaz LA, Torrecillas R. Alumina nanocomposites from powder-alkoxide mixtures. Acta Mater 2002;50:1125–1139.
202. Karp JM, Langer R. Development and therapeutic applications of advanced biomaterials. Curr Opin Biotechnol 2007;18: 454–459.
203. Russias J, Saiz E, Nalla RK, Gryn K, Ritchie RO, Tomsia AP. Fabrication and mechanical properties of PLA/HA compos-ites: A study of in vitro degradation. Mater Sci Eng C Biomim Supramolec Sys 2006;26:1289–1295.
204. Neuendorf RE, Saiz E, Tomsia AP, Ritchie RO. Adhesion between biodegradable polymers and hydroxyapatite: Rel-evance to synthetic bone-like materials and tissue engineer-ing scaffolds. Acta Biomater 2008;4:1288–1296.
205. Deville S, Saiz E, Tomsia AP. Ice-templated porous alumina structures. Acta Mater 2007;55:1965–1974.
206. Deville S, Saiz E, Tomsia AP. Using ice to mimic nacre: From structural applications to artificial bone. In: Bauerlein E, Beh-rens P, Epple M (eds). Handbook of Biomineralization. New York: Wiley, 2007:173–192.
207. Deville S, Saiz E, Tomsia AP. Freeze casting of hydroxy-apatite scaffolds for bone tissue engineering. Biomaterials 2006;27:5480–5489.
208. Deville S, Saiz E, Nalla RK, Tomsia AP. Freezing as a path to build complex composites. Science 2006;311:515–518.
209. Munch E, Launey ME, Alsem DH, Saiz E, Tomsia AP, Ritchie RO. Tough, bio-inspired hybrid materials. Science 2008;322: 1516–1520.
210. Klawitter JJ, Weinstein AM, Cooke FW, Peterson LJ, Pennel BM, Mckinney RV. Evaluation of porous alumina ceramic dental implants. J Dent Res 1977;56:768–776.
211. Calvert P, Crockett R. Chemical solid free-form fabrication: Making shapes without molds. Chem Mater 1997;9:650–663.
212. Lewis JA, Smay JE, Stuecker J, Cesarano J. Direct ink writing of three-dimensional ceramic structures. J Am Ceram Soc 2006; 89:3599–3609.
213. Franco J, Hunger P, Launey ME, Tomsia AP, Saiz E. Direct write assembly of calcium phosphate scaffolds using a water-based hydrogel. Acta Biomater 2010;6:218–228.
214. Deville S, Saiz E, Nalla RK, Tomsia AP. Strong biomimetic hydroxyapatite scaffolds. Adv Sci Technol 2006;49:148–152.
215. Hollister SJ. Porous scaffold design for tissue engineering. Nat Mater 2005;4:518–524.
216. Dellinger JG, Cesarano J, Jamison RD. Robotic deposition of model hydroxyapatite scaffolds with multiple architectures and multiscale porosity for bone tissue engineering. J Biomed Mater Res A 2007;82:383–394.
217. Hutmacher DW, Schantz JT, Lam CXF, Tan KC, Lim TC. State of the art and future directions of scaffold-based bone engineer-ing from a biomaterials perspective. J Tissue Eng Regen Med 2007;1:245–260.
218. Williams JM, Adewunmi A, Schek RM, et al. Bone tissue engineering using polycaprolactone scaffolds fabricated via selective laser sintering. Biomaterials 2005; 26:4817–4827.
219. Gao L, Li JG, Kusunose T, Niihara K. Preparation and properties of TiN-Si3N4 composites. J Eur Ceram Soc 2004;24:381–386.
220. Dhariwala B, Hunt E, Boland T. Rapid prototyping of tissue-engineering constructs, using photopolymerizable hydrogels and stereolithography. Tissue Eng 2004;10:1316–1322.
221. Czernuszka J. Biomaterials: Scaffolds for tissue regeneration. Tissue Eng 2007;13:1369–1370.
222. Russias J, Saiz E, Deville S, et al. Fabrication and in vitro charac-terization of three-dimensional organic/inorganic scaffolds by robocasting. J Biomed Mater Res A 2007;83:434–445.
223. Jongpaiboonkit L, Halloran JW, Hollister SJ. Internal structure evaluation of three-dimensional calcium phosphate bone scaffolds: A micro-computed tomograghic study. J Am Ceram Soc 2006;89:3176–3181.
224. Miranda P, Saiz E, Gryn K, Tomsia AP. Sintering and robocast-ing of beta-tricalcium phosphate scaffolds for orthopaedic applications. Acta Biomater 2006;2:457–466.
225. Kokubo T, Takadama H. How useful is SBF in predicting in vivo bone bioactivity? Biomaterials 2006;27:2907–2915.
226. Bohner M, Lemaitre J. Can bioactivity be tested in vitro with SBF solution? Biomaterials 2009;30:2175–2179.
227. Pearce AI, Richards RG, Milz S, Schneider E, Pearce SG. Animal models for implant biomaterial research in bone: A review. Eur Cells Mater 2007;13:1–10.
228. Kuznetsov SA, Huang KE, Marshall GW, Robey PG, Mankani MH. Long-term stable canine mandibular augmentation using autologous bone marrow stromal cells and hydroxyapatite/tricalcium phosphate. Biomaterials 2008;29:4211–4216.
229. Mankani MH, Kuznetsov SA, Fowler B, Kingman A, Robey PG. In vivo bone formation by human bone marrow stromal cells: Effect of carrier particle size and shape. Biotechnol Bioeng, 2001;72:96–107.
230. Mankani MH, Kuznetsov SA, Marshall GW, Robey PG. Creation of new bone by the percutaneous injection of human bone marrow stromal cell and HA/TCP suspensions. Tissue Eng A 2008;14:1949–1958.
231. Abukawa H, Shin M, Williams WB, Vacanti JP, Kaban LB, Troulis MJ. Reconstruction of mandibular defects with autologous tissue-engineered bone. J Oral Maxillofac Surg 2004;62: 601–606.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 45
Nanotechnology Group Members
Group ChairBrian Mealey, DDS, MS
Group ExpertAntoni Tomsia, PhD
Group SecretaryWayne Aldredge, DMD
Group ParticipantsThomas Dodson, DMD, MPH
Nikos Donos, DDS, MS, PhD
James Doundoulakis, DMD, MS
Shahrokh Esfandiari, BSc, MSc, DMD, PhD
Marco Esposito, DDS, PhD
David Felton, DDS, MS, FACP
Earl Freymiller, MD, DMD
William Giannobile, DDS, DMSc
Asbjorn Jokstad, DDS, PhD
Russell Nishimura, DDS
Jonathan Orenstein, DMD
Marc Quirynen, DDS
Stephen Wheeler, DDS
Nancy Deal Chandler (Silent Participant, ACP)
Michael Collins (Zimmer)
Lyndon F. Cooper, DDS, PhD (ACP)
Stig Hansson, MSc, MA, BM, PhD (Astra Tech)
Stephen Herrington (Silent Participant, Biomet 3i)
William R. Laney, DMD, MS (Quintessence)
Sandro Matter, PhD (Straumann)
Gordon Peterson (Silent Participant, Medtronic)
Mark A. Reynolds, DDS, PhD (Camlog)
Hans Schmotzer, PhD (Nobel Biocare)
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

46 Volume 26, Supplement, 2011
Nanotechnology involves the understanding and control of matter at dimensions between ~1 and
100 nanometers, where unique phenomena enable novel applications. At the nanoscale, materials differ from larger objects in their physical, chemical, and biological properties; therefore, they lend themselves to new and improved materials, systems, and devices. Application of nanotechnology is revolutionizing bio-medical engineering by allowing new types of drug delivery, synthesis of tissue modules, development of biomaterial and improved surfaces for medical de vices, in vitro and in vivo imaging methodologies, biofiltration systems, and robotic assembly, among many other exciting advances. It was natural for the nanotechnology group to focus on dental implant surfaces technologies, since surface technologies have changed significantly since the introduction of dental implants. These changes have been asso-ciated with improved implant survival and success rates. However, advances in nanotechnology offer the opportunity to impact much more than implant surfaces. The group instead focused on nanotechnol-ogy as it impacts the entire practice of implant den-tistry. This includes not only the dental implant itself, but the possibilities of improving diagnostic method-ologies; implant site preparation, restoration, and es-thetics; wound healing; drug delivery; management of peri-implant disease; surgical and restorative tech-niques; and other areas that may have an impact on aspects of dental practice outside of the arena of the dental implant itself.
During group discussions, the members frequently questioned the content expert about specific aspects of nanotechnology. In most instances, when asked, “Could nanotechnology be used to do X?,” the ex-pert’s answer was along the lines of: “Tell us what you want to do with the technology and there is a way to do it.” One of the major road blocks to translating the science of nanotechnology into the clinical practice of implant dentistry is developing funding sources to support the necessary research; therefore, a cost-benefit analysis is inherent in almost every question the group entertained.
Technologies available today have resulted in a high survival rate for dental implants. While many people throw out the “statistic” that “implants work 95% of the time,” this is clearly not a factual state-ment. Implants placed by highly skilled clinicians in specific practice environments, such as those often seen in long-term implant survival/success studies, may have a survival rate that high. However, the “95% survival statistic” masks real-world results and fails to
recognize that certain patients or certain sites within a given patient may be compromised in some way that adversely impacts implant survival/success. Ev-ery clinician performing implant therapy has had the experience of placing multiple implants in a given pa-tient and having one implant fail while the rest suc-ceed. What is it about that one implant or one implant site that resulted in failure? Likewise, why do some patients have implants that fail when others present-ing with the exact same clinical scenario have suc-cessful implant therapy? Because nanotechnology may involve significant development costs, the group recognized that nanotechnological changes may not be needed for the majority of patients in the majority of implant sites. Thus, as these technologies mature, they may be guided toward specific patients, specific sites, or specific clinical indications rather than being viewed as applicable to the majority of dental implant patients and therapies.
Specific questions were provided to the group and, following extensive discussion, a summary state-ment of the group consensus was provided below for each topic area.
What is the primary rationale for the development of the technology?
The primary reasons for development of nanotech-nologies as they relate to implant dentistry are to allow for increased success and predictability in com-promised sites and patients; to allow researchers, manufacturers, and clinicians to manage the biology at the surface and/or site; to provide for less frequent early and long-term implant failure or loss; and to improve cost effectiveness of therapy and thereby in-crease access to care.
What is the potential for nanotechnology to improve clinical outcomes (eg, enhanced predictability of clinical results with hard and soft tissue) in dental implant therapy?
A major goal of nanotechnology is to improve the ki-netics of wound healing in dental implant therapy. One of the most obvious advances is improved implant sur-face technology. While nanotechnology may improve the kinetics of interfacial wound healing involving the dental implant surface, it may also impact other implant components such as abutments. Nanotechnology may alter the bone-to-implant interface and thereby allow
Nanotechnology Group Report
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology Group
The International Journal of Oral & Maxillofacial Implants 47
for more rapid osseointegration, but nanotechnology may also play an important role in modifying the soft tissue-to-implant and soft tissue-to-abutment wound healing kinetics. In addition, improved wound heal-ing kinetics resulting from nanotechnology advances could have a major impact on the results of implant site preparation via improvements in regenerative materials including bone substitutes and membranes. A major goal of such advances would be to allow for superior and more predictable site development for implant placement in individuals and sites with com-promised bone volume or density.
Nanotechnology has great potential to be used in delivery systems for drugs, growth factors, and other compounds. Such delivery systems could be useful not only on the implant surface itself, but also on bone substitutes or via direct application to an extraction socket or prepared osteotomy site. Furthermore, nano-technology may be used in systemically administered delivery systems that might impact bone and soft tis-sues in a more widespread fashion. Nanoscale delivery systems could target growth and differentiation factors to the location where they are actually needed, and provide appropriate controlled-release kinetics to best stimulate formation or repair of tissues.
Nanotechnology may be used for real-time assess-ment of microbial colonization to aid in management of the peri-implant biofilm, as well as identification of inflammatory markers to decrease peri-implant mu-cositis/peri-implantitis. Nanotechnology may allow delivery of antimicrobial agents targeting active areas of implant infection. Similarly, nanoscale delivery sys-tems may be used to modulate inflammation locally at given implant sites or more generally via systemic delivery systems.
Nanotechnology is already being used for real time diagnostics in medicine. Relative to implant dentistry, nanodiagnostics might be useful at the time of tooth extraction by aiding in evaluation of the potential im-plant site, at the time of implant placement by helping assess bone quality or quantity at the time of osteot-omy preparation, or in evaluating factors impacting potential implant failure.
Nanotechnological improvements in instrumenta-tion could result in development of sensors to pro-vide in-situ microenvironmental information during implant surgery, such as feedback on temperature and bone density, which could result in less heat gen-eration during implant surgery. Infusion of nanomedi-cines through implant drills and release of biomodifiers during implant placement may also be possible. Nano-technology improvements in implant components and prosthetic materials may result in stronger, longer lasting, and more esthetic restorations. Nanotechnolo-gies may allow for the development and manufacture
of a predictable shorter dental implant that could be used at anatomically challenging sites, decreasing the need for advanced augmentation techniques such as sinus augmentation, vertical ridge augmentation, or nerve lateralization. Development of self-repairing nanosize materials may allow implant components to tolerate stresses and strains in ways not currently avail-able or even to self-repair cracks and fractures. Chang-es in materials may provide the opportunity to achieve true reintegration of failing implants. Nanotechnology offers the potential for sutureless flap closure.
Nanotechnology may play a role in allowing for creation of a peri-implant ligament to more closely replicate the natural tooth-ligament-bone relation-ship. While some may argue that this “advance” could lead to the same types of peri-implant disease that we see around teeth (periodontitis), the intent of such de-velopments would not be to attain a peri-implant liga-ment in all patients or sites. Instead, nanotechnology may allow for customization of dental implant thera-py in ways not currently imaginable. For example, the ability to develop a peri-implant ligament may allow for placement of dental implants in young individu-als who are still growing, to allow for connection of implants to natural teeth without potentially adverse effects, or to allow orthodontic movement of dental implants.
The real potential of nanotechnology lies not in de-veloping a one-size-fits-all change in implant therapy, but rather in allowing individualization of therapy in such a way that the technologies are applied where and when they are most needed. Given the potential costs of nanoscale technologies and the high suc-cess rates of current implant therapy, these targeted advances are more likely than a wholesale change in dental implant therapy.
What kinds of patients are most likely to need, want, or be candidates for the treatment/technology?
The most likely recipients of nanotechnological inno-vations in dental implant therapy are those patients and individual sites that currently are not candidates for dental implants. These might include, for exam-ple, medically compromised patients or individuals with potential implant sites that are biologically or anatomically compromised. Others who may ben-efit include patients with prior implant failures, ailing implants, occlusal parafunctional habits, a history of periodontitis, a history of head and neck radiation therapy, and poor oral hygiene or inflamed tissues. Nanotechnology may be particularly applicable to patients with high esthetic demands.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology Group
48 Volume 26, Supplement, 2011
What additional evidence regarding technical properties should be gathered to enhance development and enable transfer of the new technology?
Additional evidence is needed to determine what sur-face topographies will maximize the bone-to-implant interfacial shear strength. In addition, the topographical features that will best aid in the acceleration of bone-to-implant contact need to be examined. The aspects of nanotechnologies which will optimize the biome-chanical properties of the soft and hard tissue interface must be identified. The aspects of nanotechnologies that will provide the best biologic, biomechanical, and controlled release properties of regenerative materi-als (bone substitutes, membranes, etc) also need to be identified. A major question in this regard is, “How is the release of biologically active agents controlled?” That is, research is needed to determine how much biologically active agent is needed, what the agent is intended to do, when in the healing process should it be released (release kinetics), how long the agents should remain active, and how nanotechnology can aid in these solutions. Nanoscale solutions are already available in many such arenas, eg, nanoscale “smart spheres” in use in nanomedicine consisting of an inner core containing the biologically active agent, an outer core which controls release kinetics, and an external skin to protect the sphere. Research is needed to eval-uate such smart spheres for applications in implant dentistry. Finally, research is needed to determine the utility of nanotechnology for chairside diagnostics to identify from serum, saliva, or gingival crevicular fluid a panel of microbial or inflammatory markers that pre-dict peri-implant inflammation and bone loss or aid in the treatment thereof.
What are the safety issues associated with nanotechnology?
Research is needed to identify the potential health risks of using nanoparticles, as these risks are current-ly unknown. Evidence to date suggests that nano-surface alterations in materials, be they additive or subtractive, appear to be safe. Nanodiagnostic tech-nologies are needed to help identify the health risks that may be associated with nanoparticle safety.
What is the potential for the technology to improve a patient’s physical health (oral and systemic) and quality of life (ie, psychological, functional)?
An important consideration in application of nano-technology is an analysis of cost versus benefit. The potential for nanotechnology to improve a patient’s health and quality of life may be minimal in patients/sites that are likely to respond successfully to cur-rently available implant technology. Conversely, the potential is high for individuals in high-risk groups or with sites where current implant technologies might have decreased success. It is possible that if nano-technology is developed on a broad scale in implant dentistry, the costs may not be prohibitive. In some cases, nanotechnology may actually allow for implant costs to decrease. For example, targeted application of nanotechnology to patients/sites with a high risk of implant failure (surgical or restorative) or of mor-bidity associated with implant therapy may result in decreased overall cost by minimizing or eliminating the need for repeated surgical or restorative interven-tions that might occur with existing technologies.
One focus of discussion in the nanotechnology group is the potential risk of nanotechnology. Sig-nificant research is needed on health risks associated with nanotechnology. For example, there is little data available on the potential toxicity of nanoparticles. In order for these technologies to be widely effective, they must first be safe.
Is the current evidence sufficient to warrant further research and resources being directed toward the technology relative to dental implant therapy?
Without question, nanotechnology is advancing at a rapid rate. Current evidence is sufficient to warrant further research in this area. In vitro and animal stud-ies show promising preliminary results, especially in the area of nanosurface technologies. The value and usefulness of nanotechnology may be in the delivery of medicine(s), nanocoatings, topography, and biomi-metic approaches with direct applicability to improv-ing health outcomes. As stated by the group expert: “nanotechnology is a developing science whose future is nanomedicine.” With further research and evidence, nanodentistry may be added to that statement.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Nanotechnology Group
The International Journal of Oral & Maxillofacial Implants 49
What are the efficacy and effectiveness (psychological, clinical, functional, patient perspectives, etc) issues associated with nanotechnology?
Due to the potential cost associated with nanotechnolo-gy, research is needed to evaluate what level of increased effectiveness is required to justify the investment. Stud-ies will be necessary to determine whether technologi-cal innovations significantly affect the predictability and longevity of implant therapy, including in compromised patients or sites. It is important to evaluate whether nan-otechnology improves patient-centered implant out-comes. Finally, nanodiagnostic technologies are needed to help identify the effectiveness of nanotechnology innovations in implant dentistry, ie, evaluation of the value of nanotechnology will likely require diagnostic technologies that operate on a nanoscale.
What are the economic factors associated with nanotechnology?
As stated above, research must help evaluate the level of increased effectiveness needed to justify the investment in nanotechnology. Also, how can the potential immediate short-term cost increases be balanced against the potential long-term cost de-
creases that may result from technological innovation at the nanoscale? For example, if nanotechnological changes are able to increase implant longevity, de-crease implant complications/loss, and decrease costs of maintenance and repair, are those changes worth the increased up-front cost? The cost-to-benefit ratio issues that help target nanotechnology changes to appropriate patients/sites must be identified, ie, since most patients/sites may do well with current technol-ogy, what types of patients/sites would benefit most from nanotechological changes if those changes were more expensive? Finally, research is needed to deter-mine how implant therapy can be made more afford-able to a larger patient population.
What are the legal and ethical issues associated with nanotechnology?
One ethical question that must be addressed is: “What potential barriers to care may arise if nanotechnolo-gies significantly improve outcomes but also have significantly increased costs?” Another major issue is the lack of available safety data for nanoparticles. As the safety issues associated with nanoparticles are un-known, should clinical applications of the technology proceed?
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

50 Volume 26, Supplement, 2011
Stem Cell therapy
Prosthetic implants stabilize and restore function to damaged, diseased, or injured bony tissues and
represent one of the most remarkable advances in modern medical technology. Whereas advancements in materials science have produced implants with highly desirable physical properties, a remaining chal-lenge is the issue of osseointegration, both in terms of effective initiation and with respect to the long-term stability of the bone-biomaterial interface. Optimiza-tion of stable interactions between the bone and im-plant to minimize the need for subsequent revision
surgery is critical, particularly in situations such as to-tal joint replacement. Tissue reaction to the implant biomaterial, eg, excessive fibrous ingrowth, may com-promise stable bone/biomaterial interactions and could contribute to subsequent long-term implant loosening. The exact etiology of implant loosening is also under active investigation in many laboratories, and it is clear that wear debris–related responses are important for this process.1
In principle, implant loosening could presumably be lessened by at least two processes. The first of these is the promotion of a more stable bone-biomaterial inter-face, and the second is the reduction of wear debris– induced osteolysis. These are the main topics presented in this review. The specific theme here is that osteopro-genitor cells, which are principally responsible for the stabilization and remodeling of the periprosthetic bone, represent a prime candidate cell type that plays a critical role in mediating effective and stable tissue-implant in-teractions. An understanding of the mechanisms under-lying the biologic activities of these cells is thus critical to the development of effective approaches in enhancing osseointegration and long-term implant stability.
1 Director, Center for Cellular and Molecular Engineering, Department of Orthopaedic Surgery, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania.
The author reported no conflict of interest.
Correspondence to: Dr Rocky S. Tuan, Center for Cellular and Molecular Engineering, Department of Orthopaedic Surgery, University of Pittsburgh School of Medicine, 450 Technology Drive, Room 221, Pittsburgh, PA 15219. Fax: +412-624-5544. Email: [email protected]
Role of Adult Stem/Progenitor Cells in Osseointegration and Implant Loosening
Rocky S. Tuan, PhD1
The long-term stability of prosthetic implants is ultimately a function of the integrity of the biologic interaction between the resident tissues and cells and the biomaterial. Connective tissues of the skeleton undergo constant remodeling and turnover, and the interface with the implant biomater-ial is therefore a dynamic structure that results from ongoing differentiation of progenitor cells into functional cellular phenotypes. An understanding of the regulation of the mechanisms by which progenitor cells initiate and maintain their interactions with the biomaterial surface while undergoing the necessary differentiation processes is thus essential to optimizing the long-term stability of prosthetic implants. This review presents evidence that the interactions between adult mesenchymal stem cells, as the principal progenitor cell type of skeletal connective tissues, and the biomaterial surfaces are influenced by surface chemistry and topography and regulated by the extracellular matrix and growth factors. Mesenchymal stem cells are also the targets of the wear debris particles that are a by-product of implant biomaterials, resulting in direct and microenviron-mental effects, including apoptosis, suppression of proliferation and osteogenic differentiation, and the production of proinflammatory cytokines, that compromise the long-term stability of the bone-implant interface. These effects are initiated by endocytosis of the submicron particles by the mesenchymal stem cells. These observations strongly suggest that optimization of the sta-bility of implant osseointegration must address factors that enhance and promote the biologic activities of the stem/progenitor cells of skeletal connective tissues. Int J Oral Maxillofac Implants
2011;26(suppl):50–62
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

tuan et al
The International Journal of Oral & Maxillofacial Implants 51
meSenChymal Stem CellS
Identification and Characteristics Mesenchymal stem cells (MSCs) were first discovered in the bone marrow. Friedenstein et al described these “osteogenic stem cells” as clonal and fibroblas-tic stromal cells that formed adherent colonies in cul-ture and had robust osteogenic potential.2 The term mesenchymal stem cells was first coined by Caplan,3 and seminal work by Pittenger and colleagues dem-onstrated the multilineage potential of MSCs into bone, cartilage, and fat.4 Cells with similar character-istics have since been identified in and isolated from many adult tissues.5,6 MSCs were first described as the mononuclear cells from bone marrow that, when cul-tured ex vivo, were adherent colony-forming unit fi-broblasts (CFU-F7). Current approaches for identifying MSCs include the clonogenic capacity to form CFU-F in vitro, the presence of certain cell surface epitope markers, and multilineage differentiation potential.8
Unlike other stem cells, in particular embryonic stem cells and hematopoietic stem cells, there are currently no specific surface markers for MSCs, al-though there exists a collection of epitopes that are associated with cells with MSC-like characteristics. Immunotyping for cells positive for STRO-1, CD73, CD146, and CD106 and negative for CD11b, CD45, CD34, CD31, and CD117 has been shown to most reli-ably characterize the MSC population.8,9 The consen-sus of the International Society for Cellular Therapy, which is subject to future modification, is that mea-surements by flow cytometry must show that at least 95% of the MSC population expresses CD73, CD90, and CD105 and no more than 2% of the cells may ex-press CD34 (hematopoietic progenitor and endothe-lial cell marker), CD45 (pan-leukocyte marker), CD11b or CD14 (monocyte and macrophage markers), CD19 or CD79a (B cell markers), and human leukocyte anti-gen-DR (marker of stimulated MSCs).10
Because of the lack of a specific surface epitope profile, many names have been assigned to MSCs or subpopulations thereof, including mesenchymal stro-mal cells, bone marrow stromal cells, marrow-isolated adult multipotent inducible cells, multipotent adult progenitor cells, and mesenchymal progenitor cells, in addition to the original term coined by Caplan.8
tissue Sources of mSCs Subsequent to the discovery of MSCs in the adult bone marrow, cells with MSC-like characteristics have been identified in a large number of adult tissues, in-cluding tissues derived from all three germ layers. Examples of tissues where MSCs have been character-ized include but are not limited to: mesodermal (bone marrow, trabecular bone,11 synovium,12,13 cartilage,14
fat,15,16 muscle,17 and tonsil18); endodermal (thymus19); ectodermal (skin,20 hair follicle,21 and dental pulp22 [mesoderm- and ectoderm-derived]); and prenatal and perinatal tissues (umbilical cord,23 umbilical cord blood,24 and placenta25). Stem cells derived from these tissues and organs share common characteristics and are commonly referred to as MSCs or mesenchymal progenitor cells. Of special relevance to this review are the MSCs found in adult bone, which may be iso-lated by physical dissociation of the tissue followed by long-term explant of the bone chips, from which the MSCs emerge and migrate onto the culture substra-tum.11,26,27 Because of their location and derivation, these cells should thus be considered osteoprogenitor MSCs, and they are highly likely to be important for im-plant osseointegration and long-term stability.
Osteogenic Differentiation of mSCsUnder appropriate inductive conditions, MSCs un-dergo discrete osteogenic differentiation in culture.5,6 This process is stimulated by a number of factors, in-cluding supplementation with β-glycerophosphate, 1,25-dihydroxyvitamin D3, and/or bone morphoge-netic proteins (BMPs). The process is characterized by the expression of osteoblast-specific or osteoblast-associated markers, including elevated levels of the osteogenic transcription factor Runx2, collagen type I, alkaline phosphatase, bone sialoprotein, osteopon-tin, and osteocalcin; a change of cellular phenotype from a fibroblastic shape to cobblestone-shaped osteoblastlike cells; and subsequent matrix mineral-ization. When the cells undergoing osteogenic differ-entiation are placed in a three-dimensional matrix, a bony construct is formed that exhibits characteristics of engineered bone.28 Implantation of such engi-neered constructs has been used effectively to repair bone defects, such as fractures and nonunions.29
Regulation of MSC osteogenic differentiation has been under intensive investigation. In addition to the culture conditions and supplements already listed, other extracellular factors and their signaling path-ways that have been implicated include members of the Wnt, transforming growth factor-β, fibroblast growth factor, and Hedgehog families, with the req-uisite cross talk among the different pathways.5,6 In addition to these “usual suspects” of growth factors, a number of other agents and influences are also at work in controlling the proliferation/differentiation decision-making process for MSCs. These include the extracellular matrix, direct cell-cell contact, metabo-lites, and physical perturbations such as shear and compression.9,30
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell therapy
52 Volume 26, Supplement, 2011
OSSeOIntegratIOn
The process termed osseointegration refers to the sequence of events by which living bone lies in di-rect apposition to a prosthetic component without any intervening soft or fibrous tissue.31 It has been proposed that two conditions must be fulfilled for optimal osseointegration to take place: (1) the bone must be brought into close proximity of the implant materials, and (2) the cells interacting with the bio-material surface must adhere to the material surface and undergo natural maturation into tissue-specific cells and produce bone-specific extracellular matrix. Optimally, a functional implant surface, by virtue of its chemistry and topography, would also avidly adsorb those matrix molecules produced by the cells that are required for and promote cell maturation, thus influ-encing both initial cell adhesion and subsequent tis-sue development.
Optimization of the cell-implant interface thus re-quires an understanding of the specific events that mediate an intricate, intimate interaction between the osteoprogenitor cells and the implant surface, and this interaction is likely to be functionally influ-enced by both the chemistry and the topography of the biomaterial.32–35 In previous studies of cell-bio-material interactions, researchers have approached this by utilization of an experimental system of bone-derived osteoprogenitor cells to analyze the influence of surface chemistry and topography on several cellular parameters: (1) cell adhesion, (2) cell morphology, (3) expression and maturation of the osteoblastic phenotype, and (4) production and or-ganization of the extracellular matrix. Three surfaces
have been examined: polished smooth, roughened by sandblasting, and sinter-coated porous surfaces of cobalt-chrome (CoCr) or titanium (Ti) alloys, two biomaterials that are commonly used for orthope-dic and dental prostheses. Importantly, these three surfaces have been custom-fabricated to yield the composition and topography of the orthopedic pros-theses used in arthroplasty. These surfaces are pas-sivated in nitric acid and sterilized with ultraviolet light. Examples of the three surfaces, as imaged by scanning electron microscopy, are shown in Fig 1.36 The smooth surfaces appear gently undulating with narrow, parallel grooves of different depths spaced throughout the surface (Fig 1a). The sandblasted rough surfaces appear to be very uneven, with pits that range in size from several microns to several hun-dred microns; depths of these pits are variable, as is their relative spacing (Fig 1b). Porous surfaces appear globular with large peaks and valleys (pore size, 100 to 300 µm), with a fine structure similar to that seen on roughened surfaces (Fig 1c).
A cell adhesion assay was established for use with osteoprogenitor cells plated on metallic surfaces.34 Because it was not possible to directly count the cells on the opaque surfaces of the metal alloys, cells were labeled with 2’,7’-bis (2-carboxyethyl)-5-carboxyflu-orescein acetoxymethyl ester, an esterified dye that when internalized by living cells is hydrolyzed by cellular esterases to a membrane-permeable fluores-cent species. The cells were detergent-lysed and the released dye collected in the supernatant for mea-surement by spectrofluorimetry. This technique was previously shown to be accurate with linear dye in-corporation as a function of the number of cells.32,33
Fig 1 Surface topography of titanium alloy (Ti-6Al-4V) implants as visualized by scanning electron microscopy. Characteristic appearances of (a) smooth, (b) sandblasted rough, and (c) porous implants. Bar = 100 µm.
a b c
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

tuan et al
The International Journal of Oral & Maxillofacial Implants 53
Bone-derived osteoprogenitor cells adhered in greater numbers to both polished Ti and rough Ti at all time intervals tested, with cells plated on rough Ti having a slight adhesive advantage over cells plated on smooth Ti. The effect of substrate composition on cell adhesion kinetics was then tested. Cells on Ti al-loys adhered in greater numbers than those plated on CoCr alloys, suggesting that cells on the Ti alloys had an adhesive advantage over cells on CoCr (Fig 2).34
Cell morphology Cell adhesion is mediated via the establishment of focal adhesion contacts, and subsequent cell spread-ing is necessary to initiate the intracellular signaling events mediated via adhesion37 (see Fig 3). To exam-ine the degree of cell spreading, the focal contact distribution, the cytoskeletal organization (which is directly influenced by focal contact distribution), and the topography of the substrate, the author and colleagues imaged the cells by means of confocal la-ser scanning microscopy (CLSM). In this type of op-tical imaging, the laser beam can be focused onto a plane of finite width to allow optical sectioning of the cell, and the images may be digitally collected into a volumetric z-axis stack to obtain three-dimensional morphometric measurements, including the size and volume of specific areas of interest. In addition, simultaneous multichannel acquisition allows for the assessment of two or more parameters in the same optical section of the field. In this way, it is possible to relate cell spreading to focal contact distribution, ac-tin cytoskeletal organization, and surface topography to begin to understand how osteoprogenitor cells prefer to interact with the different surfaces.
Activation of integrins, receptors that interact with extracellular matrix proteins to activate intracellular signaling pathways, causes cell spreading. Integrins are heterodimers composed of α and β subunits that span the cell membrane.38 Interactions with the ex-tracellular matrix molecules are mediated largely through integrin receptor sites that recognize the peptide motif arginine-glycine-aspartic acid (RGD) present in matrix molecules such as fibronectin and vitronectin, although the α2β1 and α1β1 integrins appear to bind collagens through non-RGD sites that recognize the three-dimensional conformation of the ligand. Integrins may be phosphorylated, although phosphorylation does not seem to always correlate with signal transduction. Importantly, activated in-tegrins cluster to form the focal adhesion contact; this process is either the direct result of the structure of the underlying extracellular matrix or may itself cause reorganization of the matrix. It is clear that interactions between matrix proteins are necessary, as interference with these interactions can decrease
cell adhesion. Clustering of integrins initiates the as-sembly of a macromolecular complex that includes signaling molecules such as focal adhesion kinase (p125FAK), src, and ras, and molecules important for tethering the actin cytoskeleton to the focal contact, such as vinculin and talin39 (see Fig 3).
To characterize the interaction of osteoprogenitor cells with the two commonly used orthopedic and dental implant alloys Ti and CoCr, CLSM was first used to visualize the focal contact organization on the two surfaces. These images were digitized and used to cal-culate the area of the individual cells, the area occu-pied by focal contacts in these cells, the shape factor of the cells, and the percentage of the total cellular area occupied by focal contacts. Shape factor ([area/perimeter2] × 4π) measures the deviation from a per-fect circle, which has a shape factor of 1. Consistently, Ti alloys had smaller cell areas and more focal con-tacts, were more elongated as detected by shape fac-tor calculations, and had a greater percentage of their membranes devoted to focal contacts than cells plat-ed on CoCr alloys. The fact that cells were more elon-gated but had a smaller cell area on Ti alloys could be explained by the fact that the cells on Ti alloys were well-spread with few cellular processes, whereas on CoCr alloys, cell spreading correlated with the exten-sion of multiple processes to anchor the cells.
Next, the three-dimensional relationship of the focal contact distribution in the osteoprogenitor cells with the alloy surface was examined. Cells immuno stained for vinculin were visualized and optically sectioned by CLSM, followed by computer-aided three-dimensional
0 3 6 12Time (h)
35
30
25
20
15
10
5
0
No.
of
atta
ched
cel
ls (
×1,0
00)
* CoCr
Ti
*
*
Fig 2 Effect of composition on osteoblast adhesion upon rough Ti and CoCr. Cell adhesion was determined as a func-tion of time. Asterisks denote time-matched values that were significantly different (P < .01) between rough Ti and CoCr sur-faces. The results indicate that the degree of cell attachment was consistently greater on Ti surfaces than on CoCr surfaces.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell therapy
54 Volume 26, Supplement, 2011
reconstruction of the cell-Ti or cell-CoCr interface. The authors used this reconstructed image to section cells in the x-y plane at various depths along the z-axis (ie, the axis perpendicular to the surface) to map adhesion plaque distribution. Focal contacts were apparent at all membrane-to-surface contact points on both rough Ti and CoCr (Fig 4). On the rough Ti surface (Fig 4a), the focal contacts were distributed along the contours of the surface; on the rough CoCr surface (Fig 4b), the fo-cal contacts formed only at the relative topographic peaks. Based on these images, it was predicted that the cell would fill up the valley as well as adhering to the peaks on the rough Ti, whereas on rough CoCr, the cell would span these valleys through extension of multiple processes.
To test the validity of these predictions, the au-thors used three-channel acquisition to correlate surface reflectance, actin filament organization, and vinculin-containing focal contacts. The three-dimen-sional image was then reconstructed computation-ally and a slice examined in the x-z plane to reveal the apparent shape of the cells as outlined by the actin microfilament system, the presence of topographic metal peaks, and the distribution of the focal contacts relative to these two. On rough Ti, the actin stress fi-bers followed the contour of the surface, with focal contacts apparent along the ventral membrane of the cell. On rough CoCr, parallel actin filaments were found only in the cellular extensions that spanned valleys, and focal contacts could be visualized in these lamellipodia only on the relative topographic peaks. No focal adhesion contacts were visualized on the dorsal membrane, as would be expected as a re-sult of the lack of contact with any substrate.
These results, taken together, strongly indicate that biomaterial composition significantly affects focal con-tact formation and ordering of actin microfilament sys-tems in adherent osteoprogenitor cells (Fig 5). On Ti, the cells achieve maximal surface contact area by con-forming to the irregularities of the surface, precluding the need for the lateral spreading seen on CoCr. Focal contacts formed at all membrane-to-surface contact points on both Ti and CoCr, although the degree of formation was reduced and distribution was limited to topographic peaks on CoCr. Finally, the actin filaments followed the surface contour on Ti, whereas on CoCr, they spanned chasms consistent with the data on focal contact distribution and with cell shape. It is interest-ing to speculate that similar cellular events could take place in vivo upon placement of the metallic implant into bony sites and that these events would govern or guide subsequent reaction of the bone tissue to the respective biomaterials. Obviously, to what extent these findings are reproduced during the early stages of osseointegration in vivo remains to be investigated.
A similar dependence of MSC morphology on surface chemistry and topography has been reported recent-ly,40 and other studies have suggested that these bio-material effects are associated with changes in cellular signaling mechanisms, such as those involving Wnt.41 While the long-term consequences of such influences on implant stability remain to be clarified, these find-ings taken together strongly suggest that functional classification of biomaterial surfaces is needed to de-velop better predictive parameters for implant devel-opment and fabrication.42
Osteogenic Differentiation and extracellular matrix Organization Shah et al34,35 used BMP-2 as a potent osteoinductive agent to stimulate osteogenesis of osteoprogenitor cells plated onto a Ti alloy surface. Key findings were: (1) BMP-2–treated cells showed an elevated level of substrate adhesion; (2) the enhanced adhesion was accompanied by a larger focal adhesion contact area, as well as a more organized cytoskeleton; and (3) BMP-2 treatment resulted in enhanced osteogenesis demonstrated by a higher level of expression of os-teoblastic markers and matrix mineralization.34,35
Interestingly, these osteogenesis-associated chang-es were accompanied by discrete changes in the pro-duction and organization of extracellular matrix and in integrin levels.34,35,43,44 The effects of BMP-2 treatments were assessed on Ti surfaces 12 hours after plating by immunohistochemistry for fibronectin, vitronectin, collagen type I, osteopontin, osteocalcin, osteonec-tin, laminin, osteonectin, and laminin, in parallel with filamentous actin. Fibronectin and vitronectin showed the most extensive extracellular organization in both control and BMP-2–treated cells, suggesting that these matrix components were important for early cell ad-hesion. After BMP-2 treatment, staining for collagen type I became apparent; other components showed only intracellular staining (osteopontin, osteonectin, and osteocalcin) with no changes in organization or no detectable staining (laminin). Changes in fibro-nectin were examined in more detail. Immunoblot-ting showed a higher level of fibronectin expression in BMP-2–treated cells. Secondly, it was observed that BMP-2 treatment elevated cell adhesion to surfaces that have been conjugated with RGD, the peptide motif principally responsible for mediating the fibro-nectin-integrin interaction. This suggests that the en-hanced cell adherence was a cell-autonomous event, which was later correlated to higher levels of the fibro-nectin receptor integrin subunits α5 and β1. Finally, to test the functional significance of these BMP-2 effects, the level of p125FAK activation/phosphorylation was examined. Cells that had been pretreated with BMP-2 were harvested after 12 hours on Ti; they showed
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

tuan et al
The International Journal of Oral & Maxillofacial Implants 55
increased p125FAK expression by Western blotting. When a parallel blot was probed with a phospho-ty-rosine antibody, the extract from BMP-2–treated cells showed increased p125FAK phosphorylation above that accounted for by the increased expression. This increased p125FAK phosphorylation was suggestive of increased intracellular signaling through pathways integrated with the activated p125FAK. Subsequent findings indicate that this is a genuine BMP signaling event, in that Smad1 activation is also detected, and that there is crosstalk between the BMP/Smad1 path-way and the p125FAK pathway via the activation of the mitogen-activated kinase intermediate p38.44
Taken together, these observations clearly indicate that the interaction between osteoprogenitor cells and an implant biomaterial is critically dependent on the properties of the biomaterial and is regulated and mediated by intricate cellular and molecular mecha-nisms, which involve specific receptor-mediated sig-naling by osteoinductive factors. By correlating early events of osteoprogenitor cell–biomaterial inteac-tions with longer-term biocompatibility and adher-ence properties, such analytic studies should yield a knowledge base for the rational development and design of biomaterial surfaces that will promote in-timate initial cell-biomaterial interaction for optimal osseointegration.
Wear DebrIS–meDIateD OSteOlySIS
Subsequent to the initial osseointegrative events and the pursuant bony ingrowth into the biomater ial sur-face, the ultimate long-term stability of an implant is dependent on the continuous maintenance of the in-terface to prevent loosening. Unfortunately, retrieval studies have consistently shown that even in asymp-tomatic arthroplasty, robust bony ingrowth is seen on only a fraction of the biomaterial surface.45,46 Thus, any further compromise of the integrity of the inter-face would lead to loosening. Implant loosening is characterized by the formation of a fibrous membrane (instead of osseous integration), production of inflam-matory cytokines, and periprosthetic bone resorp-tion. Implant loosening and periprosthetic bone loss are secondary to the production of particulate wear debris.47,48 Wear debris is generated continuously by articulating motion at the bearing surfaces. Peripros-thetic bone is often subject to a very unique microen-vironment in which bone marrow cells and osteoblasts are in direct contact with the implant biomaterials.49 Cells of the monocyte/macrophage lineage play a primary role in wear-induced osteolysis, mediated in particular by their production of matrix-degrading enzymes, such as matrix metalloproteinases.50 Many other immigrant and resident cells are also active
Fig 3 Interactions of the extracellular matrix adsorbed to the biomaterial surface with cellular signaling machinery. Various extra-cellular matrix (ECM) proteins, such as fibronectin, interact with their integrin receptors, membrane-spanning heterodimers composed of an α and a β subunit. Occupation of these receptors initiates clustering into focal adhesion contacts; phosphorylation of p125FAK, the focal adhesion kinase; and subsequent activation of intracellular signal transduction pathways. Through additional associated pro-teins, the focal adhesion contact also serves as an organizing center for actin stress fibers. MAPK = mitogen-activated protein kinase.
Actin stress fibers
MAP kinase pathwayTyr phosphorylation
Biomaterial surface
ECM proteins
Fibronectin
Integrinclustering
Cytosol plasma membrane
Vinculin
Talin
FAK
Src
α-Actinin
S S S S
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell therapy
56 Volume 26, Supplement, 2011
participants in the bioreactive process.51 The biologic response to wear debris at the periprosthetic inter-face is universal with respect to implant biomaterials. An increasing volume of literature exists on the cellular and molecular mechanisms by which wear particles stimulate the host inflammatory response, predomi-nantly through macrophage activation.52 Particle/ macrophage interactions initiate signaling events by cell membrane contact alone or with phagocytosis, and activation of intracellular kinase and transcription factor is a critical component of the inflammatory process.
resident Cells The hematogenous cells (monocytes/macrophages), as well as lymphocytes and polymorphonuclear leuko-cytes (neutrophils), are resident in the tissue surround-ing an implant. Formed in the bone marrow, these
cells are mobilized into the vascular compartment; via tethering and rolling along the endothelium of the postcapillary venules, they adhere and finally migrate across the blood vessel wall to tissues, including the periprosthetic areas.51 In addition to the hematoge-nous cells and vasculoendothelial cells, two other well-recognized resident cell types, fibroblasts and osteo blasts, are responsible, respectively, for the pro-duction of the interstitial fibrous collagenous matrix in connective tissue, which provides structural sup-port and strength, and the formation of the bony ma-trix. It should be noted that the formation of osseous versus fibrous tissue must be spatiotemporally regu-lated to ensure the functional architecture of the peri-prosthetic tissue. The compromised local renewal of these cells will impair peri-implant tissue strength, which is why recruitment of these cells, for example from bone marrow or from the circulation, must be maintained for the development of a functional im-plant interface.
Osteoblasts serve another function: regulating osteoclastogenesis via production of cell mem-brane–associated receptor activator of nuclear factor κB ligand L (RANKL) and macrophage colony-stimu-lating factor (M-CSF).53 RANKL can bind either to its macrophage receptor, RANK, or to its decoy receptor, osteoprotegerin. Interaction of the osteoblast-de-rived RANKL with the macrophage RANK stimulates the mononuclear cells of the monocyte/macrophage lineage to undergo cell fusion to polykaryons. Con-nective tissue fibroblasts are likely to stimulate forma-tion of the foreign-body giant cells,54,55 and cytokines released from osteoblasts in bone in turn enhance formation of osteoclasts.56,57 These events are the hallmarks of implant loosening by mediating chronic foreign-body reactions and peri-implant osteolysis.
Fig 5 Schematic representation of osteoprogenitor cell inter-action with Ti and CoCr biomaterial surfaces.
Ti
CoCr
Fig 4 Three-dimensional relationship of cellular focal contacts with the biomaterial alloy surface. Osteoprogenitor cells labeled green for actin cytoskeleton and immunostained for the focal contact protein vinculin (bright white) were optically sectioned by CLSM, followed by computer-aided three-dimensional reconstruction of the cell-Ti or cell-CoCr interface. Optical sectioning (see plane of section) along the indicated y–z axis plane shows focal contacts (arrows) following contours of the surface on Ti (red) while remaining localized to rela-tive topographic peaks on CoCr (purple). Arrows indicate corresponding points of focal contacts and surface reflectance. Bar = 25 µm.
Plane of section
Ti CoCr
Plane of section
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

tuan et al
The International Journal of Oral & Maxillofacial Implants 57
Immigrant Cells Apart from monocytes, other leukocytes are recruited from the circulation to the interface membrane, the site of the foreign-body reaction. Lymphocytes have been found in peri-implant tissues, highlighting the existence of adaptive immune processes, which may be important in mediating metal hypersensitivity, in which metal ions derived from electrochemical corro-sion of metallic implants or metallic wear debris bind to proteins and modify them such that they are rec-ognized by lymphocytes.
Inflammation and macrophage activation in response to particulate biomaterials As depicted in Fig 6, these are critical events in the periprosthetic osteolytic process. Because they are outside the immediate scope of the present paper, the readers are referred to various other publications that provide in-depth review of the subject.58,59
effect of Wear Debris particles on Osteogenesis and Osteoprogenitor/Stem Cells A number of studies using osteoblasts or osteoblast-like cells have shown that exposure to wear debris par-ticles substantially suppressed the osteoblastic phenotype. Titanium particles disrupt osteoblast func-tion in MG-63 human osteosarcoma cells,60 trigger apoptosis in calvarial osteoblasts,61 alter osteoblast adhesive behavior,62 and stimulate chemokine pro-duction in osteoblasts.63 Most interestingly, particu-late wear debris also severely compromises the biologic activities of osteoprogenitor MSCs, including reduced proliferation, enhanced apoptosis, and sup-pressed osteogenic differentiation.64 During the course of implant life, particularly in the case of poor initial implant fixation with excessive micromotion or constant accumulation of wear particles over time, MSCs derived from the resident bone tissue and from the bone marrow component will be continuously ex-
Genetic predisposition
Mesenchymal stem cell
Osteoblast
Bone
OsteoclastForeign body giant cell
Osteolysis
Macrophages
InhibitionStimulation
Cellular process
Wear particles
Recruitment
ChemokinesMCP-1, MIP-1α
CytokinesTNF-α, RANKL, MCSFIL-6, IL-1β, Interferons
Apoptosis
CD11b/CD18TLRs
KinasesNFkb
Fig 6 Biologic reactions between implant and wear debris and host cells. IL = interleukin; MCP = monocyte chemoattractant protein; M-CSF = macrophage colony-stimulating factor; MIP = macrophage inflammatory protein; NFκB = nuclear factor κB; RANKL = receptor activator of NFκB; TLR = toll-like receptor; TNF = tumor necrosis factor.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell therapy
58 Volume 26, Supplement, 2011
posed to high concentrations of debris throughout the stage of mesenchymal bone repair, when implant fixa-tion is relatively weak. As a result of the prolonged expo-sure to particles, disruption of the normal osteogenic differentiation process of MSCs will occur, resulting in a diminished population of functional osteoblasts, thus compromising osseointegration at the bone-implant interface. During culture under osteogenic conditions, exposure of human MSCs to submicron-size titanium particles suppresses bone sialoprotein gene expres-sion, reduces collagen type I and bone sialoprotein production, decreases cellular proliferation and viabil-ity, and inhibits matrix mineralization.64–66 Prolonged exposure of bone marrow cells in vivo to implant- derived wear debris may thus effectively diminish the population of viable MSCs and compromise their dif-ferentiation into functional osteoblasts, the long-term quality of periprosthetic bone tissue, and maintenance of osseointegration (Fig 7).
particle-mediated mSC Cytotoxicity Exposure to titanium particles also adversely affects human MSC viability through the induction of apop-tosis, eliciting increased levels of the tumor suppres-sor proteins p53 and p73 in a manner dependent on material composition, particle dosage, and exposure time.64 Interestingly, these effects on MSC prolifera-tion, apoptosis, and differentiation appear to be me-diated via particle endocytosis by the MSCs67 (Fig 8). CLSM was used to serially dissect the anatomy of an MSC exposed to submicron-sized titanium particles, and internalization of titanium particles was clearly demonstrated, showing localization and distribution within the cytoplasmic domain of the cell. Agents that disrupt endocytosis, such as cytochalasin D, protect the MSCs from these particle-mediated effects, in-cluding stimulation of apoptosis and suppression of osteogenic differentiation. Our recent unpublished findings (Haleem-Smith et al, in preparation, 2011)suggest that the endocytosed particles most likely
Fig 7 Schematic representation of the initiation and progression of wear debris particle–mediated osteolysis leading to implant loosening.
TiProsthesis
Bone
Bone
Titaniumparticles
Bone
Prosthesis
Generation and exposure to wear debris
•�Titanium�particles�produced�as� wear debris
•�Titanium�particles�localized�to� periprosthetic space
•�Titanium�particles�presented�to�bone�cells� (osteoblasts and osteoclasts), monocytes/ macrophages, and mesenchymal stem cells (MSCs)
Wear debris and MSC-mediated osteolysis
•�MSCs�endocytose�titanium�particles•�MSC�proliferation�decreased,�apoptosis�increased,� substrate adhesion reduced, and osteogenic differentiation suppressed
•�Rate�of�bone�resorption,�which�is�simula�ted�by�exposure�of macrophage, exceeds rate of bone formation
•�Perisprosthetic�space�enlarged•�Events�lead�to�aseptic�loosening�of�prosthesis
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

tuan et al
The International Journal of Oral & Maxillofacial Implants 59
disrupt the cytoskeletal integrity of the MSCs, prob-ably by virtue of their physical characteristics, thus dislocating or displacing subcellular organelles and cytoskeleton and compromising cellular functional activities, such as protein synthesis, secretion, motil-ity, and receptor signaling. Finally, it also appears that exposure to titanium particles and their subsequent endocytosis activates the expression and production of several proinflammatory cytokines by the MSCs, thus adding to the osteolytic influences already ex-erted by the particulates on the hematogenous cell populations resident in the periprosthetic tissue.
Recent studies using murine bone marrow–de-rived osteoprogenitor cells and the murine MC3T3 cell line have also noted suppressed proliferation and
differentiation of osteoprogenitors and decreased matrix calcification in the presence of polymethyl-methacrylate and polyethylene particles.68,69
genetIC COntrIbutIOn tO OSteOlySIS
A possible genetic contribution to the osteolytic re-sponse is suggested from the observed clinical varia-tions. In most diseases of multifactorial origin, both environmental and genetic factors contribute to dis-ease susceptibility. The heritable component arises from the interaction of multiple minor DNA sequence variations that occur with a stable frequency within the population. The subtle changes in gene function
Fig 8 Internalization of titanium particles by human MSCs. Cells were exposed to titanium particles (1,000/cell) and then stained with acridine orange and observed by CSLM. Optical sections parallel to the substrate were taken at 0.5-µm intervals. Internalized titanium particulates appeared in the sequential confocal sections as dark holes within the acridine orange–stained cytoplasm of the MSCs. Images shown are z–axis scan confocal sections paral-lel to the substrate traversing the entire cell body of a single MSC, showing multiple dark holes and clusters of dark holes fully surrounded by the cytoplasm. Bar = 20 µm.
a
e
i
b
f
j
c
g
k
d
h
l
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell therapy
60 Volume 26, Supplement, 2011
that result from these variations can give rise to al-tered susceptibility or severity for that disease. The most common form of these DNA sequence varia-tions consists of single letter changes in the genetic code for a gene, termed single nucleotide polymor-phism (SNPs). The human genome contains approxi-mately 10 million SNPs. Currently, relatively little is known about the role that this genetic variability may play in the development of periprosthetic osteolysis.
The genes encoding many of the cytokines impli-cated in osteolysis contain SNPs that are associated with other osteolytic diseases, including osteoporosis, periodontitis, and inflammatory arthritis. Recent data suggest that some of these SNPs also correlate with osteolysis after joint replacement. Wilkinson et al70 re-ported an association between the SNP at the -238 position in the tumor necrosis factor (TNF) gene pro-moter and osteolysis following cemented total hip arthroplasy. Independent of other known risk factors for osteolysis, the carriage rate of -238A in the osteoly-sis group was approximately twice that of the controls and the local background population (odds ratio 1.7). Carriage was highest in patients with osteolysis af-fecting both the pelvis and the femur (odds ratio 2.1). A subsequent functional analysis using a luciferase reporter gene assay suggested that the -238A allele resulted in increased TNF gene activation compared to the (more common) -238G allele, in response to stimulation with polyethylene particles. Subsequent studies have also implicated the genetic variability within the interleukin-1 (IL-1) gene cluster in the de-velopment of osteolysis. IL-1 receptor antagonist (IL-1RA) is an anti-inflammatory soluble peptide that blocks the activity of IL-1α and IL-1β. Patients carry-ing the IL-1RA +2018T allele variant are less likely to have osteolysis (odds ratio 0.6).
Another associated polymorphism has a likely re-lationship with the deleterious effects of wear debris particles on osteoprogenitor cell functions, specifi-cally related to the signaling mechanisms that regu-late their osteogenic differentiation activities. The gene FRZB encodes secreted frizzled-related protein 3, which plays a role in Wnt regulation of MSC osteo-genic differentiation. A recent study showed that the carriage of the FRZB200T allele (which results in sub-stitution of the amino acid arginine for tryptophan) was negatively associated with osteolysis (odds ratio 0.62) but positively associated with the development of heterotopic ossification after total hip arthroplas-ty.71 This study suggests that allelic variants of genes associated with bone formation pathways may play a role in modulating the risk of osteolysis and hetero-topic ossification after total joint replacement.
Future DIreCtIOnS FOr reSearCh
Optimal initiation of osseointegration and effective maintenance of the tissue/cell–implant interface in the face of continuous tissue remodeling are essential for long-term implant stability. The activities of mesen-chymal stem cells (MSCs), as candidate osteoprogeni-tor cells whose key role is to bring about functional de novo bone formation in the immediate periprosthetic zone, must be properly regulated so that the implant will continue to be “biocompatible” and the bone-im-plant complex can function as a single structural unit. An understanding of the cellular and molecular mech-anisms underlying the initiation and maintenance of the cell-implant interface is thus critical to future de-velopment of enhancement strategies. The studies described here present analytic approaches to under-standing these mechanisms that should lead to the development of a rational basis for such strategies. For example, activation or functionalization of the implant surface may promote more optimal cell adherence, although the enhancement must be by necessity dy-namic, and the extent of the “dwell time” of the cells on the surface must be properly timed to avoid interfer-ence with the subsequent remodeling that naturally occurs at a healthy interface. Studies of the immobiliza-tion of various bioactive molecular entities, such as ma-trix-integrin binding motifs72 and the sonic hedgehog N-terminal signaling domain,73 on biomaterial surfaces have reported promising results in the enhancement of osteogenic differentiation of MSCs. Essential for further development are functionally predictive tests, preferably in vitro, that will permit high-throughput evaluations prior to preclinical studies. On the wear de-bris–mediated osteolysis front, because the disruptive events take place considerably later in the lifetime of an implant, the challenges for interventional therapies are formidable, since this is likely initiated at different time points and is unlikely to be diagnosed or detected until substantial osteolysis has occurred. Some consid-eration may be given to targeting the control of the endocytotic events that are required for the particle-mediated effects on the MSCs. Osteoclastogenesis may be targeted via the manipulation of receptor activator of nuclear factor κB/osteoprotegerin activities and in-flammation via tumor necrosis factor blockade; how-ever, the systemic consequences of these candidate treatment approaches on the patient must be consid-ered carefully. Finally, new information on the genetic basis of susceptibility to implant loosening, a conse-quence of the rapid advancements in genomic scienc-es, will be extremely valuable in guiding dentists in terms of definitive clinical decisions. Optimization and prolongation of bony implant stability will continue to present exciting scientific and translational challenges
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

tuan et al
The International Journal of Oral & Maxillofacial Implants 61
for biologists, engineers, and clinicians working togeth-er to enhance performance and expand applications of such medical devices.
aCknOWleDgmentS
The author acknowledges the work of previous and present members of his laboratory who have contributed to the re-search data presented here, and the funding support of the Commonwealth of Pennsylvania Department of Health in the preparation of this manuscript.
reFerenCeS
1. Bostrom M, O’Keefe R. What experimental approaches (eg, in vivo, in vitro, tissue retrieval) are effective in investigat-ing the biologic effects of particles? J Am Acad Orthop Surg 2008;16(suppl 1):S63–S67.
2. Friedenstein AJ, Petrakova KV, Kurolesova AI, Frolova GP. Heterotopic of bone marrow. Analysis of precursor cells for osteogenic and hematopoietic tissues. Transplantation 1968; 6:230–247.
3. Caplan AI. Mesenchymal stem cells. J Orthop Res 1991;9: 641–650.
4. Pittenger MF, Mackay AM, Beck SC, et al. Multilineage potential of adult human mesenchymal stem cells. Science 1999;284:143–147.
5. Chen FH, Tuan RS. Mesenchymal stem cells in arthritic diseases. Arthritis Res Ther 2008;10:223.
6. Nöth U, Steinert AF, Tuan RS. Technology insight: Adult mes-enchymal stem cells for osteoarthritis therapy. Nat Clin Pract Rheumatol 2008;4:371–380.
7. Friedenstein AJ, Chailakhjan RK, Lalykina KS. The development of fibroblast colonies in monolayer cultures of guinea-pig bone marrow and spleen cells. Cell Tissue Kinet 1970;3: 393–403.
8. Kuhn NZ, Tuan RS. Regulation of stemness and stem cell niche of mesenchymal stem cells: Implications in tumorigen-esis and metastasis. J Cell Physiol 2010;222:268–277.
9. Kolf CM, Cho E, Tuan RS. Mesenchymal stromal cells. Biology of adult mesenchymal stem cells: Regulation of niche, self-renewal and differentiation. Arthritis Res Ther 2007;9:204.
10. Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006;8:315–317.
11. Nöth U, Osyczka AM, Tuli R, Hickok NJ, Danielson KG, Tuan RS. Multilineage mesenchymal differentiation potential of human trabecular bone-derived cells. J Orthop Res 2002;20: 1060–1069.
12. De Bari C, Dell’Accio F, Tylzanowski P, Luyten FP. Multipotent mesenchymal stem cells from adult human synovial mem-brane. Arthritis Rheum 2001;44:1928–1942.
13. Djouad F, Bony C, Haupl T, et al. Transcriptional profiles discrim-inate bone marrow derived and synovium-derived mesenchy-mal stem cells. Arthritis Res Ther 2007;9:R1304–R1315.
14. Hiraoka K, Grogan S, Olee T, Lotz M. Mesenchymal progeni-tor cells in adult human articular cartilage. Biorheology 2006;43:447–454.
15. Sekiya I, Larson BL, Vuoristo JT, Cui JG, Prockop DJ. Adipo-genic differentiation of human adult stem cells from bone marrow stroma (MSCs). J Bone Miner Res 2004;19:256–264.
16. Zuk PA, Zhu M, Mizuno H, et al. Multilineage cells from hu-man adipose tissue: Implications for cell-based therapies. Tissue Eng 2001;7:211–228.
17. Nesti LJ, Jackson WM, Shanti RM, et al. Differentiation poten-tial of multipotent progenitor cells derived from war-trauma-tized muscle tissue. J Bone Joint Surg Am 2008;90:2390–2398.
18. Janjanin S, Djouad F, Shanti RM, et al. Human palatine tonsil: A new potential tissue source of multipotent mesenchymal progenitor cells. Arthritis Res Ther 2008;10:R83.
19. Rzhaninova AA, Gornostaeva SN, Goldshtein DV. Isolation and phenotypical characterization of mesenchymal stem cells from human fetal thymus. Bull Exp Biol Med 2005;139:134–140.
20. Shih DT, Lee DC, Chen SC, et al. Isolation and characteriza-tion of neurogenic mesenchymal stem cells in human scalp tissue. Stem Cells 2005;23:1012–1020.
21. Cotsarelis G, Sun TT, Lavker RM. Label-retaining cells reside in the bulge area of pilosebaceous unit: Implications for follicular stem cells, hair cycle, and skin carcinogenesis. Cell 1990;61:1329–1337.
22. Sonoyama W, Liu Y, Yamaza T, et al. Characterization of the apical papilla and its residing stem cells from human immature permanent teeth: A pilot study. J Endod 2008;34:166–171.
23. Sarugaser R, Lickorish D, Baksh D, Hosseini MM, Davies JE. Human umbilical cord perivascular (HUCPV) cells: A source of mesenchymal progenitors. Stem Cells 2005;23:220–229.
24. Lee OK, Kuo TK, Chen WM, Lee KD, Hsieh SL, Chen TH. Isola-tion of multipotent mesenchymal stem cells from umbilical cord blood. Blood 2004;103:1669–1675.
25. Yen BL, Huang HI, Chien CC, et al. Isolation of multipotent cells from human term placenta. Stem Cells 2005;23:3–9.
26. Tuli R, Tuli S, Nandi S, et al. Characterization of multipotential mesenchymal progenitor cells derived from human trabecu-lar bone. Stem Cells 2003;21:681–693.
27. Song L, Young NJ, Webb NE, Tuan RS. Origin and character-ization of multipotential mesenchymal stem cells derived from adult human trabecular bone. Stem Cells Dev 2005;14: 712–721.
28. Tuli R, Nandi S, Li WJ, et al. Human mesenchymal progenitor cell-based tissue engineering of a single-unit osteochondral construct. Tissue Eng 2004;10:1169–1179.
29. Bruder SP, Jaiswal N, Ricalton NS, Mosca JD, Kraus KH, Kadiyala S. Mesenchymal stem cells in osteobiology and applied bone regeneration. Clin Orthop Relat Res 1998;355(suppl):S247–S256.
30. Lozito T, Kolf C, Tuan RS. Microenvironmental regulation of adult mesenchymal stem cells. In: Rajasekhar VK, Vemuri M (eds). Regulatory Networks in Stem Cells. New York: Humana Press, 2009:185–210.
31. Brånemark PI, Hansson BO, Adell et al. Osseointegrated im-plants in the treatment of the edentulous jaw. Scand J Plast Reconstr Surg 1997;16:1–132.
32. Sinha RK, Tuan RS. In vitro analysis of the bone-implant inter-face. Semin Arthroplasty 1996;7:47–57.
33. Sinha RK, Morris F, Shah SA, Tuan RS. Surface composition of orthopaedic implant metals regulates cell attachment spreading, and cytoskeletal organization of primary human osteoblasts in vitro. Clin Ortho 1994;305:258–272.
34. Shah AK, Sinha RK, Hickok NJ, Tuan RS. High resolution mor-phometric analysis of human osteoblast adhesion on clini-cally relevant orthopaedic alloys. Bone 1999;24: 499–506.
35. Shah AK, Lazatin J, Sinha RK, Lennox T, Hickok NJ, Tuan RS. Mechanism of BMP-2 stimulated osteoblast adhesion to orthopaedic biomaterials. Biol Cell 1999;91:131–142.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell therapy
62 Volume 26, Supplement, 2011
36. Groessner-Schreiber B, Tuan RS. Enhanced extracellular matrix production and mineralization by calvarial osteoblasts cul-tured on titanium surfaces in vitro. J Cell Sci 1992;101:209–217.
37. Frisch SM, Vuori K, Ruoslahti E, Chan-Hui P-Y. Control of adhesion-dependent cell survival by focal adhesion kinase. J Cell Biol 1996;134:793–799.
38. Hynes RO. Integrins: Bidirectional, allosteric signaling ma-chines. Cell 2002;110:673–687.
39. Schaller MD, Parsons JT. Focal adhesion kinase and associ-ated proteins. Curr Opin Cell Biol 1994;6:705–710.
40. Myllymaa S, Kaivosoja E, Myllymaa K, et al. Adhesion, spread-ing and osteogenic differentiation of mesenchymal stem cells cultured on micropatterned amorphous diamond, tita-nium, tantalum and chromium coatings on silicon. J Mater Sci Mater Med 2010;21:329–341.
41. Olivares-Navarrete R, Hyzy S, Wieland M, Boyan BD, Schwartz Z. The roles of Wnt signaling modulators Dickkopf-1 (Dkk1) and Dickkopf-2 (Dkk2) and cell maturation state in osteo-genesis on microstructured titanium surfaces. Biomaterials 2010;31:2015–2024.
42. Dohan Ehrenfest DM, Coelho PG, Kang BS, Sul YT, Albrekts-son T. Classification of osseointegrated implant surfaces: Materials, chemistry and topography. Trends Biotechnol 2010;28:198–206.
43. Hickok NJ, Nöth U, Seghatoleslami R, et al. Integrin function and activation of signaling pathways in osteoblastic cells. Osteologie 2002;11:75–85.
44. Nöth U, Tuli R, Seghatoleslami R, et al. Activation of p38 and Smads mediates BMP-2 effects on human trabecular bone-derived osteoblasts. Exp Cell Res 2003;291:201–211.
45. Bobyn JD, Engh CA. Human histology of the bone-porous metal implant interface. Orthopaedics 1984;7:1410–1422.
46. Goldring SR, Jasty M, Roelke MS, Rourke CM, Bringhurst FR, Harris WH. Formation of a synovial like membrane at the bone-cement interface. Its role in bone resorption and im-plant loosening after total hip replacement. Arthritis Rheum 1986;29:836–842.
47. Harris WH, Schiller AL, Scholler JM, Freiberg RA, Scott R. Extensive localized bone resorption in the femur following total hip replacement. J Bone Joint Surg Am 1976;58:612–618.
48. Maloney WJ, Smith RL, Schmalzried TP, Chiba J, Huene D, Rubash H. Isolation and characterization of wear particles gen-erated in patients who have had failure of a hip arthroplasty without cement. J Bone Joint Surg Am 1995;77:1301–1310.
49. Konttinen YT, Zhao D, Beklen A, et al. The microenvironment around total hip replacement prostheses. Clin Orthop Relat Res 2005;430:28–38.
50. Newby AC. Metalloproteinase expression in monocytes and macrophages and its relationship to atherosclerotic plaque instability. Arterioscler Thromb Vasc Biol 2008;28:2108–2114.
51. Tuan RS, Lee FY, T Konttinen Y, Wilkinson JM, Smith RL. What are the local and systemic biologic reactions and mediators to wear debris, and what host factors determine or modulate the biologic response to wear particles? J Am Acad Orthop Surg 2008;16:S42–S48.
52. Lassus J, Salo J, Jiranek WA, et al. Macrophage activation re-sults in bone resorption. Clin Orthop Relat Res 1998;352:7–15.
53. Leibbrandt A, Penninger JM. RANKL/RANK as key factors for osteoclast development and bone loss in arthropathies. Adv Exp Med Biol 2009;649:100–113.
54. Ramage SC, Urban NH, Jiranek WA, Maiti A, Beckman MJ. Expression of RANKL in osteolytic membranes: Association with fibroblastic cell markers. J Bone Joint Surg Am 2007; 89:841–848.
55. Koreny T, Tunyogi-Csapo M, Gal I, Vermes C, Jacobs JJ, Glant TT. The role of fibroblasts and fibroblast-derived factors in periprosthetic osteolysis. Arthritis Rheum 2006:54:3221–3232.
56. Seo S, Lee D, Cho S, et al. ERK signaling regulates macro-phage colony-stimulating factor expression induced by tita-nium particles in MC3T3.E1 murine calvarial preosteoblastic cells. Ann N Y Acad Sci 2007;1117:151–158.
57. Shanbhag AS, Kaufman AM, Hayata K, Rubash HE. Assessing osteolysis with use of high-throughput protein chips. J Bone Joint Surg Am 2007;89:1081–1089.
58. Santerre JP, Labow RS, Boynton EL. The role of the macrophage in periprosthetic bone loss. Can J Surg 2000;43:173–179.
59. Haynes DR. Bone lysis and inflammation. Inflamm Res 2004; 53:596–600.
60. Yao J, Cs-Szabo G, Jacobs JJ, Kuettner KE, Glant TT. Suppres-sion of osteoblast function by titanium particles. J Bone Joint Surg Am 1997;79:107–112.
61. Pioletti DP, Takei H, Kwon SY, Wood D, Sung KL. The cytotoxic effect of titanium particles phagocytosed by osteoblasts. J Biomed Mater Res 1999;46:399–407.
62. Kwon SY, Lin T, Takei H, et al. Alterations in the adhesion behavior of osteoblasts by titanium particle loading: Inhibi-tion of cell function and gene expression. Biorheology 2001;38:161–183.
63. Fritz EA, Glant TT, Vermes C, Jacobs JJ, Roebuck KA. Che-mokine gene activation in human bone marrow-derived osteoblasts following exposure to particulate wear debris. J Biomed Mater Res A 2006;77:192–201.
64. Wang ML, Tuli R, Manner PA, Sharkey PF, Hall DJ, Tuan RS. Direct and indirect induction of apoptosis in human mesen-chymal stem cells in response to titanium particles. J Orthop Res 2003;21:697–707.
65. Wang ML, Nesti LJ, Tuli R, et al. Titanium particles suppress expression of osteoblastic phenotype in human mesenchy-mal stem cells. J Orthop Res 2002;20:1175–1184.
66. Wang ML, Sharkey PF, Tuan RS. Particle bioreactivity and wear-mediated osteolysis. J Arthroplasty 2004;19:1028–1038.
67. Okafor CC, Haleem-Smith H, Laqueriere P, Manner PA, Tuan RS. Particulate endocytosis mediates biological responses of human mesenchymal stem cells to titanium wear debris. J Orthop Res 2006;24:461–473.
68. Chiu R, Ma T, Smith RL, Goodman SB. Kinetics of polymethyl-methacrylate particle-induced inhibition of osteoprogenitor differentiation and proliferation. J Orthop Res 2007;25:450–457.
69. Chiu R, Ma T, Smith RL, Goodman SB. Polymethylmeth-acrylate particles inhibit osteoblastic differentiation of bone marrow osteoprogenitor cells. J Biomed Mater Res A 2006;77:850–856.
70. Wilkinson JM, Wilson AG, Stockley I, et al. Variation in the TNF gene promoter and risk of osteolysis after total hip arthro-plasty. J Bone Miner Res 2003;18:1995–2001.
71. Gordon A, Southam L, Loughlin J, et al. Variation in the secreted frizzled-related protein-3 gene and risk of osteolysis and heterotopic ossification after total hip arthroplasty. J Orthop Res 2007;25:1665–1670.
72. Avila G, Misch K, Galindo-Moreno P, Wang HL. Implant surface treatment using biomimetic agents. Implant Dent 2009;18:17–26.
73. Ho JE, Chung EH, Wall S, Schaffer DV, Healy KE. Immobilized sonic hedgehog N-terminal signaling domain enhances differentiation of bone marrow-derived mesenchymal stem cells. J Biomed Mater Res A 2007;15;83:1200–1208.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 63
Stem Cell Therapy Group Members
Group ChairTara L. Aghaloo, DDS, MD, PhD
Group ExpertRocky Tuan, PhD
Group SecretaryJohn P. Schmitz, DDS, PhD
Group ParticipantsMarcus Aboud, DMD
Edward Amet, DDS, BS, MSD
Guiseppe Cardaropoli, DDS, PhD
Steve Eckert, DDS, MS
Neal Garret, PhD
Joe Gian-Grasso, DMD
Clarence Lindquist, DDS
Martina Lulic, DDS
Richard Nejat, DDS
Thomas Oates, DMD, PhD
Mariano Sanz, MD, DDS
Lubivico Sbordone, MD, DDS
Henning Schliephake, DDS, MS, PhD
Minoru Ueda, DDS, PhD
Dan Ammon (DENTSPLY)Donald Clem, DDS (AAP)Gina DeSimone (Silent Participant, Straumann)
Susan Drapeau, PhD (Medtronic)Arthur Jee, DMD (AAOMS)
Robert Marx, DMD (Quintessence)Hai Bo Wen (Zimmer)Jennifer Woodell-May, PhD (Biomet 3i)
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

64 Volume 26, Supplement, 2011
Stem cells (SCs) are cells with the potential to de-velop into many different tissue types during early
life and growth. They may also serve to provide an enduring internal repair system to replenish other cell types throughout life. Stem cells are characterized in several ways: (1) they are unspecialized, (2) they are capable of renewing themselves through mitosis, and (3) they can be induced to develop into tissue-specific or organ-specific cells. Stem cells are also flexible, where they can be quiescent or proliferating, and they demonstrate plasticity, where they can dif-ferentiate or dedifferentiate. Stem cells can optimize tissue regeneration and repair as well as provide the targeted delivery of genetic material. Opportunities in implant dentistry exist in the areas of alveolar bone and soft tissue regeneration and repair. Evidence of the commercial interest in stem cell therapy is al-ready present as companies are marketing centrifug-es to concentrate bone marrow aspirate and delivery devices. The promise of stem cell therapy offers vast opportunities in all areas of dentistry and medicine. The modality of allogeneic stem cells as a tissue bank product is already available commercially, as well as three companies offering to bank stem cells from ex-tracted teeth.
Several types of stem cells exist; each with their own set of advantages and ethical dilemmas. Adult or somatic stem cells are isolated from adults, while embryonic stem cells (ESCs) are derived from the blastocyst of embryos (usually from unused eggs fer-tilized via in vitro fertilization techniques). ESCs are pluripotent, remain undifferentiated, and have the ability to differentiate into any cell type. In addition to the ethical and political concerns, ESCs may form teratomas and potentially induce host rejection since they are allogeneic. The most recent stem cell type is induced pluripotent stem cells (iPS cells), which are reprogrammed adult human dermal fibroblasts that are pluripotent, similar to ESCs.
Due to the intense ethical debate regarding ESCs and the relative juvenile research of iPS cells, the dis-cussions in the stem cell group focused only on adult stem cells, mostly mesenchymal stem cells (MSCs). MSCs fulfill the definition of stem cells, in that they possess self-renewal, are nonimmunogenic, and can differentiate into cells of many types including: osteo-blasts, chondrocytes, and adipocytes. Initial isolation of MSCs was defined by their ability to adhere to a plastic culture plate, separating them from hemato-poietic stem cells that do not. The MSC ability to form colonies in colony forming units-fibroblastic (CFU-F)
is also important, as are particular markers that are often utilized for MSC sorting, including: STRO-1, CD73, CD146, CD106 positivity, and CD11B, CD45, CD34, CD31, and CD117 negativity.
The following questions were provided to the stem cell group to be highlighted in the discussion and consensus in the focused group session.
What is the primary rationale for the development of the technology?
Stem cell therapy has been utilized for decades in the form of stem cell transplants for leukemia and other malignancies, as well as autogenous grafts from the iliac crest to transplant osteocompetent cells to other locations, including spine and tibia in orthopedic sur-gery and the jaws in dentistry. Although bone mar-row mesenchymal stem cells (BMSCs) are the most commonly used stem cells for transplantation, the explosion of stem cell research has identified other stem cell populations in adipose tissue, bone, brain, liver, lung, kidney, periosteum, muscle, umbilical cord blood, dental pulp, exfoliated deciduous teeth, peri-odontal ligament, apical papilla, and dental follicle. One obvious advantage of stem cell use in dentistry is to regenerate oral tissues, including: bone, gingiva, periodontal ligament, nerves, mucosa, and muscle, as well as more complex structures such as entire teeth, jaws, and face. The advantages of tissue regeneration with stem cells are the potential to regenerate these structures to their original state without scar forma-tion or a surgical transition zone as is seen with cur-rent hard and soft tissue grafting techniques. In terms of regenerating entire complex tissues, significant re-search, both preclinical and clinical, needs to be per-formed until it is available for the practicing clinician.
Even before stem cell therapy is used to replace our current grafting materials and techniques, it can be combined with the clinicians’ graft of choice. This is al-ready occurring either in clinical or preclinical studies with both autogenous and allogeneic preparations of stem cells including: bone marrow aspirate, adipose, and allogeneic marrow sources. These techniques have the ability to decrease donor site morbidity as compared to large autogenous bone harvesting, lon-ger surgical procedures, and limited bone availability, especially in elderly patients.
Stem Cell Therapy Group Report
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell Therapy Group
The International Journal of Oral & Maxillofacial Implants 65
A consensus was obtained on several primary ratio-nales for development of this technology: First, was the ability to enhance oral tissue regeneration of bone, gin-giva, and nerve; second, to reduce donor site morbidity; third, to reduce the incidence of complications; fourth, to be able to deliver predictable implant site develop-ment in medically compromised patients; and finally, to collaborate with medical colleagues/companies to fur-ther develop SC therapy for dental implant treatment.
It is hypothesized that we will be able to deliver predictable implant and site development therapy to patients that are not generally candidates for compli-cated tissue regeneration required for implant place-ment, such as patients with compromised wound healing, severe systemic diseases, and those with lo-cally compromised sites from significant bone and soft tissue loss or previous therapy failure. Finally, oral health-care providers are in the perfect position to collaborate with our medical colleagues and industry to further develop stem cell therapy to enhance the field of implant dentistry. With the abundance of stem cell sources in the oral and maxillofacial region and our experience with multiple sites of hard and soft tis-sue grafting, these goals are practical and achievable.
What is the potential for stem cell therapy to im-prove clinical outcomes in dental implant therapy?
Although dental implant success rates are generally greater than 90% to 95%, and are related to osseoin-tegration, clinicians, scientists, and the industry rec-ognize the need for continued improvement using SC therapy. Mesenchymal stem cells (MSCs) in an osteo-genic microenvironment, such as an implant osteoto-my site, provide the necessary factors for osteoblastic differentiation and bone formation. Because stem cells would be directly implanted into the site in order to enable them to respond to signaling molecules, they would decrease the need for a membrane, and could be a single product without the need for other adjuncts. It is anticipated that bone quality would be significantly improved and could contribute to en-hanced long-term success. Potentially, this is most im-portant for patients with compromised vascular and wound healing problems. Eventually, will it become possible to develop a stem cell/bone composite where cells would form bone onto the implant first, then be implanted? A common reason for improving current techniques, especially implant surface tech-nology, is to deliver predictable and improved results in these compromised patients.
A very common problem in our medically compro-mised patients, or in locally compromised sites, is lack of vascularity. It is well known that bone formation
occurs only in adequately vascularized sites. In this case, the use of stem cells may have the ability to im-prove vascularity specifically for hard tissue augmenta-tion in these compromised patients and local sites, since bone forming cells and their stem cell precursors are often found in close proximity to the vasculature. As previously stated, the use of stem cell therapy has the most potential for use in any site where the clinician would have otherwise chosen an autogenous bone graft, such as in sinus augmentations, vertical alveolar ridge augmentation, and large maxillary or mandibular defects. The authors recognize, however, that this tech-nology and its specific utilization will depend on the size and shape of each individual defect.
What kinds of patients are most likely to need, want, or be candidates for stem cell treatment/ technology?
As discussed above, stem cell therapy has the ability to repair and regenerate tissues, including bone, car-tilage, muscle, brain and spinal cord, teeth, liver, and many others. In fact, animal studies have demonstrat-ed success in many of these areas. Specifically in im-plant dentistry, patients with compromised healing, or those who require hard and/or soft tissue augmen-tation that cannot be treated by conventional meth-ods for site development before implant placement, are potential patients. This is especially the case when an autogenous graft would otherwise be necessary. Again, it is important to stress that the specific stem cell therapy should be chosen and adapted to fit each individual defect.
In the stem cell group discussion, clinicians fa-vored stem cell therapy for the most challenging defects and patients. That is for those patients who would need an autogenous bone graft, and for medi-cally compromised patients with conditions such as diabetics, for smokers, and for patients with previous radiation therapy, who may not be candidates for tra-ditional therapy or in whom previous therapies have failed. However, many unknowns exist with any new technology, including stem cell therapy, and it is un-clear whether certain diseases or medications would negatively affect MSC differentiation or function when harvested from an autogenous source. To an-swer all of these questions and concerns, when stem cell therapy is utilized, clinicians should design trials with the proper control groups and documentation to produce credible and publishable data so that re-searchers can continue to advance the field with sci-entific evidence that can ultimately improve patient care. The stem cell group recognizes, however, that with any new therapy, the popularity and desire for
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell Therapy Group
66 Volume 26, Supplement, 2011
use may be driven by technology-prone patients and/or clinicians, rather than by proven indications or effi-cacy when compared to a more traditional technique.
What is the potential for stem cell therapy to im-prove a patient’s physical health and quality of life?
Animal and human studies have demonstrated the ability of SC therapy, specifically MSCs, to regenerate tissues. Nevertheless, the question of quality of life has not yet been addressed. If stem cells replace au-togenous tissue harvesting, then the impact on phys-ical health by lack of a donor site would be quickly realized. This is also consistent with minimal inter-ruptions in daily life from a physical, psychological, and economic standpoint. For these reasons, there is a potential for improved quality of life, especially in patients who may not be candidates for dental im-plants because of compromised medical issues. SCs must be able to stimulate bone and/or gingiva forma-tion in challenging patients. This therapy must return patients to a normal life sooner. Finally, great enthu-siasm exists for SC therapy to provide more predict-able results. However, studies specifically addressing these questions must be performed and validated for SC therapy, just as they have been for other previous new technologies such as dental implants.
Is the current evidence sufficient to warrant further research and resources being directed toward stem cells for dental implant therapy?
Of course the short answer here is “yes” because preliminary success has been seen, especially with BMSCs for bone repair and regeneration. This has prompted use in the clinic for both autogenous and allogeneic stem cell preparations. But, little is known about these technologies in humans. Are they actu-ally stem cells that express the positive and negative markers as defined by the FDA and International So-ciety for Cell Therapy? Are they self-renewing once implanted in vivo in humans? May the trilineal mes-enchymal precursor be qualified as a stem cell?1 How does use of these stem cell preparations compare with traditional therapies directly? Recent studies are beginning to have some select answers, but much more research is required for definitive answers. It is also likely that multiple new technologies will need to be combined to regenerate more complex defects that often present in our implant patients, in a tissue engineering approach using cells, scaffolds, and sig-naling molecules.
What additional evidence should be gathered to enhance development and enable transfer of stem cell technology?
It is well known that the cost of health care in the Unit-ed States continues to increase, and this is likely to continue if new health-care technologies are utilized. Therefore, it is important to evaluate new technolo-gies by objective assessments to determine if the ben-efits outweigh the large costs. Specific and important questions related to health-technology assessment of SCs include: What would be the health impact? The budgetary impact? Cost effectiveness? Opportunity costs? Ethical, legal, and social issues? These issues are easy to overlook, as new technologies are often driving the research and development, rather than underlying biological hypotheses. In the sections be-low, the stem cell group discussed the additional evi-dence needed to enhance development and enable its transfer for use in implant dentistry, but keep in mind that only by health-technology assessment will clinical efficacy, effectiveness, ethics and equity, eco-nomics, and societal preference of stem cell therapy be evaluated.
For the purposes of the questions below, the stem cell group focused on adult stem cells, specifi-cally BMSCs, since these are most commonly utilized with either devices or products that are commercially available. The group also divided adult BMSC therapy into autogenous and allogeneic preparations, and both will be discussed below.
What are the technical properties associated with adult stem cells?
In terms of technical properties, there is significant evidence that should be gathered to enhance the development and enable transfer of stem cell ther-apy for implant dentistry, especially for implant site development. This proof of concept should include radiographic validation of bone regeneration, his-tomorphometry, dental implant survivability, and validation of SC content (markers, viability, colony-forming units, etc). These need to be compared to au-togenous preparations, totally devitalized allografts, and available growth factors in critical-size bone de-fects. For autogenous preparations, the patient’s age and viability of harvested cells are of primary impor-tance. But questions emerge when considering the number of stem cells in the bone marrow, which is generally thought to decrease with age. In addition to a decrease in population doublings, an increase in signs of senescence and a decrease in differentiation
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell Therapy Group
The International Journal of Oral & Maxillofacial Implants 67
capacity occurs. How viable are the isolated MSCs in terms of CFU-Fs, surface markers, and in vivo func-tion? As discussed above, the FDA and International Society for Cellular Therapy defines an MSC as an in vitro adherent cell that is positive for CD105, CD73, and CD90, and negative for CD45, CD34, CD14, CD11B, CD79a, and HLA-DR, with some minor varia-tions. Should MSCs undergo partial or terminal dif-ferentiation to the desired phenotype in vitro before they are implanted? Or, if they are placed in the prop-er microenvironment, will MSCs become the desired cell? Obviously specialized equipment is required for harvesting, isolating, and culturing autologous MSCs, and it will take time to determine the ideal isolation and manipulation procedure. There are certain sup-plies, as well as technical skills, needed by the clinician and support staff, and perhaps a successful isolation will depend on the skill of the operator.
Some of the technical properties with the use of allogeneic MSCs are similar to autogenous MSCs, such as donor age and viability and characteriza-tion of stem cells. Other issues unique to allogeneic MSCs also pose many challenges, such as methods of processing so that viability and “stemness” including multipotency and self-renewal are maintained. Allo-geneic MSCs must be transported to the operating room or office and stored until ready for use. These products often have a short window of use, which may pose significant problems if scheduling issues arise where procedures are changed or cancelled.
What are the safety issues associated with adult stem cells?
In terms of safety with autogenous MSCs, bone mar-row transplants have been performed for decades for hematologic and genetic diseases, and in the form of autogenous bone grafts from the iliac crest. There is no risk with autogenous preparations in terms of dis-ease transmission, rejection, or other routine safety concerns. However, similar to blood or other fluids or tissues prepared ex vivo, significant risk of clerical er-ror exists. Of course this risk is greater if cells are har-vested and cultured or differentiated ex vivo before they are implanted, and less if they are reimplanted immediately to the recipient site. The risk of infection also exists during processing of isolated cells, which can again be increased with ex vivo culture if there is a breakdown in sterile technique. In addition, true MSCs may retain their plasticity after transplantation and, depending on their microenvironment, they have the ability to differentiate, dedifferentiate, or re-differentiate into a different cell type than originally desired. This lack of control of MSCs poses some safe-
ty risks, where MSCs have demonstrated malignant transformation, either by telomerase gene transfer, clonal selection from ex vivo expansion, and other mechanisms resulting in several types of cancer.
Concerns certainly exist regarding the safety of al-logeneic MSCs. Primarily, this is because it is impossi-ble to screen for all known diseases or potentially new ones. It is already well-known that SCs can form tera-tomas or genetic mutations without phenotypic signs of disease that in a new, specific microenvironment or matrix can change cellular differentiation. Although allogeneic stem cell transplants are routinely utilized for cancers and allogeneic organs for transplantation, patients must either receive a human leukocyte anti-gen (HLA)-identical donor or undergo lifetime immu-nosuppression, respectively. Transplanted allogeneic MSCs are generally not rejected by the recipient host, although there are reports of immunogenic respons-es to allogeneic MSCs in vivo, even if no response was elicited in vitro.
Allogeneic MSCs for bone augmentation do not seem to carry these risks and, in fact, clinical case re-ports demonstrate at least short-term safety. Indeed, many products are screened to prevent disease trans-mission similar to allogeneic bone or skin. However, clinicians should be aware that only known diseases with available screening tests can be ruled out, and this does not guarantee that other less common or unknown diseases or infections may not occur in the future. Governmental agencies like the Food and Drug Administration (FDA) have produced guidelines to regulate stem cell-based products so that patients are not exposed to significant and unreasonable risk to permit initiation of human clinical studies. How-ever, currently available allogeneic stem cell prod-ucts are not regulated by the FDA, but instead by the American Association of Tissue Banks (AATB). Another potential safety issue unique to allogeneic stem cells is that since they must maintain their viability in order to differentiate into the desired cell type, the live cells may contain genetic mutations without any pheno-typic signs of disease that when placed into a specific host or environment may become pathologic. Cases reported in the literature demonstrate that trans-planted allogeneic stem cells may lead to tumor for-mation or teratomas.
Routine and often cumbersome testing is required to safeguard against the transmission of infectious and molecular disease. The latter is the risk most of-ten overlooked. For example, embryos derived from a donor with a family history of bone formative disease (eg, osteopetrosis) may not be the best suited donor to use as a stem cell graft for an alveolar ridge defect.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell Therapy Group
68 Volume 26, Supplement, 2011
What are the efficacy and effectiveness issues asso-ciated with adult stem cells?
Efficacy and effectiveness are very important in en-hancing development and enabling transfer of new technologies such as stem cell therapy. Generally, efficacy is determined first where a new technology would be studied under ideal conditions such as in a controlled, hospital setting with expert clinicians in the field to evaluate if the treatment in question works. Then, effectiveness should be determined employing community-based studies under routine or normal circumstances. For autogenous MSCs, for example, they should be compared to standard bone grafting materials if their efficacy and effectiveness is being evaluated for use to augment alveolar bone in preparation for implant placement. Radiographic, his-tologic, and implant survival and success rates should be equivalent with autogenous MSCs compared to the “gold standard” for each specific defect or indica-tion. Patient-reported outcomes are also important here, including physiological or functional impact (speech, swallowing, chewing, nutrition, motor and sensory function), psychological impact (satisfaction, self-image and confidence, esthetics, perception of function, and quality of life), and economic impact of treatment (direct and indirect costs, maintenance costs, third party, and disparities). When evaluat-ing efficacy and effectiveness, it must be taken into consideration that the type of stem cell therapy se-lected must be specific to the defect size, shape, and patient’s medical condition, and these factors will all require well-designed clinical studies. For allogeneic MSCs, a very similar process of study should be fol-lowed to determine efficacy and effectiveness, and only after these appropriate studies will it be clear what the specific indications are for use of particular MSC preparations.
What are the economic factors associated with adult stem cells?
Economic factors surrounding stem cell therapy must be answered in the future with correlation to efficacy and effectiveness. This is where health-technology as-sessment may play an important role in determining which new technologies should be developed and transferred into mainstream medicine. Specifically for autogenous MSCs, the costs will vary depending on the specific defect size and location, complexity of the tissue or organ being regenerated, and what additional materials or factors such as scaffolds or growth factors will be utilized in combination. Cur-rently, there are devices available to harvest, isolate,
and concentrate stem cells that would incur signifi-cant upfront costs. Then, if further ex vivo culturing to differentiate cells down a specific lineage is required, the costs will be increased.
The alternative is true for allogeneic MSC prepara-tions where costs will be specific and limited to each patient or procedure, with little to no upfront costs. Obviously, minimal additional equipment is required for use, except perhaps a water bath or –20°C freezer for thawing cells and storage, respectively. However, potential increased costs are possible per procedure, for example, if MSCs are ordered and patients resched-ule or cancel a planned surgery, especially if allogeneic products have a limited shelf-life. Costs may further increase if more stringent governmental regulation or disease screening becomes an important factor in the future. In this era of exponentially increasing health-care costs, it is always important for clinicians and scientists to keep economic factors in mind when evaluating new technologies. Availability of health-technology assessments may prove an effective meth-od for determining which of these new technologies should be developed and transferred into mainstream implant dentistry practices.
What are the legal and ethical issues associated with adult stem cells?
Sometimes there may be difficulty incorporating new technologies into mainstream clinical practice. It is well accepted that dental implant success gener-ally ranges from 90% to 95%. Specifically for stem cell therapy, minimal human studies exist and no long-term studies demonstrate efficacy and effectiveness, safety, or economic factors. If this is the case, how can clinicians ethically recommend stem cell therapy for their patients? Also, importantly, how do clinicians know current and future legal ramifications of stem cell therapy, either autogenous or allogeneic, when long-term safety issues are still unknown?
Legal and ethical issues are also important when the clinician chooses a new technology like stem cell therapy that is a support for good clinical technique, but is not a substitute for appropriate skill and training. The converse is also true, where the new technology should not be so complicated and technique sensi-tive that only 1% to 2% of all clinicians will be able to utilize stem cells. If and when adequate efficacy and effectiveness trials are available with minimal safety concerns, clinicians may be obligated to consider stem cell therapy, especially if certain procedures can be performed in a more minimally invasive manner. Finally, clinicians must provide an honest appraisal of their skill sets, comfort levels, and knowledge of each
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Stem Cell Therapy Group
The International Journal of Oral & Maxillofacial Implants 69
new technology. This is often difficult because there may be lots of health-care dollars involved, which can provide incentives to cut corners with any of the above concerns or with gathering enough evidence to develop and transfer stem cell therapy.
ConCluSionS
The stem cell group at the Academy of Osseointe-gration’s Silver Anniversary Summit on the impact of biological and technological advances on implant dentistry unanimously felt that stem cell therapy will have a significant impact on the field in both the near and distant future, especially through the enhance-ment of our current techniques for hard and soft tis-sue regeneration, while allowing clinicians to treat a population of patients that otherwise would not be candidates for routine dental implant therapy. How-ever, in addition to the isolation of autogenous or al-logeneic MSCs, implanting them on the appropriate carrier to maximize hard or soft tissue regeneration poses many challenges. As demonstrated from the use of growth factors, carriers are of the utmost im-portance and significant tissue regeneration cannot be maximized without adequate vascularity. On a fi-nal note, the topics for discussion at the summit were divided into nanotechnology, stem cell therapy, bio-engineering (or tissue engineering), and growth and differentiation, but the stem cell group would like to emphasize that it will likely be a combination of all of these new technologies that ultimately enhances the ability to regenerate hard and soft tissues and el-evates the field of implant dentistry to the next level.
The Stem Cell Therapy Group prepared a list of 17 references as a Reading List for the summit participants (references 2 through 18).
RefeRenCeS
1. Charbord P. Bone marrow mesenchymal stem cells: Historical overview and concepts. Hum Gene Ther 2010;21:1045–1056.
2. Amariglio N, Hirshberg A, Scheithauer BW, et al. Donor-derived brain tumor following neural stem cell transplantation in an ataxia telangiectasia patient. J Inflamm 2009;6:221–230.
3. Bianco P, Riminucci N, Gronthos S, Robey PG. Bone marrow stromal stem cells: Nature, biology, and potential applications. Stem Cells 2001;19:180–192.
4. Blanco P, Kuxnetsov SA, Riminucci M, Fisher LW, Spiegel AM, Robey PG. Reproduction of human fibrous dysplasia of bone in immuncompromised mice by transplanted mosiacs of nor-mal and Gsa-mutated skeletal progenitor cells. J Clin Investig 1998;101:1737–1744.
5. Engler AJ, Sen S, Sweeney HL, Discher DE. Matrix elasticity directs stem cell lineage specification. Cell 2006;126:677–689.
6. Friedenstein AJ, Piatetzky-Shapiro II, Petrakova KV. Osteo-genesis in transplants of bone marrow cells. J Embryol Exp Morph 1996;16:381–390.
7. Gerson SL. Mesenchymal stem cells: No longer second class marrow citizens. Nature Med 1999;5:262–264.
8. Grayson WL, Frohlich M, Yeager K, et al. Engineering ana-tomically shaped human bone grafts. Proc Natl Acad Sci USA 2010;107:3299–3304.
9. Haynesworth SE, Goshima J, Goldberg VM, Caplan AI. Char-acterization of cells with osteogenic potential from human marrow. Bone 1992;13:81–88.
10. Jukes JM, Both SK, Leusink A, Sterk LM, Van Blitterswijk CA. Endochondral bone tissue engineering using embryonic stem cells. Proc Natl Acad Sci USA 2008;105:6840–6845.
11. Lendeckel S, Jodicke A, Christophis P, et al. Autologous stem cells (adipose) and fibrin glue used to treat widespread trau-matic calvarial defects: Case report. J Cranio-maxillofac Surg 2004;32:370–373.
12. Marolt D, Knezevic M, Novakovic GV. Bone tissue engineering with human stem cells. Stem Cel Res Ther 2010;1:1–10.
13. McAllister BS, Haghighat K, Gonshor A. Histologic evaluation of a stem cell-based sinus-augmentation procedure. J Periodontol 2009;80:679–686.
14. Ryan JM, Barry FP, Murphy JM, Mahon BP. Mesenchymal stem cells avoid allogeneic rejection. J Inflamm 2005;2:1–11.
15. Schieke SM, Ma M, Cao L, et al. Mitochondrial metabolism modulates differentiation and teratoma formation capacity in mouse embryonic stem cells. J Biol Chem 2008;283: 28506–28512.
16. Siddappa R, Martens A, Doorn J, et al. cAMP/PKA pathway activation in human mesenchymal stem cells in vitro results in robust bone formation in vivo. Proc Natl Acad Sci USA 2008; 105:7281–7286.
17. Steinhardt Y, Aslan H, Regev E, et al. Maxillofacial-derived stem cells regenerate critical mandibular bone defefcts. Tissue Eng 2008;14:1763–1773.
18. Wang C-Y, Zhao B-H, Ai H-J, Wand Y-W. Comparison of biological characteristics of mesenchymal stem cells grown on two different titatnium implant surfaces. Biomed Mater 2008;3:1–6.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

70 Volume 26, Supplement, 2011
Growth and differentiation
Significant advancements in the fields of tooth re-placement and bone tissue engineering have been
made since the first characterization of the bone mor-phogenetic family of proteins (BMPs) in 1965.1 This discovery coincides with the placement of the first human titanium root-form dental implant that had significant research to support its use.2 Though they originated at nearly the same time, the first publica-tions suggesting the combined use of soluble factors such as BMPs and dental implants did not appear un-til 28 years later, in 1993.3 Even without additional os-teogenic factors, the success rates of osseointegrated
titanium implants have reached 95.6% to 97.5%, even in settings where the majority of patients are medi-cally compromised or current or former smokers.4,5 For those who are candidates for dental implants, this success rate is extraordinary. As such, technologic ad-vancements to bring implant therapy to patients pre-viously excluded as implant candidates for reasons related to insufficient bone quality or volume are desired. This article will address current therapeutics designed to address osseous deficiencies and outline novel strategies that may prove beneficial for future implant therapeutics.
introdUCtion to the Bone Marrow
Largely as the result of the use of marrow as a food source, it has long been recognized that bone marrow composition varies by site, with the more red marrow being confined to the middle of the animal and the yellow, or fatty, marrow existing toward the periphery. Indeed, the initial inclusion of meat into the homi-nid diet 2.6 million years ago was inferred following evidence of bone marrow removal shown by impact fractures from stone tools on sections of ungulate
1 DDS/PhD Student, Department of Biologic and Materials Sciences, University of Michigan at Ann Arbor.
2 Professor, Department of Biologic and Materials Sciences, University of Michigan at Ann Arbor.
None of the authors reported a conflict of interest.
Correspondence to: Dr Paul Krebsbach, University of Michigan, Department of Biologic and Materials Sciences, 1011 N. University Ave., Ann Arbor MI 48109. Fax: +734-763-3453. Email: [email protected]
The Use of Soluble Signals to Harness the Power of the Bone Microenvironment for
Implant Therapeutics Erica L. Scheller, BS1/Paul H. Krebsbach, DDS, PhD2
The use of soluble signals for modulation of bone formation has become a significant area of clinical research in recent years. Improvements in implant site preparation and osseointegration have already been achieved with the use of recombinant platelet-derived growth factor and bone morphogenetic proteins on osteogenic scaffolds. Other states of insufficient bone such as osteoporosis are frequently treated with inhibitors of osteoclast function or osteoblast anabolic agents. However, despite the existence of promising therapies targeting osteoblasts and osteoclasts directly, therapies utilizing indirect regulation through secondary cellular nodes of control (NOC) are just beginning to emerge. This article will review current strategies for regulation of bone formation by targeting two primary NOCs, the osteoblast and osteoclast, as well as four secondary NOCs, the vascular, hematopoietic, mesenchymal, and neural. Int J Oral Maxillofac
Implants 2011;26(suppl):70–79
Key words: bone, cell signaling, dental implant, differentiation, growth factors, regeneration, tissue engineering
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Scheller/Krebsbach
The International Journal of Oral & Maxillofacial Implants 71
limb bones.6 It has since been learned that the pri-mary function of the adult bone marrow is blood cell formation, or hematopoiesis, and in 1968 the trans-plantation of bone marrow to rescue patients with serious illnesses such as leukemia was realized.7,8 The 40 years since the first successful bone marrow trans-plant have been spent uncovering and characterizing the many cell types and signaling molecules present in this complex microenvironment. Application of this knowledge to the regeneration of the marrow’s sup-porting osseous and cartilaginous structures is a pri-mary goal of the field of bone tissue engineering.
To emphasize the complexity of this challenge, it is now appreciated that more than 30 distinct cell populations reside in close proximity to osteoblasts and osteoclasts (Fig 1).9,10 These include hematopoi-etic lineage cells, mesenchymal lineage cells, blood vessels, and neural tissue. Each of these cell popula-tions, alone or in combination, possesses the capac-ity to influence bone growth and regeneration. If one considers that the sequence of signaling between cells can vary (eg, B cell ⃗ T cell ⃗ osteoblast versus T cell ⃗ B cell ⃗ osteoblast), there are a minimum of 2.65 × 1032 unique sequences of cells/signals that
fig 1 Theoretical diagram of the marrow space adjacent to an implant. The surface of an implant is surrounded by a complex bone marrow microenvironment. More than 30 unique cell types exist in a complex matrix that can regulate bone formation. A subset of these cells is depicted here, with emphasis on the two primary nodes of control (the osteoblast and the osteoclast) and the four secondary nodes of control (the vascular, the hematopoietic, the mesenchymal, and the neural).
Neural
VascularHematopoietic
Endothelial cell
PrimaryMacrophage
Osteocyte
Osteoclast
Osteoblast
Mesenchymal
Adipocyte
Chondrocyte
HSCT cell
B cell
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and differentiation
72 Volume 26, Supplement, 2011
could potentially regulate bone formation (often with redundancies in signaling pathways). This is without even considering the important signaling role of the extracellular matrix in this environment. Though overwhelming, this complexity reaffirms the need to continue exploration of the topic with an open mind.
Current strategies for induction of bone formation at implant sites revolve around two primary nodes of control (NOC) in the bone marrow microenviron-ment. The first node encompasses modulation of the osteoblast.
the oSteoBLaSt
Osteoblasts are specialized cells that reside on the bone surface and are responsible for synthesis of the bone extracellular matrix and influence biomineralization. Osteoblasts are derived from mesenchymal stem cells (MSCs) when differentiation is induced and transcrip-tion factors such as Runx2 are activated.11 Increased bone formation can be achieved by (1) increasing the activity of mature osteoblasts, (2) increasing the num-ber of osteoblast precursor cells, (3) stimulating differ-entiation of new cells from osteoblast precursors, and (4) inhibiting osteoblast cell death.
Modulation of osteoblast formation and function is currently the most exploited strategy for bone tis-sue engineering and represents a prime target for augmenting osseointegration. Clinicians can now of-fer BMP-2–laced collagen sponges to their patients as an alternative grafting protocol for approximately US$870 per 0.5 mL (INFUSE Bone Graft, Medtronic). Although it is not yet available for craniofacial appli-cations, BMP-7, referred to as osteogenic protein 1 (OP-1), was also approved under the humanitarian de-vice exemption by the US Food and Drug Administra-tion (FDA) in 2001 (OP-1, Stryker). Currently, the cost is US$5,000 per 3.3-mg dose, to be applied for spinal fusion or fracture repair when an autograft is not fea-sible and other treatments have failed. BMPs are the prototypical bone-inducing soluble factors that were first identified as present within the bone matrix. As early as 1889, it was shown that decalcified bone could be used to heal lesions caused by osteomyeli-tis.12 Forty-nine years later, studies revealed that intra-muscular injection of an acid-alcohol extract of bone could induce a mix of bone and cartilage in rabbits.13,14 Now, 72 years later, BMP family members have been identified,1 cloned,15,16 synthetically produced,17 and delivered to patients to enhance bone regeneration. When administered locally to a bone defect, BMP-2 and BMP-7 induce the differentiation of progenitor cells into chondrocytes and osteoblasts and enhance bone formation.18–20 There are currently two ongoing
clinical trials testing localized alveolar ridge augmen-tation with the BMP-2 INFUSE bone graft for implant placement both at the time of graft placement and 6 months after graft placement.21 The expected comple-tion date for these studies is December 2010 (Table 1).
Growth and differentiation factor 5 (GDF-5) is closely related to BMP and is also a member of the transforming growth factor-beta (TGF-β) superfamily of proteins. GDF-5 stimulates limb mesenchyme ag-gregation and chondrogenesis and regulates skeletal development.22 A human recombinant form of GDF-5 coated onto beta-tricalcium phosphate (β-TCP) (Scil Technology, MD05) is undergoing clinical trials as an osteoinductive and osteoconductive bone graft mate-rial for use in dental and maxillofacial applications.21,23 Results in the rat calvarial defect model demonstrated a fivefold enhancement in bone histomorphometric parameters with GDF-5/β-TCP over β-TCP alone.23
In addition to BMPs, many growth factors are be-ing pursued as pro-osteogenic agents. Platelet-de-rived growth factor (PDGF) on β-TCP (Osteohealth, GEM21S) can be purchased for US$299 per 0.5 mL and can be used to aid regeneration of periodontal le-sions such as furcations and intrabony defects. PDGF is known to stimulate bone cell growth, promote division of precursor cells, and increase type I colla-gen synthesis by osteoblasts.24 In addition to clinical trials for bone formation, administration of PDGF in protein or adenoviral vector (gene therapy) form at the time of implant placement enhances osseointe-gration in rats.25 Fibroblast growth factor (FGF), like PDGF, can increase division of osteoblast precursors and other cells and enhance local bone formation. However, overexpression of FGF-2 in mice causes os-teopenia; this highlights the need to selectively regu-late dose and site selection.26 The main advantage of mitogenic factors such as PDGF and FGF is that, after precursor cell numbers are increased, the body can then take over and regenerate structures in a way that cannot yet be mimicked in the laboratory envi-ronment. Unlike predominantly bone-forming BMPs, local application of FGF-2 has facilitated regeneration of new periodontal ligament, cementum, and bone simultaneously in canine periodontal defects.27 The drug Trafermin (Kaken Pharmaceuticals), a human recombinant FGF-2 protein, is currently in phase III clinical trials for periodontal tissue regeneration.21 In addition, FGF coated onto the surface of titanium implants in a calcium phosphate matrix can enhance osseointegration in animal models, and a slowly de-grading FGF–gelatin hydrogel complex for repair of fenestrated implants has been successful in dogs.28,29
Though not yet used in dental applications, injec-tion of anabolic parathyroid hormone (PTH) is widely used as a treatment for osteoporosis. Recombinant
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Scheller/Krebsbach
The International Journal of Oral & Maxillofacial Implants 73
versions of the N-terminal segment (Forteo, Eli Lilly) or full-length recombinant protein (Preos, NPS Phar-maceuticals) have been tested in humans. However, only Forteo is currently approved for use by the US FDA because of unresolved concerns about the devel-opment of hypercalcemia with Preos. Anabolic PTH has multiple actions, which include enhancement of osteoblast proliferation and differentiation, increased engraftment of hematopoietic stem cells (HSCs) in new bone, and induction of bone formation.30,31 Studies with ectopic ossicles in mice suggest that an-abolic dosing of PTH (N-terminal segment) via daily subcutaneous injections can significantly enhance formation of new bone.32 Phase I clinical trials testing Forteo for augmentation of regeneration after peri-odontal surgery have been completed.33
Insulinlike growth factor (IGF) has two identified isoforms (IGF-I and IGF-II), which are the most abun-dant growth factors in bone tissue.26 IGF-I has a slight
mitogenic effect on osteoblast precursors and a sig-nificant antiapoptotic function that helps to increase the total osteoblast pool without dramatically regu-lating differentiation.26 IGF-I can also enhance osteo-blast synthesis of collagen I.34 However, this effect is balanced by increases in the production of receptor activator of nuclear factor κB ligand (RANKL) and modulation of osteoclastogenesis.35 The basic under-standing of IGF-I function and its diverse systemic ef-fects have limited its use for bone tissue engineering; however, human recombinant IGF-I has been avail-able since 1986 and was approved for use in the Unit-ed States in 2005 to treat IGF-I deficiency.36 Clinical trials to treat children of short stature associated with IGF-I deficiency have demonstrated mild improve-ment in height with once-daily subcutaneous injec-tion of 60 µg/kg IGF-I (Mecasermin, Tercica) over a period of 86 weeks.21,36 Production of IGF by the liver is regulated by growth hormone (GH) secreted by the
table 1 Summary of Clinical development of recombinant Proteins: Major anabolic therapies Undergoing testing for Medical and dental Use
Signal Summary of action Clinical status
BMP-2 MSC survival and differentiation (Edgar et al 200718 and Solmesky et al 200920) INFUSE, Medtronic
Initiation of fracture repair (Tsuji 200679) Available for dental use
Endochrondal ossification (Sasano et al 199763)
Maintenance of the HSC niche (Zhang et al 200357)
BMP-7 Differentiation of MSCs (Asahina 199680) OP-1, Stryker
Activity of mature osteoblasts (Asahina 199680) Available for medical use
GDF-5 Skeletal patterning and limb development (Hotten et al 199622) MD05, Scil Technology
Enhanced bone formation in skeletal defects (Poehling et al 200623) Phase II for dental use
PDGF Increase osteoblast precursor population (Mitlak et al 199624) GEM21S, Osteohealth
Induces osteoclastogenesis (Mitlak et al 199624) Available for dental use
Induction of VEGF production (Cooke et al 200656)
FGF-2 Increase cell division and osteoblast precursor (Murakami et al 200327) Trafermin, Kaken Pharmaceuticals
Stimulation of angiogenesis (Montesano et al 198655) Phase III for dental use
PTH Osteoblast proliferation and differentiation (Pettway et al 200830) Forteo, Eli Lilly
Increase engraftment of HSCs in new bone (Song et al 201031) Available for medical use
Phase I for dental use
IGF-I Slightly mitogenic, enhances osteoblast function (Canalis 198081) Mecasermin, Tercica
Decrease osteoblast apoptosis (Canalis 200926) Available for medical use
Induces osteoclastogenesis via RANKL (Mochizuki et al 199234)
Induction of VEGFa (Akeno et al 200233)
GH Induction of IGF-I production by the liver (Olney 200336) SimpleXx, Novo Nordisk
Promotion of lipolysis and protein synthesis (Olney 200336) Phase II for fracture repair
VEGF Regulation of angiogenesis (Kanczler and Oreffo 200846) VEGF165 plasmid/protein
HSC and monocyte recruitment, bone formation (Kanczler and Oreffo 200846) Phase III for medical use
Phase I–III indicates level of human clinical trials currently underway for the indicated use.21
BMP = bone morphogenetic protein; GDF = growth and differentiation factor; PDGF = platelet-derived growth factor; FGF = fibroblast growth factor; IGF = insulinlike growth factor; PTH = parathyroid hormone; GH = growth hormone; VEGF = vascular endothelial growth factor; HSC = hematopoietic stem cell; RANKL = receptor activator for nuclear factor κB ligand.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and differentiation
74 Volume 26, Supplement, 2011
pituitary gland, and a lack of GH significantly impairs skeletal development.37 Systemic GH has effects on many tissues, including induction of osteoblast and osteoclast activity and subsequent increases of bone remodeling.37 The use of recombinant GH to augment fracture healing has been proposed since the 1950s.38 Recent completion of a human clinical trial revealed a 26% decrease in healing times for closed tibial frac-tures with daily injection of 60 µg/kg GH (Norditropin SimpleXx, Novo Nordisk).39 GH did not significantly alter the healing time for open fractures or for closed fractures at doses under 60 µg/kg.39 Successful use of IGF-I or GH alone for bone tissue engineering or peri-odontal regeneration is unlikely but may prove useful in combination with other factors.
the oSteoCLaSt
The second primary NOC that is highly targeted in os-teoporosis therapies, but rarely utilized for bone tis-sue engineering, involves treatment to decrease both the activity and formation of osteoclasts. Bisphos-phonates such as zoledronic acid are prototypical antiresorptive agents and have a half-life in bone potentially exceeding 10 years.40 Bisphosphonates block the cytoskeletal organization of osteoclasts, inhibit formation of resorption pits, and induce os-teoclast apoptosis.41,42 Bisphosphonates are used in the treatment of osteoporosis, bone metastasis, mul-tiple myeloma, and Paget disease. Initial treatment allows osteoblasts to continue to function, resulting in a net gain in bone volume. However, for many of the bisphosphonates, the osteoblast activity de-creases after approximately 2 years because of a lack of feedback signals from the osteoclast resorption pits.43 In healing bone, such as during fracture repair, uncoupling of bone formation and resorption is un-desirable, since activity of the osteoclast is necessary to properly remodel the bone and direct osteoblast activity at the site of injury. However, the use of anti-resorptives for temporal regulation of osteoclast re-modeling may prove beneficial for future periodontal tissue engineering and implant therapy.
Newer medications are being designed to in-hibit bone resorption without the untoward effect of decreasing osteoblast activity. After observing that bone resorption increases during fasting, in-cluding at night on a circadian rhythm, Henriksen et al tested administration of glucagonlike peptide 2 (GLP-2) for treatment of osteoporosis.44 GLP-2 is a 33-amino-acid peptide produced by the intestine in response to food intake that has been assessed as a treatment for short bowel syndrome, Crohn disease, and osteoporosis. Daily subcutaneous injection of
GLP-2 before bedtime in postmenopausal women decreased serum markers of osteoclast activity for up to 8 hours without a change in markers of osteoblast function.44 At the lowest effective dose of GLP-2 there was no increase in adverse side effects over the con-trol treatment (placebo).44 A second method involves inhibition of cathepsin K (CatK), a protein expressed in lysosomes of osteoclasts that degrades type I col-lagen after acidification of the resorption pit.43 Ad-ministration of a CatK inhibitor (Odanacatib, Merck) weekly for 2 years in postmenopausal women result-ed in a 5.5% bone mass density (BMD) increase in the lumbar spine without dose-related trends in adverse events.45 This increase is similar to the 4.3% to 5.1% increase in BMD achieved with the bisphosphonate zoledronic acid in a similar postmenopausal popula-tion, but it may not have the extended uncoupling effects associated with the long half-life of bisphos-phonates.46 In addition, in mice, CatK inhibitors were successfully used in combination with anabolic PTH, suggesting a potential for combination therapy. This may be considered for clinical trials in regenerative medicine and dental implant therapy in anatomic locations with inadequate bone quality and volume.
SeCondarY nodeS of ControL
When one considers cells beyond the osteoblast and osteoclast, it readily becomes apparent that there are many other cell types and signaling pathways in the bone marrow microenvironment that may be used to enhance bone formation. Most factors that regu-late osteoblast cell function also have effects on sur-rounding populations, such as vascular endothelial cells, hematopoietic lineages, mesenchymal lineages, and neural cells. Thus, four secondary NOCs should be considered for future therapeutic advantage: the vascular, the hematopoietic, the mesenchymal, and the neural.
Vascular node of ControlTo maximize the formation of new bone around im-plant sites, cells must receive a steady nutritional sup-ply and have access to a conduit to remove metabolic waste from the actively healing wound. These pro-cesses require the establishment of a vascular bed in close contact with bone to maintain skeletal integrity, a concept that has been recognized since the 1700s.47 In 1963, it was proposed that a vascular stimulating factor was released at osseous fracture sites.48 It is now understood that the main regulators of new ves-sel formation include vascular endothelial growth fac-tor (VEGF), basic FGF, hypoxia-inducible transcription factor, PDGF, IGF-I/II, and angiopoietin.49 VEGFs are
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Scheller/Krebsbach
The International Journal of Oral & Maxillofacial Implants 75
thought to be the main regulators of angiogenesis, and VEGF in plasmid or protein form has been tested in clinical trials for treatment of peripheral artery dis-ease, limb ischemia, chronic diabetic foot ulcers, and myocardial ischemia.21 Cross talk between VEGF-pro-ducing osteoblasts and hypoxia-inducible transcrip-tion factor–producing osteoblasts and surrounding endothelial cells is critical for coupling angiogenesis and osteogenesis during bone formation.49,50 Recip-rocal studies established that endothelial cells have the ability to modulate osteoblast differentiation and enhance bone formation.51 VEGF produced by osteoblasts can up-regulate BMP-2 in microvascular endothelial cells, a fact that emphasizes the close re-lationship between these two cell types.52,53 Release of VEGF alone or in combination with BMP-4 from biomimetic scaffolds can significantly enhance bone regeneration in rodent models.54,55 Despite these successes, VEGF therapy has not yet been applied in human clinical trials for bone regeneration. FGF-2 and PDGF, discussed earlier, are also capable of stimulat-ing angiogenesis, in addition to their pro-osteogenic effects.56,57
hematopoietic node of ControlMaterials such as titanium and β-TCP have been care-fully screened for biocompatibility and developed us-ing good manufacturing practice before their use in humans. Thus, at its most basic level, modulation of the immune response is essential for successful en-graftment of foreign material or tissue into the body. However, direct regulation of the blood cells of the marrow may provide additional benefits to bone for-mation if the proper signals can be determined. One of the reasons BMPs are pro-osteogenic is that they help maintain the HSC niche and establish a fully func-tional marrow cavity in newly formed bone.58 PTH was also able to regulate HSC recruitment to newly formed bone in an ectopic ossicle model in mice.31
Mature lineages derived from HSCs also play a significant role in bone homeostasis. The recently termed osteal tissue macrophages (“OsteoMacs”) are the resident macrophage population of the bone marrow. Studies both in vitro and in vivo have shown that depletion of this population dramatically im-pairs osteoblast function and can cause complete loss of the osteoblast bone-forming surface.59 Im-plant placement is followed by a robust inflamma-tory response in which macrophages help to guide osseointegration.60 However, when the inflammation becomes chronic, implant loss may occur. Temporal regulation of the inflammatory healing response with implant surface modification, growth factors, and cy-tokines may allow facilitated increases in healing rate and bone formation.60
A common issue in dental treatment is the presence of infection. It is well appreciated that the success rate of a bone graft or osseointegration of a dental implant will decrease if an infection is present. Indeed, pre-liminary evidence shows that immunocompromised mice that lack both T cells and B cells have enhanced fracture healing.61 Additional research in the field of osteoimmunology has demonstrated that T cells are potent regulators of osteoclastogenesis via their ex-pression of the pro-osteoclastogenic factor RANKL.62 The presence of inflammation increases the local con-centration of inflammatory cytokines such as tumor necrosis factor alpha (TNF-α). Infliximab (Remicade, Centocor), a monoclonal antibody against TNF-α, has been approved by the US FDA for treatment of psori-atic and rheumatoid arthritis and effectively reduces bone destruction in inflamed joints.62 Etanercept (Enbrel, Amgen/Wyeth), a fusion protein inhibitor of TNF, is also clinically available with similar prescribing indications. Targeting the mechanisms behind these hematopoietic-osseous interactions may provide new tools to deal with infection-induced immune re-sponses at the implant site.
Mesenchymal node of ControlAlthough modulation of osteoblast function falls un-der this NOC, the function of three other mesenchy-mal lineage cells should be considered for bone tissue engineering. The first is the adipocyte. As mentioned earlier, the number of fat cells present in the marrow at any one time varies depending on area of the skel-eton, age of the host, obesity, or disease state. The mandible and maxilla generally contain very little adi-pose tissue; however, manipulation of this area with soluble factors or radiation can significantly change the ratio of red to yellow marrow. For example, irradi-ation of bone at a dose designed to prepare the host for a bone marrow transplant results in a transient fill-ing of the bone cavity with adipose tissue for 1 to 2 weeks.63 Blocking fat accumulation with a small mol-ecule inhibitor of peroxisome proliferator-activated receptor-γ (PPAR-γ), a transcription factor required for adipocyte differentiation, significantly enhances engraftment of new HSCs as well as trabecular bone formation.63
The chondrocyte is a mesenchymal derivative that plays a major role in the formation of bone during endochondral ossification, a mechanism that is used during the development of bones (excluding the clavicle and most bones of the skull). Regardless of developmental site, this process of forming bone with a cartilage intermediate is, in some cases, reproduced during bone tissue engineering by the addition of fac-tors such as BMP-2.64 Endochondral ossification be-gins with recruitment and differentiation of MSCs into
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and differentiation
76 Volume 26, Supplement, 2011
chondroblasts. This is followed by chondroblast pro-liferation and organization over the first 1 to 3 weeks. The calcifying hypertrophic chondrocytes are then removed, and subsequent osteoblast recruitment and mineralization result in new bone formation.65 This process allows relatively rapid establishment of a soft callus that is subsequently replaced by woven bone. Since cartilage is naturally an avascular tissue, factors that induce endochondral ossification instead of osteoblast stimulation directly may help keep the bioengineered graft viable while angiogenesis occurs.
Osteocytes are a third MSC-derived lineage that are embedded within the bone matrix and communicate via an extensive canalicular network of cell processes. Osteocytes are able to respond to changes in force in the external environment by changing the activity of the Wnt/β-catenin pathway, which in turn signals to the bone surface cells to regulate bone formation.66 With-out knowing the mechanism, researchers have long recognized that repeated loading of bone through regular weight-bearing activity helps to maintain and increase bone density. Although the jaws are not as ac-cessible for loading protocols as the limbs, newer tech-nologies have sought to stimulate cells of the marrow with ultrasound and pulsed electromagnetic fields. In human clinical trials, low-intensity pulsed ultrasound has enhanced repair and regeneration of fractured bone by up to 40%,67 and extension of ultrasound’s anabolic effects has also been proposed for tooth re-pair.68 The exact mechanism behind these effects is unclear, but direct regulation of precursor cell differ-entiation and expression of osteocalcin, VEGF, and the integrin family of mechanoreceptors may play a role (see Pounder and Harrison67 for a review).
neural node of Control Neural regulation of bone formation has been inferred for several decades following observations of osteo-penia secondary to neural disorders, including reflex sympathetic dystrophy syndrome, stroke, spinal cord injury, and peripheral neuropathy.69 Central regulation of calcium and phosphate serum levels requires neu-ral control of bone remodeling that is at least partly regulated through hypothalamic signal integration and sympathetic output.69 Hypothalamic regulators of BMD include leptin, neuropeptide Y, cannabinoid receptors, cocaine and amphetamine-regulated tran-script, and melanocortin 4 receptor (see Patel and Elef-teriou69 for a review). Direct targeting of hypothalamic centers for tissue engineering may seem a subject of the distant future, but indirect targets are already un-der investigation. As discussed earlier, GLP-2 is be-ing tested as a novel therapy for osteoporosis. GLP-2 functions by dampening normal circadian rhythm–induced nighttime bone remodeling.44 Beta-blockers
that inhibit neurons downstream of the hypothala-mus are commonly used to treat high blood pressure and migraine headaches. However, administration of beta-blockers such as propranolol can addition-ally increase bone formation and inhibit resorption in rodent models,69,70 implying that beta-blockers may have previously unrealized therapeutic value for bone formation.
fUtUre direCtionS
Although osteogenic factor–saturated scaffolds have proven to be useful, they are restricted to local ac-tions on surrounding cells. In situations where a site lacks sufficient stem and progenitor cells, such as with extensive trauma, radiation therapy, or advanced age, recruitment of stem cells from remote sites to aid re-generation and repair would be beneficial. This would mimic the addition of cells that have been previously harvested from the patient and expanded in vitro or augmentation with tissue grafts from another site, but it would eliminate the need for extended culture time or additional surgical manipulation. Two hu-man clinical trials have applied this concept to the treatment of ischemic heart disease.71,72 The first trial examined the ability of VEGF and granulocyte colo-ny-stimulating factor to mobilize stem cells from the bone for repair of heart muscle. The second tested the ability of GH to mobilize endothelial progenitor cells. VEGF gene transfer and recombinant granulocyte col-ony-stimulating factor in combination increased the number of circulating CD34+ progenitor cells nearly tenfold, but this did not improve myocardial perfu-sion after 3 months.71 GH increased the number of cir-culating endothelial progenitors by 1.5-fold without a change in CD34+ cells, but functional significance was not analyzed.72
These clinical trials have successfully forced pro-genitor cells into the circulation, but the circulating cells are not yet receiving the molecular instructions necessary to perform the desired function. Co-ad-ministration of an instructing factor may overcome this barrier and enhance treatment. The concept of combination therapy is certainly important. For ex-ample, because PDGF has agonist effects on both os-teoblasts and osteoclasts, combination therapy with an antiresorptive bisphosphonate increases bone density twofold over PDGF alone when administered systemically to rats.24 Another popular combination pairs a cell mitogen, such as FGF or PDGF, with an anabolic agent such as BMP. Combined therapy with basic FGF and BMP-2 significantly increased bone formation and osseointegration of dental implants placed in rabbits when compared to BMP-2 alone
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Scheller/Krebsbach
The International Journal of Oral & Maxillofacial Implants 77
after 4 weeks of healing.73 Another strategy involves enhancing the actions of osteogenic factors that are known to work well, such as BMP. For example, there are at least 10 characterized secreted BMP antago-nists (see Canalis26 for review). Administration of BMP with a corresponding block to its signaling antagonist could both reduce the required dose of BMP and in-crease its effects at the local site. Along these same lines of inhibiting the inhibitors, human neutralizing antibodies to sclerostin, a pro-osteogenic Wnt signal-ing antagonist, have gone through phase I clinical tri-als and can increase BMD in humans.26 A second trial is anticipated to start in May 2010.21 Lastly, in mice, CatK inhibitors were successfully used in combination with anabolic PTH, suggesting the potential for future combination therapy.74
In addition to re-creating native proteins, small molecule inhibitors and biomimetic scaffolds are vi-able alternatives that may reduce costs as a result of eliminating the need for biologic synthesis and ap-propriate protein folding in a host cell. A small mol-ecule antagonist of secreted frizzled receptor-1 has been reported to enhance Wnt signaling and bone formation.75 Bisphenol A diglycidyl ether (BADGE, Tocris Bioscience) is a PPAR-γ antagonist that, when administered after radiation therapy in mice, can en-hance engraftment of new marrow and subsequent bone formation.63 Scheller et al76 have provided a re-view of scaffold design strategies and uses for tissue engineering.
The development of a new technology for clinical use requires a significant amount of time, but among the soluble signals already discussed, several may be available in the next 5 years. FGF-2 is beginning phase III clinical trials for periodontal tissue regeneration; successful completion of these studies will allow the company to seek FDA approval for clinical marketing (Table 1). Anabolic PTH therapy for wound healing and regeneration in the oral cavity, although it is only in phase I trials, may move toward clinical use rapidly if successful, since the drug Forteo is already widely used for osteoporosis. Combination therapies pairing an already approved osteogenic factor (eg, BMP) with a cell mitogen (eg, PDGF, FGF-2) may also become popular. Finally, because of robust success in animals and preliminary clinical trials, the approach to soluble factor delivery may begin to shift to genetic regula-tion of factor production. This would potentially allow for increased local concentrations of factors to be pro-duced for a longer period of time. Scheller and Krebsbach77 have reviewed gene therapy in craniofa-cial applications. Myocardial injection of VEGF165 plasmid has successfully passed safety standards in human phase II clinical trials,71 and although signifi-cant clinical improvement was not achieved with this
application, animal studies suggest that VEGF gene therapy may allow for significant augmentation of periodontal tissue regeneration.54
One main challenge of regenerative medicine lies in the capacity to replace normal tissue at a specific location without toxic or other negative side effects. Activation of the Wnt pathway is a popular target for osteoblast differentiation; however, overactiva-tion of canonical Wnt signaling through β-catenin has been linked to tumor formation in extraskeletal tissues.78 As a second example, development of the CatK inhibitor balicatib was suspended because of an unexpected incidence of skin reactions and other side effects.43 In addition to safety concerns, costs and insurance coverage drive clinical use of dental therapeutics. At US$299 per 0.5 mL, PDGF (GEM21S) is the most reasonably priced, and the use of BMP-2 (INFUSE) grafts is more expensive at US$870 per 0.5 mL but still manageable in some circumstances. Injectable agents such as Forteo and Remicade can cost US$900 to US$1,500 per month and may require multiple months of use, but in the future, costs may be mitigated by health insurance coverage. Despite the required safety profile and costs involved, there are seemingly limitless possibilities for protein, small molecule, and scaffold combinations to enhance bone formation and implant osseointegration. Opti-mization and individual customization of these thera-pies will require the combined effort and imagination of many investigators to best satisfy the needs of per-sons who require implant therapy.
referenCeS
1. Urist MR. Bone: Formation by autoinduction. Science 1965;150:893–899.
2. Pilcher E. The History of Dental Implants. 2010. http://afreear-ticle.com. Accessed 16 April 2010.
3. Kawai T, Mieki A, Ohno Y, et al. Osteoinductive activity of com-posites of bone morphogenetic protein and pure titanium. Clin Orthop Relat Res 1993:296–305.
4. Andreana S, Beneduce C, Buhite R. Implant success rate in dental school setting: Retrospective study. N Y State Dent J 2008;74:67–70.
5. Romeo E, Lops D, Margutti E, Ghisolfi M, Chiapasco M, Vogel G. Long-term survival and success of oral implants in the treatment of full and partial arches: A 7-year prospective study with the ITI dental implant system. Int J Oral Maxillofac Implants 2004;19:247–259.
6. Krech S, McNeill JR, Merchant C. Encyclopedia of World Envi-ronmental History, vol 3. New York: Routledge, 2004.
7. Thomas DB, Smith CM, Sumpster JM. The proliferation of transplanted haematopoietic cells derived from bone mar-row and foetal liver. J Anat 1970;107:194–195.
8. Gatti RA, Meuwissen HJ, Allen HD, Hong R, Good RA. Im-munological reconstitution of sex-linked lymphopenic immunological deficiency. Lancet 1968;2:1366–1369.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and differentiation
78 Volume 26, Supplement, 2011
9. Metcalf D. Concise review: Hematopoietic stem cells and tis-sue stem cells: Current concepts and unanswered questions. Stem Cells 2007;25:2390–2395.
10. Phinney DG, Prockop DJ. Concise review: Mesenchymal stem/multipotent stromal cells: The state of transdifferentia-tion and modes of tissue repair—Current views. Stem Cells 2007;25:2896–2902.
11. Granero-Molto F, Weis JA, Longobardi L, Spagnoli A. Role of mesenchymal stem cells in regenerative medicine: Ap-plication to bone and cartilage repair. Exp Opin Biol Ther 2008;8:255–268.
12. Senn N. On the healing of aseptic bone cavities by implanta-tion of antiseptic decalcified bone. Ann Surg 1889;10:352–368.
13. Levander G. A study of bone regeneration. Surg Gynecol Obstet 1938;67:705–714.
14. Dimitriou R, Giannoudis PV. Discovery and development of BMPs. Injury 2005;36(suppl 3):S28–S33.
15. Rosen V, Wozney JM, Wang EA, et al. Purification and molecular cloning of a novel group of BMPs and localization of BMP mRNA in developing bone. Connect Tissue Res 1989;20:313–319.
16. Celeste AJ, Iannazzi JA, Taylor RC, et al. Identification of transforming growth factor beta family members present in bone-inductive protein purified from bovine bone. Proc Nat Acad Sci USA 1990;87:9843–9847.
17. Kubler NR, Reuther JF, Faller G, Kirchner T, Ruppert R, Sebald W. Inductive properties of recombinant human BMP-2 pro-duced in a bacterial expression system. Int J Oral Maxillofac Surg 1998;27:305–309.
18. Edgar CM, Chakravarthy V, Barnes G, Kakar S, Gerstenfeld LC, Einhorn TA. Autogenous regulation of a network of bone morphogenetic proteins (BMPs) mediates the osteogenic differentiation in murine marrow stromal cells. Bone 2007; 40:1389–1398.
19. Rosen V. BMP2 signaling in bone development and repair. Cytokine Growth Factor Rev 2009;20:475–480.
20. Solmesky LJ, Abekasis M, Bulvik S, Weil M. Bone morphoge-netic protein signaling is involved in human mesenchymal stem cell survival in serum-free medium. Stem Cells Dev 2009;18:1283-1292.
21. National Institutes of Health. http://ClinicalTrials.gov. Accessed 15 April 2010.
22. Hotten GC, Matsumoto T, Kimura M, et al. Recombinant hu-man growth/differentiation factor 5 stimulates mesenchyme aggregation and chondrogenesis responsible for the skeletal development of limbs. Growth Factors 1996;13:65–74.
23. Poehling S, Pippig SD, Hellerbrand K, Siedler M, Schutz A, Dony C. Superior effect of MD05, beta-tricalcium phosphate coated with recombinant human growth/differentiation fac-tor-5, compared to conventional bone substitutes in the rat calvarial defect model. J Periodontol 2006;77:1582–1590.
24. Mitlak BH, Finkelman RD, Hill EL, et al. The effect of systemi-cally administered PDGF-BB on the rodent skeleton. J Bone Miner Res 1996;11:238–247.
25. Chang PC, Seol YJ, Cirelli JA, et al. PDGF-B gene therapy accelerates bone engineering and oral implant osseointegra-tion. Gene Ther 2010;17:95–104.
26. Canalis E. Growth factor control of bone mass. J Cell Biochem 2009;108:769–777.
27. Murakami S, Takayama S, Kitamura M, et al. Recombinant human basic fibroblast growth factor (bFGF) stimulates periodontal regeneration in class II furcation defects created in beagle dogs. J Periodontal Res 2003;38:97–103.
28. Akagawa Y, Kubo T, Koretake K, et al. Initial bone regenera-tion around fenestrated implants in Beagle dogs using basic fibroblast growth factor-gelatin hydrogel complex with vary-ing biodegradation rates. J Prosthodont Res 2009;53:41–47.
29. Li Y, Lee IS, Cui FZ, Choi SH. The biocompatibility of nano-structured calcium phosphate coated on micro-arc oxidized titanium. Biomaterials 2008;29:2025–2032.
30. Pettway GJ, Meganck JA, Koh AJ, Keller ET, Goldstein SA, McCauley LK. Parathyroid hormone mediates bone growth through the regulation of osteoblast proliferation and dif-ferentiation. Bone 2008;42:806–818.
31. Song J, Kiel MJ, Wang Z, et al. An in vivo model to study and manipulate the hematopoietic stem cell niche. Blood 2010;115:2592–2600.
32. Schneider A, Taboas JM, McCauley LK, Krebsbach PH. Skel-etal homeostasis in tissue-engineered bone. J Orthop Res 2003;21:859–864.
33. Bashutski JD, Eber RM, Kinney JS, et al. Teriparatide and osse-ous regeneration in the oral cavity. N Engl J Med 2010;363: 2396–2405.
34. Akeno N, Robins J, Zhang M, Czyzyk-Krzeska MF, Clemens TL. Induction of vascular endothelial growth factor by IGF-I in osteoblast-like cells is mediated by the PI3K signaling path-way through the hypoxia-inducible factor-2alpha. Endocri-nology 2002;143:420–425.
35. Mochizuki H, Hakeda Y, Wakatsuki N, et al. Insulin-like growth factor-I supports formation and activation of osteoclasts. Endocrinology 1992;131:1075–1080.
36. Fintini D, Brufani C, Cappa M. Profile of mecasermin for the long-term treatment of growth failure in children and ado-lescents with severe primary IGF-1 deficiency. Ther Clin Risk Manag 2009;5:553–559.
37. Olney RC. Regulation of bone mass by growth hormone. Med Pediatr Oncol 2003;41:228–234.
38. Tran GT, Pagkalos J, Tsiridis E, et al. Growth hormone: Does it have a therapeutic role in fracture healing? Exp Opin Investig Drugs 2009;18:887–911.
39. Raschke M, Rasmussen MH, Govender S, Segal D, Suntum M, Christiansen JS. Effects of growth hormone in patients with tibial fracture: A randomised, double-blind, placebo-controlled clinical trial. Eur J Endocrinol/Eur Fed Endocrine Soc 2007;156:341–351.
40. Khan SA, Kanis JA, Vasikaran S, et al. Elimination and biochem-ical responses to intravenous alendronate in postmenopausal osteoporosis. J Bone Miner Res 1997;12:1700–1707.
41. Luckman SP, Hughes DE, Coxon FP, Graham R, Russell G, Rogers MJ. Nitrogen-containing bisphosphonates inhibit the mevalonate pathway and prevent post-translational prenyl-ation of GTP-binding proteins, including Ras. J Bone Miner Res 1998;13:581–589.
42. Hughes DE, Wright KR, Uy HL, et al. Bisphosphonates pro-mote apoptosis in murine osteoclasts in vitro and in vivo. J Bone Miner Res 1995;10:1478–1487.
43. Deal C. Future therapeutic targets in osteoporosis. Curr Opin Rheumatol 2009;21:380–385.
44. Henriksen DB, Alexandersen P, Hartmann B, et al. Disassociation of bone resorption and formation by GLP-2: A 14-day study in healthy postmenopausal women. Bone 2007;40:723–729.
45. Bone HG, McClung MR, Roux C, et al. Odanacatib, a Cathepsin-K inhibitor for osteoporosis: A two-year study in postmenopausal women with low bone density. J Bone Miner Res 2010;25:937–947.
46. Reid IR, Brown JP, Burckhardt P, et al. Intravenous zoledronic acid in postmenopausal women with low bone mineral density. N Engl J Med 2002;346:653–661.
47. Kanczler JM, Oreffo RO. Osteogenesis and angiogenesis: The potential for engineering bone. Eur Cells Mater 2008;15:100–114.
48. Trueta J, Buhr AJ. The vascular contribution to osteogenesis. V. The vasculature supplying the epiphysial cartilage in rachitic rats. J Bone Joint Surg Br 1963;45:572–581.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Scheller/Krebsbach
The International Journal of Oral & Maxillofacial Implants 79
49. Kaigler D, Krebsbach PH, Polverini PJ, Mooney DJ. Role of vas-cular endothelial growth factor in bone marrow stromal cell modulation of endothelial cells. Tissue Eng 2003;9:95–103.
50. Wang Y, Wan C, Deng L, et al. The hypoxia-inducible factor alpha pathway couples angiogenesis to osteogenesis during skeletal development. J Clin Investig 2007;117:1616–1626.
51. Kaigler D, Krebsbach PH, Wang Z, West ER, Horger K, Mooney DJ. Transplanted endothelial cells enhance orthotopic bone regeneration. J Dent Res 2006;85:633–637.
52. Bouletreau PJ, Warren SM, Spector JA, et al. Hypoxia and VEGF up-regulate BMP-2 mRNA and protein expression in microvascular endothelial cells: Implications for fracture healing. Plast Reconstr Surg 2002;109:2384–2397.
53. Kaigler D, Krebsbach PH, West ER, Horger K, Huang YC, Mooney DJ. Endothelial cell modulation of bone marrow stromal cell osteogenic potential. FASEB J 2005;19:665–667.
54. Huang YC, Kaigler D, Rice KG, Krebsbach PH, Mooney DJ. Combined angiogenic and osteogenic factor delivery en-hances bone marrow stromal cell-driven bone regeneration. J Bone Miner Res 2005;20:848–857.
55. Kaigler D, Wang Z, Horger K, Mooney DJ, Krebsbach PH. VEGF scaffolds enhance angiogenesis and bone regeneration in ir-radiated osseous defects. J Bone Miner Res 2006;21:735–744.
56. Montesano R, Vassalli JD, Baird A, Guillemin R, Orci L. Basic fibroblast growth factor induces angiogenesis in vitro. Proc Nat Acad Sci USA 1986;83:7297–7301.
57. Cooke JW, Sarment DP, Whitesman LA, et al. Effect of rhPDGF-BB delivery on mediators of periodontal wound repair. Tissue Eng 2006;12:1441–1450.
58. Zhang J, Niu C, Ye L, et al. Identification of the haematopoietic stem cell niche and control of the niche size. Nature 2003;425: 836–841.
59. Chang MK, Raggatt LJ, Alexander KA, et al. Osteal tissue mac-rophages are intercalated throughout human and mouse bone lining tissues and regulate osteoblast function in vitro and in vivo. J Immunol 2008;181:1232–1244.
60. Stanford CM. Surface modification of biomedical and dental implants and the processes of inflammation, wound healing and bone formation. Int J Mol Sci 2010;11:354–369.
61. Gaston MS, Noble BS, Simpson AHRW. Deficiency of the spe-cific immune system enhances fracture repair in-vivo. J Bone Joint Surg Br 2008;90:365.
62. Takayanagi H. Inflammatory bone destruction and osteoim-munology. J Periodontal Res 2005;40:287–293.
63. Naveiras O, Nardi V, Wenzel PL, Hauschka PV, Fahey F, Daley GQ. Bone-marrow adipocytes as negative regulators of the haematopoietic microenvironment. Nature 2009;460:259–263.
64. Sasano Y, Mizoguchi I, Takahashi I, Kagayama M, Saito T, Kuboki Y. BMPs induce endochondral ossification in rats when implanted ectopically within a carrier made of fibrous glass membrane. Anat Rec 1997;247:472–478.
65. Dimitriou R, Tsiridis E, Giannoudis PV. Current concepts of molecular aspects of bone healing. Injury 2005;36:1392–1404.
66. Bonewald LF, Johnson ML. Osteocytes, mechanosensing and Wnt signaling. Bone 2008;42:606–615.
67. Pounder NM, Harrison AJ. Low-intensity pulsed ultrasound for fracture healing: A review of the clinical evidence and the associated biological mechanism of action. Ultrasonics 2008;48:330–338.
68. Scheven BA, Shelton RM, Cooper PR, Walmsley AD, Smith AJ. Therapeutic ultrasound for dental tissue repair. Med Hypoth-eses 2009;73:591–593.
69. Patel MS, Elefteriou F. The new field of neuroskeletal biology. Calcif Tissue Int 2007;80:337–347.
70. Sato T, Arai M, Goto S, Togari A. Effects of propranolol on bone metabolism in spontaneously hypertensive rats. J Phar-macol Exp Ther 2010;334:99–105.
71. Ripa RS, Wang Y, Jorgensen E, Johnsen HE, Hesse B, Kastrup J. Intramyocardial injection of vascular endothelial growth fac-tor-A165 plasmid followed by granulocyte-colony stimulating factor to induce angiogenesis in patients with severe chronic ischaemic heart disease. Eur Heart J 2006;27:1785–1792.
72. Devin JK, Vaughan DE, Blevins LS Jr, et al. Low-dose growth hormone administration mobilizes endothelial progenitor cells in healthy adults. Growth Horm IGF Res 2008;18:253–263.
73. Lan J, Wang Z, Wang Y, Wang J, Cheng X. The effect of combination of recombinant human bone morphogenetic protein-2 and basic fibroblast growth factor or insulin-like growth factor-I on dental implant osseointegration by confo-cal laser scanning microscopy. J Periodontol 2006;77:357–363.
74. Gauthier JY, Chauret N, Cromlish W, et al. The discovery of odanacatib (MK-0822), a selective inhibitor of cathepsin K. Bioorgan Med Chem Lett 2008;18:923–928.
75. Bodine PV, Stauffer B, Ponce-de-Leon H, et al. A small molecule inhibitor of the Wnt antagonist secreted frizzled-related pro-tein-1 stimulates bone formation. Bone 2009;44:1063–1068.
76. Scheller EL, Krebsbach PH, Kohn DH. Tissue engineering: State of the art in oral rehabilitation. J Oral Rehabil 2009;36:368–389.
77. Scheller EL, Krebsbach PH. Gene therapy: Design and prospects for craniofacial regeneration. J Dent Res 2009;88:585–596.
78. Lustig B, Behrens J. The Wnt signaling pathway and its role in tumor development. J Cancer Res Clin Oncol 2003;129:199–221.
79. Tsuji K, Bandyopadhyay A, Harfe BD, et al. BMP2 activity, although dispensable for bone formation, is required for the initiation of fracture healing. Nat Genet 2006;38:1424–1429.
80. Asahina I, Sampath TK, Hauschke PV. Human osteogenic protein-1 induces chondroblastic, osteoblastic, and/or adi-pocytic differentiation of clonal murine target cells. Exp Cell Res 1996;222:38–47.
81. Canalis E. Effect of insulinlike growth factor I on DNA and pro-tein synthesis in cultured rat calvaria. J Clin Invest 1980;66: 709–719.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

80 Volume 26, Supplement, 2011
Growth and Differentiation Group Members
Group ChairClark Stanford, DDS, PhD
Group ExpertPaul Krebsbach, DDS, PhD
Group SecretaryJoseph Fiorellini, DMD, DMSc
Group ParticipantsJocelyn Feine, DDS, MS, HDRStuart Froum, DDSLuis Fujimoto, DMDJeffrey Ganeles, DMDMarjorie Jeffcoat, DMDOle Jensen, DDS, MSJanice Lee, MD, DDSJay Malmquist, DMDMichael Pikos, DDSAlan Pollack, DDSGeorge Romanos, DDS, DMD, PhDDaniel Spagnoli, DDS, PhDGil Triplett, DDS, PhDUlf Wikesjo, DDS, DMD, PhD
Lori Bateman (Silent Participant, Quintessence)Ira Cheifetz, DMD (AAOMS)Paul A. Fugazzotto, DDS (Straumann)Vicki Gaines (Silent Participant, DENTSPLY)Samuel Low, DDS (AAP)Anna Karin Lundgren, DDS, PhD (Astra Tech)William Ryan (Silent Participant, Nobel Biocare)James Thomas (Medtronic)
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 81
In the conceptualization of the Academy of Osseoin-tegration’s Silver Anniversary Summit on the impact
of biological and technological advances on implant dentistry, a variety of clinical issues were raised in the planning sessions leading up to the workshop. One of the most important clinical aspects arising out of these planning sessions was the importance of im-proving the predictability of dental implant site de-velopment for both hard and soft tissues. In order to do this, working groups were divided into the basic pyramid often used to describe tissue engineering, namely, scaffolds (bioengineering/tissue engineer-ing and nanotechnology; cell source [stem cells]; and growth factors). While the focus of the growth and differentiation group was to approach the different ways to manipulate these complex processes, the discussions really focused on soluble growth factor (GF) being used as biologics. While workshop partici-pants were divided into different groups and charged to discuss one of the four topics, the reality is that the topics are integrated and must work in synergis-tic systems to achieve the desired clinical goals of a rapid, predictable change in tissue volume expedit-ing implant therapy with (hopefully) ease of use and reduced cost, complications, time, and morbidity for our patients.
The concept of manipulation of growth and dif-ferentiation in the content talk provided by the group expert quickly focused on this interactive role of the scaffold, cell source, and growth factors in the cre-ation of microenvironments in bone; sometimes re-ferred to as a microniche in bone. As a part of the shift to regenerative medicine, the future movement will be towards combinational therapies where a scaffold structure provides timed release of factors to enhance the local activity in the complex local microenviron-ment. An important part of our expanding subject of growth factors and signal transduction events is the role of increased bone formation through key signal-ing pathways such as the wnt10 pathway, as well as the rich and complex process of TNF-alpha binding toll-like receptors, and the osteogenic expression of inflammatory macrophages that participate early in the wound-healing process. This rich interaction includes neural, vascular, mesenchymal cells (osteo-blasts, adipocytes, chrondrocytes, myoblasts) that interact and can be manipulated by both local and systemic (eg, central nervous system) control. The future scaffold constructs should address current bio-logic issues such as cellular and vascular in-growth. These also should improve physical concerns such as the ability to be modeled/shaped and rigidity.
The local release of autocrine and paracrine factors includes the well-described members of the BMP fami-ly (BMP-2 and BMP-7), PDGF, IGF-1, GH, GDF-5, PTH, etc. Most research has focused on biological behavior when used as a single factor rather than at a lower concentra-tion of a more rich mix of factors designed to interact in a predictable pleotrophic manner(s). The clinical appli-cation of these factors has focused in dentistry on the BMP-2 and PDGF used in a singular fashion, which has, in part, led to the need for supraphysiologic dosage levels for clinical efficacy. The group expert outlined multiple factors in the developmental pipeline (FGF-2 in phase III/IV trials, GH and GDF-5 in phase II, and GLP-2 and CatK inhibitor in early phase I trials), all of which hold potential. Again, it was outlined that biol-ogy of these factors needs to be considered in the con-text of the bone microenvironment. Furthermore, the desired goal sometimes is the inhibition of GF expres-sion rather than a formative or anabolic one; examples include approaches to prevent catabolic events (eg, osteoclastogenesis). The exploration of developments in axial skeleton biology needs to continue with the ex-ample of the recent clinical applications of PTH and its strong stimulatory development of cancellous bone. PTH, when placed into a carrier system that allows an intermittent release pattern, can accelerate bone for-mation. An important example outlined is the role of vascular development (angiogenesis) and the cross-talk that occurs with osteogenesis. Thus, GF can be ap-plied to the development of appropriate angiogenesis (VEGF, bFGF, HIF, PDGF, IGF-I/II, and angiopoietin) that sets the stage for osteogenesis but reduces the need for an ongoing long-term exposure to a labile soluble growth factor that is easily degraded, bound-up in in-hibited states, or sequestered from participating in the local microenvironment. As there is ongoing develop-ment in the area of clinical application of growth fac-tors to manipulate growth and development, there will be an increasing appreciation of the role of higher signaling, especially by the central nervous system, which, in time, may play a more important role in ma-nipulating the wound-healing processes that clinicians are attempting to motivate. However, today’s tools are crude with the high-burst doses of growth factors that are the equivalent of using “a nuclear weapon to kill an ant”; effective, nonspecific, and messy. The nuanced approach will come with a greater appreciation of the interactive mechanisms of scaffold delivery, ie, sequen-tial growth factor release with the correct responder cells in place. Overall, the specificity of the signal or sig-nals to produce the desired effect would be critical in predictable tissue regeneration.
Growth and Differentiation Group Report
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and Differentiation Group
82 Volume 26, Supplement, 2011
The working group then entered into a lengthy discussion that revolved around articulating the pri-mary rationale for manipulating growth and develop-ment though the use of soluble biologics (eg, growth factors and hormones) and considering the potential for these approaches in assisting in patient care. The following questions were addressed.
What is the primary rationale for the development of approaches to manipulate growth and differentiation?
The primary rationale for this ongoing pathway of discovery includes: the need to assist the surgical specialties due to the limitations of current grafting technologies, the need to develop better controlled release devices, and the need, as clinically observed, to improve the predictability of surgical grafting (re-duce morbidity, multiple surgeries, limitations in vol-ume, and patient perceptions of limitation, such as time off from work, etc). The importance of this on-going area of development is especially evident due to the frustration of clinicians who want to increase the predictability of grafting approaches and expand the indications for tissue regeneration, eg, vertical augmentation. Thus, the working group outlined the need to improve the entire site development process though judicious application of technologies that ma-nipulate growth and differentiation to expand patient eligibility, the efficacy and effectiveness of grafting in common-day practice, especially in medical compro-mised patients, with a goal to expedite therapy with reduced morbidity. This can lead to the integrated goal of working with cellular plasticity to change the “older” microniche observed in our medically compro-mised patients to a “younger” microniche that allows a recapitulation of predictable accelerated healing.
What is the potential for manipulation of growth and differentiation to improve clinical outcomes of implant therapy?
An important aspect of the working group discussion focused on the role that growth factor technologies will perform in reducing the amount of time patients are im-pacted by the site development process (eg, less time off from work), in reducing morbidity, and in expanding the range of options for the clinician who doesn’t have as much clinical experience (the effectiveness of care). One of the greatest attributes would be the potential for reduced treatment time and expanded use though sim-pler modes of biological handling and use.
Who are the patients most likely to need or want to be candidates for the use of therapies that manipu-late growth and differentiation?
Manipulation of growth and differentiation for spe-cific patient populations was discussed at length by the committee. Implant dentistry currently achieves high dental implant survival rates for most therapies, and failures are in part associated with the confound-ing systemic medical conditions that patients present with. Ultimately, the use of growth factors, if cost ef-fective, will assist in expanding the ability to care for patients with extensive confounding health histories which would currently limit or prevent dental implant therapy. To this end, the application of growth fac-tor–supported augmentation will assist the medically compromised, those with autoimmune disorders (eg, rheumatoid arthritis), diabetics, patients with con-genital anomalies, and the more general patient with very large augmentations or revisions of grafted sites with previously failed augmentations.
Will the potential for manipulation of growth and differentiation improve a patient’s physical health (oral and systemic) and quality of life (ie, psycho-logical, functional)?
In regards to the impact on the patient from the ap-plication of growth factors either indirectly (eg, graft-ing) or directly in implant therapy (eg, used directly in, on, or at the time of implant placement), the greatest impact would be to accelerate the time to completion of care with fewer interventions, less time off work, less morbidity, and overall less impact on the general quality of life (QOL) of the patient. One aspect con-sidered at length was the potential to “cost-share” the advantages of therapies a patient may already be on for other conditions (eg, osteoporosis) or to provide a new therapy to manage a number of comorbid con-ditions (low bone mass, history of corticosteroid use, etc) to facilitate a holistic response to axial skeletal needs as well as the local needs of improving the out-comes of augmentation of the local site for implant therapy. An example discussed was the application of parathyroid hormone (PTH) for osteoporosis (in place of the current emphasis on bisphosphonates) and the use of the beneficial anabolic effects of PTH for site development coupled with a more anabolic PTH-induced response to the local implant-site graft-ing approach of choice.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and Differentiation Group
The International Journal of Oral & Maxillofacial Implants 83
Is there current evidence to warrant further re-search and resources being allocated towards ma-nipulation of growth and differentiation relative to implant therapy?
In the recent past, there have been examples of growth and differentiation approaches (BMP-2, BMP-7, and PDGF) showing positive results in limited applica-tions. The clinical experience shows the advantages (eg, angiogenesis, volume development) along with the limitations (eg, cost, swelling, role of scaffold structures in outcomes of site development). To date, in implant dentistry, the application of biologics ap-pears to have the highest benefits in areas protected from mechanical loading (eg, maxillary sinus). Areas subjected to loading appear to be more limited but, to validate the role of growth factors in the augmentation process, it will be important to develop new outcome measures that are more precise than the conventional radiographic approaches used. Furthermore, it is very important to validate these therapies by understand-ing the actual biology of the developed tissues and to validate that the tissues were actually formed due to the biologic process versus being the result of the graft ma-terial, the site, the surgical approach, the scaffold, the membrane, or time of the moon, etc. There are ongo-ing investigations of systemic markers for bone devel-opment that will be helpful in tracking the outcomes of augmentation procedures. Further, as the developed tissues undergo remodeling, there is a need to know the potential for the developed tissues to undergo the normal BMU remodeling process,1 an important issue that has not, to date, been clarified. Also necessary is the need to know how dental implants placed in the augmented sites will fare over time in regards to reces-sion, bone loss, etc. All of these are important questions in the process of development of these technologies and relate to clear documentation of clinical outcomes. This raises the importance of longitudinal documen-tation of clinical outcomes and the need for ongoing research networks related to the care of patients with these technologies. In the development of the BMP-2 biologics, there were a number of clinical studies that are now approaching two decades out from the origi-nal studies. This is an example of an early population that would now have value to systematically evaluate for outcomes to date.
The evidence needed to document the role of manipulation of growth and differentiation was then considered. This was done in regards to the technical properties or problems expected and unexpected, the safety of these approaches, the efficacy and ef-fectiveness, the economic factors, and finally the potential legal and ethical issues impacting on the application of these therapies to dental patients.
What evidence is necessary for the technical proper-ties needed to manipulate growth and differentiation?
In the application of soluble biologics, the role of the carrier system is vital. The biologic can only provide one aspect to the formula to develop a tissue; the neonatal scaffold architecture needs to be protected in order to maintain the desired shape and volume. This also needs to be coupled with sufficient physical properties of the biological construct to maintain the architecture in the desired augmented area as the tissue matures. Previous attempts have been insufficient (eg, granular carrier systems leading to excess mobility of the graft mate-rial). Thus, the development of approaches needs to continue to manipulate the formative perioteum in the site of interest along with the ongoing development of optimization criterion for the carrier system itself (par-ticle size, solubility, etc). This outlined the importance of considering the role of a biologic related to the rate of release, when it is released, and the spatial process of release during wound healing. This complexity needs to be balanced with the source of cells that will/can re-spond as well as the vascular development needed for the graft to succeed. In addition, the process of tissue development may need not only hard tissue but soft tissue development (eg, keratinized mucosa or epithe-lia) that can expand at a rate to allow coverage of the developing augmented site. Specific technical issues outlined in the discussions included the need to devel-op combinational therapies that focus on vascular sup-ply as a key part of the development of combinational approaches (scaffold, cells, and factors) necessary for successful site development.
What evidence is necessary for evaluation of safety issues when manipulation of growth and differen-tiation is used?
In general, safety in the use and application of GF is crit-ical and is the basis of beneficence. The impact of a GF delivery system (eg, scaffolds) is important in managing the potential toxicity that is associated with improper dosing (too little or too much) or temporal exposure (too short or too long). To date, the exact bioactive dose of GF, such as currently used BMP-2, is unknown. The dose levels are recognized to be supraphysiologic, indi-cating much further work is needed in understanding the delivery approaches and cofactors such as binding proteins and the timing needed to achieve safe and optimal results. This outlines the risk-benefit ratio, es-pecially when the GF is used “on-label.” Unfortunately, many clinicians do not follow the developed protocols, leading to variable results blamed on the biologic rath-er than the procedure in which it was used.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Growth and Differentiation Group
84 Volume 26, Supplement, 2011
What additional evidence is needed for evaluating the efficacy and effectiveness of the application of GF in practice?
The use of biologics to manipulate growth and dif-ferentiation is aimed at a controlled recapitulation of wound healing for hard and soft tissues. To do this, a clear understanding of the osteogenic properties of the biologic construct relative to the osteodestruc-tive properties (eg, improper dose, release kinetics, scaffold binding properties, etc) is needed. The com-mittee agreed that GF constructs need to be aimed at being clinically “forgiving” to allow the average busy clinician to predictably utilize the therapies in routine practice.
What additional evidence should be gathered re-garding economic factors associated with the devel-opment of approaches to growth and differentiation?
A positive cost-benefit ratio will be critical to the incor-poration of biologic strategies for use in routine care. The current cost to bring to market soluble biologics is very high with limited return, especially when the ap-proved set of applications is limited. Data are needed to show that the putative biologic must provide a sub-stantial impact in reduced morbidity, accelerated heal-ing, higher QOL, and enhanced predictability in a wide range of patient and clinical situations. The ability to utilize such therapies leads to the potential to expedite care with less travel time, fewer visits, and less disrup-tion to a patient’s general routine. Finally, this must be at a cost-benefit ratio that is consumable within the current health-care funding system for oral health care.
What additional evidence should be gathered regard-ing legal and ethical issues associated with the devel-opment of approaches to growth and differentiation?
Health care has become increasingly complex, with new diagnostic and therapeutic approaches to ad-dress a wide range of maladies. This complexity is not necessarily assisted by the advent of new information sources (eg, the Internet). This adds to the burden of the process of informed consent for the oral health team. The process, embraced within the legal con-structs of case law, requires the present group to pro-vide a comprehensive discussion on the value of the use or non-use of biologics with a clear discussion of what is known and what is unknown about the bio-logic. A clinical team may chose to not utilize a bio-logic, but this decision needs to be assessed within a health-technology assessment of the cost-benefit weighted with the current best clinical evidence of relevant outcomes of care.
RefeRence
1. Stanford CM, Brand RA. Toward an understanding of implant occlusion and strain adaptive bone modeling and remodel-ing. J Prosthet Dent 1999;81:553–561.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 85
Findings1–4 from a number of consensus confer-ences and reviews over the last 12 years have
clearly demonstrated that, using an evidence-based approach to systematically evaluate the existing re-search supporting the efficacy of implant therapy for replacement of missing teeth, both the quality of de-sign and the inclusion of adequate outcome measures (in terms of standardization, validity, and relevance to patient) are lacking. However, despite the shortage of controlled trials and the variability in defining implant survival/success, a high number of implants that vary in design and construction are being used in patients, along with highly variable levels of clinical expertise and clinical environments worldwide. What remains for clinicians is little robust evidence regarding the performance of these devices in general populations. The inconclusive evidence is clearly insufficient for
1 Professor of Dentistry, Mayo Clinic College of Medicine, Department of Dental Specialties, Rochester, Minnesota.
2 Professor, Division of Otololarynology – Head and Neck Surgery, Department of Surgery, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada; Director of Clinics and International Relations, Institute for Reconstructive Science in Medicine, Misercordia Community Hospital, Edmonton, Alberta, Canada.
3 Professor of Dentistry, Division of Advanced Prosthodontics, Biomaterials and Hospital Dentistry, Weintraub Center for Reconstructive Biotechnology, School of Dentistry, University of California at Los Angeles.
None of the authors reported a conflict of interest.
Correspondence to: Dr Neal Garrett, Division of Advanced Prosthodontics, Biomaterials and Hospital Dentistry, Weintraub Center for Reconstructive Biotechnology, UCLA School of Dentistry, PO Box 951668, Los Angeles, CA 90095-1668. Email: [email protected]
Capturing Patient Benefits of TreatmentAlan Carr, DMD, MS1/John Wolfaardt, BDS, MDent, PhD2/Neal Garrett, PhD3
Findings from the Academy of Osseointegration State of the Science on Implant Dentistry Conference clearly demonstrate that data are lacking regarding both quality of design and adequate outcome measures (standardization, validity, and relevance to patient) to support an evidence-based systematic evaluation of implant efficacy. Despite the dearth of controlled trials and the variability in defining implant survival/success, the preponderance of evidence is viewed as lending support for consideration of dental implant therapy as a safe and predictable alternative to conventional restorations for many applications. However, this minimal conclusion undermines the best intentions of the dental profession, which is striving to substantiate to the patient, third-party providers, and the government the relative benefits and risks of various prosthetic treatment alternatives. The conclusions of multiple consensus conferences have repeatedly stressed that additional research with good strength of evidence following a broad spectrum of outcomes is vital to extend the breadth of conclusions regarding dental implant treatment efficacy. However, without a set of consensus-based core outcome measures addressing pertinent clinical and patient-centered factors, future expensive, time-consuming, and technically complex clinical studies may suffer the same critical flaws seen in the current body of research. It may be possible and useful to establish a core set of well-defined, discriminatory, and feasible outcome measures for common utilization and a hierarchy of additional recommended outcome measures for specific benefit categories. Such a standardized group of outcome measures would be likely to significantly enhance the potential for future research. In addition, with the formation of consensus guidelines, there would be an opportunity for scientific journals to promote the quality of implant dentistry research by suggesting the inclusion of these core outcome measures in studies submitted for publication. Int J Oral Maxillofac Implants
2011;26(suppl):85–92
Key words: clinical trials, consensus, dental implant, outcome measure
OutCOmes
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
86 Volume 26, Supplement, 2011
the profession, which must substantiate to the pa-tient, third-party providers, and the government the relative benefits and risks of various prosthetic treat-ment alternatives. The lack of inclusion of adequate outcome measures and poor reporting of those out-comes collected have been repeatedly described as critical limitations in a wide variety of questions focusing on implant-related factors. Since the use of dental implants for tooth replacement is growing and has been associated with the potential for “standard of care,”5 it has been recognized1–4,6,7 that it is critical to provide substantive research with good strength of evidence based on a broad spectrum of outcomes to extend the breadth of conclusions regarding dental implant treatment efficacy.
PrOblems with the Current state Of OutCOme measures in imPlant Dentistry
Both the European Association for Osseointegration Consensus Conference (EAO CC) and the Academy of Osseointegration State of the Science on Implant Dentistry (AO SSID) workshop revealed numerous specific problems with existing approaches to im-plant outcome measures. Examples abound in every section from both published proceedings.
The question of success with hard tissue augmenta-tion was taken up at both meetings. At the EAO CC, re-sults related to augmentation procedures and guided bone regeneration8 were difficult to interpret because an “analysis of available publication demonstrated, on average, a poor methodological quality, in particular with regard to… implant outcome according to well-defined success criteria…8p139 The same basic problem was also found for studies of autogenous onlay bone grafts, sinus grafting, and Le Fort I osteotomy. Similarly, the AO SSID found that studies of tissue augmentation for successful bony support of implants included a high proportion (37/90) of trials that did not include objective outcomes, and there was variability in the criteria for those that did.9 In the discussion of their analysis, Aghaloo and Moy reported that “almost half of the articles did not use objective criteria to evaluate implant success, and 75% did not report a cumulative survival rate in the form of a life table analysis.”9p60
The effect of time to implant loading was evaluated at both conferences. The AO SSID discussion indicated that even the “simple” outcome of implant survival was determined inconsistently across studies, making it im-possible to pool the results.10 As the result of limited studies with small sample sizes, the EAO review con-cluded that “definitive conclusions could not be drawn concerning survival and success rates of immediately
loaded implants compared with conventionally load-ed implants.”11p19 The working group also indicated a need for studies that include an assessment of patient critical outcomes, which is lacking studies of immedi-ate loading of implants.12 Additionally, when looking at effects of forces on peri-implant bone, there were insufficient outcome measures of occlusal forces and clinical studies with very limited numbers of implant failures,” making it “difficult to discover a possible cor-relation between occlusal forces (overload) and im-plant failures.”13p15 Even when failures were reported, the EAO working group observed that “only a few au-thors report possible reasons for implant failures.”12p53 Other questions regarding biomechanical aspects of implants indicated that studies of the effect of implant length and diameter on survival suffered from “a wide range of approaches to study design, data reporting, definition of terms, implant geometry and surface, methods of statistical analysis, and success and survival criteria. Consequently no attempt was made to apply a meta-analytic technique.”14p36 Measures of resonance frequency analysis (RFA) continue to be questioned because of a lack of validated prognostic value and normative scores for the implant stability quotient, resulting in the observation that “at the present time, the validity and relevance of RFA for clinical use have to be questioned.”15p4 Similarly, no prognostic value has been shown for Periotest measurements and “sen-sitivity may be low.”15p6 It was also not possible to apply meta-analytic techniques for evaluation of the effects of surface and material characteristics on biofilms be-cause of “heterogeneity of the studies and outcome variables.”16p72
The influence of local and systemic conditions, including smoking, diabetes, and periodontitis, on important outcome measures such as “bone loss, mi-crobial assessments, peri-implantitis, or other compli-cations,” was not able to be determined by the AO SSID working group because of a lack of reporting.17p196 EAO CC evaluation of the literature on the effects of systemic diseases on osseointegration resulted in an inability to perform any meta-analysis as a result of the “heterogeneity of the material and the method of data reporting.”18p97
Review of the issues related to soft tissue integra-tion of implants led to the conclusions that “[f ]uture research should focus on…subjective parameters of the patient also respecting the changes related to the insertion of the definitive restorations”19p94 and “[t]here is little information from human studies as-sessing the soft tissue interface using clinical outcome measurements.”19p95 Meta-analysis was also not pos-sible when looking at marginal soft tissue response to immediate loading or restoration because “many different procedures and follow-up times, time points
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Carr et al
The International Journal of Oral & Maxillofacial Implants 87
and evaluated soft-tissue parameters varied consider-ably between the different articles.”20p82 Comparisons of implant restorations to tooth-supported restora-tions for single-tooth replacement were extremely limited because of a lack of outcomes.21 Although successful treatment was frequently reported, “suc-cess criteria were rarely identified in articles,”21p74 and only survival could be evaluated.21 The nature of fail-ures and complications was frequently not available, and it was concluded that the “scientific data are not available to answer the question posed,”21p80 namely, the relative efficacy of conventional and implant res-torations for the single tooth.21 The situation is even worse for evaluation of treatment of teeth needing endodontic treatment with endodontic therapy or im-plant-supported restorations, where “sufficient data to compute the survival rates of restored root canal treated teeth” are often not provided.22p100 Typically, the evaluation criteria for success of endodontically treated teeth tend to be much more stringent than for implant restorations, “including presence or absence of periapical radiolucencies, clinical function, and his-topathological evaluation of biopsied tissue.”22p103
Evaluation of the efficacy of implant-supported prostheses for the partially and completely edentu-lous arch faced the same problems: a lack of sufficient outcomes presented or inconsistent application of outcome measures across studies. In the case of the edentulous arch, the “review of prosthetic outcomes… has been hampered to such a degree that it may prove impossible to determine the extent to which the ap-parently widely ranging differences in prosthetic maintenance across prosthetic types actually reflect important differences between groups; such differ-ences may simply reflect differences in application of the outcome measures.”23p132 Similar variability and heterogeneity among studies in outcomes was also found for partially edentulous applications, with only a few studies employing validated success criteria; “most others applied their own measures, which often were not well described, to determine an outcome.”24p167
Finally, after taking up the question of the effect of timing of implant placement with regard to ex-traction, the AO SSID found that the only significant datum available as an outcome was implant loss.25 While “esthetics was frequently cited as a reason for immediate implant placement, data on the esthetic outcome following immediate implant placement are still lacking.”25p216
In summary, every question assessed in these two extensive reviews of the implant literature was faced with severe limitations to evaluation because of the inconsistent application of definitions for critical out-comes and an overall lack of clinically relevant, valid, and patient-centered outcomes.
attemPts at COnsensus On COre OutCOmes
To address a lack of standardization and inadequate and insufficient outcomes, researchers focused on a variety of specific diseases have sought to create con-sensus in their fields for core outcomes covering a range of domains. Expert groups have been convened in areas such as cancer/oncology26,27 (the European Organization for Research and Treatment of Cancer, the Research Network of the European Association of Palliative Care), chronic pain28 (Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials), arthritis care29 (CARE conferences), and rheumatoid ar-thritis30,31 (Outcome Measures in Rheumatoid Arthri-tis Clinical Trials [OMERACT]). These efforts are based primarily on the development of expert panels of cli-nicians and researchers in the field of interest and at-tempts to come to initial agreement on core domains for outcomes, such as physical function, psychologic impact and function, treatment satisfaction, eco-nomic impacts, treatment success and complications, and methods of reporting treatment compliance/ withdrawal/loss to follow-up.
the COnCern abOut OutCOmes
The emphasis on evidence-driven health care has ex-panded dramatically over the past few decades. The strength of evidence-based methods is related to the rigor of clinical trial design. However, there have been concerns regarding both the pragmatic and intrinsic limi-tations of trials, especially randomized controlled trials.32
An important limitation of clinical trials relates to the relatively short period during which researchers are able to observe responses.33 This necessitates that surrogate outcomes be used, and frequently surrogates lack the evidence necessary to validate their prognostic value. The outcomes concern has a practical dilemma, as there is a lack of agreement as to what are the optimal pri-mary outcomes for monitoring health care. Addition-ally, if the term “outcome” means an effect related to the management of or intervention for patient health and well-being, it becomes clear that such a measure must reflect the concerns of patients, who ultimately are the true measure of the effectiveness of care. This has been addressed in rheumatology by suggesting that a hierar-chy of outcomes exists; this stresses the patient-based value of outcomes and highlights the need to validate clinical and laboratory outcomes with respect to their impact on tangible patient-perceived responses.34 This is especially pertinent to the elective management of tooth loss, a chronic condition that is managed over the long term to address a patient-perceived concern.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
88 Volume 26, Supplement, 2011
There is also the potential that outcome confu-sion exists because providers vary in their perspec-tive of care, as some provide single episodic care (ie, surgeons), while others manage the ongoing needs of patients with chronic problems, such as tooth loss. Since the focus of outcome-related research has shift-ed to clinical conditions and away from procedures/treatments, the utility of outcome refinement (OMER-ACT) and monitoring is found in a chronic illness management context. It is easy to understand that a chronic disease management context versus a treat-ment context forces clinical observations to take into account measures over time.35
OutCOmes COnsensus: sOme examPles
immPaCtTypical of many consensus efforts, the development of consensus on outcome domains and measures for assessment of chronic pain was based on the selection of a panel of experts. The initial IMMPACT consensus28 in 2002 focused on the development of critical domains of outcomes to recommend for inclusion. The panel of 27 included academic, gov-ernmental, and industry (pharmaceutical) leaders with experience in clinical application, research, or administration related to the evaluation of therapies for chronic pain. Each of the participants was pro-vided with background material with reviews of pain assessment studies and current clinical trial method-ologies prior to the consensus meeting. The domains represented in the existing literature were discussed at the consensus meeting, with two leaders guiding the discussion. Consensus on the domains to be rec-ommended was achieved by a formal vote, and the same two leaders developed the meeting summary for approval by the participants.
With the domains identified, a second consensus meeting was convened in 2003 to develop recom-mendations for core outcomes in each of the six do-mains.36 A panel of 35 experts was selected, similar in background to participants in the first meeting, with the addition of representation from a “self-help” group. Background material covering the various outcome measures in the core domains was provid-ed to participants prior to the meeting. During the discussion of the specific measures, key criteria for comparison of measures included validity, reliability, sensitivity to treatment, appropriateness, and feasi-bility (burden to patient and clinician). If this informa-tion was not available for a measure, it was no longer considered. Specific measures that had information that fulfilled these five criteria were evaluated accord-
ing to their strength for these attributes. Consensus was achieved for at least one measure in each of the six domains. It is interesting that the authors empha-size that the recommended core outcome measures are suggested for inclusion but should not be consid-ered as a necessity for publication or for regulatory requirements.
OmeraCtOne of the most refined models for the development of consensus on key outcome measures is seen in rheumatology. In 1992, OMERACT, a conference fo-cusing on outcome measures in clinical trials for rheu-matoid arthritis treatments, was convened following a series of five meetings on outcomes in clinical trials in rheumatoid arthritis from 1980 to 1992. This con-ference resulted from the recognition that outcomes across the range of clinical trials on rheumatoid ar-thritis varied considerably, often appeared to have poor validity, and did not always reflect clinically im-portant patient and clinician impacts.37 The goal of this conference was to address these concerns about the need for valid and clinically relevant measures and potentially come to agreement on a minimal core set of outcomes that could be included in all clinical trials on rheumatoid arthritis. The conferees also rec-ognized that new outcome measures would be de-veloped in the future and that additional data might change the desire to include a specific measure in the core. To respond to this need for continuing review, they have maintained an effort to continually refine the measures. This “data-driven, iterative consensus process”38 has led to conferences being convened ev-ery 2 years since 1992, with OMERACT 10 having been held in May 2010.
The OMERACT Process. Over the many years of operation of the OMERACT group, the specific meth-ods used to develop an OMERACT conference have changed slightly as it has grown, but they have fol-lowed a similar general path. Prior to a conference, an organizing committee gathers input from experts in the field, and a committee is formed to organize and guide the conference. Preparation includes develop-ment of domains to be discussed, literature review for collecting the measures to be considered, and potential additional issues that will need to be dis-cussed at the conference. Workshop discussions at the conference include presentation of critical stud-ies, agreement on domains to be included, identifica-tion of gaps in knowledge, definitions of the specific elements of agreement and disagreement, and the development of research priorities. Next, evidence from the literature and ongoing studies is reviewed for specific measures within a domain, and the final selection of the potential pool of measures is done. A
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Carr et al
The International Journal of Oral & Maxillofacial Implants 89
mixture of plenary sessions, small groups, and infor-mal discussion provides the opportunity for all partic-ipants to have a voice. Last, a plenary session is held to develop a final consensus on domains and mea-sures. In some cases, the data may not be sufficient to make a decision on specific domains and measures, and consensus may lead to the development of a re-search agenda to acquire the critical evidence. Voting is typically done via an electronic audience response system with appropriately formatted questions.
Final selection of potential measures to be evaluat-ed for inclusion in core outcomes guidelines is made using the “OMERACT filter,” which assesses whether a measure is truthful and valid, whether it possesses discrimination, and whether it is feasible. Only those measures that meet these requirements possess char-acteristics appropriate for clinical use. Tugwell et al38 define the elements of the filter as follows:
1. Truth: Is the measure truthful, does it measure what it intends to measure? Is the result unbiased and rel-evant? This criterion captures the issues of face, content, construct, and criterion validity.
2. Discrimination: Does the measure discriminate be-tween situations that are of interest? The situations can be states at one time (for classification or prognosis) or states at different times (to measure change). This criterion captures the issues of reli-ability and sensitivity to change.
3. Feasibility: Can the measures be applied easily, giv-en constraints of time, money, and interpretability? This criterion addresses the pragmatic reality of the use of the measure, one that may be decisive in determining a measure’s success.38
Only those measures that are acceptable for all three criteria “pass” this filter and possess the neces-sary characteristics for consideration as a member of the recommended outcomes set.
OMERACT Progress. From an initial grassroots ef-fort that led to approximately 80 participants at the first conference, the group had grown to almost 200 at OMERACT 9. This growth in participants is particu-larly impressive given that it requires a significant amount of volunteer time over a period of years to reach consensus on a set of outcome measures. The initial conference resulted in a set of rheumatology outcomes, which were ratified by the World Health Organization and the International League for Rheu-matology. This core set of outcomes has been under continuous review at subsequent conferences and modified as appropriate. Additional core sets of out-comes have been identified for specific diseases, and measures of cost-effectiveness and adverse events have been added.
Patient representation in the process has been broadened to highlight the domain of patient ben-efit. The inclusion of a Young Investigators’ Day at the fifth conference provided an extension of opportu-nity for participation and review to next-generation leaders and will help maintain the momentum of the organization.
Two other groups have adopted the OMERACT framework—one working on outcomes in the field of juvenile arthritis and the other in the area of ankylos-ing spondylitis—and both have developed at least an initial core set of outcomes.
OutCOme DOmains
Because judgment of treatment results requires that a broad spectrum of influencing factors be considered, outcomes may be expected to cover multiple areas relevant to the patient and dentist. Outcomes relevant to implant-based prosthodontic therapies have been proposed39 to be contained in four primary domains, with subcategories in each of the primary areas. Four primary outcome domains could be structured as: (1) longevity (including survival/success, time to retreat-ment, biologic complications, mechanical complica-tions, bone loss, and soft tissue complications); (2) economic (including initial and maintenance direct costs, indirect costs, disparities in health care, and third-party policies); (3) physiologic or functional (speech, swallowing, mastication, nutritional needs, and motor and sensory function); and (4) psychologic (including treatment satisfaction, self-image and con-fidence, esthetics, function, hygiene, treatment pref-erence, provider bias, and health-related and overall quality of life). In addition, a fifth topic—the evalua-tion and reporting of compliance with study design for subject enrollment, treatment delivery, withdraw-als, and subjects lost to follow-up—would need to be considered for standard reporting guidelines similar to sections of the CONSORT 2010 Statement.40
Guidelines could include a core set of well-defined, validated, discriminatory, and feasible outcome mea-sures for common use, as well as a hierarchy of addi-tional recommended outcome measures for specific benefit categories. Examples of critical factors to be considered in the development of guidelines on out-comes would include patient characteristics (Table 1), treatment variables (Table 2), and core outcome set(s) (Table 3) with relevance to specific implant interven-tions and dentition status.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
90 Volume 26, Supplement, 2011
POtential COntributiOns anD DevelOPments
To evaluate the effectiveness of creating core sets of outcome measures, there would need to be an objec-tive assessment of the changes in outcome measures used in clinical studies since the core measures were suggested. One would expect that if they are being utilized, the number of studies reporting the same measures would increase and the number of unique outcomes measuring the same domain would de-crease. However, for both the IMMPACT and OMER-ACT efforts, there has been no critical assessment of these factors in the literature since their recommen-dations were published. Therefore, the degree of ef-fectiveness of these models in improving the quality and comparability of studies is not known.
Intuitively, the development of one or more stan-dardized sets of core outcomes that would be relevant and desirable for studies of implant treatment out-comes, along with supplemental outcome measures for specific types of implant therapy, would seem to greatly benefit the ability of practitioners to address critical clinical questions in the future. Common mea-sures would permit researchers to combine data from multiple studies for meta-analysis and greater use in clinical environments (feasibility) to obtain effective-ness estimates. With the formation of appropriate guidelines, there would be an exceptional opportu-nity for the associated journals to promote greater quality in implant dentistry research by recommend-ing the inclusion of core outcome measures in clinical studies, similar to CONSORT guidelines.
table 1 Patient variables/Characteristics
medical
Age and health
Smoking history (pack-years)
Social history, alcohol
Diabetes (insulin- versus non–insulin-dependent)
Immunocompromise (eg, HIV, chemotherapy)
Osteoporosis
Bisphosphonates (brand, y)
Dental
Dental charting
Periodontal diagnosis (probing, bleeding, and plaque scores)
Tooth loss: perio, endo, trauma, ortho
Treatment selection considerations:• RPD, FPD, implant-supported prosthesis• Treatment cost• Adjacent teeth/restorations
Anterior: labial plate intact
Esthetic considerations/demands (eg, high versus low lip line)
edentulous site
Maxilla versus mandible
Anterior versus posterior
Posterior: tooth bound, cantilever
Papillae form
Anatomic considerations:•Bone quality and quantity•Interproximal crest level•Soft tissue (attached versus unattached)•Soft tissue biotype
Adjacent teeth: proximity, bone level
Posterior vertical deficit, vertical cantilever
RPD = removable partial denture; FPD = fixed partial denture.
table 2 treatment variables/Categories
surgical
Time of placement
Time to loading
Grafting procedures (eg, veneer, onlay, sinus elevation, socket preservation)
Grafting material (donor site)
GBR (type of membrane)
Soft tissue procedures
Healing time
Radiographic workup (CT, tomography, panoramic or periapical radiography)
implant
Surface characteristics
Internal versus external hex
Implant diameter
Implant length
Stage (one-stage versus two-stage)
Implant material (cpTi I, II, III, IV; alloy; zirconia)
restorative
Treatment provider
Abutment type
Restoration type (eg, PFM, all-ceramic, metal–acrylic resin)
Retention (cement versus screw)
Provisional
cpTi = commercially pure titanium; CT = computed tomography; GBR = guided bone regeneration; PFM = porcelain fused to metal.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Carr et al
The International Journal of Oral & Maxillofacial Implants 91
It is also recognized that the tools for assessing treatment outcomes and the consensus on the “best” measures available will evolve constantly. It is ex-pected from the previous experiences of the OMER-ACT group that a number of participants in the field will have an active interest in promoting the devel-opment of periodic international review of core and supplemental outcome measures recommended for inclusion in clinical evaluations of oral rehabilita-tion therapies, including implant and conventional prosthodontics.
referenCes
1. Laney WR. State of the science on implant dentistry: Consen-sus conference proceedings. Int J Oral Maxillofac Implants 2007;22(suppl):1–226.
2. Hammerle C, van Steenberghe D. European Association for Osseointegration: First consensus conference. Clin Oral Implants Res 2006;17(suppl 2):1–162.
3. Buser D, Taylor T. Proceedings of the third ITI consensus conference. Int J Oral Maxillofac Implants 2004;19:1–149.
4. Symposium: Towards optimized treatment outcomes for dental implants. Toronto, Ontario, April 24–25, 1998. Pro-ceedings. Int J Prosthodont 1998;11:385–521.
5. Feine JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Montreal, Quebec, Canada, May 24–25, 2002. Int J Prosthodont 2002;15:413–414.
6. Fitzpatrick B. Standard of care for the edentulous mandible: A systematic review. J Prosthet Dent 2006;95:71–78.
7. Allen PF, Thomason JM, Jepson NJ, et al. A randomized con-trolled trial of implant-retained mandibular overdentures. J Dent Res 2006;85:547–551.
8. Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res 2006;17(suppl 2):136–159.
9. Aghaloo T, Moy PK. Which hard tissue augmentation tech-niques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants 2007; 22(suppl):49–67.
10. Jokstad A, Carr A. What is the effect on outcomes of time-to-loading of a fixed or removable prosthesis placed on implant(s)? Int J Oral Maxillofac Implants 2007;22(suppl):19–48.
11. Nkenke E, Fenner M. Indications for immediate loading of implants and implant success. Clin Oral Implants Res 2006; 17(suppl 2):19–34.
12. Hobkirk JA, Wiskott HW. Biomechanical aspects of oral implants. Clin Oral Implants Res 2006;17(suppl 2):52–54.
13. Isidor F. Influence of forces on peri-implant bone. Clin Oral Implants Res 2006;17(suppl 2):8–18.
14. Renouard F, Nisand D. Impact of implant length and diameter on survival rates. Clin Oral Implants Res 2006;17(suppl 2):35–51.
15. Aparicio C, Lang NP, Rangert B. Validity and clinical signifi-cance of biomechanical testing of implant/bone interface. Clin Oral Implants Res 2006;17(suppl 2):2–7.
16. Teughels W, Van Assche N, Sliepen I, et al. Effect of material characteristics and/or surface topography on biofilm devel-opment. Clin Oral Implants Res 2006;17(suppl 2):68–81.
17. Klokkevold PR, Han TJ. How do smoking, diabetes, and peri-odontitis affect outcomes of implant treatment? Int J Oral Maxillofac Implants 2007;22(suppl):173–202.
table 3 example of treatment Outcomes for Consideration (by Domain)
longevity
Maintenance/follow-up period
Implant survival/success
Biologic complications:• Infection, bone loss• Thread exposure
Bone loss
Soft tissue complications
Mechanical complications
Prosthetic complications:• Porcelain fracture• Acrylic wear• Metal fatigue• Screw loosening• Loss of attachment retention• Cement failure• Cement in sulcus• Metal show-through
Prosthetic success (criteria)
Time to retreatment
functional
Speech
Swallowing
Mastication
Nutrition
Motor and sensory function:• Tactile threshold• EMG• Mandibular movements• Bite force• Oral clearance• Oral stereognosis
Psychologic
Treatment satisfaction
Self-image and confidence
Esthetics
Perception of function
Hygiene
Treatment preference
Provider bias
Health-related QOL
Overall QOL
Food preferences
economic
Direct costs
Indirect costs
Maintenance
Disparities in health care
Third-party policies
EMG = electromyography; QOL = quality of life.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
92 Volume 26, Supplement, 2011
18. Mombelli A, Cionca N. Systemic diseases affecting osseointe-gration therapy. Clin Oral Implants Res 2006;17(suppl 2):97–103.
19. Klinge B, Meyle J. Soft-tissue integration of implants. Clin Oral Implants Res 2006;17(suppl 2):93–96.
20. Glauser R, Zembic A, Hammerle CH. A systematic review of marginal soft tissue at implants subjected to immediate loading or immediate restoration. Clin Oral Implants Res 2006;17(suppl 2):82–92.
21. Salinas TJ, Eckert SE. In patients requiring single-tooth re-placement, what are the outcomes of implant—as compared to tooth—supported restorations? Int J Oral Maxillofac Implants 2007; 22(suppl):71–95.
22. Iqbal MK, Syngcuk K. For teeth requiring endodontic treat-ment, what are the differences in outcomes of restored end-odontically treated teeth compared to implant-supported restorations? Int J Oral Maxillofac Implants 2007;22 (suppl):96–116.
23. Bryant SR, MacDonald-Jankowsji D, Kwonsik K. Does the type of implant prosthesis affect outcomes for the completely edentulous arch? Int J Oral Maxillofac Implants 2007;22 (suppl):117–136.
24. Weber HP, Sukotjo C. Does the type of implant prosthesis affect outcomes in the partially edentulous patient? Int J Oral Maxillofac Implants 2007;22(suppl):140–172.
25. Quirynen M, Van Assche N, Botticelli D, et al. How does the timing of implant placement to extraction affect outcome? Int J Oral Maxillofac Implants 2007;22(suppl):203–223.
26. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365–376.
27. Caraceni A, Cherny N, Fainsinger R, et al. Pain measurement tools and methods in clinical research in palliative care: Recommendations of an expert working group of the Euro-pean Association of Palliative Care. J Pain Symptom Manage 2002;23:239–255.
28. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 2003;106:337–345.
29. Backman CL. Outcome measures for arthritis care research: Recommendations from the CARE III conference. J Rheumatol 2006;23:1908–1911.
30. Tugwell P, Boers M. OMERACT conference on outcome measures in rheumatoid arthritis clinical trials: Introduction. J Rheumatol 1993;20:528–530.
31. Brooks P, Hochberg M, ILAR, OMERACT. Outcome measures and classification criteria for the rheumatic diseases. A compilation of data from OMERACT (Outcome Measures for Arthritis Clinical Trials), ILAR (International League of Associa-tions for Rheumatology), regional leagues and other groups. Rheumatology (Oxford) 2001;40:896–906.
32. Pincus T, Sokka T. Evidence-based practice and practice-based evidence. Nat Clin Pract Rheumatol 2006;2:114–115.
33. Pincus T, Sokka T. Clinical trials in rheumatic diseases: Designs and limitations. Rheum Dis Clin North Am 2004;30:701–724.
34. Fries JF. The hierarchy of outcome assessment. J Rheumatol 1993;20:546–547.
35. Carr AB. Successful long-term treatment outcomes in the field of osseointegrated implants: Prosthodontic determinants. Int J Prosthodont 1998;11:502–512.
36. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005;113:9–19.
37. OMERACT, Conference on outcome measures in rheumatoid arthritis clinical trials. Proceedings. Maastricht, The Nether-lands, April 29–May 3, 1992. J Rheumatol 1993;20:527–591.
38. Tugwell P, Boers M, Brooks P, et al. OMERACT: An international initiative to improve outcome measurement in rheumatology. Trials 2007;8:38.
39. Guckes AD, Scurria MS, Shugars DA. A conceptual framework for understanding outcomes of oral implant therapy. J Pros-thet Dent 1996;75:633–639.
40. Schulz KF, Altman DG, Moher D, for the CONSORT group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med 2010;8:18.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 93
OutcOmes
In 2003, 3.7 trillion US dollars were spent worldwide on general and oral health-care services.1 In the public
domain alone, the U.S. National Institutes of Health re-ported a growth in budget from $US26 million in 1945 to nearly US$7 billion in 1990 to $US1.88 trillion in 2004. Those figures are projected to reach US$3.36 trillion in 2013.2 To put this amount into perspective, citizens of the United States spend more than US$6,000 per capi-ta on their health care annually, which translates to ap-proximately $1 out of every $7 of the US final goods and services. Over the past 40 years, as a proportion of the US gross domestic product, health-care spending increased from 5.2% in 1960 to 16.0% in 2003.3 If this previous trend serves as a prediction of future health-care costs, the provision of quality health-care services in the United States may not be sustainable.
What drives the rapid increase in health care expenditures?
Based on the latest United Nations Population Divi-sion report, the world’s population is expected to rise from the current 6.5 billion to 9.1 billion by 2050.4 Nearly all of this growth will be in the developing world. By contrast, the population of developed countries will remain almost static at 1.2 billion. How-ever, led by the United States, developed countries spend up to three times more in health-care dollars than developing and underdeveloped nations. These costs may be a result, in part, of the fact that people are demanding more health services, visiting their physicians more frequently, and utilizing new tech-nologies to improve their health states (eg, magnetic resonance imaging scans, laser treatment, and dental implants). However, an important reason for this in-crease is attributed to the introduction of innovative health technologies and their proliferation in health care.5 As a measure for cost containment, many coun-tries across the globe have focused on limiting the use of high-cost medical technologies. Today, tech-nology is the substance of health care.6 The Interna-tional Network of Agencies for Health Technology Assessment (INAHTA) defines technology as:
1 Assistant Professor, Faculty of Dentistry, Oral Health and Society Research Unit, McGill University, Montreal, Quebec, Canada.
2 Professor, Faculty of Dentistry, Oral Health and Society Research Unit, McGill University, Montreal, Quebec, Canada.
None of the authors reported a conflict of interest.
correspondence to: Dr Shahrokh Esfandiari, Faculty of Dentistry, Oral Health and Society Research Unit, McGill University, 3550 University Street, Room 206, Montreal, QC H3A 2A7, Canada. Fax: +514- 398-7220. Email: [email protected]
Health Technology Assessment in Oral HealthShahrokh Esfandiari, BSc, DMD, MSc, PhD1/Jocelyne Feine, DDS, MS, HDR2
Health-care costs are rising at an alarmingly fast rate worldwide, particularly in developed countries such as the United States. This is predominantly a result of the development of new, high-cost health technologies intended for improved diagnosis and treatment. The purpose of health technology assessment is to systematically determine the true benefits of new technologies, taking into account clinical efficacy/effectiveness and cost as well as societal preference and ethical issues. In this report, the purpose of health technology assessment is explained in light of new developments in oral health technology, particularly intraoral implants. This information is intended to educate and to challenge oral health opinion leaders to consider all of the issues involved in the development and diffusion of new oral health technologies. Int J Oral Maxillofac
Implants 2011;26(suppl):93–100
Key words: decision making, health-care costs, health technology assessment, oral health technology
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
94 Volume 26, Supplement, 2011
an application of scientific or other organized knowl-edge—including any tool, technique, product, pro-cess, method, organization or system—to practical tasks. In health care, technology includes drugs; di-agnostics, indicators, and reagents; devices, equip-ment, and supplies; medical and surgical procedures; support systems; and organizational and manage-rial systems used in prevention, screening, diagnosis, treatment, and rehabilitation.7
There is no dispute that there has been a drastic increase in the pace of research and the development of new technology. Breakthroughs in biotechnol-ogy, diagnostic imaging, organ and tissue replace-ment, molecular diagnostics, surgical techniques, and computer technology have helped tremendously to improve health care delivery and patient outcomes. However, a hefty price tag is often associated with these improvements.8 In addition to advances in sci-ence and engineering, there are many other factors that reinforce the market for health technology. The ag-ing population, new reimbursement mechanisms (ie, third-party payments), financial incentives to technol-ogy companies and clinicians, malpractice avoidance, clinician specialty training, and intellectual property and patent protection are some of these factors.6
health care versus Other marKets
In many ways, the health-care sector differs from oth-er markets exposed to technologic development.
1. Contrary to what is generally perceived, the final consumers are not the patients. It is the clinicians, the hospital management, and the regulatory agen-cies in health care who take on the technologies.
2. Clinicians are often actively involved in develop-ing and assessing a new technology, whereas in other markets, technically advanced researchers develop the products.9
3. Patients are aware of advances in health tech-nology through the media, the Internet, and direct-to-consumer advertising (eg, television advertisements on newly developed drugs). The public is quickly impressed by reports on the ben-efits of new technologies, which often contrib-utes to a chaotic environment surrounding a new technology. Those who constantly hear success stories about various technologies become tech-nology-prone.10 An abiding fascination with new technology or an attitude of technologic impera-tive by the public is common across all markets, but in health care, patients seek medical care that will help to improve their health, and advances in
medical technology are perceived as an obvious way to promote this goal. However, the perceived effectiveness of these advanced technologies may differ from the actual health gain.
4. Most government regulatory bodies seem to provide an incentive toward the development of high-quality, high-cost technology, rather than the development of good-quality, low-cost tech-nology. For instance, the assessment of a big-ticket imaging device like a computed tomographic scan is easier than assessing numerous laboratory tests.
5. High-cost technology provides a strong momen-tum for the drug and medical devices industry to market new technologies. It seems that almost all parties in health care, one way or another, have a stake in the development and rapid diffusion of innovative health technologies, suggesting that reliance on self-regulation may be risky.
6. There is an informational asymmetry in the rela-tionship between a patient and his or her health-care providers. In seeking the health services, patients rely on their agents—the providers—who are supposed to combine the information on health status and treatment options with patients’ preferences to arrive at decisions that otherwise may have been made by an informed patient. The issue, in this environment of rampant technologic advances, is that the provider (in this case the phy-sician) may not be a perfect agent. The provider may not have enough information about the new technology that he may choose to offer or not to his patients. This problem is more evident in deal-ing with high-cost technology, for which patients’ preferences, providers’ incentives, and informa-tion about the technology are all under question.
technOlOgy assessment
Technology assessment (TA) was first introduced in 1965 during deliberations of the Committee on Sci-ence and Astronautics of the US House of Represen-tatives. Congressman Emilio Daddario stated that the purpose of TA was to serve policymaking:
Technical information needed by policymakers is fre-quently not available, or not in the right form. A poli-cymaker cannot judge the merits or consequences of a technological program within a strictly technical context. He has to consider social, economic, and le-gal implications of any course of action.11
Shortly afterward, the US Congress commissioned independent studies by the National Academy of Sci-ences and Engineering and the Legislative Reference
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

esfandiari/Feine
The International Journal of Oral & Maxillofacial Implants 95
Services of the Library concerning the development and the application of TA. This led the National Sci-ence Foundation to establish the first TA program in 1972. Congress authorized the establishment of the Office of Technology Assessment in 1973, which be-came operational in 1974. The goal of this establish-ment was not to impede the development and use of technology. The intent was to help Congress become more effective in protecting the interests of the pub-lic and the private sector while enabling technology to contribute to society’s welfare. Private industry, with different aims, then used the existing platform of TA to compete in the marketplace.
The intensity of use of existing technology, the in-troduction of new technologies, and the expanded application of these new technologies are the three main mechanisms by which technologic change may contribute to the rise of health-care expenditures.12
In a thorough review of health-care expenditures,13 Rettig stated how these action mechanisms may af-fect the costs of health care through: (1) development of new treatments for previously untreatable termi-nal conditions, including long-term maintenance therapy for treatment of such diseases as diabetes, end-stage renal disease, and acquired immunodefi-ciency syndrome; (2) major advances in clinical apti-tude to treat previously untreatable acute conditions, such as coronary artery blockage via bypass grafting; (3) improvement of new procedures for discovering and treating secondary diseases within a disease, such as erythropoietin to treat anemia in dialysis pa-tients; (4) expansion of the indications for a treatment over time, increasing the patient population to which the treatment is applied; (5) continuing, incremental improvements in existing capabilities, which may improve quality; (6) clinical progress through major advances that extend the scope of medicine to condi-tions once regarded as beyond its boundaries, such as mental illness and substance abuse13; (7) a rapid development of safety and effectiveness regulations with emphasis on quality of the delivered care; and (8) an increase in labor intensity of the health-care sector, causing increases in salaries.14
health technOlOgy assessment
From World War II to the early 1970s, health-care fi-nancing in most countries was generously based on retrospective pricing, which created an environment of technology development regardless of its effects on costs.15 In recent years, the emergence of costly health technologies has led to a cost-containment policy on the health-care sector of most countries. With limited financial resources and ever-growing
health expenditures, governments around the world are actively seeking ways to improve the delivery of appropriate health care to their citizens. From retro-spective pricing to prospective budgeting, the im-position of specific regulations such as licensing for advanced medical equipment and restricting reim-bursement for costly health technology programs are a few of these measures taken to slow down growth in health expenditures.16 Although US health technology assessment (HTA) programs predate many well-known international HTA agencies (eg, Canadian Agency for Drugs and Technologies in Health, National Institute for Health and Clinical Excellence), because of politi-cal, financial, and commercial pressures, the funding for these initiatives was withdrawn in 1995.17 However, since the late 1980s in Canada and in other countries, HTA has become a rapidly growing field. There are now nine internationally known HTA groups at the national and provincial levels.18 In recent decades, their impact on decision and policymaking has increased tremen-dously.19–21 Because of their integral roles in health care, HTA groups have developed and implemented various knowledge transfer strategies to measure the effectiveness of various health technologies.22–24
The limited resources available within health care systems pose serious questions about the diffusion of health technologies. How should government responsibility be managed and demarcated? How should health-care budgets be regulated, and how should for-profit enterprises and environmental is-sues in health care, as well as the socioeconomic im-plications, be managed? These are some examples of the government challenges in diffusion of health technologies. Although evidence of efficacy for a given technology is necessary, it is not sufficient to support clinical decisions, let alone policy-related decisions.25 Therefore, governments with an ordered set of analyzed policy options have to allocate their limited resources for those health technologies that are shown to be effective; to be socially, politically, le-gally, and environmentally accepted; and to be easily used and provided by clinicians.
The results of assessments by HTA agencies play an important role in societal decision making in accepting or rejecting a new technology. This, however, should not be confused with decision making at the patient level. HTA bodies have a difficult task when dealing with costly medical technology. Most of these technologies are in an early phase of diffusion, and the emphasized difficulty in assessing the efficacy of the technology is that several alternatives to the technology may be available, which should be assessed at the same time. On the other hand, the dependency of costs and ben-efits relative to patient characteristics, the need and demand relationship, the distribution of health-care
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
96 Volume 26, Supplement, 2011
payments among population groups, and the access to a high-cost technology for different groups of patients, with all the pertinent ethical implications, are all daunt-ing tasks for these HTA bodies.26,27
The INAHTA,7 which currently represents more than 40 agencies from 20 countries, defines HTA as “the systematic evaluation of properties, effects, and/or impacts of health care technology that may address the direct, intended consequences of technologies as well as their indirect, unintended consequences. Its main purpose is to inform technology-related policy-making in health care.” In evaluating new innovative medical technologies, HTA agencies commonly em-ploy interdisciplinary groups that are responsible for proper assessment of health technologies. It is also considered that “HTA is a multidisciplinary field of policy analysis. It studies the medical, social, ethical, and economic implications of development, diffu-sion, and use of health technology.”6
In addition to their conventional role as evaluators of health technologies, HTA organizations are now promoting the production of scientific evidence,28 prompted by the frequent lack of sufficient rigorous evidence at the time of assessment. This action will help HTA organizations to identify research needs in a concrete health-care context.25 To bolster their influ-ence in the health-care system, HTA organizations are increasingly involved in the design and implemen-tation of education and training programs, which in turn help to foster critical thinking among the future main decision makers. This will teach students how to search, evaluate, interpret, and use the best scien-tific evidence to reduce the uncertainties related to clinical decision making. The training programs also encourage open discussions of the ethical, economic, and organizational conflicts in health care.29
It should also be noted that HTA is not a one-time exercise. These assessments must be continuous to ensure the use of the most appropriate and effica-cious technology. It is naive to think that previously evaluated technology will remain the best available. This line of thinking disregards the changing patterns of disease and innovations.30
By now it should be clear to the reader that, regard-less of the funding mechanism of a given health-care system, HTA can contribute to a variety of decisions. However, the context within which these decisions are made is crucially important, concerning not only the practical environmental considerations, but also the method of dissemination, both of which will have an important impact on users’ decision making. These decisions are often taken at three distinct levels: macro, meso, and micro. Macro decisions are made by stakeholders and can affect the health system as a whole (eg, government). Meso decisions are made
at a level below the macros. These decisions are made by institutions and organizations that are involved with the realities of technology implementation with-in their environment (eg, health maintenance organi-zations, hospitals). They may vary from one institution to another. Finally, micro decisions are routinely made at the level of the health professionals and their pa-tients. These decisions do not alter policy, but their impact is felt by the population at large.
HTA was initially intended to affect decision mak-ing at the macro level. However, over the years, its influence has spread to meso and micro decision makers. Figure 1 illustrates simply the path that a health technology takes from its development to its implementation and management in a health-care system. The numerous elements that HTA organiza-tions have to consider, the complex weighted effects of these elements on the evaluation process, and the chaotic environment accompanying the diffusion and the implementation of technology in a public health-care system affect decision makers at all three levels.
WhO uses hta repOrts?
HTA reports are generally used to advise or inform health technology–related policy making.8 These re-ports contribute toward improvements in the quality of health care and further development and updat-ing of a wide spectrum of guidelines, standards, and other health-care policies.
Patients and clinicians may use HTA to guide them in the appropriate use of health-care interventions. Regulatory agencies utilize HTA to establish the com-mercial use of a device, drug, or other health technol-ogies. Government health-department officials draw on HTA to design public-health programs (eg, screen-ing, vaccination). Health-care providers, employers, and payers use HTA findings in making decisions about health benefit plans and disease manage-ment programs. Politicians and lawmakers use HTA to develop policies on technologic innovation and its research and regulation and to determine how to al-locate the public funds to deliver and pay for it. Phar-maceutical and other health-care product companies use HTA to develop marketing strategies. On the oth-er hand, many hospitals and health networks use HTA to assist them in making decisions regarding health technology acquisition and management. Finally, pri-vate investors and venture capital funding companies employ HTA recommendations to develop strategies in their acquisitions and divestitures of health-care products and service companies.
One should bear in mind that the impetus for an HTA report is not necessarily a health technology.6
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

esfandiari/Feine
The International Journal of Oral & Maxillofacial Implants 97
There are three basic orientations to HTA.
1. Technology-oriented assessments. Their intent is to determine the characteristics and impacts of specific health technologies. For example, a gov-ernment health department may want to deter-mine the clinical, social, professional, industrial, or economic impacts of cochlear implants.
2. Problem-oriented assessments. These assess-ments focus on solutions and strategies to man-age a particular problem in using a technology for which alternative or complementary technologies can be used. For example, clinicians may call for the development of clinical practice guidelines to solve the problem of diagnosis of dementia.
3. Project-oriented assessments. Here, the focus is on the local use of a technology in a particular program or institution. For example, a hospital must decide whether to purchase an expensive imaging device while considering its available space, personnel, and other resources needed to install and operate the device.
In oral health, as in other health fields, there must be a need to produce HTA. If decision makers are not aware of the need to assess a technology, it is not enough to merely publish an HTA in hopes that one day the decision makers will be interested in using it. Because technology develops so rapidly, by the time the decision makers express interest, the technology may already have become obsolete. In an extensive analysis of the impact of HTA in Canada,24 Jacob and McGregor suggested that the best insurance for HTA impact is a request by decision makers for an evalua-tion. If, in the absence of such a request, evidence is mounting on the effectiveness of a new technology, it is necessary to raise awareness and stimulate the interest of decision makers about the assessed tech-nology. Issuing reports and raising public interest via the media are some of the strategies used to inform decision makers. Pharmaceutical and medical device companies often use these strategies to increase awareness of their products.
It should also be noted that the longer the interval between the HTA and the assessment of its effect on the diffusion and implementation of the technology, the harder it will be to evaluate the true effect of the HTA on using the technology. As a result of this, HTA will bear no traceable accountability for its influence on the provision of the technology. Therefore, it is not only important to produce HTA to improve the quality of health care; it is just as important to continuously as-sess the effect of HTA recommendations on decision makers.24 Therefore, innovative dissemination tools are needed to effectively transfer these recommendations.
Oral health expenditures
In most developed countries, oral health is a signifi-cant economic activity. In the United States, expen-ditures for oral health care services, including the prevention and treatment of dental caries, reached an astounding $92 billion in 2008.31 This figure does not account for dental care expenditures for services provided by dentists (and by nondentists in hospital settings) for the management of severe early child-hood caries, cleft lip or cleft palate, or facial injuries. In Canada, 2007 expenditures on dental services were forecast to make up 6.2% (CDN$9.8 billion) of total health-care expenditures.32 In most developed countries, oral health is a private market, and public funds account for only 10% to 15% of total expendi-tures in oral health. This means that, for the majority of the population, oral health care services are out-of-pocket expenses. This is a major contributing factor to oral health disparities across population groups of all ages.
Economicevaluation
Clinicalef�cacy Effectiveness
Societalpreference
Macro(i.e. government)
Meso(i.e. hospital
administrators)
Decision-making
Implementation
Micro(i.e. patients& providers)
Ethics,equity, &
legal issuesHealth technology
assessment
Fig 1 Simplified diagram of the attributes of health-care tech-nology and the levels of decision making regarding its use.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
98 Volume 26, Supplement, 2011
Oral hta
Considering the economic, social, industrial, ethical, and legal importance of the provision of oral health, it is surprising that there is still no established frame-work to use HTA to assess oral health technologies like other innovative health technologies. Oral health care in the United States and Canada, as in most other industrialized countries, is mainly private. Only those who receive social assistance and children in some re-gions are covered under public dental health plans. The majority of the population must pay for their dental treatments out of their pockets. In this pri-vate market, other than sporadic inspections by local regulatory associations, there is no accountability for the new dental technologies that avail themselves to dentists on a daily basis. One would think that the decision-making process would be much simpler in a private health-care system than in a publicly funded one. This may be the case when most decisions are made at the micro level. Dentists often are the ones who choose, adopt, and implement the technology in their clinics. The HTA in a privately funded health-care system will still have to include the same factors that involve the diffusion of the technology, with the ex-ception that the decision-making environment is less chaotic. This is a result of the fact that decisions on adopting dental technologies are made at the micro level by the dental providers.
There is now a call for the recognition of the impor-tance of technology assessment in oral health among industrialized countries.33,34 To date, there is no offi-cial document that considers the use of HTA for as-sessing oral health technologies in Canada. For much the same reasons that medical technologies are rig-orously assessed, oral health technologies also need to be evaluated. It seems that whoever pays for the technology determines how it is assessed.
Most so-called technology assessment studies in dentistry are either concentrated on the clinical ad-vantages of a technology or the economic evaluation of it under the umbrella of cost-effectiveness stud-ies.19–22 There is no debate that accounting for the cost of a dental technology is crucially important in sustaining its provision.35 However, social, industrial, ethical, and legal assessments of technology are also important, especially once the use of that technology is proposed as a standard of care (eg, the mandibular two-implant overdenture).
The determination of a technology’s stage of adop-tion and diffusion may be the primary purpose of an assessment, which indicates that there is no single correct time to conduct an HTA in both medical and dental health care.6
the rOle OF clinical experience in Oral hta
Questions regarding the safety, cost implications, impact on existing treatment options, and especially suitable training of new technologies are often ig-nored in dentistry because of the ease of introduction and the perceived benefits by dentists as well as pa-tients. The diffusion of implant technology illustrates the real difficulties of evaluating an oral health tech-nology in an adequately comprehensive manner be-fore its insidious diffusion (or lack thereof ) takes place.
Once a technology such as implant therapy has passed through different steps of oral HTA (OHTA), it is useful to determine whether providers, in this case dentists, can deliver the technology to the public. Even when a technology like the dental implant is proven to be affordable and effective and it is shown that patients prefer it to other available alternative treatments, the decision makers still need to know who can provide that technology. If access to the technology becomes difficult, it will avail itself to few-er members of the public. In addition, if provision of the technology requires specific skills so that only spe-cialists may be able to provide it, then that fact should be reflected in the assessment of that technology by the evaluators.
It is accepted that one of the most important fac-tors in a patient’s decision-making process to accept a health technology is the clinical competence of the physician.36 On the other hand, it has been found that doctors who have more expertise in delivering the medical technology and have a sympathetic attitude toward their patients are more likely to convince their patients to accept the offered treatment. Such physi-cians are perceived by patients to have an enhanced involvement in patients’ disease management, which in turn will lead to a more appropriate use of the tech-nology.37 If the role of the clinician’s experience in the adoption of a given health technology is important for its overall assessment, then the effect of clinical experience in the successful provision of implant therapy must be taken into account in performing an OHTA on this technology.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

esfandiari/Feine
The International Journal of Oral & Maxillofacial Implants 99
hOW Ohta aFFects the clinical perFOrmance OF dentists
While some dental practitioners tend to underesti-mate the need for clinical training for new innovative technologies, some tend to be overwhelmed by the attributes of new technologies and therefore shy away from their use. Achieving an equilibrium between these two attitudes regarding the clinical expertise required to use dental technologies can tremendously enhance the clinical performances of dental clinicians and help to reduce the perceived difficulty of provid-ing the new technology to patients in need. Let us con-sider the specific example of mandibular two-implant overdenture technology. If an OHTA on this technol-ogy were available to clinicians, one could assume that it would have reduced some of the unnecessary anxi-ety that may have been associated with the provision of this technology by general practitioners. As a result, patients would have better access to this technol-ogy than if it were offered exclusively by highly skilled prosthodontic specialists. This by no means diminishes the importance of specialist training in the provision of safe and effective prosthetic implant therapy. How-ever, an OHTA would use the evidence to demonstrate the capacity of inexperienced general practitioners to provide successful implant overdentures.38 Ideally, the question, “How much training is enough to provide an implant overdenture in a safe and effective manner?” would have been answered in that OHTA. This informa-tion would be useful for patients, clinicians, and other stakeholders who are concerned with the decimation of this technology.
New dental technologies have brought colossal benefits to patients, but they have also brought a collective responsibility to dentists to use these tech-nologies appropriately. It is evident that dental clini-cians are the active users of oral health technologies.4 However, they should seek out evidence and famil-iarize themselves with technology assessment tools. Both the assessors and the users of the dental tech-nology—the dentists—should see the uptake of the OHTA as a shared commitment. Therefore, the onus is on clinicians to do their parts in building the evidence base for dental care, to conduct research, and, mini-mally, to simply ask “What is the evidence?” Failing to offer patients a newly assessed and acceptable dental technology is at the very least unethical and, in some instances, could be considered illegal.39
In summary, all those in the dental field have a role as active participants in OHTA and dissemination. How we approach this task will determine the future growth and sustainability of high-quality oral health care to serve patients.
reFerences
1. Peterson PE. The World Oral Health Report 2003. Continu-ous Improvement of Oral Health in the 21st Century–The Approach of the WHO Global Oral Health Program. http://www.who.int/oral_health/media/en/orh_report03_en.pdf. Accessed 10 January 2010.
2. Reinhardt UE, Hussey PS, Anderson GF. US health care spending in an international context. Health Aff (Millwood) 2004;23(3):10–25.
3. US Department of Health and Human Services. Centers for Medicare and Medicaid Services. R1881A3: Review of Form HCFA-1450 for Inpatient and Outpatient Bills. http://www.cms.gov/QuarterlyProviderUpdates/JUL2003/list.asp. Accessed 10 January 2010.
4. United Nations. World Population Prospects, The 2006 Revi-sion. New York: United Nations, 2007.
5. Oh EH, Imanaka Y, Evans E. Determinants of the diffusion of computed tomography and magnetic resonance imaging. Int J Technol Assess Health Care 2005;21:73–80.
6. Goodman C. HTA 101: Introduction to Health Technology Assessment. Falls Church, VA: The Lewin Group, 2004:12.
7. International Network of Agencies for Health Technology As-sessment. Global Networking for Effective Health Care. HTA resources 2007. http://www.inahta.org/HTA/Glossary/#_T. Accessed 21 November 2007.
8. Skinner JS, Staiger DO, Fisher ES. Is technological change in medicine always worth it? The case of acute myocardial infarction. Health Aff (Millwood) 2006;25:w34–w47.
9. Robinson JC, Luft HS. The impact of hospital market struc-ture on patient volume, average length of stay, and the cost of care. J Health Econ 1985;4:333–356.
10. d’Adler MA. The transfer of medical information. A journal-ist’s view. Int J Technol Assess Health Care 1988;4:59–63.
11. Deliberations of the Subcommittee on Science Research and Development of the Committee on Science and Astronau-tics, Technology Assessment, 90th Cong, 1st Sess (1967) (statement of Emilio Q. Daddario, Chairman).
12. Gelijns A, Rosenberg N. The dynamics of technological change in medicine. Health Aff (Millwood) 1994;13(3):28–46.
13. Rettig RA. Medical innovation duels cost containment. Health Aff (Millwood) 1994;13(3):7–27.
14. Cuyler RN. The challenge of partial hospitalization in the 1990s. Psychiatr Hosp 1991;22(2):47–50.
15. Weisbord BA. The health care quadrilemma: An essay on technological change, insurance, quality of care and cost containment. J Econ Lit 1991;24:523–552.
16. Hurst JW. Reforming health care in seven European nations. Health Affairs (Millwood) 1991;10(3):7–21.
17. Sullivan SD, Watkins J, Sweet B, Ramsey SD. Health technol-ogy assessment in health-care decisions in the United States. Value Health 2009;12(suppl 2):S39–S44.
18. Hivon M, Lehoux P, Denis JL, Tailliez S. Use of health tech-nology assessment in decision making: Coresponsibility of users and producers? Int J Technol Assess Health Care 2005;21:268–275.
19. Battista RN, Banta HD, Jonnson E, Hodge M, Gelband H. Les-sons from the eight countries. Health Policy 1994;30:397–421.
20. Battista RN, Lance JM, Lehoux P, Regnier G. Health technol-ogy assessment and the regulation of medical devices and procedures in Quebec. Synergy, collusion, or collision? Int J Technol Assess Health Care 1999;15:593–601.
21. Cookson R, Maynard A. Health technology assessment in Europe. Improving clarity and performance. Int J Technol Assess Health Care 2000;16:639–650.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Outcomes
100 Volume 26, Supplement, 2011
22. Bero LA JA. How consumers and policy-makers can use systematic reviews for decision-making. Ann Intern Med 1997;127:37–42.
23. Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD, Thom-son MA. Closing the gap between research and practice: An overview of systematic reviews of interventions to promote the implementation of research findings. Br Med J 1998;317:465–468.
24. Jacob R, McGregor M. Assessing the impact of health technology assessment. Int J Technol Assess Health Care 1997;13:68–80.
25. Granados A. Health technology assessment and clinical deci-sion making: Which is the best evidence? Int J Technol Assess Health Care 1999;15:585–592.
26. Jabbour N, Gagandeep S, Mateo R, et al. Live donor liver transplantation without blood products: Strategies devel-oped for Jehovah’s Witnesses offer broad application. Ann Surg 2004;240:350–357.
27. Bonsel GJ. Methods of Medical Technology Assessment with an Application to Liver Transplantation [thesis]. Rotterdam, The Netherlands: Erasmus University, 1991.
28. Granados A. Health technology assessment and clinical deci-sion making: Which is the best evidence? Int J Tech Assess Health Care 1999;15:590–591.
29. Granados A. Clinical decisions: Balancing evidence, uncer-tainty, resources and values. Informatiu AATM 1997;11:1–3.
30. Eisenberg JM. Ten lessons for evidence-based technology assessment. JAMA 1999;282:1865–1869.
31. Accounting for the Cost of US Healthcare: A New Look at Why Americans are Spending More. McKinsey Global Insti-tute website. http://ww1.mckinsey.com/mgi/publications/US_healthcare/pdf/US_healthcare_Chapter1.pdf. Accessed 10 January 2010.
32. Canadian Institute for Health Information. National Health Expenditure Trends, 1975–2007. Ottawa: Canadian Institute for Health Information, 2005.
33. Axelsson S, Dahlgren H, Svensson A, et al. Need to Assess Dental Care. Stockholm: The Swedish Council on Technology Assessment in Health Care, 2000.
34. Leake JL, Birch S, Lewis DW. Technology assessment in den-tistry. J Can Dent Assoc 1994;60:1066–1070.
35. Esfandiari S. Oral Health Technology Assessment: Study of Mandibular 2-implant Overdenture. Berlin: Lambert Academic, 2010:10.
36. Dawn AG FS, Lee PP, Enyedi LB. Parents’ expectations regard-ing their children’s eye care: Interview results. Am J Ophthal-mol 2003;136:797–804.
37. Markaki A, Antonakis N, Hicks CM, Lionis C. Translating and validating a training needs assessment tool into Greek. BMC Health Serv Res 2007;7:65.
38. Esfandiari S, Lund JP, Thomason JM, et al. Can general den-tists produce successful implant overdentures with minimal training? J Dent 2005:34:796–801.
39. Rashti B, Esfandiari S, Lemieux G, Feine J. When it comes to new technologies, are you fulfilling your professional man-date? J Can Dent Assoc 2008:74:627–628.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 101
Outcomes Group Members
Group Expert and ChairNeal Garrett, PhD
Group Expert and ChairJocelyne Feine, DDS, MS, HDR
Group SecretarySteven E. Eckert, DDS, MS
Group MembersEdward Amet, DDS, BS, MSD
Thomas Dodson, DMD, MPH
James Doundoulakis, DMD, MS
Shahrokh Esfandiari, BSc, MSc, DMD, PhD
Marco Esposito, DDS, PhD
Joe Gian-Grasso, DMD
Marjorie Jeffcoat, DMD
Asbjorn Jokstad, DDS, PhD
Clarence Lindquist, DDS
Jay Malmquist, DMD
Edwin McGlumphy, DDS, MS
Regina Mericske-Stern, DDS, PhD
Michael Norton, BDS, FDS, RCS (Ed)
Jonathon Orenstein, DMD
Alan Pollack, DDS
Mariano Sanz, MD, DDS
Lyndon F. Cooper, DDS, PhD (ACP)
Alice DeForest (Silent Participant, AAP)
Samuel Low, DDS (AAP)
Hans Schmotzer, PhD (Nobel Biocare)
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

102 Volume 26, Supplement, 2011
Today’s clinicians are faced with an influx of new technologies that claim to improve implant ther-
apy. Thus, they must be able to determine which are worthwhile and appropriate to use.
The assessment of oral health technology involves the compilation of all available information on that technology (see Fig 1, page 97). Decision makers at all levels can also use this type of information.
The strongest technology assessment evidence comes from combining or comparing multiple stud-ies that have been carried out in different situations and with different populations. In order to properly combine or compare data from different studies, a core set of outcome variables would need to be gath-ered in all studies.
In order to define these core outcomes, the out-comes group discussed and identified common issues that could potentially be affected by new technolo-gies, including: (1) the time necessary for treatment: from initial intervention to definitive prosthesis; (2) the cost of treatment; (3) the quality of osseointegra-tion; (4) expansion of patient base; (5) ease of use (ie, simplicity of the new technique); and (6) enhanced quality of the restoration.
The outcomes group also identified the kind of in-formation that should be gathered in studies of new technologies, including: (1) time; (2) technique sim-plicity; (3) durability; (4) longevity; (5) cost; (6) restora-tion; and (7) adverse events.
In addition, the group decided there is a need for a core set of outcomes for clinical studies in dental implant therapy. These would allow for the accumula-tion of data across studies and also “compensate” for underpopulated studies.
The outcomes group also agreed on the fact that specific areas of evaluation should be addressed, includ-ing: (1) patient satisfaction (psychological domain); (2) quality of life (psychological domain); (3) prosthesis stability (longevity domain); (4) implant stability (lon-gevity domain); (5) soft tissue stability (longevity or physiological domain); (6) bone stability (longevity or physiological domain); and (7) costs (economic domain).
Finally, the group suggested various ways for the Academy’s membership to reach a consensus on the variables and outcome measures that it would rec-ommend for future technology assessment research studies. Options could include the development of a small expert panel to recommend domains and mea-sures or the expert panel could develop a conference plan to build broad participation in setting the rec-ommended domains and measures.
The recommendation of standardized outcome variables and measures in the assessment of implant technologies would be a very important and vital contribution to the advancement of implant care. With this, the Academy would confirm its primary role as a major player in the assessment and transfer of im-plant technology in this century.
Outcomes Group Report
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 103
Audience Response Results
A wireless, anonymous polling technology was used in the final plenary session to allow all Summit par-ticipants to log their opinions about each of the biotechnologies as well as the conclusions from the
outcomes group. These results provide a summary of how the participants voted on each biotechnology and the outcomes issues following the Summit. The votes were taken on six questions that were the same for all of the biotechnologies. The voting on outcomes was for another set of questions. The results of the voting are shown below.
ART ResulTs CompARed by TeChnology
1. There is a significant dental implant patient population that could benefit from:
2. The following technology has the potential to significantly improve clinical outcomes with dental implants:
83%
75%
59%
60%
0% 20% 40% 60% 80% 100%
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
70%
70%
53%
53%
0% 20% 40% 60% 80%
38%
27%
28%
36%
0% 10% 20% 30% 40%
66%
56%
33%
47%
0% 20% 40% 60% 80%
48%
57%
58%
46%
0% 20% 40% 60% 80%
83%
75%
59%
60%
0% 20% 40% 60% 80% 100%
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
70%
70%
53%
53%
0% 20% 40% 60% 80%
38%
27%
28%
36%
0% 10% 20% 30% 40%
66%
56%
33%
47%
0% 20% 40% 60% 80%
48%
57%
58%
46%
0% 20% 40% 60% 80%
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Audience Response Results
104 Volume 26, Supplement, 2011
3. The following technology has the potential to significantly improve physical health outcomes for dental implant patients:
4. The following technology has the potential to significantly improve quality of life outcomes (eg, function) for dental implant patients:
5. The potential benefit of the following technology will justify its estimated cost:
83%
75%
59%
60%
0% 20% 40% 60% 80% 100%
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
70%
70%
53%
53%
0% 20% 40% 60% 80%
38%
27%
28%
36%
0% 10% 20% 30% 40%
66%
56%
33%
47%
0% 20% 40% 60% 80%
48%
57%
58%
46%
0% 20% 40% 60% 80%
83%
75%
59%
60%
0% 20% 40% 60% 80% 100%
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
70%
70%
53%
53%
0% 20% 40% 60% 80%
38%
27%
28%
36%
0% 10% 20% 30% 40%
66%
56%
33%
47%
0% 20% 40% 60% 80%
48%
57%
58%
46%
0% 20% 40% 60% 80%
83%
75%
59%
60%
0% 20% 40% 60% 80% 100%
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
Tissue engineering
Growth and differentiation
Nanotechnology
Adult stem cell
% Agree/strongly agree responses
70%
70%
53%
53%
0% 20% 40% 60% 80%
38%
27%
28%
36%
0% 10% 20% 30% 40%
66%
56%
33%
47%
0% 20% 40% 60% 80%
48%
57%
58%
46%
0% 20% 40% 60% 80%
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Audience Response Results
The International Journal of Oral & Maxillofacial Implants 105
6. Tissue engineering has the potential to have a significant impact on dental implant therapy in:
7. growth and differentiation technology has the potential to have a significant impact on dental implant therapy in:
40% 40%
16%
4% 0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
20.73%
46.34%
24.39%
8.54%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
30.77%
37.18%
25.64%
6.41%
0%
5%
10%
15%
20%
25%
30%
35%
40%
13.70%
28.77%
47.95%
9.59%
0%
10%
20%
30%
40%
50%
60%
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
40% 40%
16%
4% 0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
20.73%
46.34%
24.39%
8.54%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
30.77%
37.18%
25.64%
6.41%
0%
5%
10%
15%
20%
25%
30%
35%
40%
13.70%
28.77%
47.95%
9.59%
0%
10%
20%
30%
40%
50%
60%
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
40% 40%
16%
4% 0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
20.73%
46.34%
24.39%
8.54%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
30.77%
37.18%
25.64%
6.41%
0%
5%
10%
15%
20%
25%
30%
35%
40%
13.70%
28.77%
47.95%
9.59%
0%
10%
20%
30%
40%
50%
60%
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
40% 40%
16%
4% 0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
20.73%
46.34%
24.39%
8.54%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
30.77%
37.18%
25.64%
6.41%
0%
5%
10%
15%
20%
25%
30%
35%
40%
13.70%
28.77%
47.95%
9.59%
0%
10%
20%
30%
40%
50%
60%
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
Less than5 years
5–10years
11–20years
More than20 years
8. nanotechnology has the potential to have a significant impact on dental implant therapy in:
9. Adult stem cell technology has the potential to have a significant impact on dental implant therapy in:
ouTComes
1. When assessing a technology for implant therapy, it is important to include more than just standard clinical measures of implant survival/success (ie, implant in function, no mobility, no pain, no infection, and minimal bone loss).
4%
5.33%
6.67%
30.67%
53.33%
0% 10% 20% 30% 40% 50% 60%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
5.41%
6.76%
47.30%
40.54%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
6.85%
5.48%
5.48%
28.77%
53.42%
0% 10% 20% 30% 40% 50% 60%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Audience Response Results
106 Volume 26, Supplement, 2011
2. It is important to identify and measure outcomes of implant based therapy that include life quality, function (as rated by the patient), cost, and preference.
3. A consensus on the appropriate outcomes for implant therapy should be developed.
Added QuesTIons
The participants were also polled twice to rank indications related to dental implant therapy that should be the focus of future research to enhance clinical outcomes. The results of the polling indicated that vertical ridge aug-mentation and the prevention and treatment of peri-implantitis are priority areas. These two clinical challenges should be strongly considered by the AO in its strategic planning as topics for future workshops to identify those therapies and areas of research that would enhance the long-term success of dental implants.
4%
5.33%
6.67%
30.67%
53.33%
0% 10% 20% 30% 40% 50% 60%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
5.41%
6.76%
47.30%
40.54%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
6.85%
5.48%
5.48%
28.77%
53.42%
0% 10% 20% 30% 40% 50% 60%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
4%
5.33%
6.67%
30.67%
53.33%
0% 10% 20% 30% 40% 50% 60%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
5.41%
6.76%
47.30%
40.54%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
6.85%
5.48%
5.48%
28.77%
53.42%
0% 10% 20% 30% 40% 50% 60%
Strongly disagree
Disagree
Neutral
Agree
Strongly agree
1. The highest priority to address is: 2. of these, which has the highest priority to address with regard to techniques, materials, and outcomes assessment? (multiple choice)
Responses
percent Count
Socket augmentation 6.58% 5
Vertical ridge augmentation 38.16% 29
Lateral ridge augmentation 3.95% 3
Sinus augmentation 0% 0
Soft tissue esthetics 10.53% 8
Implant prosthetics 11.84% 9
CAD/CAM technology 2.63% 2
Management of peri-implant disease 26.32% 20
Totals 100% 76
Responses
percent Count
Vertical ridge augmentation 48.65% 36
Management of peri-implant disease 51.35% 38
Totals 100% 74
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 107
The AO’s Silver Anniversary Summit included pre-sentations by leading scientists and clinical scholars
on the subjects of bioengineering, growth and differ-entiation factors, nanotechnology, stem cell research, and outcomes assessment. The Summit’s participants convened in small working groups to answer questions regarding the impact of each of the areas on implant dentistry. Unique to the Summit was the inclusion of thought leaders, as “Call to Action” speakers, in oral and maxillofacial surgery, periodontics, and prosthodontics, who were charged with providing a futuristic overview of the clinical impact of the biological and technological advances presented at the Summit from their specialty’s perspective. I had the distinct honor of being the “Call to Action” speaker for oral and maxillofacial surgery. My re-flections on the Summit proceedings and personal call to action are as follows:
With regard to bioengineering, I was impressed with Dr Athanasiou’s presentation on the imminent possibility of regenerating articular cartilage for temporomandibu-lar joints but the inherent difficulty in engineering bone constructs in light of the requirement for specific dimen-sions, morphologies, vascularization, and mechanical re-quirements. Much research will be required to enhance the technology for the creation of predictable and viable osseous grafts that may need not only bioengineering but also the incorporation of findings from research on stem cells, signaling molecules, and nanotechnology.
The bioengineering section reaffirmed that the re-quirements of the host must be considered when de-signing the tissue construct. The size and volume of the defect must be determined. The need and amount of soft and hard tissue genesis should be determined to optimize the construct. Based on these determinations, the specific needs of the bioengineered construct can be identified. Regardless of the excellence of the construct, the nature of the receptor site must be considered to en-hance a successful outcome. For example, the vascular supply may be altered due to scar formation in the re-cipient bed. In addition, inflammatory changes due to the local impact of the oral biofilm will need to be con-trolled preoperatively, at the time of surgery, and during the postoperative phases to optimize the cascade of the healing process.
Dr Tuan gave an inspiring presentation on stem cell research. The participants and I strongly agree that the oucome of stem cell research will have significant poten-tial to enhance wound healing and the regeneration of soft and hard tissues. I was struck by the many types of stem cells available for research and the potential limita-tions on their investigation. I was also informed of the “hidden” dangers that may lurk in using stem cells with
regard to the transfer of genetic abnormalities and the possible reversion of transformed stem cells to their ini-tial biotypes.
In this regard, stem cells can be differentiated and directed. Different sources of stem cells act differently. The key is to control their direction and the microenvi-ronment for their development into specific tissues and to enhance their incorporation into the new host.
Autogenous stem cells originate from the individual patient. The cells are then differentiated and enhanced in number. However, current use of autogenous stem cells for bone or soft tissue development in the oral environ-ment lacks controlled studies with defined endpoints. The current application of autograft-derived stem cells is therefore empirical. However, depending on research outcomes, the future use of autogenous stem cells has significant potential to change how we treat hard and soft tissue defects for implant site development. Cellular harvesting methods, storage, directing the cells to form hard or soft tissue, and many other factors must be de-fined in well-controlled studies.
Allogeneic stem cells originate in one person to be used in another patient. The use of cryopreserved allo-geneic stem cells is being marketed as one source of cells that promote bone formation. Because these cells survive and join the host as long-lasting cells, the transplanted and viable genome of the host must be benign. If oncogenes are present in the donated alloge-neic stem cells, there is the potential, although small, for later tumor development. Donors must be meticulously screened. Another question pertains to these allogeneic cells. There needs to be convincing evidence that they are stem cells and not cells that have some qualities of stem cells. The current reports in the literature are lim-ited. Significant basic research and clinical trials are nec-essary for the verification of these cells as stem cells.
The topic of nanotechnology for bioengineering was brilliantly addressed by Dr Tomsia. Unfortunately, the use of nanotechnology for restorative materials was not a topic for the Summit, and the presenters and I feel this is a subject for a future AO-sponsored congress. I was im-pressed with the need for surface patterning in the suc-cessful response of cells and complex molecules to the nanoparticles. Of practical significance is the application of nanotechnology to the surface modifications of den-tal implants with the beneficial outcome of enhanced bone-to-implant contact.
The nanosurface modifications include either nano-level additives or nano-level reduction of the surface. The nanosurface increases fibrin attachment, increases platelet deposition, and increases contact osteogenesis. Which is better: addition to the oxide surface of a titanium
Oral and Maxillofacial SurgeryMichael S. Block, DMD
Call to aCtion
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Call to action
108 Volume 26, Supplement, 2011
implant or surface etching? It will be necessary for future research to demonstrate clinically significant enhance-ments by nanotechnology to implant surfaces beyond what is currently available and proven to be highly suc-cessful.
It should also be noted from Dr Tomsia’s presentation that nanomaterials can be fabricated in a multitude of shapes using printing methods to form lattice struc-tures. The individual lattice fibers can also be specifically engineered to suit the clinical application of the mate-rial. The potential for specifically designed nanomateri-als to aid in delivery of soluble factors and cells is very significant for future prevention and management of peri-implant diseases.
I was enlightened by the outstanding presentation of Dr Krebsbach on the current and future application of growth and differentiation factors or signaling molecules on hard and soft tissue regeneration. This section primari-ly focused on bone morphogenetic proteins after a com-prehensive overview of currently investigated growth and differentiation factors. These included platelet-derived growth factor, vascular endothelial growth factor, trans-forming growth factor Beta, and growth hormone. One differentiation factor, recombinant bone morphogenetic factor-2 (rhBMP-2) is commercially available and FDA cleared for marketing and use in sinus augmentation and reconstruction of dental extraction sockets. The use of bone morphogenetic proteins is expanding into therapies that are currently off-label and will need controlled clinical trials. For example, can rhBMP-2 be combined with differ-ent carriers and used with various scaffolds? The partici-pants in this working group agreed that further clinical data would be beneficial on the expanded use of this soluble signaling molecule. Other currently available sig-naling molecules, such as platelet-derived growth factor, act by cellular recruitment and initiating the natural pro-cess of wound healing. An intact vascular supply at the surgical site seems to be important to allow for cell re-cruitment and de novo angiogenesis that is critical for bone formation.
A major challenge is to engage and optimize the natural healing response when using signaling mol-ecules. For example, when an individual molecule like rhBMP-2 is used, it is applied at high concentrations. I feel that methods need to be developed that promote physiologic optimal complex multiple signal-dosing re-sponses. The future may utilize bioreactors or living cell constructs with guided cell-seeding to allow for syner-gistic responses. These may be delivered through a new-ly designed nanostructure.
In summary, my view is that the goal should be to pro-vide a material/device/biologic that results in a physio-logic response—with the symphonic coordination of multiple factors to optimize the tissue response— especially in severely compromised sites.
When we consider the application of new technolo-gies to clinical practice, their use requires development within the current regulatory and ethical environment. Development with translation into clinical practice, the establishment of efficacy, and the education of clinicians and the public to using a new biologic may take 10 years or longer. There will always be overlapping of current, new, and developing materials.
Streamlining the process of development may be the key to avoid excessive time delays. This may require not only university- and industry-based research but con-sortiums of clinical investigators through collaborative endeavors and practice-based research networks. The new technologies must be critically evaluated for effica-cy, safety, cost effectiveness, and enhanced patient out-comes in comparison to current therapies. Consortiums of multiple dedicated centers of excellence can be used to generate meaningful evidence-based data from which to recommend the use of a new product or therapy.
The participants and I feel that we need to establish standard measurable endpoints for our studies; demand these studies from our commercial partners; and avoid using products or providing therapies without their veri-fication of predictable success and outcomes that may not be significantly better clinically for our patients. For example, how significant is it to raise success to 98% from 95% for a typical implant procedure? What works? What does not work? Is it site-related failure or patient-related failure?
As I indicated above, the consortium concept would be one possible approach to address these questions on the new technologies. The consortium concept begins with a central clearing location or institution. Statisti-cians are included to develop the study and establish sample size through power analyses. There is a common protocol for many sites to pool their data. All sites are required to follow the protocol and site funding may vary according to the demands of the study. For ex-ample, the Cancer Research Institute has been funded and has shown that the consortium concept allows for many clinically relevant and important questions to be answered.
In conclusion, trust among clinicians and patients was a common message conveyed by the participants of the Summit. I feel strongly that “the community of practice is a laboratory for technology assessment.” We will need to be more judicious in our acceptance of new products and therapies based on the new technologies in order that our patients are well served, and then mutual trust will be a guaranteed outcome.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 109
This has been a special opportunity to expand our hori-zons and for innovative exploration of the future. The
responsibility of a call to action presenter is to weigh all new information and offer suggestions as to when and how it will be implemented.
Our initial step, as a discipline, must be to establish the criteria of success for dental implants with specific endpoint measures. It is necessary to form an ad hoc committee and charge it with reporting its result at the next Academy of Osseointegration meeting in Washington, DC, in 2011. This committee may decide to abide by the prevailing criteria from Albrektsson and Zarb in 1986 or may see fit to modify it. It is impossible to create prospective research protocols without identifying a universal definition of success. I do not anticipate that this will pose a financial hardship and expect it to be an easily accomplished goal.
The next topic concerns the need for premarket inves-tigation of new products. In the early days of osseointegra-tion, extraordinary time was consumed before changing products. The contemporary system has reversed the pro-cess to a point where new products are routinely dispensed to the profession with inadequate investigation. Clinicians are frequently asked to try new devices and to report on their success without informing the patient that we are con-ducting research. It is a hazardous, nonscientific approach that cannot bode well for the implantologist. I suggest that the Summit co-chairs, Peter Moy and Vince Iacono, create this committee immediately.
A third topic is the value of creating a registry for den-tal implants. It will be necessary to form still another com-mittee to design appropriate methodology if the AO is in favor of the project. It will require a computer program, for the reasons Tom Taylor has just indicated, that is both efficient and user friendly. A large practice may be able to have a dedicated individual to post this information on a daily basis. A new or young practitioner with minimal staff probably will find this to be a significant burden at the end of each practice day.
There is much background information that will influ-ence the quality of the data provided in such a registry. As an example, what is the surgical background of the practitioner? We cannot anticipate that first-, second-, or third-year residents will perform at the same level as an experienced practitioner. We also need to have informa-tion on the background of the patient as to their physical health status. What type of bone volume and quality are available for the implant? What level of experience would be valuable for a difficult situation?
It is important to note that dentistry is a cottage industry with no federal funding for this process and there appears to be minimal third-party involvement. Therefore, we may meet significant resistance from practitioners for a registry.
This has been an extraordinary opportunity to look into the crystal ball. Having had the opportunity to participate in the early clinical research of the two growth factors that are
available today, I thought of the words of William James, a philosopher at the end of the 19th century. He noted that true rewards are not only a result of reasoned analysis, but include intuition, impulse, and the ability to cut to the chase. It is amazing that 110 years later these same skills have been significant in expanding the successful use of dental im-plants. In the introductory period, they were placed in one stage and we returned in a different time frame to do a sec-ond surgery. We loaded them deliberately. Our profession has made the transitions from edentulous patients to par-tially dentate to the single implant. There is no other area of dentistry to replace a missing tooth that has the background of investigation and information available for the patient to have an evidence-based option. Although there were meet-ings with the American Dental Association this past week about evidence-based dentistry, it will take a Herculean ef-fort with significant financial support before we can depend on this methodology to make clinical decisions.
Where is the future for the regenerative technologies that were presented in a masterful fashion on the first day? The Academy is not in the position financially to contribute to further research in these fields and it is obvious that the individuals who shared their expertise have far greater expe-rience. It would seem appropriate that we share the results of our fine summit with organizations that fund investiga-tions, such as the National Institutes of Health. This will re-quire the dedication of individuals who are willing to donate their time to organize and prepare white papers discussing current evidence and considering time tables of availability.
We cannot invest in randomized control trials to study outcomes without returning to the initial issue of identify-ing criteria of success. It serves no purpose to have a vari-ety of trials with a different endpoint analysis. When one considers our patients’ opinion of the outcome, there are few mysteries. Most patients do not congratulate us on the volume of bone we have developed or on the success of the implant. They do appreciate a procedure that is com-fortable and not nearly as complicated as they anticipated. Most patients measure the outcome in the posterior region of the mouth based on their capability to masticate. Obvi-ously, the satisfaction in the anterior region of the mouth will depend upon the esthetic result. The patient’s opinion of the outcome may or may not require an expensive, time-consuming endeavor. Of course, this would then save con-siderable financial investment and man hours.
Although I understand the benefits of HTA, I think this has to be something for future consideration, as we have already been told that finances are limited. It is important that those issues suggested that have accomplishable goals move forward. The work should be addressed by ad hoc committees with short tenures.
This summit meeting has provided an opportunity for all of us to reexamine our cherished beliefs. Our horizons have been expanded and we have been provided with an opportunity to move forward in a valuable direction.
PeriodonticsMyron Nevins, DDS
Call to aCtion
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

110 Volume 26, Supplement, 2011
This reminds me of when, as a freshman in dental school in 1970, a world-class expert on cariology basi-
cally told us we had made a mistake choosing dentistry as a profession because within 18 months there would be a vaccine for caries on the market. I suggest you place the same value on what you are going to hear today as I should have based on what I heard back then.
I thought I would put my thoughts together by giv-ing some definition as to what we consider short term, mid term, and long term, because I think these are very important considerations. Had we had short-term, mid-term, and long-range options in the voting process, I think we would have had different outcomes to many of the questions for most of the domains in this workshop.
Having said that, I would also say that it was really amazing to go to each breakout group and listen to what they were talking about. The bottom line for every group was that this biotechnology is for the 5% of cases that, for some reason or other, do not work—lack of anatomy, lack of bone quality, medical compromise, or some other problem. Well, I think we need to get our heads out of the sand. It is not a 5% lack of success that we confront on a daily basis. It is much higher than that from the stand-point of failure to integrate, loss of integration, and all of the other complications in between. It is much higher than that worldwide. Perhaps in your practice it is 5%, but in general it is much, much higher, and that is why I think these discussions have much more importance than just for that 5%.
Bioengineering, as was pointed out very eloquently by David Cochran, is a conglomeration of all of the technolo-gies. For this reason we had some overlap in all of these sections, and that is why they came out with very similar results in their reports. In the short term, however, what we are currently seeing is probably what we are going to see, by and large, over the next 5 to 10 years, without a dramatic upswing in application.
In the mid term, the applications to which we should broaden our reach are totally unclear, but I think the tech-nology is there and will become very promising. In the long term, bioengineering or tissue engineering is likely to be the solution for many of the problems that we con-sider insurmountable today. For example, the model of bioengineering a tooth, with all of its tissue components, has already been done in Japan. It has been reported, so obviously the next issue will be how to control and har-ness it. But the technology is with us today.
A problem to consider in regenerating a missing tooth is why the patient lost the tooth in the first place. Most teeth are lost due to caries or restorative failure that was initiated by caries. Why replace that caries-prone append-age with the same thing when we already have something
better? This is what this Academy is all about. Now that is the opinion of a prosthodontist, so take it for what it’s worth. Similarly, generation of periodontium around the dental implant seems to me a nightmare because the periodontium is what probably caused many of our pa-tients to be needing our services to begin with, so why repeat some of nature’s errors?
Considering nanotechnology, I think in the short term there is a high likelihood of direct application, particular-ly, primarily, and probably exclusively in implant surface and abutment surface technology. We are already seeing some preliminary results in this area. In the mid term to long term, continuing development will likely be increas-ingly competing with and complementing biological al-ternatives to alloplastic devices, so I can see competition in which way is a better solution to take forward. But, in the end, they are going to blend and complement each other very nicely in ways that we cannot even dream of today.
I think the two most profound statements in this sum-mit came from one person. “The major issue is the fund-ing, and it is very expensive.” Thank you very much, Tony Tomsia, for really laying it on the line. That is our bottom line problem today in dental and medical research and will continue to be so as we try to scramble to provide treatment for our patients. I will also say, however, that there is really a very good example of a hydrophilic im-plant surface currently being used in dentistry. The ref-erences for that are primarily under Marcus Textor and colleagues, and I think that is something we all need to be aware of. So, as Tony would argue, just because we can do it doesn’t always mean that we should do it, and I think this is the bottom line for all of the sessions we have expe-rienced over the course of the Summit.
I noted that the stem cell group very wisely made the decision to limit their discussion to adult stem cells, and primarily autogenous stem cells, which is the bone graft that you all did Tuesday morning. That is, in a sense, stem cell engineering. I think anything beyond that autog-enous use of the patient’s own cells, not in an in vitro en-hanced manner but simply in a transplanting or perhaps somewhat purifying and then replanting situation, is the extent we are going to see in dentistry for many, many years. It will be at least 30 years before anything much beyond that comes out. I would argue that the potential is good in the very long term for clinical applications in humans. The analogy that can be drawn from the stem cell scientists at my university is that it took 30 years for monoclonal antibodies to go from first good laboratory results to first clinical trial in humans on a very limited ba-sis and that was for life-threatening disease. So how do you think we are going to say we want to be the first on
ProsthodonticsThomas D. Taylor, DDS, MSD
Call to aCtion
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Call to action
The International Journal of Oral & Maxillofacial Implants 111
the block to do this new technology to replace a missing tooth? I do not think we are going to go there, but again, I might be very wrong on this topic.
One fascinating issue addressed by Rocky Tuan that I was totally unaware of was the phenomenon of mi-croparticles and deosseointegration or disintegration he has explored in orthopedic implants. When he was discussing this, I concurred with the person next to me, “that’s orthopedics” (not dentistry), where you have fric-tion between two moving bodies; we do not have that with dental implants, so this is outside of the scope of what we do. Then I thought for a second back to some work we are doing at the University of Connecticut and let’s think for a minute about the zirconia abutment that we are placing into the titanium dental implant, putting it under non-axial load, cycling it in a moist environment a few million times, and expecting nothing to happen. If you put that abutment onto the implant one time and remove it, there is something deposited on that zirconia and, as you increase that over time, you will get an in-creased residue of particulate titanium, some adherent to the zirconia, but some particles are loose and floating around. And this, again, comes from unpublished data that I believe was just accepted for publication, showing zirconia coupled with titanium in a cyclical load area up to a million cycles. Coupling titanium and zirconia has a high risk for debris coming off at this interface and has the potential to cause not only wear problems and loosening of components, but also soft or hard tissue problems, because these particles are in the micrometer range and fully capable of being phagocytized by cells in the adjacent tissue. So perhaps we now have another area to look at for potential peri-implant disease.
Growth and differentiation, which was a very difficult topic and session for me compared to the others, I think is very likely to have a substantial impact in prosthodontics. It is already occurring in surgical aspects of prosthodon-tics. Mid term, I think we have great potential for specific surgical applications in the use of these materials. In the long term it is very likely to be a primary focus of treat-ment regimens in combination with other components, such as scaffolds and cells. But I would also argue that the use of systemic therapies to elicit local responses, such as in elective dental surgeries, is accompanied by the risk of undesirable side effects that we must not lose track of.
In regard to the outcomes topic, you all voted in the heavy affirmative that the standardization of parameters of study design was important to pursue. I think it is promising in the short term as new investigations are getting started, but there is going to be a lag time and a catch-up time before we get some true benefits from this changing methodological approach. In the mid term, I think it is very promising as a means to obtain meaningful and comparable results, and clearly in the long term it is necessary and inevitable as a means to control
technology and its ever-greater expansion. And I thank Lyndon Cooper, who broke it down into simple terms that a prosthodontist could understand. He said the out-comes we need to focus on are: is the patient happy, is the implant stable, is the prostheses stable, is the soft tissue stable, is the bone stable, and is the cost within reason?
The idea of an implant registry was addressed in the infancy of the Academy of Osseointegration—the mid to late1980s—and the AAOMS, the AAP, and the ACP de-cided it was necessary to be done in conjunction with the Veteran’s Administration. Each of those organizations funded one or two people to attend meetings on the topic in Washington, DC. We met for several days once, and then for several days a few months later. We came up with all of the reporting forms we needed, we bought what was considered a huge computer at that time to start accumulating these data, and we all went home and nobody did anything. Why? Because there was no mandate for us to do it, there was no personal advantage for us to do it, and there was some risk in doing it for both external and internal reasons. In addition, with dentists typically being sole practitioners and hard-working, the last thing they are going to do at the end of the day is sit down and fill out a bunch of forms for some distant registry. In my opinion, the only way a registry is going to work is if it is a governmentally mandated requirement. That would mean that if you do implant dentistry, you must report it to the registry. If it is not mandated with consequences for noncompliance, you are probably not going to do it.
Now I have a comment on the organization of the Sum-mit. I think we had a very severe oversight: the absence of information technology, computer-driven design and fabrication of prosthetic components. This is a techno-logic area that should have been addressed, particularly from the prosthodontic point of view. Also, restorative/prosthodontic material science technology could or should have been covered in the Summit because it is with us, we are already well into it, but we can’t keep up with it. Keep in mind that the most common complica-tion in implant dentistry is prosthodontic component failure. It is much higher than the 5% you see reported in the best of studies. Even in those best of studies that show a 5% failure rate of implants, there are 35% to 40% prosthetic complications. That is where we are having our problems with our implant patients. That is where Mrs Jones, who gets treated successfully by you, the surgeon, comes to me and expects that same amount of success. I cannot promise that. That is a deficiency in our treat-ment regime that needs to be aggressively addressed, and I would suggest that the AO, the ACP—somebody—organize something that would bring about discussion of the very broad range of prosthodontic problems associ-ated with dental implants.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Call to action
112 Volume 26, Supplement, 2011
In summary, I would say again that our success rate in implant dentistry is definitely not 95%. It is much lower and we need to recognize that fact. The possibilities as described here are truly limitless, but we must pick the correct pathways with which to address our very lim-ited resources and that is the challenge. Technology is already exponentially outpacing clinical dentistry. As a clinician, I cannot keep up, but the alternative to trying to do so is just not an option. We need to be organized
in our approach to it. The triad of academic and teaching centers, evidence-based practices, and industrial part-ners must be exploited—emphasis on exploited—to the full extent possible. I am intentionally ignoring govern-mental agencies here, because usually that ends up not getting us where we want to go or, if it does, it makes it a much slower process. So, the future is going to be very, very interesting.
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Oral & Maxillofacial Implants 113
AO Summit AttendeeS
Marcus F. Abboud, DMD University of Bonn Bonn, Germany
Tara L. Aghaloo, DDS, MD, PhD Department of Oral and Maxillofacial Surgery UCLA School of Dentistry Los Angeles, California
Wayne A. Aldredge, DMD Holmdel Periodontics Holmdel, New Jersey
Edward M. Amet, DDS, BS, MSD Reconstructive and Implant Dental Center Overland Park, Kansas
Daniel Ammon (Sponsor) Dentsply Tulsa Dental Specialties Tulsa, Oklahoma
Kyriacos Athanasiou, BS, MS, PhM, PhD University of California Davis Department of Biomedical Engineering Davis, California
Lori A. Bateman (Silent Sponsor) Quintessence Publishing Company Hanover Park, Illinois
Joel S. Berger, DDS, MD The San Diego Center for Oral and Maxillofacial Surgery San Diego, California
Neel B. Bhatavadekar, BDS, MS, MPH Pune, Maharashtra India
Michael S. Block, DMD (Call to Action Speaker) Metairie, Louisiana
Giuseppe Cardaropoli, DDS, PhD UMDNJ–New Jersey Dental School Newark, New Jersey
Nancy Deal Chandler (Silent Sponsor) American College of Prosthodontists Chicago, Illinois
Ramiz A. Chaudhry, DDS Selden, New York
Ira Cheifetz, DMD (AAOMS) Oral and Maxillofacial Surgery of Central New Jersey Mercerville, New Jersey
Donald S. Clem, DDS (AAP) Fullerton, California
David L. Cochran, DDS, PhD Department of Periodontics University of Texas Health Science Center San Antonio, Texas
Michael Collins (Sponsor) Zimmer Dental Carlsbad, California
Lyndon F. Cooper, DDS, PhD Department of Prosthodontics University of North Carolina School of Dentistry Chapel Hill, North Carolina
Daniel R. Cullum, DDS Implants Northwest Coeur D’Alene, Idaho
Jeremy Curtis (Silent Sponsor) Zimmer Dental Carlsbad, California
Christopher J. Damien, PhD (Sponsor) Dentsply International York, Pennsylvania
Alice DeForest (Silent Sponsor) American Academy of Periodontology Chicago, Illinois
Gino DeSimone (Silent Sponsor) Straumann US Andover, Massachusetts
Thomas B. Dodson, DMD, MPH Department of Oral and Maxillofacial Surgery Massachusetts General Hospital Boston, Massachusetts
Nikos Donos, DDS, MS, FHEA, FDSRCSEngl, PhD UCL Eastman Dental Institute London, United Kingdom
James H. Doundoulakis, DMD, MS Cosmetic Dental Rehabilitation PC New York, New York
Susan Drapeau, PhD (Sponsor) Medtronic Memphis, Tennessee
Steven E. Eckert, DDS, MS Rochester, Minnesota
Shahrokh Esfandiari, BSc, MSc, DMD, PhD Oral Health and Society Research Unit McGill University Montreal, Quebec
Marco Esposito, DDS, PhD Department of Oral and Maxillofacial Surgery The University of Manchester School of Dentistry Manchester, United Kingdom
Jocelyne Feine, DDS, MS, HDR Oral Health and Society Research Unit McGill University Montreal, Quebec
David A. Felton, DDS, MS Department of Prosthodontics University of North Carolina School of Dentistry Chapel Hill, North Carolina
Joseph P. Fiorellini, DMD, DMSc Department of Periodontics University of Pennsylvania Philadelphia, Pennsylvania
Earl G. Freymiller, DMD, MD UCLA School of Dentistry Los Angeles, California
Stuart J. Froum, DDS New York University College of Dentistry New York, New York
Paul A. Fugazzotto, DDS Milton, Massachusetts
Luis J Fujimoto, DMD New York, New York
Vicki Gaines (Silent Sponsor) Dentsply Tulsa Dental Specialties Tulsa, Oklahoma
German O. Gallucci, Dr Med Dent, DMD Department of Restorative Dentistry and Biomaterial Sciences Harvard School of Dental Medicine Boston, Massachusetts
Jeffrey Ganeles, DMD Florida Institute for Periodontics and Dental Implants Boca Raton, Florida
Neal Garrett, PhD UCLA School of Dentistry Los Angeles, California
Joseph E. Gian-Grasso, DMD Philadelphia, Pennsylvania
William V. Giannobile, DDS, DMSc University of Michigan School of Dentistry Ann Arbor, Michigan
Stig Hansson, MSc, MA, BM, PhD Astra Tech Ab Askim, Sweden
William Hartman (Observer) Quintessence Publishing Company Hanover Park, Illinois
Andrea L. Henderson, DDS (Young Clinicians Committee) UCLA School of Dentistry Los Angeles, California
Stephen Herrington (Sponsor) Biomet 3i Palm Beach Gardens, Florida
Kenneth F. Hinds, DDS Laguna Niguel, California
Vincent J. Iacono, DMD (Summit Co-Chair) Department of Periodontology and Implant Dentistry Stony Brook University School of Dental Medicine Stony Brook, New York
Arthur Jee, DMD (AAOMS) Bethesda, MD
Marjorie K. Jeffcoat, DMD University of Pennsylvania School of Dental Medicine Philadelphia, Pennsylvania
Robert L. Jeffcoat, PhD Vine Brook Research Corporation Bryn Mawr, Pennsylvania
Ole T. Jensen, DDS, MS Denver, Colorado
Asbjorn Jokstad, DDS, PhD University of Toronto Faculty of Dentistry Toronto, Ontario
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

AO Summit Attendees
114 Volume 26, Supplement, 2011
James N. Kenealy (Sponsor) Biomet 3i Palm Beach Gardens, Florida
Paul Krebsbach, DDS, PhD University of Michigan Biologic and Materials Sciences Ann Arbor, Michigan
William R. Laney, DMD, MS (Quintessence) Rio Verde, Arizona
Janice S. Lee, DDS, MD San Francisco, California
Clarence C. Lindquist, DDS Washington, District of Columbia
Samuel B. Low, DDS (AAP) University of Florida Gainesville, Florida
Martina Lulic, DDS The University of Hong Kong Faculty of Dentistry Pun Hong Kong
Anna Karin Lundgren, DDS, PhD (Sponsor) Astra Tech Mölndal, Sweden
Jay P. Malmquist, DMD Portland, Oregon
Robert Marx, DMD (Quintessence) Department of Oral and Maxillofacial Surgery University of Miami School of Medicine Miami, Florida
Sandro Matter, PhD Institut Straumann AG Basel, Switzerland
Edwin A. McGlumphy, DDS, MS Columbus, Ohio
Brian L. Mealey, DDS, MS San Antonio, Texas
Regina D. Mericske-Stern, DDS, PhD Department of Prosthodontics University of Bern School of Dental Medicine Bern, Switzerland
Peter K. Moy, DMD (Summit Co-Chair) UCLA School of Dentistry Los Angeles, California
Richard Nejat, DDS Advanced Periodontics and Implant Dentistry New York, New York
Joerg Neugebauer, DDS, PhD University Cologne Koln, Germany
Myron Nevins, DDS (Call to Action Speaker) Swampscott, Massachusetts
Russell D. Nishimura, DDS Westlake Village, California
Michael R. Norton, BDS, FDS, RCS (Ed) London, United Kingdom
Thomas W. Oates, DMD, PhD Department of Periodontics University of Texas Health Science Center San Antonio, Texas
Jonathan H. Orenstein, DMD Marlton, New Jersey
Gordon Peterson (Silent Sponsor) Medtronic Memphis, Tennessee
Joan Pi-Anfruns, DDS (Young Clinicians Committee) UCLA School of Dentistry Los Angeles, California
Michael A. Pikos, DDS Coastal Jaw Surgery Palm Harbor, Florida
Alan S. Pollack, DDS Park Avenue Periodontal Associates New York, New York
Marc Quirynen, DDS Catholic University Leuven Leuven, Belgium
Mark A. Reynolds, DDS, PhD Department of Periodontics University of Maryland Dental School Baltimore, Maryland
Georgios Romanos, DDS, Dr Med Dent, PhD Division of Periodontology University of Rochester Rochester, New York
Scott Root (Silent Sponsor) Astra Tech, Inc Waltham, Massachusetts
Steven J. Rosenstein, DMD Aventura, Florida
William Ryan (Sponsor) Nobel Biocare Yorba Linda, California
Mariano Sanz, MD, DDS University Complutense Madrid Faculty of Odontology Madrid, Spain
Ludovico Sbordone, MD, DDS Department of Surgery University of Pisa Pisa, Italy
Alex R. Schaer, PhD Camlog Biotechnologies AG Basel, Switzerland
Henning Schliephake, DDS, MD, PhD Goerg-August-Universitat Gottingen Gottingen, Germany
John P. Schmitz, DDS, MS, PhD Shavano Park, Texas
Hans Schmotzer, PhD (Sponsor) Nobel Biocare Holding AG Balsberg, Switzerland
Daniel B. Spagnoli, DDS, PhD University Oral Maxillofacial Surgery Denver, North Carolina
Clark M. Stanford, DDS, PhD University of Iowa Dows Institute for Dental Research Iowa City, Iowa
Richard M. Sullivan, DDS (Sponsor) Nobel Biocare USA Yorba Linda, California
James C. Taylor, DMD, MA Ottawa, Canada
Thomas D. Taylor, DDS, MSD Department of Reconstructive Sciences University of Connecticut Health Center Farmington, Connecticut
James Thomas (Sponsor) Medtronic Memphis, Tennessee
Antoni Tomsia, PhD Lawrence Berkeley National Laboratory Berkeley, California
Maurizio Tonetti, DMD, PhD Genova, Italy
R. Gilbert Triplett, DDS, PhD Baylor College of Dentistry Dallas, Texas
Rocky Tuan, PhD Center for Cellular and Molecular Engineering Department of Orthopaedic Surgery University of Pittsburgh Pittsburgh, Pennsylvania
Minoru Ueda, DDS, PhD Department of Oral and Maxillofacial Surgery Nagoya University Graduate School of Medicine Nagoya, Japan
Stephen S. Wallace, DDS Central CT Dental Implant Center Waterbury, Connecticut
Hai Bo Wen Zimmer Dental Inc Carlsbad, California
Stephen L. Wheeler, DDS Encinitas, California
Ulf M. E. Wikesjo, DDS, DMD, PhD Medical College of Georgia Martinez, Georgia
Mollie A. Winston, DDS Atlanta, Georgia
Mark E. Wong, DDS Houston, Texas
Jennifer Woodell-May, PhD (Sponsor) Biomet Biologics Warsaw, Indiana
© 2011 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY.. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.