Embed Size (px)
Citation preview

IrishMedicalJournal
Official Journal of theIrish MedicalOrganisation
˜ Established 1867 ˜
JUNE 2013 Volume 106 ■ Number 6
163 This MonthIMJ Commentary
164 Rotavirus Vaccination Gains Wider Acceptance With itsIntroduction Into the UK Vaccination Programme
Editorial165 To Screen or Not to Screen for Subclinical Hypothyroidism in
Pregnancy?A Freyne, B Byrne
Original Papers166 Non-Pulmonary Chronic Diseases in Adults with Cystic Fibrosis:
Analysis of Data from the Cystic Fibrosis RegistryR Somerville, A Jackson, S Zhou, G Fletcher, P Fitzpatrick
169 Delayed Prescriptions: Attitudes and Experiences of GeneralPractitioners in the MidwestM Hayes, A Faherty, D Hannon
171 The National Newborn Bloodspot Screening Programme (NNBSP)Process Review 2010P Jennings, M Hegarty, L Smith
173 A Profile of Elderly Fallers Referred for Physiotherapy in theEmergency Department of a Dublin Teaching HospitalF Crehan, D O’Shea, JM Ryan, F Horgan
176 Presentation and Management of Gastrointestinal StromalTumoursAM Mongan, V Malik, S Rowley, Z Claxton, C Muldoon, D O’Toole, N Ravi, JVReynolds
179 Length of Stay Following Elective Surgery –Can We Improve Efficiency?JG Solon, JC Coffey, DA McNamara
Case Report181 Case 2: Silicosis
DT Murphy, DM Murphy, JG Murray, SP Gaine
182 Double Trouble – Ureteric Obstruction Due to Bilateral UrothelialCarcinomaGJ Nason, F O’Kelly, DW Mulvin
Research Correspondence184 Recurring Themes Arising During Medical Research Ethics
Committee ReviewE Kelleher, A Stanton, G Vale, D Smith
Occasional Piece186 Non Heart Beating Organ Donation in Adults:
A Clinical Practice GuidelineJ O’Rourke
Letters to the Editor162 Impulsive-Compulsive Behaviours in Parkinson’s Disease –
Prevention is Better than Cure
SA Ryan, SS O’Sullivan
188 Are Girls with Turner Syndrome Obese?M Nadeem, EF Roche
Book Reviews190 ABC of Ear, Nose and Throat
MP Colreavy
190 ABC of Breast Diseases Fourth EditionA Lowery, ADK Hill
191 Continuing ProfessionalDevelopment
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 161

162Ir
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
EditorJFA Murphy, FRCPI
Assistant to the EditorLorna Duffy
Director of Finance & AdministrationSusan Clyne
IMO Management CommitteeDr Matthew Sadlier (President)Dr Trevor Duffy (Vice President and Chair,Consultant Committee)Professor Sean Tierney (Hon Treasurer)Dr Padraig Mc Garry (Hon Secretary)Dr Ray Walley (Chair, GP Committee)Dr Brett Lynam (Chair, PHD Committee)Dr John Donnellan (Chair, NCHD Committee)Dr Paul McKeown (Immediate Past President)
Subscriptions 2013Annual Subscription:
Ireland, UK, EU €250Outside EU €400
Address: IMJ Editorial OfficeIMO House, 10 Fitzwilliam Place, Dublin 2Tel: (01) 676 7273. Fax: (01) 661 2758
E-mail: [email protected] Web: www.imj.ie
© Irish Medical Journal 2012. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any other means – electronic, mechanical,photocopying, recording or otherwise without prior permission in writing from the Irish Medical Journal.
Impulsive-Compulsive Behavioursin Parkinson’s Disease –Prevention is Better than CureSir,
We read with interest the account by Wilson et al of impulsecontrol disorders in patients with Parkinson’s disease (PD)receiving dopamine replacement therapy.1 The prevalence ofimpulsive-compulsive behaviours (ICBs) in patients with PD isapproximately 14% and includes pathological gambling,compulsive sexual behaviour, compulsive spending, binge eating,punding and the addiction-like compulsive use of dopaminergicmedications.2 Early recognition and prevention of ICBs, coupledwith awareness of clinical risk factors for their development is ofparamount importance given the lack of specific treatments forthese debilitating behaviours. We always warn our PD patients andtheir families/care-givers specifically about these potentialcomplications when commencing dopamine replacementtherapies and the need to seek medical advice promptly shouldthey develop. We believe that this is a policy that should beinstituted in all centres treating patients with PD.
We agree with the authors that management of ICBs shouldconsist of modifications to dopamine replacement therapy,especially dopamine agonists. However, it is increasinglyrecognized that a constellation of symptoms similar to addictivedrug withdrawal can develop in PD patients who are taperingdoses of dopamine agonists (DAs), termed the Dopamine AgonistWithdrawal Syndrome (DAWS). The frequency of patientsdeveloping DAWS seems to be over 15% and is more frequentlyseen in patients with ICBs who are weaned off DAs.3 DAWS is asevere, stereotyped cluster of physical and psychologicalsymptoms that correlate with DA withdrawal in a dose-dependentmanner, cause clinically significant distress or social/occupationaldysfunction, are refractory to levodopa and other Parkinsondisease medications, and cannot be accounted for by other clinicalfactors. Treating physicians need to be aware of the potential fordeveloping DAWS in PD patients with ICBs.
Lastly the authors comment on the use of deep brain stimulation(DBS) in patients with ICBs. As stated it seems that ICBs andpunding behaviours may persist, worsen or develop for the firsttime post DBS but it seems that where the ICBs are recognizedpre-operatively a positive outcome post DBS is more likely.4
SA Ryan, SS O’SullivanNeurology Department, Cork University Hospital, Wilton, CorkEmail: [email protected]
References1. Wilson L, Sheehan J, Thorpe M. Three cases of impulse control disorder in
Parkinson’s disease patients receiving dopamine replacement therapy. Ir Med J.2013; 106: 24-5.
2. Djamshidian A, Averbeck BB, Lees AJ, O’Sullivan SS. Clinical aspects ofimpulsive behaviours in Parkinson’s disease. J Neurol Sci. 2011 Nov15;310:183-8.
3. Pondal M, Marras C, Miyasaki J, Moro E, Armstrong MJ, Strafella AP, Shah BB,Fox S, Prashanth LK, Phielipp N, Lang AE. Clinical features of dopamine agonistwithdrawal syndrome in a movement disorder clinic. J Neurol NeurosurgPsychiatry. 2013 Feb;84:130-5.
4. Lhommee E, Klinger H, Thobois S, Schmitt E, Ardouin C, Bichon A, Kistner A,Fraix V, Xie J, Aya Kombo M, Chabardès S, Seigneuret E, Benabid AL, MertensP, Polo G, Carnicella S, Quesada JL, Bosson JL, Broussolle E, Pollak P, Krack P.Subthalamic stimulation in Parkinson’s disease: restoring the balance ofmotivated behaviours. Brain. 2012 May;135:1463-77.
The Role
Working with the IRFU Medical Committee, the Head of Medical Services will operate at the cutting-edgeof professional sport in Ireland. The successful candidate will be responsible for designing, developing andimplementing medical and related strategies, plans and objectives which will deliver a world class medicalservice for professional rugby players employed by the IRFU and which will deliver up to date advice andpolicies to inform the wider amateur game at club and schools level.Primary responsibilities will be:
Medical Standards – ensuring medical personnel implement the highest possible medical and ethical•standards in all aspects of work.Medical Policy/Strategy – developing IRFU medical policy as well as define medical practices and•procedures in consultation with the IRFU Medical Advisory Committee and ensuring implementation ofthe agreed policy.Player Medical Care – Foster and maintain close links with and between national and provisional Team•doctors in relation to player injuries. Ensure that the IRFU are advised on all significant developments inthe field of preparation and care of players involved in contact sports to ensure that our systems can trulybe regarded as world classFinance – planning and reporting on current and forecast medical budgets detailing analysis of current•and expected expenditure.Injury Prevention / Rehabilitation – designing and implementing high quality and robust injury•prevention and rehabilitation processes.Anti-Doping Policy – ensuring International Rugby Board and related associations / bodies’ anti-doping•and substance abuse policies are properly adopted by the IRFU.
The CandidateThe successful candidate will have:•Full Registration with Medical Council•Excellent communication skills•Aminimum of 3 years’ experience working in Elite sport•A record of clinical excellence in a relevant field•
The Opportunity
This is an exciting role which enables the successful candidate to work across the entire spectrum of rugbyin Ireland and represents a unique opportunity to meet the medical demands of Irish Rugby as a majorsporting organisation both nationally and internationally.The successful candidate will receive a remuneration and benefits package commensurate with thisresponsibility. This position is being offered on a 3 year Fixed Term, Part-Time basis. Applicants shouldnote that this role will be based in Dublin.
Please forward your Curriculum Vitae (in confidence) with a covering letter supporting your application [email protected] or by post to Maurice Dowling, HR Director, IRFU,
10/12 Lansdowne Road, Ballsbridge, Dublin 4.
Closing date for applications is 21st June 2013.The IRFU is an equal opportunities employer.
IRFU Head of Medical ServicesThe Irish Rugby Football Union (IRFU) is the governing body for the sport of rugby union in Ireland.We are currently inviting applications for the position of ‘Head of Medical Services’.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 162

163This Month
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
In this Month’s IMJ
Non-Pulmonary chronic diseases in adults with cysticfibrosis: analysis of data from the cystic fibrosis registry:Somerville et al have reviewed the non-pulmonary sequelae ofcystic fibrosis (CF). Their findings are based on the 1027 patientson the CF registry. Among the adult CF patients, 25.7% havediabetes, 42.7% have bone disease, 11.6% have liver disease. Thecorresponding rates in children are much lower. The authors pointout that the non-pulmonary CF complications pose manychallenges.
Delayed prescriptions: attitudes and experiences ofgeneral practitioners in the Midwest: Hayes et al haveaddressed the issue of delayed prescriptions for antibiotics. It isfelt that they involve patients in their own illness and itsmanagement. Over one third of GPs use them at least once a day.As along as the patient has clear instructions about when tocommence treatment the practice appears to be safe.
A profile of elderly fallersreferred for physiotherapy inthe emergency department ofa Dublin teaching hospital:Crehan et al have examined theprofile of elderly fallers. The meanage was 84.88 years and 75.5%were female. All had slow walkingspeed and 65% had poor gripstrength. Three quarters weredescribed as being frail.
Presentation and management of gastrointestinalstromal tumours: Mongan et al describe a series of 78 patientswith gastrointestinal stromal tumours (GIST). The median age atpresentation was 66 years with a relatively similar number of menand women. The majority 90% received surgery. Imatinib wasadministered to 25%. The 5 year survival was 89%. The authorsemphasise the very encouraging results.
Length of stay following elective surgery- can we improveefficiency? Solon et al surveyed 20 consultant surgeons on theirattitudes to length of stay (LOS) for common surgical procedures.There was a broad consensus for most operations exceptlaparoscopic cholecystectomy and haemorrhoidectomy. Factorsthat help to reduce stay include pre-assessment clinics, day ofsurgery admission and day case surgery.
Non heart beating organ donation in adults: a clinicalpractice guideline: O’Rourke describe the practice of non heartbeating donation (NHBD) compared with brain stem deathdonation. It offers a practical alternative when the criteria for brainstem death cannot be satisfied. The international experience isalso documented.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 163

164 CommentaryIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
The Rotavirus vaccine1 is being introduced into the UKvaccination programme in July 2013. The Department ofHealth (UK) said that the move would mean thousands ofyoung children would be spared hospital stays and hundredsof thousands of GP visits. David Elliman at RCPCH stated ‘thisis an important advance as while rotavirus does not causemany deaths in the UK, it does cause a huge amount ofsuffering’. He added that the vaccine has been used for someyears in the US, so though new to us there is a large body ofexperience showing that it is safe and effective. Dame SallyDavies, the chief medical officer said that it is upsetting to seeour children in hospital. Currently more than 40 countriesinclude a rotavirus vaccine in their immunisation schedule.
Two doses of the oral monovalent vaccine Rotarix will beadministered with the other vaccines before age 4 months. Itis a live attenuated vaccine and can be administeredconcomitantly with all routinely recommended infant vaccines.
It is anticipated that the vaccine will half the number of casesof vomiting and diarrhoea. It will reduce rotavirus associatedhospital admissions by 70%. It is not part of the Irishimmunisation programme at present but is available on anindividual case basis. Into the future GPs are likely to receiveincreased numbers of enquiries about the vaccine fromparents particularly those with a child in a crèche.
Rotavirus is the most common cause of severe gastroenteritisin children particularly in the winter months. It was firstidentified by Ruth Bishop in Melbourne in 1973. It causesdiarrhoea by increasing the turnover of enterocytes leading tothe population of blunted villi by immature cells that areincapable of normal absorption. There is a 24 to 72 hourincubation followed by between 3 and 8 days of vomiting anddiarrhoea. Usually rotavirus excretion stops within 10 days ofthe onset of symptoms. Nearly all children are affected by age5 years but those under 2 years are the most susceptible agegroup. It is transmitted from person to person through thefaecal-oral route or contact with contaminated objects such astoys. The impact of Rotavirus infection on babies and youngchildren has been well studied. While most children recover ontheir own, it can cause severe illness and hospitalisation insome cases. In the UK it causes 750,000 episodes ofdiarrhoea and 80,000 GP consultations annually. It isresponsible for 45% of diarrhoea related admissions andaccounts for 20% of the diarrhoeal illness seen in emergencydepartments. The disease burden from rotavirus in Ireland isconsidered to be high. In hospitalised children less than 2years, 1 in 38 have a laboratory confirmed rotavirus infection2.A Dublin study3 (Crumlin and Temple Street) found that 1% ofall hospital admissions are due to rotavirus diarrhoea. In a 2year period it utilised 2,305 bed days. The clinical casedefinition of rotavirus gastroenteritis is an episode of diarrhoea(passage of 3 or more loose or watery stools within a day),with or without vomiting, where rotavirus was identified in astool sample. Severity of gastroenteritis can be determined bya clinical scoring system, the Vesikari scale4, which assessesthe duration and intensity of diarrhoea and vomiting, theintensity of fever, use of rehydration therapy or hospitalizationfor each episode. Scores range from 0 to 20, where higherscores indicate greater severity. An episode of gastroenteritiswith a score of 11 or greater is considered severe.
In the US routine Rotavirus vaccination was introduced in2006. Rotavirus diarrhoea related hospital admissions havedecreased by two thirds. Prior to approval the FDA directedmanufacturers to enrol and follow up 60,000 infants in trials5.Vaccine associated intussusception, a problem with a previousproduct in the 1990s, was not encountered in this recentstudy. Post-marketing surveillance following distribution of 14million doses did not suggest an increased risk of adverseevents. The uptake of the vaccine in the US has beenimpressive and in 2010 almost 60% of children aged 19 to 35months had been vaccinated. By 2008 the rotavirus detectionrate had reduced by 64%. Also diarrhoea among children whohad not received the vaccine had also declined due to reducedherd exposure. During the 2008 winter rotavirus season,50,000 hospitalisations were avoided across the US.
More recently a slight increase in risk of intussusception afterthe vaccine was reported from Mexico6. The intussusceptionrisk is 1 of every 60,000 vaccinated infants. The increased riskis after the first dose, in the first month but especially in thefirst 7 days. This is substantially less than the intussusceptionrisk of 1 in 10,000 encountered with Rotashield, a vaccinewithdrawn in 1999. The likely mechanism is that intestinalreplication of the virus vaccine causes a local inflammatoryresponse in the lymphatic tissue. The vaccine, however, hasbeen very effective in Mexico and has reduced childhooddiarrhoea deaths by 700 annually. To further minimise this riskthe WHO recommends that the first dose of the vaccine beadministered when infants are 14 weeks of age or younger.The vaccine is licensed for ages 6-24 weeks. A rarepostulated association of rotavirus vaccine with Kawasakidisease has not been substantiated in a recent analysis7. Thevaccine is contraindicated in children with severe combinedimmunodeficiency and those who have had a previousintussusception.
In summary the arguments in favour of the rotavirus vaccineare threefold. It will reduce diarrhoea morbidity in infants andyoung children, it will reduce medical attendances at the 3interfaces of GP, emergency department, hospitalisation and insocietal terms it will reduce working days lost by parents.
JFA MurphyEditor
References1. Miren IG, Cunliffe N. Welcoming rotavirus vaccine to the UK
immunisation schedule. BMJ 2013;346:7-8.2. Lynch M, O’Halloran F, Whyte D, Fanning S, Cryan B, Glass RI.
Rotavirus in Ireland: national estimates of disease burden, 1997-1998.Pediatr Infect Dis J 2001;20:693-8.
3. Harrington M, Butler C, Cafferkey M. Rotavirus infection inhospitalised children: incidence and impact on healthcare resources.IJMS 2003;172:33-36
4. Vesikari clinical severity scoring system manual. Path version 1.3 20115. Glass RI, Patel M, Parashar U. Lessons from the US rotavirus
vaccination program. JAMA 2011;306:1701-2.6. Patel M, Lopez-Collada V, Bulhoes MM et al. Intussusception risk and
health benefits of rotavirus vaccination in Mexico and Brasil. N Engl JMed 2011;364:2283-92.
7. Hua W, Izureta H, Slade B et al. Kawasackie disease after vaccination:reports to the vaccine adverse event reporting system 190-2007.Pediatr Infect Dis J 2009;28:944-7.
Rotavirus Vaccination Gains Wider Acceptance With itsIntroduction Into the UK Vaccination Programme
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 164

165Editorial
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
Not unlike screening for gestational diabetes, controversy prevailsover the value of screening for thyroid disease in pregnancy.Fortunately, overt hypothyroidism is rare in pregnancy (0.3-0.5%)because it is associated with infertility and increased rates of firsttrimester miscarriage. Studies suggest that obstetriccomplications such as hypertension, placental abruption, pretermdelivery, perinatal morbidity and mortality are increased in womenwith hypothyroidism in pregnancy1 and there is evidence that theoffspring of untreated mothers have neuropsychological andcognitive impairment. Subclinical hypothyroidism (Elevated TSHand normal Free T4) is estimated to be present in 2 – 2.5% ofpregnant women. It is not as clearly associated with adverseobstetric and neonatal outcome but there is some evidence thatmaternal subclinical hypothyroidism is associated with impairedpsychomotor development in the offspring2.
Most expert groups advise targeted screening of mothers whohave risk factors for thyroid disease e.g. If symptomatic, residencein an area of iodine deficiency, family or personal history of thyroiddisease, known Thyroid Peroxidase antibodies, Type I diabetesmellitus, history of preterm labour or miscarriage, history of heador neck radiation, BMI > 40 kg/m2, infertility and Age >30years3. It is estimated, however, that one third of cases will bemissed with targeted screening and some experts are calling foruniversal screening claiming that this will be more cost effectivewith an estimated saving of more than 8 million dollars for every100,000 women screened4. This estimate is based on theassumption that detection and treatment of the 2.5% women withsubclinical hypothyroidism will impact on the neurocognitivedevelopment of their offspring.
This does not appear to be the case, however. A paper in theNEJM in 2010 reports the results of a well conducted trial where21,846 women less than 16 weeks gestation had serum takenand were randomized to be tested for TSH and T4 immediately orfollowing delivery5. Those that were tested in early pregnancy andhad TSH levels above the 97.5th centile, free T4 less than the2.5th centile or both were deemed screen positive and treatedwith thyroxine. Bloods were repeated six weeks later and doseadjusted to a target TSH of 0.1 – 1.0 mIU/L. The primary studyoutcome was IQ at 3 years of age in the children of the womenwho tested positive.
4.6% of the screening group tested positive and 5% of thecontrol group and about 5% of these cases had both a high TSHand low free T4. Both groups were comparable in terms ofbaseline and socioeconomic characteristics and had similargestational age at delivery, rates of preterm birth and birth weight.The analysis based on intention to treat showed a meanstandardized IQ at 3 years of age of 100 in the screening groupand 99.2 in the control group (p=0.40) and the proportions ofchildren with an IQ of less than 85 was 12.1% compared to 14.1%(p=0.39). There was no difference between groups in otherpsychological assessments (CBCL and Brief-P scores). 79% ofwomen in the screening group were compliant with medicationand the results were unchanged when on- treatment analysis wasperformed.
At approximately 10 to 12 weeks gestation the fetal thyroid canconcentrate iodine and synthesise iodothyronines but hormonalsynthesis is limited until the 18th to 20th week. For this reason,the fetus is thought to be dependent on maternal T4 and T3 inthe first trimester when neurodevelopment is occurring. It is
possible that screening for and treatment of maternal subclinicalhypothyroidism occurred too late in gestation (median 13 weeks 3days) in this study but, in practical terms, this is the time thatwomen present for antenatal care. Preconceptual screening maybe of benefit in women planning pregnancy or attending infertilityclinics. Major deficits in our understanding of fetal and placentalthyroid physiology remain, however. Thyroid hormone receptor isnot expressed in fetal tissue until 8-10 weeks and the placenta isrich in T III deiodinase that converts maternal thyroxine to inactiverT3 such that a large percentage of maternal thyroxine neverreaches the fetus. Thus, the hypothesis that administration ofthyroxine to a mother with subclinical hypothyroidism may impacton the neurocognitive development of her fetus may be toosimplistic.
Perhaps the primary end point of this study, namely IQ at 3 years,did not have the sensitivity to detect subtle differences inoutcome between the two groups. It is reassuring, however, tonote that the mean IQ in the children born to the women withsubclinical hypothyroidism was not different from that of thenormal population. Hypothyroidism has been associated withpsychomotor deficits, delays in language development, orientation,vision abnormalities and behavioural changes5. This study was notdesigned to examine for all of these end points. There is currentlyanother RCT examining the impact of screening and treatment onIQ at 5 years of age6. This study focusing on the intellectualfunction of offspring at five years of age will hopefully shed morelight on the subject. Secondary outcomes include motor andpsychomotor development, behavioural and social competenciesand some obstetric complications.
The paper by Lazarus et al5 is important in the interim because itprovides randomized controlled data on neurocognitive outcomefollowing screening for subclinical hypothyroidism and thyroxinesupplementation in pregnancy. It clearly shows that there is noinfluence on infant outcome in terms of IQ at 3 years of age. Atthe present time screening for and treating subclinicalhypothyroidism in early pregnancy has no proven maternal andfetal benefit and the results of the ongoing NICHD study will notbe available until 2015.
A Freyne, B ByrneCoombe Women and Infants University Hospital, Cork St, Dublin 8
References1. Ross DS. Hypothyroidism during pregnancy: Clinical manifestations ,
diagnosis and treatment. Up to Date 2012.2. Haddow JE, Palomaki GE, Allan WC et al. Maternal thyroid deficiency
during pregnancy and subsequent neuropsychological development ofthe child. New England Journal of Medicine 1999; 341: 549- 55.
3. Stagnaro-Green A , Abalovich M, Alexander E et al. Guidelines of theAmerican Thyroid Association for the diagnosis and management ofthyroid disease during pregnancy and postpartum. Thyroid2011;21:108-1125.
4. Thung SF, Funai EF and Grobman WA. The cost effectiveness ofuniversal screening in pregnancy for subclinical hypothyroidism. Am JOG 2009;20:267.e1
5. Lazarus JH, Bestwick JP, Channon S et al. Antenatal thyroidscreening and childhood cognitive function. New England Journal ofMedicine 2010: 366: 493-501.
6. NICHD. Thyroid therapy for mild thyroid deficiency in pregnancy.Bethesda, MD: National Library of Medicine (http://www.clinicaltrials.gov/ct/show/NCT 00388297).
To Screen or Not to Screen for Subclinical Hypothyroidism inPregnancy?
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 165

166 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
IntroductionIreland has the highest rate of CF in the world, with an estimatedincidence of 1/13531 and prevalence of 2.98/10,000.2 AlthoughCF is still the most frequently diagnosed fatal genetic illness inCaucasians, life expectancy has improved dramatically in recentdecades.3-8 The median survival for Irish males and females bornin 1985-1994 is now predicted to be 51.1 and 39.0 yearsrespectively.9 This increased longevity has translated into anincrease in the Irish adult CF population of approximately 2% peryear since 2002.10 The three main non-pulmonary chronicdiseases associated with CF are diabetes, liver disease and bonedisease. The incidence of diabetes and bone disease increaseswith age,5,11-13 whereas liver disease is usually diagnosed inchildhood.14,15 The prevalence of diabetes is reported to beapproximately 36% in adults aged 18-30 and 52% in adults aged>40.16 Approximately 20-60% of CF patients have some evidenceof liver disease and 5-15% develop cirrhosis.5,14,17 23.5% of adultswith CF are estimated to have osteoporosis and 38%osteopenia.18 As patients grow older, it can be expected thatthese non-pulmonary CF-related chronic diseases will become agreater source of morbidity among this adult population.4,11,19
MethodsThis study used data from the CFRI, including all patients alive on31/12/2009. The aims were: to describe the demographics of theIrish adult CF population, to assess the prevalence of diabetes,liver disease and osteoporosis/osteopenia in adult patients and tocompare these with the paediatric population and to identify thedemographic and clinical features of these diseases in the adultpopulation.
Since 2001, the CFRI has gathered clinical and demographicinformation on all enrolled people with CF in Ireland, both atbaseline and annually.20 As of 2010, 90% of the Irish CFpopulation were enrolled.10 The variables included in this analysiswere: age, gender, CF genotype, highest forced expiratory volumein one second (FEV1) of 2009, highest body mass index (BMI) of2009, number of hospitalisations and respiratory exacerbationsrequiring intravenous (IV) antibiotics in the last 12 months andpresence of the following complications: pancreatic insufficiency,chronic Staphylococcus aureus infection, chronic Pseudomonasinfection, liver disease, diabetes, osteoporosis/osteopenia anddepression. In recording of data by CFRI staff, number ofrespiratory exacerbations requiring IV antibiotics (hereafterreferred to as “respiratory exacerbations”) is recorded as thenumber of times IV antibiotics were prescribed for a respiratoryinfection in the last year. Diabetes is recorded as present if thepatient is documented as being on insulin in the last year, whereasliver disease, depression and osteoporosis/osteopenia (recordedtogether) are considered present if documented in the medicalnotes in the last year. Chronic infection is considered present ifthe patient has had 3 or more documented isolates of the
organism in the last year. In the case of Pseudomonas, thisincludes all types of Pseudomonas organisms.
Adults were defined as those ≥18 years of age; those <18 wereconsidered children. Age was used as a continuous variable inregression analysis, and in other adult analyses age was examinedin two ways. To give an overall view, 5 year age groups werecreated with the ≥40 year old patients grouped together due tosmall numbers. Given that patients over 40 may differsystematically from younger patients, a variable with two groupswas also created, greater than/equal to or less than 40 years old.Proportions in groups were compared using χ2 test or Fisher’sexact test as appropriate. Means in groups were compared usingstudent’s t test for two groups and ANOVA for more than twogroups. Where values were not normally distributed, the Mann-Whitney U test was used to compare medians in groups. Adjustedmeans were obtained using ANCOVA. Logistic regression wasused to adjust for confounders and variables which had asignificance of p<0.10 on univariate analysis were entered into themultivariable models. A p value of <0.05 was taken to besignificant.
ResultsDemographics of the Adult CF PopulationOf the 1027 patients with CF who were enrolled with the CFRIand alive on 31/12/2009; 531 (51.7%) were ≥18 years of age(range 18-59). 312 (58.8%) were male and there was nosignificant difference in the distribution of the sexes across theage groups (p=0.864, Figure 1). In terms of genotype, 288(54.2%) were ∆F508 homozygous, 173 (32.6%) were ∆F508heterozygous, 40 (7.5%) were another genotype, 14 (2.6%) wereunknown and 16 (3.0%) were untested. There was no significant
Non-Pulmonary Chronic Diseases in Adults with CysticFibrosis: Analysis of Data from the Cystic Fibrosis RegistryR Somerville, A Jackson, S Zhou, G Fletcher, P FitzpatrickUCD School of Public Health Physiotherapy and Population Science, Belfield, Dublin 4
AbstractThe international literature shows that the demography of cystic fibrosis (CF) is changing, with patients increasingly surviving intoadulthood. As they age, patients with CF become more susceptible to specific non-pulmonary chronic diseases. In this study, adultdata from the CF Registry of Ireland (CFRI) was used to determine the prevalence and associated features of these diseases. 104(25.7%) adults had diabetes versus 13 (2.9%) children (p<0.001). Liver disease was present in 47 (11.6%) adults and 26 (5.7%)children (p=0.002). 173 (42.7%) adults had bone disease versus 25 (5.5%) children (p<0.001). Adults with one non-pulmonarychronic disease, for example liver disease, were more likely to have another (p=0.002), those with diabetes and bone disease had ahigher number of hospital admissions in the last 12 months (p<0.001 for both) and higher rates of depression (p=0.046 andp=0.049, respectively). These results highlight a number of challenges for the Irish healthcare system.
Figure 1 Age and Sex Distribution of Adult Population
To receive CPD credits, you must completethe questions online at www.imj.ie.
CPD available online at www.imj.ie and questions on page 191
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 166

167Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
difference in genotype by five year age groups (p=0.486), by twoage groups (p=0.179), or by sex (p=0.098).
Non-Pulmonary Chronic DiseasesInformation regarding the presence of diabetes, liver disease andbone disease was available for a group of 405 adults (76.27%).These patients did not differ significantly (in terms of sex, BMI,genotype and FEV1) from those for whom information wasmissing with the exception of a slightly lower median age (25.45versus 28.07 years, p<0.001).
Comparison of Adult and Paediatric CF Populations104 (25.7%) adults had been diagnosed with diabetes comparedwith 13 (2.9%) children (p<0.001). Liver disease was present in47 (11.6%) adults and 26 (5.7%) children (p=0.002). 173 (42.7%)adults had osteoporosis/osteopenia as compared with 25 (5.5%)children (p<0.001).
Associated Demographic and Clinical Features in the Adult CFPopulationDiabetesIn the adult population, there was no significant difference in theprevalence of diabetes between the sexes (p=0.258) or acrossthe five age groups (p=0.206). Diabetic patients had a highermedian number of admissions (p<0.001) and respiratoryexacerbations (p=0.023) and a higher prevalence of chronicPseudomonas infection (72.1% versus 58.8%, p=0.016). Themean BMI and FEV1 values of diabetic patients were lower, butthis did not reach statistical significance. 7/104 (6.7%) adults withdiabetes had depression, versus 6/301 (2.0%) of those without(p=0.046). The results of the univariate logistic regressionanalysis for factors associated with diabetes in adults are shownin Table 1. On multivariate logistic regression, adjusted for all otherfactors that were significant (p<0.10) on univariate analysis exceptpancreatic insufficiency; ∆F508 homozygosity, bone disease andliver disease were significantly associated with diabetes (Table 2,model one). When pancreatic insufficiency was added to thismodel all other relationships became insignificant (Table 2, modeltwo) indicating that the relationships are confounded by thestrong inter-relationships between diabetes, pancreaticinsufficiency and ∆F508 homozygosity.
Liver DiseaseAmong the adult patients, there was a significant associationbetween liver disease and ∆F508 homozygosity (p=0.018) butnot sex (p=0.128). There were significant associations betweenliver disease and diabetes and osteoporosis/osteopenia (p=0.002for both, Figure 2).
Osteoporosis/OsteopeniaIn the adult population, there was no significant association
between osteoporosis/osteopenia and ∆F508 homozygosity(p=0.191) or sex (p=0.411) but those with bone disease had ahigher prevalence of chronic Pseudomonas infection (68.8%versus 57.3%, p=0.019). Adults with bone disease were older, witha median age of 26.2 versus 24.8 (p=0.009) and the ageadjusted mean BMI (p=0.003) and FEV1 (p<0.001) weresignificantly lower in those with bone disease. Adults with bonedisease had a higher median number of admissions (p<0.001)and respiratory exacerbations (p<0.001) than those without. Therewas also a significant association (p<0.001) between bonedisease and diabetes. 9/173 (5.2%) adults with bone disease haddepression, versus 4/232 (1.7%) of those without (p=0.049).
DiscussionOver half (51.7%) of the patients in this study were ≥18 years ofage. This is in keeping with the documented increase in the adultCF population both in Ireland, with 49% aged ≥18 years in 200720
and 52.7% in 2010,10 and in countries such as America.4,17 Theneed to review services in Ireland in order to ensure they aremeeting the needs of the adult CF population has been
Table 1 Factors Associated with Diabetes on Univariate LogisticRegression Analysis
Variable RegressionCo-efficient (OR) p value
Age† 0.017 (1.02) 0.261
Sex†† -0.264 (0.77) 0.259
BMI† -0.052 (0.95) 0.181
∆F508 homozygous††† 0.756 (2.13) 0.002
Pancreatic insufficiency 2.700 (14.88) <0.001
Osteoporosis or osteopenia 0.819 (2.27) <0.001
Liver disease 0.984 (2.68) 0.002
Depression 1.266 (3.55) 0.026
Chronic Staphylococcus aureus infection -0.519 (0.60) 0.064
Chronic Pseudomonas infection 0.594 (1.81) 0.017
Number of hospitalisations† 0.217 (1.24) 0.005
Number of respiratory exacerbations† 0.061 (1.063) 0.303
† Per unit increase†† Female versus male
††† Versus all other genotypes
Table 2 Multivariate Logistic Regression Analysis of FactorsAssociated with Diabetes
VariableUnadjusted OR
(95% ConfidenceInterval)
Model oneAdjusted OR*
(95% ConfidenceInterval)
Model twoAdjusted OR**
(95% ConfidenceInterval)
rrF508homozygous†
2.13 (1.30 – 3.47)*** 1.89 (1.14 – 3.15)*** 1.65 (0.98 – 2.79)
Pancreaticinsufficiency
14.88(3.58 – 61.90)*** N/A 19.78
(2.65 – 147.56)***Osteoporosisor osteopenia
2.27 (1.44 – 3.57)*** 1.69 (1.04 – 2.76)*** 1.3 (0.79 – 2.14)
Liver disease 2.68 (1.43 – 5.00)*** 2.1 (1.08 – 4.10)*** 1.88 (0.96 – 3.70)
Depression 3.55 (1.16 – 10.81)*** 1.38 (0.40 – 4.84) 1.39 (0.40 – 4.76)
ChronicStaphylococcusaureus infection
0.60 (0.344 – 1.03) 0.65 (0.36 – 1.17) 0.62 (0.35 – 1.13)
ChronicPseudomonasinfection
1.81 (1.11 – 2.95)*** 1.33 (0.77 – 2.30) 1.21 (0.70 – 2.10)
Number ofhospitalisations††
1.24 (1.07 – 1.45)*** 1.15 (0.96 – 1.36) 1.10 (0.93 – 1.31)
† Versus all other Genotypes†† Per unit increase* Adjusted for F508 homozygosity, chronic Pseudomonas and Staphylococcus
aureus infection, osteoporosis/osteopenia, liver disease, depression andnumber of hospitalisations
** Adjusted for F508 homozygosity, chronic Pseudomonas and Staphylococcusaureus infection, osteoporosis/osteopenia, liver disease, depression, number ofhospitalisations and pancreatic insufficiency
*** p<0.05N/A Not applicable
Figure 2 Association of Liver Disease with Diabetes and Bone Disease in Adults
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 167

168 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
recognised by many organisations, including the CFRI.20 A 2009Health Service Executive report commented on inadequatefacilities across CF services and the need to prioritiseimprovement of adult services.8 As well as this, the concept oftransition of care from paediatric services is clearly important.4,8,11
The prevalence of bone disease reported in this study is inkeeping with the literature. The prevalence of diabetes and liverdisease are likely underestimated, especially in those withsubclinical disease, due to the way in which data are collected.However, what is clear is that, in keeping with the literature, theprevalence of all of these conditions is significantly higher inadults than in children. Given that complications are monitored forin both paediatric and adult clinics, this is unlikely to be due tobetter case-finding in adults.
Each of these non-pulmonary chronic diseases comes with itsown complications. Diabetes is the most common and is ofparticular significance due to its associated worse pulmonaryfunction and increased mortality.3,4,6,11,12,17,19,21-23 One large studydetermined the age-adjusted mortality rates in those with andwithout diabetes to be 4.2 and 1.5 per 100 person-yearsrespectively, with an increased mortality rate in diabeticsirrespective of age.24 Unlike diabetes, chronic liver disease in CFadults tends to run a mild course, but it can be associated withrapid decompensation14,15 necessitating liver transplant.4,15 Bonedisease can lead to fractures and consequent pain, dysfunctionand deformity11 and vertebral fractures can be a contraindicationto lung transplant.7,13,18
While the burden of non-pulmonary chronic disease on individualswith CF cannot be assessed from a study such as this, theanalysis shows some interesting findings. A relationship betweendiabetes and liver disease in CF has previously been shown bothin Europe and the United States19,23 and this study confirms thatpatients with one non-pulmonary chronic disease were more likelyto have been diagnosed with another. Those with diabetes orbone disease were also more likely to have been admitted tohospital in the last 12 months. This increased number ofhospitalisations may be due to ascertainment bias, as patientswho are hospitalised more frequently are more likely to havecomorbidities picked up,19 however it may also reflect increasedseverity of disease. The risk of depression in CF adults, especiallyin those with poorer lung function has been previouslydocumented.25 Although small numbers prohibited more detailedanalysis, this study suggests a link between non-pulmonary CF-related chronic diseases and depression. Further research isneeded, as depression may be underreported from studies suchas this which rely on documented diagnoses as opposed toscores from validated instruments.25
In summary, while great advances have been made in CF care,which have translated into increased longevity, it is important toconsider the challenges this improving survival poses not just toindividual patients, but also to the Irish healthcare system andhealth care professionals in all areas of adult medicine, who maybecome more likely to encounter CF patients in their dailypractice.17 This study highlights the need to continue to invest inadult CF care, in what have historically been paediatric focusedservices. As well as infrastructural investment, funding forresearch into the causes and prevention, screening andmanagement strategies for these non-pulmonary chronic diseasescould provide new avenues in CF care and help ensure thatincreasing quantity of life is matched by a good quality of life forpatients with CF.11,25
Correspondence: R SomervilleUCD School of Public Health Physiotherapy and PopulationScience, Woodview House, Belfield, Dublin 4Email: [email protected]
AcknowledgementThe staff of Cystic Fibrosis Registry of Ireland for providing thedata for this study.
References1. Farrell P, Joffe S, Foley L, Canny GJ, Mayne P, Rosenberg M.
Diagnosis of cystic fibrosis in the Republic of Ireland: epidemiologyand costs. Ir Med J. 2007 Sep;100:557-60.
2. Farrell PM. The prevalence of cystic fibrosis in the European Union. JCyst Fibros. 2008 Sep;7:450-3.
3. O’Sullivan BP, Freedman SD. Cystic fibrosis. Lancet. 2009May;373:1891-904.
4. Yankaskas JR, Marshall BC, Sufian B, Simon RH, Rodman D. Cysticfibrosis adult care: consensus conference report. Chest. 2004Jan;125:1-39.
5. Bilton D. Cystic fibrosis. Medicine. 2008;36:273-8.6. Alexander S, Bridges N. Cystic fibrosis related diabetes. Pract Diab Int.
2010;27:198-200.7. Aris RM, Merkel PA, Bachrach LK, Borowitz DS, Boyle MP, Elkin SL,
Guise TA, Hardin DS, Haworth CS, Holick MF, Joseph PM, O’Brien K,Tullis E, Watts NB, White TB. Guide to bone health and disease incystic fibrosis. J Clin Endocrinol Metab. 2005 Mar;90:1888-96.
8. Health Service Executive. Services for People with Cystic Fibrosis inIreland. Dublin: 2009.
9. Jackson AD, Daly L, Jackson AL, Kelleher C, Marshall BC, QuintonHB, Fletcher G, Harrington M, Zhou S, McKone EF, Gallagher C, FoleyL, Fitzpatrick P. Validation and use of a parametric model forprojecting cystic fibrosis survivorship beyond observed data: a birthcohort analysis. Thorax. 2011 Aug;66:674-9.
10. The Cystic Fibrosis Registry of Ireland. Annual Report 2010. Dublin:2012.
11. Dobbin C, Bye P. Adults with cystic fibrosis: meeting the challenge!Intern Med J. 2003;33:593-7.
12. Mackie AD, Thornton SJ, Edenborough FP. Cystic fibrosis-relateddiabetes. Diabet Med. 2003 Jun;20:425-36.
13. Javier RM, Jacquot J. Bone disease in cystic fibrosis: what’s new?Joint Bone Spine. 2011 Oct;78:445-50.
14. Lamireau T, Monnereau S, Martin S, Marcotte JE, Winnock M, AlvarezF. Epidemiology of liver disease in cystic fibrosis: a longitudinal study. JHepatol. 2004 Dec;41:920-5.
15. Colombo C, Battezzati PM, Crosignani A, Morabito A, Costantini D,Padoan R, Giunta A. Liver disease in cystic fibrosis: A prospectivestudy on incidence, risk factors, and outcome. Hepatology. 2002Dec;36:1374-82.
16. van den Berg JM, Kouwenberg JM, Heijerman HG. Demographics ofglucose metabolism in cystic fibrosis. J Cyst Fibros. 2009 Jul;8:276-9.
17. Wilschanski M, Durie PR. Patterns of GI disease in adulthoodassociated with mutations in the CFTR gene. Gut. 2007;56:1153-63.
18. Paccou J, Zeboulon N, Combescure C, Gossec L, Cortet B. ThePrevalence of Osteoporosis, Osteopenia, and Fractures Among Adultswith Cystic Fibrosis: A Systematic Literature Review with Meta-Analysis. Calcif Tissue Int. 2010;86:1-7.
19. Marshall BC, Butler SM, Stoddard M, Moran AM, Liou TG, Morgan WJ.Epidemiology of cystic fibrosis-related diabetes. J Pediatr. 2005May;146:681-7.
20. The Cystic Fibrosis Registry of Ireland. Annual Report 2007. Dublin:2009.
21. Moran A, Becker D, Casella SJ, Gottlieb PA, Kirkman MS, MarshallBC, Slovis B. Epidemiology, pathophysiology, and prognosticimplications of cystic fibrosis-related diabetes: a technical review.Diabetes Care. 2010 Dec;33:2677-83.
22. Brennan AL, Geddes DM, Gyi KM, Baker EH. Clinical importance ofcystic fibrosis-related diabetes. J Cyst Fibros. 2004 Dec;3:209-22.
23. Minicucci L, Lorini R, Giannattasio A, Colombo C, Iapichino L, RealiMF, Padoan R, Calevo MG, Casciaro R, De Alessandri A, Haupt R.Liver disease as risk factor for cystic fibrosis-related diabetesdevelopment. Acta Paediatr. 2007 May;96:736-9.
24. Chamnan P, Shine BS, Haworth CS, Bilton D, Adler AI. Diabetes as adeterminant of mortality in cystic fibrosis. Diabetes Care. 2010Feb;33:311-6.
25. Riekert KA, Bartlett SJ, Boyle MP, Krishnan JA, Rand CS. Theassociation between depression, lung function, and health-relatedquality of life among adults with cystic fibrosis. Chest. 2007Jul;132:231-7.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 168

169Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
IntroductionA delayed prescription is one, which is given to a patient by adoctor for an appropriate antibiotic (in the case of this research), itis not meant to be used unless symptoms worsen or do not startto settle in the expected timescale. The delayed prescription hasoften been described as a method of compromise in situationswhere the doctor feels there is no clinical indication for anantibiotic, but the patient requests one. It can also provide a safetynet for the doctor, as we do not know who is at risk ofsubsequently developing rare but important complications ofinfection. Respiratory tract infections account for 60% of allantibiotic prescribing in primary care. NICE guidance onprescribing antibiotics for minor respiratory illnesses wasintroduced in 2008.1 Three different management strategies forantibiotics were outlined: no antibiotic prescribing, delayedprescribing and immediate prescribing. However, not all GPsendorse their use. Insights obtained from qualitative researchshow that some GPs had concerns that they may be missing ormasking serious illness, leading to medico legal issues. Some alsoworried that their patients may consider them incompetent.2 Ourspecific aims were to examine the attitudes and experiences ofGPs in the Mid- Western region toward the use of antibiotics ingeneral practice and to describe practice demographics.
MethodsWe applied for ethical approval to the ICGP ethics committee andwere granted approval in October 2010. The HSE Primary Careunit supplied us with a list of all 215 private and GMS GPs in theMid-Western area including Clare, Limerick and North Tipperary.The breakdown of doctors in each area is shown in Table 1. Weused a sample population of141 doctors from the Mid-Western region for thiscross sectional study. Werandomly selected 43doctors in Limerick city(30% 43/141), 34 doctors inCounty Limerick (24%34/141), 39 doctors inCounty Clare (28% 39/141)and 25 doctors in North Tipperary (18% 25/141) to roughly equateto the geographical spread of GPs throughout the region.Controls were not necessary as this was a cross sectional study.Data was collected by postal questionnaire over a 5-week periodfrom October 20th 2010 to November 24th 2010. Each GPreceived an explanatory letter with brief introduction,questionnaire and stamped addressed envelope for return. Allresponses were anonymous.
Results141 questionnaires were posted, 103 responses were received(response rate of 73%). All replies were complete and suitable forinterpretation.
Section 1: Attitudes and experiences32 GPs (31%) strongly agreed and 65 GPs (63%) agreed thatantibiotics are over used in general practice (majority). 2 of theGPs surveyed remained neutral. 4 GPs (4%) disagreed thatantibiotics are over used in general practice. 4 GPs (4%) feltunder pressure to prescribe an antibiotic several times a day. 35GPs (34%) felt under pressure to prescribe an antibiotic at leastonce a day. 40 GPs (39%) felt under pressure to prescribe anantibiotic once a week. 19 GPs (18%) felt under pressure toprescribe an antibiotic once a month. 5 GPs felt under pressure toprescribe an antibiotic less than once a month. All 103 GPs whoresponded were familiar with the term ‘Delayed’ or ‘Deferred’prescriptions. 20 GPs (19%) strongly agreed and 41(40%) agreedthat delayed prescriptions are a safe prescribing strategy. 31 GPs(30%) remained neutral. 7 GPs (7%) disagreed and 4(4%)strongly disagreed that delayed prescriptions is a safe prescribing
Delayed Prescriptions: Attitudes and Experiences of GeneralPractitioners in the MidwestM Hayes1, A Faherty2, D Hannon1
11 Greaney Close, Raheen, Limerick2The Surgery, Clane, Co Kildare
Abstract141 questionnaires were posted to GPs randomly selected in the Mid-West. 103 responses were received. 32 GPs (31%) stronglyagreed and 65 GPs (63%) agreed that antibiotics are over used in general practice. 35 GPs (34%) felt under pressure to prescribean antibiotic at least once a day. 41 GPs (40%) agreed that delayed prescriptions are a safe prescribing strategy. 53 GPs (51%)agreed that delayed prescriptions have the potential to reduce antibiotic use. 33 GPs (32%) disagreed that giving delayedprescriptions increases the duration of the consultation. 49 GPs (47%) agreed that delayed prescriptions decrease the likelihood ofreturn visit in the same illness. 55 GPs (53%) agreed that delayed prescriptions help to involve patients in managing their own illness.46 GPs (45%) disagreed that patients find delayed prescriptions confusing. The majority of GPs (41/39.8%) use delayedprescriptions once a week or at least once a day (34/33%).
Table 1 Number of GPs in eacharea of the Midwest
Number Percentage
Limerick City 69 32.1%
County Limerick 50 23.3%
County Clare 57 26.5%
North Tipperary 39 18.1%
Total 215 100%
Figure 1 Delayed prescriptions have the potential to reduce antibiotic use
Figure 2 Do you use delayed prescriptions in your clinical practice?
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 169

170 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
strategy. 32 GPs (31%) strongly agreed and 53 GPs (51%)agreed that delayed prescriptions have the potential to reduceantibiotic use. 11 GPs (11%) remained neutral. 4 GPs (4%)disagreed and 3GPs (3%) strongly disagreed that delayedprescriptions have the potential to reduce antibiotic use. 5 GPs(5%) strongly agreed and 22 GPs (21%) agreed that givingdelayed prescriptions increases the duration of the consultation.31 GPs (30%) remained neutral. 33 GPs (32%) disagreed and 12GPs (12%) strongly disagreed that giving delayed prescriptionsincreases the duration of the consultation.
27 GPs (26%) strongly agreed and 49 GPs (47%) agreed thatdelayed prescriptions decrease the likelihood of return visit in thesame illness. 13 GPs (13%) remained neutral. 11 GPs (11%)disagreed that delayed prescriptions decrease the likelihood ofreturn visit in the same illness, while 3 GPs (3%) stronglydisagreed. 31 GPs (30%) strongly agreed and 55 GPs (53%)agreed that delayed prescriptions help to involve patients inmanaging their own illness. 9 GPs (9%) remained neutral. 5 GPs(5%) disagreed that delayed prescriptions help to involve patientsin managing their own illness, while 3 GPs (3%) stronglydisagreed. 3 GPs (3%) strongly agreed that patients find delayedprescriptions confusing (minority). 7 GPs (7%) agreed thatpatients find delayed prescriptions confusing. 31 GPs (30%)remained neutral. 46 GPs (45%) disagreed and 16 (15%) stronglydisagreed that patients find delayed prescriptions confusing. 5GPs surveyed (4.9%) use delayed prescriptions several times aday. 34 GPs surveyed (33%) use delayed prescriptions at leastonce a day. 41 GPs (39.8%) surveyed use delayed prescriptiononce a week. 13 GPs (12.6%) use delayed prescriptions once amonth. 10 GPs surveyed (9.7%) never use delayed prescriptionsor use them less than once a month.
Section 2: Demographics81 responders were male (79%) and 22 were female (21%). 51responders (49%) worked in single-handed practices while 52(51%) worked in group practices. 57 responding GPs (55%) workin an urban setting. 38 (37%) work in a rural setting. 8 GPs (8%)work in a mixed setting. 77 (75%) responding GPs werevocationally trained. 26 (25%) were not. 32 responding GPs(31%) work in a training practice. 71 (69%) do not. 52 GPs (50%)see >30 patients/day on average (majority). 44 GPs (43%) see20-30 patients/day on average. 6 (6%) responding GPs see 10-19 patients/day on average. Only 1 responding GP (1%) sees<10 patients/day on average. 18 responding GPs (17.5%) havebeen working in GP between 0 and 9 years. 32 responding GPs(31%) have been working in GP between 10 and 19 years. 33responding GPs (32%) have been working in GP between 20 and29 years (majority). 19 responding GPs (18.5%) have beenworking in GP between 30 and 40 years. 1 responding GP (1%)has been working in GP > 40 years.
DiscussionThe first RCT of delayed prescriptions for respiratory symptomswas undertaken by Little et al in 1997, the delayed group filledonly 31% of the antibiotic prescriptions with no apparent seriousharm.3 A further study by Little et al showed that more of those
initially prescribed antibiotics returned to the surgery with sorethroat (38% v 27% in the other two groups).4 A Cochrane reviewby Arnold et al of interventions to improve antibiotic prescribingpractices in ambulatory care showed that patient-basedinterventions, particularly the use of delayed prescriptions forinfections for which antibiotics were not immediately indicatedeffectively reduced antibiotic use by patients and did not result inexcess morbidity.5 A systematic review of five trials (four based inthe UK and one in New Zealand) undertaken by Arroll et allooked at whether or not delayed prescriptions actually reducedantibiotic use in respiratory tract infections. There was aconsistent reduction in antibiotic usage in the five trials includedin the review suggesting that the delayed prescription is aneffective means of reducing antibiotic usage for acute respiratoryinfections.6
But are patients satisfied with delayed prescriptions? A study inthe BJGP in 2003, looked at patients’ responses to delayedprescriptions for acute upper respiratory tract infections. Just overhalf of the responders (53.1%) claimed to have consumed theirantibiotics. 87.1% were confident about taking the decision as towhether to use their antibiotics and 92.5% would choose toreceive a delayed prescription again.7 One Irish study looking atthe use of delayed prescriptions for non- specific URTI, sorethroat and cough showed that 64% (29/45) of patients got theantibiotics from the pharmacy, 36% (16/45) of patients consumedthe antibiotics and 29% (13/45) of patients did not use theantibiotics but got them from the pharmacy. Patient confidence indeciding whether or not to use the antibiotics was high.8
A US study in JAMA in 2006 showed that in acute otitis mediadelayed prescriptions reduces parents’ use of antibiotics from87% to 38%. In addition the parents that managed withoutantibiotics were more likely to say they would do without the nexttime (63% v 28%, P<0.001).9 Delayed prescribing of topicalantibiotics is probably the best strategy for managing acuteconjunctivitis in primary care say Everitt and colleagues. 10 Itreduced antibiotic use, showed no evidence of medicalisation,provided similar duration and severity of symptoms to immediateprescribing and reduced re-attendance for eye infections. Withregard to our study most GPs surveyed feel that antibiotics areoverused with 63% agreeing and 31% strongly agreeing with thestatement. The majority of GPs surveyed felt under pressure toprescribe antibiotics when they felt the antibiotic was unnecessarywith 39% feeling under pressure to prescribe in this circumstanceat least once a week and 34% at least once a day.
All responding GPs were familiar with the concept of delayed ordeferred prescriptions. The majority (40%) felt that delayedprescriptions were a safe prescribing strategy, however, a largeproportion (30%) remained neutral. Overall GPs felt that delayedprescriptions had the potential to cut down on antibiotic use with51% of GPs surveyed agreeing and 31% strongly agreeing. Themajority of GPs surveyed (32%) disagreed that giving a delayedprescription increases the duration of the consultation. 47% ofGPs surveyed agreed and 26% strongly agreed that delayedprescribing was seen to decrease the likelihood of return visit inthe same illness. Delayed prescribing was also seen as a way ofinvolving the patient in the management of their illness with 53%of GPs surveyed agreeing and 30% strongly agreeing with thisidea. The concept of patients finding delayed prescriptionsconfusing was denounced by the majority of GPs surveyed (45%).With regard to the usage of delayed prescriptions the majority ofGPs surveyed (39.8%) use them once a week, 33% use themonce a day, 12.6% use them once a month, 9.7% use them lessthan once per month or never and the minority 4.9% use themseveral times a day in their practice. Therefore the delayedprescription for antibiotics continues to be a useful managementoption for the majority of GPs surveyed.
This study provides information about the use of delayedprescriptions in routine general practice in the Mid-West. Delayed
Figure 3 Is your practice in an urban or rural setting?
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 170
171Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
prescribing of antibiotics has been shown in several studies to bea safe method of prescribing in various diagnoses including acuteotitis media, sore throat, cough and acute conjunctivitis in bothadults and children3-6,9,10. As long as patients have clear andspecific information about when to use antibiotics and when toreturn for assessment delayed prescribing of antibiotics for URTIis probably as safe or safer than other strategies and isacceptable to patients.11
Correspondence: M Hayes1 Greaney Close, Raheen, LimerickEmail: [email protected]
Refevrences1. Tan T, Little P, Stokes T. Antibiotic prescribing for self-limiting
respiratory tract infections in primary care: Summary of NICEguidance. BMJ 2008; 337:a437.
2. Little P. Delayed Prescribing of antibiotics for upper respiratory tractinfection. With clear guidance to patients and parents it seems to besafe. BMJ 2005; 331: 301-302.
3. Little P, Williamson I, Warner G, Gould C, Gantley M, Kinmonth A L.Open randomised trial of prescribing strategies in managing sorethroat. BMJ 1997; 314:722.
4. Little P, Gould C, Williamson I, Warner G, Gantley M, Kinmonth A L.Reattendance and complications in a randomised trial of prescribing
strategies for sore throat: the medicalising effect of prescribingantibiotics. BMJ 1997; 315:350-352.
5. Spurling G, Del Mar C, Dooley L, Foxlee R. Delayed antibiotics forsymptoms and complications of respiratory infections. CochraneDatabase 2004; 18: CD 004417.
6. Arroll B, Kenealy T, Kerse N. Do delayed prescriptions reduceantibiotic use in respiratory tract infections? A systematic review. Br JGen Pract. 2003; 53: 871-877.
7. Edwards M, Dennison J, Sedgwick P. Patients’ responses to delayedantibiotic prescription for acute upper respiratory tract infections. Br JGen Pract. 2003; 53: 845-850.
8. Fitzpatrick S. The pros and cons of delayed prescriptions. Forum 2007Vol 24 Number 8.
9. Spiro D M et al. Wait-and-see Prescription for the Treatment of AcuteOtitis Media: A Randomized Controlled Trial. JAMA 2006; 296:1235-41.
10. Everitt H A, Little P, Smith P W F. A randomised controlled trial ofmanagement strategies for acute infective conjunctivitis in generalpractice. BMJ 2006; 333:321.
11. Butler C C, Rollnick S, Pill R, Maggs-Rapport F, Stott N.Understanding the culture of prescribing: qualitative study of generalpractitioners’ and patients’ perceptions of antibiotics for sore throats.BMJ 1998; 317: 637-642.
The National Newborn Bloodspot Screening Programme(NNBSP) Process Review 2010P Jennings, M Hegarty, L SmithDepartment of Public Health, HSE Midlands, Area Office, Tullamore, Co Offaly
IntroductionThe National Newborn Bloodspot Screening Programme(NNBSP) in Ireland commenced in 1966 with screening forphenylketonuria (PKU). The programme developed toaccommodate screening for homocystinuria (HCU), classicalgalactosaemia, maple syrup urine disease (MSUD) and congenitalhypothyroidism1. These conditions may result in serious disabilityor premature death if early treatment is delayed. Laboratorytesting is carried out by the National Newborn BloodspotScreening Laboratory (NNBSL) while sample taking occurs inboth hospital and community settings. The birth rate in Ireland hasincreased steadily from 14.4 per 1000 population (53,924) in1999 to 16.7 per 1000 population (73,724) in 20102. Newbornscreening for cystic fibrosis (CF) had been recommended inseveral reports3,4. A multidisciplinary group established by theHSE, including the Cystic Fibrosis Association of Ireland (CFAI),also recommended this ‘as soon as services and infrastructure arein place to meet newly identified need’5.
MethodsA National Steering Group was set up by the HSE in 2009 todesign and oversee the implementation of a Newborn CysticFibrosis Screening Programme which meets the appropriategovernance and quality assurance standards6. The group wished
to ‘review the state of preparedness of the existing NNBSP fromthe perspective of its governance and quality assurance systems,in preparation for the development of the newborn screeningprogramme for cystic fibrosis’. This was achieved by documentingexisting processes in relation to the newborn screeningprogramme, comparing them with the current national guidelinesfor newborn screening and identifying to what extent therecommendations of the two previous reviews7,8 had beenimplemented and identifying gaps.
The review included the NNBSL which coordinated theprogramme nationally and the hospitals, LHO areas anddomiciliary midwives who were involved in providing the newbornscreening service at local level. The NNBSL data were gatheredthrough questionnaire, interview and consultation with the Directorof the NNBSL. A questionnaire was designed for a previousreview4 by identifying several critical points in the system. Thiswas further developed for use in the current review and waspiloted in one hospital and one LHO area. Questionnaires,together with a letter explaining the review, were issued inNovember 2009 to Directors of Nursing and/or Midwifery inmaternity hospitals (20), Directors of Public Health Nursing(DPHN) in LHO areas (32) and Practicing Domiciliary Midwives(16). Data were analysed using SPSS version 17.0.
AbstractThe National Newborn Bloodspot Screening Programme (NNBSP) incorporates screening for several conditions where earlyidentification helps prevent serious disability or mortality. A national group was established (2009) to plan for the inclusion ofscreening for cystic fibrosis (CF); as part of this process a review of the existing NNBSP was undertaken. Information was obtainedthrough consultation with the Director of the National Newborn Bloodspot Screening Laboratory (NNBSL) and survey of maternityunits (20), Local Health Office (LHO) areas (32), and practicing domiciliary midwives (16). Response rate: hospitals 100%; LHOareas 100%; domiciliary midwives 56%. Potential for strengthening quality assurance was identified e.g. single comprehensivescreening register, consistent and timely procedures for checking results. Recommendations, many of which have since beenimplemented, included overall governance structure, liaison officer, quality assurance programme, ring-fenced funding, standardisedunique identifier, dedicated laboratory IT system, secure web-based transmission of results and fail-safe method of tracking samples.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 171
172 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
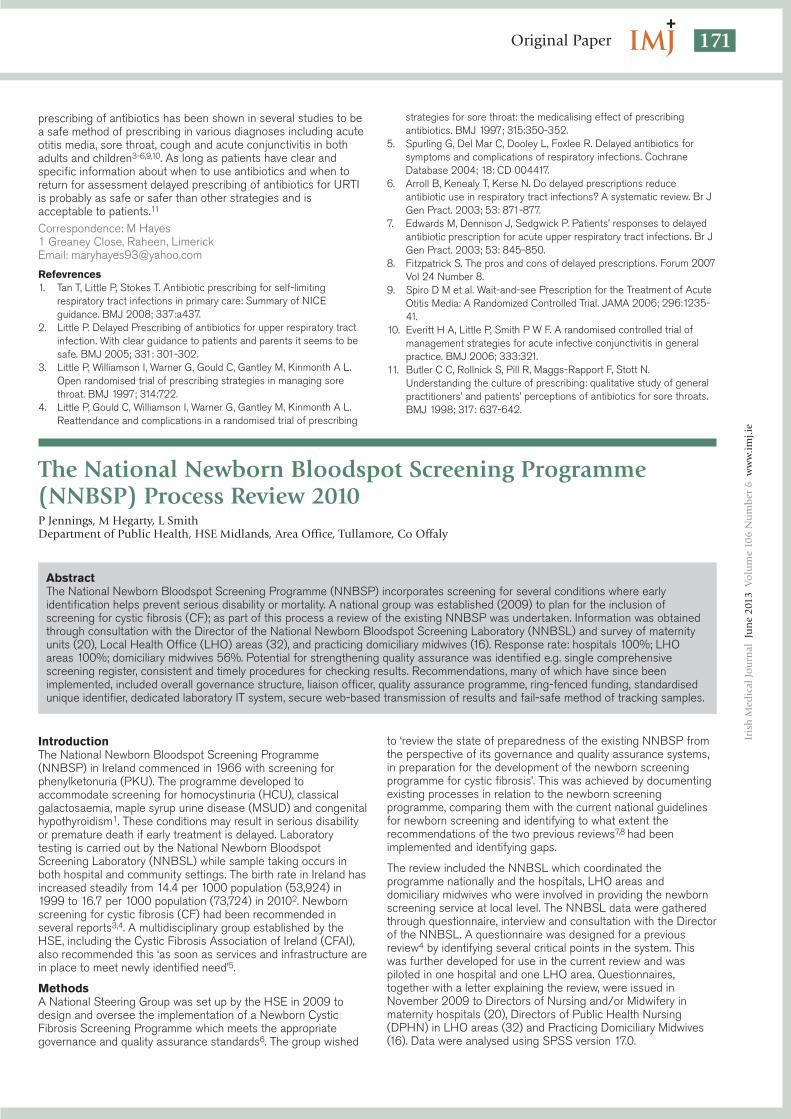
ResultsInformation from the NNBSL was reported by its Director.Response rate (after follow up) was 100% from maternity units/LHO areas and 56% from domiciliary midwives. There wereseveral points along the screening pathway where qualityassurance controls may be strengthened and these are classifiedmainly under governance and tracking (Figure 1).
GovernanceResponsibility for newborn screening in the hospital was held by avariety of management, medical or midwifery personnel whileresponsibility clearly lay with the DPHN in the community. Qualitymanagement initiatives had been implemented by the NNBSL.However there was no overall national quality assurance and auditincluding the non-laboratory elements. The position in relation toavailability of written protocols at local level had improvedconsiderably since the 2004 review7. A need was identified forlocal written protocols to cover recording of information in relationto newborn screening and recording and checking of results.While the NNBSL guidelines were quite specific in this regard,the detailed procedure was not being applied in all areas.
Tracking and documentationAt birth, not all babies are allocated a chart number and the lackof a standardised unique identification number to record on thescreening card of each infant was identified. While there wasgenerally timely notification of the request for screening to theDPHN or to Paediatrics /Special Care Baby Units, there was alack of standardisation of request forms and mode of notification.Practice in terms of recording and checking of screeninginformation varied widely and there was no single comprehensivescreening register. While results of positive tests and repeatrequests were issued in a timely manner, some delays werereported in issue of negative results within the required timeframeprimarily due to staff shortages.
Responsibility for checking recording of results was designated in90% of hospitals and 75% of LHOs. Roughly four fifths ofhospitals and LHO areas checked recording of information relatedto results. Of these, frequency of this check was at least weekly in85% of hospitals and 66% of LHOs. Other findings consistent
with previous reviews included the continued lack of a ClinicalLiaison Officer within the NNBSL, the lack of a defined, ring-fenced budget for the programme and the absence of a failsafemethod of sample tracking in the laboratory.
DiscussionThe Department of Health (DoH) is responsible for policy issuesin relation to the National Newborn Bloodspot ScreeningProgramme (NNBSP). The implementation of a nationallyconsistent screening programme requires a national governancestructure supported by national policy and quality standards. Thisshould ensure that each element of the screening programme isreaching internationally accepted screening criteria on an on-going basis, through audit, monitoring and evaluation. The needfor a defined and ring-fenced budget was identified as in otherreviews7,8 and this recommendation needs to be implemented.
The day-to-day co-ordination of the NNBSP is undertaken by theNNBSL. The Department of Health report9 states that theultimate responsibility for ensuring that all infants are offeredscreening rests with the HSE and maternity units holdresponsibility for ensuring that all children born in hospital areoffered screening. The maternity units are also responsible forensuring that the DPHN is notified of all children dischargedbefore screening has taken place. However, the lack of clarity interms of overall responsibility noted in the 2004 review7 persisted.A senior management lead is required within each of the fourHSE areas with operational responsibility and accountability fornewborn screening. The hospital and LHO leads should have areporting relationship to this individual in relation to the screeningprogramme. Domiciliary midwives hold responsibility for newbornscreening for domiciliary births in accordance with HSE ClinicalGovernance.
Timely sample taking facilitates early diagnosis. According tocurrent guidelines, samples should be collected between 72 hoursand 120 hours from birth. Where babies are discharged fromhospital more than 72 hours after birth the sample taking andrecording is completed in the hospital. Where this time span isless than 72 hours, the hospital advises the DPHN that sampletaking and recording needs to be completed in the community.Discharges in this category have almost doubled over the past 10years and reached 53% of births in 201010. Not all babies areallocated a chart number so it is essential to generate astandardised unique ID for each infant. A comprehensive, singlescreening register is essential to facilitate uniform recording ofsample taking in all areas, timely identification of missed babies,and programme audit. The request for screening to DPHN andpaediatric or special care baby units requires standardisedelectronic notification. The lack of a failsafe method of sampletracking within the laboratory identified in 20078 continues topresent a clinical risk to the programme. A dedicated laboratoryscreening IT system is required to enable specimen identificationthroughout the laboratory process.
The co-ordination of the clinical pathway for the positive infant ismanaged effectively by the Director of the NNBSL. This includesorganising appropriate referral of the screened positive baby tothe clinical services. However, at local level, responsibility forchecking to ensure a result is returned for every infant is notstandardised. While there are some excellent practices andprocedures in place, this needs to be comprehensive in allhospitals and LHO areas. Secure web-based transmission of allresults is required to ensure timely return of results. This coupledwith timely and standardised checking of results is essential toavoid implications for a baby who is not screened or for whom thesample is mislaid. Real time issuing of results should be thetarget. A high quality screening programme is required to ensurethat it does more good than harm. The PAC review7
recommended annual audit of the national newborn screeningprogramme together with establishment of a national IT system tofacilitate it.
Figure 1 Flowchart and Critical Points for NNBSP in the Republic of Ireland
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 172

173Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
A number of quality management measures have beenimplemented by the NNBSL and it is accredited by ClinicalPathology Accreditation, UK. The NNBSL regularly undertakesaudit as part of the quality management system. However, audit ofthe non-laboratory aspects of the programme to date is a veryrare occurrence, not surprisingly given the various methods ofrecording and storing data and the lack of IT systems to facilitateit. For routine audit of the screening programme it is importantthat key performance indicators are accessible in an efficientmanner. The NNBSL has standard operating procedures for alllaboratory testing procedures and reporting. The NNBSL alsoprovides and regularly updates guidelines for screening for use bystaff in hospitals, LHO areas and domiciliary midwives.Considerable work has been undertaken in several hospital andLHO areas in relation to developing protocols. Some of these, inconjunction with national guidelines1, could be used to provide abasic national protocol with provision for amendments byindividual hospital or LHO areas to accommodate specific localissues. This would provide a national standard which wouldfacilitate future audit of the programme.
This review aimed to describe the process of newborn screeningin the various settings rather than to audit practice in this area. Itis subject to the usual limitations of self-reported data. Howeverthe maximum response rate achieved in hospitals and LHO areasis a major strength. The lack of a national standardised processdid create difficulties, particularly in relation to the wide variety ofprocedures for recording data and checking results. Since thereview was undertaken the findings were progressed by theNational Steering Group for Cystic Fibrosis Screening. Thestructures for the governance and management of the NNBSPhave been agreed and are specified in NNBSL (2011)11. Systemstandards and targets have been developed for programmeperformance assessment. Pending availability of a unique HSEidentifier (expected 2013) an interim Unique Perinatal Identifier(UPI) is being issued to all babies born. This is formed by theHospital HIPE code of the birth hospital followed by theHealthcare Record Number of the baby. Babies who are not bornin Irish hospitals are issued with an identification number by theDPHN in the area in which their birth is registered. Advanceshave been made in relation to provision of a single screeningregister through modification of the existing immunisationsregisters and child health IT systems. A dedicated laboratory ITsystem is being developed. This will provide failsafe tracking,transmission of results and will have capability to interface withHSE systems. A liaison person has been appointed to thelaboratory. These developments will help to enhance the quality ofthe NNBSP.
Correspondence: P JenningsDepartment of Public Health, HSE Midlands, Area Office,Tullamore, Co OffalyEmail: [email protected]
AcknowledgementsP Mayne, Director NNBSL; the directors of public health nursingand of nursing/midwifery together with their staff who contributedto this review; the Newborn Screening for Cystic Fibrosis NationalSteering Group, the staff of the Department of Public Health,HSE, Tullamore including A McNamara, I Kelly and C Brennan; TGreally, Department of Public Health Limerick and all those whoprovided comment on various drafts or otherwise contributed tothis review.
References1. National Newborn Screening Laboratory. A practical guide to newborn
screening in Ireland. 4th edition, National Newborn ScreeningLaboratory, Children’s University Hospital, Temple St., Dublin 1. (2009)www.nnsp.ie.
2. Central Statistics Office. Vital Statistics Fourth Quarter and YearlySummary 2010.www.cso.ie/releasespublications/othercsopublications/statisticalyearbookof ireland2011edition/. Accessed 12.09 12.
3. Working group on Newborn Cystic Fibrosis. 2000 The Interim Reportof the working Group on Newborn Cystic fibrosis Screening. 2000.
4. Programme of Action for Children. Implementation of Newborn CysticFibrosis Screening in the Republic of Ireland. The Newborn CysticFibrosis Screening Working Group. (2004).
5. Pollock, R. Blueprint for the Future. Treatment of Cystic Fibrosis inIreland: Problems and Solutions 2005. (2005).www.cfireland.ie/articles.php/publications/_information__bookletsAccessed April 8th 2010.
6. Health Service Executive. Project Plan for Implementation of NewbornScreening for Cystic Fibrosis Programme. Cystic Fibrosis ScreeningSteering Group, HSE. 2009.
7. Programme of Action for Children Review of the National ScreeningProgramme for Inherited Metabolic Disorders. Dublin: The HealthBoards Executive. (2004).
8. Green, A. Report of External Review of the National NewbornScreening Laboratory. (2007).
9. Department of Health. Report of the Metabolic Disorders WorkingGroup. Dublin. 1993.
10. Economic and Social Research Institute. Perinatal Statistics Report2010. http://www.esri.ie/health_information/nprs/nprs_reports/accessed 13/09/2012.
11. National Newborn Bloodspot Screening Laboratory .A practical guideto newborn screening in Ireland. 5th edition,: National NewbornBloodspot Screening Laboratory, Children’s University Hospital,Temple St., Dublin 1. 2011 www.nnbsp.ie
A Profile of Elderly Fallers Referred for Physiotherapy in theEmergency Department of a Dublin Teaching HospitalF Crehan1, D O’Shea2, JM Ryan1, F Horgan2
1St Vincent’s University Hospital, Elm Park, Dublin 42School of Physiotherapy, RCSI, 123 St Stephen’s Green, Dublin 2
AbstractIreland has an ageing population and the elderly are over-represented in Emergency Departments (ED) - a quarter of thesepresentations resulting from falls. A prospective study design was employed using a convenience sample to profile elderly fallersreferred for physiotherapy in ED. Forty-subjects were assessed over 14 weeks. Mean age was 84.88 years (s.d. 7.3) and 31 (77.5%)were female. All demonstrated slow walking speed and 26 (65%) demonstrated poor grip strength. A quarter of subjects reportedfear of falling and 30 (75%) were classified as frail. Elderly fallers in ED are a frail group of socially vulnerable patients whodemonstrate a risk of further falls. Osteoporosis had been diagnosed in 9 (22.5%) subjects – a low prevalence compared withinternational research, but 25 (62.5%) subjects had never had a DEXA scan. The prevalence of frailty in the sample of elderly fallersin this study was very high (75%).
To receive CPD credits, you must completethe questions online at www.imj.ie.
CPD available online at www.imj.ie and questions on page 191
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 173

174 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
IntroductionIreland like many other countries has seen a steady increase inlife expectancy and has an ageing population1. A recent studydemonstrated that 11% of the Irish population were aged 65 orolder and 2.7% were over 80 years of age2. There will be aprojected 44% increase in the number of people over 65 in thenext ten years. The greatest increase will occur in the over 80population with the number in this group expected to doublebetween 2011 and 20313. A better understanding of healthcareneed and utilisation of services among the elderly Irish populationis essential for policy planning3.
A fall has been defined as “inadvertently coming to rest on theground, floor or other lower level, excluding intentional change inposition to rest in furniture, wall or other objects”4. Theconsequences of falls in the elderly population can be severe andinclude hospitalisation, nursing home placement, and changes inhealth status, social isolation and increases in morbidity andmortality5. Falls are common in the community dwelling elderlypopulation with 30% of this cohort falling in a one-year period6. In2008, the Health Service Executive (HSE) reported that 50% ofpeople who are 80 years or more fall each year7. It has beenreported that older people are over-represented in EmergencyDepartments (ED) in Ireland and 17% of all ED presentations areaccounted for by the over 65 year old age group7. Fallers accountfor up to a quarter of this population8 and so the management offallers in ED is an important issue. The ED offers healthcareprofessionals an excellent opportunity to identify elderly fallersand those at risk of falls. The aim of this study was to describe theprofile of community dwelling adults over 65, who were referredfor physiotherapy in the Emergency Department (ED) of a DublinTeaching Hospital after a fall.
MethodsSt Vincent’s University Hospital is one of the Dublin AcademicTeaching Hospitals with 479 in-patient beds. There is a 24-hourED catering for patients over the age of 14. A prospective,observational study design was used in the ED of St Vincent’sUniversity Hospital, Dublin. Inclusion and exclusion criteria weredeveloped by liaising with the senior physiotherapist,physiotherapy manager, research supervisor, Clinical NurseSpecialist (CNS) and consultants in the relevant area. Patientsover 65 who had been referred for physiotherapy in the ED after afall as defined by WHO4 were included and the SeniorPhysiotherapist in ED, who acted as a gatekeeper, identifiedpotential subjects. Patients with an Abbreviated Mental Test Score(AMTS) of below 6 were excluded. St Vincent’s Research EthicsCommittee granted ethical approval.
Subjects were interviewed about fall details, falls history, fracturehistory, osteoporosis, visual impairment, footwear, assistivedevices, previous physiotherapy involvement, fear of falling,steadiness, environment, markers of frailty and urinaryincontinence. Demographic data and history were establishedfrom the medical charts. The Timed Up and Go (TUG) test9 wasassessed as a measure of gait speed and falls risk and gripstrength was assessed using a Jamar dynamometer. The validityand reliability of these outcome measures have been describedpreviously9,10. During the TUG, subjects were asked to rise from achair of 46cm with armrests11 walk 3m and return to chair, at theirnormal gait speed using usual gait aid and footwear. Activity wastimed and compared to age and gender normative values12.
ResultsDemographic ProfileThere were 40 subjects recruited over a 14-week period with anage range from 67 to 99 and a mean age of 84.88 (s.d. 7.3)years. During that period a further 8 elderly fallers had left thedepartment before assessment, 4 patients were excluded due toa diagnosis of collapse rather than fall. Three patients wereexcluded due to poor cognition and 3 refused to participate. Themajority of subjects were female and only 9 (22.5%) subjects
were male. Many of the participants lived alone (72.5%) and halfused a frame to mobilise. There were 9 (22.5%) subjects who hadbeen diagnosed with osteoporosis but only 15 (37.5%) had everhad a DEXA scan. Of the elderly fallers who were referred tophysiotherapy service in ED, over three quarters (77.5%) wereadmitted to hospital. Only four subjects (10%) were dischargedhome from ED. Nearly one third (37.5%) of this population denieda previous fall. Only 3 (7.5%) of the subjects did not use a mobilityaid and over half used a frame to mobilise. However, only 9(22.5%) subjects reported that a physiotherapist had providedtheir mobility aid. The same percentage reported that family hadprovided the mobility aid.
Details of FallsThe most frequent location of the falls was indoors as 33 of thesubjects (82.5%) fell indoors. The majority of subjects (65%)sustained an injury after the fall. The most common injury wasbruising (12.5%) followed by Colles fracture and pelvic fracture(10%). Head lacerations (7.5%) and humeral fractures (7.5%) werealso prevalent. Over 40% of the falls happened between 10amand 12 noon and only 20% of falls happened between the hoursof 10pm and 6am. Slippers were the most frequent footwear wornat the time of fall (35%) followed by walking shoes (30%). Therewere 5% of subjects who were barefoot at the time of fall and afurther 5% who were wearing only socks.
Falls Risk ProfileThere were thirteen risk factors for falls included in this study.Study subjects displayed 8-12 of these risk factors and the meanwas 8 risk factors (s.d. 1.9). There were 10 (25%) subjects whoreported fear of falling. Of these subjects, seven acknowledgedthat they restricted their activity. A summary of prevalence of fallsrisk is summarised in Table 1.
FrailtyFrailty was assessed based onFried’s classification13. Gripstrength data was analysed forsubjects’ dominant upper limband compared to normativedata14. For four subjects,dominant upper limb gripstrength could not beassessed due to radialfracture, humeral fracture or severe gout. In these cases the non-dominant reading was analysed. There was 65% of the populationthat had grip strength below normal values for their age andgender15. A high percentage of subjects (37.5%) were unable tocomplete the TUG test as they required assistance to stand fromchair or assistance to mobilise. Of those who did complete theTUG, the mean time taken to complete the test was 45.95 (s.d.34.081) seconds ranging from 15 to 140 seconds. All of thesubjects required longer to complete the TUG than aged matched
Table 1 Prevalence of Falls Risk Factors
N=40 Number (%)
TUG speed below normal 40 (100)
Dependant on mobility aid 37 (92.5)
Polypharmacy 31 (77.5)
Stairs at home 30 (75)
Living alone 29 (72.5)
CNS Meds 28 (70)
Grip Strength below normal 26 (65)
Previous falls 25 (62.5)
Visual deficit 23 (57.5)
Urinary Incontinence 22 (55)
Recent change in activity levels 22 (55)
Fear of falling 10 (25)
No bedside light 4 (10)
Table 2 Frequency of Markers ofFrailty
N=40 Number(%)
Slow Walking Speed 40 (100)
Decreased Grip Strength 26 (65)
Self-reported Exhaustion 22 (55)
Inactivity 21 (52.5)
Un-intentional Weight Loss 14 (35)
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 174

175Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
controlled community dwelling adults13. A summary of thefrequency of markers of frailty is shown in Table 2. All of thesubjects displayed slow walking speed, the majority displayedweak grip strength (65%) but just over a third (35%) reported un-intentional weight loss.
Thirty (75%) of the subjects in this study were classified as frailbased on Fried’s classification13. It was calculated that the meannumber of markers displayed was 3 (s.d. 1.2). Two of the subjectsdid not display any markers of frailty but three displayed all fivemarkers. There were 4 (10%) subjects who were classified asnon-frail and 6 (15%) who were classified as pre-frail. Anindependent t-test found that there was no difference in numberof falls in the preceding year between those who were classifiedas frail or not frail (t=-0.244, df=38, p=0.809).
DiscussionComparison with previous studies shows that elderly fallersreferred for physiotherapy in ED were older, and more sociallyvulnerable than the general ED elderly population in the samesetting. Previous studies have reported mean age of elderly EDpresentations to be 75.8 years16 or 76.35 years8. It has beenfound that fallers in ED were significantly older (mean age of 79years) than non-fallers17. Further study would be required toestablish if elderly fallers referred for physiotherapy in ED areolder than the fallers who are not referred for physiotherapy.
The frequency of living alone for elderly patients who present toED was previously shown to be 42%8. However 72.5% ofsubjects in this study lived alone indicating that fallers referred forphysiotherapy in ED are a group of socially vulnerable elderly.There were 22.5% of the subjects in this study who had beendiagnosed with osteoporosis. However research has shown that40-50% of women and 25% of men are likely to developosteoporosis16 suggesting that osteoporosis may be under-diagnosed in this population. Only 7.5% of the subjects in thisstudy were independently mobile and half used a frame. Of thosewho had a mobility aid, only 22.5% reported getting it from aphysiotherapist and the same percentage reported that a familymember had provided the mobility aid. This suggests that theremay be an unmet need for this group of subjects who may neverhad any intervention by a physiotherapist despite a decline inmobility. Further study in this area seems warranted.
The profile of the subjects in this study is of a frail group. Threequarters were classified as frail according to Fried’s classificationsystem and in total 90% were classified as frail or pre-frail.Previous studies have documented a frailty prevalence of 6.9% inthe community dwelling elderly8. Therefore, the prevalence offrailty in the population of elderly fallers referred for physiotherapyin ED is higher than in community dwelling elderly population18.There were 65% of this study cohort who displayed decreasedgrip strength than age and gender matched controls, andtherefore were more at risk of disability and mortality19. A highpercentage of subjects were unable to complete TUG. Previousresearch has advised that inability to complete the TUG is morepredictive of falls than slow walking speed20. All of the subjectswho were able to complete the TUG, required more time to do sothan age and gender matched controls. This portrays the studypopulation as having gait and balance limitations. Interpretation ofthis must be limited as the TUG was carried out after the subjectshad presented to ED after a fall and had various injuries.
In conclusion, elderly fallers presenting to the ED were older, frailand socially vulnerable adults who are likely to require admissionto hospital. The resource implications of this are significant at themoment and are likely to increase given the ageing population.Previous studies have documented a frailty prevalence of 6.9% inthe community dwelling elderly8. The prevalence of frailty in thesample of elderly fallers in this study was very high (75%). Thesepatients displayed risks of further falls with slow TUG speed or aninability to complete the TUG. Polypharmacy and decreased grip
strength were also common. Slippers were the most frequent formof footwear worn at the time of falling. The prevalence ofOsteoporosis in this group was low compared with internationalresearch, but the majority of subjects had never had a DEXAscan. A future study could include all fallers attending the ED todescribe their demographic and frailty profile, and to determinetheir needs with regard to management and follow-up services.
Correspondence: F CrehanSt Vincent’s University Hospital, Elm Park, Dublin 4Email: [email protected]
AcknowledgementsThe staff and patients of St Vincent’s University Hospital
References1. Banerjee A, Mbamalu D, Ebrahimi S, Khan AA, Foo Chan, T (2011)
The prevalence of polypharmacy in elderly attenders to an emergencydepartment-a problem with a need for an effective solutionInternational Journal of Emergency Medicine 4.
2. Naughton C, Drennan J, Treacy P, Fealy G, Kilkenny M (2010) The roleof health and non-health related factors in repeat emergencydepartment visits in an elderly urban population Emergency MedicineJournal 27;683-7.
3. TILDA (2011) Fifty plus in Ireland 2011- First results from the IrishLongitudinal Study on Ageing (TILDA)http://www.tcd.ie/tilda/events/first%20wave%20results/Tilda_Master_First_Findings_Report.pdf (accessed 4th June 2011).
4. World Health Organisation - WHO (2007) Global Report on FallsPrevention in Older Agehttp://www.who.int/ageing/publications/Falls_prevention7March.pdf(accessed 15 Jan 2011).
5. Davis AJ, Kenny RA (1996) Falls Presenting to the Accident andEmergency Department: Types of Presentation and Risk FactorProfile Age and Ageing 25;362-6.
6. Tinetti ME, Speechely M, Ginter SF (1988) Risk factors for fallsamong elderly persons living in the community New England Journalof Medicine 29:319:1701-7.
7. HSE (2008) Report of the National Steering Group on the Preventionof falls in Older People and the Prevention and Management ofOsteoporosis throughout lifehttp://www.hse.ie/eng/services/Publications/services/Older/Strategy_to_Prevent_Falls_and_Fractures_in_Ireland%E2%80%99s_Ageing_Population_-_Full_report.pdf (accessed 5th April 2011).
8. Fealy GM, Treacy M, Drennan J, Naughton C, Butler M, Lyons I (2011)A profile of older emergency department attendees: findings from anIrish study Journal of Advanced Nursing 00(0), 000–000. doi:10.1111/ j.1365-2648.2011.05800.x.
9. Podsiadlo D, Richardson S (1991) The Timed “Up and Go”: a test ofbasic functional mobility for frail elderly persons Journal of AmericanGeriatrics Society 39:142-8.
10. Coldham F, Lewis J, Lee H, (2006) The Reliability of One vs ThreeGrip Trials in Symptomatic and Asymptomatic Subjects Journal ofHand Therapy 19:318-27.
11. Siggeirsdottir K, Jonsson BY, Jonsson H Jr, Iwarsson S (2001) Thetimed ‘Up and Go’ is dependent on chair type Clinical Rehabilitation16:609-16.
12. Bohannon R (2006) References Values for the Timed Up and GoTest: A Descriptive Meta-Analysis Journal of Geriatric PhysicalTherapy 29:64-8.
13. Fried LP, Tangen CM, Walston J, Newman AB, Hirsh C, Gottidiener J,Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA (2001) Frailty inolder adults: evidence for a phenotype Journal of Gerontology SeriesA: Biological Sciences and Medical Sciences 56:M146-56.
14. Bohannon RW, Peolsson An, Massy-Westropp, Desrosiers J, Baer-Lehman J (2006) Reference values for adult grip strength measuredwith a Jamar dynamometer: a descriptive meta-analysis Physiotherapy92:11-15.
15. Bohannon R (2006) References Values for the Timed Up and GoTest: A Descriptive Meta-Analysis Journal of Geriatric PhysicalTherapy 29:64-8.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 175
176 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
16. Kenny RA, de Siun A (2006) Older People Attending the ED with aFall or Blackout: A pilot study Technical report 6 to HSE (2008)http://www.lenus.ie/hse/handle/10147/76639 (accessed 14th June2011).
17. Naughton C, Mc Grath E, Drennan J, Johnson F, Lyons I, Treacy P,Fealy G, Butler M (2011) The profile and follow-up of patients whoattend the Emergency Department following a fall InternationalEmergency Nursing doi:10.1016/j.ienj.2011.07.005.
18. Kanis JA, Johnell O, Oden A, Sembo I, Redlund-Johnell I, Dawson A,De Laet C, Jonsson B (2000) Longterm risk of osteoporotic fracturein Malmo Osteoporosis Int 11:669-74.
19. Bohannon RW (2008) Hand-grip dynamometry predicts futureoutcomes in aging adults Journal of Geriatric Physical Therapy31:3-10.
20. Large J, Gan N, Basic D, Jennings N (2006) Using the Timed Up andGo Test to stratify elderly inpatients at risk of falls ClinicalRehabilitation 20:421-28.
Presentation and Management of Gastrointestinal StromalTumoursAM Mongan, V Malik, S Rowley, Z Claxton, C Muldoon, D O’Toole, N Ravi, JV ReynoldsDepartment of Surgery, St James’s Hospital, James’s St, Dublin 8
IntroductionGastrointestinal stromal tumours (GISTs) represent the mostcommon mesenchymal neoplasm of the digestive tract.1Previously thought to arise from smooth muscle, GISTs wereclassified as leiomyomas, leiomyosarcomas or schwannomas.2Mesenchymal neoplasms of the gastrointestinal tract with aphenotype ranging from indeterminate to minimally orincompletely myogenic or neural, are now termed GISTs. GISTsare associated with the interstitial cell of Cajal (ICC), and mayoriginate from multipotential mesenchymal stem cells.3 Most(>90%) express the proto-oncogene CD117 (KIT), a growthfactor receptor with tyrosine kinase activity. Immunophenotypicmarkers such as CD34, DOG-1, SMA, Desmin, S-100 and h-caldesmon demonstrate more variable expression.4Morphologically, GISTs may be subdivided into spindle, epithelioidor mixed type.5
Clinically significant GISTs are relatively rare (incidence1.5/100,000/year), but microscopic undiagnosed GISTs are farmore common.6 Peak age of diagnosis is 60 years.7 GISTs maydevelop anywhere along the GI tract, but most arise in thestomach (70%).8 Surgery represents the only chance for cure.Five-year survival after surgical resection ranges from 19%-75%.1,7,9-11 Minimally invasive approaches are increasinglyemployed, particularly for small(<5cm) lesions.12 Prognosis isdetermined by the US National Institutes of Health (NIH)consensus criteria based on tumour size and mitotic index.5 Theemergence of tyrosine kinase inhibitors(TKI) has revolutionizedthe treatment of advanced and recurrent GIST. This study aims toreview the changing presentation, management and outcomesassociated with GIST in a single institution.
MethodsA retrospective analysis of all patients diagnosed with GIST in ahigh volume, upper gastrointestinal tertiary referral centre from1997-2011 was performed. Tumours were reviewed bypathologists for confirmation of GIST nature. Clinical andhistological data were retrieved from a prospectively maintainedGIST database. The study included patients presenting withprimary GIST and those diagnosed with an incidental GIST whileundergoing investigation or treatment for a synchronous tumour.
Both primary and incidental GISTs were included in allsubsequent analysis except survival analysis. Survival analysis wasconducted on primary GISTs only. Univariate analysis wasperformed using Mann-Whitney U test (nonparametric continuousdata) and Fisher test (categorical variables). All statistical testswere two-sided, with the threshold of significance set at p<0.05.Kaplan-Meier survival curves were plotted. Survival differenceswere determined using the log-rank test.
ResultsPatient Characteristics78 consecutive patients (36 male/42 female) with a median ageof 66 (range 10-93) were diagnosed with GIST at this unitbetween 1997 and 2011. Gastrointestinal bleeding was the mostcommon presenting complaint (28%) (Table 1). GIST was anincidental diagnosis in 17 patients (22%) undergoing investigationand treatment for synchronous gastrointestinal cancers, mostbeing oesophageal adenocarcinoma (82%). One patient wasdiagnosed with gastric adenocarcinoma and two with colorectalcancer. Endoscopy was the most frequently used method todiagnose GIST in the 61 patients with primary GIST (100% gastricGIST, 45% non-gastric GIST). Staging CT scans were performedin 60 patients (98%), PET in 18 patients (26%). Endoscopicultrasound (EUS) was performed in 18 of the 50 patients withprimary gastric GIST, of whom eight underwent FNA. FNArevealed malignant cells in five of these cases (63%).
Tumour CharacteristicsMost GISTs were located in the stomach (n=60, 77%), the fundusbeing the most frequent gastric site (Table 1). Tumour size rangedfrom 0.1-20 cm (median 5.0cm). Mucosal ulceration was noted in12 specimens (15%) and tumour necrosis in 22 samples (28%).Median (range) mitotic rate was 2 (0-100) per 50 High PowerField (HPF). Most specimens (92%) were CD117 positive byimmunohistochemistry, CD34 was positive in 72% of cases.Infrequent mutations included DOG-1 (28%), SMA (6%),Vimentin (8%), S-100 (5%), Desmin(3%) and Actin (4%). Themost common histological subtype was spindle cell carcinoma(65%), followed by mixed epithelioid/spindle cell, (15%) andepithelioid cell (13%).
AbstractGastrointestinal stromal tumour (GIST) is the most common mesenchymal tumour of the gastrointestinal tract. The aim of this studywas to present the experience of a single centre. A prospective GIST database from 1997 to 2011 in a tertiary referral centre wasreviewed. 78 patients (36 male/42 female) with a median age of 66 (range 10-93) were diagnosed with GIST during this period.Surgery was the primary treatment for 70 patients (90%); 19 (24%) resections were laparoscopic. Nineteen patients (24%) receivedImatinib therapy. At a median follow up of 3 years, 10 patients (15%) had recurrence. Five-year survival was 89%. Surgery remainsthe mainstay of treatment. Minimally invasive approaches may be carried out with high cure rates. This study highlights the changingpresentation and treatment approach, as well as the excellent outcomes achievable for GIST tumours.
To receive CPD credits, you must completethe questions online at www.imj.ie.
CPD available online at www.imj.ie and questions on page 191
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 176
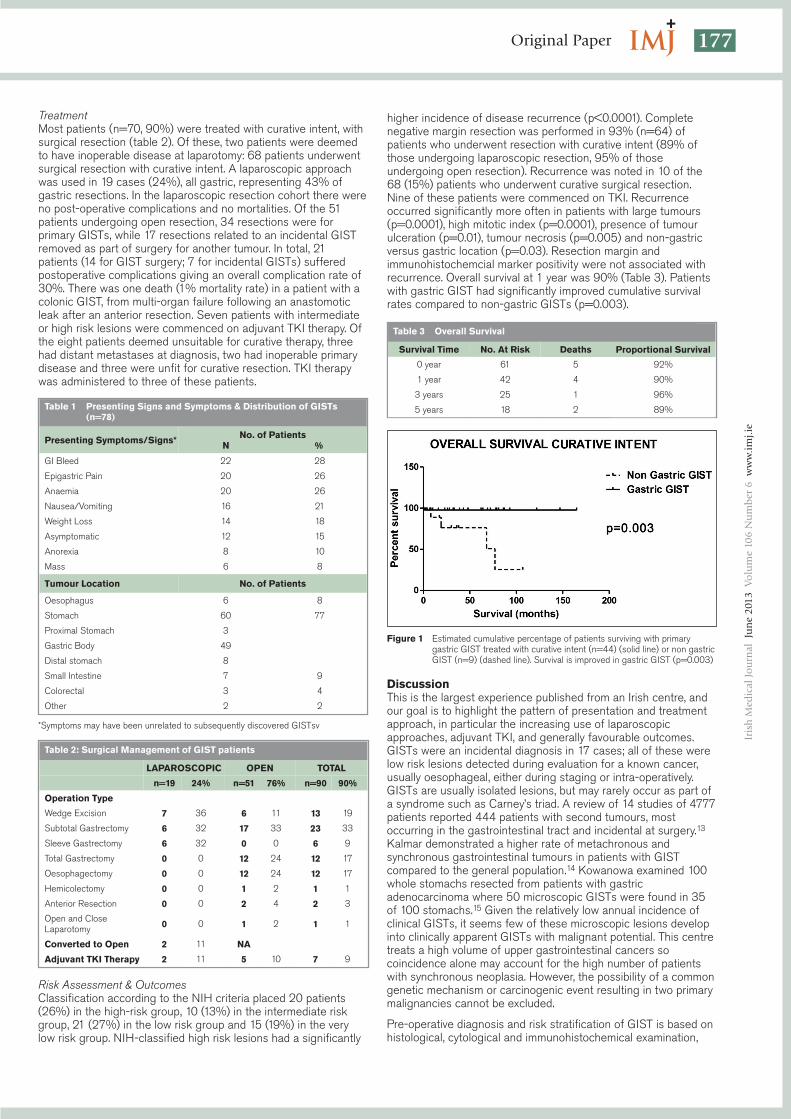
177Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
TreatmentMost patients (n=70, 90%) were treated with curative intent, withsurgical resection (table 2). Of these, two patients were deemedto have inoperable disease at laparotomy: 68 patients underwentsurgical resection with curative intent. A laparoscopic approachwas used in 19 cases (24%), all gastric, representing 43% ofgastric resections. In the laparoscopic resection cohort there wereno post-operative complications and no mortalities. Of the 51patients undergoing open resection, 34 resections were forprimary GISTs, while 17 resections related to an incidental GISTremoved as part of surgery for another tumour. In total, 21patients (14 for GIST surgery; 7 for incidental GISTs) sufferedpostoperative complications giving an overall complication rate of30%. There was one death (1% mortality rate) in a patient with acolonic GIST, from multi-organ failure following an anastomoticleak after an anterior resection. Seven patients with intermediateor high risk lesions were commenced on adjuvant TKI therapy. Ofthe eight patients deemed unsuitable for curative therapy, threehad distant metastases at diagnosis, two had inoperable primarydisease and three were unfit for curative resection. TKI therapywas administered to three of these patients.
Risk Assessment & OutcomesClassification according to the NIH criteria placed 20 patients(26%) in the high-risk group, 10 (13%) in the intermediate riskgroup, 21 (27%) in the low risk group and 15 (19%) in the verylow risk group. NIH-classified high risk lesions had a significantly
higher incidence of disease recurrence (p<0.0001). Completenegative margin resection was performed in 93% (n=64) ofpatients who underwent resection with curative intent (89% ofthose undergoing laparoscopic resection, 95% of thoseundergoing open resection). Recurrence was noted in 10 of the68 (15%) patients who underwent curative surgical resection.Nine of these patients were commenced on TKI. Recurrenceoccurred significantly more often in patients with large tumours(p=0.0001), high mitotic index (p=0.0001), presence of tumourulceration (p=0.01), tumour necrosis (p=0.005) and non-gastricversus gastric location (p=0.03). Resection margin andimmunohistochemcial marker positivity were not associated withrecurrence. Overall survival at 1 year was 90% (Table 3). Patientswith gastric GIST had significantly improved cumulative survivalrates compared to non-gastric GISTs (p=0.003).
DiscussionThis is the largest experience published from an Irish centre, andour goal is to highlight the pattern of presentation and treatmentapproach, in particular the increasing use of laparoscopicapproaches, adjuvant TKI, and generally favourable outcomes.GISTs were an incidental diagnosis in 17 cases; all of these werelow risk lesions detected during evaluation for a known cancer,usually oesophageal, either during staging or intra-operatively.GISTs are usually isolated lesions, but may rarely occur as part ofa syndrome such as Carney’s triad. A review of 14 studies of 4777patients reported 444 patients with second tumours, mostoccurring in the gastrointestinal tract and incidental at surgery.13
Kalmar demonstrated a higher rate of metachronous andsynchronous gastrointestinal tumours in patients with GISTcompared to the general population.14 Kowanowa examined 100whole stomachs resected from patients with gastricadenocarcinoma where 50 microscopic GISTs were found in 35of 100 stomachs.15 Given the relatively low annual incidence ofclinical GISTs, it seems few of these microscopic lesions developinto clinically apparent GISTs with malignant potential. This centretreats a high volume of upper gastrointestinal cancers socoincidence alone may account for the high number of patientswith synchronous neoplasia. However, the possibility of a commongenetic mechanism or carcinogenic event resulting in two primarymalignancies cannot be excluded.
Pre-operative diagnosis and risk stratification of GIST is based onhistological, cytological and immunohistochemical examination,
Figure 1 Estimated cumulative percentage of patients surviving with primarygastric GIST treated with curative intent (n=44) (solid line) or non gastricGIST (n=9) (dashed line). Survival is improved in gastric GIST (p=0.003)
Table 1 Presenting Signs and Symptoms & Distribution of GISTs(n=78)
Presenting Symptoms/Signs* No. of PatientsN %
GI Bleed 22 28
Epigastric Pain 20 26
Anaemia 20 26
Nausea/Vomiting 16 21
Weight Loss 14 18
Asymptomatic 12 15
Anorexia 8 10
Mass 6 8
Tumour Location No. of Patients
Oesophagus 6 8
Stomach 60 77
Proximal Stomach 3
Gastric Body 49
Distal stomach 8
Small Intestine 7 9
Colorectal 3 4
Other 2 2
*Symptoms may have been unrelated to subsequently discovered GISTsv
Table 2: Surgical Management of GIST patients
LAPAROSCOPIC OPEN TOTAL
n=19 24% n=51 76% n=90 90%
Operation Type
Wedge Excision 7 36 6 11 13 19
Subtotal Gastrectomy 6 32 17 33 23 33
Sleeve Gastrectomy 6 32 0 0 6 9
Total Gastrectomy 0 0 12 24 12 17
Oesophagectomy 0 0 12 24 12 17
Hemicolectomy 0 0 1 2 1 1
Anterior Resection 0 0 2 4 2 3
Open and CloseLaparotomy 0 0 1 2 1 1
Converted to Open 2 11 NA
Adjuvant TKI Therapy 2 11 5 10 7 9
Table 3 Overall Survival
Survival Time No. At Risk Deaths Proportional Survival
0 year 61 5 92%
1 year 42 4 90%
3 years 25 1 96%
5 years 18 2 89%
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 177

178 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
typically from endoscopic biopsy. GIST appears as a submucosalmass at endoscopy and a definitive diagnosis based solely onendoscopic biopsy may be difficult to establish. Thus, anincreasing role for EUS in identifying GISTs has emerged, andFNA under EUS guidance is used to provide a tissue diagnosis.However, EUS-FNA is unsuitable for sites where it is difficult topuncture the tumour (gastric cardia or small intestine). In addition,GISTs may contain areas with different cellularity and necrosisand an accurate assessment of mitotic activity cannot bedetermined. EUS-FNA has significant limitations but remains auseful investigation, particularly in patients for whom previousendoscopic biopsy was unsuccessful in establishing a diagnosis.Gastric GISTs tend to have a more favourable clinical course thannon-gastric GISTs of comparable size.8 This is reflected in thenewer risk classification systems of Miettinen and Lasota whichinclude tumour site as a prognostic variable. Our cohort of gastricGISTs of size 2-10cm had lower rates of recurrence compared tonon-gastric GISTs of the same size (3% versus 38%, p=0.02).
Most patients were treated with curative intent (90%), perhapsreflecting referral bias to this specialist centre. Surgery remainsthe only curative treatment for primary localized GIST. Organ-preserving wedge excision was the most frequently performedoperation. The aim of surgery is to achieve complete resectionwith gross negative margins, consistent with standard surgicaloncological principles although a consensus conference on GISTstated that positive microscopic margins or R1 do not compromisesurvival.12 This is refuted in other studies.16,17 We advocate a goalof negative margins, but there is no data to justify extensivemargins, and a microscopically involved margin does not demandfurther surgery.
Lymph involvement is rare, and lymphadenectomy unwarranted.7Most GISTs are located in the stomach with an exophytic growthpattern, making them technically very accessible. Given thesefeatures, a laparoscopic approach to GIST resection appearsappealing. However, the role of laparoscopy is not completelyclear. The 2007 National Comprehensive Cancer Network(NCCN) task force recommended that laparoscopic techniquesmay be used for tumours up to 5cm in size.12 Novitsky et alstudied long-term outcomes of resected gastric GISTs up to8.5cm in size, demonstrating three-year disease-free survival of92% in their series of 50 laparoscopic resections.18 Similarly, ourcohort of 19 laparoscopic resections had excellent results with nopost-operative complications, deaths or recurrences after amedian follow-up of two years. Median tumour size in this cohortwas 3.0 cm (range 1.9-6.0 cm). All laparoscopic resections wereperformed in the latter half of the study period.
Most recurrences occur within two years but late (>5 years)recurrences have been described, so long term follow-up isimportant.19 Median time to recurrence in our cohort was 29months (range 1-45 months). Five-year survival may be as high as92% for low risk GISTs, while for high risk GISTs the 5-yearsurvival rate is less than 30%.20,21 The overall 5-year survival inour series was 89%. Most patients who developed recurrentdisease in our cohort were treated with TKI (90%). At a medianfollow-up of 54 months seven of these nine patients are still alive.The phase III, double-blind, placebo-controlled, multicenterACOSOG Z9001 study showed that adjuvant therapy is safe, andsignificantly improves recurrence-free survival compared toplacebo when given postoperatively.22 The success of TKItreatment has changed the treatment paradigm for GIST and TKIsare increasingly prescribed in this centre. Adjuvant TKI wasadministered to 7 patients with intermediate and high risk lesionsin our series, six of these in the latter half of the study period.Median follow-up of these patients is 21 months, with norecurrences to date.
GISTs represent an unusual but increasingly encounteredneoplasm. Synchronous tumours appear to occur with greaterfrequency than in the general population and this potentially non-
random association requires further investigation. While GISTscontinue to present a diagnostic and therapeutic challenge, ourexperience demonstrates the excellent oncologic outcomes andfavourable safety profile that may be obtained, with increasing useof laparoscopic resections and adjuvant TKI the principle currenttrends.
Correspondence: JV ReynoldsDepartment of Surgery, Trinity Center, St James’s Hospital,James’s St, Dublin 8Email: [email protected]
References1. Connolly EM, Gaffney E, Reynolds JV. Gastrointestinal stromal
tumours. Br J Surg. 2003 Oct;90:1178-86.2. Appleman HD, Helwig EB. Gastric epithelioid leiomyoma and
leiomyosarcoma (leiomyoblastoma). Cancer. 1976 Aug;38:708-28.3. Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM.
Gastrointestinal pacemaker cell tumor (GIPACT): gastrointestinalstromal tumors show phenotypic characteristics of the interstitial cellsof Cajal. Am J Pathol. 1998 May;152:1259-69.
4. Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohistochemicalspectrum of GISTs at different sites and their differential diagnosiswith a reference to CD117 (KIT). Mod Pathol. 2000 Oct;13:1134-42.
5. Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ,Miettinen M, O’Leary TJ, Remotti H, Rubin BP, Shmookler B, SobinLH, Weiss SW. Diagnosis of gastrointestinal stromal tumors: Aconsensus approach. Hum Pathol. 2002 May;33:459-65.
6. Casali PG, Jost L, Reichardt P, Schlemmer M, Blay JY. Gastrointestinalstromal tumours: ESMO clinical recommendations for diagnosis,treatment and follow-up. Ann Oncol. 2009 May;20 Suppl 4:64-7.
7. DeMatteo RP, Lewis JJ, Leung D, Mudan SS, Woodruff JM, BrennanMF. Two hundred gastrointestinal stromal tumors: recurrence patternsand prognostic factors for survival. Ann Surg. 2000 Jan;231:51-8.
8. Emory TS, Sobin LH, Lukes L, Lee DH, O’Leary TJ. Prognosis ofgastrointestinal smooth-muscle (stromal) tumors: dependence onanatomic site. Am J Surg Pathol. 1999 Jan;23:82-7.
9. Pierie JP, Choudry U, Muzikansky A, Yeap BY, Souba WW, Ott MJ. Theeffect of surgery and grade on outcome of gastrointestinal stromaltumors. Arch Surg. 2001 Apr;136:383-9.
10. Perez EA, Livingstone AS, Franceschi D, Rocha-Lima C, Lee DJ,Hodgson N, Jorda M, Koniaris LG. Current incidence and outcomes ofgastrointestinal mesenchymal tumors including gastrointestinalstromal tumors. J Am Coll Surg. 2006 Apr;202:623-9.
11. Mucciarini C, Rossi G, Bertolini F, Valli R, Cirilli C, Rashid I, MarcheselliL, Luppi G, Federico M. Incidence and clinicopathologic features ofgastrointestinal stromal tumors. A population-based study. BMCCancer. 2007;7:230.
12. Demetri GD, Benjamin RS, Blanke CD, Blay JY, Casali P, Choi H,Corless C, Debiec-Rychter M, DeMatteo R, Ettinger D, Fisher G,Fletcher C, Gronchi A, Hohenberger P, Hughes M, Joensuu H, JudsonI, Le Cesne A, Maki R, Morse M, Pappo A, Pisters P, Raut C, ReichardtP, Tyler D, Van der Abbeele A, von Mehren M, Wayne J, Zalcbers J.NCCN Task Force report: management of patients withgastrointestinal stromal tumor (GIST)—update of the NCCN clinicalpractice guidelines. J Natl Compr Canc Netw. 2007 Jul;5 Suppl 2:S1-29; quiz S30.
13. Agaimy A, Wunsch PH, Sobin LH, Lasota J, Miettinen M. Occurrenceof other malignancies in patients with gastrointestinal stromal tumors.Semin Diagn Pathol. 2006 May;23:120-9.
14. Kalmar K, Tornoczky T, Poto L, Illenyi L, Kalmar Nagy K, Kassai M,Horvath OP. Gastrointestinal stromal tumours in a single institute: isthere an association to other gastrointestinal malignancies? MagySeb. 2004 Oct;57:251-6.
15. Kawanowa K, Sakuma Y, Sakurai S, Hishima T, Iwasaki Y, Saito K,Hosoya Y, Nakajima T, Funata N. High incidence of microscopicgastrointestinal stromal tumors in the stomach. Hum Pathol. 2006Dec;37:1527-35.
16. Fernandez JA, Sanchez-Canovas ME, Parrilla P. [Controversies in thesurgical treatment of primary gastrointestinal stromal tumours (GIST)].Cir Esp. 2010 Aug;88:69-80.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 178

179Original Paper
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
17. Gouveia A.M. PAP, Capelinha A.F, De la Cruz D, Silva P, Lopes J.M.Surgical margin status and prognosis of gastrointestinal stromaltumor. World J Surg Oncol. 2008;32:2375-82.
18. Novitsky YW, Kercher KW, Sing RF, Heniford BT. Long-term outcomesof laparoscopic resection of gastric gastrointestinal stromal tumors.Ann Surg. 2006 Jun;243:738-45; discussion 45-7.
19. Nannini M BG, Pallotti MC, Di Battista M, Santini D, Paterini P,Maleddu A, Mandrioli A, Lolli C, Saponara M, Di Scioscio V, ZompatoriM, Catena F, Fusaroli P, Dei Tos AP, Pantaleo MA. Late recurrences ofgastrointestinal stromal tumours (GISTs) after 5 years of follow-up.Med Oncol. 2012;29:144-50.
20. Bucher P, Taylor S, Villiger P, Morel P, Brundler MA. Are there anyprognostic factors for small intestine stromal tumors? Am J Surg.2004;187:761-6.
21. J Butt SR, P.J. Byrne, J.V. Reynolds. Management of gastrointestinalstromal tumours: a single-centre experience. Ir J Med Sci.2007;176:157-60.
22. Dematteo, RP, Ballman KV, Antonescu CR, Maki RG, Pisters PW,Demetri GD, Blackstein ME, Blanke CD, von Mehren M, Brennan MF,Patel S, McCarter MD, Polikoff JA, Tan BR, Owzar K. Adjuvant imatinibmesylate after resection of localised, primary gastrointestinal stromaltumour: a randomised, double-blind, placebo-controlled trial. Lancet,2009. 373: 1097-104.
Length of Stay Following Elective Surgery – Can We ImproveEfficiency?JG Solon1, JC Coffey2,3, DA McNamara1
1Department of Colorectal Surgery, Beaumont Hospital, Beaumont, Dublin 92Department of Surgery, and 3Centre for Interventions in Infection, Inflammation and Immunity (4i), Graduate Entry MedicalSchool, University of Limerick
IntroductionAdmission of patients for elective surgery has becomeincreasingly difficult1,2. Health Service Executive (HSE) policymandates reductions in the duration of Emergency Department(ED) stay, resulting in prioritised access to what is a finite andlimited bed capacity. Cancellations adversely affect patients3,impact negatively on hospital resources and reduce surgicaltraining opportunities. Too often elective patients cancelled on oneday become the following day’s emergency.
A number of initiatives have been implemented to varying degreesin different institutions to improve organisational efficiency butsignificant variations in practice occur. Length of hospital stay(LOS) for scheduled procedures varies between hospitals4.Increased use of day surgery, improved discharge planning, lessinvasive surgical techniques and more appropriate anaesthesiaand analgesia can all contribute to reduced LOS5. Same dayadmission for major surgical procedures might reduce a patient’soverall hospital stay but careful planning is needed to avoidcancellation or delays on the proposed day of surgery. Pre-operative assessment clinics and appropriate administrativeprotocols are a necessary precursor to its successfulimplementation. Earlier discharge from hospital after surgery canalso reduce LOS, however some operations carry a risk of seriouscomplications that might not become apparent even within 24hours of surgery6. Facilities to treat such complications promptlymust be present if surgeons are to have the confidence todischarge patients earlier after surgery. In 2011, The ElectiveSurgery Programme was launched as a collaborative initiativebetween the Royal College of Surgeons in Ireland and the HSEwith a view to optimising the surgical pathway of patientsfocussing on a number of key areas including LOS and day casesurgery rates.
The aims of this study were to assess the practice and attitudesof members of the Irish Association of Coloproctology in relationto appropriate LOS for a selection of general and colorectalsurgical operations and to assess the current status of day caseand day of surgery admissions (DOSA) within the Irish healthcaresystem.
MethodsThe Irish Association of Coloproctology (IACP) is an all-Irelandorganisation of surgeons specialising in colon and rectal surgery.All Republic of Ireland consultant members of the IACP werecirculated with a questionnaire and asked to reply anonymously inless than 30 days. Consultants were asked about the availabilityof anaesthetic pre-assessment clinics for 7-day, 5-day and daypatients as well as the feasibility of admitting patients on the dayof surgery. The facility to guarantee re-admission of patients whodevelop a complication of surgery was recorded. Respondentswere asked to quantify the average LOS considered appropriatefor a number of common surgical operations as well as thepercentage of all such patients who would be considered suitablefor day case surgery. These were HSE selected procedures thatthe association was requested to advise upon as a specialistgroup. Consultants were asked to specify the acceptable“average” and “optimal” LOS for patients undergoing either a righthemicolectomy or partial colectomy, including both open andlaparoscopic operations and encompassing all diagnosesencountered in their practice. Respondents had the opportunity tohighlight areas of concern or recommendations in a free textsection. Data outlining 2011 national statistics relating topercentage of patients treated as a day case and actual length ofstay were provided by the national Elective Surgery Programme.
ResultsThere were 20 respondents to the questionnaire comprising a
AbstractIncreasing emergency admissions place significant demands on limited hospital resources. We assessed national practices andresources for initiatives to reduce length of stay (LOS) and thereby improve efficiency of resource utilisation. Consultant members ofthe Irish Association of Coloproctology received a questionnaire seeking information about available initiatives aimed at reducingLOS. 20 out of 32 (62.5%) consultants responded to the questionnaire. Pre-assessment clinics for day surgery were available to18(90%). Only 13 (65%) had access to pre-assessment clinics for patients requiring longer admissions. 11 (55%) could admit majorcases on the day of surgery. Only 9 (45%) surgeons could guarantee immediate re-admission of patients discharged from hospital ifneeded. There was a divergence of opinion regarding the acceptable average LOS and percentage suitable for day surgery for avariety of common surgical procedures. This study highlights a number of key areas in which certain well-established initiatives couldimprove efficiency.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 179

180 Original PaperIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
62.5% response rate (n=20/32). Respondents includedconsultant surgeons based in university teaching hospitals,regional hospitals and county hospitals, as well as surgeons whoheld joint appointments to more than one hospital. Most surgeons(n=18, 90%) could refer patients for pre-operative anaestheticassessment if day case surgery was planned. This facility was lessdeveloped for patients requiring longer admissions with only 65%(13/20) of respondents having access to pre-assessment in thissetting. Day of surgery admission (DOSA) is recognised bysurgeons as being a useful strategy in reducing LOS. Only 55%(11/20) of consultants had access to DOSA for patientsundergoing major surgery.
The acceptable average LOS (in days) as suggested byrespondents for a variety of commonly performed surgicalprocedures as well as the percentage of each deemed suitable tobe done as a day case is illustrated in Table 1. There was a broadconsensus on the acceptable average LOS for all exceptlaparoscopic cholecystectomy, laparoscopic adhesiolysis andhaemorrhoidectomy. Similarly, there was a divergence of opinionsregarding the percentage of patients undergoing such operationswho would be suitable for day surgery. On average, only 44%,42.5%and 55% of patients were considered suitable for daysurgery in each procedure respectively. Several surgeonscommented that they would be reluctant to perform any of thesethree operations as a day case. This is at variance from the BritishAssociation of Day Surgery recommendation for laparoscopiccholecystectomy of 60% being suitable for day case surgery7.This may well be related to concerns in managing patients whodevelop post-operative complications in the community. Thevariation may be explained in part by the differing availability offree GP and public health nursing care between the NationalHealth Service (NHS) and HSE systems. Less than half ofsurgeons (n=9, 45%) could avail of guaranteed immediatesurgical re-admission of patients who develop post-operativecomplications. The majority had to refer such patients to theEmergency Department to await a bed. Surgeons commentedthat they would consider discharging post-operative patientsearlier if they were confident in their hospital’s ability to re-admitpatients with post-operative problems to a surgical bed promptly.
More significant operations demonstrated a greater variability inthe LOS considered appropriate by different surgeons. Theaverage acceptable LOS for patients undergoing a righthemicolectomy or large bowel excision was 6.4 days (range4 – 10 days) and 6.7 days (range 4 – 10 days) respectively. Theoptimal LOS was 4.4 days (range 2 – 7 days) and 4.8 days (range2 – 7 days) for each operation. It is noteworthy that the actualresults reported by the Elective Surgery Programme differsubstantially from these aspirations.
DiscussionInternational best practice, personal experience and unique localfactors are used by surgeons to determine the appropriate LOSfor patients following elective surgery. While initiatives to reduceLOS can improve the utilisation of limited available resources, it is
imperative that the correct infrastructure and support processesare available prior to implementation of system-wide changes toavoid adverse patient outcomes8. Such initiatives, while not alwaysimmediately cost-neutral, have the potential to improve efficiencyof bed use over time.
In the present series, a broad consensus on the acceptableaverage LOS and percentage of patients suitable for day casesurgery exists among consultant colorectal surgeons for manycommonly performed procedures. Despite this apparentconsensus, comparisons to actual 2011 HSE national data onelective admissions and day case percentage targets shownational practice differs from these aspirations. A highlightedlimiting factor to performing procedures as day cases was theinability to re-admit patients who experience a post-operativecomplication directly to a surgical ward. Non-availability of animmediate bed not only potentially compromises the outcome butit also reduces patient satisfaction. In the present series, only45% of surgeons could guarantee urgent re-admission of theirpatients who experience complications. Large bowel resectionsare often performed in patients with major medical co-morbiditieswhich can make estimating an “appropriate” LOS difficult.Nonetheless, respondents felt an average LOS of 6.4 for righthemicolectomy and 6.7 days for large bowel resection wasappropriate. This varies significantly from actual practice in 2011(Table 2).The study participants were explicitly asked about LOSrelating to the surgical procedure. Prolongation of LOS by medicalco-morbidity or placement issues are not included in theestimates, which by their nature exclude such variation. It wasnoted that centralisation of cancer surgery has resulted in somesurgeons practicing on multiple sites. Such surgeons may ofnecessity adapt their practice to ensure patient safety dependingon the services and staffing available at each centre and theirpersonal commitments on each site. A shorter optimal LOS of 4.4and 4.8 days respectively was thought possible with appropriatesupport.
Out-patient pre-operative assessment ensures that patients areoptimally prepared for surgery and significantly reduces the risk ofcancellation on the day of surgery9. While nearly all respondentshad the facility for pre-operative anaesthetic assessment ofproposed day cases, less than two-thirds had such facilitiesavailable for 5 or 7 day admissions. Such patients tend to havesignificant medical co-morbidities or are undergoing major surgerywith potential for significant complications. Availability of timelypre-assessment for such cases could optimise medical conditions,reducing the risk of cancellation or postponement on the day ofsurgery, thereby improving utilisation of scarce theatre time andreducing patient distress. This area of practice is currently apriority for development in most anaesthetic departments.
Table 1 Respondents were asked to state the acceptable averagelength of stay for a number of common operations as well asthe percentage of patients having each operation who wouldbe suitable for day case surgery
Mean LOS(range)
Mean % Day Case(range)
Laparoscopic Cholecystectomy 1.3 (1 – 3) 44 (0 – 90)
Open Inguinal Hernia 1 (0.5 – 2) 73 (10 – 100)
Diagnostic Laparoscopy 1 (0.5 – 1) 70 (0 – 100)
Umbilical Hernia 1 (0.5 – 3) 81 (25 – 100)
Pilonidal Sinus Excision 1.2 (1 – 3) 79 (0 – 100)
Laparoscopic Adhesiolysis 1.6 (1 – 3) 42.5 (0 – 90)
Laparoscopic Inguinal Hernia 1 (1) 72 (0 – 100)
Haemorrhoidectomy 1.55 (0.5 – 3) 55 (0 – 100)
Table 2 Irish national data for elective admissions 2011
TotalElective
DayCases
%Day
Case
NationalDay Case
rateTargets*
LOS ofpatients
LaparoscopicCholecystectomy
3397 781 23 40 2.2
Open Inguinal Hernia 2235 1181 52.8 90 2.1
DiagnosticLaparoscopy
1097 749 68 90 3.5
Umbilical Hernia 726 426 58.7 95 2.1
Pilonidal SinusExcision
542 342 63 95 2.1
LaparoscopicAdhesiolysis
292 135 46.1 95 2.7
Haemorrhoidectomy 360 157 43.6 60 2.0
Right Hemicolectomy 350 0 0 - 12.0
Left Hemicolectomy 94 0 0 - 12.6
*Agreed targets with Elective Surgery Programme
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 180
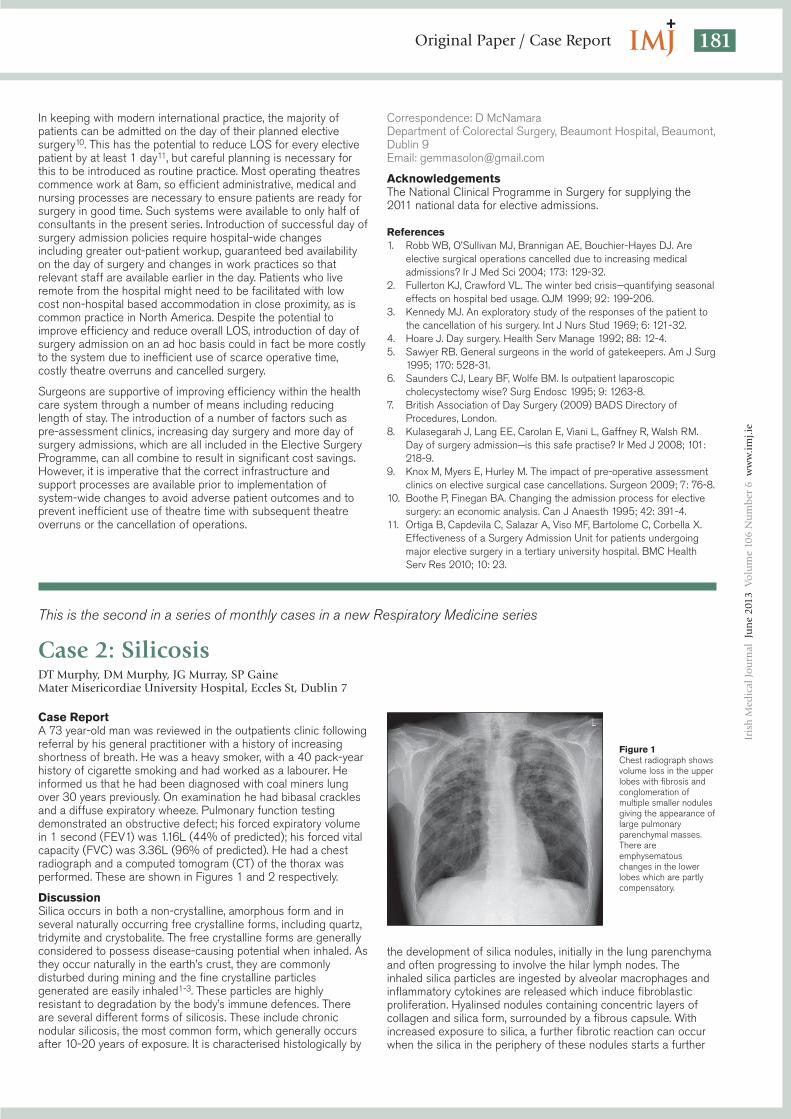
181Original Paper / Case Report
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
In keeping with modern international practice, the majority ofpatients can be admitted on the day of their planned electivesurgery10. This has the potential to reduce LOS for every electivepatient by at least 1 day11, but careful planning is necessary forthis to be introduced as routine practice. Most operating theatrescommence work at 8am, so efficient administrative, medical andnursing processes are necessary to ensure patients are ready forsurgery in good time. Such systems were available to only half ofconsultants in the present series. Introduction of successful day ofsurgery admission policies require hospital-wide changesincluding greater out-patient workup, guaranteed bed availabilityon the day of surgery and changes in work practices so thatrelevant staff are available earlier in the day. Patients who liveremote from the hospital might need to be facilitated with lowcost non-hospital based accommodation in close proximity, as iscommon practice in North America. Despite the potential toimprove efficiency and reduce overall LOS, introduction of day ofsurgery admission on an ad hoc basis could in fact be more costlyto the system due to inefficient use of scarce operative time,costly theatre overruns and cancelled surgery.
Surgeons are supportive of improving efficiency within the healthcare system through a number of means including reducinglength of stay. The introduction of a number of factors such aspre-assessment clinics, increasing day surgery and more day ofsurgery admissions, which are all included in the Elective SurgeryProgramme, can all combine to result in significant cost savings.However, it is imperative that the correct infrastructure andsupport processes are available prior to implementation ofsystem-wide changes to avoid adverse patient outcomes and toprevent inefficient use of theatre time with subsequent theatreoverruns or the cancellation of operations.
Correspondence: D McNamaraDepartment of Colorectal Surgery, Beaumont Hospital, Beaumont,Dublin 9Email: [email protected]
AcknowledgementsThe National Clinical Programme in Surgery for supplying the2011 national data for elective admissions.
References1. Robb WB, O’Sullivan MJ, Brannigan AE, Bouchier-Hayes DJ. Are
elective surgical operations cancelled due to increasing medicaladmissions? Ir J Med Sci 2004; 173: 129-32.
2. Fullerton KJ, Crawford VL. The winter bed crisis—quantifying seasonaleffects on hospital bed usage. QJM 1999; 92: 199-206.
3. Kennedy MJ. An exploratory study of the responses of the patient tothe cancellation of his surgery. Int J Nurs Stud 1969; 6: 121-32.
4. Hoare J. Day surgery. Health Serv Manage 1992; 88: 12-4.5. Sawyer RB. General surgeons in the world of gatekeepers. Am J Surg
1995; 170: 528-31.6. Saunders CJ, Leary BF, Wolfe BM. Is outpatient laparoscopic
cholecystectomy wise? Surg Endosc 1995; 9: 1263-8.7. British Association of Day Surgery (2009) BADS Directory of
Procedures, London.8. Kulasegarah J, Lang EE, Carolan E, Viani L, Gaffney R, Walsh RM.
Day of surgery admission—is this safe practise? Ir Med J 2008; 101:218-9.
9. Knox M, Myers E, Hurley M. The impact of pre-operative assessmentclinics on elective surgical case cancellations. Surgeon 2009; 7: 76-8.
10. Boothe P, Finegan BA. Changing the admission process for electivesurgery: an economic analysis. Can J Anaesth 1995; 42: 391-4.
11. Ortiga B, Capdevila C, Salazar A, Viso MF, Bartolome C, Corbella X.Effectiveness of a Surgery Admission Unit for patients undergoingmajor elective surgery in a tertiary university hospital. BMC HealthServ Res 2010; 10: 23.
This is the second in a series of monthly cases in a new Respiratory Medicine series
Case 2: SilicosisDT Murphy, DM Murphy, JG Murray, SP GaineMater Misericordiae University Hospital, Eccles St, Dublin 7
Case ReportA 73 year-old man was reviewed in the outpatients clinic followingreferral by his general practitioner with a history of increasingshortness of breath. He was a heavy smoker, with a 40 pack-yearhistory of cigarette smoking and had worked as a labourer. Heinformed us that he had been diagnosed with coal miners lungover 30 years previously. On examination he had bibasal cracklesand a diffuse expiratory wheeze. Pulmonary function testingdemonstrated an obstructive defect; his forced expiratory volumein 1 second (FEV1) was 1.16L (44% of predicted); his forced vitalcapacity (FVC) was 3.36L (96% of predicted). He had a chestradiograph and a computed tomogram (CT) of the thorax wasperformed. These are shown in Figures 1 and 2 respectively.
DiscussionSilica occurs in both a non-crystalline, amorphous form and inseveral naturally occurring free crystalline forms, including quartz,tridymite and crystobalite. The free crystalline forms are generallyconsidered to possess disease-causing potential when inhaled. Asthey occur naturally in the earth’s crust, they are commonlydisturbed during mining and the fine crystalline particlesgenerated are easily inhaled1-3. These particles are highlyresistant to degradation by the body’s immune defences. Thereare several different forms of silicosis. These include chronicnodular silicosis, the most common form, which generally occursafter 10-20 years of exposure. It is characterised histologically by
the development of silica nodules, initially in the lung parenchymaand often progressing to involve the hilar lymph nodes. Theinhaled silica particles are ingested by alveolar macrophages andinflammatory cytokines are released which induce fibroblasticproliferation. Hyalinsed nodules containing concentric layers ofcollagen and silica form, surrounded by a fibrous capsule. Withincreased exposure to silica, a further fibrotic reaction can occurwhen the silica in the periphery of these nodules starts a further
Figure 1Chest radiograph showsvolume loss in the upperlobes with fibrosis andconglomeration ofmultiple smaller nodulesgiving the appearance oflarge pulmonaryparenchymal masses.There areemphysematouschanges in the lowerlobes which are partlycompensatory.
92031-IMJ JUNE 2013_TF 10/06/2013 08:31 Page 181

182 Case ReportIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
fibrotic reaction, a cascade which can lead to progressive massivefibrosis (PMF).
In chronic nodular silicosis, multiple small (usually 1-5 mm, butcan reach up to 10 mm) symmetrically distributed, roundedcentrilobular nodules are typically seen on high resolution CTimaging with an upper lobe predominance. The hilar andmediastinal lymph nodes typically calcify, resulting in acharacteristic ‘egg-shell’ calcification appearance. Acceleratedsilicosis as the name suggests, occurs sooner (afterapproximately 3-10 years of exposure), but with otherwise similarfeatures to chronic nodular silicosis. Acute silicosis can occurafter exposure to a large volume of silica, for example insandblasters. These patients present with increasing dyspnoeawithin 1 to 3 years following exposure.
PMF is defined by larger (>1cm) opacities due to progressivefibrosis and coalescence of the nodules. Over time fibrotic massesoccur with associated distortion of the adjacent interstitium and
paracicatritial emphysema developing between the masses andthe pleura. In addition, silicosis is associated with increasedincidence of lung cancer (especially in smokers) andtuberculosis4-6. It has been reported that pulmonary tuberculosisoccurs in 25% of patients with silicosis, particularly those withprogressive massive fibrosis. Those exposed to silica are also atincreased risk of developing lung fibrosis and chronic interstitialpneumonia, most commonly usual interstitial pneumonia (UIP).Imaging plays a role in distinguishing the features of the variousoccupational lung diseases and also in the assessment of diseaseactivity and response to treatment7.
There is no satisfactory treatment for silicosis. Management iscentred on primary prevention and in those who develop thecondition, surveillance for tuberculosis, lung cancer and COPD,with the importance of smoking cessation stressed. Thankfully, inthe western world, the prevalence of pneumoconiosis such assilicosis, coal workers lung and berylliosis have decreased due tothe decline of the mining industry, better industrial hygiene andincreased awareness of the conditions. Although only a smallpercentage (10%) of coal miners develop silicosis, depending onthe type of mining undertaken, the disease unfortunately remainsan ongoing problem in developing countries.
Correspondence: S GaineDepartment of Respiratory Medicine, Mater MisericordiaeUniversity Hospital, Eccles St, Dublin 7Email: [email protected]
References1. Banks DE, Bauer MA, Castellan RM, and Lapp NL. Silicosis in surface
coalmine drillers. Thorax, 1983. 38:275-8.2. Seaton A, Ruckley VA, Addison J, and Brown WR, Silicosis in barium
miners. Thorax, 1986. 41:591-5.3. Warrell DA, Harrison BD, Fawcett IW, et al. Silicosis among grindstone
cutters in the north of Nigeria. Thorax, 1975.30:389-98.4. Cowie RL. The epidemiology of tuberculosis in gold miners with
silicosis. Am J Respir Crit Care Med, 1994.150:1460-2.5. Hnizdo E, Murray J, and Klempman S. Lung cancer in relation to
exposure to silica dust, silicosis and uranium production in SouthAfrican gold miners. Thorax, 1997. 52: 271-5.
6. Leung CC, Law WS, Chang KC, et al.,Initial experience on rifampinand pyrazinamide vs isoniazid in the treatment of latent tuberculosisinfection among patients with silicosis in Hong Kong. Chest, 2003.124: 2112-8.
7. Sirajuddin A, Kanne JP. Occupational lung disease. J Thorac Imaging.2009 Nov;24:310-20.
Figure 2 Axial CT thorax: Note the high density material within the soft tissuecomponents on the mediastinal windows (left panels) which may be dueto calcification or represent the deposited silica crystals as well as thefibrotic reaction which is most evident on the corresponding lungwindows (right panels). Also note the early cavitation in the left upperlobe which is typically caused by ischaemic necrosis or occasionally whencomplicated by TB. Lymph nodes in the mediastinum can also behyperdense and can calcify. Like most inhalational lung disorders,findings are most marked in the apical and posterior portions of theupper lobes and apical segments of the lower lobes.
Double Trouble - Ureteric Obstruction Due to BilateralUrothelial CarcinomaGJ Nason, F O’Kelly, DW MulvinDepartment of Urology, St Vincent’s University Hospital, Elm Park, Dublin 4
IntroductionUpper tract urothelial carcinoma (UTUC) accounts for ~5%of allurothelial cancers, with a four-fold increased risk in the renalpelvis. Synchronous bilateral tumors are an extremely rareoccurrence with few reports in the literature. Opennephroureterectomy with resection of an ipsilateral bladder cuff isthe reference standard surgical treatment of UTUC1. Haematuria
is the most common presenting complaint for UTUC. We reportthe case of synchronous bilateral urothelial carcinomas of theureters in a gentleman presenting with frank haematuria.
Case ReportA 69year old smoker was referred to our unit, a tertiary referralcentre, following an episode of acute urinary retention and three
AbstractUpper tract urothelial carcinoma (UTUC) represents ~5% of all urothelial carcinomas. Synchronous bilateral tumors are extremely rarewith only 19 reports in the literature. Haematuria is the main presenting complaint. We report a case of synchronous bilateral tumors ofthe ureters in a gentleman with frank haematuria treated with staged aggressive resection.
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 182

183Case Report
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
episodes of frank haematuria in the past year. Clinical examinationwas unremarkable and digital rectal exam revealed abenign40gram prostate. Serum creatinine was 220. Flexiblecystoscopy was normal. MR Urogram was performed due to renalimpairment and revealed bilateral hydronephrosis, more severe onthe left side with bilateral hydroureter (Figure 1).
Subsequent retrograde pyelogram and ureteroscopy revealedproximal obstruction of both ureters and biopsy of these lesionsrevealed low grade non invasive urothelial papillary carcinoma,pTa. Urine cytology demonstrated atypical cells consistent withurothelial carcinoma. CT thorax, abdomen and pelvis revealed non-specific sub centimetre pulmonary nodules. A renogram showeda non functioning left kidney with good preservation of rightkidney function. Following discussion at the uro-pathology multidisciplinary conference, the patient was offered a two stageradical surgical approach. A left radical nephroureterectomy wasinitially performed. Six weeks later, the second stage involved aright distal ureterectomy, cystoprostatectomy and right cutaneousureterostomy formation. Histology demonstrated high gradepapillary urothelial carcinoma of the ureter with invasion into thesubepithelial connective tissue. The proximal ureteric marginswere negative. Renal pelvis, left kidney, bladder and prostate werebenign, pT2, Nx, R0.
He has recovered well from this radical surgical approach, hisrenal function has normalised and is currently undergoingadjuvant chemotherapy. This case adds to the current literaturedemonstrating the rare occurrence of bilateral ureteric cancer andhighlighting the need for upper tract imaging with haematuria.
DiscussionPrimary UTUC is a rare urological disease. Approximately 5% ofall urothelial carcinomas occur in the kidneys and ureters (upperurinary tract). The vast majority of upper urinary tract tumors arisein the kidney, comprising 4–15% of all primary kidney neoplasmsin the United States, whereas ureteric tumors represent only 1%1.There are limited reports of bilateral synchronous ureteric tumourswith only 19 reports in the literature (Table 1). In 2004, Holmang
et al reported a series of 936 upper tract tumors, 15 had bilateralsynchronous upper tract tumors with only two having bilateralureteric tumors, one was treated with a nephroureterectomy andcontralateral local resection, the other was treated with bilaterallocal resections2. Brown et al reported a series of 434 patientswith UTUC, 184 had had a nephroureterectomy as primarycurative treatment. Open radical nephroureterectomy with removalof a bladder cuff was used in 158 patients (85.9%) andlaparoscopic radical nephroureterectomy with open bladder-cuffexcision n 26 (14.1%)3.
The gold standard of open radical nephroureterectomy withresection of a bladder cuff is being challenged by minimallyinvasive approaches to the managing of upper urinary tracturothelial carcinoma (UTUC) with laparoscopicnephroureterectomy a feasible alternative to an open procedure4.Recent data has showed improved survival in patients withbladder cancer who have a multimodal treatment withchemotherapy, a stronger argument can be made for any patientsuspected of having a high-risk UTUC to receive chemotherapybefore surgery. This position is strongly supported in that patientswith UTUC often sustain a significant loss of renal reserve as aresult of surgery, frequently in the setting of advanced age orchronic renal insufficiency. This factor essentially precludes theability to deliver effective doses of cytotoxic chemotherapy aftersurgery5. In the setting of a non functioning kidney, as in this case,reduced dose adjuvant chemotherapy is appropriate.
Synchronous bilateral ureteric tumours are an extremely rareoccurrence. This case demonstrates a radical surgical approach,performed at an interval, needs to be considered in the decisionprocess.
Correspondence: GJ NasonDepartment of Urology, St Vincent’s University Hospital, Elm Park,Dublin 4Email: [email protected]
References1. Ristau BT, Tomaszewski JJ, Ost MC. Upper tract urothelial carcinoma:
current treatment and outcomes. Urology. 2012 Apr;79:749-56.2. Holmäng S, Johansson SL. Synchronous bilateral ureteral and renal
pelvic carcinomas: incidence, etiology, treatment and outcome. Cancer.2004 Aug 15;101:741-7.
3. Brown GA, Busby JE, Wood CG, Pisters LL, Dinney CP, Swanson DA,Grossman HB, Pettaway CA, Munsell MF, Kamat AM, Matin SF.Nephroureterectomy for treating upper urinary tract transitional cellcarcinoma: Time to change the treatment paradigm? BJU Int. 2006Dec;98:1176-80.
4. K.C. Latchamsetty, C.R. Porter. Treatment of upper tract urothelialcarcinoma: a review of surgical and adjuvant therapy. Rev Urol, 8(2006), 61–70.
5. Lerner SE, Blute ML, Richardson RL, Zincke H. Platinum-basedchemotherapy for advanced transitional cell carcinoma of the upperurinary tract. Mayo Clin Proc1996; 71: 945–50.
6. Kang CH, Yu TJ, Hsieh HH, Yang JW, Shu K, Shiue YL. Synchronousbilateral primary transitional cell carcinoma of the upper urinary tracts:ten patients with more than five years of follow-up. Urology. 2004Feb;63:380-2.
7. Tan LB, Tserng BR, Huang WH, Tarn CJ. Synchronous bilateralcarcinoma of the ureter in association with unilateral incompleteduplication of the ureter. Urol Int. 1996;56:196-9.
8. Zungri E, Chéchile G, Algaba F, Diaz I, Vilá F, Castro C. Treatment oftransitional cell carcinoma of the ureter: is the controversy justified?Eur Urol. 1990;17:276-80.
9. Levine RL, Airhart RA. Bilateral synchronous transitional ureteralcarcinoma: two additional cases. South Med J. 1977 Dec;70:1418-20.
10. Talavera JM, Carney JA, Kelalis PP. Bilateral, synchronous, primarytransitional cell carcinoma of the ureter: report of 2 cases add reviewof literature. J Urol. 1970 Nov; 104:679-83.
Figure 1MR Urogramdemonstratingbilateralhydroureter withmid uretericobstruction
Table 1 Previous reported bilateral synchronous ureteric tumours
Journal Year AuthorNumber
ofcases
Treatment
BJU Int. 2006 Brown et al.3 8 Nephroureterectomy
Cancer 2004 Holmang et al.2 2 Local resection andcystectomy
Urology 2004 Kang et al.6 32 local resections andone nephroureterectomyand cystectomy
Urol Int. 1996 Tan et al.7 1Nephroureterectomy andcontralateral localresection
European Urology 1990 Zungri et al.8 1
South Med J 1977 Levine et al.9 2 Local resections
J Urol. 1970 Talvera et al.10 2 Local resections
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 183

184 Research CorrespondenceIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
IntroductionAll clinical research projects are required to undergo ethicalreview. Until 2010, in Ireland, each hospital medical researchethics committee (REC) had its own application form. This wasseen to act as a potential impediment to research.1 Of particularconcern were projects involving multiple research sites, whereresearchers were required to complete a number of differentforms for the one multi-centre study. Hence in 2009 aconsultation group was formed, including representatives frommany of the RECs across Ireland, with the aim of designing astandard application form that could be adopted by all RECs. Theform was designed to be used for the ethical review of health-related research studies that were not clinical trials of medicinalproducts for human use as defined by the European Communities(Clinical Trials on Medicinal Products for Human Use)Regulations, 2004, (Statutory Instrument 190 of 2004). The formwas finalised in late 2010,2 and adopted for use by BeaumontREC at that time. This audit had two purposes: to assess thevolume and types of comments made during committee reviewand, to assess if the changeover to the new standard applicationform had any impact on the volume or type of comments made.
MethodsAll clinical research studies, except clinical trials of medicinalproducts, reviewed by the Beaumont Hospital (Medical Research)Ethics Committee between January and June 2010, and betweenJanuary and June 2011, were included in this audit. The type ofstudy, the study intervention and level of the principal investigatorwere recorded for each application. All comments made by thecommittee are documented in the monthly meeting minutes. Inorder to optimise consistency and so as to avoid bias, commentsfrom 2010 and 2011 were collected and analysed according tomonth order i.e. January comments for both 2010 and 2011 wereanalysed first followed by February comments for both 2010 and2011.
Each comment was classified according to the following criteria;Category - most categories were derived from the sectionheadings of the new standardised application form: general studyand administrative details; study design and descriptors; studyparticipants; informed consent; inclusion of vulnerable groups;research procedures; data protection; human biological material;radioactive material; medical devices; indemnity; cost and resourceissues; other ethical issues; and participant documentation. Natureof comment; Requests for a change to the application orparticipant documentation, or for further information orclarification; Level of importance of comment; major /intermediate / minor. Qualitative data was also extracted byrecording a short summary of each comment.
The above data was entered into a spreadsheet and underwent
both qualitative and quantitative analysis. Wilcoxon rank-sum(Mann Whitney) tests were used to test for between yeardifferences in the volume, category, nature or level of importanceof the comments.
ResultsEighty-six ethical review applications were analysed in total, 52from 2011 and 34 from 2010. This represented all applicationsconsidered at full committee meetings (other than clinical trials ofmedicinal products under S.I. 190/2004) between January andJune of those two years. The majority of applications weresubmitted by medical consultants, accounting for 54% of the total(n=47). Surgical consultants accounted for 10% (n=9), as didnon-consultant hospital doctors (NCHDs) and laboratoryscientists. Paramedical staff and other allied health professionalsmade up 9% of submissions (n=8). Four studies were sent backfor a complete rewrite of the protocol, application form and patientdocumentation prior to resubmission for ethical review – two fromeach six-month period.
There were in total 915 queries made by the REC concerning the86 applications. Between January and June 2010, 409 commentswere made concerning 34 applications – 173 were requests for
Recurring Themes Arising During Medical Research EthicsCommittee ReviewE Kelleher1, A Stanton2, G Vale2, D Smith1
1RCSI, 123 St Stephen’s Green, Dublin 22Beaumont Hospital, Beaumont, Dublin 2
AbstractA standard application form for the ethical review of health-related research studies has recently been adopted by many Irish medicalresearch ethics committees. In order to assess the impact of the new form, we reviewed all comments made by the BeaumontHospital Ethics Committee during two six-month periods, immediately prior to adoption of the new form (2010), and soon afterwards(2011). Neither volume nor comment type differed significantly between the two observation periods. Participant documentation(information leaflets and consent forms) accounted for the largest proportion of comments (2010; 44%, 2011; 37%). Other commonareas prompting queries were study administration (7%), design (12%) and procedures (13%), participant selection and recruitment(8%), and lastly data protection (9%). Because of these findings, the standard operating procedures of the committee have beenrevised – use of provided template participant documentation is strongly encouraged, and a “Recurring Review Themes” checklist ishighlighted to all applicants.
Table 1 displays requests for further information and for changesduring 2010 and 2011, according to category and level ofimportance (minor, intermediate, major)
Requests
2010 2011
FurtherChange
FurtherChange
Information Information
General Details 23 (0,5,18) 8 (5,3,0) 8 (1,1,6) 21 (4,6,11)
Study Descriptors 8 (5, 3, 0) 18 (8, 2, 8) 35 (3, 14, 18) 24 (3, 4, 17)
Study Participants 17 (6, 7, 4) 12 (1, 7, 4) 35 (9, 16, 10) 7 (3, 1, 3)
Informed Consent 10 (2, 1, 7) 4 (0, 2, 2) 10 (0, 7, 3) 2, (0, 0, 2)
Vulnerable Groups 8 (0, 7, 1) 3 (0, 1, 2) 8 (3, 4, 1) 2 (0, 1, 2)
Research Procedures 28 (1, 16, 11) 8 (0, 4, 4) 62 (2, 45, 15) 17 (2, 6, 9)
Data Protection 21(5, 6, 10) 17 (3, 10, 4) 28 (2, 16, 10) 18 (8, 3, 7)
Biological Material 5 (0, 3, 2) 5 (2, 3, 0) 7 (1, 3, 3) 5 (1, 2, 2)
Medical Devices 0 (0, 0, 0) 2 (0, 0, 2) 1 (0, 0, 1) 0 (0, 0, 1)
Indemnity 2 (0, 0, 2) 3 (1, 0, 2) 10 (0, 1, 9) 4 (0, 1, 3)
Cost & Resources 10 (0, 5, 5) 2 (1, 1, 0) 15 (1, 8, 6) 2, (1, 0, 1)
Other 1 (0, 0, 1) 3 (0, 1, 2) 1 (0, 1, 0) 5 (2, 3, 0)
ParticipantDocumentation
19(4, 8, 7)
170(86, 51, 14)
22(9, 10, 3)
199(84, 69, 24)
Total 152 236 242 285
Data as total number of queries (minor, intermediate, major)
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 184

185Research Correspondence
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
further information (mean±SD per application; 5.1±4.5), and 236were requests for changes to the protocol or participantdocumentation (6.9±6.1). During the same period in 2011, 527comments were made concerning 52 applications (furtherinformation requests; n=242, 4.7±3.9, and change requests;n=285, 5.5±4.6,). Two-sample Wilcoxon rank-sum (Mann-Whitney) tests showed no significant difference in numbers ofcomments per application, category type, nature of comment, norcomment level of importance, between the two periods.
Table 1 shows the volume, nature and level of comments made ineach category for each period. It is clear that in both 2010 and2011, ‘Participant Documentation’ accounted for the greatestproportion of comments – 170 out of 388 in 2010 (44%) and 199out of 527 in 2011 (38%). It can also be seen that the other areasprompting a large number of comments were general studydetails and administration (7%), study design and descriptors(12%), study research procedures (13%), participant selection andrecruitment (8%), and lastly data protection (9%). These 5categories alongside participant documentation accounted for88% of all queries.
It was noted that within each of the six categories accounting forgreater than 5% of comments, there were common themes orsub-categories. The 6 categories and any sub-categories thatprompted at least 1% of the total comments, along with the mostcommon queries or required corrections are illustrated in Figure 1.This figure forms the basis of a checklist provided to applicants tothis committee, aiming to reduce committee queries andcomments through highlighting our previous most commoncomments, queries and requests for changes.
DiscussionWhile adoption of a standard application form for the ethicalreview of health-related research studies by the majority ofmedical research ethics committees country-wide is a welcomeinitiative towards streamlining the review process, this audit clearlydemonstrates that it had little or no impact on the volume ornature of comments made by the Beaumont Hospital (MedicalResearch) Ethics Committee. The second major finding of thisaudit was that a very limited number of areas accounted for a veryhigh proportion of comments – queries concerning participantdocumentation prompted 40% of comments, and five othercategories (general study details and administration, study designand descriptors, study research procedures, participant selectionand recruitment, and data protection) were responsible for afurther 48% of all queries. As a consequence of these findings,the standard operating procedures of the Beaumont Hospital(Medical Research) Ethics Committee have been revised. Firstlythe table of recurring review themes and comments is provided asa checklist to all investigators intending to submit an application tothe REC. Secondly use of provided template participantinformation leaflets and participant consent forms in drafting theparticipant documentation is strongly encouraged.
Our findings are likely to be generalisable to other Irish RECsreviewing clinical studies and using the standard application form– it is to be anticipated that the same common issues are raisedby many committees. Hence we have made our checklists andtemplate participant documentation freely available to all on ourwebsite www.beaumontethics.ie/application/index. It is hoped andanticipated that through identifying and highlighting the commonsources of REC queries to future applicants, that completion ofthe application form and participant documentation will beimproved, and that fewer comments will be raised by the REC. Ifthis does occur, applicants will gain ethical approval with a lessernumber of document adjustments, the workload of REC memberscould be considerably reduced, and the timelines of the reviewprocess would be likely to shorten. This question will be thesubject of a future audit.
Correspondence: E KelleherRCSI, 123 St Stephen’s Green, Dublin 2Email: [email protected]
References1. Morrissey M. Review of Research Ethics Committees & Processes in
Republic of Ireland. HSE Research Ethics Review Group. 2008.2. Research Ethics Committee Standard Application Form for the ethical
review of health-related research studies which are not clinical trialsof medicinal products as defined in S.I. 190/2004. StandardApplication Form Consultation Group. Version 5.4, 9.8.10.
Recurring Review Themes and Comments: A Checklist for Applicants
General StudyDetails/
Administration
(n=60, 7%)
StudyInvestigators(n=22, 2%)
Is a Beaumont Hospital consultantinvolved?Ensure the principal investigator isconsistent throughout the applicationInclude an expert co-investigator ifnecessary
Queries about IrishMedicines Board(IMB) issues(n=6, 1%)
Is the application for a clinical trial?(If so, a different application applies)
StudyDescriptors
(n=106, 12%)
Statistical Analysis(n=26, 3%)
Provide details of sample size
Provide a power calculation
Justification forelements of thestudy (n=13, 1%)
Justify the outcome measures
Is the timeframe practical?
StudyParticipants
(Recruitment &Selection)
(n = 71, 8%)
Inclusion / ExclusionCriteria (n=18, 2%)
Ensure consistency throughout theapplication
Are all the criteria justified?
Recruitment(n=21, 2.3%)
Comment on the feasibility of recruitingadequate numbers
How will participants be recruited?
ResearchProcedures
(n=115, 13%)
Provide moredetails(n=35, 4 %)
What procedures will participantsundergo?
Justify use of procedures
Clarify what is partof routine careand what is not(n=18, 2%)
What exactly does the study involve, andhow is it separate from the treatmentpatients already receive?
Queries regardingaspects of treatment(n=15, 2%)
Provide specifics of what is involved ifthe research study is also part of theparticipant’s treatment
DataProtection
(n=84, 9%)
Data Access(n=10, 1%)
Will medical records be accessed?
Who will be accessing the data?
Confidentiality(n=11, 1%)
Will identifiable data be collected?
Will data be anonymised or coded?
Data Storage(n=19, 2%)
Where will data be stored?
Will data leave the hospital?
Will data be sent abroad?
ParticipantDocumentation
(informationleaflets,
consent forms,questionnaires,and any other
documentationprovided to theparticipants)
(n=369, 40%)
Clarify informationin patientdocumentation(n=110, 12%)
State if a procedure is part of theparticipant’s standard care or if it is anadditional procedure for researchpurposes
State who has access to data collected
Additionalinformationrequired (n=59, 6%)
Include contact details of investigator(s)
State risks of participating
State what will happen to data collected
Grammar /Formatting(n=37, 4%)
Correct typos
Correct inappropriate use of headings
Adjust font size
Adjust layout
Missing documents(n=10, 1%)
Provide information leaflets specific tonext-of-kin, parents etc.
Figure 1 The most common comments made by Beaumont Hospital (MedicalResearch) Ethics Committee, in response to 86 submitted applicationforms and participant documentation during two six-month periods in 2010and 2011, are grouped according to category and sub-category. Numbersof comments, and the percentage of the total number of comments(n=915) in each category and sub-category are indicated. This figure formsthe basis of a checklist provided to applicants to this committee, aiming tohighlight common comments, queries and requests for changes.
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 185

186 Occasional PieceIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
IntroductionThis clinical practice guideline is derived from the NHBD protocolapproved by Beaumont Hospital Clinical Ethics Forum in 2011 andendorsed by the Intensive Care Society of Ireland in 2012. Thisguideline has been welcomed by the Medical Council of Ireland.NHBD has the support of the HSE National Organ Donation andTransplantation Office. Its development is cited as a keyrecommendation in an external review of transplantation services2011.1 It has also received support from the National Directorateof Nursing and Midwifery and the Coroner’s Society of Ireland. Inthe United Kingdom, NHBD is supported by the Intensive CareSociety, in Australia and New Zealand it is supported by theirsocieties of Intensive Care Medicine (ANZICS). In North America,NHBD has been supported by three Institute of Medicinecommittees, the Canadian Council on Organ Donation, theAmerican Medical Association, and the Society of Critical CareMedicine.2 NHBD was the standard before the widespreadadoption of BSD criteria. NHBD later declined, as it was believedthat the organs donated were inferior to those following BSD.Today, outcome data demonstrate almost equivalent renal andpulmonary graft survival.3-5,6-8 Although hepatic transplantationfrom NHB donors is associated with an increased incidence ofvascular and biliary complications, these may be minimised bystringent donor criteria.9-11
The Maastricht ClassificationPotential NHB donors may be divided into 5 categories.12
Category 1 are patients who arrive in hospital dead. Categories 2and 5 are patients in whom resuscitation has been attempted, butare pronounced dead following unsuccessful resuscitation, eitherfollowing out-of-hospital cardiac arrest (Category 2), or in-hospitalcardiac arrest (Category 5). This clinical guideline includespatients in categories 3 or 4 only, i.e. they will be controlled organdonors; those in whom an exact warm ischaemic time (WIT) isknown. While definitions vary, the WIT begins when the systolicblood pressure or oxygen saturation fall below 40mmHg or 40%respectively, and ends with cold perfusion (range: 35-60mmhg,35-60%).
Maastricht Category 3: These patients have devastating non-recoverable neurological injury, typically secondary to traumaticbrain injury (TBI), but occasionally due to hypoxic ischemicencephalopathy (HIE). Poor prognostic factors in HIE includemyoclonic status epilepticus, loss of pupillary or corneal reflexesand extensor posturing, a high neuron specific enolase and loss ofSSEPs. These criteria may be assessed after 72 hours or afterday 6 if the patient was subjected to induced hypothermia.13
Maastricht Category 4: These patients are likely to fulfill thecriteria for BSD, however brainstem testing cannot be performeddue to the degree of haemodynamic instability or imminent
Non Heart Beating Organ Donation in Adults: A ClinicalPractice GuidelineJ O’RourkeDepartment of Anaesthesia and Intensive Care Medicine, Beaumont Hospital, Dublin 9
AbstractNon heart beating organ donation (NHBD) occurs when a patient donates organs following the determination of death by cardio-respiratory criteria. It is also know as Donation after Cardiac Death (DCD) or Donation after Circulatory Death (DCD). This is distinctfrom Donation after Brainstem Death (DBD), which until 2011, accounted for all cadaveric organs (organ from deceased persons)donated within the Republic of Ireland. NHBD is an important initiative that has the potential to be life-saving. When compared tointernational protocols, the NHBD protocol at Beaumont Hospital is both conservative and restrictive. It offers an alternative whenconditions of brainstem death (BSD) cannot be satisfied and, since implementation a number of successful transplants have beenperformed from NHB donors.
Table 1 Outcomes for transplanted organs
KidneyTransplantation NHBD BSD Author
(Reference)
Graft survival at 5 years(No. of patients) 76.2% (N=748) 76.4% (N=6888) Summers DM
2010 (3)
Graft survival at 10 years(No. of patients) 71% (N=382) 65% (N=1089) Cooper JT
2004 (4)
Graft survival at 6 years(No. of patients) 73% (N=708) 72% (N=97 990) Rudich SP
2002 (5)
Lung Transplantation NHBD BSD Author(Reference)
Patient Survival at 5 years(No of patients) 76% (14/18) 63% (244/406) De Oliviera NC.
2010 (6)
Patient Survival at 2 years 95% 20/21 86% 66/77 Erasmus ME.2010 (7)
Patient Survival at 2 years(No of patients) 87% (33/36) 69%
(9660/14000)Mason DP.2008 (8)
Liver Transplantation NHBD BSD Author(Reference)
Graft Survival at 1 : 3 : 5years (No of patients)
81% : 73% : 69%200
83% : 75% : 69%1828
Taner CB 2012(9)
Graft Survival at 1:5:10years (No of patients)
69% : 56% : 44%141
82% : 73% : 63%282
De Vera E2009 (10)
Graft survival at 1:2:5years (No of patients)
74% : 68% : 3%19 Equivalent 438 Nguyen H
2009 (11)
Protocol Schematic
Patient with devastating head injury/Severe hypoxic brain injury, patient fulfilsmany but not all brainstem death criteria
Decision to redirect therapy towards comfort measures only by admittingconsultant and ICU consultant
Controlled withdrawal of medical treatments consideredPatient deemed a potential candidate for donation after cardiac death
Second medical opinion regarding futility if admitting consultant is not aneurosurgeon or neurologist.
Second Intensive care consultant opinionAll (Admitting consultant, Neurosurgeon or Neurologist plus Two ICU consultants)
agree with futility decision, Opinion of Coroner sought
Family discussion regarding redirection of care towards palliative measures onlyQuestion of patient’s wishes and family wishes regarding organ donation
Consent discussion and detailed explanation of process of donation after cardiacdeath
Consent for antemortem interventions such as bloods, heparin administrationTime out: Intensive Care Medicine, Nursing and Transplantation retrieval teams
Designated time for withdrawal of ventilatory supportWithdrawal of life sustaining therapy as scheduled
90 minute maximum period
Death confirmed by cardiorespiratory criteria after a 5 minute period of monitoredasystole (first 5 minute period)
5 minute Stand down time during which patient may be transferred to theatre fororgan donation operation, sterile prep and draping (second 5 minute period)This second period of 5 minutes has elapsed without any auto resuscitation
Organ donation operation begins
Figure 1
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 186
187Occasional Piece
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
cardiac arrest. NHBD may represent the only feasible way thatthese patients may donate organs.
Over-Riding PrinciplesUnless there is consensus between all clinicians and among allfamily members then NHBD will not be pursued. Care of thedying patient is of paramount importance and measures tomaintain the comfort and dignity of the patient will not becompromised for organ donation. No interventions that couldpossibly cause pain or distress before death are acceptable.Blood sampling to facilitate microbiology and crossmatching, andheparin administration are permissible and are specificallyaddressed in the consent process.
Futility within the ICUDecisions regarding futility are made by the primary admittingconsultant and the intensivist. If the patient is deemed a potentialcandidate for NHBD, the opinion of a second intensivist isrequested. As the primary injury is neurological, the opinion of aneurologist or neurosurgeon should be documented beforeconsidering NHBD.
Inclusion CriteriaThe criteria are similar but not identical to those used followingBSD. An incidence of delayed graft function is expected andtherefore stringent age and comorbidity restrictions should apply.The patient must be dependant on ventilatory or inotropic supportto the extent that they are likely to die within 90 minutes ofwithdrawal. While there are several predictive tools, theexperience and insight of the intensive care staff are perhapsmost valuable. The agreement of the coroner is required in thevast majority of cases where the potential for organ donationexists. It is reasonable to discuss all potential patients with thecoroner.
Exclusion CriteriaThese are identical to organ donation following BSD. Thiopentonelevels, where applicable must be less than 5 mg/l (equivalent toBSD criteria).
ConsentEvery attempt will be made to ascertain the patient’s wishes withrespect to organ donation. Unless NHBD has support of all thefamily, then it would not be pursued, assurances are given thatthey may change their minds at any time. Premortem bloodsampling and systemic heparinisation are specifically addressed.A detailed explanation relating to the withdrawal of life sustainingtherapies and possible stand-down after 90 minutes will be given.Information is given on which organs may be retrieved and thesubsequent care of the deceased.
Time Out ProcessThe participants will be the senior clinician and nursing staff fromthe ICU, the transplantation retrieval team and theatre staff. Theobjectives are to clarify roles and ensure the requisite equipmentis available. It is essential that any staff member who may havepersonal or ethical difficulties with organ donation be given theopportunity to abstain and allow a replacement be found.
Premortem InterventionsThe patient will be heparinised, standard dosages are 300unit/kg. The patient may remain in the ICU or be transferred to anappropriate area with privacy for family members wherewithdrawal of life-sustaining therapies will occur.
The Withdrawal ProcessMechanical ventilation and inotropic support will be withdrawn,sedative infusions will not be weaned. The ICU doctor willadminister sedative, analgesic or antisialogogue medications asappropriate to optimise patient comfort. The patient’s vital signswill continue to be monitored and recorded from when life-sustaining therapies are withdrawn to the time of death. If deathdoes not occur within 90 minutes from the withdrawal of life
sustaining therapies then it is reasonable to stand-down organdonation as the dying process may be prolonged.
The Determination of deathThis will be in accordance with the Academy of Medical RoyalColleges Criteria 2008.14 Asystole is defined as “absent or nearabsent electrical activity with no evidence of cardiac output” i.e.absent peripheral pulsation or arterial line trace. Death is certifiedafter 5 minutes of monitored asystole, pulselessness, apnoea,absent pupillary reactions, corneal reflexes and absent responseto supraorbital pressure.
Stand-down timeThis is a second 5 minute period after the diagnosis of death. Inthis time the patient continues to be monitored for breathingmovements or return of an arterial waveform. Should this occur, afurther observation period of 5 minutes is mandatory after thisactivity has disappeared, before proceeding with organ donation.This stand-down time maybe used to transfer the patient to thetheatre where sterile preparation and draping may begin. Noincision will be made until this 5 minute stand down has elapsed.
Care of the body of the deceased patientThe remains of the deceased patient are cared for in accordancewith current practice. The patient’s family may wish to spend timewith the deceased before the remains are taken to the mortuary.
Education, Audit and Clinical GovernancePerhaps the key to success is education through lectures, smallgroup sessions and the widespread dissemination of a locallyagreed policy on NHBD. Some have ethical concerns with respectto NHBD: specifically the determination of futility, blood samplingand heparin administration. Agreement must be reached betweenat least three consultants with respect to futility. All patients haveintravascular access for blood sampling and volumes of blooddrawn are small. There is no evidence that heparin at the time ofwithdrawal of life sustaining therapies has any impact on thepatient or shortens the patient’s life.15 Regular in-service sessionsand in particular ‘after event reviews’ are especially helpful in ourown experience to promote NHBD. In all hospitals considering aNHBD program, an oversight committee should be established.The local ethics committee as well as other managementstructures may need to approve the protocol. Finally, there shouldbe a clear pathway of audit and clinical governance and theprotocol subjected to regular review.
The intensive care community holds a vital fiduciary role in organdonation on behalf of the lay community. NHBD is nothing new;education, audit, the endorsement of learned bodies and thepublication of national standards will, in time see its phasedreintroduction.
Correspondence: J O’RourkeDepartment of Anaesthesia and Intensive Care Medicine,Beaumont Hospital, Dublin 9Email: [email protected]
References1. Neuberger J, Pfetter P, Tsui S. External Review of Organ
Transplantation services in Ireland: October 2011. IKA SupportMagazine, Winter2011.http//issuu.com/ikasupport/docs/supportmagwinter2011(accessed 23 January 2013).
2. Dubois JM, DeVita M. Donation after cardiac death in the UnitedStates: How to move forward. Crit Care Med 2006; 34:3045-3046.
3. Summers DM, Johnson R, Allen J, Fuggle SV, Collett D, Watson CJ,Bradley JA. Analysis of factors that affect outcome aftertransplantation of kidneys donated after cardiac death in the UK: acohort study. Lancet 2010; 376:1303-11.
4. Cooper JT, Chin L, Kreiger NR, Fernandez LA, Foley DP, Becker YT,Odorico JS, Kalayoglu M, Sollinger HW, D’Alessandro AM. Donationafter Cardiac Death: The University of Wisconsin Experience withRenal Transplantation. Am J Transplant 2004; 4: 1490-4.
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 187

188 Occasional Piece / Letter to the EditorIr
ish
Med
ical
Jou
rnal
Jun
e20
13Vo
lum
e10
6N
um
ber
6w
ww
.imj.i
e
5. Rudich SM, Kaplan B, Magee JC, Arenas JD, Punch JD, Kayler LK,Merion RM, Meier Kreische HU. Renal Transplantation performedusing non-heart beating organ donors: going back to the future.Transplantation 2002; 74: 1715-1720.
6. De Oliveira NC, Osaki S, Maloney JD, Meyer KC, D’Alessandro AM,Love RB. Lung Transplantation with donation after cardiac deathdonors: Long-term follow up in a single centre. J Thorac CardiovascSurg 2010; 139: 1306-15.
7. Erasmus ME, Verschuuren EA, Nijkamp DM, Vermeyden JW, Van DerBij W. Lung Transplantation from non heparinised category III non-heart-beating donors. A single-centre report. Transplantation 2010;89: 452-7.
8. Mason DP, Murthy SC, Gonzales–Stawinski GV, Budev MM, MehtaAC, McNeill AM, Pettersson GB. Early experiences with lungtransplantation from donors after cardiac death. J Heart LungTransplant 2008; 27: 561-3.
9. Taner CB, Bulatoo IG, Willingham DL, Perry DK, Sibulesky L,Pungpapong S, Aranda-Michel J, Keaveny AP, Kramer DJ, NguyenJH. Events in procurement as risk factors for ischemic cholangiopathyin liver transplantation using donation after cardiac death donors. LiverTranspl 2012; 18: 101-112.
10. De Vera ME, Lopez Solis RC, Dvorchik I, Campos S, Morris W,Demetris AJ, Fontes P, Marsh JW. Liver transplantation using donation
after cardiac death donors: long term follow up from a single centre.Am J Transplant 2009; 9: 773-781.
11. Nguyen JH, Bonatti H, Dickson RC, Hewitt WR, Grewal HP,Wilingham DL, Harnois DM, Schmitt TM, Machicao VI, Ghabril MS,Keavney AP, Aranda-Michel J, Satyanarayana R, Rosser BG, HinderRA, Steers JL, Hughes CB. Long term outcomes of donation aftercardiac death liver allografts from a single center. Clin Transplant2009; 23: 168-173.
12. Koostra G. Statement on non-heart beating donor programs.Transplant Proc 1995; 27: 2965.
13. Young GB. Neurological prognosis after cardiac arrest. N Engl J Med2009; 361: 605-11.
14. Sir Liam Donaldson Chief Medical Officer. A Code of Practice for thediagnosis and confirmation of death. Academy of Medical RoyalColleges. 2008. http/www.aomrc.org.uk/publications/statements(accessed 23 January 2013).
15. Bernat JL, D’Allesandro AM, Port FK, Bleck TP, Heard SO, Medina J,Rosenbaum SH, DeVita MA, Gaston RS, Merion RM, Barr ML, MarksWH, Nathan H, O’Connor K, Rudow DL, Leichtman AB, Schwab P,Ascher NL, Metzger RA, McBride V, Graham W, Wagner D, Warren J,Delmonico FL. Report of a national conference on donation aftercardiac death. Am J Transplant 2006; 6: 281-291.
Are Girls with Turner Syndrome Obese?Sir
Girls with TS may experience high body mass index. Whether highbody mass index in those with Turner syndrome are due tooverweight or short stature is unclear. We examined weight,height and body mass index in 32 girls with Turner syndrome.Obesity has been reported in those with Turner syndrome (TS)1-3.We aim to examine whether patients with TS who have higherbody mass index (BMI), compared with general population, areobese or just short. BMI in 32 girls with TS aged over 12 yearswas examined. Height and weight were measured. Ethicalapproval was obtained from our local hospital ethics committee.BMI was calculated using the following equation: BMI= weight(Kg)/height (m)2. The SPSS for Windows software, version 21.0was used for data analysis. Descriptive statistics were measured.t-Test was used to compare the mean between the groups.
Structural X abnormalities were the commonest chromosomalabnormalities (14/32; 43.75%). Mean (SD) height (cm) was148.26 (9.01) cm. Of 32 girls, the majority of girls (28/32; 87.5%)received growth hormone (GH). With respect to weight,comparison between girls with TS and age- and sex-matched Irishgeneral population4 was performed. Weight did not differsignificantly between patients with TS (mean 54.9 kg; SD 15.71)and general population (mean 52.9; SD 6.5), (p value 0.52).Compared with age-matched Irish general population4, subjectswith TS were shorter, with height SDS being -2.1 (p value 0.00).Mean (SD) BMI was 25.02 (6.73), with mean BMI-SDS (0.68)being significantly higher than 0 (p value 0.002). Mean (SD) BMIdid not differ significantly between girls with monosomy 45, X
[24.91 (2.94)], those with mosiacism sex chromosome withoutstructural abnormalities [23.19 (2.63)] and individuals with Xstructural abnormalities with or without mosiacism [24.81 (6.4)], (pvalue 0.79).
We found that girls with TS, of whom the majority received GH,have similar weight, but higher BMI, compared with age- and sex-matched general population. Girls with TS were significantlyshorter, compared with general population. This can explain thehigh BMI in those with TS. In conclusion, high BMI in those withTS may be due to short stature, not to overweight. High BMI inthose with TS should be interpreted in the context of short stature.
M Nadeem, EF RochePaediatric Department, Trinity College Dublin, AMNCH, Tallaght,Dublin 24Email: [email protected]
References1. Donaldson MD, Gault EJ, Tan KW, Dunger DB. Optimising
management in Turner syndrome: from infancy to adult transfer, ArchDis Child 2006;91:513-20.
2. Bondy CA; Turner Syndrome Study Group. 2007, Care of girls andwomen with Turner syndrome: a guideline of the Turner SyndromeStudy Group, J Clin Endocrinol Metab 2007;92:10-25.
3. Gravholt CH, Juul S, Naeraa RW, Hansen J. Morbidity in TurnerSyndrome. J Clin Epidemiol 1998;51:147-15.
4. Hoey HM, Tanner JM, Cox LA. Clinical growth standards for Irishchildren. Acta Paediatr Scand Suppl 1987;76:1-31.
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 188

189Book Reviews
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
ABC of Ear, Nose andThroatEditors: Harold S. Ludman, Patrick J. BradleyPublisher: WileyISBN: 978-0-470-67135-1Price: $45.95
I have many fond memories of using the ABC series of booksas a medical student. Indeed if I am not mistaken I think aformer version was my first ENT textbook as a fourth medstudent!! This volume is edited by two bastions of EnglishENT and indeed the contributing authors comprise animpressive list in itself.
The chapter topics are very well structured. I especially likethe clinically relevant topics such as – “Pain in the ear”,“Throat pain”, “Facial pain” – as these bring together clinicallycommon presentations under one heading. Particularlyrelevant in this age of problem based learning.
In an ever expandingera ofsubspecialisation, it’sa difficult task towrite and indeed edita book coveringENT. From skull basesurgery to facialplastics – manymedical studentscan find itbewildering.However the authorsof this textbook haveavoided this for themost part due to useof well constructedtables and medicalimages. Indeedsome Junior ENTtrainees would derive benefit from using this as a study guidee.g. Acoustic Neuromas – surgical management, FacialPlastics. It is mentioned in the Preface that ENT can accountfor a substantial fraction of GP consultations. Chapters suchas “Hearing impairment in Children”, “Vertigo and Imbalance” Ifeel would be excellent reference guides to the busy GPtrying to reassure and inform an ever increasingly “Google”knowledgeable clientele.
The one slight niggle would be the relative paucity ofpaediatric ENT detail when compared to the space given toadult conditions e.g. Airway Obstruction and Stridor. HoweverI realise that this again can be extremely difficult to achieve ina text trying to appeal to a broad base.
In summary, I would strongly recommend this text to medicalstudents, nursing graduates perhaps considering becomingadvanced practitioners in ENT and GP’s. Other allied healthprofessionals indeed would also find parts of it extremelyhelpful.
Hopefully it will take its well earned place in the timehonoured “ABC” slot on the shelf; easily accessible for thatlast minute bit of pre exam preparation!
MP ColreavyDepartment of Otolaryngology, Head and Neck Surgery,Mater and Children’s University Hospitals, Dublin
ABC of Breast Diseases FourthEditionEditor: J Michael DixonPublisher: Wiley-BlackwellISBN: 978-1-4443-3796-9Price: $46.95
ABC of Breast Disease is a concise book summarising the currentmanagement of breast disease. This is the fourth edition of a seriespublished over the last 17 years. There are 17 chapters withcontributions from Surgeons, Oncologists, Radiologists, Pathologists,Geneticists, Psychologists and Statisticians, providing representationfrom every division of the multidisciplinary environment in whichbreast disease is managed today. Each chapter addresses a differentarea of breast cancer management and contains a summary/overviewof the main teaching points to focus the reader’s attention.
The chapters are well written and the text is enhanced withappropriate use of tables, graphs, clinical photographs andradiological images which lead to a visually appealing layout. Thechapter subjects are well selected with little overlap betweenchapters; the topics covered include epidemiology of breast cancer,genetics, screening, psychological aspects of breast disease, breastreconstruction, and assessment and management of benign andmalignant breast disease. The update of this text is timely as the pastfew years have seen the publication of potentially practice changingtrials in the surgical management of breast cancer, particularly inrelation to axillary disease. Additionally, systemic therapy for breastcancer is constantly evolving and there is an excellent chapter on therole of systemic treatment of primary operable breast cancer whichsummarises concisely much of the data amassed from years ofclinical trials in breast cancer treatment upon which our current use ofchemotherapy and targeted therapies is based. Given the breadth ofexpanding literature in this area, it is appropriate that this book beupdated at regular intervals in order to remain evidence-based.
This text will be of significantinterest to the generalpractitioner dealing with benignbreast disease and follow-up ofbreast cancer patients in thecommunity. Indeed the authorshave stated a specific aim ofmaking this book of practicaluse to doctors in primary careby the inclusion of topics suchas referral guidelines. Thecaveat here is that Irishpractitioners must be awarethat the National CancerControl Programme (NCCP)referral guidelines and breastscreening guidelines aredistinct from the UK guidelinesdocumented in the text.
The book is also likely to be useful for hospital-based practitionerswho may use the book as a resource for refreshing one’s memory onthe evidence for selection of systemic therapy and also for educatingjunior staff and medical students on the many aspects of breastdisease. This book would be appropriate to have available in anysymptomatic breast unit and is an excellent example of concise,informative and evidence-based text.
A Lowery, ADK HillBeaumont Hospital, Beaumont, Dublin 9
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 189

www.pulsejobs.com
• 52% of our Doctors joined PULSE viarecommendation from their colleagues
• Attractive rates of pay• We have dedicated Recruitment Consultants
that specialise in your grade and sub-specialty• Our 24/7 On-call services mean we can offer
you even more opportunities
Building relationships is central to whatwe do. That’s why Doctors choose PULSE.
Why is PULSE the number one Locum agency inPsychiatry?
In Psychiatry we’re the best
• A&E• General Medicine• Paediatrics• Surgery• Anaesthetics• General Practice
Due to exceptionally high demand in the NHS (England, Wales &Scotland) we have country wide locum opportunities in Acute & GPprimary care environments. With both short term & long termpositions in every discipline. The following are areas of high demand:
Oneleading agency,two great opportunities
UK wide LocumOpportunities for Acute
Doctors and GPs!
PULSE can also give you: • Access to Revalidation Services• Daily Payroll• Recommendation Bonus -
earn £250 for every friendyou refer to us*
• NHS Trusts and various PrivateOrganisations rely on us
• At PULSE we have direct access tomore jobs than any other agency
Get connected today:
0044 1992 [email protected]
To register with PULSE Doctors orPULSE GPs contact us today:
0044 161 245 [email protected]
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 190

Non-Pulmonary Chronic Diseases inAdults with Cystic Fibrosis: Analysisof Data from the Cystic FibrosisRegistry
R Somerville, A Jackson, S Zhou, G
Fletcher, P Fitzpatrick. Ir Med J. 2013; 106:
166-8.
Question 1
The number of patients on the CF registryis
a) 1-300b) 301-600c) 601-900d) 901-1200e) 1201-1500
Question 2
The proportion of adult CF patients withdiabetes is
a) 1-6%b) 7-13%c) 14-20%d) 21-27%e) 28-34%-
Question 3
The proportion of adult CF patients withbone disease is
a) 1-10%b) 11-20%c) 21-30%d) 31-40%e) 41-50%-
Question 4
The proportion of adult CF patients withliver disease is
a) 1-5%b) 6-10%c) 11-15%d) 16-20%e) 21-25%
Question 5
The proportion of children CF patients withdiabetes is
a) 1-2%b) 3-4%c) 5-6%d) 7-8%e) 9-10%
A Profile of Elderly Fallers Referredfor Physiotherapy in the EmergencyDepartment of a Dublin TeachingHospital
F Crehan, D O’Shea, JM Ryan, F Horgan. Ir
Med J. 2013; 106: 173-6.
Question 1
The mean age of the patients was
a) 65-70 yearsb) 71-75 Yearsc) 76-80 yearsd) 81-85 yearse) 86-90 years
Question 2
The proportion of patients with poor gripstrength was
a) 50-55%b) 56-60%c) 61-65%d) 66-70%e) 71-75%
Question 3
The proportion of patients with slowwalking speed was
a) 20%b) 40%c) 60%d) 80%e) 100%
Question 4
The proportion of patients living alone was
a) 55-60%b) 61-65%c) 66-70%d) 71-75%e) 76-80%
Question 5
The proportion of female patients was
a) 60-65%b) 66-70%c) 71-75%d) 76-80%e) 81-85%
Presentation and Management ofGastrointestinal Stromal Tumours
AM Mongan, V Malik, S Rowley, Z Claxton,
C Muldoon, D O’Toole, N Ravi, JV
Reynolds. Ir Med J. 2013; 106: 176-9.
Question 1
The number of cases of gastrointestinalstromal tumours was
a) 50-60b) 61-70c) 71-80d) 81-90e) 91-100
Question 2
The proportion of patients treated withsurgery was
a) 50%b) 60%c) 70%d) 80%e) 90%
Question 3
The 5 year survival rate was
a) 65-70%b) 71-75%c) 76-80%d) 81-85%e) 86-90%
Question 4
The proportion of patients who receivedImatinib was
a) 5-10%b) 11-15%c) 16-20%d) 21-25%e) 26-30%
Question 5
The proportion of patients with arecurrence was
a) 5%b) 10%c) 15%d) 20%e) 25%
191Continuing Professional Development
Iris
hM
edic
alJo
urn
alJu
ne
2013
Volu
me
106
Nu
mb
er6
ww
w.im
j.ie
Continuing Professional Development
To receive CPD credits, you must complete the question online at www.imj.ie.
92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 191

92031-IMJ JUNE 2013_TF 10/06/2013 08:32 Page 192