Embed Size (px)
Citation preview

JOINT PATHOLOGYJOINT PATHOLOGY
FERDA ÖZKAN M.D.
YEDITEPE UNIVERSITY MEDICAL FACULTY

OBJECTIVESOBJECTIVES
Review joint structure
Explain inflammatory processes of Joints
Describe types of arthritis

JOINTSJOINTS
Nonsynovial- (solid)- synarhtoses: Lack joint space-fibrous synarthroses -synchondroses
Synovial- have joint space

Synovial JointSynovial Joint

Synovial JointsSynovial Joints
The boundry of the joint space is formed by the synovial membrane
Two types of synovial cells
Type A- (macrophage like) phagocytic and synthetize hyaluronic acid
Type B- (fibroblast like) produce various proteins

SYNOVIOCYTESSYNOVIOCYTES

ARTICULAR HYALINE ARTICULAR HYALINE
CARTILAGECARTILAGE
Articular hyaline cartilage is composed of type 2 collagen, water, proteoglycans and chonrocytes.
The water and proteoglycans give hyaline cartilage its turgor and elasticity and limit friction.

Chondrocytes synthetize the matrix as well as enzymatically digest it
Matrix turnover is controlled as chondrocytes secrete the degenerative enzymes in an inactive form and enrich the matrix with enzyme inhibitors

Cytokines such as IL-1 and TNF trigger degradative process
The source of cytokines include
-Chondrocytes-Synoviocytes-Inflammatory cells

CHRONIC INFLAMMATORY CHRONIC INFLAMMATORY SYNOVITIS SYNOVITIS

Arthritis - IntroductionArthritis - Introduction
Inflammation of joints - CommonCommon site for autoimmune
injury– Heart valves & Joints - damage –
Exposure of hidden antigens.Infections.Degeneration – Age/Stress/life
style
Use it or Loose it….!

Arthritis – Clinical features:Arthritis – Clinical features:
Pain Inflammation - capsule, synovium,
periosteum. Swelling:
inflammation, effusion, proliferation. Restricted movement
pain, fluid, synovial swelling, damage.
Deformity mal-alignment, erosion, ankylosis

18.04.23
Arthritis Clinical Arthritis Clinical Classification:Classification:Monoarthritis:
– Local, asymmetric, secondary.– Acute: Bacterial, Trauma,
Crystal, Reactive– Chronic :Tuberculosis, Lyme,
Fungal, Trauma, Tumors.Polyarthritis:
– Chronic, symmetric, systemic.– Autoimmune, degenerative,
Crystal.– Rarely infective.

18.04.23
Polyarthritis ClassificationPolyarthritis Classification::
Autoimmune: – Rheumatoid,Ankylosing
spondilitis, Psoriatic , Reiter’s syndrome, enteropathic
Degenerative: Osteroarthritis Crystal Deposition:
– Gout – Monosodium urate– CPPD - Pseudo Gout
Infective - Septic, TB, Lyme etc. rare.

Rheumatoid Arthritis

RHEUMATOID RHEUMATOID ARTHRITISARTHRITISAutoimmune chronic systemic
inflammatory disorder Attacks joints, causing a
nonsuppurative proliferative inflammatory synovitis
Destruction of articular cartilage and ankylosis of the joints

RHEUMATOID RHEUMATOID ARTHRITISARTHRITIS Symmetric, small joints Usually in hands
metacarpophalangeal and proximal interphalangeal joints
Feet, wrists,ankles, elbows and knees
Joints swollen, warm, painful particulary in the morning or following inactivity

Epidemiology of RAEpidemiology of RA
Prevalence about 1-3% of population
Female : Male ratio = 3-5:1
Concordance in identical twins 30%


Its pathogenesis is complex and incompletely understood, involving both type III (antigen-antibody complex) and type IV (T helper lymphocyte / macrophage-mediated) hypersensitivity reactions.

PathogenesisPathogenesis
Inciting agent activates immune system immunological reactions immune complexes in synovial fluid activate complement inflammatory response joint destruction.
Earliest change is inflammation and edema of synovium with increased vascularity and increased production of synovial fluid– shows evidence of CD4+ T helper cells
migrating into the joint.

Next steps:– synovial villi hypertrophy, – synovial cells proliferation, – increased vascularisation
(angiogenesis) – pannus form (granulation tissue
that grows across surface of articular cartilage from adjacent synovium).

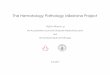
Marked synovial hypertrophy Marked synovial hypertrophy with formation of villi.with formation of villi.

Subsynovial tissue containing Subsynovial tissue containing a dense lymphoid aggregatea dense lymphoid aggregate

Synovial angiogenesis
Tissue section of rheumatoid synovial pannus showing prominent new blood vessel formation

Hyperplastic synovium may spread over and erode into cartilage and bone.
This destructive proliferation of synovium is known as pannus.
Large numbers of inflammatory cells (T and B lymphocytes, plasma cells and macrophages) take up residence within the synovium.
These secrete inflammatory mediators (cytokines, prostaglandins etc.) into the synovial fluid.

This figure demonstrates – destruction of
articular cartilage (open arrow; osteoclastic cells)
– by synovial pannus (solid arrow).
It is thought that the pannus destroys the cartilage by production of metalloproteinases.

Pannus can also destroy bone by recruiting osteoclasts to resorb bone matrix (open arrow).
Osteoclasts are very sensitive to IL1 and TNF, resorbing bone in response to production of these cytokines by the inflammatory cells infiltrating the pannus (solid arrow).

Production of metalloproteinases by synovial cells is induced by the inflammatory cytokines IL1 and TNF- which are both produced by chronically inflamed synovium.
These cytokines also cause synovial cells to proliferate and are probably responsible for the development of pannus.

The muscles waste around the joint Hyperemia develops The joint capsule is distended Destruction of unprotected bone at
joint margin and subchondral bone by pannus
Later leading to marked joint damage and capsular laxity
Leading to deformity and fibrous ankylosis
Eventually bony ankylosis of the joint.

N.Synovium - - R.Arthritis:N.Synovium - - R.Arthritis:

RA - Pannus:RA - Pannus:
Hyperplastic Hyperplastic inflammed inflammed synoviumsynovium

Skin RA Nodule:Skin RA Nodule:

Skin RA Nodule:Skin RA Nodule:

Rheumatoid Nodule (skin):Rheumatoid Nodule (skin):
PalisadingPalisadingMacrophagesMacrophages
CentralCentralFibrinoidFibrinoidNecrosisNecrosis

Subcutaneous rheumatoid nodule with an Subcutaneous rheumatoid nodule with an area of necrosis surrounded by a palisade area of necrosis surrounded by a palisade of macrophages and scattered chronic of macrophages and scattered chronic inflammatory cells.inflammatory cells.

Joint involvement in RA:Joint involvement in RA:

Swan Neck Deformity in RA:Swan Neck Deformity in RA:

Joint Destruction in RA:Joint Destruction in RA:
Swan NeckDeformity

RA Joint destruction, RA Joint destruction, ankylosis:ankylosis:

EExtraarticular manifestationsxtraarticular manifestations Weight loss, malaise and fever; Lymphadenopathy Skin (rheumatoid nodules – in 50%, at
periarticular positions subject to high external pressure; inflammatory granulomatous lesions; vasculitis (leukocytoclastic vasculitis and palpable purpura)
Eye (keratoconjunctitis, scleritis, episcleritis) Respiratory (pleurisy, pleural effusions,
interstitial fibrosis, rheumatoid nodules, bronchiolitis)
Cardiac (pericardial effusion, pericarditis, myocarditis, endocarditis, valvular heart disease)
Peripheral nerves: nerve compression by synovitis or tenosynovitis, syndrome of mononeuritis multiplex.

Gastrointestinal (adverse effects from drugs)
Renal (amyloidosis, drug induced nephropathy, renal tubular acidosis)
Neurologic (entrapment syndromes – especially carpal tunnel, peripheral neuropathy from vasculitis – sensory and motor, mononeuritis multiplex)
Hematologic (anemia, leucopenia, lymphoma, thrombocytosis)
Hand deformities (fusiform swelling spindle shape to fingers)
Cervical spine involvement.

Juvenile Rheumatoid Juvenile Rheumatoid Arthritis:Arthritis:
Before age 16 Multisystem involement -
Spleenomegaly, Starts with systemic involvement
unlike RA. No serum RA Factor – Seronegative Antinuclear Antibody (ANA) +ve
autoimmune.

Juvenile Rheumatoid Juvenile Rheumatoid ArthritisArthritis
Still (1887) : rheumatoid arthritis in children
Common connective tissue disease in children age 15 or less, 65% male.
Either oligoarticular (<5 joints), polyarticular (5 or more joints) or systemic.
Compared to classic rheumatoid arthritis, oligoarthritis is more common; – systemic large joints are affected more than
small joints, – no rheumatoid nodules are present, – no rheumatoid factor is present, – ANA positive.



Associated with HLA-DRB1, infections by mycobacteria, bacteria, viruses.
70% recover– 10% have residual severe joint deformities
Symptoms: systemic onset with fever, rash, hepatosplenomegaly, generalized lymphadenopathy, serositis; also warm and swollen joints; pericarditis, myocarditis, pulmonary fibrosis, glomerulonephritis, uveitis, growth retardation.
Sites: knees, wrists, elbows, ankles. Micro: similar morphologic changes as
rheumatoid arthritis.

Seronegative Seronegative spondyloarthropathyspondyloarthropathy Inflammatory joint diseases that all
share a common pathology and strong association to the HLA-B27 antigen and are negative for rheumatoid factor (seronegative).
Used to be referred to as variants of rheumatoid arthritis as they share many pathologic and radiologic features with rheumatoid arthritis. – ‘Spondylos’ is Greek for vertebrae.

Ankylosing Spondylitis (Marie-Strumpell’s disease)
Psoriatic Arthritis (PsA)Reactive Arthritis (ReA)
(Reiter’s syndrome)Enteropathic Spondylitis
(Enteropathic synovitis)Undifferentiated spondylitis

Ankylosing SpondylitisAnkylosing Spondylitis (Marie-Strumpell’s disease)(Marie-Strumpell’s disease) Chronic inflammatory disorder primarily affecting
the axial skeleton Affected joints tend to fibrosis and ankylosis. Cause unknown,
– Strongly associated with HLA-B27 histocompatibility antigen (90%)
Affects up to 1% of population– Affects teenage boys
Chronic synovitis destroys articular cartilage and causes bony ankylosis
Inflammation of tendinoligamentous insertion sites cause osteophytes.
Symptoms: low back pain that gets progressively.

AS - fusion of vertebral AS - fusion of vertebral bodies due to bridging bodies due to bridging ssyndesmophytes.yndesmophytes.

Scoliosis in Ankylosing Scoliosis in Ankylosing SpondylitisSpondylitis

Psoriatic Arthritis (PsA)Psoriatic Arthritis (PsA)
Inflammatory arthritis in 2-7% of those with psoriasis (psoriasis affects 1-2% of population).
Most have previous long history of psoriasis– all forms of psoriasis can develop
arthritis. High association with HLA-B27
and HIV infection.

Reactive Arthritis (ReA)Reactive Arthritis (ReA) (Reiter’s syndrome)(Reiter’s syndrome)
Post-infectious disorder (not a local infection, but a reaction).
Classic triad (Reiter – 1916) of arthritis, urethritis and conjunctivitis following infection. – Reiter’s syndrome is now
not the preferred name (Reiter was involved with Nazi politics and medical experiments).
Syndrome now considered consisting of:1) Arthritis (asymmetric) 2) Urethritis(mild)3) Conjunctivitis (mild)4) Mucocutaneous lesions (oral erosions/ulcers).

Reiter’s Syndrome: Reiter’s Syndrome: conjunctivitisconjunctivitis

Reiter’s Reiter’s Syndrome Syndrome ::IritisIritis

Reiter’s SyndromeReiter’s Syndrome : Urethritis : Urethritis

Organisms in Reiter’sOrganisms in Reiter’s
Shigella FlexneriSalmonellaS.typimurium – othersYersinia enterocoliticaCampylobacter JejuniChlamydia trachomatisUreaplasma urealyticum

Enteropathic Spondylitis Enteropathic Spondylitis (Enteropathic synovitis)(Enteropathic synovitis) Joint manifestations associated with
chronic inflammatory bowel diseases:– ulcerative colitis– Crohn’s disease.
Can also be associated with intestinal bypass surgery (bypass arthritis-dermatitis syndrome), infectious gastroenteritis, pancreatic disease, biliary cirrhosis, coeliac disease (gluten sensitive enteropathy) and Whipple’s disease.

Undifferentiated spondylitisUndifferentiated spondylitis
Patients who have some of the features of seronegative spondyloarthropathy, but do not meet the criteria for the well recognised conditions.
They may be an early stage of a known spondyloarthropathy, an atypical variant of a known spondyloarthropathy or an unknown type of spondyloarthropathy.

Hemophilic arthropathyHemophilic arthropathy Common feature of hemophilia
– more common in knee, ankle and elbow Hemorrhage induces a synovial proliferation,
chronic inflammation release of degradative proteinases joint damage.
Recurrent bleeding irreversible damage.Stages of the disease: Stage 1 – acute hemoarthrosis in child when
begin to walk Stage 2 – subacute or chronic arthritis Stage 3 – end-stage arthropathy (chronic
destructive arthropathy with joint instability, fibrous ankylosis, osteophytic overgrowth)

OsteoarthritisOsteoarthritis
Degenerative joint disease (osteoarthritis) Progressive erosion of articular cartilage
associated with aging, trauma, occupational injury
Usually age 50+ years (present in 80% at age 65 years)
Cartilage degradation may be mediated by IL-1 Sites: men in hips, women in knees and hands;
usually one joint or same joint bilaterally, at least initially
Symptoms: pain worse with use of joint, crepitus, limited range of motion, nerve root compression; Heberden nodes in fingers of women only (osteophytes at DIP joints).

OsteoarthritisOsteoarthritis

OsteoarthritisOsteoarthritis
Degenerative joint disease ( wear and tear)
Insidious disease affecting elderly
Deep achy pain worsen with use, morning stiffness, crepitus, and limitation of movement

Xray: deformity of joint with loss of
bone substance and cartilage, loss of joint space, migration of joint, osteophyte formation, sclerosis of subchondral bone, subchondral bone cysts.

Gross: – sloughing of cartilage, – bone eburnation (friction smooths and burnishes
the exposed bone to resemble ivory), – joint mice (dislodged pieces of cartilage and
subchondral bone), – cysts (synovial fluid forced into fractures via ball-
valve-like mechanism), – osteophytes (bony outgrowths at margins of
articular surface), – pannus (fibrous synovium that covers periphery
of articular surface) Loose body: may form if portion of articular
cartilage breaks off; has the tide mark of articular cartilage,
normally loose body is nourished by synovium and continues to grow, has a tree ring appearance; no clumped atypical chonodrocytes; no unevenly distributed chondrocytes.


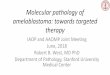
Severe osteoarthritis with small islands of residual articular cartilage next to exposed subchondral bone.
1, Eburnated articular surface.2, Subchondral cyst. 3, Residual articular cartilage.

Micro: – ghost chondrocytes (no nuclei) or
necrotic chondrocytes; – irregular thinning, fragmentation
and fibrillation of thinned cartilage; – subchondral cysts with mucoid fluid
surrounded by sclerotic bone; – advanced cases have synovial
hyperplasia with lymphoid follicles.

NormalNormal -- Femur Head -- -- Femur Head -- OAOA
Normal Osteoarthritis

Femur Osteroarthritis:Femur Osteroarthritis:

Joint Mice or Loose Bodies:Joint Mice or Loose Bodies:

Spine Osteophytes (OA):Spine Osteophytes (OA):

OsteoarthritiOsteoarthritis:s:•Narrow joint space•Lipping – osteophyte
•Dislocation•Osteoporosis.

Osteophyte formation:Osteophyte formation:

Bone cysts in OA:Bone cysts in OA:

Osteoarthritis: AnkylosisOsteoarthritis: Ankylosis
varus deformity of the knee and collapse of the joint space with destruction of the medial cartilage and the subchondral cortex (open arrowheads).

Osteoarthritis:Osteoarthritis:
Lateral view of the left knee shows sclerosis with marked osteophyte formation (arrows). The osteophytes are best seen in this view.

Differentiating Differentiating Features:Features:
Rheumatoid Arthritis:Rheumatoid Arthritis: Young, small joints Autoimmune. Synovial Inflammation synovium Cartilage
Osteoarthritis:Osteoarthritis: Old, Large joints Degenerative. Cartilage
degeneration. Cartilage Synovium

GoutGout Arthritis Arthritis
Gout is a chronic disease, but it is characterised by episodes of acute inflammation of affected joints.
These episodes cause often dramatic pain and swelling of the affected joint and surrounding soft tissues

In gout the inflammatory stimulus is deposition of urate crystals in joints in individuals who have raised serum levels of urate due to a variety of causes.
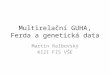
Deposits of monosodium urate crystals surrounded by inflammatory cells (mainly macrophages) which produce IL-1 in response to these crystals.

Pathogenesis of Gouty Pathogenesis of Gouty ArthritisArthritis

Big Toe in Gout:Big Toe in Gout:

Joint Destruction in Gout:Joint Destruction in Gout:

Big Toe in GoutBig Toe in Gout

Gout Tophi:Gout Tophi:

Gouty TophusGouty Tophus

Urate Crystals (Gout):Urate Crystals (Gout):

Pseudo GoutPseudo Gout
• Calcium PyroPhosphate Deposition diseaseCalcium PyroPhosphate Deposition disease• CPPDCPPD• Chondrocalcinosis.Chondrocalcinosis.

Calcium pyrophosphate crystal Calcium pyrophosphate crystal deposition diseasedeposition disease
Pseudogout, chondrocalcinosis. Common finding in arthritic joints (age 50+ years,
30% of patients are at least 85 years old) Calcium pyrophosphate crystals (chalky white
deposits) develop first in menisci and intervertebral discs, may seed the joint and elicit neutrophilic response.
- Knee is common site; 50% have involvement of several joints at diagnosis
50% get significant joint damage. Secondary to the prior joint damage:
hyperparathyroidism, hemochromatosis, hypomagnesemia, hypothyroidism, ochronosis, diabetes mellitus
Microscopy: small rectangular (rhomboid) crystals that are weakly positive birefringent; may have histiocytic and giant cell reaction around these crystals.

CPPD-Arthritis (pseudo gout):CPPD-Arthritis (pseudo gout):

Pseudo Gout–Pseudo Gout–Calcium Calcium pyrophoshatepyrophoshate

Synovial fluid containing Synovial fluid containing calcium pyrophosphate calcium pyrophosphate crystalscrystals

Arthritis Comparison:Arthritis Comparison:

BursitisBursitis
Bursae are closed, round, flattened sacs that are lined by synovium and separate bare areas of bone from overlapping muscles (deep bursae) or skin and tendons (superficial bursae).
They occur at areas of friction or possible impingement.
When inflamed, – the synovial cells increase in thickness and may
show villous hyperplasia. – Bursal lining eventually may be replaced by
granulation tissue prior to fibrous tissue formation. – The bursa becomes filled with fluid, which is often
rich in fibrin. Hemorrhage sometimes occurs.


Pigmented villonodular synovitisPigmented villonodular synovitis
A benign proliferative disorder of uncertain etiology that affects synovial lined joints, bursae, and tendon sheaths.
Two Forms:– The diffuse form typically involves the large
joints, while the localized form typically occurs around the small joints of the hands and feet.
– The localized form often occurs around tendon sheaths and is then termed giant cell tumor of the tendon sheath.

Pathologic featuresPathologic features
Gross Thickened synovium, with a combination of
villous and nodular proliferation. Two types of villi are present in the diffuse
form, – coarse villi with a "shag carpet" appearance – fine or fernlike villi.
The nodular component is seen predominantly in tendinous or extra-articular lesions.– The nodules are well demarcated and may be
sessile or pedunculated, although they lack a true capsule.


Microscopy Characterized by the presence of
hemosiderin-laden multinucleated giant cells. In addition, lipid-laden macrophages,
fibroblasts, and other large polyhedral-shaped mononuclear cells are present, have abundant cytoplasm, and possess oval nuclei.
Hemosiderin also is found within the surrounding tissues (characteristic pigmented appearance).
The lesions tend to be hypervascular and demonstrate synovial hyperplasia.


"The gem cannot be polished without friction, nor man
perfected without trials or problems (or exams)…!."
--Chinese proverb