Embed Size (px)
Citation preview
Joint Hospital Surgical Grand Round21 Dec 2002
Management of Gallbladder PolypsDr David IP Shing Fai
Department of Surgery
United Christian Hospital
What is a Polypoid Lesion of Gallbladder?PLG
• Any elevated lesions of the mucosal surface of the gallbladder wall
• Definition of PLG by USG:– similar echogenicity to GB wall– project into lumen– fixed– lack displacement– lack acoustic shadow– may or may not have a pedicle
Prevalence of PLG• USA
– 3-7% in healthy subjects
• Denmark– male: 4.6%
– female: 4.3%
• Japan– male: 6.28%
– female: 9.5%
• Chinese– 6.9%
Classification of polypoid lesions of gallbladder
Christensen and Ishak (1970)
1. Benign – True tumors
• adenoma
• Mesodermal: lipoma, leiomyoma, haemangioma
– Pseudotumors• Hyperplasia: adenomyomatosis
• Polyp: inflammatory, cholesterol
2. Malignant– adenocarcinoma
Common types of PLG
• Cholesterol polyp (40-70%)
• Inflammatory polyp
• Adenomyomatous hyperplasia
• Adenoma
• Carcinoma
USG diagnosis of PLG
• Senitivity 90.1% (Yang et al, 1992)• Specificity 93.9% (Yang et al, 1992 )• False -ve:
– thickened GB wall may obscure small polyps– presence of GS mask detection of polyp
• False +ve: Other lesions that may mimic GB polyps– Small GS impacted in GB wall– Thick bile (sludge ball)– Mucosal folds
Natural history of PLG1. Moriguchi et al 1996
– 109 patients with PLG
– FU with USG x 5yrs
– 4 patients received cholecystectomy
– 2 patients died of other causes
– 1 patient developed CA gallbladder, but location different form previous polyp
– rest of patients: size of lesion did not change in 88.3%
– Conclusion• Most polypoid lesions of gallbladder detected by USG are beni
gn
Natural history of PLG
2. Csendes A et al 2001– 111 patients with PLG <10mm – Clinical and USG FU for 71 months (mean)– Result:
• none of the patients developed biliary symptom, gallstone or carcinoma of gallbladder
• 50% similar size
• 23.5% shrank or disappeared
• 26.5% in number or size
Indications for cholecystectomy
1. Possibility of Malignancy/ Malignant change of these lesions
2. Symptoms
Indications for cholecystectomy
Possibility of malignancy– Small polypoid carcinomas can be curatively re
sected, best prognosis– Early detection and differentiation of neoplastic
lesion from non-neoplastic one is important
Features of neoplastic PLG on US
• Solitary lesion
• Diameter >10mm
• Sessile appearance
• Low echogenicity
• Rapid growth
• USG alone cannot definitely distinguish adenocarcinoma from non-neoplastic lesions
Indications for cholecystectomy
Indications for cholecystectomy
Possibility of malignancy– Size of polyp >10mm
• prevalence of malignancy 37-88%– Johnson CD et al 1997– Kubota K et al 1994– Majeed AW et al 1995– Shinkai H et al 1998– Chijiwa K 1994
• cholesterol polyp:– 73% <10mm– 28% >10mm
• Adenocarcinoma– 9% <10mm– 18% 11-15mm– 46% 16-20mm
Indications for cholecystectomy
Possibility of malignancy– Coexist gallstone
• 85% in malignant PLG, 59% in benign PLG– Tinsley AR et al 1975
– Smok G et al 1986
– Bivins BA et al 1975
– Albores-Saavedra J et al 1980
– Edelman DS et al 1993
Indications for cholecystectomy
Possibility of malignancy– Solitary PLG– Sessile lesion
• Ishikawa O et al 1989
– Polyp rapid in size• Hachisuka K et al 1986
• Chijiwa K et al 1994
• Koga A et al 1988
– Old age: >50
Features of non-neoplastic PLG on EUSEndoscopic Ultrasonography
• Demonstrates the fine structure• Cholesterol polyps (95%)
– Echogenic spot– Aggregation of echogenic spots
• Adenomyomatosis– Multiple microcysts– Comet tail artefact
• Other lesions are diagnosed as neoplastic
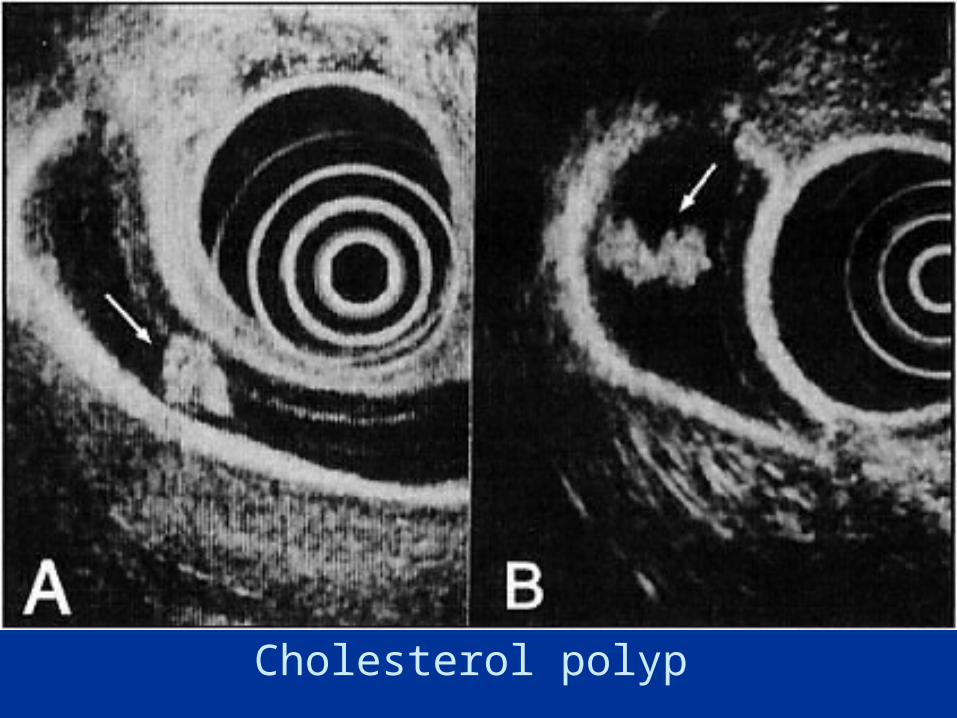
Cholesterol polyp
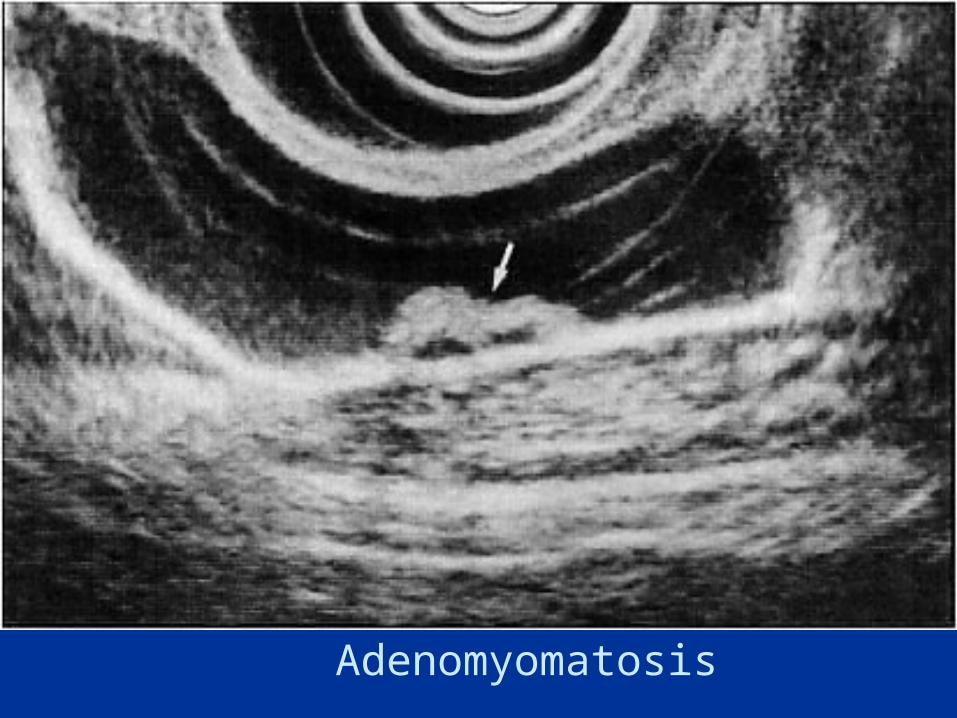
Adenomyomatosis

Carcinoma
• EUS (endoscopic ultrasound) highly accurate for differentially diagnosing polypoid gallbladder lesions (97%)– Sugiyama et al 2000– Azuma et al 2001
Indications for cholecystectomy
Kimura K et al 2001• 46 consecutive patients with pedunculated polypoid
lesions of the gallbladder >10mm diagnosed as non-neoplasms at the initial EUS enrolled in study
• FU EUS• Results:
– No changes in lesions observed in 43/46– Remaining 3 with spontaneous self-detachment of the lesions
• Conclusion:– EUS is useful for determining treatment indications for
PLG– Even the lesions are large, contributes to avoiding
unnecessary surgery
Indications for cholecystectomy
EUS
• Recommended when USG cannot rule out neoplastic lesion
• Save cholecystectomy
Indications for cholecystectomy
• ? Symptoms– abdominal pain, episodic vomiting, bloating, fat
ty food intolerance, dyspepsia– polyp loosen and may obstruct or prolapse into
cystic duct
Symptomatic PLG• Jones-Monahan et al, 2000
– Retrospective review of 45 patients with PLG receiving cholecystectomy
– 93.3% had resolution of symptoms postoperatively with a mean FU 179+/-505 days
• Terzi et al, 2000– All asymptomatic patients had benign PLG whi
le all patients with malignant PLG are symptomatic
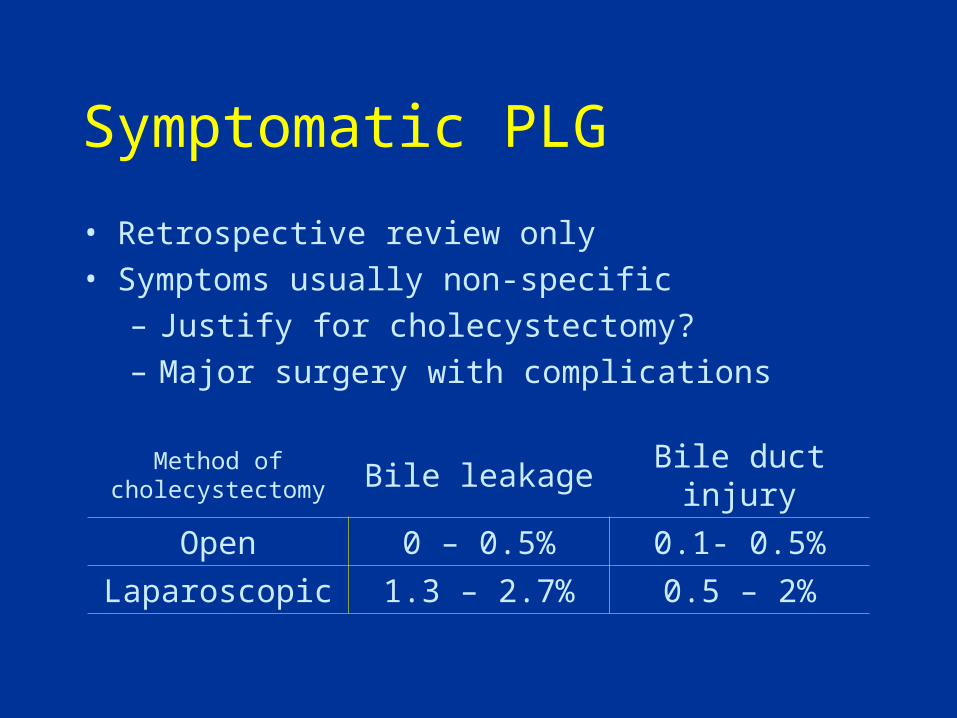
Symptomatic PLG
• Retrospective review only
• Symptoms usually non-specific
– Justify for cholecystectomy?
– Major surgery with complications
Method of cholecystectomy Bile leakage Bile duct injury
Open 0 – 0.5% 0.1- 0.5%
Laparoscopic 1.3 – 2.7% 0.5 – 2%
Conclusion
• Neoplastic lesion detected on USG/ EUS– Cholecystectomy is warranted
• Non-neoplastic PLG on USG/ EUS– Not require cholecystectomy
– Not require regular follow• Natural history
• Majority of these lesion will remain unchanged
• Symptomatic non-neoplastic PLG– Do not recommend cholecystectomy
– Further prospective study
Thank you
• Adenoma carry a risk of developing into adenocarcinoma– Adenoma-carcinoma sequence
• Both adenoma and carcinoma require cholecystectomy
• Distinguishing between these two lesions is not essential to management
Indications for cholecystectomy