Embed Size (px)
Citation preview
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Joint Commission Update
CAMSS State Association ConferenceJune 1, 2017
Client name/ Presentation Name/ 12pt - 2
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Objectives
Identify updates and changes to the survey process
Indicate common standards that could impact the Medical Staff
Provide examples of compliance for common findings on survey

Client name/ Presentation Name/ 12pt - 3
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
SAFER Matrix

Client name/ Presentation Name/ 12pt - 4
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
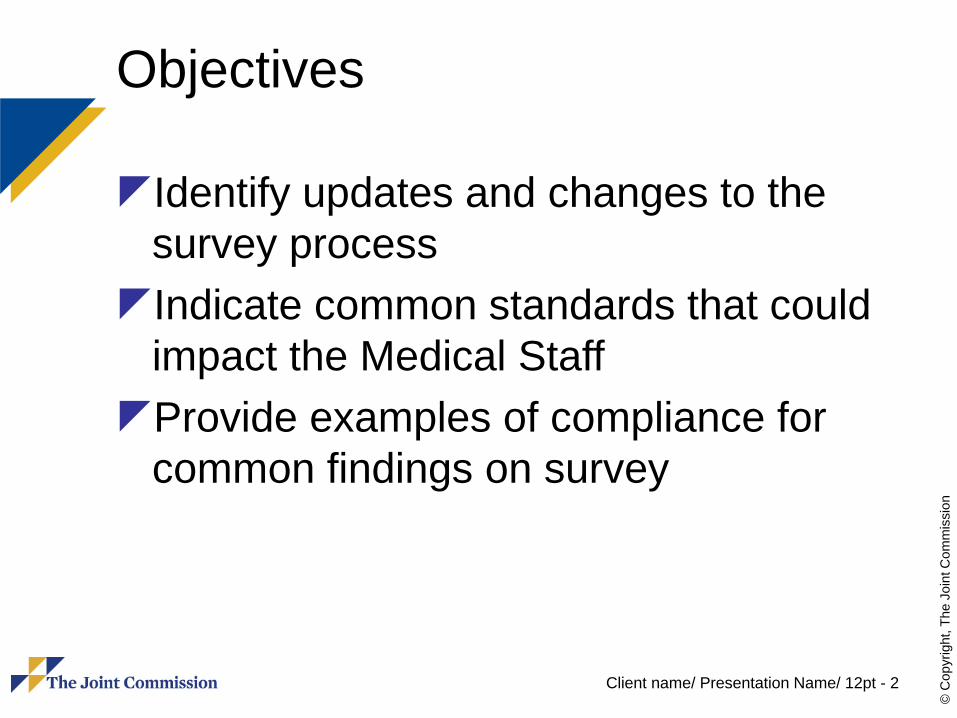
SAFER Matrix
Client name/ Presentation Name/ 12pt - 5
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
SAFER Matrix

Client name/ Presentation Name/ 12pt - 6
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
SAFER Matrix
Client name/ Presentation Name/ 12pt - 7
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Top Three Challenging Medical Staff StandardsMS. 01.01.01, Medical Staff BylawsMS.08.01.01, Focused Professional
Practice EvaluationMS.08.01.03, Ongoing Professional
Practice Evaluation
Client name/ Presentation Name/ 12pt - 8
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Medical Staff Bylaws and MS.01.01.01MS.01.01.01 - Medical staff bylaws
address self-governance and accountability to the governing body. (37 Elements of Performance)
Medical Staff Bylaws must address all Elements of Performance 12 - 36
Client name/ Presentation Name/ 12pt - 9
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Review the Bylaws for each EP 12 – 36 of standard MS.01.01.01
Each element must be included in the bylaws although the detail may be contained in another document (Example: Credentialing Manual)
Any missing element must be scored at that EP plus EP 3
Do the Bylaws describe a Structure (12) for the Medical Staff?
Client name/ Presentation Name/ 12pt - 10
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Membership on the Medical Staff is defined by Qualifications to be a member (13) A process described to delineate privileges and
renewal of privileges (14) Members are assigned to categories of the medical
staff with defined duties and privileges (15) Members that may vote are defined (17) A process described to credential and recredential
membership on the medical staff (26) A process described to appoint and reappoint (27)

Client name/ Presentation Name/ 12pt - 11
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Members may be removed by automatic suspension, summary suspension or termination or reduction of privileges
Indications are described for automatic (28), summary (29) and termination/reduction (30) of privileges
A process is described for automatic (31), summary (32) and termination/reduction (33) of privileges

Client name/ Presentation Name/ 12pt - 12
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Members have a right to appeal decisions through a fair hearing
The process to schedule (34) and conduct (34) a fair hearing is described
The composition of the fair hearing committee is described (35)
Full descriptions may be contained in a Fair Hearing and Appeal Manual

Client name/ Presentation Name/ 12pt - 13
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Officers of the Medical Staff Are listed in the Bylaws (19) A process is described to select and
remove officers (18)

Client name/ Presentation Name/ 12pt - 14
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Medical Executive Committee Function and Size is described (20) Selection and removal of members is described (21) Composition including MDs and others is described
(22) MEC authority is described and when MEC acts for
the Medical Staff (23) Conflict Resolution: MEC and the Medical Staff (20)

Client name/ Presentation Name/ 12pt - 15
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.01.01.01, EPs 12 - 36
Bylaws—process to adopt and amend (24) Rules and Regulations and Policies—process to
adopt and amend (25) When Departments exist the bylaws contain the
qualifications for Chairs and their roles and responsibilities (36)
The bylaws describe basic requirements for H&P, practitioners that may perform the H&P and update requirements (16)
Client name/ Presentation Name/ 12pt - 16
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.01, FPPE (4 of 9 EPs)
EP 1: A period of FPPE is implemented for all initially requested privileges
EP 3: The performance monitoring process is clearly defined and includes each of the following elements:– Criteria for conducting performance monitoring– Method for establishing a monitoring plan specific
to the requested privilege– Method for determining the duration of
performance monitoring– Circumstances under which monitoring by an
external source is required
Client name/ Presentation Name/ 12pt - 17
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.01, FPPE (4 of 9 EPs)
EP 4: Focused professional practice evaluation is consistently implemented in accordance with the criteria and requirements defined by the medical staff
EP 5: The triggers that indicate the need for performance monitoring are clearly defined
Client name/ Presentation Name/ 12pt - 18
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.01, FPPE (4 of 9 EPs)
EP 1: FPPE requirement for all new applicants with privileges, all existing medical staff requesting new privileges and all for cause indications– Effective January 1, 2008– No exceptions, even if data is difficult to
gather (Advanced Practice Providers)

Client name/ Presentation Name/ 12pt - 19
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.01, FPPE (4 of 9 EPs)
EP 3: the FPPE process is clearly predefined with criteria, monitoring methods, monitoring duration, and circumstances for monitoring by an external source– Activity or time period
– Time period may not allow complete privileges to be utilized
– High volume provider has provided significant patient care before time period ends
– Activity or time period, depending on which is met first
Client name/ Presentation Name/ 12pt - 20
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.01, FPPE (4 of 9 EPs)
EP 4: All aspects of EP 3 are consistently implemented
EP 5: Triggers indicating a need for focused review are clearly defined– A single incident—Perforation– A trend—exceeds a number of validated
patient or staff complaints, exceeds peer use of reversal agents for sedation
Client name/ Presentation Name/ 12pt - 21
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.03 (2 of 3 EPs)
EP 1: There is a clearly defined process in place that facilitates the evaluation of each practitioner’s professional practice
EP 3: Information resulting from the ongoing professional practice evaluation is used to determine whether to continue, limit, or revoke any existing privilege (s)

Client name/ Presentation Name/ 12pt - 22
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MS.08.01.03 (2 of 3 EPs)
EP 1: Each practitioner type has a defined process for evaluation
EP 3: OPPE information is used to determine continuation, limitation, or revocation of any existing privilege(s)– Advanced practitioner provider
– Approach to evaluation is different and not defined
– Data lacking to formulate useful objective information for decisions
Client name/ Presentation Name/ 12pt - 23
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
The Challenge for These StandardsRelevant information for performance
evaluation of advanced practice providers may not be readily available
Most information is tagged to the attending physician rather than the advanced practice provider
Client name/ Presentation Name/ 12pt - 24
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
What Information Can Be Used
Periodic chart reviewDirect observationMonitoring of diagnostic and treatment
techniquesDiscussion with other individuals
involved in the care of each patient including consulting physicians, assistants, and nursing and administrative personnel
Client name/ Presentation Name/ 12pt - 25
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
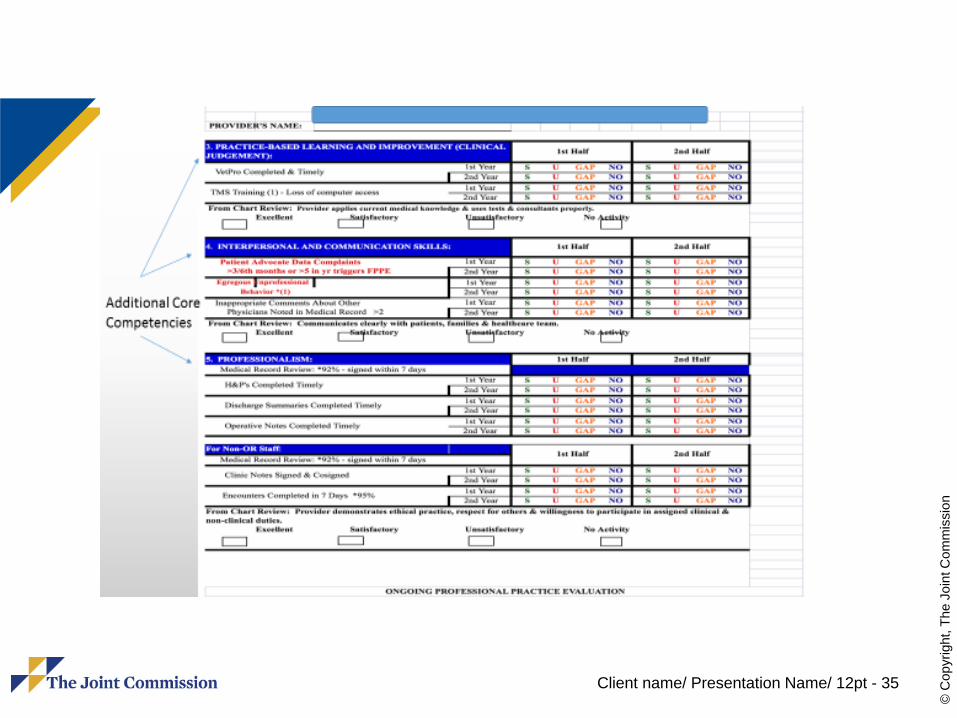
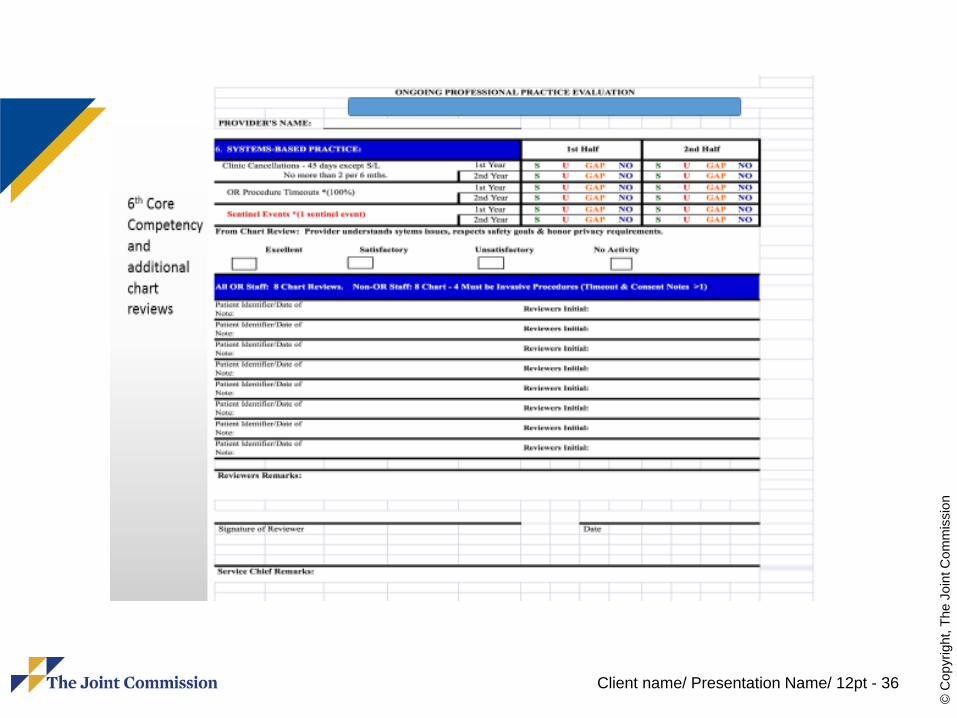
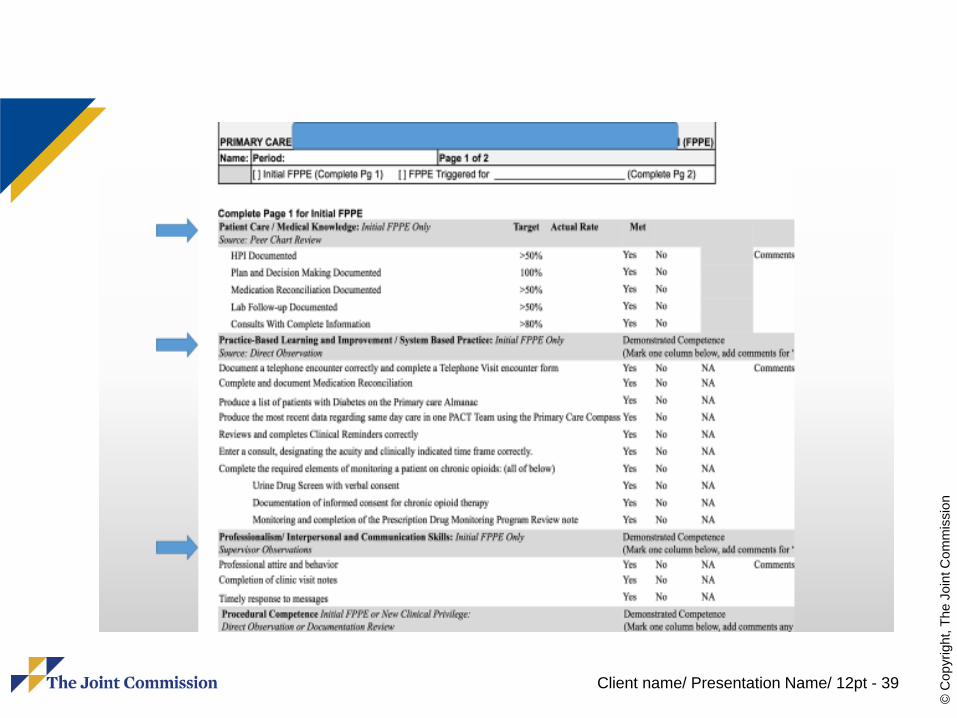
Best Practice
Direct observation and evaluation of a patient encounter
Performed by sponsoring physician or a peer advanced practice provider
Evaluation form used to track observations
Client name/ Presentation Name/ 12pt - 26
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
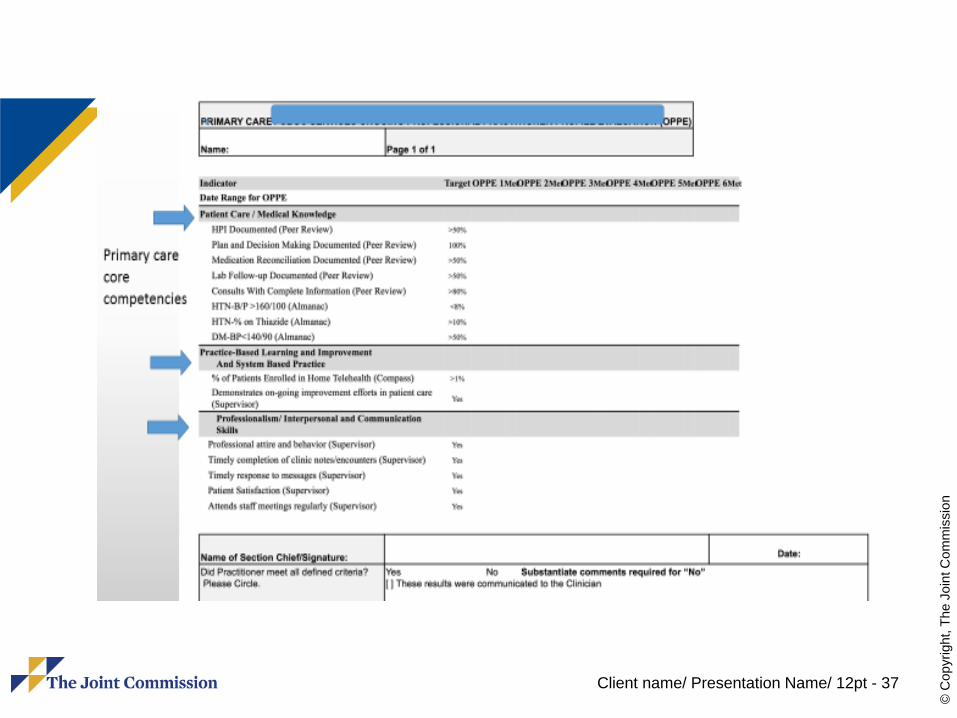
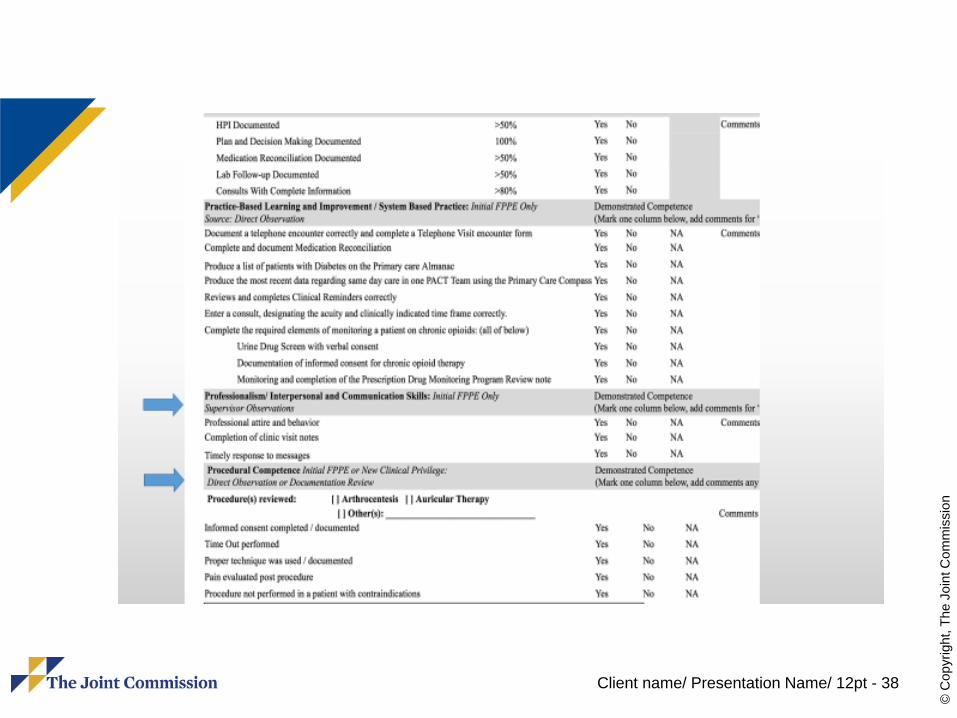
Evaluation Form
Questions about care, treatment and services answered with a Yes, No or Not Applicable
Patient medical record number used to document the specific patient encounter
Medical staff determines how many observations are required
Client name/ Presentation Name/ 12pt - 27
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Examples of Questions
History and Physical appropriate and pertinent?
Progress notes adequate to follow the patient’s course?
Appropriate lab and imaging studies?Appropriate medication ordering?Appropriate and timely consultations?

Client name/ Presentation Name/ 12pt - 28
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Examples of Questions
Medication reconciliation completed?Informed consent obtained?Sterile technique observed?Appropriate participation in the time
out?Overall evaluation for this reporting
period? Satisfactory or Unsatisfactory

Client name/ Presentation Name/ 12pt - 29
© C
opyr
ight
, The
Joi
nt C
omm
issi
on

Client name/ Presentation Name/ 12pt - 30
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 31
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 32
© C
opyr
ight
, The
Joi
nt C
omm
issi
on

Client name/ Presentation Name/ 12pt - 33
© C
opyr
ight
, The
Joi
nt C
omm
issi
on

Client name/ Presentation Name/ 12pt - 34
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 35
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 36
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 37
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 38
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Client name/ Presentation Name/ 12pt - 39
© C
opyr
ight
, The
Joi
nt C
omm
issi
on

Client name/ Presentation Name/ 12pt - 40
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Other Challenging Medical Staff StandardsMS.01.01.01, EP 5: The medical staff complies with
the medical staff bylaws, rules and regulations, and policies
MS.06.01.01, EP 1 and EP 2: Privileges are delineated and approved only after determination the hospital has the required resources
MS.06.01.05, EP 2: Evaluation of all of the following are included in the criteria:– When renewing privileges review of the
practitioner’s performance within the hospital
Client name/ Presentation Name/ 12pt - 41
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
MM.09.01.01, Antimicrobial StewardshipCDC: 20% to 50% of antibiotics
prescribed unnecessarily or inappropriately
CDC: annually 2 million illnesses and 23,000 deaths due to antibiotic resistant bacteria in the US

Client name/ Presentation Name/ 12pt - 42
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 1: Leadership
Leaders establish antimicrobial stewardship as an organizational priority
Examples-Accountability documents -Budget plans -Infection prevention plans -Performance improvement plans -Strategic plans -Using the electronic health record to collect antimicrobial stewardship data :
Client name/ Presentation Name/ 12pt - 43
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 2: Education of Staff and LIPs The [critical access] hospital educates staff and licensed
independent practitioners involved in antimicrobial ordering, dispensing, administration, and monitoring about antimicrobial resistance and antimicrobial stewardship practices. Education occurs upon hire or granting of initial privileges and periodically thereafter, based on organizational need.
Acceptable materials and methods of education are determined by the organization and should be based on acceptable practice. Examples include: Written materials, presentations, online education, classes, conferences, annual education days, CMEs etc.
Client name/ Presentation Name/ 12pt - 44
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 3: Education of patients
The [critical access] hospital educates patients, and their families as needed, regarding the appropriate use of antimicrobial medications, including antibiotics
o Emergency department patients who are prescribed antimicrobials. o Ambulatory and clinic patients surveyed under the hospital program who are prescribed antimicrobials. o Hospitalized patients who will be discharged on antimicrobials.
Client name/ Presentation Name/ 12pt - 45
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 4: Antimicrobial Stewardship Multidisciplinary TeamThe [critical access] hospitals and NCC
has an antimicrobial stewardship multidisciplinary team that includes the following members, when available in the setting:– Infectious disease physician – Infection preventionist(s) – Pharmacist(s) – Practitioner

Client name/ Presentation Name/ 12pt - 46
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 5: Core Elements
The [critical access] hospitals antimicrobial stewardship program includes the following core elements– Leadership commitment– Accountability– Drug expertise– Action– Tracking– Reporting– Education

Client name/ Presentation Name/ 12pt - 47
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 6: Multidisciplinary Protocols
The [critical access] hospitals and NCC antimicrobial stewardship program uses organization-approved multidisciplinary protocols (for example, policies and procedures)
Based on the population served and the services provided

Client name/ Presentation Name/ 12pt - 48
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 6: Examples of Protocols
Antibiotic Formulary Restrictions Assessment of Appropriateness of Antibiotics for Community-Acquired
Pneumonia Assessment of Appropriateness of Antibiotics for Skin and Soft Tissue
Infections Assessment of Appropriateness of Antibiotics for Urinary Tract
Infections Care of the Patient with Clostridium difficile (c.-diff) Guidelines for Antimicrobial Use in Adults − Guidelines for
Antimicrobial Use in Pediatrics Plan for Parenteral to Oral Antibiotic Conversion Preauthorization Requirements for Specific Antimicrobials Use of Prophylactic Antibiotics

Client name/ Presentation Name/ 12pt - 49
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 7: Data
The [critical access] hospitals collects, analyzes, and reports data on its antimicrobial stewardship program.
The collection, analysis and reporting on outcomes of the program establishes actual implementation
Client name/ Presentation Name/ 12pt - 50
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
EP 8: Action
The [critical access] hospital takes action on improvement opportunities identified in its antimicrobial stewardship program

Client name/ Presentation Name/ 12pt - 51
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Key References
Centers for Disease Control and Prevention’s Core Elements of Hospital Antibiotic Stewardship Programs (See http://www.cdc.gov/getsmart/healthcare/pdfs/core-elements.pdf
National Quality Partners Playbook: Antibiotic Stewardship in Acute Care. Washington, D.C.: NQF, May 2016

Client name/ Presentation Name/ 12pt - 52
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Focus on Reducing Inpatient SuicideFor inpatient psychiatric hospitals,
inpatient psychiatric units in general acute care hospitals, and non-behavioral health units DESIGNATED for the treatment of psychiatric patients (i.e. special rooms/safe rooms in Emergency Departments or Medical Units)
Client name/ Presentation Name/ 12pt - 53
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Environment of Care
EC.02.06.01, Element of Performance 1require hospitals to establish and maintain a
safe, functional environment. Element of Performance # 1 states “Interior spaces meet the needs of the patient population and are safe and suitable to the care, treatment, and services provided”. Therefore, ligature and self-harm risks must be identified and eliminated

Client name/ Presentation Name/ 12pt - 54
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Focus on Reducing Inpatient Suicides1200 to 1500 inpatient suicides each
year in the United States70 to 75 percent by hangingLigature risks no longer acceptable in
areas specified for treatment of behavioral health care patients with suicide risk

Client name/ Presentation Name/ 12pt - 55
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Approach to Ligature Risks
Identify all ligature risks in the environmentWhen possible immediately eliminate all
ligature risksWhen immediate removal is not possible--
While risks are in the process of being eliminated, policies and procedures must be developed and implemented to mitigate the harm posed by such risks.
Client name/ Presentation Name/ 12pt - 56
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Mitigation Plans for Ligature Risk
• Ensuring that leadership and staff are aware of the current environmental risks• Identifying patients’ risk for suicide or self-harm, then implement appropriate interventions based upon risk.• Ongoing assessments and reassessments of at-risk behavior as defined by the organization.• Ensuring the proper training of staff to properly identify patients’ level of risk and implement appropriate interventions
Client name/ Presentation Name/ 12pt - 57
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Mitigation Plans for Ligature Risk
• Incorporating suicide risk and self-harm reduction strategies into the overall Quality Assessment/Performance Improvement (QAPI) program - see LD.01.03.01 EP 21.• If equipment poses a risk but is necessary for the safe treatment of psychiatric patients (i.e. medical beds with side rails on a geriatric unit), the organization must consider these risks in patients’ overall suicide/self-harm risk assessments, then implement appropriate interventions to diminish those risks
Client name/ Presentation Name/ 12pt - 58
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Non-Behavioral Health Care UnitsIn non-behavioral health units (i.e.
Emergency Rooms or Medical Inpatient Units) that are NOT DESIGNATED specifically for the treatment of psychiatric patients; however, where psychiatric patients may temporarily reside, ligature/self-harm environmental risks must also be identified.
Client name/ Presentation Name/ 12pt - 59
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Non-Behavioral Health Care UnitsAll physical risks not required for the
treatment of the patient that can be removed, must be removed. Furthermore, an appropriate level of effective surveillance must be implemented if self-harm risks remain in the environment. Organizational policies and procedures must adequately guide staff in the assessment of patients’ risk for suicide/self-harm and the implementation of interventions based upon the patients’ individual needs.

Client name/ Presentation Name/ 12pt - 60
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Resources
Sentinel Event AlertsBooster PacksDesign Guide for the Built Environment
of Behavioral Health Facilities, April 2017, Edition 7.2, James M. Hunt, AIA, NCARB and David M. Sine, DrBE, CSP, ARM, CPHRM

Client name/ Presentation Name/ 12pt - 61
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Orientation of Medical Staff
MS.01.01.01, EP 36: If departments of the medical staff exist, the roles and responsibilities of the department chair, which are defined by the organized medical staff, include the following:– Orientation and continuing education of all
persons in the department or service
Client name/ Presentation Name/ 12pt - 62
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Orientation of the Medical Staff
PC.01.01.01, EP 24:– Provides orientation and training to any
clinical and nonclinical staff in effective and safe care, treatment, and services (for example, medication protocols, de-escalation techniques)
Client name/ Presentation Name/ 12pt - 63
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Orientation of the Medical Staff
PC.03.05.17, EP 2– The hospital trains staff on the use of
restraint and seclusion, and assesses their competence, at the following intervals–At orientation–Before participating in the use of
restraint and seclusion–On a periodic basis thereafter

Client name/ Presentation Name/ 12pt - 64
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Orientation of the Medical Staff
WT.03.01.01: Staff and licensed independent practitioners performing waived tests are competent
EP 1: Responsibility for orientation and training EP 2: LIPs who perform waived testing receive orientation according
to hospital services and documented EP 3: LIPs have been trained for each test and the training is
documented EP 4: LIPs who perform waived testing requiring an instrument have
been trained on its use and maintenance and documented EP 5: Competency is validated by two of four methods per test EP 6: Competence is assessed at least at the time of orientation and
at least annually thereafter, and documented. LIPs may include this in credentialing and privileging if the test falls within the specialty and testing does not involve an instrument (Provider-performed microscopy is not a waived test)

Client name/ Presentation Name/ 12pt - 65
© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Continuing Medical Education
MS.12.01.01Continuing education if an adjunct to
maintaining clinical skills and current competence
EP 4: Must be documented by transcript or attestation depending on state
EP 2 and 4: Documentation of restraint education for those who provide restraint and seclusion only