Embed Size (px)
Citation preview

John Stoukides MDChief, Division of Geriatrics and Palliative MedicineRoger Williams Medical CenterProvidence, R.I.
The Far Reaching Impact of ADPatient
4 million affected Increasing with aging population 70% live at home
Family Loss of productivity of caregivers Painful process Significant incidence of depression and
medical illnessSociety
$100 Billion / year
Impact of Alzheimer’s Disease on Caregivers More than 70% of patients with
Alzheimer’s disease live at home, and almost 75% of home care is provided by family and friends1
46% to 59% of caregivers reported depression, according to various studies2,3
1. Alzheimer’s Association. Available at: http://www.alz.org. Accessed October 7, 2004.2. Gallagher D et al. Gerontologist. 1989;29:449-456.3. Cohen D et al. Behavior, Health and Aging. 1990;1:171-182.

ALZHEIMER’SANNUAL COST TO U.S.
Heart Disease $ 183 Billion Diabetes 112
Cancer 109 Stroke 45 Pulmonary Disease 24 Pneumonic Influenza 22 Chronic Liver Disease 9 HIV/AIDS 7
Alzheimer’s 110
Alzheimer’s average cost to each family is$25,000/ year and 100 hours/week.

Dementia - Definition
An unusual loss of mental function Acquired, persistent impairment in
multiple areas of intellectual function not due to delirium.
A symptom of many diseases, not a diagnosis
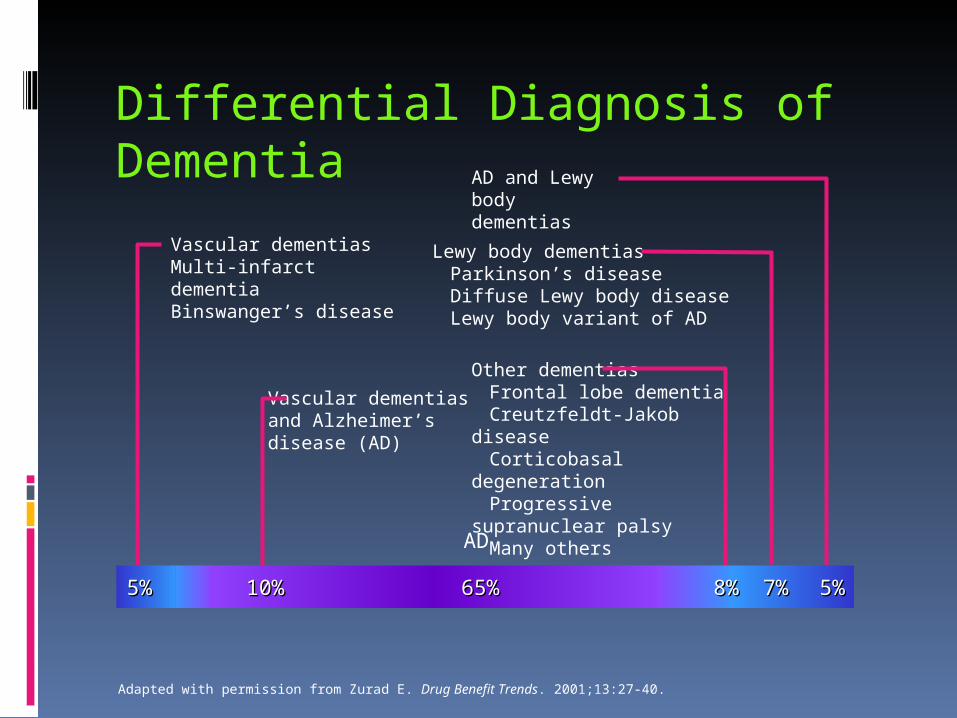
Differential Diagnosis of Dementia
AD
Vascular dementiasMulti-infarct dementiaBinswanger’s disease
Vascular dementiasand Alzheimer’s disease (AD)
AD and Lewy body dementias
Lewy body dementiasParkinson’s diseaseDiffuse Lewy body diseaseLewy body variant of AD
Other dementias
Frontal lobe dementiaCreutzfeldt-Jakob diseaseCorticobasal degenerationProgressive supranuclear
palsyMany others
Adapted with permission from Zurad E. Drug Benefit Trends. 2001;13:27-40.
5%5% 10%10% 65%65% 8%8% 7%7% 5%5%
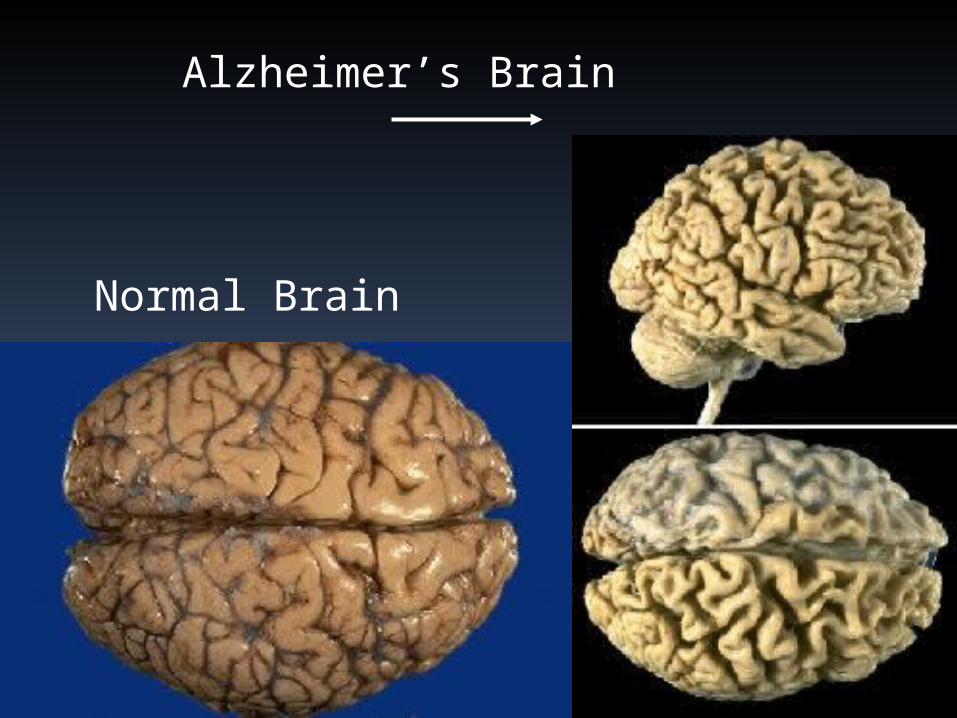
Normal Brain
Alzheimer’s Brain

Beginning Symptoms of AD
Progressive memory loss recent events including time and place
Difficulty with complex tasks Inability to use reasoning strategies Problems finding words Disorientation to location and
direction Have difficulty reorienting them
selves to recent event Depression
Mid-Stage Alzheimer’s Disease Requires assistance with activities of daily living Language and communications degrade Impaired judgment Emotional instability Psychiatric instability Personal hygiene decreases Inappropriate responses Unaware of surroundings Trouble distinguishing people - familiar vs.
strangers Are mostly unaware of their cognitive loss

Late Stage Alzheimer’s Disease
Agitation, depression, delusions diminishNeed for tranquilizers lessenedBrain activity severely disruptedVulnerable to seizures, aspirations and
pneumoniaMotor skills deteriorate
Lose ability toWalkCommunicateChew and swallow
Assume fetal position Ultimate outcome - death
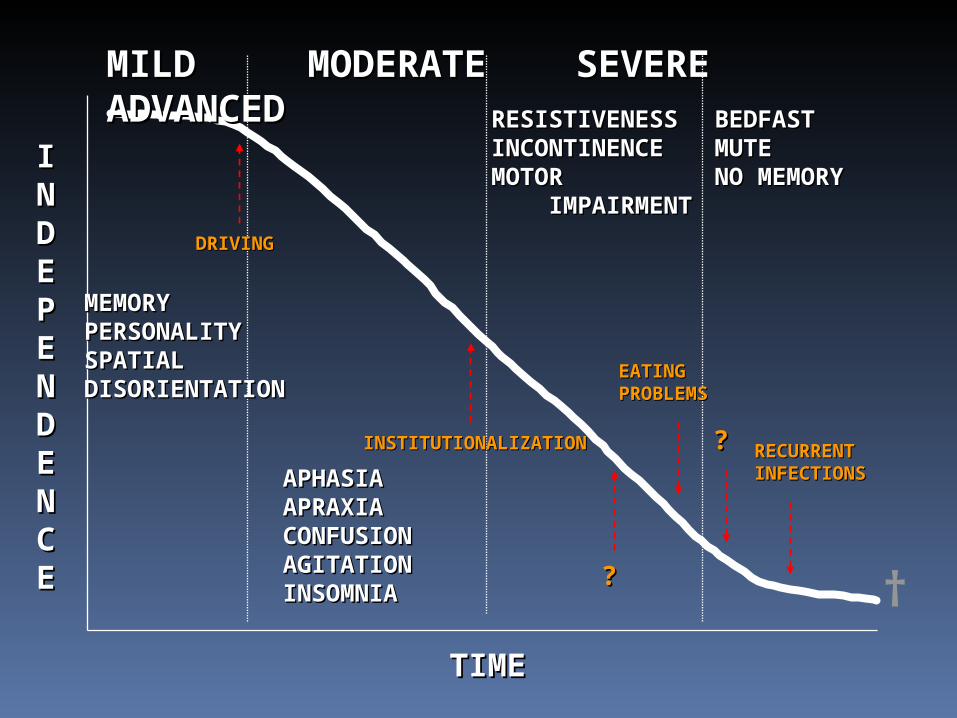
MILD MODERATE SEVEREMILD MODERATE SEVERE ADVANCED ADVANCED
MEMORYMEMORYPERSONALITYPERSONALITYSPATIALSPATIALDISORIENTATIONDISORIENTATION
APHASIAAPHASIAAPRAXIAAPRAXIACONFUSIONCONFUSIONAGITATIONAGITATIONINSOMNIAINSOMNIA
RESISTIVENESSRESISTIVENESSINCONTINENCEINCONTINENCEMOTOR MOTOR IMPAIRMENTIMPAIRMENT
BEDFASTBEDFASTMUTEMUTENO MEMORYNO MEMORY
TIMETIME
IINNDDEEPPEENNDDEENNCCEE
EATING EATING PROBLEMSPROBLEMS
RECURRENT RECURRENT INFECTIONSINFECTIONS
??
??INSTITUTIONALIZATIONINSTITUTIONALIZATION
DRIVINGDRIVING
†

Delirium in the Elderly
Acute decline in attention and cognition Potentially life threatening Preventable in most cases
Accounts for 49% of all hospital days in pts over 65
Complicates 20% of all hospital admissions
Precipitating factor in most hospitalizations
Associated with very high mortality rate Is a medical emergency

Clinical Features
Acute onset Fluctuating course Inattention(difficulty focusing, sustaining attention,
maintaining conversation)
Disorganized thinking (disorganized or incoherent speech rambling or irrelevant or illogical)
Altered level of consciousness Cognitive deficits Perceptual disturbances
Psychomotor changes Hyperactive Delirium: agitation, hyper-
vigilance, inappropriate excitement and perceptual disturbances
Hypoactive Delirium: reduced motor activity, inattentive, easily distracted and unable to sustain a train of thought.
Additional Features
Various Emotional Disturbance Fear Depression Euphoria perplexity
Baseline Characteristics Vulnerability Advanced age Organic Brain disease (stroke, dementia,
PD) Acute Medical Illness Sensory Impairment Diminished ADL’s (activities of daily living) Polypharmacy Alcohol Use Medication misuse Toxin ingestion
Precipitating Factors
Addition of more than three medications to medical regimen
Infection Dehydration Immobility (restraints) Malnutrition Temperature extremes
Examples of symptoms
You ask the person for his phone number after probing it is clear he doesn’t know it
Memory impairment
During the interview the person dozes off while you are asking questions
Alerted level of consciousness (lethargy)
As you ask a question the person keeps repeating the answer from a previous question
inattention
Examples of symptoms
The person is in a restaurant for breakfast and angrily says “why the F%@$ are they giving me eggs for dinner”
Disorientation
Person startles easily at any sound or touch, eyes open wide
ALOC vigalant
You ask why the person is stopped is sitting in their car and he says “I’ve gotta get to the yellow brick road”
Disorganized thinking

Examples of symptoms
As you interview the person she keeps looking at the corner then blurts out “what is that man doing there”
Perceptual disturbance (visual hallucinations)
As you begin the interview the person is looking around the room. You call her name and touch her she momentarily looks at you then starts looking around again
Inattention
Examples of symptoms
You introduce yourself and he says what are you doing in my home
Disorientation
You walk into the room and the person says “lucy where have you been, You said you’d be right back”
Disorientation
During the encounter the person is continuously fidgeting, dressing and undressing himself
Psychomotor agitation
Examples of symptoms
Between questions the person is carrying on a conversation with her husband who is not present
Perceptual disturbance (auditory hallucinations)
You ask the person if she is able to call a family member and she says “it depends on the type of party I’m at: I need a comb”
Disorganized thinking
The person remains motionless in a chair and performs tasks very slowly
Psychomotor retardation
Helping Patients with Troublesome Behaviors Patients with significant cognitive
impairment in most cases can not be reality oriented
Patients with agitation should be considered acutely medically ill until proven otherwise
Pacify and re-direct is usually best approach
Conclusion
Alzheimer’s disease is a extremely common and unfortunately incurable condition in the elderly
It has a slow steady progression, acute changes in it’s course frequently represent an acute medical illness
Alzheimer’s patients have an inability to accurately report reality or be reoriented to their current situation
Confronting an Alzheimer’s patient will frequently escalate the unwanted behaviors.





























