Embed Size (px)
Citation preview

9/14/12
1
JNC-8: Process, Critical Questions and Future Reports
Barry L. Carter, Pharm.D., FCCP, FAHA, FASH The Patrick E. Keefe Professor in Pharmacy
Department of Pharmacy Practice and Science College of Pharmacy and
Professor, Department of Family Medicine Roy J. and Lucille A. Carver College of Medicine
University of Iowa
Disclosure of Relationships Over the past 5 years
Grant Support: NIH, AHRQ, VA HSR&D.
I have had NONE of the following: Consultant, Speakers Bureau, Major Stock Shareholder, or Other Support from Industry.
Learning Objectives At the compleKon of the presentaKon, parKcipants will be able to: 1. Describe the evidence quality grading and recommendaKon strength process used by JNC-‐8 which will be used to formulate the guidelines.
2. Compare and contrast the JNC-‐8 systemaKc review and guideline development process with previous hypertension guidelines.
3. Discuss the three main criKcal quesKons being addressed by JNC-‐8.

9/14/12
2
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Joint National Committee on Prevention, Detection,
Evaluation, & Treatment of High Blood Pressure (JNC)
JNC 7: 2003 JNC 6: 1997 JNC 5: 1992 JNC 4: 1988 JNC 3: 1984 JNC 2: 1980 JNC 1: 1976
Detection, Evaluation, &Treatment of High Blood
Cholesterol in Adults (ATP, Adult
Treatment Panel)
ATP III Update: 2004 ATP III: 2002 ATP II: 1993 ATP I: 1988
Clinical Guidelines on the Identification, Evaluation, &
Treatment of Overweight and Obesity in Adults
Obesity: 1998
NHLBI Adult CVD Prevention Guidelines
NHLBI-sponsored Adult CVD Prevention Guidelines
JNC V
Optimal 110 120 130 140 150 160 170 180 190 200 210 220
JNC IV. Arch Intern Med. 1988;148:1023-1038. JNC V. Arch Intern Med. 1993;153:154-183. JNC VI. Arch Intern Med. 1997;157:2413-2446. Chobanian AV et al. JAMA. 2003;289:2560-2572.
JNC I JNC II JNC III JNC IV JNC VI
Border- line
ISH
Stage 1 Stage 1
Stage 2
Stage 3
High- normal
High- normal
Normal Normal
Optimal
SBP (mm Hg)
Normal
Border- line
ISH
Stage 4
No recommendations for SBP in JNC I
or JNC II
JNC 7
Stage 1
Prehyper- tension
Normal
Stage 3
Stage 2
JNC I. JAMA. 1977;237:255-261. JNC II. Arch Intern Med. 1980;140:1280-1285. JNC III. Arch Intern Med. 1984;144:1045-1057.
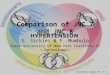
Hypertension: A Moving Target JNC BP Classifications: SBP
Stage 2
JNC VI. Arch Intern Med. 1997;157:2413-2446.
OPTIMAL < 120 and < 80
NORMAL < 130 and < 85
STAGE 1 140-159 or 90-99
STAGE 2 160-179 or 100-109
STAGE 3 ≥ 180 or ≥ 110 H
yper
tens
ion
NORMAL < 120 and < 80
PREHYPERTENSION 120-139 or 80-89
STAGE 1 140-159 or 90-99
STAGE 2 ≥ 160 or ≥ 100
JNC 7 (2003) JNC VI (1997)
JNC 7 Emphasizes Importance of Low BP
HIGH NORMAL 130-139 or 85-89
JNC 7. JAMA. 2003;289(19):2560-2572.

9/14/12
3
Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) EXPRESS
National Heart, Lung, and Blood Institute
National High Blood Pressure Education Program
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
My Observations About Previous Structure and Process
JNC- V (1993): Chairman – Ray Gifford, Jr. MD Subcommittee on Pharmacologic TX: Edward D. Frohlich, MD chair
Started June 1991, published January 1993
JNC- VI (1997): Chairman – Sheldon Sheps, MD Prevention and Treatment Chair: Norman Kaplan, MD
Started September 1996, published November 1997
JNC-7 (2003): Chairman: Aram Chobanian, MD Started December 2002, published May 2003
JNC- 8 (pending): Co-Chairs: Paul James, MD, Suzanne Oparil, MD Prevention and Treatment Chairs: William Cushman, MD, Jackson Wright, MD
Started August 2008, report for comment expected fall 2012.
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Institute of Medicine Report: Quality Chasm
“In its current form, habits, and environment, American health care is incapable of providing the public with the quality health care it expects and deserves.”
Current: Decision making is based on training and experience. New: Decision making is based on evidence.
Patients should receive care based on the best available scientific knowledge. Care should not vary illogically from clinician to clinician or from place to place.
Evidence-based Clinical Practice Guidelines can help make this vision a reality
Institute of Medicine, Crossing the Quality Chasm: New Health System for the Twenty-first Century. Washington: National Academy Press, 2001

9/14/12
4
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ACC/AHA Guidelines Grading Schema
Evidence Quality
Level of Evidence A Recommendation based on evidence from multiple randomized
trials or meta analyses
Level of Evidence B Recommendation based on evidence from a single randomized
trial or nonrandomized studies
Level of Evidence C Recommendation based on expert opinion, case studies, or
standards of care
10
Evidence-Based Clinical Practice Guidelines for CVD Prevention
AHA Level of Evidence A in Current Guidelines*
*in guidelines with level of
evidence
11.7% 26.4%
15.3% 13.5%
12.0% 22.9%
6.4% 6.1%
23.6% 0.3%
9.7% 11.0%
19.0% 4.9%
4.8%
0% 10% 20% 30%
AF Heart failure
PAD STEMI
Perioperative Secondary prevention
Stable angina SV arrhythmias
UA/NSTEMI Valvular disease
VA/SCD PCI
CABG Pacemaker
Radionuclide imaging
Scientific Evidence Underlying ACC/AHA Guidelines (JAMA. 2009; 301: 831 – 841)
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
NHLBI Evidence Quality Grading and Recommendation Strength
Evidence Quality High
Well-designed and conducted RCTs
Moderate RCTs with minor limitations Well-conducted observational
studies
Low RCTs with major limitations Observational studies with major
limitations
Recommendation Strength
A – Strong
B – Moderate
C – Weak
D – Against
E – Expert Opinion
N – No Recommendation
12

9/14/12
5
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Adult CVD Guidelines: NHLBI approach
Advice to NHLBI from advisory groups: Update risk factor guidelines (hypertension, cholesterol, obesity) Develop an integrated guideline Use an evidence-based approach including systematic reviews
The NHLBI guideline development process Was established to assure rigor and to minimize bias Methods being used meet many of the new IOM standards
Two recent IOM reports set new standards “Finding What Works in Health Care” – standards for systematic
reviews “Clinical Practice Guidelines We can Trust” – standards for developing
trustworthy CPGs
Evidence-Based Clinical Practice Guidelines for CVD Prevention
NHLBI Systematic Review and Guideline Development Process
Literature Searched; Eligible Studies
Identified
Studies Quality Rated; Data Abstracted
Evidence Tables Developed;
Body of Evidence Summarized
External Review of Guideline
Drafts; Revised as Needed
Guidelines Disseminated &
Implemented
Graded Evidence Statements &
Recommendations Developed
Expert Panel Selected
Topic Area Identified
Critical Questions & Study Eligibility Criteria Identified
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Expertise Represented
Hypertension, primary care, cardiology, nephrology, clinical trials, research methodology, evidence-based medicine, epidemiology, guideline development and implementation, nutrition/lifestyle, nursing, pharmacy, systems of care, and informatics
Panel also includes senior scientists from NHLBI and NIDDK with expertise in hypertension, clinical trials, translational research, nephrology, guideline development, and evidence-based methodology

9/14/12
6
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
JNC 8 CommiYee Members Co-‐Chair: Suzanne Oparil MD
Jackson T. Wright, Jr. MD, PhD
Sandra J. Taler, MD
Joel Handler, MD
Barry L. Carter, PharmD
Daniel T. Lackland, DrPH
Sidney C. Smith, Jr., MD
Olugbenga Ogedegbe, MD, MPH, MS
Cheryl Dennison Himmelfarb, RN, ANP, PhD
Co-‐Chair: Paul A. James MD
Laura Svetkey, MD, MHS
Michael L. LeFevre, MD, MSPH
Raymond R. Townsend, MD
William C. Cushman, MD
Thomas D. MacKenzie, MD, MSPH
Andrew S. Narva, MD (Ex-‐Officio)
Lawrence J. Fine, MD, DrPH (Ex-‐Officio)
Eduardo OrKz, MD, MPH, NHLBI Lead, Ex-‐Officio, Non-‐VoKng Member
* 4 members had relaKonships to disclose; 13 had no relaKonships to disclose. Panel members disclose their relaKonships and recuse themselves from voKng on evidence statements and recommendaKons relevant to their relaKonships.
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
How the Process Has Evolved Strictly evidence-based
Focus only on randomized controlled trials assessing important health outcomes (no use of intermediate/surrogate measures)
Every included study is rated for quality by two independent reviewers using standardized tools
Evidence statements graded for quality using prespecified criteria
Separate grading for recommendations
Independent methodology team to ensure objectivity of the review
Initial set of recommendations focused on 3 key questions
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
How Were Questions Selected?
Panel Chairs and NHLBI staff developed questions based on their expertise, brief literature review, and speaking with colleagues
These questions were sent to panel members to review, revise, and add or delete questions
Resulted in 23 questions, which were sent to all panel members Panel members discussed these questions on conference calls, then
independently ranked the 3-5 questions felt to be of highest priority
The five highest ranked questions discussed further and prioritized

9/14/12
7
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Rationale for the Questions
Interest in assessing the evidence to support 140/90 mm Hg as a treatment threshold or goal
Should the treatment threshold / goal be lower in populations with diabetes, chronic kidney disease, coronary artery disease, stroke, and other co-morbidities or characteristics?
Should the treatment threshold / goal be different in older adults?
Use of different treatment thresholds and goals is confusing
Is there evidence that treatment to lower BP with a particular drug or drug class improves outcomes compared to another?
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Critical Questions and I/E Criteria
Critical Question (CQ) in PICO format Population
Intervention/Exposure
Control/Comparator
Outcomes
Study Inclusion/ Exclusion criteria: Types of studies (e.g., RCTs, epidemiology, systematic reviews)
Subgroups (e.g., elderly, diabetes)
Specific outcomes (e.g., CVD mortality, MI, stroke, HF)
Implementa)on WG Thomas Pearson MD, PhD
Wiley Chan MD
Lifestyle WG Robert Eckel MD John Jakicic PhD
Risk Assessment WG David Goff Jr. MD,
PhD Donald M. Lloyd-‐Jones MD, ScD
Cholesterol Panel
Neil Stone MD Alice Lichtenstein DSc Jennifer Robinson MD
Obesity Panel Michael Jensen
MD Donna Ryan MD
BP Panel Paul James MD Suzanne Oparil
MD
Execu)ve CommiBee Sidney Smith Jr. MD
Expert Panel Composition
• Diversity and balance of expertise
• Diversity of demographics
• Conflict of interest management

9/14/12
8
Evidence-Based Clinical Practice Guidelines for CVD Prevention
NHLBI Adult CVD Prevention Guidelines
Expert Panels and WorkGroups
22
Implementation WG Implementability Guidance (GLIA) Implementation Science Review
Lifestyle WG Evidence Review on
Diet & Physical Activity 3 CQs (1 SR)
Risk Assessment WG Evidence Review & Risk
Prediction Model 2 CQs+model (1 SR)
Cholesterol Panel Evidence Review on Cholesterol Tx
3 CQs
Obesity Panel Evidence Review
on Obesity 5 CQs (2 SRs)
BP Panel Evidence Review
on BP Tx 3 CQs
Five draft reports released for public comment, one at a time
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Question 1
Among adults with hypertension, does initiating antihypertensive pharmacological therapy at specific BP thresholds improve health outcomes? − When to initiate drug treatment?
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Question 2
Among adults, does treatment with antihypertensive pharmacological therapy to a specified BP goal lead to improvements in health outcomes? − How low should you go?

9/14/12
9
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Question 3
In adults with hypertension, do various antihypertensive drugs or drug classes differ in comparative benefits and harms on specific health outcomes? − How do you get there?
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Inclusion/Exclusion Criteria
Randomized Controlled Trials RCTs are subject to less bias and represent the gold
standard for determining efficacy and effectiveness1
Search dates: 1966 to present
Minimum one-year follow-up period
Studies with sample sizes less than 100 excluded
1 Institute of Medicine. 2011. Finding What Works In Health Care. Standards For Systematic Reviews. Washington, DC: The National Academies Press.
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Populations Included
Adults 18 years of age and older
Prespecified subgroups including: Diabetes
Chronic kidney disease
Proteinuria
Coronary artery disease
Peripheral artery disease
Previous stroke
Heart Failure
Older Adults
Men and women
Racial and ethnic groups
Smoking

9/14/12
10
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Outcomes
Overall mortality, CVD-related mortality, CKD-related mortality, myocardial infarction, heart failure, hospitalization for heart failure, stroke
Coronary revascularization (includes coronary artery bypass surgery, coronary angioplasty and coronary stent placement), peripheral revascularization (includes carotid, renal, and lower extremity revascularization)
End stage renal disease (i.e., kidney failure resulting in dialysis or transplant), doubling of creatinine, halving of eGFR
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Literature Review and Assessment Process
Systematic search of literature for the CQ Citations found using inclusion/exclusion criteria Papers screened and reviewed for inclusion Result: unbiased list of studies based on a priori criteria
Quality of each included study rated Good, Fair, Poor
NHLBI study rating instruments Controlled intervention studies Cohort and cross-sectional studies Case-control studies Systematic reviews and meta-analyses
Evidence-Based Clinical Practice Guidelines for CVD Prevention
NHLBI Study Assessment Tool: Controlled Intervention Studies
Criteria Yes No Other 1.Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT?
5. Were the people assessing the outcomes blinded to the participants’ group assignments?
7. Was the overall drop-out rate from the study at its endpoint 20% or less than the number originally allocated to treatment?
14. Were all randomized participants analyzed in the group to which they were originally assigned (i.e., did they use an intention-to-treat analysis)?
Quality Rating (Good, Fair, Poor) (see guidance) Rater #1 initials: Rater #2 initials: Additional Comments (If POOR, please state why):

9/14/12
11
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Data Abstraction and Evidence Tables
Information from individual studies Key data abstracted into a database Evidence table for each study/paper: subjects, sample size,
intervention, comparison, results
Evidence summaries by Critical Question Tables and text of major elements relevant to the CQ
Graded evidence statements Multiple ESs for each CQ
Graded recommendations based on the evidence Multiple ESs could result in a single recommendation
31
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ArEcles Screened = 1496
Good = 8
Included = 44
Total Abstracted = 26
Excluded = 1452 (Did not meet prespecified
inclusion criteria)
Poor = 18 Fair = 18
Question 1: Among adults with hypertension, does initiating antihypertensive pharmacological therapy at
specific BP thresholds improve health outcomes?
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ArEcles Screened = 1978
Good = 17
Included = 92
Total Abstracted = 56
Excluded = 1886 (Did not meet prespecified
inclusion criteria)
Poor = 36 Fair = 39
Question 2: Among adults, does treatment with antihypertensive pharmacological therapy to a specified
BP goal lead to improvements in health outcomes?

9/14/12
12
Evidence-Based Clinical Practice Guidelines for CVD Prevention
ArEcles Screened = 2662
Good = 15
Included = 101
Total Abstracted = 66
Excluded = 2561 (Did not meet prespecified
inclusion criteria)
Poor = 35 Fair = 51
Question 3: In adults with hypertension, do various antihypertensive drugs or drug classes differ in comparative
benefits and harms on specific health outcomes?
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Adult CV Guideline Report Content
Methods description
Critical questions With study eligibility criteria and rationale
Summary of evidence for each CQ Summary tables and text ( e.g. “24 studies, 10 RCTs…)
Graded evidence statements (ES) Rationale for ES based on specific studies or previous systematic reviews Graded High, Medium, Low
Graded recommendations Rationale for the recommendation based on the evidence Graded A, B, C, D, E, or N
Reference citations 35
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Conclusion
The new NHLBI-sponsored adult CV guideline reports Are strictly evidence based Will not look like the previous guidelines Will have more depth and rigor; will have less breadth Will be released in 2012, one at a time as they are
ready Will use evidence based strategies for Implementation
36

9/14/12
13
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
New reports vs Previous reports
The new guideline reports will not look like the previous guidelines! Recommendations are based on systematic reviews of RCTs
Restricted to a few critical questions
More depth, less breadth (More rigor, less comprehensive)
The new guideline reports will look more similar to each other than in the past Previous reports used different methods and structure
New reports are using the same methods and structure
37
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Next Steps
Evidence statements and recommendations (in progress)
Draft report (in progress)
Review of the draft report by: Other federal agencies (CDC, CMS, AHRQ, HRSA, VA, etc.)
Invited organizations and individuals
Public
Revisions based on comments received
Final report
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Summary • JNC 8 is close • Hope to build on the current effort for future guidelines
• While there is a need for a complete evidence-‐ based document, there will be areas where evidence is lacking
• IntegraKon of experts/specialists with primary care providers to facilitate true change

9/14/12
14
Active Learning Example You are a reviewer for a study in hypertension. The study is described as a randomized, controlled trial comparing two different drugs on major cardiovascular events. In your review you find that: 1. the paper describes there are about 33% who dropped out. 2. You also find that despite proper design, 20% in each study
arm actually crossed over to other arm. It is not clear in the methods how these crossovers were analyzed.
3. When subjects had a heart aYack or stroke, or other event, the individual who determined if an event actually occurred was aware which treatment the subject received.
Questions 1. How do you think you would rate the quality of this study
(Good, Fair, or Poor)?
2. How likely do you think this study will carry significant weight in making treatment recommendaKons?
3. If this is the only study in the literature that could be used to answer one of your criKcal quesKons and you must make a specific recommendaKon or statement, what strength do you think this recommendaKon might have? (Strong, Moderate, Weak, Against, Expert Opinion, No RecommendaKon)
Thank You
Contact Information: