Embed Size (px)
DESCRIPTION
Citation preview

Prevention of Prematurity and Stillbirth - Epidemiology, Evidence, and Research
James A. Litch, MD, DTMHDirector, Perinatal Interventions Program Global Alliance for Prevention of Prematurity and Stillbirth (GAPPS)
Clinical Assistant Professor,Department of Global HealthDepartment of Epidemiology

Outline
• Millennium Development Goals (MDGs) progress • Definitions• Epidemiology• What we know - Evidence review for interventions• What we don’t know - Research activities
• Note - All numbers reported in this presentation are estimates impeded by a variety of assumptions and classification/reporting systems

Millennium Development Goals (MDGs)
Global <5 child mortality rate has declined by a third, from 89 deaths per 1,000 live births in 1990 to 60 in 2009.
All regions, except sub-Saharan Africa, Southern Asia and Oceania, have seen reductions of at least 50 per cent.
Number of deaths in children under five worldwide declined from 12.4 million in 1990 to8.1 million in 2009.
Nearly 12,000 fewer children dying each day.

Millennium Development Goals (MDGs)
In developing regions, maternal mortality ratio dropped by 34% between 1990 and 2008, from 440 maternal deaths per 100,000 live births to 290 maternal deaths.
Despite proven interventions that could prevent disability or death during pregnancy and childbirth, maternal mortality remains a major burden.

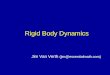
Definition of preterm birth: Babies born alive before 37 completed weeks of pregnancy
What is preterm birth?
Late and moderate
preterm
32 to <37 weeks
84%
Very preterm28 to <32 weeks10%
Extremely preterm
< 28 weeks
5%
Source: Chap 5, Born Too Soon
Born Too Soon Report

Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(10)62187-3.
What is stillbirth?• Classification for most LMIC is a birthweight of at least 1000 g or a
gestational age of at least 28 weeks (third trimester stillbirth)– Essential for international comparability, poorly applied – New stillbirth estimates for 193 countries published in Lancet
Series use this definition – WHO definition — a "fetal death late in pregnancy" and allows each
country to define the gestational age at which a fetal death is considered a stillbirth for reporting purposes. Some countries define stillbirth as early as 16 weeks of gestation, whereas others use a threshold as late as 28 weeks (1000 g).
• In some high-income countries other definitions are used – In UK stillbirths are counted from 24 weeks– In USA, Australia and New Zealand from 20 weeks
If high income country stillbirth definitions were used for all countries then the global total would be much higher
eg for USA with WHO definition 13,070, USA definition 27,500

Major Causes of Under-5 Deaths Globally
Cause of Mortality Annual <5 Deaths
Respiratory infections 2 million
Diarrheal diseases 1.6 million
Malaria 1.1 million
Preterm births 1 million
Childhood-cluster diseases
1 million
HIV/AIDS 340,000
Tuberculosis 40,000
Sources: Jamison, Sonbol, Jamison et al. 2006; Lawn, Wilczynska-Ketende et al. 2006; Stanton, Lawn et al. 2006
3.2 millionStillbirths
Not counted

Changes in Causes of Newborn Deaths

Note: rates by country are available on the accompanying wall chart. Not applicable=non WHO Members StateSource: Blencowe et al National, regional and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications
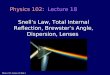
Of the 11 countries with the highest rates, 9 are in Africa
First ever national estimates of preterm birth for 192 countries – where are the highest rates?
11 countries with preterm birth rates over 15% 1.Malawi2.Congo3.Comoros4.Zimbabwe5.E. Guinea6.Mozambique7.Gabon8.Pakistan9.Indonesia10.Mauritania11.Botswana
Born Too Soon Report

Note: rates by country are available on the accompanying wall chart. Not applicable=non WHO Members StateSource: Blencowe et al National, regional and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications
Preterm births – where are the biggest numbers?
Truly a global problem, affecting all countries60% are in South Asia and sub-Saharan Africa but with less care
10 countries account for 60% of the world’s preterm births1.India2.China3.Nigeria4.Pakistan5.Indonesia6.United States of America7.Bangladesh8.Philippines9.Dem Rep Congo10.Brazil
Born Too Soon Report

Preterm Births by Gestational Age and Region for 2010
• 75% of preterm deaths are in Sub-Saharan Africa and Southern Asia
• 80% of 32-37 week preterm babies can survive with essential care
• Level of care determined by gestational age

Causes of Death Due to Preterm Birth
Underlying Pathology Cause of DeathLung immaturity Hypoxia
Acute respiratory distress syndrome (ARDS)
Inability to tolerate labor Birth asphyxia
Poor temperature regulation Hypothermia
Infection SepsisPneumonia
Poor feeding HypoglycemiaDehydrationPour weight gain

Challenges for Preterm Prevention: Multiple Social, Biological, and Clinical Risk Factors• Chorioamnionitis • Bacterial vaginosis• Periodontal disease• Maternal morbidity• Incompetent cervix• Low pre-pregnancy weight• Poor weight gain• Twins, triplets• Congenital malformations• Genetics• Prior preterm birth
• Poor nutrition• Poor pregnancy weight gain• Maternal age• Marital status• Poverty• Black race• Tobacco use• Substance use• Stress • Physical exertion

Country variation in stillbirth rates
Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(10)62187-3.
10 countries account for 66% of the world’s stillbirths – and 66% of neonatal deaths and 60% of maternal deaths 1. India2. Pakistan3. Nigeria4. China5. Bangladesh6. Dem Rep Congo7. Ethiopia8. Indonesia9. Tanzania10. Afghanistan
Stillbirth rates (deaths per 1000
livebirths)
Lowest countries1.Finland (2)2.Singapore (2)
Highest countries192. Nigeria (42)193. Pakistan (47)
Stillbirth rates (deaths per 1000
livebirths)
Lowest countries1.Finland (2)2.Singapore (2)
Highest countries192. Nigeria (42)193. Pakistan (47)
2.6 (2.08 to 3.79) million stillbirths 98% occur in low-income and middle-income countries

Stillbirths during labour – 1.2 million a year
Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(10)62187-3.
Approximately of 40% of stillbirths are during labor

Major Causes of stillbirths1. Childbirth complications2. Maternal infections in pregnancy (eg
syphilis, malaria)3. Maternal conditions, especially
hypertension and diabetes4. Fetal growth restriction5. Congenital abnormalities
Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(10)62187-3.
These overlap with the causes of maternal and neonatal deaths

• Identified evidence-based interventions to prevent preterm birth and stillbirth
• About 2,000 studies on preterm birth, stillbirth or
related interventions were evaluated.
• Out of 82 existing interventions, 49 were selected
for in-depth reviews. • Selection was based on the presence of a reasonable amount of evidence and relevance
to low- and middle-income countries.
• Commissioned by Gates Foundation
• Available at www.gapps.org
2010 Global Report on Preterm Birth & Stillbirth


Summary of assessments for INTRAPARTUM preterm birth and stillbirth interventions (based on GRADE system)

Premature baby carePrevention of preterm birth
• Essential and extra newborn care (thermal care, feeding support, early breastfeeding, and vitamin K at delivery
• Neonatal resuscitation
• Prolonged Skin-to-Skin Care
• Management of premature babies with complications especially respiratory distress syndrome, infections and jaundice
• Progressing towards comprehensive neonatal intensive care
Management of preterm labor
•Prophylactic corticosteroids
•Antibiotics for pPROM
•Tocolytics to slow down labor
Reduction of preterm birth
Mortality reduction among babies born preterm
• Preconception care package especially family planning
• Smoking cessation and employment safeguards of pregnant women (PG to prevent recurrent preterm birth)
• Antenatal care package
• Effective childbirth care
Quality evidence and strong recommendation for LMICs to reduce the burden of preterm birth
Priority interventions for preterm baby care team due to unique capability of driving significant preterm mortality reduction in a cost-effective manner

21
Estimated Lives Saved of Premature Babies in Settings with Universal Coverage of Basic Interventions (without NICU)
520,000 lives (55%) saved of premature babies could be prevented if adequate management of preterm labor and birth.
760,000 lives (80%) saved if family planning included in model.

Prevention of intrapartum stillbirth
Prevention of antepartum stillbirth
•Effective childbirth care
•Neonatal resuscitation
•Progressing towards comprehensive Emergency Obstetric Care
Management of intrapartum
complications•Management of prolonged labor•Magnesium sulfate•Antibiotics•Active management of third stage•Induction of labor at or beyond 41 completed weeks
Reduction of antepartum stillbirth
Reduction of intrapartum stillbirth
• Preconception care package especially family planning
• Antenatal care package/BPP• Periconceptual folic acid and
maternal nutrition• Malaria in pregnancy (IPTp/ITN)• Syphilis screening and treatment• Diabetes screening and
management• Smoking cessation and fetal
growth restriction management
Quality evidence and strong recommendation for LMICs to reduce the burden of stillbirth
Born Too Soon Report

Modeling reduction in stillbirth: 10 evidence-based interventions
Interventions considered in the model99%
coverage Stillbirths
Reduction
1 Periconceptual folic acid fortification 27,000 1%
2 Malaria in pregnancy - ITNs & IPTp 35,000 1%
3 Syphilis screening and treatment 136,000 5%
4 Hypertensive diseases in pregnancy and management 57000 2%
5 Diabetes screening and management 24,000 1%
6 Fetal growth restriction management 107,000 4%
7 Induction of labor at or beyond 41 completed weeks 52,000 2%
8,9,10 Obstetric Care (3 levels of care) 696,000 28%
Total Stillbirths Averted1,134,00
0 45%
Basic antenatal
care
Advanced antenatal
care
Childbirth care
Source: Pattinson R et al. Stillbirths: how can health systems deliver for mothers and babies? Lancet 2011.
1.1 million stillbirths (45%) could be prevented.1.6 million (70%) if family planning included in model.
0.7 million (30%) could be prevented by obstetric care alone.But need higher coverage and quality of care

Potential for lives saved through steroid injections for women in preterm labor
Respiratory complications due to lung immaturity (RDS) are the commonest cause of death in preterm babies.
Single course of antenatal steroids to women in preterm labour: •31% Mortality reduction (RR 0.69, 95% CI 0.58 to 0.81) for babies in settings where ventilation (+/-surfactant is standard of care (Cochrane review))
•53% reduction in mortality in 4 studies in middle income countries (RR 0.47, 95% CI 0.35 to 0.64)
Could save about 400,000 babies each year if reached 95% of women in preterm labor (LiST analysis)
Dexamethasone is low cost (<$1) and available in many settings but low coverage in low and middle income settings
One of the 13 priority medicines listed by UN Commodities Commission
Born Too Soon Report
Source: Chap 6 , Born too soon,

Potential for lives saved through continuous skin-to-skin care
Baby is tied skin to skin with mother 24 hours a day for days/weeks providing
•thermal care•increased breastfeeding, better weight gain•reduced infections and links to additional supportive care, if needed, and earlier discharge
Mortality reduction 51% for babies < 2000 gm, in facilities, clinically stable and started within one week compared to incubator care
Effective entry point for care of preterm babies
Chap 5 and 5, Born too Soon>Impact data from Lawn et al ‘Kangaroo mother care’ to prevent neonatal deaths due to preterm birth complications. Int J Epid: 2010,Conde Aguedelo Cochrane review 2011
Could save about 450,000 babies each year if reached 95% of preterm babies (LiST analysis)
Born Too Soon Report

Thank you
Global Alliance to Prevent Prematurity and Stillbirth (GAPPS) leads a collaborative, global effort to increase awareness and accelerate innovative research and development to make every birth a healthy [email protected] [email protected]









![Logic Models Handout 1. Morehouse’s Logic Model [handout] Handout 2](https://img.pdfslide.us/doc/110x75/56649e685503460f94b6500c/logic-models-handout-1-morehouses-logic-model-handout-handout-2.jpg)