Embed Size (px)
Citation preview
Jennifer Smith & Kelly Strine
Congestive Heart Failure
Congestive Heart Failure• Results from any structural or functional disorder that impairs the ability of
the ventricle to contract and effectively pump blood to meet the metabolic needs of the tissue.
• Affects the cardiovascular and pulmonary system• Associated with a hypercoagulable state• Increased trend of heart failure with preserved ejections fraction of 50% or
higher• Classified as “diastolic”(preserved ejection fraction) or “systolic” (reduced
ejection fraction• Patients may have both diastolic and systolic dysfunction
(Dunphy, Winland-Brown, Porter & Thomas, 2011)
NYHA Functional Classifications• Class I: No limitation of physical activity; ordinary physical activity does not
cause undue fatigue, palpitations, or dyspnea
• Class II: Slight limitation of physical activity; comfortable at rest, but ordinary activity results in fatigue, palpitations, or dyspnea
• Class III: Marked limitation of physical activity; comfortable at rest, but less than ordinary activity results in fatigue, palpitations, or dyspnea
• Class IV: Unable to carry on any physical activity without discomfort; symptoms present at rest if any activity is undertaken, discomfort is increased
(McMurray, 2010)
Pathophysiology• Myocardial injury leads to pathologic remodeling of left ventricle affecting its
size, shape, and function impairing its contraction• Neurohumoral imbalance, increased cytokines, and inflammatory changes• Apoptosis results in energy starvation and oxidative stress• Tissue hypoperfusion• Elevated levels of norepinephrine, angiotensin II, aldosterone, endothelin,
vasopressin, and cytokines• Inadequate delivery of oxygen• Results in pulmonary and systemic venous hypertension• Progressively worse if left untreated• Exacerbated by additional injury (e.g. myocardial infarction)• Sympathetic Stimulation- increased heart rate• Activation of renin-angiotensin-aldosterone system• Hypertrophy
(McMurray, 2010)
Etiology• Coronary Heart Disease• Myocardioal Infaction• Hypertension• Diabetes• Cardiomyopathy• Valvular Disease• Arrhythmias• Congenital Heart Defects• Thyroid Disorders• Alcohol/Cocaine or other Drug use
(Dunphy, Winland-Brown, Porter & Thomas, 2011)
Pathophysiology• Systolic Dysfunction
Forward Heart Failure
• Diastolic DysfunctionBackward Heart Failure
• Left Sided Heart Failure
• Right Sided Heart Failure
(Dunphy, Winland-Brown, Porter & Thomas, 2011)
Incidence• Affects approximately 5 million in U.S.• Over 550,000 diagnosed each year• Primary reason for 12-15 million office visits• 6.5 million hospital days per year• 80% of hospitalized patients >65• <1% in those less than 50• Most common Medicare diagnoses• More common in males• African Americans have higher risk
(Hunt et al, 2011)
Screening• Evaluate potential risk factors with thorough history• Assess patient’s ability to perform ADL’s• Assess fluid volume status, orthostatic BP, BMI• Screen for cardiac risk factors• Initial laboratory evaluation• Twelve lead electrocardiogram• Echocardiogram• Coronary arteriography in patients presenting with HF
and angina• Stress testing
Risk Factors• Coronary Artery Disease• Myocardial Infarction• Hypertension • Valvular Heart Disease• Diabetes Mellitus• Cardio toxic Medications• Genetics (Familial cardiomyopathy)• Mediastinal Radiation• Obesity/Metabolic Syndrome• Rheumatic Heart Disease• Obstructive Sleep Apnea• HIV• Illicit drugs and ETOH• Congenital Heart Defect• Kidney disease
(Hunt et al, 2011)
Subjective Clinical Findings• Dyspnea at rest worse with exertion• Fatigue• Generalized weakness• Exercise Intolerance• Fluid Retention, Edema• Abdominal bloating • Nocturnal nonproductive cough• Orthopnea• Paroxysmal nocturnal dyspnea• Wheezing at night with no history of asthma or infection• Anorexia or dull pain right upper quadrant
(Dunphy, Winland-Brown, Porter & Thomas, 2011)
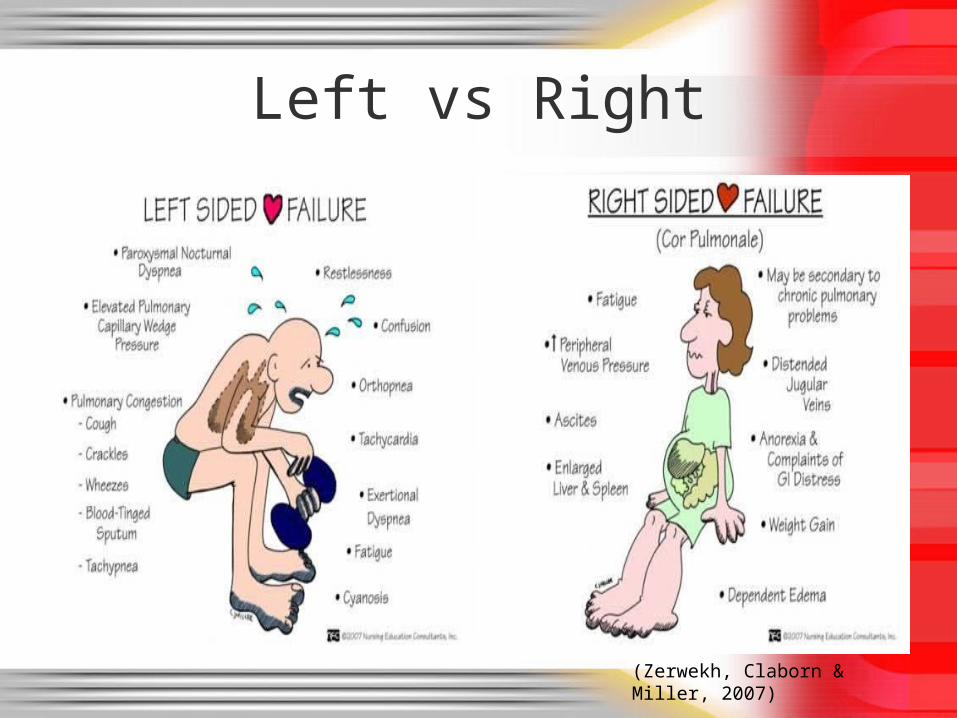
Left vs Right
(Zerwekh, Claborn & Miller, 2007)
Physical Findings• Rales and sometimes wheezing• Peripheral edema• Cool extremities• Ascites• Elevated JVD• S3 gallop • Pre-sacral edema• Scrotal Edema• Hepatomegaly• Hypoxemia• Pleural effusion and tenderness• Worsening mitral or tricuspid regurgitation• May have an arrhythmia• Altered mental status
(Dunphy, Winland-Brown, Porter & Thomas, 2011)
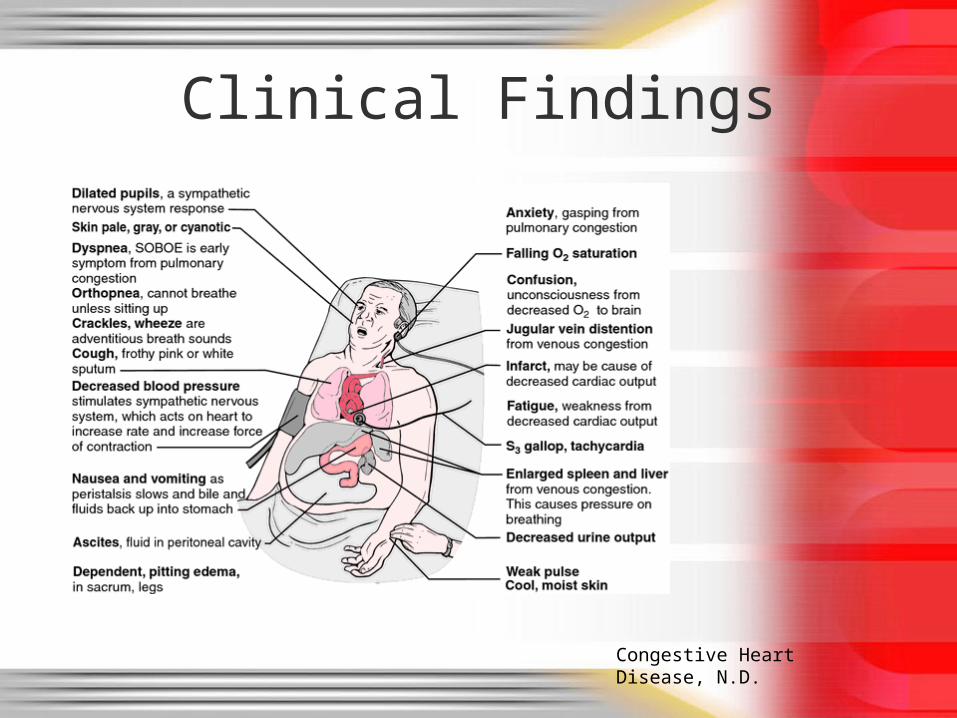
Clinical Findings
Congestive Heart Disease, N.D.
Differential Diagnosis• Pulmonary embolism• Exertional asthma• Cardiac ischemia• COPD• Constrictive pericarditis• Nephrotic syndrome• Cirrhosis• Venous occlusive disease• Anemia• Sepsis• Hyperthyroidism• Peripheral edema
(Domino, 2011)
Social Considerations• Alcohol consumption should be no more than 1 glass of wine per day.
• Dietary sodium restriction of 2 grams per day or lower is recommended.
• Regular exercise should be encouraged as it improves functional status and decreases symptoms. Cardiac rehab is available to assist with this.
• Abstaining from cigarette smoking and avoidance of second hand smoke is recommended.
• Immunizations from influenza and pneumococcal vaccine can reduce risk of respiratory infection.
Laboratory Tests• Complete blood count• Urinalysis• CMP or serum electrolytes to include calcium, magnesium, blood urea
nitrogen, serum creatinine, fasting blood glucose• GFR• Lipid panel• Liver Function Tests• Thyroid Stimulating Hormone• Serum natriuretic peptide (BNP)• HGA1C • Laboratory tests for rheumatologic diseases such as amyloidosis and
pheochromocytoma
Diagnostics• Chest x-ray (PA and lateral) • Two-dimensional echocardiogram is most useful test to determine ejection
fraction and valvular abnormalities• Twelve-lead electrocardiogram• Maximal Exercise Stress Testing• Nuclear imaging for estimation of ventricle size, perfusion, and systolic
function• Coronary arteriography with angina or ischemia• Endometrial biopsy • Holter monitoring• Electrophysiology studies• Cardiac MRI or transesophageal Doppler 2D echocardiography• Peak flow or spirometry
Management• Goal of therapy is to decrease symptoms, hospitalizations, and
prevent premature death• Reduce pulmonary venous pressure and congestion• Identify and treat the cause of the heart failure • Recognize and treat underlying heart disease or comorbidities such
as diabetes hypertension or hyperlipidemia• Adjust diuretics therapy to maintain dry weight• Rate control for atrial fibrillation• Eliminate tachycardia• Treat hypertension• Prevent thrombus formation
(Dunphy, Winland-Brown, Porter & Thomas, 2011)
Non-Pharmacological• Fluid Restrictions < 2L/day• Low Sodium Diet < 2 g/day• Daily weights after voiding in the morning• Exercise program and rehabilitation program• Lifestyle modifications: smoking cessation, alcohol limitations, illicit drug use• Coronary Revascularization• Valve Replacement• Cardiac Transplant• Resynchronization• Implantable cardioverter-defibrillator (ICD)• Biventricular Pacing• Treat anemia
(McMurray, 2010)
Pharmacological• Diuretics including loop diuretics, thiazides, potassium-sparing • Angiotensin-converting enzyme (ACE) inhibitors (1st line with diuretics)• Angiotensin-II receptor antagonist- Losartan, Valsartan• Aldosterone antagonist- (Spironolactone)• Hydralazine in combination with nitrate• Beta-blockers (1st line therapy in systolic dysfunction)• Digoxin• Calcium channel blocker (Amlodipine)• Vasodilators-nitrates• Anticoagulants• Antiplatelets• Inotropic agents (dobutamine, milrinone)• Morphine for acute treatment of associated pulmonary edema• NSAIDS contraindicated
(Verdecchia, et al., 2009)
Complications• Declining functional capacity• Electrolyte disturbances• Acute pulmonary edema• Frequent hospitalizations• Atrial fibrillation• Left ventricular thrombus• Cerebral embolism• Sudden death from arrhythmia• Renal failure• Death
(Owan et al, 2006)
Follow Up• Cardiologist Referral is recommend at the onset of symptoms.
• The Joint Commission has established mandated core measures for hospitalized patients. Assessment of left ventricular function with Ejection Fraction (EF) noted If EF less than 40% patient must be placed on an ACEI or ARB Counseling on smoking cessation must occur Discharge education must include activity level, diet, discharge medications, follw0up
appointments, weight monitoring, what to do if symptoms worsen
• Upon discharge home, it is recommended that patients have intensive home-care surveillance with home care nurses to decrease the need for hospitalization.
• Patients should be seen by their provider within 1 week of discharge and at least every 3 months thereafter.
Consultation/Referral• Multidisciplinary Team Approach• Refer patients with suspected heart failure and a BNP between 100 and 400
pg/ml to have transthoracic Doppler 2D echocardiography and to see a cardiologist within 2 weeks
• Seek specialist advise before offering second-line treatment to patients with HF due to left ventricular systolic function
• Pulmonologist• Cardiac Rehab Program• Support Groups• Dietician• Home Health• Transplant• Hospice
References• Aurigemma, G.P. & Gaasch, W.H. (2004, September). Diastolic heart failure. The New England
Journal of Medicine. 351(11), 1097-1105.• Congestive heart disease. (n.d.) Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing,
and Allied Health, Seventh Edition. (2003). Retrieved January 25 2014 from http://medical-dictionary.thefreedictionary.com/Congestive+heart+disease
• Domino, F. (2011). Griffith’s 5 Minute Clinical Consult. 19th Ed. Lippincott Williams & Wilkins.• Dunphy, L. M., Winland-Brown, J. E., Porter, B. O., & Thomas, D. J. (2011). Primary care: The art
and science of advanced practice nursing. (3 ed.). Philadelphia, PA: F.A. Davis Company.
• Hunt, S.A., Abraham, W.T., Chin, M.H., Feldman, A.M., Francis, G.S., Ganiats, T.G., Jessup, M., Konstam, M.A., ACC/AHA 2005 Guideline update for the diagnosis and treatment of heart failure adult: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines: Developed in collaboration with the American College of Chest Physician and the International Society for heart and lung transplantation. Circulation, 2005, 112, 154-235.
doi://10.1161/CIRCULATIONAHA.105.167586.• Homma, S., Thompson, J.L., Pullicino, P.M., Levin, B., Freudenberger, R.S., Teerlink, J.R.,
Ammon, S• Graham, S., Sacco, R.L., Mann, D.L., Mohr, J.P., Massie, B.M., Labovitz, A.J., Anker, S.D., Lok,
D.J., Ponikowski, P., Estol, C.J., Lip, G., Di Tullio, M.R., Sanford, A.R., Mejia, V., Gabriel, A.P.,
Valle, M.L., & Buchsbaum, R. (2012, May). Warfarin and aspirin in patients with heart failure and
sinus rhythm. The New England Journal of Medicine. 366(20), 1859-1869.
McMurray, J.V. (2010). Systolic heart failure. The New England Journal of Medicine. 362(3), 228-38.
References• Owan, T.E., Hodge, D.O., Herges, R.M., Jacobsen, S.J., Roger, V.L., & Redfield, M.M. (2006,
June). Trends in prevalence and outcome of heart failure with preserved ejection fraction. The
New England Journal of Medicine. 355(3). 251-259.• Verdecchia, P., Angeli, F., Cavallini, C., Gattobigio, R., Gentile, G., Staessen, J. A., et al. (2009).
Blood pressure reduction and renin-angiotensin system inhibition for prevention of congestive heart failure: A meta-analysis. European Heart Journal, 679-688.
• Zerwekh, J., Claborn, J. C., & Miller, C. J. (2007). Memory notebook of nursing. (4 ed., Vol. 2). New York, NY: Nursing Education Consultants.
Questions1. The treatment goals for HF include:
A. Improve symptoms
B. Optimize fluid volume status
C. Restore normal oxygenation
D. Identify and treat etiology
E. All the above
2. The practitioner should pay particular attention to the presence of which of the following findings that suggest HF on the physical exam:
E. Elevated JVD
F. Peripheral edema
G. Third heart beat
H. Diminished lung sounds
I. Both A and C
J. All of the above
Questions3. Patients that have heart failure with an ejection fraction >50% are classified as:
A. Systolic heart failure
B. Diastolic heart failure
4. How would a patient that has dyspnea on less-than ordinary exertion would be classified according to the NYHA
A. NYHA Class I
B. NYHA Class II
C. NYHA Class III
D. NYHA Class IV
5. The most useful diagnostic test to evaluate patients with heart failure is:
E. CXR
F. Stress Test
G. 2-D echocardiogram
6. The following would be a contraindication in ACEI except:
A. Angioedema
B. Hypernatremia
C. Serum creatinine > 3.0
D. Hyperkalemia >5.5
7. Which medication classification can be substituted for ACEI:
E. Beta-blockers
F. Vasodilator
G. Angiotensin II Receptor Blocker
H. Aldosterone antagonists
8. Patients taking aldosterone antagonists require frequent monitoring for:
I. Increased edema
J. Worsening HF
K. Hyperkalemia
L. Hypotension
Questions
Questions9. Patients taking diuretics should be monitored frequently for:
A. Renal dysfunction
B. Electrolyte abnormalities
C. Symptomatic hypotension
D. Gout
E. All of the above
10. Diuretics should be administered at doses high enough to:
F. Allow the patient to eat and drink whatever they want
G. Improve signs and symptoms of congestion
H. Reduce blood pressure enough that a ACEI will not be required