Embed Size (px)
Citation preview

Jeffrey S. Weber, MD, PhD Deputy Director
Laura and Isaac Perlmutter Cancer Center Professor of Medicine
NYU Grossman School of Medicine New York, NY

ECHO Series: Patient Interaction in Optimizing Treatment of Advanced Melanoma
Agenda
Part 1: Diagnosis and Management of Melanoma
I. Pathophysiology of Advanced Melanoma a. Tumor microenvironment and resultant disease processes b. Evading immune recognition – multiple tumor mechanisms c. Factors contributing to underdiagnosis/misdiagnosis/late diagnosis of melanoma
II. Therapeutic Mechanisms of Action in Advanced Disease a. Immune checkpoint inhibition
i. CTLA-4 inhibition and anti-tumor effects ii. PD-1 inhibition and anti-tumor effects
b. Oncolytic virus immunotherapy and anti-tumor effects
III. Clinical Trial Data and the Treatment of Advanced Melanoma a. Current treatment guidelines b. Clinical trial data on immune checkpoint inhibitors in melanoma
i. Immunotherapy regimens in the first-line treatment of unresectable, metastatic melanoma. ii. Immunotherapy regimens in the second-line treatment of unresectable, metastatic melanoma.
iii. Immunotherapy agents in the adjuvant setting c. Determination of patient response
i. Response Evaluation Criteria in Solid Tumors (RECIST) ii. Immune response-related criteria and CTLA-4 and PD-1 inhibition
IV. Recognition and Management of Immune-Related AEs a. What are immune-related adverse events?
i. Location, presentation, identification, and timing ii. Communication of potential AEs to the individual patient
b. Management of irAEs i. Management options and recommendations
ii. Monitoring for response
V. Shared Decision-Making in the Management of Melanoma a. Benefits of shared decision-making b. Strategies to implement shared decision-making in clinical practice c. Patient education d. Decision aids e. NCCN goals of conversation
Part 2: Case Studies in Melanoma
VI. Case Studies Conclusions Questions and Answers

ECHO Series: Patient Interaction in Optimizing Treatment of Advanced Melanoma
FACULTY
Jeffrey S. Weber, MD, PhD Deputy Director
Laura and Isaac Perlmutter Cancer Center Professor of Medicine
NYU Grossman School of Medicine New York, NY
PROGRAM OVERVIEW
This program will review the diagnosis and management of patients with advanced or metastatic melanoma.
TARGET AUDIENCE
This activity is designed to meet the educational needs of medical oncologists, dermatologists, and other healthcare providers involved in the care of patients with melanoma.
LEARNING OBJECTIVES
Upon the completion of this program, attendees should be able to:
• Develop individualized treatment plans for the management of advanced or metastatic melanoma that incorporate clinical trial data and current treatment guidelines
• Recognize and effectively manage immune-related adverse events associated with the use of immune checkpoint inhibitors
• Implement shared decision-making in clinical practice to improve patient interaction and education
ACCREDITATION STATEMENT
Med Learning Group is accredited by the Accreditation Council for Continuing Medical Education to provide
continuing medical education for physicians.
This CME activity was planned and produced in accordance with the ACCME Essentials.
CREDIT DESIGNATION STATEMENT
Med Learning Group designates this live activity for a maximum of 1.0 AMA Category 1 CreditTM. Physicians
should claim only the credit commensurate with the extent of their participation in the live activity.

NURSING CREDIT INFORMATION
Purpose: This program would be beneficial for nurses involved in the treatment of patients with melanoma.
Credits: 1.0 ANCC Contact Hour.
CNE Accreditation Statement: Ultimate Medical Academy/CCM is accredited as a provider of continuing
nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. Awarded 1.0
contact hour of continuing nursing education of RNs and APNs.
DISCLOSURE POLICY STATEMENT
In accordance with the Accreditation Council for Continuing Medical Education (ACCME) Standards for Commercial Support, educational programs sponsored by Med Learning Group must demonstrate balance, independence, objectivity, and scientific rigor. All faculty, authors, editors, staff, and planning committee members participating in an MLG-sponsored activity are required to disclose any relevant financial interest or other relationship with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services that are discussed in an educational activity.
DISCLOSURE OF CONFLICTS OF INTEREST
Dr. Weber has intellectual property or is a patent holder on a PD-1 biomarker by Biodesix and on a CTLA-4 biomarker by Moffitt Cancer Center. He has received consulting fees from BMS, Merck, GSK, Genentech, Array, Alkermes, AstraZeneca, Celldex, Sellas, Biond, Pfizer, CytomX, WindMIL, and Proteanr. He has been contracted for research with NextCure; and has ownership interests in Biond, ImmunoMax, and CytomX.
CME Content Review The content of this activity was independently peer reviewed.
The reviewer of this activity has nothing to disclose.
CNE Content Review The content of this activity was peer reviewed by a nurse reviewer.
The reviewer of this activity has nothing to disclose.
Staff Planners and Managers
The staff, planners, and managers reported the following financial relationships or relationships to products or
devices they or their spouse/life partner have with commercial interests related to the content of this CME/CE
activity:
Matthew Frese, MBA, General Manager of Med Learning Group, has nothing to disclose.

Christina Gallo, SVP, Educational Development for Med Learning Group, has nothing to disclose.
Marcello A. Morgan, MD, MPH, Medical Director for Med Learning Group, has nothing to disclose. Lauren Welch, MA, VP, Accreditation and Outcomes for Med Learning Group, has nothing to disclose.
Lisa Crenshaw, Senior Program Manager for Med Learning Group, has nothing to disclose.
Russie Allen, Accreditation and Outcomes Coordinator for Med Learning Group, has nothing to disclose.
DISCLOSURE OF UNLABELED USE
Med Learning Group requires that faculty participating in any CME activity disclose to the audience when
discussing any unlabeled or investigational use of any commercial product or device not yet approved for use
in the United States.
During this lecture, the faculty may mention the use of medications for both FDA-approved and non-approved
indications.
METHOD OF PARTICIPATION There are no fees for participating and receiving CME credit for this live activity. To receive CME/CNE credit
participants must:
1. Read the CME/CNE information and faculty disclosures.
2. Participate in the web-based live activity.
3. Submit the evaluation form to Med Learning Group.
You will receive your certificate upon completion.
DISCLAIMER
Med Learning Group makes every effort to develop CME activities that are science based.
This activity is designed for educational purposes. Participants have a responsibility to use this information to
enhance their professional development in an effort to improve patient outcomes. Conclusions drawn by the
participants should be derived from careful consideration of all available scientific information. The participant
should use his/her clinical judgment, knowledge, experience, and diagnostic decision making before applying
any information, whether provided here or by others, for any professional use.
For CME questions, please contact Med Learning Group at [email protected]

Contact this CME provider at Med Learning Group for privacy and confidentiality policy statement information
at http://medlearninggroup.com/privacy-policy/
Provided by Med Learning Group
Co-provided by Ultimate Medical Academy/Complete Conference Management (CCM).
Supported by an educational grant from Merck & Co., Inc. Copyright © 2020 Med Learning Group. All rights reserved. These materials may be used for personal use only. Any rebroadcast, distribution, or reuse of this presentation or any part of it in any form for other than personal use without the express written permission of Med Learning Group is prohibited.

1
ECHO Series: Patient Interaction in Optimizing Treatment of
Advanced Melanoma
Jeffrey S. Weber, MD, PhD
Deputy Director
Laura and Isaac Perlmutter Cancer Center
Professor of Medicine
NYU Grossman School of Medicine
New York, NY
Disclosures
• Dr. Weber has received consulting fees from BMS, Merck, GSK, Genentech, Array, Alkermes, AstraZeneca, Celldex, Sellas, Biond Biologics, Pfizer, CytomX, WindMIL, and Proteon. He has been contracted for research with NextCure and has ownership interests in Biond, ImmunoMax, and CytomX. He has intellectual property or is a patent holder on a PD‐1 biomarker by Biodesix and on a CTLA‐4 biomarker by Moffitt Cancer Center.
• During the course of this lecture, faculty may mention the use of medications for both FDA‐approved and non‐approved indications.
This activity is supported by educational grant from Merck & Co., Inc.

2
Melanoma Statistics 2020
American Cancer Society (ACS). Key statistics for melanoma skin cancer. (www.cancer.org/cancer/melanoma‐skin‐cancer/about/key‐statistics.html). Accessed May 16, 2020.
• One person dies every 77 minutes from melanoma
• Annual new cases increased 53% over the last decade
• Average age at diagnosis = 65 years
• Melanoma accounts for ~1% of all skin cancer diagnosesbut comprises a large majority of skin cancer‐related deaths
Melanoma quick stats
• 100,350 new cases (60,190 men, 40,160 women)
• 6850 deaths (4610 men, 2240 women)2020 in the US
• Whites: ~2.6% (1 in 38)
• Hispanics: ~0.6% (1 in 167)
• Blacks, Asians/Pacific Islanders: ~0.1% (1 in 1000)
Lifetime risk of developing melanoma
Pathophysiology of Advanced Melanoma

3
What Is Melanoma?
Melanoma is caused by a constitutive dysregulation in melanocytes escaping immune surveillance and leading to tumor formation.
Image courtesy of Dr. Jeffrey Weber.
Melanoma
Pathogenesis of Melanoma
Seuradge J, Wong E. McMaster Pathophysiol Rev. (pathophys.org/melanoma/). Accessed May 16, 2020.
BRAF = B‐type Raf proto‐oncogene; PTEN = phosphatase and tensin homologue; CD = cluster of differentiation.

4
Stages of Melanoma—I and II
NCCN. Cutaneous melanoma. V2.2020. (Images available at https://visualsonline.cancer.gov/details.cfm?imageid=7277; https://visualsonline.cancer.gov/details.cfm?imageid=7283; https://visualsonline.cancer.gov/details.cfm?imageid=12521; https://visualsonline.cancer.gov/details.cfm?imageid=12528). Accessed May 16, 2020.
Stage I
Stage II
Clinical Staging (cTNM)
Stage T N M
0 Tis N0 M0
IA T1a N0 M0
IB T1bT2a
N0N0
M0M0
IIA T2bT3a
N0N0
M0M0
IIB T3bT4a
N0N0
M0M0
IIC T4b N0 M0
Pathological Staging (pTNM)
Stage T N M
0 Tis N0 M0
IA T1aT1b
N0N0
M0M0
IB T2a N0 M0
IIA T2bT3a
N0N0
M0M0
IIB T3bT4a
N0N0
M0M0
IIC T4b N0 M0
Stages of Melanoma—III and IV
NCCN. Cutaneous melanoma. V2.2020. (Image available at https://visualsonline.cancer.gov/details.cfm?imageid=7285). Accessed May 16, 2020.
Clinical Staging (cTNM)
Stage T N M
III Any T, Tis ≥N1 M0
IV Any T Any N M1
Pathological Staging (pTNM
Stage T N M
IIIA T1a/b, T2a N1a, N2a M0
IIIB T0 N1b, N1c M0
T1a/b, T2a N1b/c, N2b M0
T2b, T3a N1a/b/c, N2a/b M0
IIIC T0 N2b/c, N3b/c M0
T1a/b, T2a/b, T3a
N2c, N3a/b/c M0
T3b, T4a Any N ≥N1 M0
T4b N1a/b/c, N2a/b/c M0
IIID T4b N3a/b/c M0
IV Any T, Tis Any T M1
Stage IIIStage IV

5
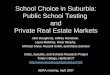
Patient Survival Decreases as Melanoma Disease Stage Increases
Gershenwald JE, et al. CA Cancer J Clin. 2017;67:472–492.
N 5‐YR 10‐YRT1a 5225 98% 98%T1b 2495 99% 96%T2a 3254 96% 92%T2b 748 93% 88%T3a 1590 94% 88%T3b 1150 86% 81%T4a 538 90% 83%T4b 691 82% 75%
Years Since Diagnosis
Melanoma‐Sp
ecific Su
rvival Probab
ility
1.0
0.9
0.8
0.7
0.6
0.50.0
1 2 3 4 5 6 7 8 9 10
Melanoma Unusual Presentations
Images courtesy of Dr. Geoffrey Gibney.

6
Mechanisms of Action of Immune Therapy in Advanced Disease
Avoiding Immune Surveillance
Modified from Schreiber RD, et al. Science. 2011;331:1565‐1570.
CTLA‐4 = cytotoxic T lymphocyte‐associated protein 4; MHC = major histocompatibility complex; PD‐1 = programmed (cell) death 1; PD‐L1 = PD ligand 1; TNF = tumor necrosis factor; CD = cluster of differentiation; NK = natural killer; IFN = interferon; IL = interleukin; MDSC = myeloid‐derived suppressor cells; Treg = regulatory T cell.

7
Immune Checkpoint Blockade CTLA‐4 and PD‐1/PD‐L1 Inhibitors
Ribas A. N Engl J Med. 2012;366:2517‐2519.
FDA‐Approved Immune Checkpoint and Oncolytic Therapies in Melanoma (June 2019)
1. Eggermont AM, et al. N Engl J Med. 2016;375:1845‐1855. 2. Hodi FS, et al. N Engl J Med. 2010;363:711‐723. 3. Wolchok JD, et al. N Engl J Med. 2017;377:2503‐2504. 4. Weber J, et al. N Engl J Med. 2017;377:1824‐1835. 5. Robert C, et al. N Engl J Med. 2015;372:320‐330. 6. Long GV, et al. J Clin Oncol. 2018;36(suppl): abstract 9503. 7. Pembrolizumab (Keytruda®) prescribing information (PI) 2020 (www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf). 8. Eggermont AM, et al. N Engl J Med. 2018;378:1789‐1801. 9. Postow MA, et al. N Engl J Med. 2015;372:2006‐2017. 10. Andtbacka RH, et al. J Clin Oncol. 2015;33:2780‐2788.
Regimen Indication Benefit
Ipilimumab (IPI)1–3 • Resected stage III melanoma• Unresectable advanced melanoma
• Recurrence rate reduced by 24%• Response rate 11–19%
Nivolumab3–5 • Resected stage III & IV melanoma• Unresectable advanced melanoma
• Recurrence rate reduced by 35% over IPI• Response rate 40–44%
Pembrolizumab6–8 • Unresectable advanced melanoma• Resected stage III melanoma
• Response rate 34–42%• Recurrence-free survival 71% (at 18 mo)
Nivolumab/IPI3,9 • Unresectable advanced melanoma • Response rate 58–61%
T-VEC10 • Unresectable advanced melanoma • Durable response rate 16%
mo = month(s).

8
KEYNOTE‐006 Study Design (NCT01866319)
Robert C, et al. N Engl J Med. 2015;372:2521‐2532.
• Primary endpoints: PFS and OS• Secondary endpoints: ORR, DoR, and safety
Patients• Unresectable, stage III or IV melanoma
• ≤1 previous therapy, excluding anti–CTLA‐4, PD‐1, or PD‐L1 agents
• Known BRAF V600 status
• ECOG PS 0/1
• No active CNS metastases
Stratification factors
• ECOG PS (0 vs 1)• Line of therapy (first vs second)• PD‐L1 status (positive vs negative)
Pembrolizumab10 mg/kg IV Q2W
for 2 years
Pembrolizumab10 mg/kg IV Q3W
for 2 years
Ipilimumab3 mg/kg IV Q3W
x 4 doses
n = 279
n = 277
n = 278
R(1:1:1)N = 834
ECOG = Eastern Cooperative Oncology Group; PS = performance status; CNS = central nervous system; IV = intravenous; Q2W = every 2 weeks; Q3W = every 3 weeks; PFS = progression‐free survival; OS = overall survival; ORR = objective/overall response rate; DoR = duration of response.
KEYNOTE‐006: 5‐Year Outcomes
• Phase 3 randomized trial of pembrolizumab (n = 556; combined 2 schedules) vs ipilimumab (n = 278) in patients with unresectable stage III or IV melanoma
Robert C, et al. Lancet Oncol. 2019;20:1239‐1251.
Pembrolizumab Ipilimumab
5-year OS 38.7% 31.0%
4-year PFS 23.0% 7.3%
Complete response 14.0% 3.0%
Grade 3-5 TRAEs 17.0% 20.0%
Overall Survival Median overall survival, months (95% Cl)Ipilimumab 15.9 (13.3‐22.0)Combined pembrolizumab groups 32.7 (24.5‐41.6)HR O.73 (95% Cl, 0.61‐0.88); p=0.00049
Overall Su
rvival (%)
00 5 10 15 20 25 30 35 40 45 50 55 60 65
10
20
30
40
50
60
70
80
90
100 III II
I II
II I
I II I I I I III IIIIII IIIIIIIIII
I IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII
IIII
IIIIII

9
Treat until progression
orunacceptable
toxicity
NIVO 3 mg/kg Q2W +IPI‐matched PBO
NIVO 1 mg/kg + IPI 3 mg/kg Q3W for
4 doses, then NIVO 3 mg/kg Q2W
IPI 3 mg/kg Q3W for 4 doses +
NIVO‐matched PBO
Stratify by:
• Tumor PD‐L1 expression*
• BRAFmutation status
• AJCC M stage
n = 314
n = 316
n = 315
Randomized, double‐blind, phase 3 study to compare NIVO + IPI or NIVO alone to IPI alone
CheckMate 067: Study Design
Wolchok JD, et al. N Engl J Med. 2017;377:1345‐1356.
R1:1:1
• Unresectable ormetastatic melanoma
• Previously untreated
• 945 patients
AJCC = American Joint Committee on Cancer; NIVO = nivolumab; PBO = placebo.
Nivolumab + ipilimumab
(n = 314)Nivolumab(n = 316)
Ipilimumab(n = 315)
Best overall response, n (%)
Complete response (CR) 61 (19%) 52 (16%) 16 (5%)
Partial response (PR) 122 (39%) 88 (28%) 43 (14%)
Stable disease (SD) 38 (12%) 30 (10%) 69 (22%)
Progressive disease (PD) 74 (24%) 121 (38%) 159 (50%)
Unable to determine 19 (6%) 24 (8%) 28 (9%)
Objective response (CR and PR)
Patients with response, n(% [95% CI])
183(58% [53–64])
140(44% [39–50])
59(19% [15–24])
Odds ratio for comparison with IPI (95% CI), P-value
6.46 (4.45–9.38)P <.001
3.57 (2.48–5.15)P <.001
CheckMate 067: Overall Response
Wolchok J, et al. N Engl J Med. 2017;377:1345‐1356.

10
0 9 12 18 36 693 6 15 33 3921 2724 30 42 48 66636057545145
OS (%
)
100
90
70
50
30
0
80
60
40
20
10
Months
NIVO+IPI
NIVO
IPI
316 292 266 245 231 214 201 191 181 175 171 164 158 150 144 140 135 139 137 135 130 78 14 0
315 285 253 227 203 181 163 148 135 128 113 107 99 94 93 90 86 84 81 77 73 36 12 0
314 292 265 247 226 221 209 200 198 192 186 180 178 171 166 160 154 159 157 155 150 92 14 0
52%
44%
26%IPI
53%
46%
30%
64%
59%
45%
58%
52%
34%
No. at risk
CheckMate 067: OS at 5 Years of Follow‐Up
Larkin J, et al. Cancer Res. 2017;77(13 suppl): abstract CT075. Wolchok JD, et al. N Engl J Med. 2017;377:1345–1356. Hodi FS, et al. Lancet Oncol. 2018;19:1480‐1492. Larkin JM, et al. Ann Oncol. 2019;30(suppl 5): abstract 2545.
NIVO+IPI (n = 314)
NIVO(n = 316)
IPI(n = 315)
mOS, mo(95% CI)
NR(38.2‒NR)
36.9 (28.3‒58.7)
19.9 (16.9‒24.6)
HR vs IPI(95% CI)
0.52(0.42‒0.64)
0.63(0.52‒0.76) —
HR vs NIVO(95% CI)
0.83(0.67‒1.03) — —
NIVO
NIVO+IPI
NR = not yet reached.
CheckMate 067: Safety
Hodi FS, et al. Lancet Oncol. 2018;19:1480‐1492.
Discontinuation due to adverse event:40% NIVO‐IPI 13% NIVO15% IPI

11
CheckMate‐511: Evaluation of Less Toxic NIVO+IPI Dosing Regimen
Months
OS
(%
)
0102030405060708090
100
0 3 6 9 12 15 18 24 2721
88.2%(NIVO3+IPI1)
88.0% (NIVO1+IPI3) 81.0%
(NIVO1+IPI3)
79.7% (NIVO3+IPI1)
Overall survival
In spite of reversing the doses, there were no clinically meaningful differences for
ORR, PFS, or OS between groups
Investigator-Assessed Response
ResponseNIVO3 + IPI1
(n = 180)NIVO1 + IPI3
(n = 178)Best overall response, No. (%)
CR 27 (15.0) 24 (13.5)PR 55 (30.6) 66 (37.1)SD 21 (11.7) 21 (11.8)PD 62 (34.4) 47 (26.4)Unknown 15 (8.3) 20 (11.2)
ORR (95% Cl), % 45.6 (38.1–53.1) 50.6 (43.0–58.1)P-value 0.35
Median time to response, mo (range)
2.83 (2.0–17.9) 2.79 (2.3–10.5)
Ongoing responses/ responders, n (%)
63/82 (76.8) 68/90 (75.6)
Median DoR, months NR NR
ORR = overall/objective response rate; DoR = duration of response.
Lebbé C, et al. J Clin Oncol. 2019;37:867‐875. Lebbé C, et al. ESMO, 2018: abstract 4311 (https://oncologypro.esmo.org/meeting‐resources/esmo‐2018‐congress/Initial‐results‐from‐a‐phase‐3b‐4‐study‐evaluating‐two‐dosing‐regimens‐of‐nivolumab‐NIVO‐in‐combination‐with‐ipilimumab‐IPI‐in‐patients‐with‐advanced‐melanoma‐CheckMate‐511). Accessed May 16, 2020.
CheckMate 238: Adjuvant Therapy for Resected Stages IIIB/C/IV Melanoma—Study Design
Weber J, et al. N Engl J Med. 2017;377:1824‐1835. NCT02388906 (https://clinicaltrials.gov/ct2/show/NCT02388906?term=NCT02388906&draw=2&rank=1). Weber JS, et al. Ann Oncol. 2019;30(suppl 5): abstract 3493. Accessed May 16, 2020.
Patients with:
• High‐risk, completely resected stage IIIB/IIIC or stage IV melanoma
• No prior systemic therapy
• ECOG PS 0/1
Follow‐up
Maximum treatment duration of
1 year
NIVO 3 mg/kg IV Q2W and
IPI PBO IV Q3W for 4 doses,
then Q12W from week 24
IPI 10 mg/kg IV Q3W for 4 doses,
then Q12W from week 24 and
NIVO PBO IV Q2W
1:1
n = 453
n = 453
Stratified by:
1) Disease stage: IIIB/IIIC vs IV M1a or M1b vs IV M1c
2) Tumor PD‐L1 status at a 5% cutoff
• Primary endpoint: RFS
• Minimum follow‐up of 36 months for all patients
Database lock: January 31, 2019.

12
Checkmate‐238: RFS in All Patients
Weber JS, et al. Ann Oncol. 2019;30(suppl 5): abstract 3493.
NIVO(n = 453)
IPI (n = 453)
Events, n 188 239
Median RFS, mo (95% CI)
NR (38.7‒NR)
24.9 (16.6‒35.1)
HR (stratified) = 0.68 (95% CI, 0.56–0.82)P <.0001 by log-rank test
58%
70%
62%
45%
61%
51%RFS (%)
Months
0
10
20
30
40
50
60
70
80
90
100
0 6 12 18 24 273 9 15 21 30 45
NIVO
IPI
No. at risk
36 3933 42
453 316 254 221 203 193365 272 235 209 185 170 122 37 12 0
453 353 311 280 261 249394 331 290 270 243 234 178 50 13 0
NIVO
IPI
RFS = recurrence‐free survival.
KEYNOTE‐054 (EORTC 1325): Study Schema
Eggermont AMM, et al. N Engl J Med. 2018;378:1789‐1801. NCT02362594 (https://clinicaltrials.gov/ct2/show/NCT02362594?term=NCT02362594&draw=2&rank=1). Accessed May 16, 2020.
N = 1019
RANDOM
IZED
• Primary endpoint: RFS (6 months), RFS percentage with PD‐L1 positive tumor expression
• Secondary endpoints: DMFS and OS (overall vs PD‐L1 tumor expression), AE
PEMBRO 200 mg IV Q3Wup to 1 year
n = 514
PBOIV Q3W
up to 1 year
n = 505
Randomized, phase 3 study of adjuvant PEMBRO after complete resection of high‐risk stage III melanoma
• ≥18 years old with melanoma
• Complete surgical resection of stage III disease
• No ocular/mucosal melanoma
• No prior medical therapy for melanoma treatment
• No previous CTLA‐4 treatment
Trial dates: 7/2015–7/2023 (estimated)
1:1
RECURRENCE Optional
retreatment:
PEMBRO 200 mg IV Q3W up to 2
years
Part 1: Post‐surgical Part 2: Post‐recurrence
DMFS = distant metastases‐free survival; AE = adverse event.

13
EORTC 1325/KEYNOTE‐054: New RFS Analysis (ASCO 2020)
Cut‐off date (Sept 30, 2019) — duration of follow‐up: median 3 years; 473 RFS events
Slide courtesy of Dr. Alexander Eggermont.
*Stratified by stage given at randomization
Treatment arm Total Event 3 years (95% Cl) HR* (95% Cl)Pembrolizumab 514 190 63.7 (59.2‐67.7%) 0.56 (0.47‐0.68)Placebo 505 283 44.1 (39.6‐48.4%) ReferenceStratified* Logrank P‐value: <0.001
HR: 0.56
Pembrolizumab 514 412 374 351 333 314 189 29 0Placebo 505 360 298 259 226 215 126 28 0
Patients at Risk
Months
% Alive and Recurrence‐free
75.4%
60.2%68.2%
47.1%
67.3%
44.1%
0
0 6 12 18 24 30 36 42 48
10
20
30
40
50
60
70
80
90
100
Talimogene Laherparepvec (T‐VEC)
Courtesy of Dr. Jeffrey Weber.
GM‐CSF = granulocyte macrophage colony‐stimulating factor.

14
Talimogene Laherparepvec (T‐VEC) Phase 3 Study
Andtbacka RH, et al. J Clin Oncol. 2015;33:2780‐2788.
Events/n (%) mOS, mo (95% CI) T-VEC 80/163 (49) 41.1 (30.6–NE)GM-CSF 57/86 (66) 21.5 (17.4–29.6)HR = 0.57 (95% CI, 0.40–0.80); log-rank P <.001
Patient Incidence of AEs (T-VEC)
AEs in 292 patientsAny Grade Grade 3 or 4
No. (%) No. (%)Fatigue 147 (50.3) 5 (1.7)Chills 142 (48.6) 0 (0)Pyrexia 125 (42.8) 0 (0)Nausea 104 (35.6) 1 (0.3)Influenza-like illness 89 (30.5) 2 (0.7)Injection-site pain 81 (27.7) 3 (1.0)Vomiting 62 (21.2) 5 (1.7)Diarrhea 55 (18.8) 1 (0.3)Headache 55 (18.8) 2 (0.7)Myalgia 51 (17.5) 1 (0.3)Arthralgia 50 (17.1) 2 (0.7)Pain in extremity 48 (16.4) 4 (1.4)Pain 47 (16.1) 2 (0.7)Peripheral edema 35 (12.0) 2 (0.7)Constipation 34 (11.6) 0 (0)Cough 31 (10.6) 0 (0)Decreased appetite 30 (10.3) 0 (0)Pruritis 28 (9.6) 0 (0)Cellulitis 17 (5.8) 6 (2.1)Injection-site erythema 15 (5.1) 0 (0)Dyspnea 13 (4.5) 3 (1.0)Injection-site pruritis 5 (1.7) 0 (0)
IIIB/IIIC/IVM1a
OS (%
)
100
80
60
40
20
5 100 15 20 25 30 35 40 45 50 55 60
IVM1b/IVM1c
Study month
Study month
OS (%
)
100
80
60
40
20
5 100 15 20 25 30 35 40 45 50 55 60
T‐VEC
T‐VEC
GM‐CSF
GM‐CSF
Events/n (%) mOS, mo (95% CI) T-VEC 109/131 (83) 13.4 (11.4–16.2)GM-CSF 44/55 (80) 15.9 (10.2–19.7)HR = 1.07 (95% CI, 0.75–1.52); log-rank P= .71
Unique Features of Immunotherapy
• Tumor response kinetics
– Responses can differ from those associated with chemotherapy and targeted therapy, which has led to the development of immune‐related response criteria (irRC)
– One can see slow regression, progression followed by regression, or even new lesions that arise, followed by regression of all existing disease
• Immune‐related adverse events (irAEs)
– Adverse events also differ from those seen with targeted and chemotherapy and usually are due to autoinflammatory side effects or irAEs
Wolchok JD, et al. Clin Cancer Res. 2009;15:7412‐7420. Weber JS, et al. J Clin Oncol. 2015;33:2092‐2099.

15
CTLA‐4 Blockade: Progression Followed by Regression Paradoxical Kinetics of Response to Ipilimumab
Saenger YM, Wolchok JD. Cancer Immunol. 2008;8:1.
Metastatic melanoma
Week 20: regression Week 36: still regressing
Screening Week 12: progression
Managing Immune‐Related Adverse Events (irAEs)
Optimizing Patient Outcomes

16
Possible Mechanisms for irAEs
Postow MA, et al. N Engl J Med. 2018;378:158‐168.
irAEs: Clinical Spectrum
Michot JM, et al. Eur J Cancer. 2016;54:139‐148.
Hypophysitis
Dry mouth
Hypothyroidism
Hepatitis
Rash and vitiligo
Pancreatitis andautoimmune diabetes
Uveitis andorbital inflammation
Enterocolitis
Pneumonitis
Adrenal insufficiency
Arthralgia

17
Immune Checkpoint Inhibitors (ICIs): Considerations
• ICIs block, augment, and amplify T‐cell activity, enhancing tumor recognition and attack
• Collaterally, this amplification can aggravate normal healthy tissue, thereby creating inflammatory “autoimmune‐like” effects (ie, an “‐itis” or “‐opathies”)
• Any new symptoms should be under high consideration as being related to ICI treatment
• Rule out other possible etiologies to symptoms
• Toxicity grading should guide management
– Use CTCAE to be familiar with specific irAE grading
• irAEs typically are mild to moderate and often respond toimmunosuppressant therapy
• Early identification, reporting, and intervention can impact outcomes of symptom management, adherence to medication scheduling, and quality of life
Champlait S, et al. Ann Oncol. 2016;27:559‐574. Madden KM, Hoffner B. Clin J Oncol Nurs. 201721(4 suppl):30‐41.
CTCAE = Common Terminology Criteria for Adverse Events.
Pattern of Onset of irAEs: Kinetics
• Onset is typically 6–12 weeks after start of therapy
– Can occur at any time point, ie, days, weeks, or months after starting therapy
– May wax and wane for up to 2 years
• May impact 1 or more organ systems
• Intensity can range from mild to severe
• Dosing, frequency, and the combination of drugs/therapies can influence toxicity
Modified from Weber JS, et al. J Clin Oncol. 2012;30:2691‐2697.
Toxicity grade
Week0
Week3
Week6
Week6
Time (wk)
Rash, pruritis Diarrhea, colitisLiver toxicity Hypophysitis
0 2 4 6 6 10 12 14
wk = week(s).

18
Incidence of Most Common irAE
Corrie P. Prescriber. 2016;27(7):23‐28.
Ipilimumab PD-1 InhibitorsIpilimumab + Nivolumab
Any body system 27% 16% 56%
Colitis 12% 3% 15%
Skin 3% 2% 6%
Endocrinopathy• Hypopituitarism• Hypothyroidism
3%<1%
<1%1%
NR1%
Liver 2% 3% 20%
Most common cause of death from irAEs is colonic perforation.
NR = not reported.
Management of irAEsBased on CTCAE Severity Grade
Michot JM, et al. Eur J Cancer. 2016;54:139‐148. Puzanov I, et al. J Immunother Cancer. 2017;5:95. Brahmer JR, et al. J Clin Oncol. 2018;36:1714‐1768.
Severity CTCAE Grade
Patient CareSetting Steroids
Other Immunosuppressive
Drugs
Immunotherapyand Subsequent
Approach
1 Ambulatory Not recommended Not recommended Continue
2 Ambulatory
Not recommended upfrontTopical steroids or systemic
steroids oral 0.5–1 mg/kg/d for persistent grade 2
Not recommended Suspend* temporarily
3 HospitalizationSystemic steroids oral or IV 1–2 mg/kg/d for ≥3 d then taper over
4–6 wk
Consider for patients with lack of improvement after 2–3 d of
steroid courseOrgan specialist advised
Suspend and discuss resumption based on risk/benefit ratio with
patient
4
Hospitalization; consider
intensive care unit
Systemic steroids IV methylprednisolone 1–2 mg/kg/d and switch to oral prednisone for
≥3 d with taper over 4–6 wk
Consider for patients with lack of improvement after 2–3 d of
steroid courseOrgan specialist advised
Discontinue permanently
*Outside of skin or endocrine disorders, where immunotherapy can be maintained.irAE = immune‐related adverse event; CTCAE = Common Terminology Criteria for Adverse Events; IV = intravenous.

19
Additional Management Considerations
Weber JS, et al. J Clin Oncol. 2015;33:2092‐2099. Gangadhar TC, Vonderheide RH. Nat Rev Clin Oncol. 2014;11:91‐99. Brahmer JR, et al. J Clin Oncol. 2018;36:1714‐1768. Madden KM, Hoffner B. Clin J Oncol Nurs. 2017;21(4 suppl):30‐41.
Symptom management
Steroid Refractory No response or worsening symptoms on steroids
• Additional immunosuppressant treatment may be needed
− Infliximab 5 mg/kg—may repeat Q4W (GI/colitis)
− Mycophenolate mofetil 1 g twice daily (hepatic)
− Cyclosporine or intravenous immunoglobulin (IVIG) (neurologic)
− Methotrexate
• Do not discontinue steroids; continue and taper when symptoms respond• Collaborate with specialists
Supportive Measures • High dose or prolonged use >4 wk ± additional suppressant therapy
− Consider prophylaxis with antimicrobial/antifungal/antiviral to prevent opportunistic infections (PCP, shingles, candida)
− Collaborate with specialists for long-term/permanent organ dysfunction
GI = gastrointestinal; PCP = pneumocystis pneumonia.
TSH = thyroid‐stimulating hormone; ACTH = adrenocorticotropic hormone; Sx = symptoms; BP = blood pressure; NA+ = sodium; OTC = over the counter.
Slide courtesy of Dr. Jeffrey Weber.
Type of irAE ManagementEndocrine • Hypothyroidism: treat with thyroid hormone, usually long-term
• Hyperthyroidism: in symptomatic patients, treat with beta blockers (propranolol or atenolol)
• Hypophysitis: hormone replacement therapy; consider steroids for headaches or other neurological problems
• Adrenal Insufficiency precautions
GI • Colitis: diet adjustment, systemic administration of steroids, treatment with infliximab if steroid refractory.
• Wean steroids over ~4 weeks
Dermatologic • Topical antihistamines/steroids, OTC medications, behavior modification (ie, heat)
• Initiate corticosteroids (oral or IV depending on severity) to be weaned over several weeks
Neurologic • Consider high-dose steroids (1–2 mg/kg or equivalent)
• Plasmapheresis or IVIG may be required for myasthenia gravis or Guillain Barre syndrome
• Neuroleptics for neuropathy management as needed
Musculoskeletal/Arthritis
• Consider work up for rheumatoid arthritis—needs referral
• If negative, continue supportive care
• Consider 0.5 mg–1.0 mg/kg prednisone or equivalent
irAEs: System‐Based Management and Long‐Term Considerations

20
irAEs: System‐Based Management and Long‐Term Considerations (continued)
LFT = liver‐function test; SOB = shortness of breath; DOE = dyspnea on exertion; EKG = electrocardiogram; CPK = creatine phosphokinase; R/O = rule out; CXR = chest x‐ray; CT = computed tomography (scan); UA = urinalysis; BUN = blood urea nitrogen; Echo = echocardiogram.
Slide courtesy of Dr. Jeffrey Weber.
IrAE Management
Hepatic • Consider high-dose (HD) steroids (1–2 mg/kg or equivalent)• Monitor LFTs—return to grade 1• R/O viral hepatitis• Mycophenolate if steroid refractory
Pulmonary • Consider HD steroids (1–2 mg/kg or equivalent)• Supportive O2
• CXR, CT
Renal • Consider HD steroids (1–2 mg/kg or equivalent)• Monitor output, UA, BUN/creatinine
Ocular • Consider HD steroids (1–2 mg/kg or equivalent)• Ophthalmologic steroid drops, opthalmalogic referral
Cardiac • Consider HD steroids (1–2 mg/kg or equivalent)• Cardiology consult, Echo, EKG, Troponin, CPK levels
Relevant Resources
Guidelines for Management of Immunotherapy Toxicities
2017 ESMO www.esmo.org/Guidelines/Supportive-and-Palliative-Care/ Management-of-Toxicities-from-Immunotherapy
2017 SITC Society for Immunotherapy of Cancer Toxicity Management Working Group. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. See Puzanov I, et al, J Immunother Cancer. 2017;5:95.
2018 ASCO/NCCN Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. See Brahmer JR, et al, J Clin Oncol. 2018;36:1714-1768.
ESMO = European Society for Medical Oncology; SITC = Society for Immunotherapy of Cancer; ASCO = American Society of Clinical Oncology; NCCN = National Comprehensive Cancer Network.

21
Case Studies
Case Study 1—GI and Neurologic Toxicity

22
Case 1—GI and Neurologic Toxicity: Presentation
• A 52‐year‐old man with a distant history of a primary melanoma has abdominal pain and chronic nausea
• After being seen in an ED, he has a CT scan showing an intra‐abdominal 5 cm mass
• A transabdominal CT‐guided biopsy is done on an outpatient basis; it shows evidence of melanoma, with S100, Melan‐A, and SOX‐10 positive cells
• The result shows BRAF that is V600K mutated
• CT of the chest shows small lung nodules
ER = emergency department.
What treatment would you use for this patient?

23
Case 1—GI and Neurologic Toxicity: Initial Treatment
• The treating oncologist elected to treat the patient with ipilimumab/nivolumab combination immunotherapy
• After one dose of the combination, the patient’s nausea and anorexia diminished
• However, after 4 doses, he had low‐grade fatigue and feverishness
• CT scans showed an excellent response at week 12, and maintenance nivolumab was begun
Case 1—GI and Neurologic Toxicity: Follow‐Up
• Just prior to the second nivolumab dose, the patient experienced 2 days of anorexia, a single episode of vomiting, and 5 episodes of diarrhea
• His temperature rose to 38.5⁰C (101.3⁰F)
• In clinic, his creatinine was 1.3, and he mentioned that he had dark urine
Your next plan of action is to…
⁰ = degrees; C = Celsius; F = Fahrenheit.

24
Treatment Considerations
Case 1—GI and Neurologic Toxicity: Hospital Admission
• He was admitted to the hospital, had blood cultures, and was started on broad‐spectrum antibiotics; he had several additional diarrheal stools just after admission
• He was hydrated and C Diff titers were taken and proved to be positive
• KUB/upright showed an ileus and CT scan showed distal large bowel stranding and wall thickening
• Steroids were instituted immediately after admission, with 125 mg solumedrol given once in the ED, then a plan for twice a day IVPB for 2 days, followed by 125 mg IVPB once a day
KUB = kidney, ureter, and bladder; IVPB = intravenous piggyback.

25
Case 1—GI and Neurologic Toxicity: Hospitalization
• The patient was also treated for C diff with a dose of vancomycin, but the ileus did not improve; he required narcotics for pain relief
• He had 7 diarrheal BMs the second day of admission and continued hydration
• Fevers had abated, and the patient felt better the third day of admission, but he developed bloody diarrhea and continued to have 7–8 minimal diarrheal BMs a day
Your plan at this time would be…
BM = bowel movement.
Treatment Considerations

26
Case 1—GI and Neurologic Toxicity: Infliximab
• Sigmoidoscopy showed diffuse ulcerations in the sigmoid/descending colon; the GI physician did not obtain biopsies
• The patient received infliximab at 5 mg/kg
• By day 4, 24 hours later, the patient had improved significantly, and the diarrhea had disappeared
• He was eating normally and was discharged 2 days later, ie, on the 6th day after admission, on a 100 mg oral prednisone taper
Case 1—GI and Neurologic Toxicity: Follow‐Up
• Patient was better when seen a week later, and then still felt well 2 weeks later
• He returned to work as a brewery manager 2 weeks after discharge
• His steroids finished in 40 days
• According to his wife, the patient seemed confused 2 weeks after finishing the steroids
• He was seen by the NP at the clinic and was felt to have a normal neurologic and psych exam
NP = nurse practitioner.

27
Case 1—GI and Neurologic Toxicity: Fever
• 2 days later, he developed a fever and contacted the on‐call physician; he was told to come to the hospital to be seen
• He had a fever to 39⁰C (102.2⁰F), and he seemed confused
• Neurologic exam showed short‐term memory loss and slight confusion, which he denied
Your next plan of action is…
Treatment Considerations

28
Case 1—GI and Neurologic Toxicity: Further Testing
• The patient was hydrated and treated with empiric antibiotics; there was no clear diagnosis
• MRI scan of the brain was completely within normal limits
• LP that night showed normal opening pressures, slightly decreased glucose, normal protein, and 80 lymphocytes/mm3; Gram stain was normal
• Viral and infectious CSF titers were all normal, and initial bacterial and viral cultures were negative
Your plan for this patient is…
LP = lumbar puncture; CSF = cerebrospinal fluid.
Treatment Considerations

29
Case 1—GI and Neurologic Toxicity: Consult
• Neurologic consult felt that this was likely limbic encephalopathy
• CSF cytologies were all negative
• The day of admission and for 2 days thereafter, the patient was oriented to self but not place or date and could not remember what he had done for a living before or the physician’s name
• He was started on IV solumedrol at 125 mg BID for 2 days; the next day he got a single dose of solumedrol at 125 mg
BID = twice daily.
Case 1—GI and Neurologic Toxicity: Final Follow‐Up
• The patient started to recognize the physician and recovered his short‐term memory 3 days after admission, but he admitted that he was still confused
• He was switched to 120 mg prednisone PO, tapering over 48 days; he was discharged home 4 days after admission, feeling well
• He returned to work 45 days after hospital discharge, feeling well but not quite at full energy
• On disease evaluation, he had an excellent response, which has been maintained 3 years from starting therapy
PO = by mouth (oral).

30
Case Study 2: Pulmonary Toxicity With Endocrinopathy
Case 2: Pulmonary Toxicity With Endocrinopathy: Presentation
• A 72‐year‐old man developed a growing non‐pigmented lesion on the chest wall; he was told by his PCP that it is an actinic keratosis
• The lesion continued to grow and was eventually biopsied by a dermatologist
• It is a 12 mm Clark’s V lesion with no ulceration but 20 mitoses/mm2
• After a wide local excision and a sentinel lymph node biopsy, a single left axillary node is found to be positive
• The patient elects to be treated with adjuvant nivolumab every 4 weeks at 480 mg intravenously
PCP = primary care physician/provider.

31
Case 2—Pulmonary Toxicity With Endocrinopathy: Symptomology
• After 8 months, the patient develops a chronic cough and is given an inhaler and antibiotics by his PCP, with minimal relief
• After several weeks of coughing, he comes to the oncologist for his regularly scheduled infusion and describes low‐grade fever and fatigue that has been going on for 2 weeks
• His labs are within normal limits, except for a slightly low lymphocyte count
Your plan of action would be to…
What would you do for this patient?

32
Case 2—Pulmonary Toxicity With Endocrinopathy: ED
• The patient is masked and is sent to the ED, where he has a nasal swab obtained for SARS‐CoV‐2
• In the ED, pulse oximetry shows 95%, and a chest X‐ray is obtained that shows questionable hazy left lower lobe infiltrate
• The chest and heart exams are normal
• The viral swab comes back negative 2 hours later
• Should he be sent back to the office that afternoon for therapy?
At this time, your plan is to…
Treatment Considerations

33
Case 2—Pulmonary Toxicity With Endocrinopathy: Testing in ED
• The oncologist speaks with the ED physician and requests a CT chest with contrast
• The CT shows diffuse pulmonary infiltrates in LLL, RUL, and RML of lungs without evidence of consolidation
• The patient is asked to ambulate with the pulse oximeter on, and his saturation drops to 91% with walking; he seems quite short of breath
• The ED doc orders T4, TSH, and ACTH after the scan is done
Your plan is to…
LLL = lower‐left lobe; RUL = right upper lobe; RML = right middle lobe (all of lung).
Treatment Considerations

34
Case 2—Pulmonary Toxicity With Endocrinopathy: Hospital Admission
• The patient is admitted and received solumedrol twice in 24 hours at 125 mg per dose
• Pulmonary consultant adds antibiotics and but does not feel that bronchoscopy is indicated
• COVID‐19 infection is felt to be low probability
• The patient rapidly improves on steroids; he is discharged 2 days later, breathing better on 120 mg prednisone, which will be tapered to 0 over 36 days
Case 2—Pulmonary Toxicity With Endocrinopathy: Follow‐Up
• When the patient returns to clinic a week later, the oncologist notices that the TSH taken in the ER was quite low and the T4 is borderline high.
• The ACTH is normal, and all other labs are within normal limits.
• On exam, the patient is breathing comfortably and has a normal chest exam, but he is tachycardic at 112 bpm.
• His coughing has diminished.
At this time, your plan for this patient is to…
bpm = beats per minute.

35
Treatment Considerations
Case 2—Pulmonary Toxicity With Endocrinopathy: Thyroid Dysfunction
• The patient had a chest X‐ray that was normal, with pulse oximetry that was 97% on room air, and changed to 96% with walking the halls
• Repeat TFTs show that the T4 is high and the TSH is quite low; the diagnosis is hyperthyroidism due to nivolumab
• After a phone consult with the endocrinologist, the oncologist rechecks the TFTs 2 weeks later and finds that the TSH is now elevated at 20, and the T4 and T3 are quite low; the diagnosis is rebound hypothyroidism due to nivolumab
• The patient notes profound fatigue

36
Case 2—Pulmonary Toxicity With Endocrinopathy: Final Follow‐Up
• The patient is placed on levothyroxine sodium (Synthroid®) replacement at 75 mcg daily, and he feels better within several days
• There is a repeat CT chest 4 weeks later that is essentially normal; TSH at that point is 6, and the levothyroxine sodium is increased to 100 mcg daily
• The patient is offered the opportunity to restart nivolumab adjuvant therapy but declines
• He will be scanned every 3 months for another year, then every 6 months for 3 years, with labs and an exam at each visit
Other Notes

37
Key Take‐Aways
• Immunotherapies can produce durable responses in patients with advanced melanoma
• Long‐term survival is now around 50% in patients with advanced melanoma who are treated with combination immunotherapy
• Anti‐tumor immune responses can be unconventional and may be delayed
• Adverse events are often highly manageable, especially if reported and addressed at the onset
• Grading symptoms → guides management
Thank you!
Questions and Answers

38
https://advancedmelanoma.posterprogram.com
Optimizing Treatment of Advanced Melanoma Poster Portal