Embed Size (px)
Citation preview

Risk factors and long-term consequences of proteinuria in renal transplantationJean-Michel Halimi, Tours, France
Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain
Prof. Jean-Michel HalimiHôpital Bretonneau
CHU de Toursservice de néphrologie-immunologie Clinique
Tours, France
slide 1
Thanks to the organisers for inviting me to the congress. Everybody thinks that we havenothing to know more about proteinuria because everybody knows proteinuria. I want toshow you that it's not true and we have new exciting findings about proteinuria in renaltransplantation.
slide 2

This is the Loire Valley and the Loire River, it's not the Bosphorus river as you can see.
slide 3
These are the points I want to cover during the next 20 or 25 minutes because I think wefinish at 3.30 and not at 3 o'clock.
slide 4

The first point is how should I measure proteinuria or albuminuria?
slide 5
It's quite simple but it's important to say again that proteinuria is a low cost parameter tomeasure and it's a biochemical method. It's Ok for routine use but more and more in centresall over the world we know that urinary albumin excretion is measured. We needimmunological methods, nephelometry, ELISA, RIA whatever. The cost is higher. It's ok forresearch, it's probably ok for routine use but in some centres they can use it on a daily basis.
slide 6

The second question we have to look at is where does early proteinuria come from?
slide 7
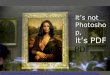
You have a patient who had proteinuria before transplantation and after transplantation, hestill has proteinuria. For has long does this proteinuria originate from the native kidneys?That's a big question. In a very elegant study, D'Cunha and co-workers looked at that. Hereon the y-axis, you have proteinuria and on the x-axis, you have the follow-up in weeks. Thatis proteinuria before transplantation and then, you have proteinuria at 1 week, 2 weeks 3weeks and so forth. What can you see is that after 3-4 weeks, the proteinuria that you hadyou no longer see it.
slide 8
So, after one month, most of the time, proteinuria comes from the graft, it does not come fromthe native kidneys. That's an important lesson.
slide 9
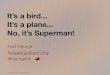
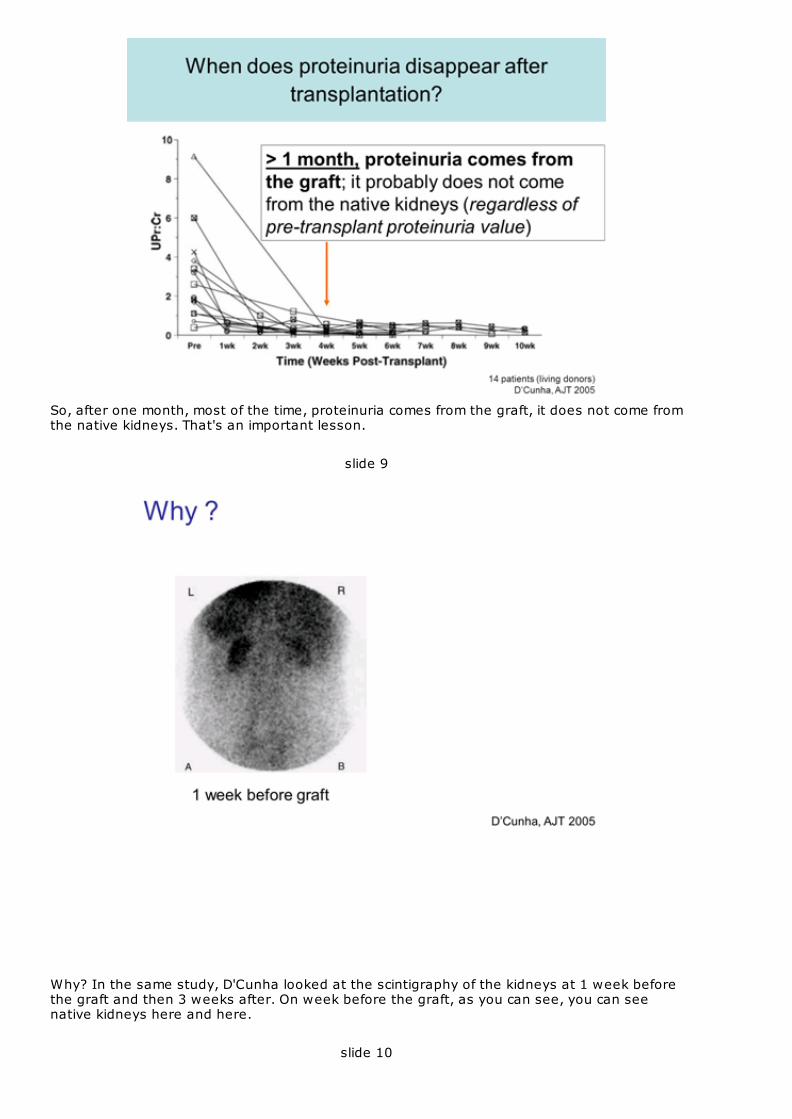
Why? In the same study, D'Cunha looked at the scintigraphy of the kidneys at 1 week beforethe graft and then 3 weeks after. On week before the graft, as you can see, you can seenative kidneys here and here.
slide 10
Then 3 weeks afterwards, after the transplantation, you don't see them. You see the newgraft but you don't see the native kidneys. So, native kidneys no longer function 3 weeksfollowing transplantation. So the proteinuria cannot originate from them.
slide 11

What does proteinuria tell us about the quality of the graft?
slide 12
When you look at the relationship between early proteinuria, early meaning 1 month to 3months after transplantation and parameters regarding donor cardiovascular events,ischemia-reperfusion injury lesions, you see that the risk of having proteinuria was muchgreater in patients who had received a kidney from an older donor and if he hadcardiovascular events before the graft, before the death it's also a risk factor. If the warmischemia time is warm, it's also a risk factor. So finally, early proteinuria is associated withdonor cardiovascular parameters and ischemia-reperfusion injury lesions. In another paper,we also proved that proteinuria and microalbuminuria are also associated with excessivesodium intake, history of acute rejection and smoking.
slide 13

Our patients have changed in the last 25 years, donors, recipients and some of us too.
slide 14
When you look at the prevalence of proteinuria at 3 months after transplantation duringthese different periods of time 1985-1989, 1990-1994 and then early 2000, the prevalence ofproteinuria the method is the same, the threshold is the same, the lab is the same, thecentre is the same. When you look at the prevalence, it's not the same. With time, more andmore you have proteinuria at 3 months where usually before a few years ago, 20-25 yearsago even more you didn't have proteinuria in these patients. So when we say extendedcriteria donors, it means something and it shows in the urine.
slide 15
What does proteinemia tell us about renal histology?
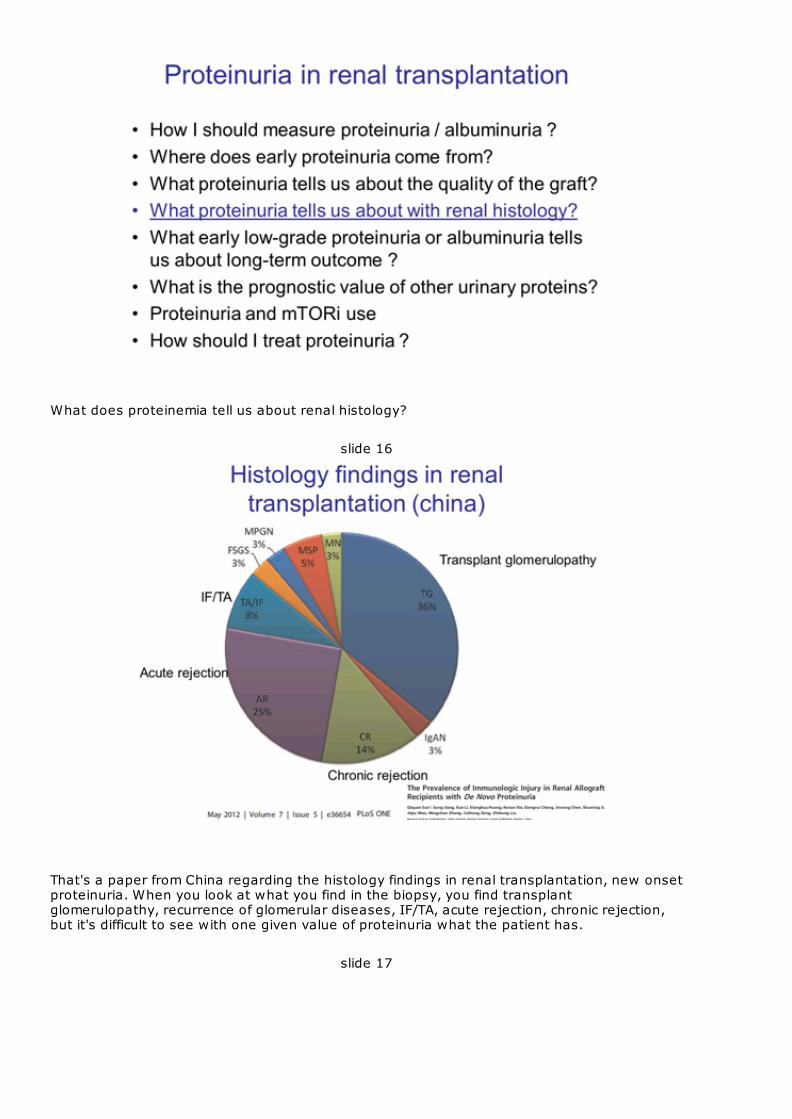
slide 16
That's a paper from China regarding the histology findings in renal transplantation, new onsetproteinuria. When you look at what you find in the biopsy, you find transplantglomerulopathy, recurrence of glomerular diseases, IF/TA, acute rejection, chronic rejection,but it's difficult to see with one given value of proteinuria what the patient has.
slide 17
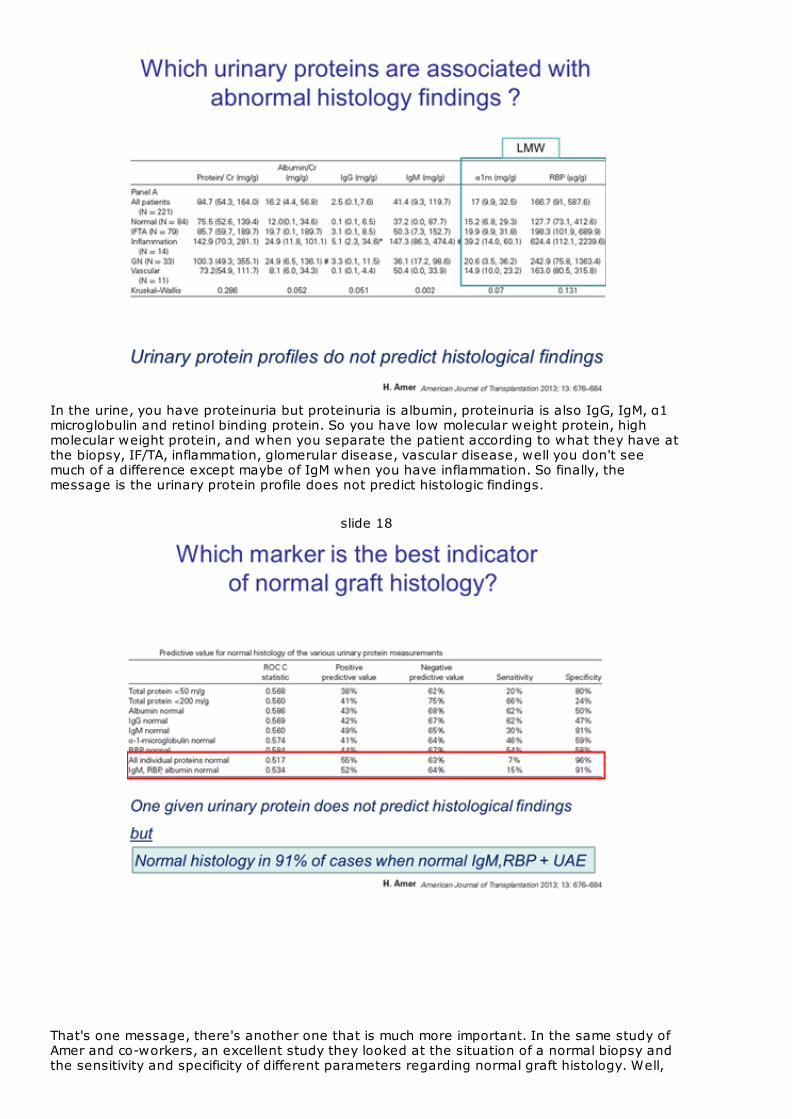
In the urine, you have proteinuria but proteinuria is albumin, proteinuria is also IgG, IgM, α1microglobulin and retinol binding protein. So you have low molecular weight protein, highmolecular weight protein, and when you separate the patient according to what they have atthe biopsy, IF/TA, inflammation, glomerular disease, vascular disease, well you don't seemuch of a difference except maybe of IgM when you have inflammation. So finally, themessage is the urinary protein profile does not predict histologic findings.
slide 18
That's one message, there's another one that is much more important. In the same study ofAmer and co-workers, an excellent study they looked at the situation of a normal biopsy andthe sensitivity and specificity of different parameters regarding normal graft histology. Well,
again when you look at the albumin, IgG, IgM, α1 microglobulin, RBP you don't see realsensitivity or specificity of these parameters. But when you look at together IgM, RBP andalbumin, if all of these 3 parameters are normal, the specificity is 91% meaning that normalhistology is found in 91% of cases when these parameters are normal. So maybe it is not thatimportant to do a biopsy in these patients.
slide 19
What does proteinuria tell us about long-term outcome regarding survival, graft survival,diabetes mellitus, GSA? We'll see that.
slide 20
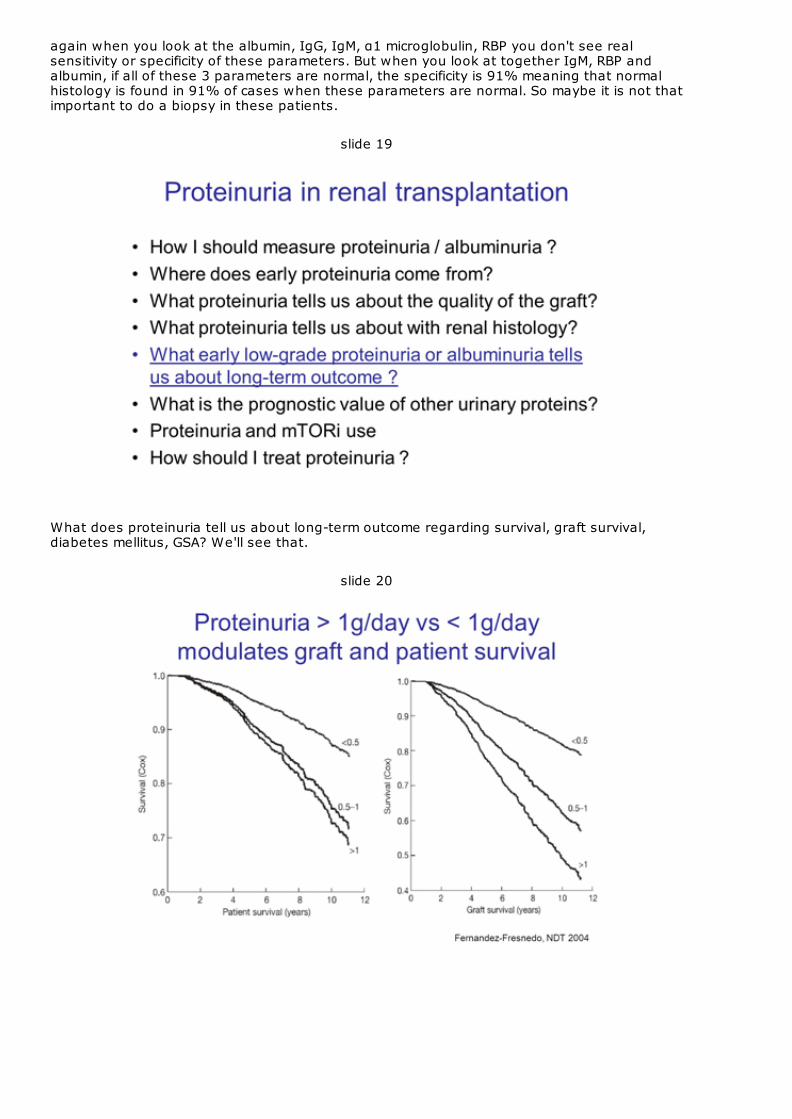
One of the first papers regarding this issue was the paper of Fernandez-Fresnedo, anexcellent paper looking at the relationship between proteinuria and graft and patient survival.It's easy to see that the more proteinuria you have, the worst prognosis you have for thepatient and for the graft.
slide 21
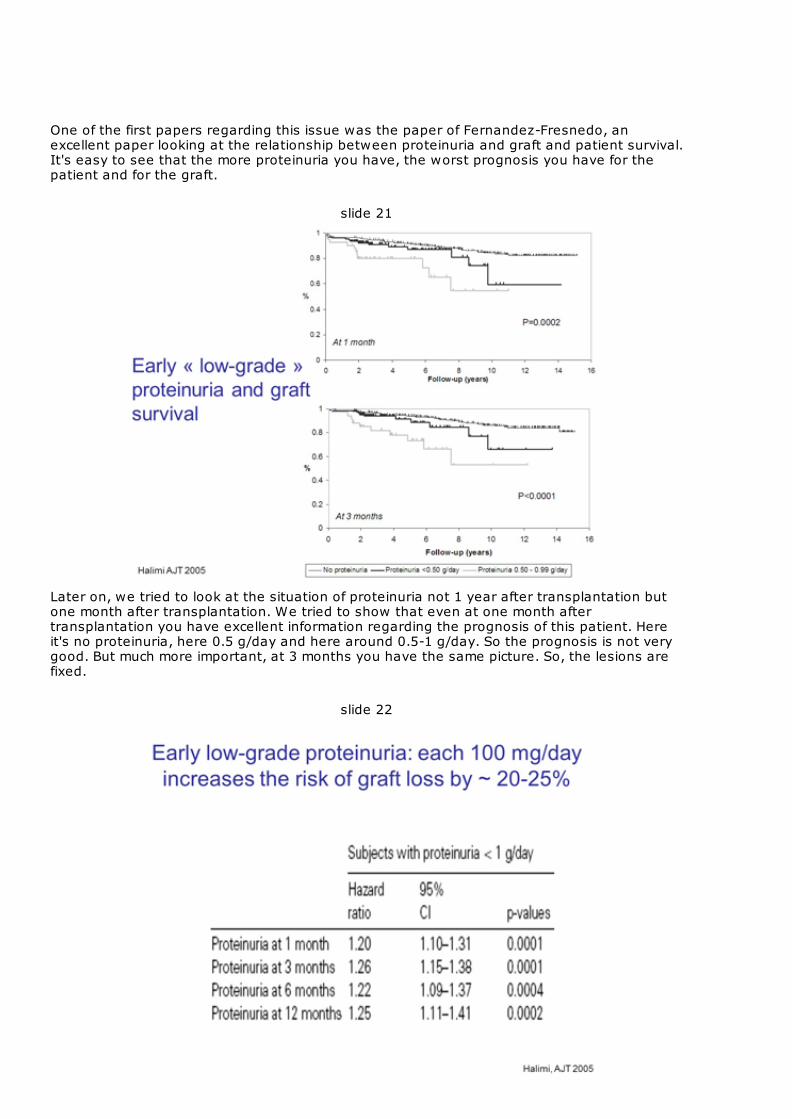
Later on, we tried to look at the situation of proteinuria not 1 year after transplantation butone month after transplantation. We tried to show that even at one month aftertransplantation you have excellent information regarding the prognosis of this patient. Hereit's no proteinuria, here 0.5 g/day and here around 0.5-1 g/day. So the prognosis is not verygood. But much more important, at 3 months you have the same picture. So, the lesions arefixed.
slide 22
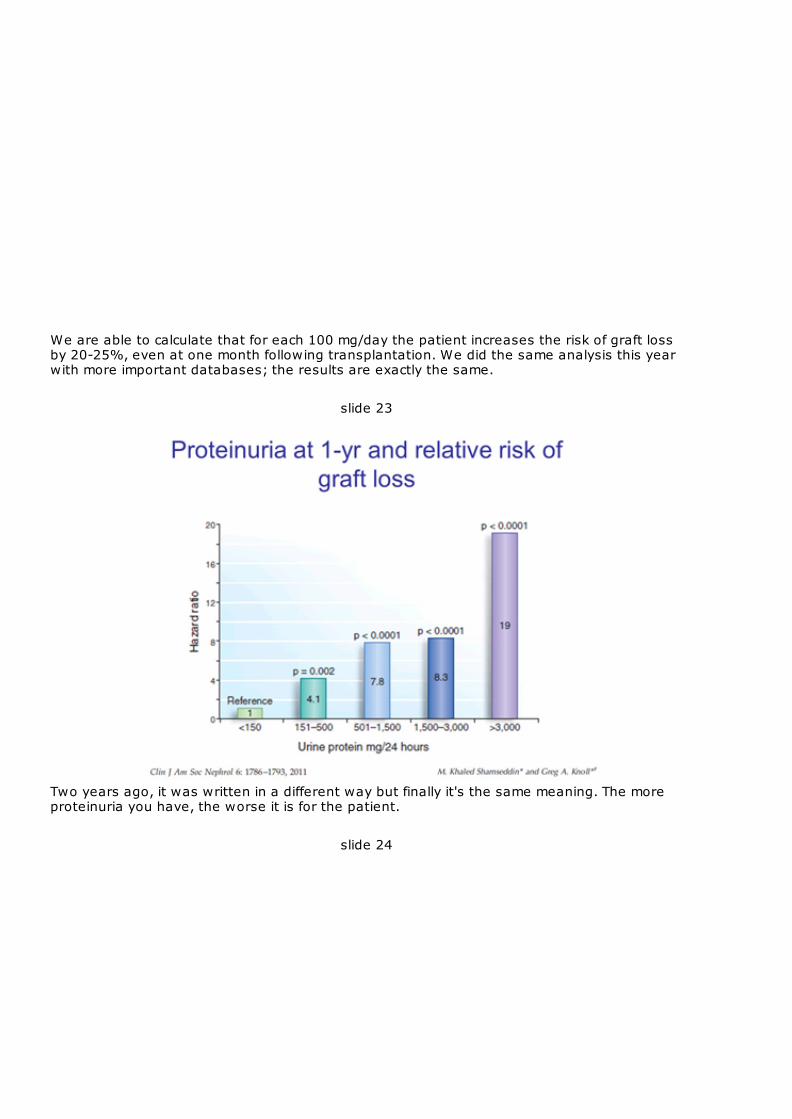
We are able to calculate that for each 100 mg/day the patient increases the risk of graft lossby 20-25%, even at one month following transplantation. We did the same analysis this yearwith more important databases; the results are exactly the same.
slide 23
Two years ago, it was written in a different way but finally it's the same meaning. The moreproteinuria you have, the worse it is for the patient.
slide 24
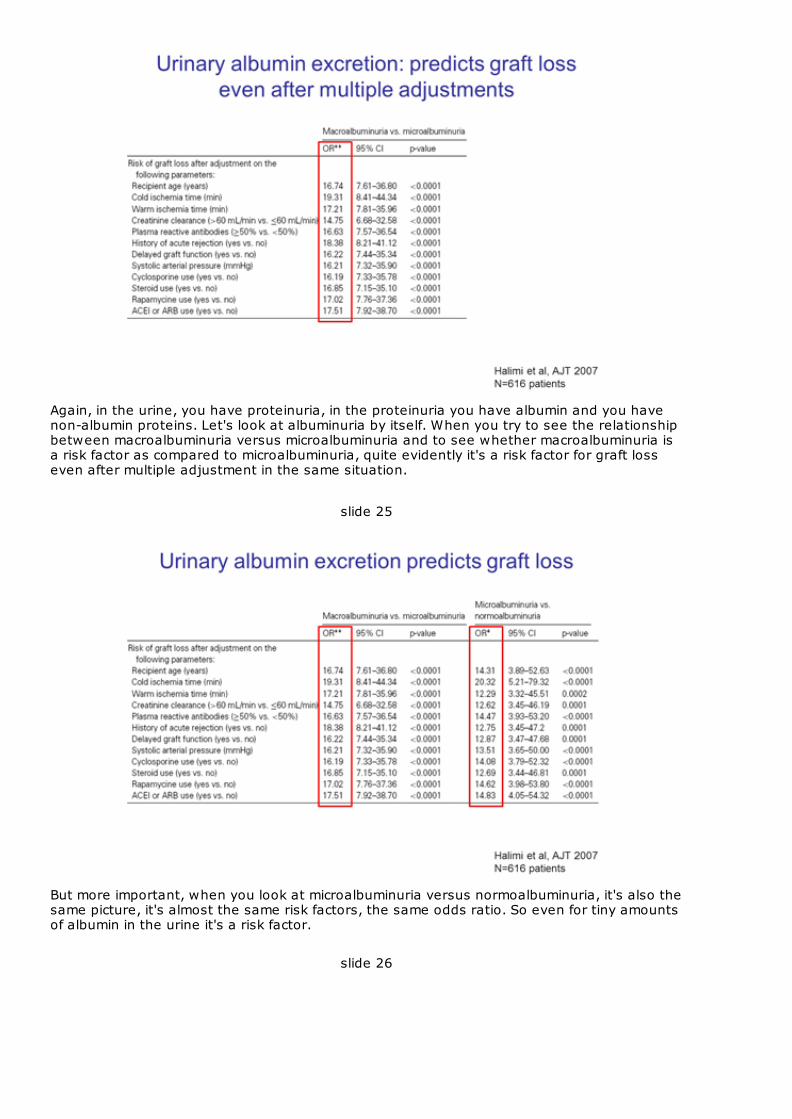
Again, in the urine, you have proteinuria, in the proteinuria you have albumin and you havenon-albumin proteins. Let's look at albuminuria by itself. When you try to see the relationshipbetween macroalbuminuria versus microalbuminuria and to see whether macroalbuminuria isa risk factor as compared to microalbuminuria, quite evidently it's a risk factor for graft losseven after multiple adjustment in the same situation.
slide 25
But more important, when you look at microalbuminuria versus normoalbuminuria, it's also thesame picture, it's almost the same risk factors, the same odds ratio. So even for tiny amountsof albumin in the urine it's a risk factor.
slide 26
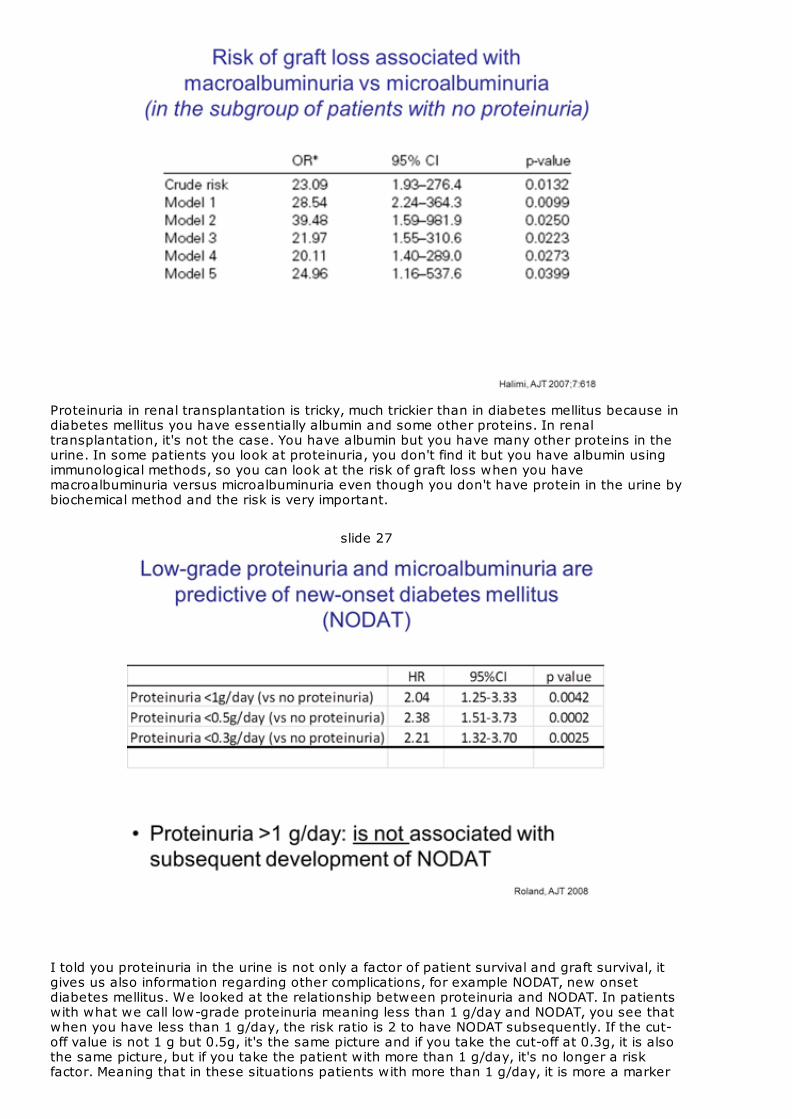
Proteinuria in renal transplantation is tricky, much trickier than in diabetes mellitus because indiabetes mellitus you have essentially albumin and some other proteins. In renaltransplantation, it's not the case. You have albumin but you have many other proteins in theurine. In some patients you look at proteinuria, you don't find it but you have albumin usingimmunological methods, so you can look at the risk of graft loss when you havemacroalbuminuria versus microalbuminuria even though you don't have protein in the urine bybiochemical method and the risk is very important.
slide 27
I told you proteinuria in the urine is not only a factor of patient survival and graft survival, itgives us also information regarding other complications, for example NODAT, new onsetdiabetes mellitus. We looked at the relationship between proteinuria and NODAT. In patientswith what we call low-grade proteinuria meaning less than 1 g/day and NODAT, you see thatwhen you have less than 1 g/day, the risk ratio is 2 to have NODAT subsequently. If the cut-off value is not 1 g but 0.5g, it's the same picture and if you take the cut-off at 0.3g, it is alsothe same picture, but if you take the patient with more than 1 g/day, it's no longer a riskfactor. Meaning that in these situations patients with more than 1 g/day, it is more a marker
of renal disease obviously but in patients with low-grade proteinuria and microalbuminuria,it's more a marker of endothelial dysfunction.
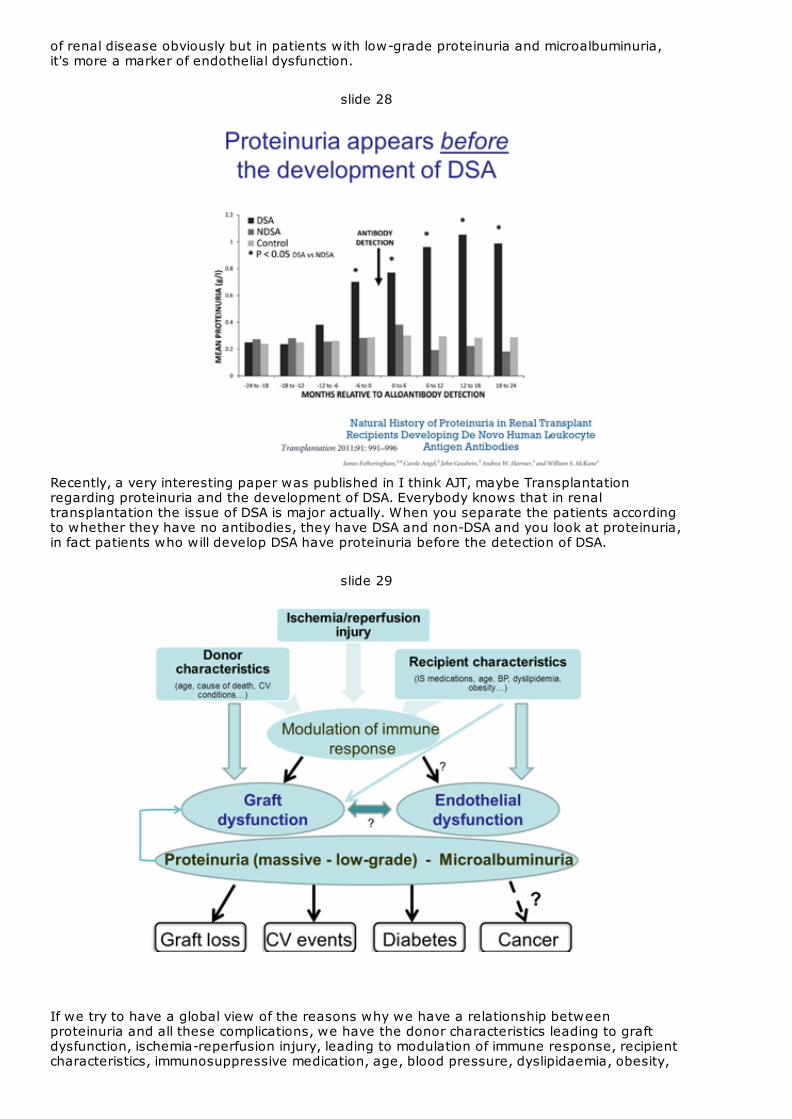
slide 28
Recently, a very interesting paper was published in I think AJT, maybe Transplantationregarding proteinuria and the development of DSA. Everybody knows that in renaltransplantation the issue of DSA is major actually. When you separate the patients accordingto whether they have no antibodies, they have DSA and non-DSA and you look at proteinuria,in fact patients who will develop DSA have proteinuria before the detection of DSA.
slide 29
If we try to have a global view of the reasons why we have a relationship betweenproteinuria and all these complications, we have the donor characteristics leading to graftdysfunction, ischemia-reperfusion injury, leading to modulation of immune response, recipientcharacteristics, immunosuppressive medication, age, blood pressure, dyslipidaemia, obesity,
leading to endothelial dysfunction. I don't know exactly how it works between the two but afew papers now look at this relationship. In the end, as a marker, you have microalbuminuriaalmost nothing in the urine, low-grade proteinuria or massive proteinuria leading to graftdysfunction and these parameters indicate a higher risk of diabetes mellitus, cardiovascularevents, graft loss and maybe we have a paper regarding this issue cancer but it was notproven by the studies.
slide 30
But you have albumin.
slide 31
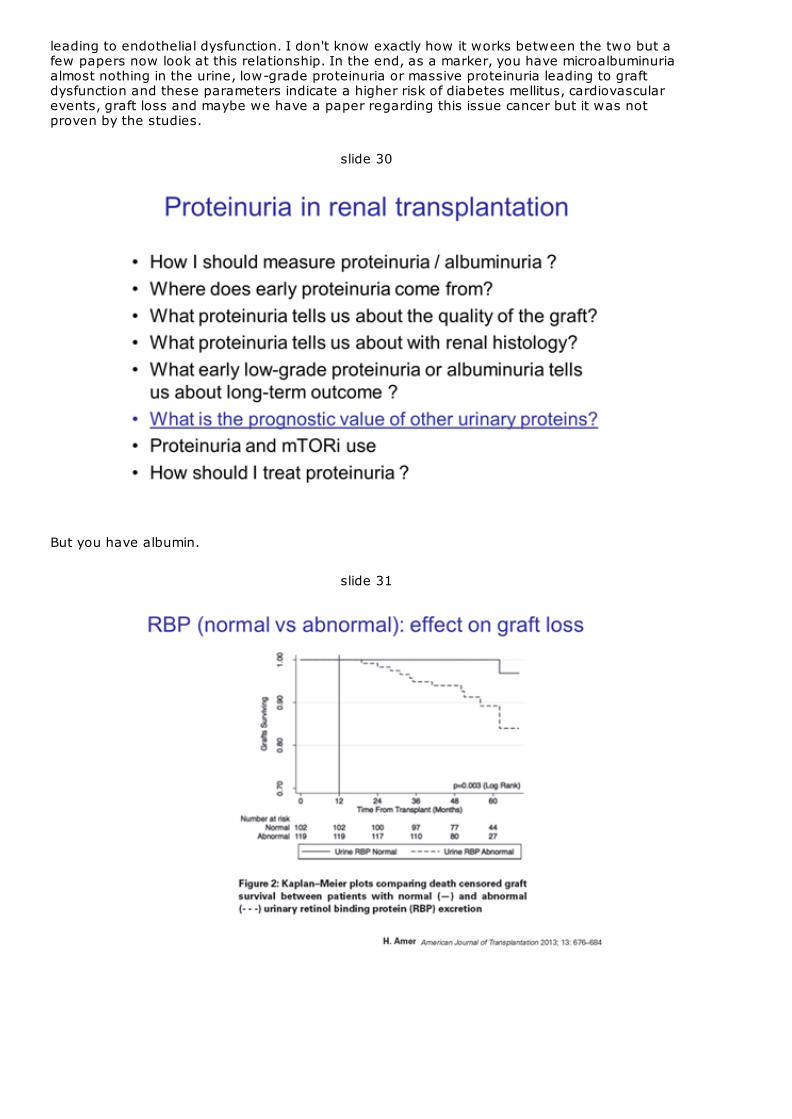
I told you have also other proteins in the urine. What about these other proteins? Are theyimportant regarding the prognosis of this patient and the graft survival of the patient? Yes,they are. For example, RBP. When RBP is abnormal at 1 year the survival is much less in thispatient.
slide 32
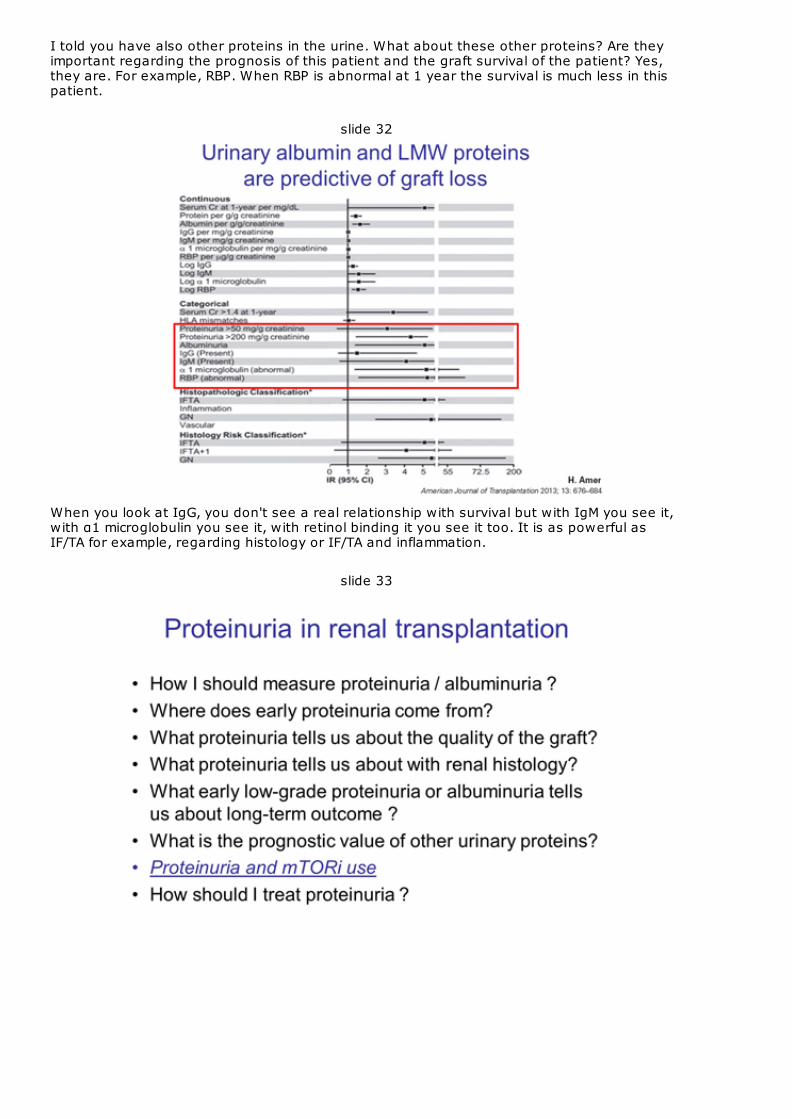
When you look at IgG, you don't see a real relationship with survival but with IgM you see it,with α1 microglobulin you see it, with retinol binding it you see it too. It is as powerful asIF/TA for example, regarding histology or IF/TA and inflammation.
slide 33
There was a big issue a few years ago regarding the relationship between proteinuria andmTOR inhibitor use. Everybody knows that in some patients suing mTOR inhibitors you mayhave proteinuria.
slide 34
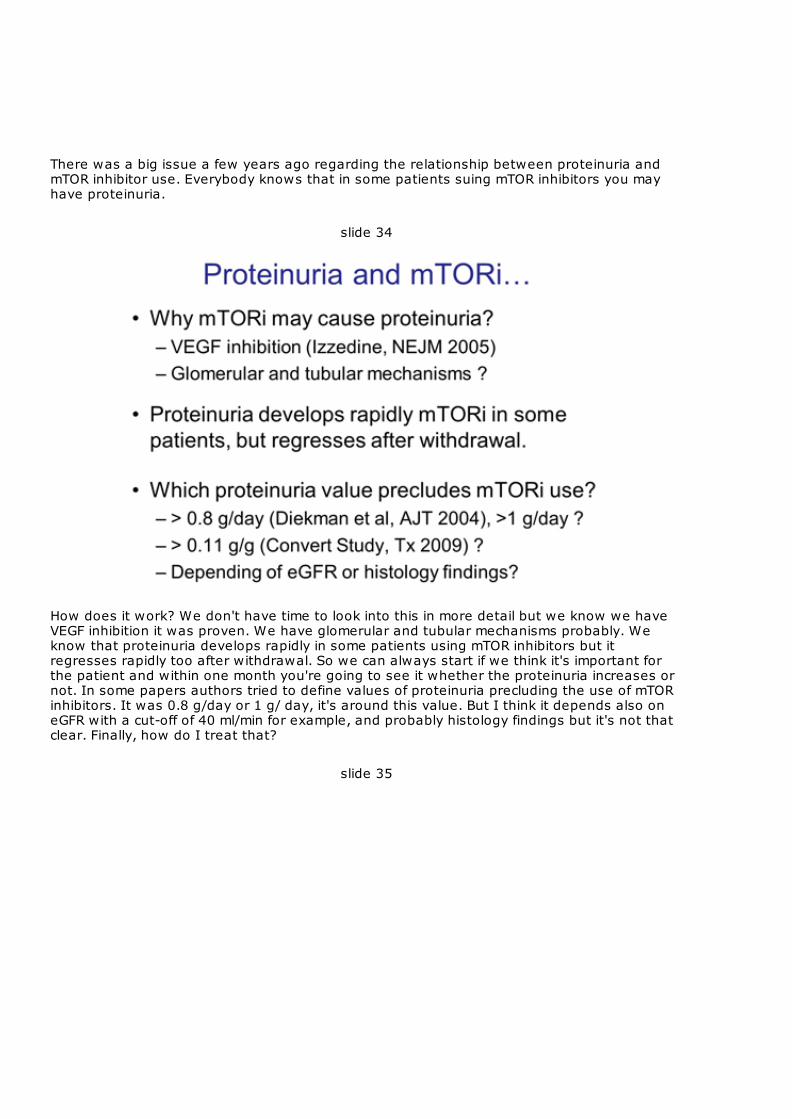
How does it work? We don't have time to look into this in more detail but we know we haveVEGF inhibition it was proven. We have glomerular and tubular mechanisms probably. Weknow that proteinuria develops rapidly in some patients using mTOR inhibitors but itregresses rapidly too after withdrawal. So we can always start if we think it's important forthe patient and within one month you're going to see it whether the proteinuria increases ornot. In some papers authors tried to define values of proteinuria precluding the use of mTORinhibitors. It was 0.8 g/day or 1 g/ day, it's around this value. But I think it depends also oneGFR with a cut-off of 40 ml/min for example, and probably histology findings but it's not thatclear. Finally, how do I treat that?
slide 35
How do I treat at proteinuria?
slide 36
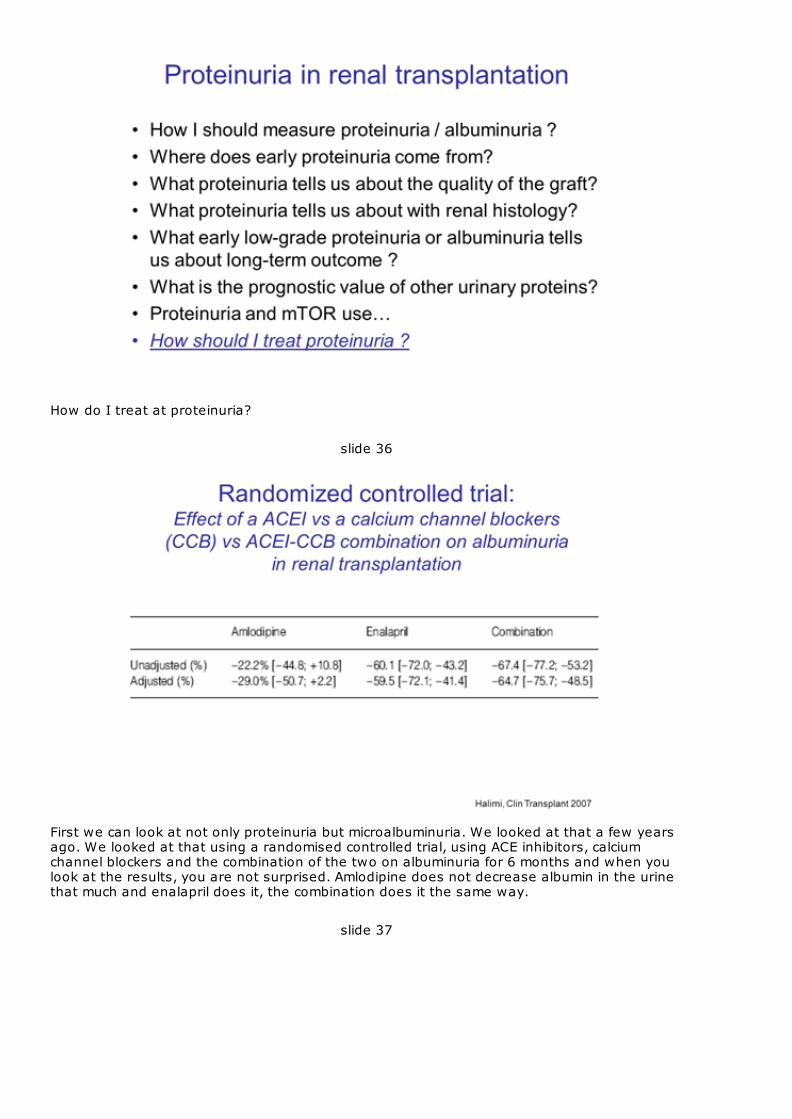
First we can look at not only proteinuria but microalbuminuria. We looked at that a few yearsago. We looked at that using a randomised controlled trial, using ACE inhibitors, calciumchannel blockers and the combination of the two on albuminuria for 6 months and when youlook at the results, you are not surprised. Amlodipine does not decrease albumin in the urinethat much and enalapril does it, the combination does it the same way.
slide 37

I'm not going to dwell a lot on the use of RAS blockers in patients with proteinuria. I know it'sgoing to be treated in a few minutes but in my mind for patients with microalbuminuria or low-grade proteinuria, RAS blockers probably reduce the value of proteinuria and albuminuria butdoes it do anything good about the renal function? I'm not sure about that. It's differentprobably in patients with massive proteinuria.
slide 38
Finally, we have the last two slides. The take home messages. First of all, for routine use wecan sue proteinuria, we can use albuminuria, it's ok, it's good to do that and to do itfrequently in our patients. For research we need more than that, we need RBP, we needproteomics, we need metabolomics, if you can afford that. I can't at this time. The thirdmessage, important message I think for the practice, after 1 month following transplantationproteinuria originates from the graft not the native kidneys. So persistent or new onsetproteinuria requires biopsy. Early proteinuria provides information regarding the quality of thegraft. So the quality of the organ we've done the work on for many years it providesinformation regarding ischemia-reperfusion injury, donor age, cardiovascular history and soforth. Proteinuria levels are higher in patients who will subsequently develop DSA ascompared to those who will not.

slide 39
When RBP, IgM, and albumin are normal, 91% of the time the histology will be absolutelynormal. So maybe in these patients we won't need to do a biopsy, which remains anaggressive performance. Proteinuria is a strong predictor of graft loss. Everybody knows that.Probably albuminuria, the low molecular weight proteins are also a predictor of cardiovascularevents, it's also a predictor of death. Interestingly microalbuminuria and low-gradeproteinuria predicts the development of NODAT because they are markers of endothelialdysfunction.
Regarding mTOR inhibitors and proteinuria it’s safe to use them when proteinuria is less than1 g/day most of the time but if proteinuria develops and you want to stop it, well we knowthat proteinuria will regress it after withdrawal so it’s not a big issue finally. For the therapeutic options, we’ll look at the presentation of Armando Torres. I think formassive proteinuria blood pressure reduction, use of RAS blockers are important. For theother situations low-grade proteinuria, microalbuminuria I use them but I don’t know. Thankyou.