Embed Size (px)
Citation preview

Fracture strength and fracture patterns of root filled teethrestored with direct resin restorations
N.A. Taha a,b,*, J.E. Palamara a, H.H. Messer a
aMelbourne Dental School, University of Melbourne, Melbourne, AustraliabDepartment of Conservative Dentistry, Jordan University of Science and Technology, Conservative Dentistry Department, PO Box 3864,
Irbid 21110, Jordan
1,2
j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5
a r t i c l e i n f o
Article history:
Received 19 February 2011
Received in revised form
10 May 2011
Accepted 11 May 2011
Keywords:
Root filled teeth
Resin composites
Fracture strength
Fracture pattern
a b s t r a c t
Objective: To compare fracture characteristics of root-filled teeth with variable cavity design
and resin composite restoration.
Methods: 80 extracted intact maxillary premolars were divided randomly into eight groups;
(1) intact teeth; (2) unrestored MOD cavity; (3) unrestored MOD cavity plus endodontic access
through the occlusal floor; (4) unrestored MOD plus endodontic access with axial walls
removed; (5) MOD restored with resin composite; (6) MOD plus endodontic access, resin
composite; (7) MOD plus extensive endodontic access, resin composite; (8) MOD plus
extensive endodontic access, GIC core and resin composite. A ramped oblique load was
applied to the buccal cusp in a servohydraulic testing machine. Fracture load and fracture
patterns were recorded. Fracture loads were compared statistically using 1-way ANOVA,
with Dunnett test for multiple comparisons.
Results: Unrestored teeth became progressively weaker with more extensive preparations.
Endodontic access confined within the occlusal floor did not significantly affect strength
compared to an MOD cavity. Loss of axial walls weakened teeth considerably [292 + 80 N vs
747 + 130 N for intact teeth]. Restoration increased the strength of prepared teeth particu-
larly in teeth without axial walls. Teeth with a GIC core were not significantly weaker than
intact teeth [560 + 167 N]. Failures were mostly adhesive at the buccal interface, with the
fracture propagating from the buccal line angle of the occlusal floor (MOD and MOD plus
access groups) or of the proximal box (axial wall removed).
Conclusions: Direct restorations increased fracture resistance of root filled teeth with exten-
sive endodontic access. Both restored and unrestored teeth showed similar fracture patterns.
# 2011 Elsevier Ltd. All rights reserved.
avai lab le at www . s c ien c edi r ect . co m
journal homepage: www.intl.elsevierhealth.com/journals/jden
1. Introduction
Direct tooth-coloured restorations are often used for root-
filled teeth as a relatively low cost, aesthetic alternative to
cuspal coverage restorations. Historically, both amalgam and
resin composite restorations have been widely used even for
* Corresponding author at: Department of Conservative Dentistry, JordDepartment, PO Box 3864, Irbid 21110, Jordan. Tel.: +962 776566110; fa
E-mail addresses: [email protected], [email protected] (N
0300-5712/$ – see front matter # 2011 Elsevier Ltd. All rights reserveddoi:10.1016/j.jdent.2011.05.003
posterior teeth, with composite resin direct restorations
showing good long term outcomes. More recent studies3,4
have indicated less favourable but still reasonably high
survival of teeth with direct restorations, and the prospective
studies of Mannocci et al.5,6 indicate good outcomes with both
amalgam and resin composite restorations (plus a prefabri-
cated post) over the medium term (3 years). Clearly the choice
an University of Science and Technology, Conservative Dentistryx: +962 2 7258907.
.A. Taha).
.

j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5528
of restoration will depend on remaining tooth structure, with
direct restorations limited to teeth with substantial coronal
dentine. In addition to aesthetic considerations, an acceptable
restoration must restore function and preserve the remaining
tooth structure against fracture.
Root-filled teeth are at increased risk of fracture. Caries and
excessive removal of dentine during root canal treatment,
rather than low moisture content and increased brittleness7,8
reduce tooth strength. Endodontic procedures reduce tooth
strength modestly compared to extensive cavity prepara-
tions,9 but only as long as the endodontic access is confined to
the occlusal floor of the cavity. Loss of axial dentine walls,
which is common in teeth requiring root filling, greatly
weakens teeth.8
Resin composite restorations have the advantage of
bonding to tooth structure, which might strengthen the tooth
and offer an alternative restorative technique to cuspal
coverage. However, polymerization shrinkage is a serious
drawback of these materials, resulting in cuspal strains with
subsequent stress or disruption of the bond, microleakage and
recurrent caries. Attempts at minimizing this problem have
included the use of low shrink composites,10 incremental
placement11 and the use of liners including glass ionomer,
flowable composites and polyacid-modified resin compo-
sites.12–14 The performance of direct resin composites for
the restoration of root filled teeth has been investigated
experimentally ever since posterior resin composite materials
were first introduced15–17 and clinically in both retrospective
and prospective clinical studies. Despite the less favourable
outcomes in comparison with cuspal coverage restorations
reported in retrospective studies,3,4 two randomised clinical
trials found superior performance compared to amalgam
restorations in terms of fracture resistance, but with a
problem of recurrent caries. Similar survival to full coronal
coverage was observed over a three year period.5,6
In experimental studies, fracture resistance to static
loading has been used as a measure of the effect of cavity
preparation and/or restoration on tooth strength. Although
the fracture load is typically much higher than functional
occlusal loads, it is still a valid method for comparing
restorative materials and different cavity designs.
Adhesive resin composite restorations have been reported
to increase the fracture resistance of root filled teeth
compared to non adhesive fillings.18–22 Fibre reinforced resin
composite has also been studied as a conservative restoration,
but was not found to improve the fracture strength compared
to conventional resin composite.23 Different bonding sys-
tems18 and base materials including glass ionomer cement
(GIC) and composites24 have also been investigated for their
effect on fracture strength.
This experimental study was conducted to compare the
fracture resistance of extracted root filled maxillary premolars
with variable cavity design and direct restoration techniques
using resin composite. In a previous study,25 preserving the
proximal dentine walls of an endodontic access cavity and
placement of a glass ionomer base beneath the resin
composite restoration of root filled maxillary premolars
significantly reduced cuspal deflection and microleakage but
did not affect the strains within cusps. The null hypothesis of
this study is that preserving the proximal dentine and
placement of a GIC base will improve the fracture strength
and result in a more favourable fracture pattern of root filled
maxillary premolars restored with direct resin composites.
2. Materials and methods
Overview: Three different cavity preparations were tested:
MOD, MOD plus endodontic access confined to the occlusal
floor of the MOD cavity, and MOD plus extensive endodontic
access with the axial walls removed between the proximal
boxes and access preparation (Fig. 1). Teeth were then restored
with direct resin composite material, plus an additional group
in which a GIC core was placed in teeth with the extensive
endodontic access before placing resin composite. All teeth
were then subjected to an oblique load of 458 to the vertical on
the buccal cusp until fracture.
Tooth selection and mounting: Eighty intact, non carious
maxillary premolars were used in this study. Teeth of similar
size were selected by measuring the buccolingual width in
millimetres using a digital calliper and allowing a maximum
deviation of 10% from the determined mean.25 The teeth were
then randomly assigned into eight groups (n = 10). The project
was approved by the Ethics in Human Research Committee of
the University of Melbourne. Teeth were stored in 1%
chloramine T solution in distilled water (pH = 7.8) (Sigma–
Aldrich Co., St. Louis, MO, USA) for two weeks. Teeth were
mounted vertically in dental stone within nylon mounting
rings.9,25,26 Dental stone covered the roots to within 2 mm of
the cementoenamel junction (CEJ), to approximate the support
of alveolar bone in a healthy tooth.
Cavity preparations: The teeth were prepared as follows.
Group 1: Intact teeth (control).
Group 2: A standardized MOD cavity was prepared using a
tungsten carbide round-ended fissure bur (Komet H21R,
Brasseler, Lemgo, Germany) in a high speed handpiece with
water coolant so that the bucco-lingual width of the occlusal
isthmus was one third of the width between buccal and lingual
cusp tips, and the buccolingual width of the proximal box was
one third of the bucco-lingual width of the crown. The gingival
floor of the box was 1 mm coronal to the cementoenamel
junction; occlusal depth was 3.0 mm and the total depth 5–
6 mm (Fig. 1). The cavosurface margins were prepared at 908
and all internal angles were rounded. Consistency in cavity
preparation was ensured by parallel preparation of the facial
and palatal walls of the cavity.
Group 3: An MOD cavity was prepared similarly to group 2,
then an endodontic access cavity confined within the occlusal
floor was cut leaving the proximal dentine walls intact. Root
canals were prepared using the ProTaper rotary nickel–
titanium system (Dentsply, Maillefer, Ballaigues, Switzerland)
and filled by cold lateral condensation using gutta percha and
AH Plus root canal sealer (Dentsply, Maillefer Detrey,
Konstanz, Germany). Gutta percha was removed to 2 mm
below the CEJ. Excess sealer was removed with a cotton pellet
moistened with alcohol.
Group 4: Teeth were prepared similarly to group 3, but the
endodontic access included the removal of all dentine
between the proximal box and the pulp chamber. Root canals
were prepared and obturated similarly to group 3.

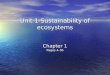
Fig. 1 – Diagram of cavity preparations and direction of fractures in the prepared unrestored teeth. The basic preparation was
an MOD cavity with the following dimensions: occlusal depth of 3 mm, isthmus width of 1/3 inter-cuspal distance, and
proximally to 1 mm above the CEJ. The endodontic access was either confined to the floor of the pulp chamber with axial
walls (orange) intact or with the walls removed. (For interpretation of the references to colour in this figure legend, the
reader is referred to the web version of the article.)
Fig. 2 – Experimental setup of a tooth in the testing
machine, with a round-ended steel cylinder of 1.3 mm
radius applied to the palatal incline of the buccal cusp at
an angle of 458 to the vertical.
j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5 529
Restoration:
Group 5 (MOD cavity): The entire cavity preparation was
etched with 37% phosphoric acid (Super Etch, SDI Limited,
Bayswater, Australia; batch no. 030648) for 20 s, rinsed with
air–water spray for 10 s and dried for 20 s. A bonding agent
(AdperTM Single Bond, 3 M ESPE, St Paul, USA, lot no. 184141)
was applied and light cured for 20 s, and the cavity was
incrementally restored with OD3 shade resin composite
(Glacier, SDI Limited, Australia, batch no. 050489). Three
increments were placed and cured using a LED light curing
source (Bluephase C8, CE Ivoclar, Vivadent AG, F1-9494
Schaan, Liechtenstien) at an intensity of 800 mW/cm2 for 40 s.
Group 6 (MOD plus endodontic access): The cavity was
restored with resin composite, as in group 5. The first
increment was packed into the canal orifices and covered
the proximal boxes to the level of the occlusal floor. The last
two increments covered the entire mesiodistal and buccolin-
gual width of the cavity.
Group 7 (MOD plus extensive endodontic access, resin
composite restoration): A similar restoration to group 6 was
placed. The first increment was packed into canal orifices and
both proximal boxes to a depth of approximately 1 mm.
Group 8 (MOD plus extensive endodontic access, GIC core
and resin composite): Prior to restoration with composite a
10% polyacrylic acid dentine conditioner was applied for 10 s
and a glass ionomer base (Fuji VII, lot # 0609270. GC
Corporation, Tokyo, Japan) was placed above the gutta-percha
to reproduce the floor of an MOD cavity. The teeth were then
restored with resin composite as above.
After restoration teeth were stored in an incubator at 378 C
in 100% humidity for 24 h before testing.
Teeth were subjected to a 45 degree oblique compressive
load applied to the palatal incline of the buccal cusp, at a
crosshead speed of 0.5 mm/min in a servohydraulic material

Fig. 3 – Box plot of the effect of cavity preparation on
fracture strength of unrestored teeth.
0
100
200
300
400
500
600
700
800
900
Intac
tMOD
Acces
s
No axia
l+Com
posit
e
No axia
l+Line
r
Group
Frac
ture
Loa
d (N
ewto
ns)
RestoredUnrestored
Fig. 4 – Stacked bar graph of the effect of restoration on
fracture strength of the prepared teeth. The lower part of
each bar is the mean fracture load for unrestored cavity
preparations, whilst the upper bar is the mean load
following restoration. Standard error bars apply to the
mean for restored teeth.
j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5530
test system (MTS model 801, MTS Corporation, Minneapolis,
USA) using a round-ended steel cylinder of 1.3 mm radius
(Fig. 2). The force required to fracture the tooth was recorded in
Newtons.
Data analysis: Data were analysed using one way ANOVA
followed by the Dunnett T3 test for multiple comparisons, at
the 5% significance level.
Fracture patterns were evaluated under a stereomicro-
scope and categorized according to location, the restoration–
tooth interface where fracture occurred, the point of initiation
of the fracture and the severity of the fracture. Mode of failure
(adhesive, cohesive, mixed) was assessed using standard
criteria20,27 at a magnification of 20�. Representative samples
were also gold sputtered for studying the fracture surface
under the scanning electron microscope (SEM) at magnifica-
tion of 200�.
3. Results
3.1. Unrestored teeth
Intact teeth fractured at a load of 747 � 130 N (Fig. 3). Teeth
became progressively weaker with more extensive cavity
preparations. MOD cavity preparation reduced fracture
strength by 37.5% (467 � 141 N, p = 0.001 compared with intact
teeth). Endodontic access confined within the occlusal floor
did not further reduce strength compared to an MOD cavity
(442 � 132 N, p = 0.99 compared with MOD). Removal of axial
walls further weakened teeth considerably (mean load at
fracture 292 � 80 N, only 39.1% of intact teeth).
3.2. Restored teeth
Restoration increased the strength of prepared teeth, but
the increase was significant only in preparations involving
loss of axial walls (Fig. 4). Following restoration, teeth with
an MOD cavity (541 � 186 N) and teeth without axial walls
and restored with a GIC core (560 � 167 N) were not
significantly weaker than intact teeth (747 � 130 N). Teeth
restored with resin composite only were weaker than intact
teeth (451 � 206 N, p = 0.028 when axial walls were present;
449 � 102, p = 0.001 when axial walls were not present).
3.3. Fracture patterns
Intact teeth fractured consistently within the buccal cusp
(Table 1 and Fig. 5). Most fractures (7/10) were above the CEJ,
whilst 3/10 were below the CEJ, with only one subcrestal.
Unrestored teeth with cavity preparations demonstrated
consistent patterns of fracture of the buccal cusp, extending
subcrestally. In the MOD and MOD plus endodontic access
groups, the crack initiated at the buccal line angle of the
occlusal floor (Fig. 5), except for one tooth in the latter group
where the crack initiated in the mid-floor region. In teeth with
the axial walls removed, the fracture initiated at the buccal
proximal line angle. All cracks propagated obliquely to the
buccal root surface.
Restored teeth also failed in consistent patterns within
each group. Other than 2/10 fractures within the buccal cusp in
the MOD group, failure was predominantly adhesive between
restorative material and tooth structure, when observed at the
light microscopic level and confirmed with SEM of represen-
tative samples (Fig. 6). Debonding of the restoration was
predominantly at the buccal interface with the cavity wall
(Fig. 7), with at most 2/10 teeth per group debonding at the
palatal interface. As in the unrestored teeth, the crack initiated
at the buccal line angle of the cavity preparation, either at the
occlusal floor (MOD and MOD plus access groups) or at the floor
of the proximal box (teeth with the axial wall removed). The
fractures extended obliquely to the buccal surface and were
mostly subcrestal except in the restored MOD group where 3/
10 were supracrestal.

Table 1 – Fracture patterns for unrestored and restored teeth.
Group/procedure Level Pattern Margin
Supracrestal Subcrestal Within cusp From line angle Other Buccal Palatal
Group 1: intact teeth 9 1 10 – 0 – –
Unrestored cavity preparations
Group 2: MOD cavity 0 10 0 10 0 – –
Group 3: MOD + endo access 0 10 0 9 1 – –
Group 4: MOD, no axial walls 0 10 0 10 0 – –
Restored teeth
Group 5: MOD, composite 3 7 2 8 0 10 0
Group 6: access + composite 0 10 0 9 1 8 2
Group 7: no axial walls, composite 0 10 0 10 0 8 2
Group 8: no axial walls, GIC liner 1 9 1 9 0 7 2
Margin: the cavity margin (either buccal or palatal) at which debonding between the restoration and tooth structure occurred (see Fig. 7).
From line angle: fracture propagated from either the buccal–occlusal or the buccal–proximal line angle, obliquely towards the buccal root
surface (see Fig. 7). ‘‘Other’’ indicates a more complex fracture pattern.
Fig. 5 – Side view of fracture patterns of intact and unrestored teeth. (A) Intact tooth, fracture within buccal cusp; (B) MOD
cavity, subcrestal fracture beginning from buccal line angle of the occlusal floor; (C) MOD plus endodontic access, same
pattern as B; (D) axial walls removed, subcrestal fracture initiated at buccal proximal line angle.
j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5 531

Fig. 6 – A scanning electron microscope view of the fracture
surface at 200T magnification, showing predominantly
adhesive failure at the interface with dentine with some
areas of localized cohesive failure within enamel.
Fig. 7 – Front and side view of fracture patterns of restored teeth
of the line of fracture. Failures were predominantly adhesive at
line angle at the occlusal floor (MOD plus access groups) (A–C) or
removed (D–F).
j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5532
4. Discussion
Methods: Despite its limitations, fracture testing remains a
common experimental method of evaluating restorative
procedures for root filled teeth. Reeh et al. highlighted the
shortcomings of destructive methods of testing, which
include the non-physiologic loads required to cause frac-
ture, the variation amongst teeth used in experimental
studies, and differences in test conditions leading to
fracture.17 Differences in tooth morphology (such as the
difference in cross-sectional shape of the cervical area
between first and second premolars) may also influence
fracture susceptibility and patterns. However, highly con-
sistent fracture patterns were observed in this study despite
the inclusion of both first and second premolars. The
direction and location of the applied load and the shape
of the loading tip may all influence results, and the results
should be extrapolated to clinical patterns of failure with
some degree of caution.
Before proceeding with testing of the eight experimental
groups, additional groups were prepared and tested for the
effect of periodontal ligament simulation and thermal cycling
on fracture strength. Fracture load was unaffected by either
thermal cycling or the presence of a simulated periodontal
ligament as has also been previously reported,28,29 and
therefore neither was included in the main study. The
with a schematic illustration of the initiation and extension
the buccal interface. The crack propagated from the buccal
at the floor of the proximal box for teeth with the axial wall

j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5 533
embedding material should ideally simulate the capacity of
bone to absorb masticatory load and therefore withstand the
load applied in mechanical testing. However there is no
consensus on the material that should be used and it varies
greatly amongst studies: acrylic resin19,22,30 or polystyrene
resin20,27 and die stone.21,31
In the present study, an oblique load (458 to the long axis of
the tooth) was applied to the occlusal incline of the buccal cusp
using a rounded loading tip, which contacted the enamel
surface away from the restoration margin. This pattern of
loading was intended to simulate normal working side
occlusal contacts. In previous studies, the direction of the
applied load has included axial loading on both buccal and
palatal cusps16,17,32 or at 308 to the vertical on the buccal cusp
incline,27 or at the tooth-restoration interface.15,18,22
Cavity preparations: Since the early work of Vale,33 numer-
ous authors have documented the weakening effect of cavity
preparations on tooth strength and fracture resistance,
although relatively few have investigated the effect of
endodontic procedures. Reeh et al. using non-destructive
strain measurements, reported that endodontic access had
little effect (5%) on cuspal stiffness compared with an MOD
cavity preparation (63% reduction relative to intact teeth).9 In
that study, however, endodontic access was confined to the
occlusal floor of the cavity preparation. In contrast, cuspal
stiffness was markedly reduced when endodontic access
included removal of the axial walls of dentine adjacent to each
proximal box.26 In this study, endodontic access confined to
the occlusal floor also had minimal impact on fracture
resistance (3%) but loss of axial walls reduced fracture strength
by more than 60% relative to intact teeth. These results are
very similar to other fracture studies16,32 despite differences in
cavity preparations and in the type and location of loading.
Extensive cavity preparation and endodontic access clearly
cause a major reduction in fracture resistance, regardless of
how it is measured.
Hood proposed a cantilever beam hypothesis to explain
loss of fracture resistance. According to this hypothesis, cusps
of teeth with MOD cavity preparations function as a cantilever
beam, with the extent of deflection under load influenced by
both beam thickness and length (to the third power).34 Hence a
deeper, wider cavity will result in substantially greater cusp
deflection for a given load, with the cavity floor serving as the
fulcrum for bending. The buccal–occlusal line angle thus
becomes the site of fracture initiation. When the endodontic
access is confined within the occlusal cavity floor, the fracture
occurs at a much higher point (the occlusal floor) than when
the axial walls are removed (buccal proximal line angle). This
concept has been previously confirmed in molars26 and is
clearly illustrated in this study (Fig. 4) showing the deeper
location of fracture initiation with loss of the axial walls of the
proximal box.
Based on the remaining cusp thickness after the MOD
preparation it was not judged necessary to place an intracanal
post. Several studies have found a reinforcing effect of
placement of fibre or titanium posts in addition to direct
resin composite restorations, without negatively affecting the
fracture pattern.19,35,36 A retrospective clinical study reported
a survival rate of root filled teeth restored with either a
prefabricated post or a cast post to be 83% over a 10 year
period.37 On the other hand placement of a fibre post with or
without cusp capping with resin composite did not result in
additional benefit compared to composite resin restoration
without post and cusp capping.38 One study27 found that glass
fibre posts reduced fracture resistance of root filled teeth with
moderate tooth structure loss and did not restore the fracture
resistance of teeth with major loss of tooth structure.
Restorations: Restoration with resin composite generally
increased fracture strength relative to the unrestored teeth,
though not always to a statistically significant level. Two of the
four restored groups were not significantly weaker than intact
teeth. As in many similar studies, the variation within groups
was large, making it difficult to achieve statistical significance.
Most previous studies have similarly demonstrated a
strengthening effect of resin composite restorations com-
pared to unrestored teeth with similar cavity prepara-
tions,16,17,32,39 but achieving comparable strength to intact
teeth has been more variable. Soares et al.20 found that none of
the restorative techniques employed recovered strength to
levels of sound nonrestored teeth, and MOD cavities restored
with resin composite placed with direct technique (similar to
our study) were stronger than those restored with laboratory
processed resin and indirect technique. This was attributed to
more conservative cavity preparation with the direct tech-
nique.
Several dentine bonding systems have been developed to
improve the bond strength of composite resin to tooth
structure. Generally dentine bonding systems are reported
to increase fracture resistance.18,22 Siso et al.19 found a total
etch two step adhesive more effective in increasing the
fracture strength than a one step adhesive which is similar to
findings by others.21,22 The use of two step adhesive systems
(as used in this study) is still a common practice amongst
clinicians and in experimental studies.19,20,38
The use of glass ionomer under resin composite restora-
tions has been recommended to improve marginal adapta-
tion.25,40 Despite the lower mechanical properties compared to
resin composites, placement of a glass ionomer liner in this
study did not negatively affect the fracture strength. Similar to
findings of other studies16,18 it improved fracture strength of
the restored teeth to levels not significantly different from the
intact tooth. This could be related to the ability of glass
ionomer to bond to dentine and act as absorber for strains
encountered during polymerization shrinkage and mastica-
tion by virtue of its intrinsic porosity.41,42 It should be noted,
however, that the standard deviation for this group was large,
and fracture strength was not significantly greater than in the
group restored with resin composite alone.
The patterns of fracture of restored teeth were very
consistent in this study, closely following the patterns for
unrestored teeth with similar cavity preparations. Failure
typically occurred by debonding at the buccal interface, with
cuspal fracture extending obliquely from the buccal line angle
of the floor of the cavity preparation (Fig. 5). Depending on the
extent of the endodontic access, the fracture occurred from
the occlusal floor of the MOD preparation or more deeply from
the buccal proximal line angle. The similarity in fracture
patterns between unrestored and restored teeth suggests that
failure occurs in two stages: firstly, debonding occurs at the
buccal interface between the restoration and cavity wall.

j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5534
Following debonding, the buccal cusp behaves as a cantilever
beam as in the unrestored tooth, and fractures in the same
manner.
Fracture patterns have varied widely in experimental
studies, which can be attributed only in part to loading
conditions. With vertical loading applied equally to cuspal
inclines of both buccal and palatal cusps,9,20,32 fracture was
predominantly vertically through the restoration and the
middle of the proximal box, extending into the root. This
pattern occurred in teeth with direct bonded restorations, but
marginal failure with cuspal fracture was also seen,20 Despite
similar loading conditions, others have reported that fracture
always occurred at the restoration–tooth interface and never
within the restorative material itself.16,21 Oblique loading
typically involves adhesive failure at the tooth–restoration
interface (15,16,18, this study). On the other hand loading
crowned teeth was reported to cause cohesive failure within
the veneer with fracture initiating at the contact area
regardless of the loaded cusp.43
Clinical implications: Preservation of all remaining sound
coronal dentine should be a primary objective in prevention of
fractures of root filled teeth. A conservative endodontic access
which preserves the axial dentine is recommended whenever
possible, but is often precluded by the extent of previous caries
and restorations.
In terms of fracture resistance, resin composite restora-
tion provides some strengthening effect, but based on
previous experimental and retrospective clinical studies
does not provide the same degree of long term protection as
cusp coverage restorations.2,44 Perhaps direct restoration
should be considered a valid interim restoration for root
filled teeth before cuspal coverage can be provided. However
teeth should be continuously monitored for the risk of
recurrent caries.6,45
5. Conclusion
Endodontic access with loss of axial walls weakened teeth by
60% compared to intact teeth. Direct resin composite restora-
tion significantly increased fracture resistance of these teeth,
with a GIC core resulting in fracture strength similar to that of
intact teeth.
Acknowledgment
We would like to thank Mr. Geoff Adams from Melbourne
Dental School, University of Melbourne for his assistance in
the statistical analysis.
r e f e r e n c e s
1. Hansen EK, Asmussen E. In vivo fractures of endodonticallytreated posterior teeth restored with enamel-bonded resin.Endodontic Dental Traumatology 1990;6:218–25.
2. Hansen EK, Asmussen E, Christiansen NC. In vivo fractures ofendodontically treated posterior teeth restored withamalgam. Endodontic Dental Traumatology 1990;6:49–55.
3. Aquilino SA, Caplan DJ. Relationship between crownplacement and the survival of endodontically treated teeth.Journal of Prosthetic Dentistry 2002;87:256–63.
4. Salehrabi R, Rotstein I. Endodontic treatment outcomes in alarge patient population in the USA: an epidemiologicalstudy. Journal of Endodontics 2004;30:846–50.
5. Mannocci F, Bertelli E, Sherriff M, Watson TF, Ford TR. Three-year clinical comparison of survival of endodontically treatedteeth restored with either full cast coverage or with directcomposite restoration. Journal of Prosthetic Dentistry2002;88:297–301.
6. Mannocci F, Qualtrough AJ, Worthington HV, Watson TF, PittFord TR. Randomized clinical comparison of endodonticallytreated teeth restored with amalgam or with fiber posts andresin composite: five-year results. Operative Dentistry2005;30:9–15.
7. Papa J, Cain C, Messer HH. Moisture content of vital vsendodontically treated teeth. Endodontic Dental Traumatology1994;10:91–3.
8. Sedgley CM, Messer HH. Are endodontically treated teethmore brittle? Journal of Endodontics 1992;18:332–5.
9. Reeh ES, Messer HH, Douglas WH. Reduction in toothstiffness as a result of endodontic and restorativeprocedures. Journal of Endodontics 1989;15:512–6.
10. Palin WM, Fleming GJ, Nathwani H, Burke FJ, Randall RC. Invitro cuspal deflection and microleakage of maxillarypremolars restored with novel low-shrink dentalcomposites. Dental Materials 2005;21:324–35.
11. Visvanathan A, Ilie N, Hickel R, Kunzelmann KH. Theinfluence of curing times and light curing methods on thepolymerization shrinkage stress of a shrinkage-optimizedcomposite with hybrid-type prepolymer fillers. DentalMaterials 2007;23:777–84.
12. van Dijken JW. Durability of resin composite restorations inhigh C-factor cavities: a 12-year follow-up. Journal ofDentistry 2010;38:469–74.
13. Alomari QD, Reinhardt JW, Boyer DB. Effect of liners on cuspdeflection and gap formation in composite restorations.Operative Dentistry 2001;26:406–11.
14. Cho E, Chikawa H, Kishikawa R, Inai N, Otsuki M, FoxtonRM, et al. Influence of elasticity on gap formation in a liningtechnique with flowable composite. Dental Material Journal2006;25:538–44.
15. Trope M, Langer I, Maltz D, Tronstad L. Resistance tofracture of restored endodontically treated premolars.Endodontic Dental Traumatology 1986;2:35–8.
16. Wendt Jr SL, Harris BM, Hunt TE. Resistance to cusp fracturein endodontically treated teeth. Dental Materials 1987;3:232–5.
17. Reeh ES, Douglas WH, Messer HH. Stiffness ofendodontically-treated teeth related to restorationtechnique. Journal of Dental Research 1989;68:1540–4.
18. Hernandez R, Bader S, Boston D, Trope M. Resistance tofracture of endodontically treated premolars restored withnew generation dentine bonding systems. InternationalEndodontic Journal 1994;27:281–4.
19. Siso SH, Hurmuzlu F, Turgut M, Altundasar E, Serper A, Er K.Fracture resistance of the buccal cusps of root filledmaxillary premolar teeth restored with various techniques.International Endodontic Journal 2007;40:161–8.
20. Soares PV, Santos-Filho PC, Martins LR, Soares CJ. Influenceof restorative technique on the biomechanical behavior ofendodontically treated maxillary premolars. Part I: Fractureresistance and fracture mode. Journal of Prosthetic Dentistry2008;99:30–7.
21. Ausiello P, De Gee AJ, Rengo S, Davidson CL. Fractureresistance of endodontically-treated premolars adhesivelyrestored. American Journal of Dentistry 1997;10:237–41.

j o u r n a l o f d e n t i s t r y 3 9 ( 2 0 1 1 ) 5 2 7 – 5 3 5 535
22. Hurmuzlu F, Serper A, Siso SH, Er K. In vitro fractureresistance of root-filled teeth using new-generation dentinebonding adhesives. International Endodontic Journal2003;36:770–3.
23. Sengun A, Cobankara FK, Orucoglu H. Effect of a newrestoration technique on fracture resistance ofendodontically treated teeth. Dental Traumatology2008;24:214–9.
24. Hofmann N, Just N, Haller B, Hugo B, Klaiber B. The effect ofglass ionomer cement or composite resin bases onrestoration of cuspal stiffness of endodontically treatedpremolars in vitro. Clinical Oral Investigations 1998;2:77–83.
25. Taha NA, Palamara JE, Messer HH. Cuspal deflection, strainand microleakage of endodontically treated premolar teethrestored with direct resin composites. Journal of Dentistry2009;37:724–30.
26. Panitvisai P, Messer HH. Cuspal deflection in molars inrelation to endodontic and restorative procedures. Journal ofEndodontics 1995;21:57–61.
27. Soares CJ, Soares PV, de Freitas Santos-Filho PC, Castro CG,Magalhaes D, Versluis A. The influence of cavity design andglass fiber posts on biomechanical behavior ofendodontically treated premolars. Journal of Endodontics2008;34:1015–9.
28. Stewardson DA, Shortall AC, Marquis PM. The effect ofclinically relevant thermocycling on the flexural propertiesof endodontic post materials. Journal of Dentistry;38:437–42.
29. Soares CJ, Pizi EC, Fonseca RB, Martins LR. Influence of rootembedment material and periodontal ligament simulationon fracture resistance tests. Brazilian Oral Research2005;19:11–6.
30. Plotino G, Buono L, Grande NM, Lamorgese V, Somma F.Fracture resistance of endodontically treated molarsrestored with extensive composite resin restorations.Journal of Prosthetic Dentistry 2008;99:225–32.
31. Al-Wahadni A, Gutteridge DL. An in vitro investigation intothe effects of retained coronal dentine on the strength of atooth restored with a cemented post and partial corerestoration. International Endodontic Journal 2002;35:913–8.
32. Soares PV, Santos-Filho PCF, Queiroz EC, Araujo TC, CamposRE, Araujo CA, et al. Fracture resistance and stressdistribution in endodontically treated maxillary premolarsrestored with composite resin. Journal of Prosthodontics2008;17:114–9.
33. Vale WA. Cavity preparation. Irish Dental Review 1956;2:33–41.
34. Hood J. Biomechanics of the intact, prepared and restoredtooth: some clinical implications. International Dental Journal1991;41:25–32.
35. Nothdurft FP, Seidel E, Gebhart F, Naumann M, Motter PJ,Pospiech PR. The fracture behavior of premolar teeth withclass II cavities restored by both direct compositerestorations and endodontic post systems. Journal ofDentistry 2008;36:444–9.
36. Sorrentino R, Salameh Z, Zarone F, Tay FR, Ferrari M. Effectof post-retained composite restoration of MOD preparationson the fracture resistance of endodontically treated teeth.Journal of Adhesive Dentistry 2007;9:49–56.
37. Gomez-Polo M, Llido B, Rivero A, Del Rio J, Celemin A. A 10-year retrospective study of the survival rate of teethrestored with metal prefabricated posts versus cast metalposts and cores. Journal of Dentistry 2010;38:916–20.
38. Mohammadi N, Kahnamoii MA, Yeganeh PK, Navimipour EJ.Effect of fiber post and cusp coverage on fracture resistanceof endodontically treated maxillary premolars directlyrestored with composite resin. Journal of Endodontics2009;35:1428–32.
39. Daneshkazemi A. Resistance of bonded compositerestorations to fracture of endodontically treated teeth.Journal of Contemporary Dental Practice 2004;5:51–8.
40. Krejei I, Lutz F, Krejei D. The influence of different basematerials on marginal adaptation and wear of conventionalclass II composite resin restorations. QuintessenceInternational 1988;19:191–8.
41. Davidson CL. Glass-ionomer bases under posteriorcomposites. Journal of Esthetic Dentistry 1994;6:223–4.
42. van Dijken JW, Kieri C, Carlen M. Longevity of extensiveclass II open-sandwich restorations with a resin-modifiedglass-ionomer cement. Journal of Dental Research1999;78:1319–25.
43. Bonfante EA, Sailer I, Silva NR, Thompson VP, Dianne RekowE, Coelho PG. Failure modes of Y-TZP crowns at differentcusp inclines. Journal of Dentistry 2010;38:707–12.
44. Sorensen JA, Martinoff JT. Intracoronal reinforcement andcoronal coverage: a study of endodontically treated teeth.Journal of Prosthetic Dentistry 1984;51:780–4.
45. Alves dos Santos MP, Luiz RR, Maia LC. Randomised trial ofresin-based restorations in Class I and Class II beveledpreparations in primary molars: 48-month results. Journal ofDentistry 2010;38:451–9.