Embed Size (px)
Citation preview

Prof. Javier García Fernández MD, Ph.D, MBA.Chairman of Anesthesia & Perioperative Medicine Department
Puerta de Hierro Universitary HospitalProf. of Anaesthesia and Perioperative Medicine. AutonomaMedical School. UAM
Madrid‐Spain

CV and Conflict of interest
• Chairman of Anaesthesia, Critical Care and Pain
Department. Puerta de Hierro Univ. Hospital. Madrid
• Ph.D. UCM. Madrid
• MBA. UCM. Madrid
• Expertise: Pediatric Anaesthesia and critical care, mechanical
ventilation.
SCIENTIFIC ACTIVITY• Patents: 1• Oral presentations: 85• Lectures: 152• Book Editor: 3 ; Book Chapters: 33• Director of Ph.D.: 3• Grants and Prizes: 12• Director of training course s: 14• Journal associated editor : 4• Journals Referee: 4• Indexed publications (Medline): 55; F.I. 45,99
• I have received research grants from:
Maquet, GE, Dräger, Spacelab, Masimo,
Covidine, Abbot and Baxter
• I have been invited to form part of the
advisory board of several of those
companies but I prefer to keep
independent and open to what new
technologies are offering to us
• I don´t have any conflict of interest for
this lecture but ..I don´t want you to go
sleep so I am going to provoke you…

© Drägerwerk AG & Co. KGaA, 2019 •3
Visitado - 52/195🇩🇪 Alemania, 🇸🇦 Arabia Saudita, 🇦🇷 Argentina, 🇦🇹 Austria, 🇧🇴 Bolivia, 🇧🇬 Bulgaria, 🇨🇦 Canadá, 🇨🇱Chile, 🇨🇳 China, 🇨🇾 Chipre, 🇨🇴 Colombia, 🇨🇷 Costa Rica, 🇭🇷 Croacia, 🇨🇺 Cuba, 🇪🇨 Ecuador, 🇪🇬Egipto, 🇪🇸 España, 🇺🇸 Estados Unidos, 🇵🇭 Filipinas, 🇫🇮 Finlandia, 🇫🇷 Francia, 🇬🇷 Grecia, 🇭🇺Hungría, 🇮🇩 Indonesia, 🇮🇷 Irán, 🇮🇪 Irlanda, 🇮🇱 Israel, 🇮🇹 Italia, 🇯🇵 Japón, 🇲🇰 Macedonia del Norte, 🇲🇦 Marruecos, 🇲🇽 México, 🇳🇴 Noruega, 🇳🇱 Países Bajos, 🇵🇪 Perú, 🇵🇱 Polonia, 🇵🇹 Portugal, 🇬🇧Reino Unido, 🇷🇴 Rumania, 🇷🇺 Rusia, 🇷🇸 Serbia, 🇸🇬 Singapur, 🇿🇦 Sudáfrica, 🇸🇪 Suecia, 🇨🇭 Suiza, 🇹🇭 Tailandia, 🇹🇷 Turquía, 🇺🇦 Ucrania, 🇺🇾 Uruguay, 🇻🇳 Vietnam

Agenda
• Introduction and a little revision of lung physiology (which is one thing that RCTs cannot destroy…)
• Why it is important to perform Intra‐operative Lung Protective Ventilation (i‐LPV)
• Describe and understand the mechanisms of “Intra‐operative VILI” (Ventilator Induced Lung Injury) ?
• How we can improve our delivery of Mechanical Ventilation and feel more confident ..
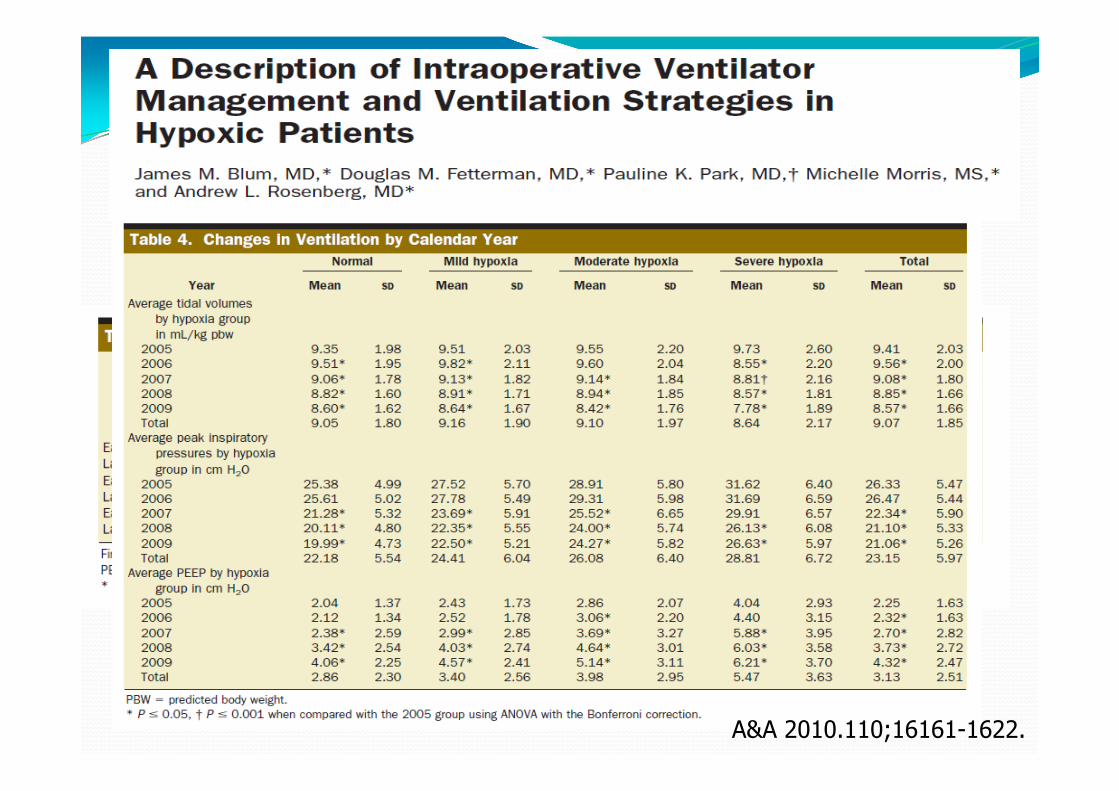
University of Michigan Medical Center, review of all operations performed between 2005‐ 2009, using a general anesthetic which at least 1 arterial blood gas determination was made.
83,866 ABGs were obtained in 27,101 patients
Excluding cardiac and thoracic procedures
Four cohorts of arterial blood gases were identified with P/F > 300, P/F= 300‐201, P/F = 200‐101, P/F < 100.
Positive end‐expiratory pressure (PEEP), peak inspiratory pressures (PIPs), FIO2, oxygen saturation (SaO2), and tidal volume in mL/kg PBW were compared
A&A 2010.110;16161-1622.
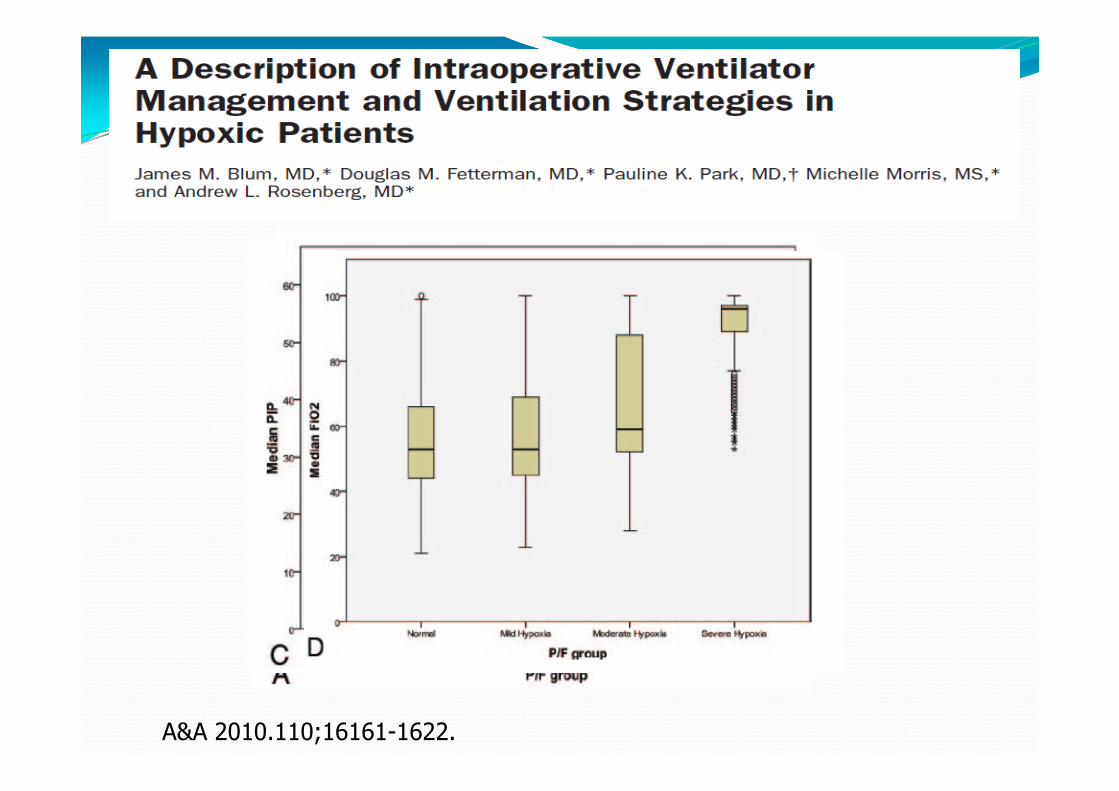
A&A 2010.110;16161-1622.
A&A 2010.110;16161-1622.
Conclusions Similar ventilation strategies in mL/kg PBW and PEEP were used among patients regardless of P/F ratio
The results of this study suggest that anesthesiologists, in general, are treating hypoxemia with higher FIO2 and letting increase the PIP, but never use low Vt, high levels of PEEP and recruitment maneuvers as in intensive care units are starting to do for improving oxygenation
A&A 2010.110;16161-1622.
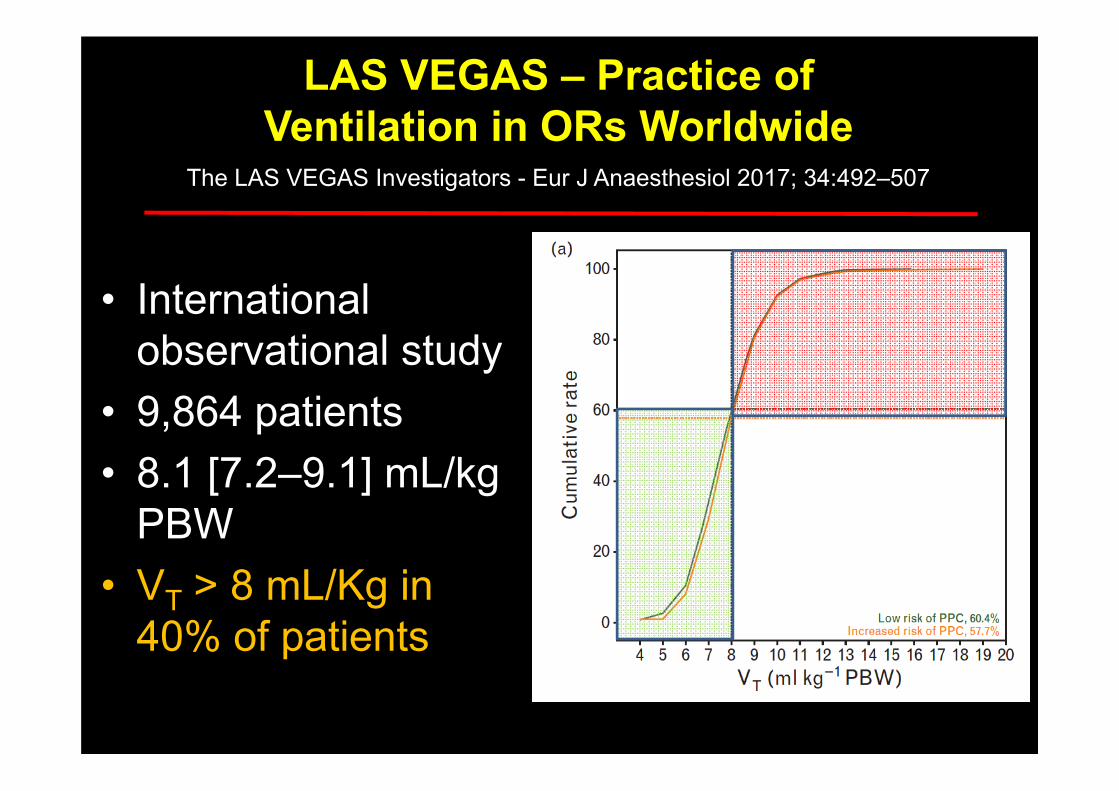
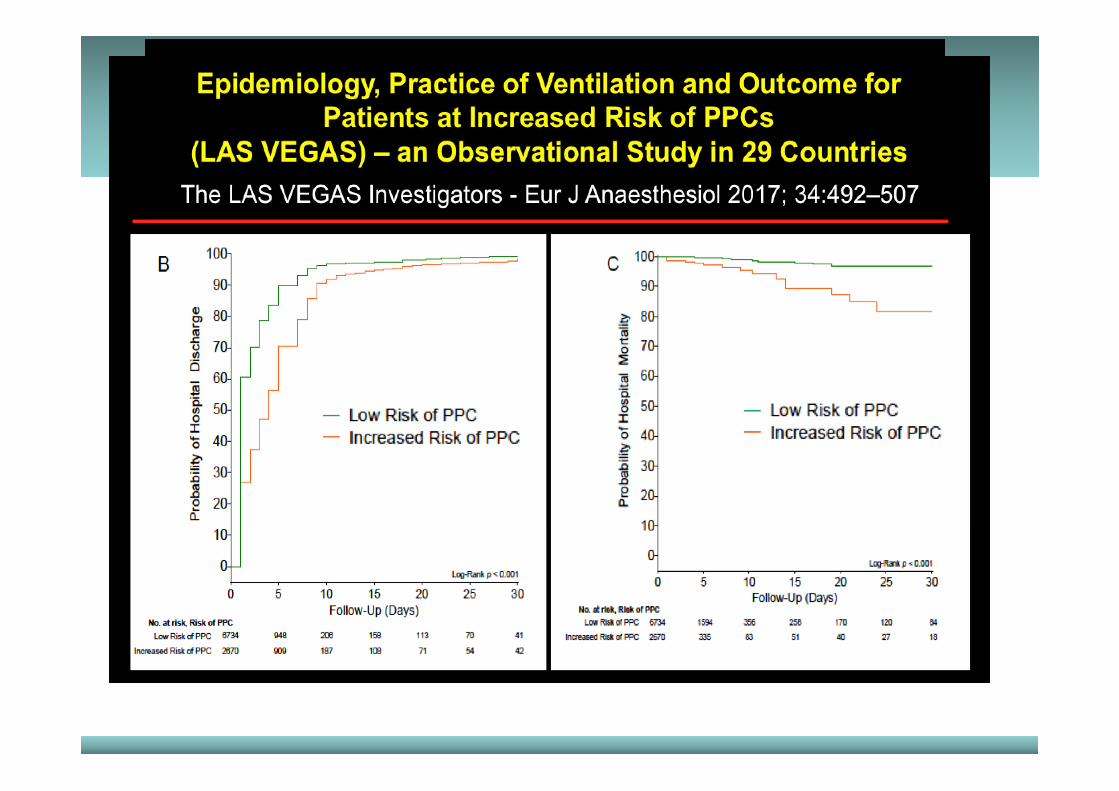
• International observational study
• 9,864 patients• 8.1 [7.2–9.1] mL/kg
PBW• VT > 8 mL/Kg in
40% of patients
LAS VEGAS – Practice of Ventilation in ORs Worldwide
The LAS VEGAS Investigators - Eur J Anaesthesiol 2017; 34:492–507
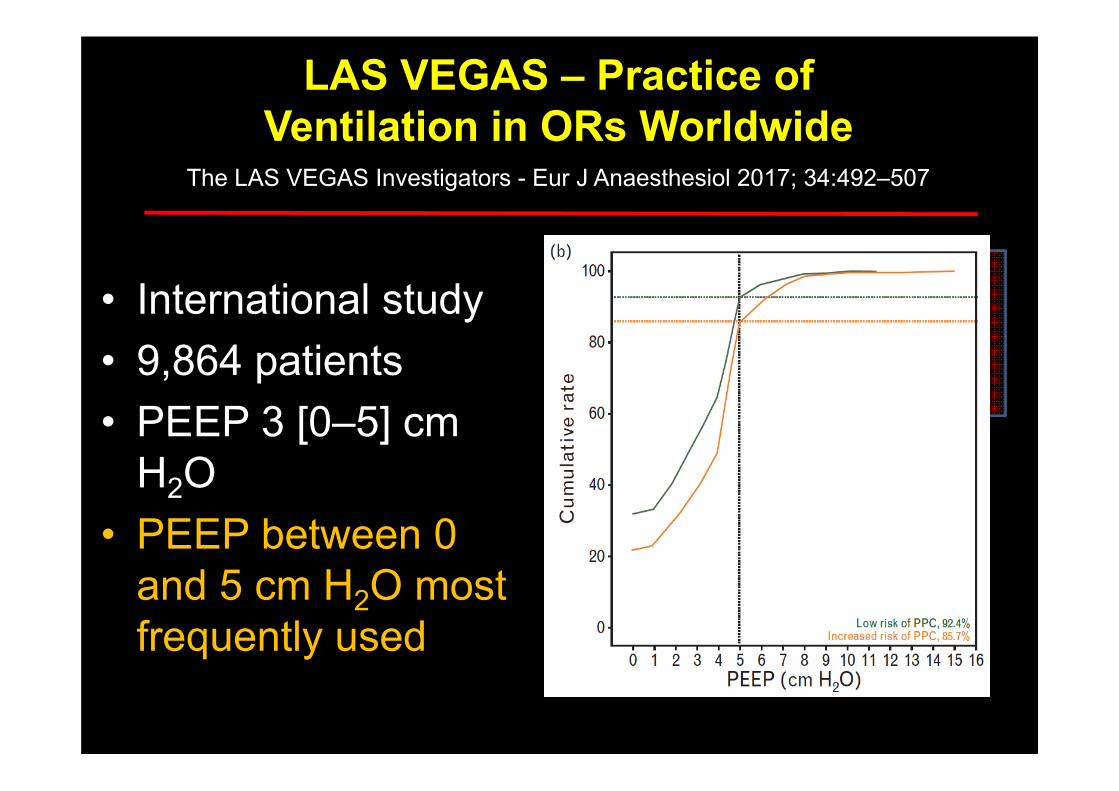
• International study• 9,864 patients• PEEP 3 [0–5] cm
H2O • PEEP between 0
and 5 cm H2O most frequently used
LAS VEGAS – Practice of Ventilation in ORs Worldwide
The LAS VEGAS Investigators - Eur J Anaesthesiol 2017; 34:492–507

• International study• 9,864 patients• P 12.5 [8.0-18.0]
cm H2O• P > 13 cm H2O
in 45 % of patients
LAS VEGAS – Practice of Ventilation in ORs Worldwide
The LAS VEGAS Investigators - Eur J Anaesthesiol 2017; 34:492–507

Paolo Pelosi. ESA. June 2017.


“To keep learning, sometimes it is crucial to unlearn, what you have studied before”
Aristotle
And this is very painful…
How important is this ?
• 230 millions of surgical operations every year under general anaesthesia
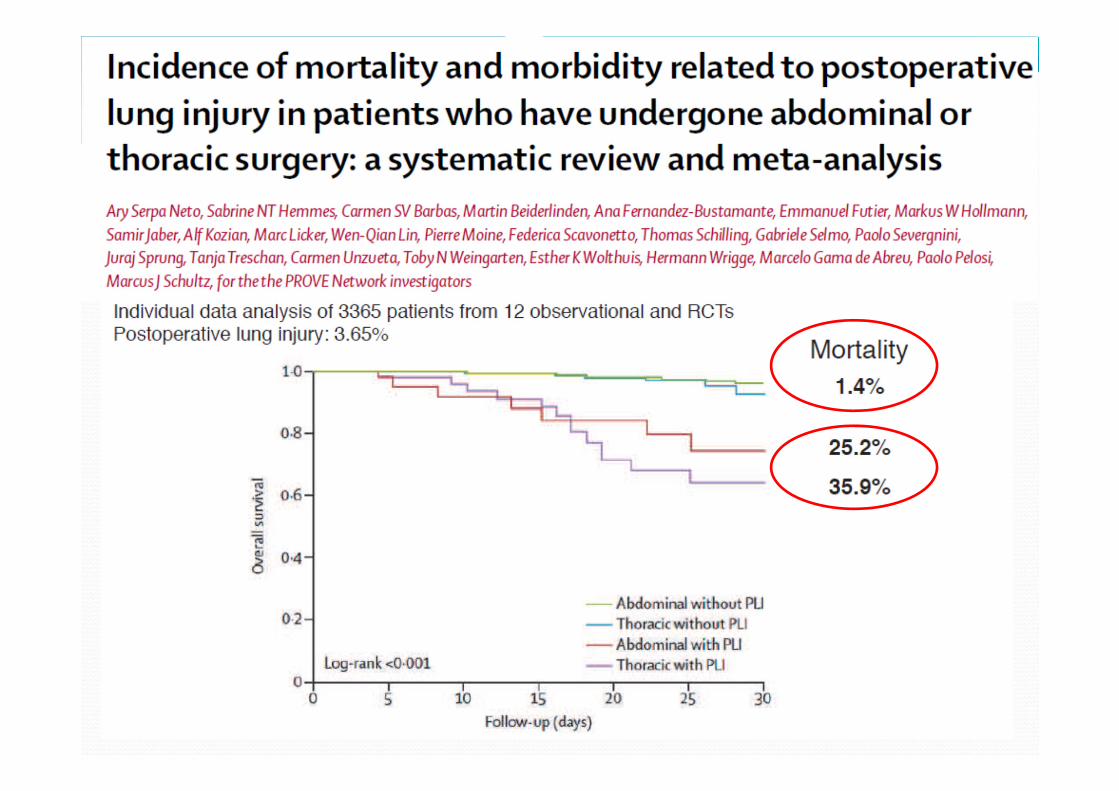
• 10 % (some report up to 59 %) of the patients have PPC (postoperative pulmonary complication)‐ pneumonia, ARDS, ARF, re‐intubation, etc..
• It means 23 millions of PPC a year
• What are the consequences ?
•20
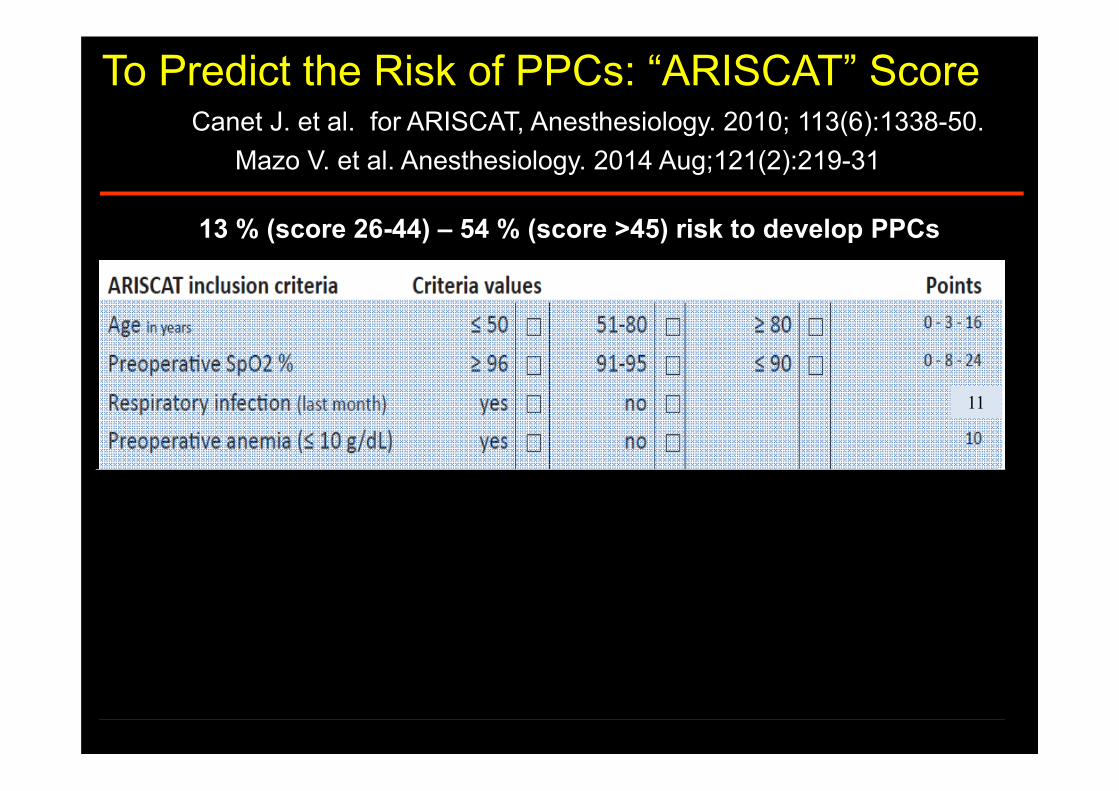
To Predict the Risk of PPCs: “ARISCAT” Score
13 % (score 26-44) – 54 % (score >45) risk to develop PPCs
Canet J. et al. for ARISCAT, Anesthesiology. 2010; 113(6):1338-50.
11
Mazo V. et al. Anesthesiology. 2014 Aug;121(2):219-31
Physiology and Pathology of Postoperative Pulmonary Complications
• PPC: increase • Mortality • Mobility• No sense Heath cost: because nobody want this
• Pneumonia (at floor): 15 days x 600 euro/d = 9,000 euros
• 207 billions euros the minimum cost of PPC
• 20,000 surgeries/year = 18 millions euro /year
• Can we do something to reduce PPC?
•25
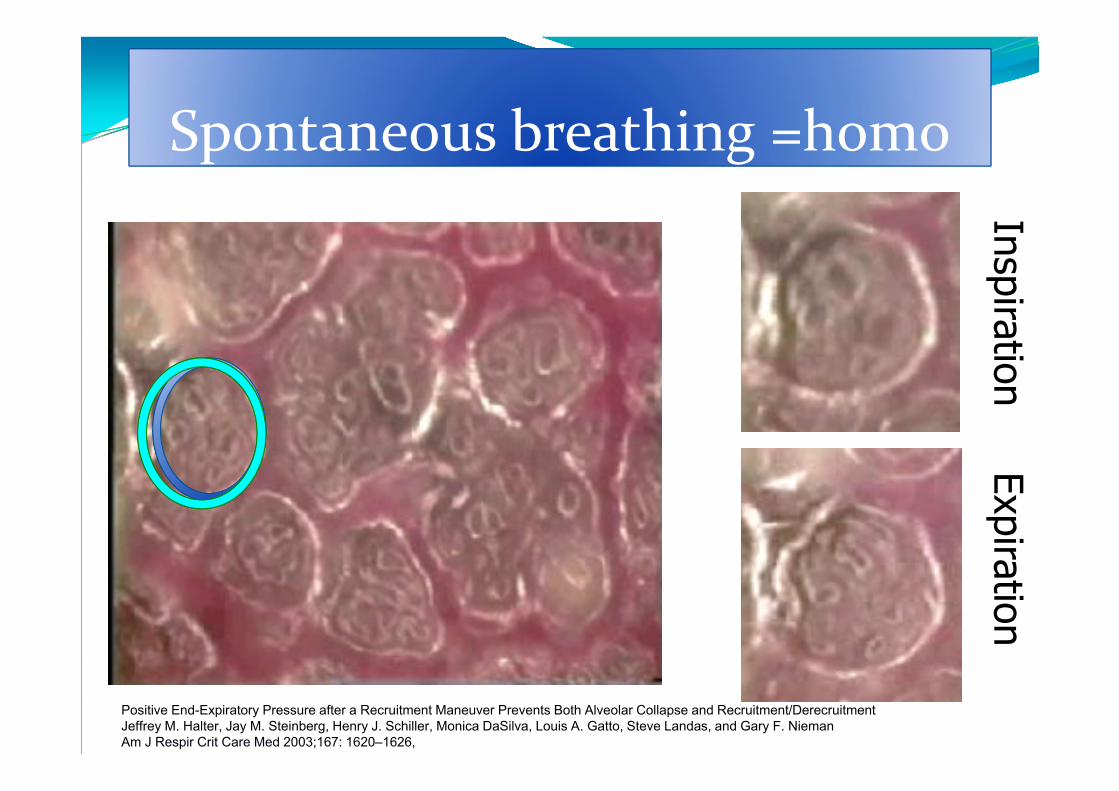
Spontaneous breathing =homoInspiration
Expiration
Positive End-Expiratory Pressure after a Recruitment Maneuver Prevents Both Alveolar Collapse and Recruitment/DerecruitmentJeffrey M. Halter, Jay M. Steinberg, Henry J. Schiller, Monica DaSilva, Louis A. Gatto, Steve Landas, and Gary F. NiemanAm J Respir Crit Care Med 2003;167: 1620–1626,
Physiopathology of VILI: Normal breathing Lungs are designed to receive an homogenous, well distributed, low tidal volume of 6 ml/kg of PBW
If you have an increase in the oxygen demand, the physiologic response is an increase in respiratory rate and change I:E ratio to 1:1, by an active exhalation
Just what neonates always do !!!!
NO ATELECTASIS, NO CYCLIC COLLAPSE, NO CYCLIC OVERINFLATION
Everybody loves homogeneity in mechanical ventilation
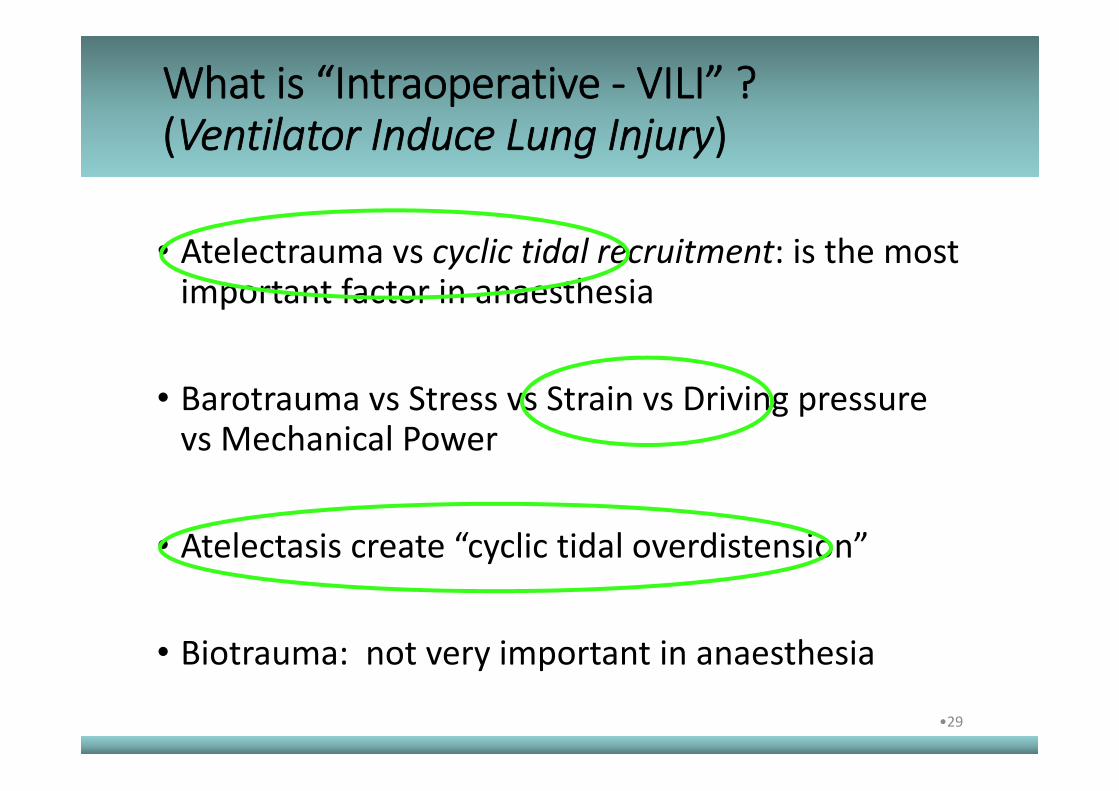
• Atelectrauma vs cyclic tidal recruitment: is the most important factor in anaesthesia
• Barotrauma vs Stress vs Strain vs Driving pressure vs Mechanical Power
• Atelectasis create “cyclic tidal overdistension”
• Biotrauma: not very important in anaesthesia
What is “Intraoperative ‐ VILI” ? (Ventilator Induce Lung Injury)
•29
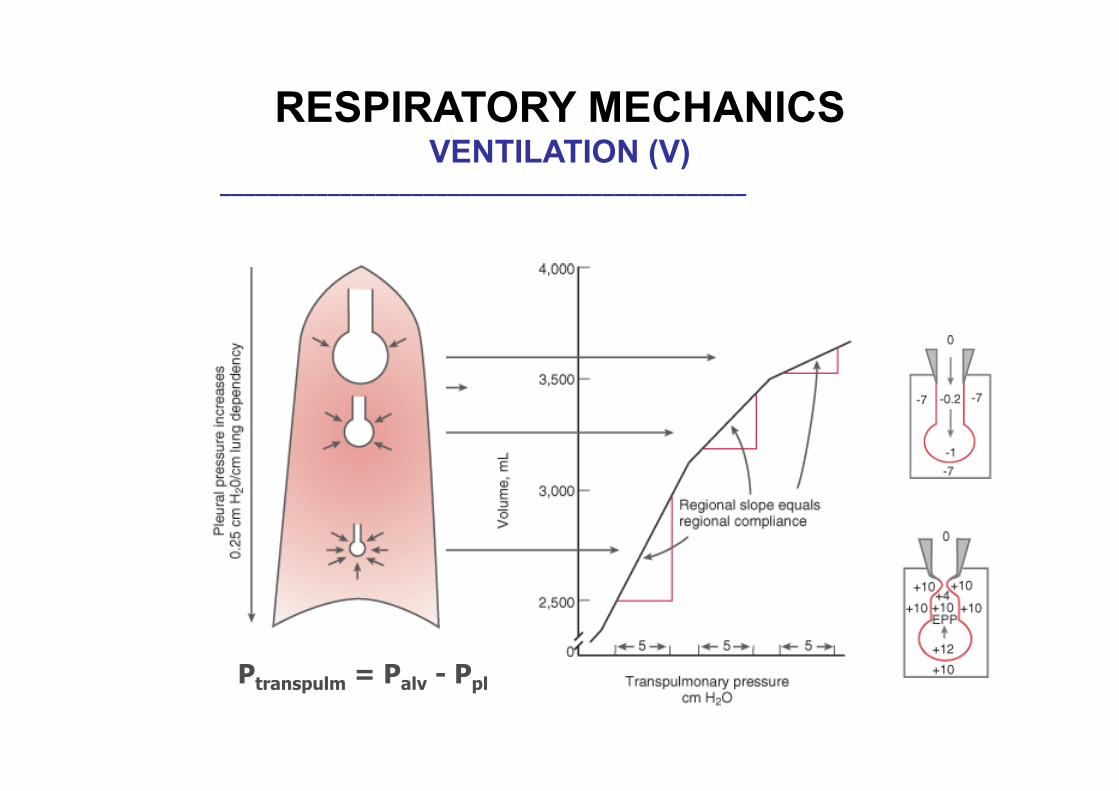
Ptranspulm = Palv - Ppl
____________________________________________
RESPIRATORY MECHANICSVENTILATION (V)

Ratio of ventilation to perfusion (V/Q) Mechanical ventilation

Ratio of ventilation to perfusion (V/Q) Spontaneous breathing
•____________________________________________
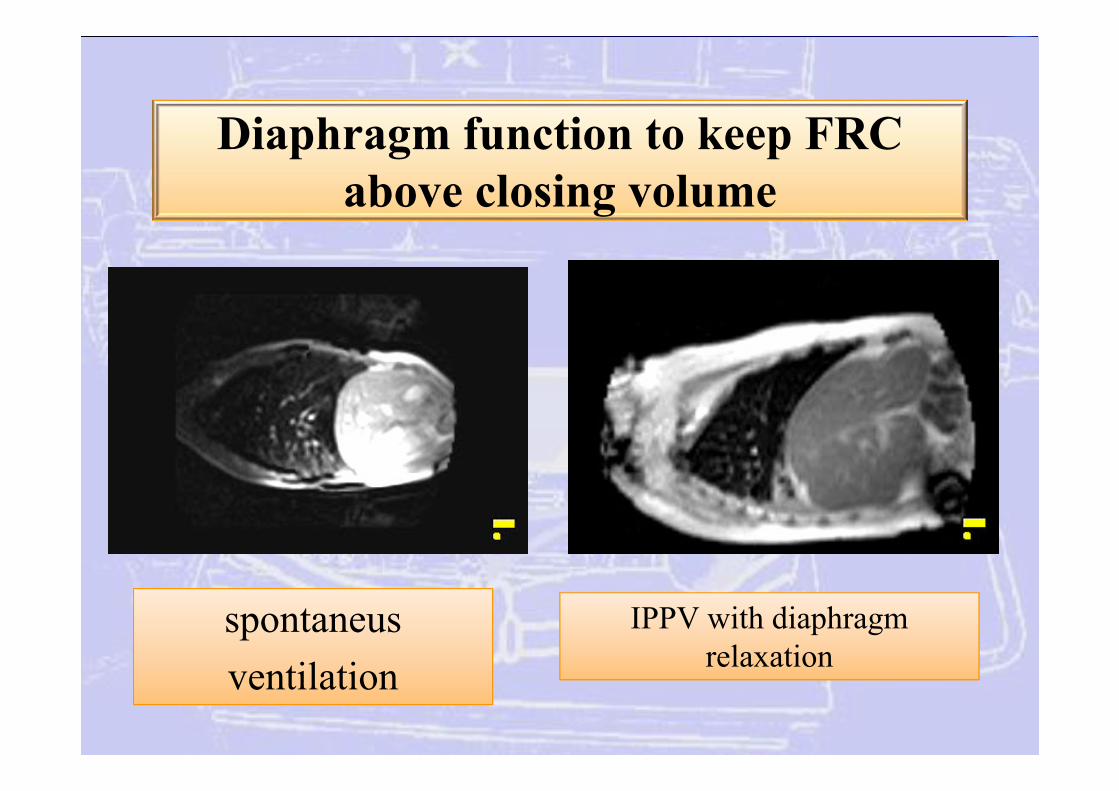
Diaphragm function to keep FRC above closing volume
IPPV with diaphragm relaxation
spontaneusventilation
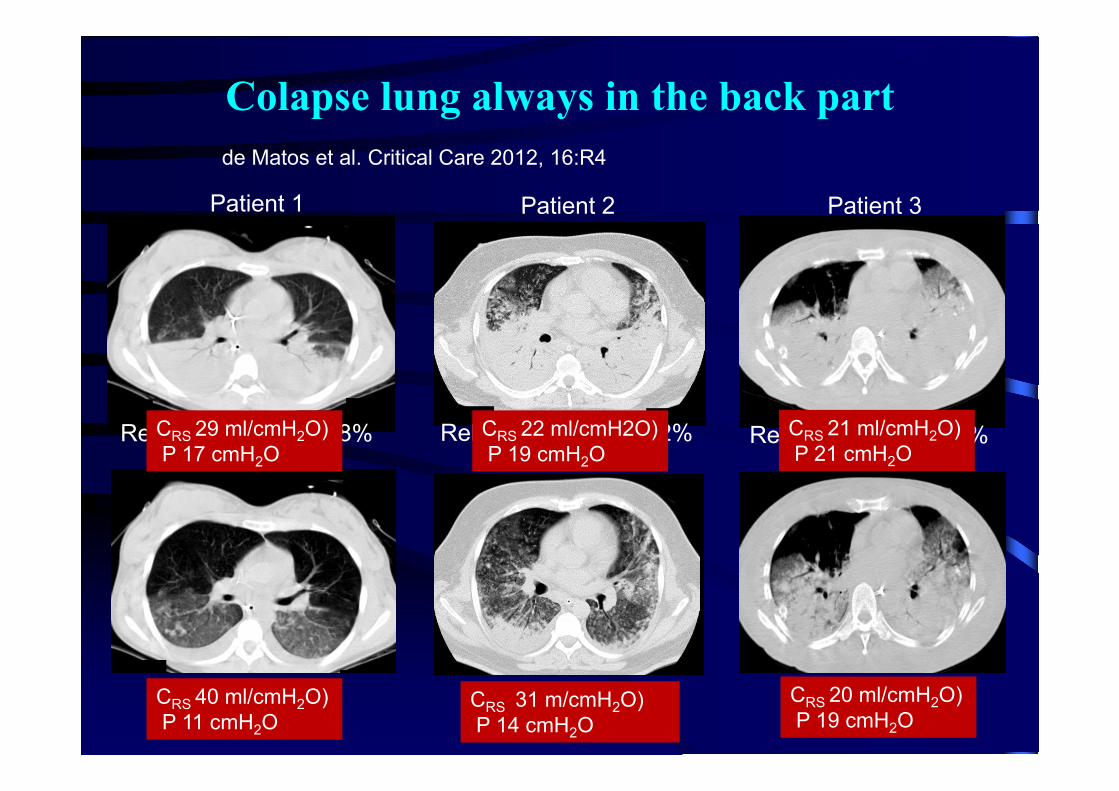
Colapse lung always in the back part
Relative response: 98% Relative response: 82% Relative response: 5%
de Matos et al. Critical Care 2012, 16:R4
Patient 1 Patient 2 Patient 3
CRS 29 ml/cmH2O)P 17 cmH2O
CRS 40 ml/cmH2O)P 11 cmH2O
CRS 22 ml/cmH2O)P 19 cmH2O
CRS 31 m/cmH2O)P 14 cmH2O
CRS 21 ml/cmH2O)P 21 cmH2O
CRS 20 ml/cmH2O)P 19 cmH2O