Embed Size (px)
Citation preview

Implementing Evidence‐Based Practices in North CarolinaJanuary 24, 2014

Building an Evidence Based System of Care
Arthur C. Evans, Ph.D., Commissioner
Philadelphia Department of Behavioral Health and Intellectual disAbility Services

Philadelphia Behavioral Health System
Single payor (Medicaid, state & federal block grants, local grant) behavioral health system operated by the City
$1b Service system for children, adults & families
Substance Abuse and Mental Health
Broad range of services from acute care hospitals to small niche outpatient programs
System transforming around the principles of recovery and resilience

What is the goal of EBP’s?
A. Implement EBP to fidelity
B. Implement EBP in context of local community
C. Improve the likelihood of best outcomes

Need to spend wisely: Do what has the greatest probability of
achieving the desired recovery & resilience outcomes
Rationale for Emphasis on EBP's

Take Home Messages
Evidence Based Practices can be successfully implemented The primary reason that EBP’s should be implemented is to improve outcomes An implementation and systems change framework is useful for EBP adoption A systems perspective is needed A Developmental approach is necessary

Background

Evolution of the EBP Field:3 Generations
1st : Effectiveness Science (initial) Build it and they will come approach Emphasis on manuals, tool kits and dissemination Heavy emphasis on defining evidence; what’s in, what’s out
2nd : Implementation Science (current) Understand that there is a science behind implementation itself Specific strategies are needed for successful implementation Emphasis on uptake, fidelity
3rd : Sustainability Science (emerging) Understanding that sustaining practice requires a different set of skills and
strategies than implementation Emphasis on long‐term integration of EBP’s into existing organizations and
systems Focus on the utility of EBP’s ; a means to an end; outcomes!

Categories of Evidence
Evidence ‐Based‐Supported‐Informed ‐Suggested


Recovery Oriented System of Care

Four Building Blocks to Transformational Change
Community & Cross Systems Collaboration
Optimize Treatment Services
Recovery Support Services
Fiscal & Administrative
Policy & Procedure Alignment

ROSC: Building Block Strategies
Optimize clinical service delivery Orient and re‐engineer services around the goal of long‐term recovery with an understanding of their role in that process
Optimize the clinical effectiveness of treatment services through the use of empirically supported treatments, individualized approaches (i.e., co‐occurring, trauma informed, culturally competent, developmentally appropriate, etc)
Add and integrate recovery support services Add those recovery support services that are needed to support long‐term recovery for individuals and their families
Utilize both free standing and integrated services that are embedded within treatment and add another dimension to the treatment process

ROSC: Building Block Strategies
Fiscal and Administrative Policy & Procedures Ensuring that policy and procedures support the practice changes that have been implemented
Remove administrative & fiscal barriers to recovery‐oriented practice
Build Cross‐Systems Partnerships and Community Recovery Capital Goal: resilient and healthy communities
Communities’ capacity to prevent behavioral health challenges, intervene early when they occur and support individuals who are in the recovery process
Requires public health strategies

Evidence‐Based Practice and Innovation Center
Build an Evidence Informed System of Care(Evidence‐Based Principles, Practices, Programs, Policies)
Build Organizational and System Capacity
Focus on Outcomes

Beck Initiative
2007 – CBT works but community mental health providers aren’t delivering it Training
+ consultation+ certification+ sustainability support+ financial off‐set for time in training

Beck Initiative
Started with Outpatient
Exported/adapted throughout system
Milieu Training & Recovery Oriented CT for Schizophrenia
Over 200 therapists trained in 28 agencies
77 % achieving initial certification
Demonstrated feasibility of training community providers in CT

THERAPIST PERSPECTIVE"The Beck Initiative and the use of CBT have transformed the way I offer therapeutic services. I feel much more equipped when it comes to assisting my patients by having an effective tool I have been schooled on. Learning such practices such as guided discovery or examining thought processes is quite relevant to the needs of my patients and has proved rewarding."
" The techniques learned through the Beck Initiative have been instrumental in organizing both members AND myself with needed skills to move the Recovery process forward. My members have already begun responding with improvements in reduction of symptoms since training began less than six months ago."
CLIENT PERSPECTIVE“I liked knowing that some day I wouldn’t need to come to therapy, because at some point there is a end and I will be able to things on my own”“By discussing my thoughts she helps me go in the right direction when I am stuck on something and then I see and feel better about myself”
“I have had a lot of therapists and she is one of the best. I feel the cognitive therapy is going to be very helpful to me”
“I haven’t felt this good in 30 years.”
Cognitive Therapy Feedback

Trauma Initiative
Trauma Initiative – Prolonged Exposure ‐ TF‐CBT ‐Sanctuary Model– PE: 4 day workshop +audio consultation on 2 cases
Philadelphia Alliance for Child Trauma Services– TF‐CBT ‐ CF‐TSI– TF‐CBT: 2 day workshop, 6 months group consultation, 1 day booster

7 teams Outpatient, Adult Residential and ACT teams 6 months intensive training and consultation Currently receiving additional 6 months of consultation
DBT Initiative

Other EBP’s
Functional Family Therapy
Multi‐Systemic Family Therapy
Motivational Interviewing
etc.

Temple University Hospital Extended Acute Care Pilot Program
Optimal Evidence‐Based Treatment & Discharge Planning Recovery‐Oriented
Cognitive Therapy (CT‐R) Certified Peer Specialists Families Community
Excursions/Life Skills Training
Medical Collaboration
Comprehensive Assessments Collateral Information Standardized Assessment
Instruments
Continuity of Care Assertive Community
Treatment (ACT) Team

Preliminary Findings
Reduction of falls, assaults, & restraints Reduction of medications (IM PRNs)

10 Lessons Learned

#10: Identify Outcomes Before Implementation
outcomes and evaluation identified up front
system assessment, id system need and how the EBP fits and addresses need, how EBP goes across the continuum
build the EBP into the Quality Improvement process
agree on data/outcome selection and sharing with EBP Purveyors

#9: Build Payor (Administrative) Capacity Simultaneously
Payors have to change as the provider system is changing
Payors and system administrators must have the capacity and competency to oversee implementation and incorporation of EBP’s
Program administrators need standards

#8: Shift from Training to Implementation Model
Focus on organizational capacity from the beginning
Metrics and “fidelity” should include organizational factors
Should have standards for practitioners, organizations and systems to evaluate the progress of the implentation

#7: Incorporate a Multi‐Level, Developmental Perspective
Understand phases both within and across various EBP implementations Maturity of EBP implementations changes approach Phases happen at various levels within the system

Pre‐Implementation(Readiness) Implementation Sustainability
Practitioner• Clinician Qualifications (education, culture…)
• Training• Fidelity Assessment
• Ongoing Supervision
Organization• Assessment of General Capacity
• Programmatic & Organizational Fit
• WorkforceCapacity
System• Determining EBP Need• Role of EBP within the System
• Financing• Triaging• “Marketing”
• Outcomes & Evaluation
• Scalability
Developmental Focus of Tools, Training & TA (Examples)

#6: Each EBP Implementation is Different
While there are commonalities across all implementations, EBP’s are different and their implementations will be different
Multiple approaches can be used to effectively introduce EBP’s into a system: rfp's, payor pay for training, enhanced rates, etc
Understand dimensions of difference (e.g., CBT is general practice vs Prolonged Exposure is very specific)
Context matters. Systems are different (eg Managed systems)

#5: Move Beyond provider readiness and general capacity
Providers vary greatly in their readiness to successfully implement EBP’s
However, readiness may not be enough. Some may have the organizational capacity, but other factors may impinge on implementation
Providers may have to build other capacities simultaneously with the EBP because they are necessary (eg data collection, standardized assessments)
Clearly knowing both the general and specific capacities is critical (ie capacity needed for all EBP’s and for the specific EBP being implemented)

#4: Select providers wisely
Implementing EBP’s is a significant investment and not all providers are ready to effectively adopt new practices
There will be attrition. Intentionally minimize it. Some providers better suited for some EBP’s Selection goes beyond capacity and includes issues such as “bandwidth”, populations served and likelihood to deliver the practice to the appropriate population

#3 Determine Sustainability Plan before Implementation Begins
Understand the fiscal, administrative, clinical and workforce issues necessary for sustainability Be clear on the system need prior to implementation. What is the utility Articulate standards across all levels from practitioner to policymaker

#2: Build in system level work with purveyors
Work with EBP developers on the programmatic and systems issues that go beyond training Partnership should result in mutual benefits Get lessons learned from other system implementations

#1: It’s a Marathon, Not a Sprint
Successful implementation occurs when practices are sustained and there is a culture change within provider organizations and the broader system
Recognize the complexity of large‐scale change Use a Continuous Quality Improvement Framework for EBP Implementation (does the system get better at it over time)

#1: Use EBP’s to Address Challenges
Emphasize the utility of EBP’s Fit EBP’s into other system priorities and goals Use EBP’s to address specific challenges facing a provider and/or system (e.g., engagement, retention, recidivism, employment, housing, etc)

Fitting The Pieces Together
Individual receiving services
EBP developer / trainer
Treatment Setting / Organization
EBP

Connecting the Dots
Pay for Performance Housing initiative

39
Pay for Performance ‐ Sample Adult Inpatient Matrix

Permanent Supportive Housing Initiative
Housed 1916 single adults since 2008• 1461 had a history of street homelessness• High rate of retention
Used Evidence Based Practices and Principles and Recovery Framework Specialized Package of Clinical Services Leverage Medicaid dollars for housing resources

Change Management Process

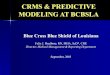
Start with Early Adopters
0
50
100
150
200
250
300
Cumulative Adopters
Early Adopters
Incentives Requirements
Largest # ofAdoptersLargest # ofAdopters
Cumulative adopters of Hybrid Seed Corn in Iowa between 1927 and 1941Classic diffusion study by
Ryan & Gross
Education
Mid‐StageAdopters
Late‐StageAdopters

Taking a systems perspective that attends to multiple levels of analysis is important for successful EBP implementation
Must work simultaneously at the practitioner, organizational and systems levels
Focus of EBP implementation should be on the achievement of outcomes
Summary