Embed Size (px)
Citation preview
YEAR FIVE, QUARTER TWO MALARIA
DIAGNOSIS AND TREATMENT PROGRESS
REPORT
January-March, 2020
Private Health Sector Project

The Private Health Sector Project is a technical assistance project to support the Government of Ethiopia. The Private Health Sector Project is managed by Abt Associates Inc. and is funded by the United States Agency for International Development (USAID) under Contract No. AID-663-LA-16-00001. Recommended Citation: Private Health Sector Project. Year Five, Quarter Two, Malaria Diagnosis and Treatment Progress Report (January-March 2020). Abt Associates Inc. Rockville, MD. Submitted to: Dr. Mesfin Tilaye Agreement Officer’s Representative Health Network Program Advisor
USAID| Ethiopia Addis Ababa, Ethiopia
Submitted by: Dr. Mesfin Teferi, Chief of Party USAID| Private Health Sector Project
Abt Associates Inc. 1 6130 Executive Blvd
1 Rockville, Maryland 20852 1 T. 301.347.5000 1 F. 301.913.9061
1 www.abtassociates.com

YEAR FIVE, QUARTER TWO MALARIA
DIAGNOSIS AND TREATMENT PROGRESS REPORT
DISCLAIMER The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development (USAID) or the United States Government


PAGE
\* MERG
CONTENTS
Acronyms 31.
Program description
51.1
General Overview
51.2
General Objectives
61.3
Strategies
62.
Performance report
82.1
Improving an Enabling Environment for the Private Health Sector Engagement
82.2
Increasing Access to Malaria Case Management
92.2.1
New workplace facilities assessment for technical support
92.2.2
Provision of malaria diagnosis and treatment
102.2.3
Supportive supervision of health facilities and providers
222.3
Private Health Care System Strengthened
212.3.1
Capacity building for transition
222.3.2
Supply chain management and rational drug use enhanced
222.4
Program Learning and Innovative Ventures Enhanced for the Private Health Sector
262.4.1
Advocacy for operational manuals
262.4.2
Mapping mid to large private farmlands in Gambella and Benishangul Gumuz regions
Error! Bookmark not defined.2.4.2.1 Summary of mapping in Benishangul Gumuz
region 24
2.4.2.2 Summary of mapping in Gambella region Error! Bookmark not defined.2.4.2.3
Summary of mapping in Amhara region 26
2.4.3. Piloting temporary malaria clinics to the MMWs. Error! Bookmark not
defined.2.4.5. Develop success stories on the benefits of temporary clinics in BG 30
2.4.6. Develop a toolkit to help to guide the implementation and provision of temporary malaria
clinics to seasonal MMWs and IDPs262.4.7. Develop mass community awareness

PAGE
\* MERGE
creation sessions on malaria prevention and treatment for seasonal migrant workers273.
Transitioning Activities
274.
Challenges and Solutions
305.
Major Activities for Year Five , Quarter Two
336. Malaria Program Activity Matrix, Year Five, Quarter Two (January-March 2020)
35Annex B: Number of facilities reported in Quality 1mprovement for malaria
diagnosis and treatment Error! Bookmark not defined.
I
List of Tables
Table 1. List of PHSP-supported sites by region (October –December
2019) 6
Table 2. Number of malaria suspected and confirmed cases by region
at PHSP-supported private health facilities 13
Table 3. Malaria cases treated, admitted, referred and malaria-related
deaths in PHSP-supported private health facilities 14
Table 4. Malaria cases by age and sex in PHSP-supported facilities
15
Table 5. Malaria blinded-rechecking performance on PPM-facilities
(January - March 2020) 17
Table 6. Number of malaria laboratory sites visited by region and
training status (January – March 2020) 18
Table 7: Availability of Laboratory Commodities (January – March
2020) 21
Table 8: Quality Assurance and EQA Practices (January – March
2020) 22
Table 9: Supportive supervision findings from 58 health facilities
(January –March 2020) 23
Table 10: Summary of post-transition mentoring visits in PPM
facilities 24
Table 11: Summary of the post-transition mentoring visits at
RHB/THO/EPSA hubs and RLs (January – March 2020) 32

PAGE
\* MERG
List of Figures
Figure 1: Trends in malaria diagnosis and treatment in PHSP-
supported facilities (January-March 2020) 14
Figure 2: Malaria case identification and treatment by workplace sites
at PHSP-supported facilities (January-March 2020) 15

PAGE
\* MERGE
ACRONYMS
AL Artemether Lumefantrine
AM Artemeter
BG Benishangul Gumuz
CQ Chloroquine
EPHI
EQA
FDRE
FMOH
HMIS
Ethiopian Public Health Institute
External Quality Assurance
Federal Democratic Republic of Ethiopia
Federal Ministry of Health
Health Management Information System
IDP Internally Displaced Persons
IEC Information, Education and Communication
IM Intramuscular
IV Intravenous
JSS
MMW
NMCEP
Joint Supportive Supervision
Mobile and Migrant Workers
National Malaria Control and Elimination Program
OPD
PF
PHEM
Outpatient Department
Plasmodium Falciparum
Public Health Emergency Management
PHSP Private Health Sector Project
PMI President’s Malaria Initiative
PO Per Oral
PPM Public-Private Mix
PQ
PV
Primaquine
Plasmodium Vivax
PW Pregnant Women
RDT Rapid Diagnostic Test
RHB
RRF
Regional Health Bureau
Requesting and Reporting Form
SNNPR
Southern Nations, Nationalities, and Peoples Region
SOP Standards of Practice

PAGE \*
MERGE
TAC Technical Advisory Committee
TB
TBF
THO
TRDT
TWG
USAID
WHO
Tuberculosis
Total Blood Film
Town Health Office
Total Rapid Diagnosis Test
Technical Working Group
United States Agency for International Development
World Health Organization

PAGE
\* MERGE
1. PROGRAM DESCRIPTION
1.1 General Overview
The Private Health Sector Project (PHSP) is funded by the United States Agency for International
Development (USAID) and the President’s Malaria Initiative (PMI). The project’s technical areas
include malaria diagnosis and treatment, HIV care and treatment, Public Private Mix (PPM)
Directly Observed Therapies (DOTS), family planning (FP), and maternal, neonatal, and child
health (MNCH). PHSP’s main objectives are to enable an environment for private sector
engagement in health improvements, to increase access to quality services for diseases of public
health importance, to strengthen private health care systems, and to implement program learning
and innovative ventures to enhance evidence-based decision making. This quarterly report
focuses on PHSP activities related to malaria implemented from January to March 2020.
To increase the provision of malaria treatment and care services in Ethiopia, PHSP provides
technical and financial assistance to private and workplace health facilities to enable quality
malaria diagnosis and treatment. In Year Five Quarter three , the project provided technical
support and monitored performance of health services provided in 163 health facilities (18 in Afar,
27 in Amhara, 15 in Beneshangul Gumuz, 14 in Dire Dawa, 13 in Gambella, 35 in Oromia, 24 in
Tigray, and 17 in Southern Nations, Nationalities, and Peoples region). PHSP also monitored
performance in 32 workplace facilities, including 12 facilities from the Federal Democratic
Republic of Ethiopia Sugar Corporation. Within the same period, these facilities evaluated 80,882
malaria suspected cases, of which 13,434 malaria patients were confirmed and received
treatment.
PHSP continued providing technical support to 1631 private for profit facilities and 32 workplace
health facilities. In addition, PHSP enrolled 2 new workplace facilities that have 12 clinics located
in Gambella. In total, PHSP supported 32 workplace health facilities during Quarter Two. PHSP
is also supporting Benishangul Gumuz and Gambella regions introducing innovative approaches
to establish access for malaria diagnosis and treatment for migrant workers and refugees.
PHSP conducted region-specific workshops and orientation sessions with regional officials,
woreda program managers, and PPM health facility owners and directors to prepare them for a
smooth transition and to strengthen their connections so private facilities can continue receiving
support from government health agencies.
1 Three PHSP-supported facilities were closed during this reporting period (2 in Gambella and 1 in Amhara)

PAGE \*
MERGE
The project also supported the PPM malaria facilities by conducting phone-based mentoring,
conducted supportive supervision in some facilities, and addressed their challenges by providing
trainings, clinical seminar, registers, and job aids, preparing the facilities for laboratory microscopy
EQA, and ensuring their access to pharmaceutical supplies. A list of PHSP-supported sites can
be found on Table 1.
Table 1. List of PHSP-supported health facilities by region (January - March 2020)
Region Private-for-profit
health facilities
Workplace
health
facilities
Temporary
malaria
clinics
Total
Afar 18 10 0 28
Amhara 27 3 0 30
Beneshangul Gumuz 15 0 1 16
Dire Dawa 14 0 0 14
Gambella 13 3 0 16
Oromia 35 8 0 43
SNNPR 17 3 0 20
Tigray 24 5 0 39
Total 163 32 1 196
1.2 General Objectives
The malaria component of the project has the following objectives:
● Increase access to and uptake of malaria services in private health facilities and
workplaces focusing on mobile and migrant workers (MMW)
● Enhance the capacity of local partners to ensure the sustainability of public-private mix
(PPM) partnerships
● Enhance pharmaceutical supply chain management and rational drug use at private
health facilities, including workplaces
● Enhance program learning and innovative ventures
● Generate evidence on malaria service needs of the migrant and mobile workforce for
decision-making and programming
1.3 Strategies
To meet the project’s targets and mitigate the main challenges faced in the past, such as poor
access to malaria prevention and management services for seasonal migrant workers and the

PAGE
\* MERGE
lack of national policy on PPM malaria, PHSP applied the following implementation strategies in
Quarter Two:
● Work collaboratively with the National Malaria Control and Elimination Program
(NMCEP), Regional Health Bureaus (RHBs) and other stakeholders to improve the
policy and legal environment to engage the private health sector in the delivery of
malaria treatment and prevention.
● Actively participate in the national Technical Working Group (TWG) and Technical
Advisory Committee (TAC) and advocate for the inclusion of the private sector in
national malaria prevention and control planning, implementation and monitoring.
● Facilitate finalization, printing and distribution of PPM implementation guidelines to all
private health facilities supported by PHSP and other stakeholders.
● Facilitate a national consultative workshop to increase the engagement and participation
of stakeholders to implement innovative approaches towards malaria prevention and
control for MMWs in Ethiopia.
● Support the NMCEP to produce a national policy directive based on the inputs from the
consultative workshop.
● Advocate for customization of training content and duration of malaria case management
for clinicians in private practice.
● Provide technical and financial support to RHBs in Beneshangul Gumuz and Gambella
to formulate and disseminate region-specific guidance to access malaria case
management services in public health facilities by MMW and refugees.
● Enhance access to malaria case management by MMW in private facilities and
workplaces in malaria endemic areas by providing technical support.
● Collaborate with RHBs to run temporary and seasonal clinics by deploying health
providers to provide malaria case management to MMW in clusters of farms.
● Provide technical support to farms to establish adequate workplace health facilities to
provide malaria case management per the national protocol.
● Train permanent farm workers in malaria diagnosis and treatment and deploy them to
farms without access to private or public health facilities.
● Enroll new private for-profit or not-for-profit health facilities operating in towns with an
elevated presence of MMW and refugees.

PAGE \*
MERGE
● Ensure high quality of malaria case management in private facilities by providing
training, mentoring, joint supportive supervision (JSS) and implementing continuous
quality improvement visits.
● Build knowledge and practices of MMW on prevention and control interventions against
malaria.
● Build capacity of providers in supported health facilities to collect and report performance
data directly to PHSP using data transfer with smart phones or making telephone calls.
This significantly helps to increase the capabilities of the PPM health facilities in
strengthening the sustainability of the data reporting to the government system.
● Perform mapping to estimate the size of mobile and migrant workforce and access to
malaria care and prevention, particularly in Benishangul Gumuz and Gambella regions.
● Generate evidence through innovate implementation approaches and operational
research.
2. PERFORMANCE REPORT
2.1 Improving an Enabling Environment for the Private Health Sector Engagement
PHSP is an active member of the TAC and TWGs supporting the NMCEP at the federal and
regional health bureau levels. The project provided technical support to the Federal Ministry of
Health during the national malaria program desk review workshop. During the desk review
assessment participants reviewed the contents of WHO references, national guidelines, national
policy documents, national reports/surveys, national recording and reporting tools, training
materials and identified the following constrains in the private sector:
● National malaria indicators are not disaggregated by public and private facilities, except
the PPM facilities
● Private facilities have no access towards the national malaria program activities and
drugs
● Delays in the approval of PPM malaria guidelines and lack of policy implementation
manual to implement the malaria prevention and management to mobile and migrant
workers and refugees
PAGE
\* MERGE
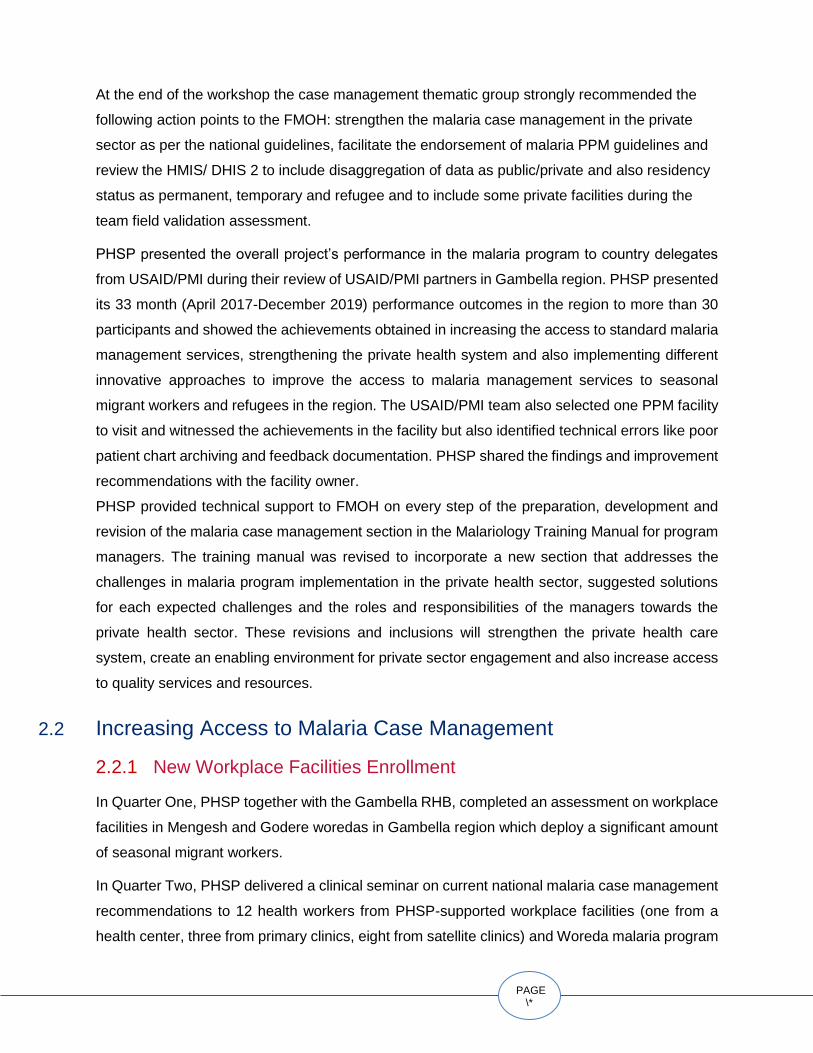
At the end of the workshop the case management thematic group strongly recommended the
following action points to the FMOH: strengthen the malaria case management in the private
sector as per the national guidelines, facilitate the endorsement of malaria PPM guidelines and
review the HMIS/ DHIS 2 to include disaggregation of data as public/private and also residency
status as permanent, temporary and refugee and to include some private facilities during the
team field validation assessment.
PHSP presented the overall project’s performance in the malaria program to country delegates
from USAID/PMI during their review of USAID/PMI partners in Gambella region. PHSP presented
its 33 month (April 2017-December 2019) performance outcomes in the region to more than 30
participants and showed the achievements obtained in increasing the access to standard malaria
management services, strengthening the private health system and also implementing different
innovative approaches to improve the access to malaria management services to seasonal
migrant workers and refugees in the region. The USAID/PMI team also selected one PPM facility
to visit and witnessed the achievements in the facility but also identified technical errors like poor
patient chart archiving and feedback documentation. PHSP shared the findings and improvement
recommendations with the facility owner.
PHSP provided technical support to FMOH on every step of the preparation, development and
revision of the malaria case management section in the Malariology Training Manual for program
managers. The training manual was revised to incorporate a new section that addresses the
challenges in malaria program implementation in the private health sector, suggested solutions
for each expected challenges and the roles and responsibilities of the managers towards the
private health sector. These revisions and inclusions will strengthen the private health care
system, create an enabling environment for private sector engagement and also increase access
to quality services and resources.
2.2 Increasing Access to Malaria Case Management
2.2.1 New Workplace Facilities Enrollment
In Quarter One, PHSP together with the Gambella RHB, completed an assessment on workplace
facilities in Mengesh and Godere woredas in Gambella region which deploy a significant amount
of seasonal migrant workers.
In Quarter Two, PHSP delivered a clinical seminar on current national malaria case management
recommendations to 12 health workers from PHSP-supported workplace facilities (one from a
health center, three from primary clinics, eight from satellite clinics) and Woreda malaria program

PAGE \*
MERGE
officers. All participants received the malaria case management guidelines, pocket reference
booklets, laboratory register, and a malaria morbidity register.
As a result of PHSP’s efforts to consolidate the sustainability of the government’s support to
private facilities, the regional health bureau officials and the woreda’s malaria program officer in
Gambella reached a consensus to provide the five newly enrolled workplace facilities with all the
essential commodities needed for malaria case management and will receive supportive
supervision after the end of the project. This is a key achievement for PHSP as it will guarantee
the continuity of malaria diagnosis and treatment in priority locations.
2.2.2 Provision of Malaria Diagnosis and Treatment
During this quarter a total of 81,768 malaria suspected cases were tested, 94% (75,051) using
blood film and 6% (6,717) using RDT. A total of 13,450 malaria cases were identified with
microscopy (12,077) and RDT (1,372) and 100% of cases were treated (Table 2). The number
of cases reported in this quarter is comparable to the number of cases (13,800) reported last
year in the same season (Fig-1).
Plasmodium falciparum (PF) parasite is the major cause of malaria for more than 72% (9,634)
of patients; P. vivax for 26% (3,509) and the remaining 2% (306) are mixed infections. Three
regions accounted for 66% of the total P. falciparum malaria: Gambella (31%), SNNPR (22%)
and Afar (13%). The highest malaria cases due to P.vivax were reported in SNNPR region
(34%) followed by Oromia (15%) (Table 3).
There was an increase in the number of cases reported from SNNP region (3,382) compared to
Quarter One this year (3,060) and same season (1,542) in 2019 because of increase influx of
workers into the sugar factories in Omo zone. More than 66% of the cases are reported from
workplace clinics in Kuraz Sugar project I and II where there was huge influx of workers. PHSP
has alerted the case build up to the RHB and the Sugar Corporation to enhance their
interventions, and has provided training in malaria case management and malaria microscopy to
the professionals in the workplace clinics.
In total, 72% of malaria confirmed cases were adults and 15% were children under five.
Regarding children confirmed cases, 29% were reported in Benshangul Gumuz and 21% in
Gambella, meaning that those regions account for 50% of all the under five children confirmed
cases. In Quarter Two, males were more affected by malaria than females (64% and 35%
respectively) and the overall rate of malaria in pregnant women was 2.3%. The highest number
of adult cases were reported in Tigrai (13%) and Benshangul (8%) (Table 4).

PAGE
\* MERGE
PPM facilities detected 9,940 P. falciparum cases and 61% of them received Artemether
Lumefantrine (AL) with single dose primaquine while 36% of them received AL only which might
be due to an interruption of PQ supply. There were also 3,509 P.vivax cases and 55% of them
received radical cure and 43% of them received only chloroquine. This report evidences the need
to roll-out primaquine for gametocidal clearance and radical cure that needs to be implemented
at full scale and clinicians need continuous clinical mentoring on use of PQ (Table 3).
Based on the residency status, 2,200 seasonal migrant workers and 115 refugee had received
malaria diagnosis and treatment services in PPM facilities. This data disaggregation by residency
status needs to be strengthened as it helps to inform the source of the burden of malaria in the
regions for evidence-based planning of malaria prevention and control in the region. Moreover,
PHSP will share the lessons learned so it can be replicated in public health facilities.

PAGE \*
MERGE
Table 2. Number of malaria suspected and confirmed cases by region at PHSP-supported private health facilities
(January –March 2020)
Region
All malari
a suspected
cases
Total cases
Microcopy RDT
TBF Pos % PF PV Mixed TRDT Pos % PF PV Mixed
Afar
7,595 1,627 7,400 1,556
21.0
% 1,229 315 12 195 71 36.4% 37 34 0
Amhara 14,62
3 1,206
14,26
1 1,150 8.1% 713 432 5 362 55 15.2% 15 31 9
Beneshangul Gumuz 9,795 1,691 9,795 1,691
17.3
% 1,211 479 1 0
0 0 0 0 0
Dire Dawa 1,522 132 1,522 132 8.7% 120 12 0 0 0 0 0 0 0
Gambella
8,443 3,293 8,128 3,172
39.0
% 2,863 168 141 315 121 38.4% 105 0 16
Oromia 20,24
0 954
17,77
2 730 4.1% 331 384 15 2,468 224 9.1% 89 135 0
SNNPR 13,60
3 3,382
12,66
6 2,928
23.1
% 1,776
1,05
5 97 937 454 48.5% 297 147 10
Tigray
5,947 1,165 3,507 718
20.5
% 515 203 0 2,440 447 18.3% 333 114 0
Total
81,76
8
13,450
75,05
1
12,07
7
16.1
%
8,758
3,04
8
271
6,717
1,372 20.4%
876
461 35
TBF= Total Blood Film; TRDT= Total Rapid Diagnostic Test; PF= Plasmodium falciparum; PV=
Plasmodium vivax; Pos= Positive

PAGE
\* MERGE
Table 3. Malaria cases treated, admitted, referred and malaria-related deaths in PHSP-supported private health facilities
(January –March 2020)
Region Total
cases
Total
treated
Treated Number of malaria cases
AL AL+PQ CQ CQ+PQ Quinine AM Artesunate Admitte
d
Referred Deaths
Afar 1,627 1,627 0 1,278 0 349 0 0 0 0 0 0
Amhara 1,206 1,206 505 151 360 89 0 89 12 9 0 0
Beneshangul Gumuz 1,691 1,691 37 1,162 74 405 8 5 0
0 0 0
Dire Dawa 132 132 43 57 11 1 2 0 18 18 0 0
Gambella 3,293 3,293 1,572 1,495 94 75 1 14 42 0 14 0
Oromia 954 954 53 380 31 443 0 5 42 0 0 0
SNNPR 3,382 3,382 507 1,499 614 577 2 155 28 46 10 0
Tigray 1,165 1,165 848 0 317 0 0 0 0 14 0 0
Total 13,450 13,450 3,565 6,022 1,501 1,939 13 268 142 87 24 0
CQ= chloroquine; AL= Artemether lumefantrine; AM= Artemether; PQ= primaquine

PAGE \*
MERGE
Table 4. Malaria cases by age and sex in PHSP-supported facilities
(January –March 2020)
Region Total cases
treated
Age in years and sex disaggregation
< 5 5 – 14 >=15 PW*
Total
Male Female Male Female Male Female Male Female
Afar 1,627 118 121 165 146 711 366 - 994 633
Amhara 1,206 101 60 83 82 590 290 - 774 432
Beneshangul Gumuz 1,691 269 232 160 145 499 386 31 928 763
Dire Dawa 132 2 1 17 5 76 31 - 95 37
Gambella 3,293 401 307 268 235 1,060 1,022 16 1,729 1,564
Oromia 954 46 32 83 71 464 258 - 593 361
SNNPR 3,382 143 113 110 62 2,310 644 7 2,563 819
Tigray 1,165 23 15 128 53 815 131 18 966 199
Total 13,450
1,103 881
1,014 799 6,525 3,128 72 8,642 4,808
PW= Pregnant women
Figure 1: Trends in malaria diagnosis and treatment in PHSP-supported facilities
(January 2019 - March 2020)
2.2.3. Workplace Performance
The project provided technical support to 32 workplace facilities that are engaged in malaria
case management services and they have investigated a total of 27,649 workers for malaria

PAGE
\* MERGE
using blood film 21,200 (77%) and RDT 6,449 (23%) (Figure 2). Workplace facilities diagnosed
5,044 malaria cases making a parasite positivity rate of 18.2% and all received appropriate
treatment.
A total of 52 malaria cases were admitted for inpatient treatment, 41 in Oromia and 11 in
SNNPR. An additional 15 patients with severe malaria (14 from Gambella and 1 from SNNPR)
were referred to other hospital for inpatient treatment.
Figure 2: Malaria case identification and treatment in PPM-workplace clinics (January - March 2020)
2.2.4. Laboratory Services Related to Malaria
2.2.2.1 PHSP PROGRAM REVIEW AND TRANSITION WORKSHOP
PHSP organized a program review and transition workshop held in Dire Dawa and Afar.
Participants discussed challenges and shared recommendations for collaboration to sustain
public health programs run by private HFs after program transition and close out.
2.2.2.2 MALARIA EQA As depicted in Table 5, PHSP supported regional laboratories to conduct blinded rechecking
malaria microscopy EQA in 19 private health facilities in Afar, Amhara and Tigray regions. A total
of 524 slides were collected and rechecked by regional labs. Of the total slides collected, 505
slides were concordant with 96% of confidence. The EQA service coverage (12%) is low because
the larger regions (Amhara, Oromia, SNNPR, Tigrai) are not regularly preforming EQA for malaria
in both public and private facilities.

PAGE \*
MERGE
Table 5: Malaria blinded-rechecking performance on PPM-facilities (January - March 2020)
Region
PPM Malari
a sites
Sites with EQA
# EQA Slides
Collected
# Slides
Rejected
# Slides Recheck
ed
Result
# Concordant Slides
# Discorda
nt Slides
Concordance Rate (%)
Afar 15 7 192 0 192 179 13 93
Amhara 28 3 83 0 83 82 1 99
Beneshangul Gumuz
15 -
-
0 -
0 0
Dire Dawa 14 9 249 0 249 244 5 98
Gambella 11 0 -
0 -
0 0
Oromia 32 0 -
0 -
0 0
SNNP 18 0 -
0 -
0 0
Tigray 25 9 -
0 -
0 0
Total 158 19 154 0 524 505 19 96
2.2.2.3 TRAINING PROVIDED
● PHSP provided malaria microscopy training for 22 lab professionals (F=8, M=14) invited
from PPM Malaria sites in Afar, Amhara, Oromia and SNNP.
2.2.2.4 JOINT SUPPORTIVE SUPERVISION FINDINGS OF MALARIA LABORATORY
● PHSP conducted joint supportive supervision to 58 PPM malaria facilities. The
supervision findings of the laboratory section are summarized on Table 8.
2.2.2.5 VISITED SITES AND TRAINING
● From the visited PPM sites in the five regions only 54% of them have trained manpower
on malaria laboratory microscopy which shows the high turnover of trained staff. Though
gap-filling training and onsite mentoring are needed, with the current state of COVID-19
outbreak, PHSP will try to provide phone based support to the laboratory technicians
(Table 6).
Table 6: Number of malaria laboratory sites visited by region and training status

PAGE
\* MERGE
(January – March 2020)
Site Support and Training
All
Region
s
Afar Amhara
Benishan
gul
Gumuz
Dire
Dawa Oromia
# of Supported Sites 109 18 27 15 14 35
# Sites Visited 58 18 18 8 8 6
% of sites visited 53 100 67 53 57 17
Training
Total number of laboratory
professionals 69 19 32 14 0 4
Number of trained staffs on lab
malaria microscopy 37 13 16 6 0 2
% of trained staffs on lab malaria
microscopy 54 68 50 43 0 50
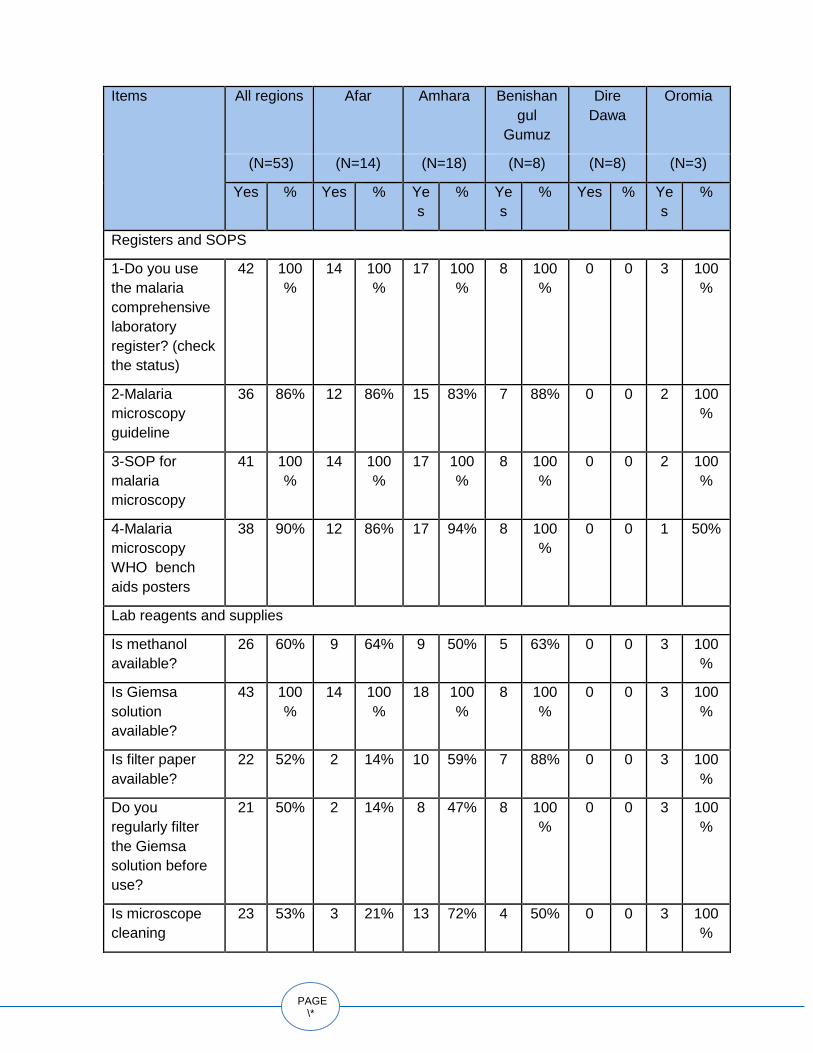
2.2.2.6 AVAILABILITY OF LAB DOCUMENTS AND SUPPLIES
● All visited PPM facilities had the comprehensive laboratory registration and were using it
properly to complete the data. Additionally, more than 85% of the facilities have one of
the provider support tools on their bench.
● 100% of the supervised facilities had Giemsa solution and 60% have methanol solution
which indicate progress on having crucial solutions for microscopy available. However,
only 50% of them filter the solution before usage, which might be due to the shortage of
filter paper in the market and public facilities.
● 93% of the visited facilities have slide boxes for slide storage and 95% of them have
frosted slides which both of them support for proper blind slide rechecking EQA (Table
7).
● Between 50% and 60% of the sites have microscope cleaning solution and filter paper,
respectively.
Table 7: Availability of Laboratory Commodities (January – March 2020)
PAGE \*
MERGE
Items
All regions Afar Amhara Benishan
gul
Gumuz
Dire
Dawa
Oromia
(N=53) (N=14) (N=18) (N=8) (N=8) (N=3)
Yes % Yes % Ye
s
% Ye
s
% Yes % Ye
s
%
Registers and SOPS
1-Do you use
the malaria
comprehensive
laboratory
register? (check
the status)
42 100
%
14 100
%
17 100
%
8 100
%
0 0 3 100
%
2-Malaria
microscopy
guideline
36 86% 12 86% 15 83% 7 88% 0 0 2 100
%
3-SOP for
malaria
microscopy
41 100
%
14 100
%
17 100
%
8 100
%
0 0 2 100
%
4-Malaria
microscopy
WHO bench
aids posters
38 90% 12 86% 17 94% 8 100
%
0 0 1 50%
Lab reagents and supplies
Is methanol
available?
26 60% 9 64% 9 50% 5 63% 0 0 3 100
%
Is Giemsa
solution
available?
43 100
%
14 100
%
18 100
%
8 100
%
0 0 3 100
%
Is filter paper
available?
22 52% 2 14% 10 59% 7 88% 0 0 3 100
%
Do you
regularly filter
the Giemsa
solution before
use?
21 50% 2 14% 8 47% 8 100
%
0 0 3 100
%
Is microscope
cleaning
23 53% 3 21% 13 72% 4 50% 0 0 3 100
%

PAGE
\* MERGE
solution
available?
Are frosted
slides
available?
41 95% 14 100
%
17 94% 7 88% 0 0 3 100
%
Is slides box
available?
40 93% 12 86% 17 94% 8 100
%
0 0 3 100
%
2.2.2.7 QUALITY ASSURANCE AND EQA PRACTICES
● 69% of the supervised facilities are storing slides for EQA and 63% of them use both
thick and thin film. This result is because the regional laboratories are not doing EQA
regularly which affects the motivation of the facilities to store slides (Table 8).
● Almost 100% of sites label reagents name, include the date of preparation and expiry
date and stored reagents away from the sun light
● Over 60 % of sites performed IQC and documented results
Table 8: Quality Assurance and EQA Practices (January – March 2020)
Quality
Assurance
All regions Afar Amhara Benishang
ul Gumuz
Oromia
(N=43) (N=14) (N=18) (N=8) (N=3)
Yes % Yes % Yes % Yes % Yes %
Do you store
slides for
rechecking?
29 69% 8 57% 12 67% 8 100
%
3 50%
Do you perform
both thick and thin
films?
27 63% 9 64% 9 50% 6 75% 3 100
%
Do you determine
parasite loads?
21 49% 7 50% 5 28% 6 75% 3 100
%
Are the reagents
labeled with its
name, date of
preparation
andexpiry date?
43 100
%
14 100
%
18 100
%
8 100
%
3 100
%

PAGE \*
MERGE
Are the reagents
stored away from
direct sunlight
and moisture in
lockable cabinet?
43 100
%
14 100
%
18 100
%
8 100
%
3 100
%
Have you ever
had interrupted
malaria laboratory
services due to
shortages of
reagents, supplies
and microscope
problem?
6 14% 0 0% 6 33% 0 0% 0 0%
Do you perform
IQC for stored or
new reagents
before use?
29 67% 7 50% 12 67% 8 100
%
2 67%
If yes, do you
document the
result?
19 66% 2 29% 9 75% 7 88% 1 50%
Do you perform
daily preventive
maintenance for
the microscope?
40 93% 14 100
%
15 83% 8 100
%
3 100
%
Have you been
involved in
malaria laboratory
EQA in the past 6
months?
13 30% 8 57% 5 28% 0 0% 0 0%
If yes to Qn. 20,
do you have
documented
feedback?
8 62% 8 100
%
0 0% 0 0
2.2.2.8 DISTRIBUTION OF MATERIALS
● PHSP distributed IQC and preventive maintenance logs for PPM malaria sites in Dire
Dawa and Gambella regions.
2.2.2.9 CHALLENGES AND MITIGATION ACTIVITIES
● Weak regional EQA for malaria. To improve EQAs PHSP discussed with the respective
regional laboratories and suggested doing at least one EQA every quarter and include
PPM facilities during their program.

PAGE
\* MERGE
● Some challenges remained from the past quarter, namely the high trained staff turnover
which prompts the need for gap-filling trainings and reinforcing provider support tools.
● Most sites do not perform thin blood film due to lack of methanol. PHSP discussed with
the facilities and suggested doing thin films by procuring methanol solution from the
market. The regional laboratories also agreed to provide the solution whenever it is in
stock.
● Lack of proper microscope cleaning solutions. PHSP informed sites to use other
recommended options to clean microscopes.
2.2.2.10 QUARTER THREE ACTIVITIES
● Provide remote (phone based) technical support to facilities
● Submit performance report of facilities to regional labs so that facilities with poor quality
can be supported to improve the quality of malaria or TB diagnosis.
● Prepare End of Project Report summarizing PHSP strategies, lessons learned and best
practices.

PAGE \*
MERGE
2.3 Private Health Care System Strengthened
2.3.1 Capacity Building
PHSP organized and provided a capacity building training on malaria case management to 38
trainees (by sex: 30 males and 8 females and by profession: 8 MDs, 10 HOs and 20 nurses) from
25 PPM-malaria health facilities. At the end of the training all trainees received the full packages
of the training materials in hard copies and 25 (66%) of them scored the minimum requirement
for certification which was a score of 70% and above.
The project also organized a one day clinical seminar for a total of 20 trainees, (by sex: 12
males and 8 females, by profession: 2 MDs, 4 HOs and 14 nurses) from 16 PPM-malaria health
facilities. Participants were trained on the new updates on malaria case management and how
to record cases using the laboratory comprehensive and malaria morbidity registers.
2.3.2 Supportive Supervision of Health Facilities and Providers
PHSP performed supportive supervision site visits to 58 PPM-health facilities in six regions to
evaluate the availability of provider support tools and anti-malaria drugs, oversee clinical
practices and case recording and reporting trends. A summary of the supportive supervisions
can be found in Table 9.
Table 9: Supportive supervision findings from 58 health facilities (January –March 2020)
Checked parameters ALL
Regio
ns Afar
Amhar
a BG Dire Dawa Oromia
% of Sites Visited from total supported
53%
100
% 67% 53% 57% 17%
General information
Providing the malaria care by trained staffs 72% 89% 83% 25% 63% 67%
Report malaria data weekly using PHEM 75% 22% 100% 100% 100% 100%
Report malaria data monthly using HMIS 98% 94% 100% 100% 100% 100%
Use the malaria morbidity and mortality register 86% 89% 89% 88% 63% 100%
Availability of provider support tools
Malaria diagnosis and treatment guideline 80% 59% 94% 100% 57% 100%
Malaria diagnosis and treatment training manual 91% 89% 100% 100% 57% 100%

PAGE
\* MERGE
Fever management algorithm poster 47% 72% 6% 100% 25% 60%
Dosing chart for AL, CQ, PQ and Quinine 82% 94% 89% 88% 50% 60%
Desktop reference
71%
100
% 61% 100% 25% 25%
Parenteral Artesunate poster 36% 50% 11% 100% 0% 25%
Case management practices
Order blood film/RDT for all patients with fever 95% 94% 100% 100% 86% 100%
Patients with P.F take the first dose of AL at OPD 49% 17% 56% 100% 33% 80%
Patients with P.falciparum infection receive SDPQ
76%
100
% 61% 100% 25% 100%
Patients with P.vivax receive radical cure
78%
100
% 67% 100% 14% 100%
Provide pre referral treatment 46% 38% 35% 100% 43% 25%
Provide anti-malaria drugs for uncomplicated blood
film negative febrile cases 20% 6% 50% 0% 0% 25%
Inpatient malaria case management
Facilities providing inpatient services for severe
malaria 63% 39% 78% 100% 50% 50%
Types of injections used for severe malaria
treatment
IV Artesunate 40% 14% 43% 50% 50% 50%
IM Artemether 54% 71% 50% 88% 0% 0%
IM/IV Quinine 17% 0% 14% 13% 25% 100%
Availability of the following anti-malarial drug in the facility
Adult AL doses 45% 50% 56% 13% 50% 25%s
Pediatric AL formulations 18% 12% 22% 0% 38% 25%
Chloroquine tablets 66% 78% 83% 75% 13% 25%
Chloroquine syrup 38% 44% 61% 25% 0% 0%
Quinine PO 7% 0% 17% 13% 0% 0%
Quinine IV 11% 0% 11% 13% 13% 50%
Artesunate 25% 6% 28% 50% 25% 50%
Artemether 41% 28% 61% 88% 0% 0%
Primaquine 46% 61% 44% 75% 0% 25%

PAGE \*
MERGE
Summary of Supportive Supervision Visits
2.3.2.1 SERVICE PROVISION BY TRAINED HEALTH WORKERS
● 72% of the supervised PPM-malaria facilities are providing malaria management
services by trained healthcare providers. This indicates there is a continous turnover of
trained staff as the coverage during last quarter was 78%.
2.3.2.2 AVAILABILITY OF PROVIDER SUPPORT TOOLS
● 80% and 71% of the supervised facilities had the recently published malaria case
management guideline and desktop reference respectively.
2.3.2.3 THE RECENT CLINICAL PRACTICE
● 100% of the PPM facilities are investigating all febrile patients using microscopy or RDT.
● The utilization of Primaquine for radical cure increased progressively from 62% in
Quarter One to 78% in Quarter Two. The utilization of Primaquine for gametocidal
clearance increased from 73% to 76% respectively.
● During the reporting period 20% of the supervised facilities were managing malaria
clinically which indicates the challenges due to high trained staff turnover.
● 43% of the supervised facilities referred severe malaria cases after giving Artesunate
injection as pre-referral treatment.
2.3.2.4 DATA RECORDING AND REPORTING SYSTEM
● 98% of the facilities are reporting cases monthly using the health management
information system (HMIS).
● 86% of the supervised facilities during this quarter are using the malaria morbidity
register to register cases.
2.3.2.5 AVAILABILITY OF ANTI-MALARIA DRUGS
● In this quarter the supply of AL, PQ and artesunate to the facilities is frequently
interrupted due to the national shortage of drugs. In the supervised facilities 45% had
AL, 66% had CQ, 25% had Artesunate injection and 46% Primaquine tablet.
2.3.2.6 MAJOR ACTIONS TAKEN DURING THE SUPERVISION
● PHPS technical teams provided training, clinical seminar, provision of provider support
tools, onsite, and phone-based briefing on the new updates to facilities who had no

PAGE
\* MERGE
trained provider and to providers who were not following national recommendations.
● PHSP technical team discussed with the federal and regional Ethiopian Pharmaceuticals
Supply Authority (EPSA) hubs and nearby government structures (health center,
Town/District Health Office) to resolve drug stockout by distributing the drugs to facilities
whenever the central EPSA transport the drugs to the regional EPSA hubs.
● Morbidity, laboratory register and the malaria case management guidelines were given
by PHSP to those sites who have finished the registers and lost the guidelines.
2.3.2 Supply Chain Management and Rational Drug Use Enhanced
● PHSP provided orientation on Logistic Management Information System (LMIS) to 38
malaria program focal persons in private facilities (8 Female and 30 Male) by integrating
with malaria case management training in Adama.
● PHSP conducted in-person and phone based supportive supervision to 58 health
facilities to monitor availability of drugs and logistics essential for malaria diagnosis and
treatment. The availability of drugs is described above in Table 9. As shown on the table
the overall availability of malaria tracer drugs in the supervised facilities demonstrate the
persistent shortage of drugs. This is due to the national level recurrent shortage of anti-
malaria drugs and delayed requests from facilities to respective suppliers. The project
has been facilitating the supply at central as well as regional EPSA hub levels. Currently,
there is a shortage of malaria treatment drugs especially at Gambella EPSA which the
project has been facilitating the supply through communication with regional EPSA and
catchment health centers. The project will continue to improve the availability when
available at EPSA, facilitate focal persons to make consumption based report and to
maintain the proper utilization of LMIS tools for the effective IPLS implementation
● While 75% of the facilities use RRF to request refill of their stocks of antimalarials from
EPSA or nearby public facility, only 55% update their bin cards to monitor transaction of
anti-malaria drugs.

PAGE \*
MERGE
2.4 Program Learning and Innovative Ventures Enhanced for the Private Health Sector
2.4.1 Operational Manuals to Increase Access to Anti-malaria Interventions in Gambella and Benshangul Gumuz
PHSP held advocacy discussions and consultative workshops in Gambella and BG regions and
drafted region specific operations manuals that will help the regions to improve access to
standardized malaria management and vector control services for refugees and MMWs. The
manuals have been reviewed by all stakeholders in the regions have been submitted to the
RHB management for review and approval. The manual is approved for implementation by
Benshangul Gumuz RH and is waiting for endorsement by the Gambella RHB.
The presence of these implementation manuals will facilitate the access for malaria diagnosis
and treatment by MMW and refugees in the regions and the lessons learned from these regions
are expected to be an input to develop a national policy in relation to MMWs and refugees.
2.4.2. Toolkit to Guide the Implementation and Provision of Temporary Malaria Clinics to Seasonal MMWs and IDPs
Based on the experiences from the temporary malaria clinics operation in Tigray, BG, Gambella
and Amhara regions, PHSP developed a toolkit to provide guidance on how regions or other
stakeholders can establish temporary malaria clinics to MMWs and also how the malaria
management services can be integrated with other programs (WASH, IMNCI, etc.) if needed.
The document can be used as a guiding tool on how to initiate and deliver malaria case
management to migrant and seasonal workers deployed to remote areas where there are no
public or private health facilities.
The toolkit describes the purpose and benefits of the temporary malaria clinics, how to
implement and set-up the clinics in remote areas, the communication system, the steps in
establishing the clinics, the possible challenges and solutions during the implementation and
operation of the clinics, orientation materials to the clinic providers and checklists to supervise
the clinics activity.
This toolkit will be introduced to the regions and other stakeholders in a one day consultative
workshop in Quarter Three.

PAGE
\* MERGE
2.4.3. Mass Community Awareness Creation Sessions on Malaria
Prevention and Treatment for Seasonal Migrant Workers
In collaboration with BG RHBs, PHSP developed leaflets in Amharic describing how malaria is
transmitted, its symptoms, diagnosis, treatment, prevention approaches to serve as health
education tools at the farm sites. Additionally, PHSP also prepared important awareness
messages to be released vial microphones at the camps’ departure and arrival areas of the
MMWs. These messages were updated from the radio messages which the RHB used to
broadcast via local FM radio. PHSP will be monitoring the entry of MMW following the minor
rainy season in April and May.
3-TRANSITIONING ACTIVITIES
3.1-Transition Workshops
PHSP conducted transition workshops in Afar region and Dire Dawa city administration with 48
participants. The objective of these workshops was to inform and prepare all stakeholders to
take over responsibility for support and activities related to all private health facilities involved in
malaria diagnosis and treatment. Private facilities and zonal /RHBs focal persons attended the
workshops.
During the workshops the participants agreed to sustain the advances up to date and maintain the
linkage created with the government system in providing the 32 PPM facilities with lab reagents
and drugs supply, malaria EQA, JSS, capacity buildings and integrate DHIS/2 into the private
facilities before the project phases out.
In Quarter Three, PHSP will do a post-transition follow up to monitor the sustainability of malaria
services in health facilities.
3.2 Post-transition Follow-up
3.2.1Post-transition Mentoring of PPM Facilities
In Quarter One, PHSP transitioned selected PPM facilities from the four larger regions to the
government system after conducting a transition workshop and reaching a consensus with
RHB/THO officials. In Quarter Two PHSP conducted a post transition follow up to 38 PPM facilities
(25 PPM in Amhara, 10 in Oromia and 3 in Tigray) with woreda malaria program managers with
the objective of monitoring the status of the transitioned PPM facilities and the performance of the
PPM facilities after the transition in maintaining the standard provision of the program activities.

PAGE \*
MERGE
Summary of findings:
● Oromia and Amhara regions had a training in malaria case management and nine
private health facilities (one from Amhara and eight from Oromia) participated in the
training (Table 10).
● All mentored facilities are reporting cases in accordance to the national protocol.
● After the transition 20 (53%) of the mentored facilities started or continued storing slides
for EQA and 12 (31%) of them participated in malaria microscopy EQA and only 7 (58%)
of them received feedback. This low storage of slides and participation in EQA is due to
the poor malaria EQA coverage both in Tigrai and Oromia regions.
● 18 (47%) of the mentored facilities had history of stock out after the transition and 14
(78%) of them reported their status to the nearby woreda/EPSA hub and only 5 (36%) of
them refilled their stock.
Actions taken:
● PHSP urged the PPM facilities to continue the reporting cases using HMIS/DHIS-2 and
storing slides for EQA and suggested improving malaria EQA by properly storing slides
and submitting timely requisitions of drugs in advance to prevent being out of stock.
Table 10: Summary of the post-transition mentoring visits in PPM-facilities
(January - March 2020)
S/N Indicators
Results from the total number
of facilities visited=38
1
The number of PPM facility who received a training organized by
RHB/THO after the transition
9
2
The number of PPM facilities who submitted data to the government
system properly
38
3 The number of facilities who store slides for EQA 20
4
The number of PPM facilities who participated in the recent EQA after
transition
12
5 The number of PPM facilities who received feedback of the last EQA. 7
6
The number of PPM facilities who are stock out for program drugs in
the past one month
18
7
The number of PPM facilities who reported their stock out to
RHB/THO/EPSA Hub
14
8 The number of PPM facilities who got refill of their stock out 5

PAGE
\* MERGE
9 The number of PPM facilities having expired drugs 3
A. Number of facilities who segregated the expired drugs 3
B. Number of facilities who transferred the drugs to RHB/THO
for disposal
0
10
The number of PPM facilities who received visit by RHB/THO for
supportive supervision
11
3.2.2 Post-transition Mentoring of RHBs/THO/EPSA Hubs and Regional
Laboratories
In Quarter One PHSP transitioned selected PPM facilities from the four big regions to the
government system after conducting a transition workshop and reaching a consensus with
RHB/THO officials. This quarter PHSP conducted a post transition mentoring of three regions and
15 THOs with the objective of monitoring the status of those government structures in maintaining
the linkage of the PPM facilities with the government system after the transition.
Summary of findings:
● Only seven government structures (RHBs and THOs) supported eight transitioned PPM
facilities in the past quarter and two regions organized a training and invited nine
participants from PPM health facilities.
● One region conducted annual review meetings however no representatives from PPM
were invited to the meeting.
● Twelve RL or THOs collected slides from 10 PPM facilities for EQA and seven facilities
received feedback from the EQA.
● 12 (67%) of the mentored EPSA hubs/THOs are refilling drugs to their catchment PPM
facilities.
● All mentored RHBs/THO are getting facilities performance as per the reporting protocol
(Table 11).
Actions taken:
● PHSP team appreciated the regions/THO/EPSA hub and RL who integrated the PPM
facilities into the government system during their capacity building program, microscopy
EQA, supplying drugs and collecting their data. However a discussion was held with
them to strengthen the linkage with the PPM facilities.

PAGE \*
MERGE
Table 11: Summary of the post-transition mentoring visits at RHB/THO/EPSA hubs and RLs (January – March 2020)
No. Indicators
N=18
1. Number of RHBs and THO who supported PPM facilities after the transitioning 7
2. Number of RHB/THO who conducted training after the transitioning 2
3. Number of private health facilities who participated in the training 9
4. Number of RHB/THO who conducted JSS after the transitioning 7
5. Number of PPM facilities supervised by the JSS 8
6.
Number of RHB/THO who conducted workshop/review meeting after the
transitioning 2
7. Number of PPM facilities invited to the workshop/review meeting 0
8.
Number of Regional laboratory/THO who collected slides for EQA after the
transitioning 12
9. Number of PPM facilities included in the slide collection 10
10.
Number of RL/THO who distributed previous quarter EQA feedback to PPM facilities 7
11.
Number of EPSA/THO who refilled program drugs as per the request of PPM
facilities 12
12. Number of THO/RHBs who received data from PPM facilities 18
4-COVID-19 PANDEMIC PREPAREDNESS ACTIVITIES
The COVID-19 pandemic has affected Ethiopia and it could have a devastating impact on the
health system, specially the malaria program since the clinical manifestations of both suspected
cases overlap and premature information shared in social media about the effect of chloroquine
phosphate in treating COVID related pneumonitis may lead to overconsumption, stock
out/shortages of the drug for the treatment of P.vivax malaria and development of unwanted
drug toxicity.
To combat the negative impacts on the malaria program and facilitate the proper preparedness
of the PPM facilities against COVID-19, the project is remotely supporting PPM facilities on the
following major points:
● Sensitize and inform RHBs/THO to include private providers during training/orientation
on COVID-19.

PAGE
\* MERGE
● Advocate to include the private sector facilities in training, capacity building including
provision of personal protective equipment (PPE).
● The PPM facilities are alerted to implement patient triaging and isolation, use personal
protective equipment, report suspected cases of COVID-19, and conduct health
education sessions to prevent the spread of the pandemic to their staff and their clients.
● Implement the PMI technical guidance in the context of COVID-19 pandemic.
● Encourage the PPM facilities to use chloroquine tablets only for patients with P.vivax
malaria and use PPE whenever they evaluate patients, especially patients with fever and
report WHO suspected cases of COVID-19 to the nearby task force.
5. CHALLENGES AND SOLUTIONS
● The pandemic of COVID-19 restricted PHSP’s ability to provide in-person site level
support and implement the different planned activities to improve the access of malaria
prevention and management to MMWs. To solve this gap PHSP is conducting phone-
based mentoring and discussions.
● Restriction of movement is hindering officers from supporting workplace clinics in
Gambella and from distributing drugs to the facilities (Mengesh and Godere).
● Delays in approving the PPM-malaria implementation guideline by the FMOH.
● Shortage and interrupted supply of the anti-malaria drugs specially artemether –
lumefantrine and Primaquine. To prevent further shortages PHSP continued its
advocacy at central and regional Ethiopian Pharmaceuticals Supply Agency (EPSA)
hubs to improve the supply system to PPM-HFs
● PPM-malaria sites are not participating in the malaria microscopy EQA in Amhara,
Tigrai, and Oromia regions, even though most of the PPM malaria sites are storing
slides for EQA. (Continued advocacy at Ethiopian Public Health Institute and regional
reference laboratories to regularly include the PPM-HFs for malaria microscopy EQA)
● High turnover of trained OPD clinicians and laboratory staff. To mitigate rapid human
resources turnover PHSP provided onsite orientation, clinical seminar, gap-filling
training, and provider support tools.
● Delays in approval of the newly developed operation manual by Gambella regional
health bureaus. PHSP held a discussion with Gambella regional health bureau heads to

PAGE \*
MERGE
activate the regional team to evaluate and approve the drafted region specific manual
and agreed with them to approve it with the coming two weeks.

PAGE
\* MERGE
3. MAJOR ACTIVITIES FOR YEAR FIVE , QUARTER THREE
The following activities are planned to be implemented in Quarter Three, however, all activities
are subject to change due to the coronavirus epidemic unfolding as well as GOE and USAID’s
guidelines.
● Advocate for the approval, printing and distribution of PPM-malaria implementation
guidelines.
● Participate in the national strategic plan development and advocate for inclusion of
private sector engagement in NSP
● Participate in preparation GF application for malaria
● Finalize the approval and start the implementation of the region specific operation
document to improve the access of malaria management and prevention services to
MMWs and refugees.
● Finalize and endorse the developed toolkit used to guide the implementation and
provision of temporary malaria clinics to seasonal MMWs and IDPs and conduct
regional trainings so regional and district health officials can plan and implement
mobile clinics without external support..
● Finalize the development of region specific community SBCC materials and prepare
them to create awareness on malaria prevention and treatment for seasonal MMWs.
● Strengthen the capturing of the MMW and refugee data in our PPM-malaria facilities
using the morbidity register.
● Advocate for the collection of migrant worker information on weekly PHEM reporting
forms.
● Prepare the End of Project report for malaria program
● Participate in TAC and TWG meetings and advocate for:
✔ Approval of PPM implementation guideline by the FMOH.
✔ Disaggregation of the private data at the Woreda level.
✔ The need of developing a guiding policy document to address the malaria issue of
MMWs.
✔ The need of starting a malaria laboratory EQA as quickly as possible.

PAGE \*
MERGE
✔ Consideration of the MMWs and refugees during the distribution of malaria
commodities to the regions where those populations are huge in number.
✔ Continue providing the technical support to FMOH and RHBs.
✔ Support and network the private facilities to the regional laboratories to conduct
malaria EQA.
✔ Conduct clinical mentoring and supervision to selected PPM-facilities.
✔ Follow the transition process and manage accordingly.

PAGE \*
MERG
ANNEX-A MALARIA PROGRAM ACTIVITY MATRIX, YEAR FIVE, QUARTER TWO; JANUARY –MARCH 2020
Indicator Indicator /output Planned
Achieved
1 Coordinate with BG and Gambella RHB to create region specific and consistent guidance about migrant worker access to public health posts/facilities
# of guideline 2 2
2 Participate in FMOH TAC meetings. # of times 2 2
3 Print and distribute malaria PPM-IG # of guidelines 300 0
4 Develop a mapping report # of copies 2 2
5 Establish 40 temporary malaria clinics # of clinics 40 21
6 Provide parasitological diagnostic services to 100% of suspected patients
Percentage 100 100
7 Provide malaria treatment according to the national guidelines for 100% of malaria patients in the facilities
Percentage 100 100
8 Strengthen the enrollment of PPM-malaria facilities to malaria microscopy EQA.
# of sites 158 26
9 Print and distribute monitoring and evaluation tools (Comprehensive Lab Register, Malaria Morbidity register, HMIS, PHEM reporting forms) to facilities
# of sites 163 163






























