Embed Size (px)
Citation preview

ch
January 2016 Volume 15 Issue 1
QuarterWatch™ 2015 Quarter 1 and 2 Report:Focus on a new sleep medication, changing opioid use,
and new diabetes medications The latest edition of ISMP’s QuarterWatch™ (see Box below) providesan overview of drug safety issues reflected in adverse drug events re-ported to the US Food and Drug Administration (FDA) in the first two
quarters of 2015 (the latest data available for research). The report is based on com-bined FDA MedWatch data, but trends focus on 2015 quarter 2 reports. Based onthese data, the report identifies:
Signals for the new sleep medication suvorexant (BELSOMRA)Changes in opioid use, specifically a decline in HYDROcodone exposure andan increase in exposure to higher potency opioids Update on new diabetes drugs that block the protein sodium-glucose cotrans-porter 2 (SGLT2)—canagliflozin (INVOKANA), dapagliflozin (FARXIGA), andempagliflozin (JARDIANCE)
Signals for suvorexantSleep medication targets newly discovered neurotransmitters. Suvorexant isa novel sleep medication prescribed for chronic insomnia, which affects 1 out of 3adults worldwide. The drug, first marketed in 2015, blocks the effects of two recentlydiscovered neurotransmitters called orexins that are active in the complex sleep-awake process. Orexin receptors receive wakefulness signals and interact with manyother neurotransmitters (e.g., histamine, DOPamine, norepinephrine, acetylcholine,serotonin).
Most sedative-hypnotics, such as zolpidem (AMBIEN) and ALPRAZolam (XANAX),target gamma-aminobutyric acid (GABA) receptors to enhance their depressant ef-fects on the central nervous system (CNS). Suvorexant blocks orexin receptors thatreceive wakefulness signals. An absence of all or most orexin-producing neuronshas been closely linked to narcolepsy, a condition leading to severe daytime sleepi-ness. The manufacturer of suvorexant, Merck, expected the new drug would helppeople sleep at night by blocking orexin receptors without the complications of im-pairing other elements of the CNS, as seen with sedative-hypnotic medications tar-geting GABA receptors.
U-500 insulin pen arriving soon. Wewere happy to learn that over the holidaysthe US Food and Drug Administration(FDA) approved Lilly’s application for a U-500 regular insulin pen (HUMULIN R U-500 KWIKPEN). U-500 insulin is indicatedfor patients with type 1 and type 2 diabeteswho need more than 200 units of insulinper day. The U-500 pen holds a 3 mL,1,500 unit insulin cartridge and is the samesize as other Lilly pens but dials in 5-unitincrements rather than 1-unit increments(Figure 1). The device has an aqua penbody to differentiate it from other insulinpens. Until now, U-500 insulin was onlyavailable in a vial, and since there is noU-500 syringe, it had to be administeredwith either a U-100 insulin syringe that re-quired a dose conversion to U-100 mark-ings, or a tuberculin (TB) syringe that re-quired conversion to volume markings.
Most medication errors with HumuLIN RU-500 in vials have been due to dosingconfusion when the dose was prescribedin units or volume corresponding to theU-100 syringe or TB syringe markings. It’simportant to mention that when switchingto the new pen, dose conversions are nolonger needed. The pen’s dose windowshows the number of units of HumuLIN RU-500 to be injected. The pen will then de-liver the proper volume that correspondsto the dose. Again, NO dose conversionis required. However, keep in mind thatpatients using U-500 insulin from a vial willstill communicate their dose in U-100 unitmarkings or volume, so you will need toverify the dose and syringe or device used
continued on page 2—SAFETY briefs >
continued on page 2—QuarterWatch >
Quarterwatchwa
What is QuarterWatch™?
QuarterWatch™ is an independent ISMP surveillance program that monitors adversedrug events reported to FDA by manufacturers, health professionals, and the public.The agency releases for research excerpts of all reports it receives into its adverseevent reporting system (FAERS). The goal of QuarterWatch™ is to identify signals thatmay represent important drug safety issues. The term signal means evidence judgedto be substantial enough to warrant publication but which requires further investigationto determine its frequency and establish a causal relationship to the suspect drug.
Figure 1. New HumuLIN R U-500 KwikPen dialsin 5-unit increments.

January 2016 Volume 15 Issue 1 Page 2
Clinical trials and FDA approval. During clinical trials, suvorexantdemonstrated a half-life of 12 hours, meaning many patients would stillhave a therapeutic effect upon awakening after 8 hours. Unlike many
other sleep medications, suvorexant also accumulated with repeated daily dosing.For example, after 7 days of administration, the half-life of 40 mg of suvorexant hadgrown from 12 to 17 hours in older men and to 20 hours in older women. Many pa-tients on a 40 mg dose might experience a therapeutic effect for the entire 24-hourperiod, potentially leading to daytime sleepiness. But the effects of a lower 10 mgdose would fall below the expected therapeutic range within a few hours of takingthe evening dose, potentially leading to early awakening.
Merck sought approval of the highest dose tested (40 mg), which showed the greatesteffect on total sleep time—an increase of 46 minutes (but only 23 minutes longerthan the placebo). The trials also demonstrated secondary benefits including a de-crease in the time to fall asleep and the number and duration of awakenings duringthe night. However, the clinical trials had limitations, including small numbers ofcarefully selected patients studied for short durations. The trials excluded patientstaking antidepressants, antipsychotics, stimulants for attention deficit hyperactivitydisorder (ADHD), mood stabilizers, and anxiolytics. More than 20% of the adult pop-ulation takes these psychoactive drugs. Thus, it was a challenge to draw valid con-clusions about what might happen when this new kind of sleeping medication witha different mechanism of action was marketed to large patient populations.
The FDA, concerned about potential impairment of next-day driving and alertness,insisted on a 10 mg initial dose, which Merck had abandoned after preliminarystudies showed marginal efficacy; it prolonged sleep by only 5 minutes (not statisti-cally significant) longer than the placebo. An optional increase to 20 mg was alsoapproved, which prolonged sleep by 23 minutes longer than the placebo.
Reported adverse events. Given this pre-approval trial data, it’s not surprisingthat, among the 1,016 adverse events reported during the first 2 quarters of 2015,the most frequent reports (42%) were associated with a lack of effect (e.g., “drug in-effective”), although there was no statistical difference between lower (10 mg) andhigher (20 mg) doses. The next largest group of adverse events involved sleep dis-turbances (32%), including nightmares, abnormal dreams, hallucinations, sleepparalysis, and sleep walking. Impaired alertness involving somnolence, headache,dizziness, fatigue, amnesia, memory impairment, or confusion, comprised 28% ofthe adverse event cases. A few case reports (n = 5) indicated the consequences ofimpairment, including traffic accidents, falls, and head injuries. Our evaluation didnot detect any relationship between a higher dose (greater than 10 mg) and morefrequent reports of impaired alertness.
Another group of patients (22%) described paradoxical reactions: instead of becomingsleepy, they reported agitation, anxiety, irritability, nervousness, tremors, restlesslegs syndrome, and muscle spasms. Many of these paradoxical effects have alsooccurred during withdrawal of a benzodiazepine sleep aid. Thus, it is conceivablethat some of these cases might be occurring because patients switched from benzo-diazepine sleep aids to suvorexant and experienced withdrawal symptoms from thebenzodiazepine. About 5% of the adverse event reports indicated depression, suicidalideation, and suicidal behaviors, although reports could include more than one ofthese terms. Numerous cardiac symptoms, including palpitations, chest pains, andother arrhythmias were also reported.
continued on page 3—QuarterWatch >
> QuarterWatch—continued from page 1
© 2016 ISMP. Reproduction of the newsletter or its content for use outside your facility, including republication of articles/excerpts or posting on a public-access website, is prohibited without written permission from ISMP.
at home. You can find a brief video andmore information about the new pen,which will be available in April, at:www.humulin.com/hcp-u-500.aspx. Notethat the 20 mL vial of U-500 insulin will re-main available, and the revised U-500package insert includes the use of bothU-500 vials and pens. Therefore, U-100and TB syringe conversion tables are in-cluded, which may give rise to some con-fusion. These tables are NOT to be asso-ciated with the pen dosage form. ISMPrecommends strongly considering usingthe U-500 pen as a way to eliminate doseconversion problems.
Effective and compassionate follow-up to an error. While using the originalprescription to verify a refill for the anti-depressant EFFEXOR XR (venlafaxine ex-tended release), a pharmacist discoveredthat the prescription had incorrectly beenfilled on the previous refill with 75 mg cap-sules instead of 150 mg capsules. Twomonths prior, the patient was started onEffexor XR 37.5 mg daily with instructionsto titrate up to 75 mg daily over the firstmonth. The patient was then to receive150 mg daily after the first month. Wewrote about an error caught when dis-pensing refills in our February 2011 issueand recommended to always verifyagainst the original prescription.
However, what stood out in this recentevent is the pharmacist’s persistence infollowing up with the prescriber and thepatient as well as his advocacy on behalfof the patient with the prescriber. Afterdiscovering the error, the pharmacist con-tacted the prescriber and was directedto move forward with the 150 mg strengthas originally prescribed. The pharmacistthen called the patient to inform her ofthe error. When assessing how the patientwas feeling given the error, he discoveredthat she in fact was feeling very well andwas planning to be away from home for acouple weeks. Given the patient’s currentcondition and travel plans, the pharmacistreached back out to the prescriber to rec-
cont’d from page 1
continued on page 3—SAFETY briefs >
Quarterwatchwa

January 2016 Volume 15 Issue 1 Page 3
Conclusion. Suvorexant is the first drug to affect a new kind of neuro-transmitter that interacts with many other neurotransmitters. Althoughapproved for long-term use, the drug was evaluated only in small num-
bers of patients in short duration trials of a few months. This means that tens ofthousands of patients will be exposed to a drug about which both scientific knowledgeand ongoing safety surveillance are limited. Specific safety concerns about suvorexantinclude whether the warnings against taking the drug with alcohol (CNS depressanteffects are additive) and not to drive or engage in any dangerous activity the nextday are realistic. In addition, little information exists about the extent of accumulationand other adverse effects with prolonged use.
Changes in Opioid UseHYDROcodone exposure decreases. For many years, HYDROcodone with acet-aminophen (VICODIN, LORTAB, others) has been the most widely used opioid,and also the most frequently dispensed outpatient prescription drug of any kind, ac-cording to data from IMS Health. Until August 2014, HYDROcodone was classifiedas a US Drug Enforcement Administration (DEA) Schedule III controlled substance.
Given its potential for abuse, the opioid was reclassified in 2014, after years of study,as a Schedule II controlled substance, which requires substantial, additional safe-guards associated with record-keeping, storage, and prescribing—no telephone pre-scriptions or refills are allowed, for example.
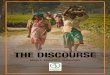
Because of the new prescribing and dispensing restrictions, HYDROcodone withacetaminophen has fallen from first to third place as the most widely prescribedtherapeutic drug—a decline of 8 million prescriptions from levels in 2011 (Figure 1,graph ). The decline in utilization is so substantial that it reduced overall usageacross the entire opioid drug class (Figure 1, graph ). Given that most illicit use ofopioids begins when individuals get the drug from family or friends, this substantialreduction in availability could have long-term benefits.
ommend that the patient be kept on Ef-fexor XR 75 mg. After further discussionwith the pharmacist and patient, the pre-scriber agreed to the pharmacist’s rec-ommendation. We would like to highlightthis pharmacist’s effective and compas-sionate response to the error as well hisadvocacy for his patient. We hope othersfollow his example. For recommendationson how to respond to an error, please referto the article entitled There seems to be amistake with my prescription in our No-vember 2014 issue.
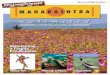
Label characteristic contributes to er-rors. The way the manufacturer’s strengthis oriented on a product container labelis an important safety consideration, es-pecially for pharmacists, pharmacy pur-chasers, and medication safety officers.The Apotex brand of ARIPiprazole tabletsis a case in point. Take a look at the bottlesin Figure 1. Bottle size, shape, label, andcontainer colors are all similar. Still, youwould certainly be able to identify whatthe medication is. It is the way the productstrength appears that is troubling. Sincemost drug containers are round, whenstrengths appear to the far right of the la-bel, they may easily be missed if the con-tainer is turned just slightly (Figure 1). Thedrug name may be readily visible but notthe strength. Confirmation bias could leadto a mix-up. In this case, the font size usedto express the strength is also muchsmaller than the font size used for the drugname, which may add to the confusion. Apharmacist told us that he recently picked
cont’d from page 2> QuarterWatch—continued from page 2
continued on page 4—QuarterWatch >
continued on page 4—SAFETY briefs >Figure 1. Opioid prescription trends, 2008-2015 Q2
Quarterwatchwa
A
A
B
B
C D
Figure 1. Strength may easily be missed if thebottle is slightly turned to the right.

January 2016 Volume 15 Issue 1 Page 4
OxyCODONE exposure increases. On the other hand, higher potencyoxyCODONE (OXYCONTIN, others) prescriptions, alone or in combinationwith acetaminophen (PERCOCET, others), have continued to increase
steadily. From 2008 through the first quarter of 2015, exposure to oxyCODONE alonenearly doubled, from 3.4 million to 6.2 million prescriptions per calendar quarter. AlthoughoxyCODONEprescription numbers are only one-third of those of HYDROcodone prod-ucts, oxyCODONEaccounted for more than twice as many overdose cases in emergencydepartments, according to the Drug Abuse Warning Network (DAWN). Thus, oxy-CODONE use has been a target of many regulatory policies including abuse-resistantformulations of extended-release oxyCODONE, a risk management program, strength-ened warnings for long-acting opioids, and physician education to urge compliancewith prescribing instructions.
Growth most rapid for high-potency opioids used to treat dependence.Themost rapidly growing group of prescribed opioids are long-acting, higher potency drugsincluding methadone and buprenorphine, which are used for the treatment of depend-ence and are intended to block withdrawal effects without producing euphoric moodchanges. Products with buprenorphine were the fastest growing among the 13 mostfrequently prescribed opioids—an increase of 67% since early 2011 to reach 3 millionprescriptions in the second quarter of 2015. These data do not show whether the increasereflects greater numbers of patients with opioid addiction, a higher rate of addictiontreatment, or both.
Growth with low-potency opioids. Low-potency opioid use–primarily cough med-ications–also grew moderately. The saw-tooth pattern in Figure 1 (graph on page 3)indicates seasonal use during the winter quarters.
Conclusion. Our analysis shows that additional DEA restrictions on the most widelyused opioid—HYDROcodone with acetaminophen—greatly reduced exposure to thedrug. Less reassuring was the steady increase in the use of higher potency opioids(Figure 1, graph on page 3) such as oxyCODONE. Therapeutic drugs containingopioids have been a major safety problem for more than a century. The Centers forDisease Control and Prevention (CDC) reported 18,893 overdose deaths in 2014 from licitand illicit use of opioids, a 14% increase from the previous year, emphasizing again thepublic health risks of these drugs. The sheer numbers rank it among the most importantcauses of accidental death. By comparison, other deaths in 2013 included 19,974 homicidesand 35,369 motor vehicle accident deaths. Controlling the use of opioids is greatly com-plicated by the lack of alternatives for treating moderate to severe pain, and the widespreadneed for this treatment. Managing the risks of a product that has substantial hazards butneeds to be widely available for legitimate use is a safety challenge of the first magnitude.
Update on new diabetes drugsRapid growth of new diabetes drugs. Both prescription volume and adverse drugevent reports are increasing rapidly for canagliflozin (Invokana), dapagliflozin (Farxiga),and empagliflozin (Jardiance). These medications belong to a new class of drugs used fortreating type 2 diabetes that blocks the SGLT2 protein, which binds to sugar and transportsit back into circulation. The drugs lower blood sugar by causing the kidneys to excretesome of the glucose rather than returning it to circulation. Despite limited long-term dataon safety and benefits, these new drugs have moved rapidly into widespread clinical use.Canagliflozin, approved in 2013, reached 1.1 million dispensed outpatient prescriptions inthe second quarter of 2015 according to data from IMS Health, followed by dapagliflozinwith 411,000 and empagliflozin with 136,000, both approved in 2015.
> QuarterWatch—continued from page 3
1-week “ROTATION” at ISMPA couple more seats are available in ourweeklong ISMP Practitioner in ResidenceProgram scheduled from February 29 toMarch 4, 2016, at ISMP’s office in subur-ban Philadelphia, PA. The rigorous pro-gram provides healthcare professionalswho have medication safety responsibili-ties with a unique opportunity to workclosely with ISMP staff using our concep-tual model for identifying and controllingmedication risks. For details, visit:www.ismp.org/consult/practitioner.asp.
ISMP Fellowships availableISMP is now accepting applications forthe 2016-2017 yearlong Fellowships. Fordetails, please visit our website at:www.ismp.org/profdevelopment/ or sendan email to: [email protected].
up the wrong bottle and nearly dispensedthe wrong strength.
Sometimes graphic designers and review-ers view sample label print-outs on a flatsurface, without considering how the labelwill look when applied to a round con-tainer, or how the product will be storedand later used. When we checked labelgraphics from other US ARIPiprazolegeneric manufacturers, they all had thestrength either immediately following thedrug name on the same line or had thestrength centered immediately beneaththe drug name, as it should be. Whenthere’s a choice of brands for specificproducts, avoid labels that separate thedose/strength from the product name. Agood reference to check for container la-bel appearance is DailyMed, a serviceprovided by the US National Library ofMedicine (http://dailymed.nlm.nih.gov/dailymed/index.cfm). Whenever possible,use barcode scanning when selectingproducts. Also, make sure labels are fac-ing forward when bottles are stored on ashelf.
cont’d from page 3
continued on page 5—QuarterWatch >
Quarterwatchwa
C
D

January 2016 Volume 15 Issue 1 Page 5
> QuarterWatch—continued from page 4Reported adverse events. Adverse drug event reports over the last 12months increased roughly in line with patient exposure, with 5,484 newcases for canagliflozin, 1,805 for dapagliflozin, and 455 for empagliflozin.
The most frequently reported side effects of all three drugs are genital fungal or bac-terial infections. For canagliflozin, 1,464 infection cases (27% of all cases) were re-ported in 12 months; 379 (21%) for dapagliflozin, and 93 cases (20%) for empagliflozin.While these infections are normally treatable and occur frequently without SGLT2inhibitor drug treatment, the relative risk in clinical trials was 3- to 4-fold. The presenceof glucose in the urine and bladder creates a favorable environment for infections,and FDA also warned of bacterial infections that spread to the urine or kidneys withpotentially life-threatening consequences. In December 2015, FDA warned that ithad identified 19 cases of urosepsis or kidney infections, all of which required hos-pitalization, including two that required hemodialysis because of acute kidney failure.
We also observed increasing numbers of reports of metabolic acidosis–a potentiallylife-threatening disorder not understood prior to approval that has been the focus oftwo FDA Drug Safety Communications. In its May 2015 communication, the FDAidentified 20 cases. In a December 2015 update, the agency identified 73 cases. Ourmost recent adverse event data identifies many additional possible cases, includinga total 168 cases for canagliflozin, 80 cases for dapagliflozin, and 12 cases for em-pagliflozin. Because it is not known how many cases go unreported, it is not possibleto estimate the incidence of this adverse effect.
Conclusion.There are reasons to ask whether many of the mechanisms for loweringblood sugar still make sense biologically. The earliest oral diabetes medications–sulfonylureas–work by stimulating the pancreas to secrete more insulin. But is thisa good idea in patients whose insulin-secreting cells are already impaired? A secondgroup of agents–thiazolidinediones–lower blood sugar by inducing fat cells toabsorb more circulating glucose. But is it a good idea in mostly obese patients toinduce their fat cells to absorb more sugar, thereby causing additional weight gain?Similar questions could be asked about this new class of drugs—SGLT2 inhibitorsthat cause some of the circulating glucose to flow into the bladder and urinarytract, which normally do not have substantial glucose concentrations.
The rapid market uptake of SGLT2 inhibitors brings new uncertainties about the effectsof treatment on the health of patients with type 2 diabetes. Postmarket surveillancedata indicate thousands of cases of genital fungal and bacterial infections, mostly inwomen, mirroring the results of clinical trials (11% of women and 4% of men). To thesewell-characterized risks are added many fewer but more severe cases of metabolicacidosis and other adverse effects on the kidneys. Whether the long-term clinical ben-efits of these drugs outweigh the increasing evidence of their risks remains uncertain.
The full QuarterWatch™ report with references can be viewed at: www.ismp.org/quarterwatch/default.aspx.
If you would like to subscribe to this newsletter, visit: www.ismp.org/sc?id=386
ISMP Medication Safety Alert! Community/Ambulatory Care (ISSN 1550-6290) © 2016 Institute for Safe Medication Practices(ISMP). Subscribers are granted permission to redistribute the newsletter or reproduce its contents within their practice site or facilityonly. Other reproduction, including posting on a public-access website, is prohibited without written permission from ISMP. This is a peerreviewed publication.
Report medication and vaccine errors to ISMP: Call 1-800-FAIL-SAF(E), or visit www.ismp.org/MERP or www.ismp.org/VERP. ISMPguarantees the confidentiality of information received and respects the reporters’ wishes regarding the level of detail included in publications.
ismp.org consumermedsafety.org twitter.com/ISMP1 facebook.com/ismp1 medsafetyofficer.org
Editors: Michael Gaunt, PharmD; Michael Cohen, RPh, MS, ScD (hon), DPS (hon); Judy Smetzer, BSN, RN, FISMP; Ann Shastay, MSN, RN, AOCN. ISMP, 200 LakesideDrive, Suite 200, Horsham, PA 19044. Email: [email protected]; Tel: 215-947-7797; Fax: 215-914-1492.
Quarterwatchwa
Rooting out errors in your community pharmacy
There is a need for every communitypharmacy to find a way to identifyand control risk in order to prevent
or mitigate harm from errors. One way toassist in this process is to conduct a thor-ough root cause analysis following anevent or after a close call of what couldhave been a serious event. Identifyingroot causes during an investigation of amedication error adds considerable valueby pointing out significant underlying andfundamental systemic conditions that in-crease the risk of adverse events. Thekeys to success of the process are thequality of the information collected in thereports, the careful analysis of the infor-mation, and the subsequent actions takento improve the system and prevent harm.
The Root Cause Analysis Workbook forCommunity/Ambulatory Pharmacy (www.ismp.org/tools/rca/) provides communitypharmacies with a coordinated set oftools designed to meet regulatory require-ments in the full investigation of thecauses of a sentinel event—an unex-pected occurrence involving death or se-rious physical or psychological injury orrisk thereof—and identify and implementeffective strategies to prevent this or asimilar occurrence. The RCA workbookis designed to help community pharma-cies take a process-driven, system-basedapproach to address this critical issue.
To aid pharmacies, the RCA workbookcontains sample forms that can be used.Each of these forms is also available sep-arately with each column/field electroni-cally fillable so you can easily use themto record and save your findings.

ISMP MedicationSafetyAlert!ÒCommunity/Ambulatory Care Edition
ACAA 1January 2016
Issue Problem Recommendation Organization Assessment Action Required/Assignment DateCompleted
Severe harm and death associated with medication errors and drug-drug interactions with low-dose oral methotrexate
10/15 One harmful and two fatal errors with low-doseoral methotrexate have been reported. Two ofthe patients who suffered severe toxic eventswere taking no more than 20 mg ofmethotrexate per week. Incidents occurred dueto a combination of baseline patient riskfactors (renal dysfunction, hypoalbuminemia),drug-drug interactions (amoxicillin, lefluno-mide), and medication errors (pharmacylabeling error led to daily use).
Use a weekly dosage regimen default whenoral methotrexate orders are entered; requirea hard stop verification of an appropriateoncologic reason for daily orders; and educatepatients, including reminding patients thattaking extra doses is dangerous, and providingthem with a free ISMP handout (www.ismp.org/sc?id=316). Employ drug-drug and drug-disease interaction screening and resolvealerts with prescribers. Screen patients forrisk factors and obtain baseline and periodiclab studies.
Ribavirin and riboflavin mix-ups
10/15 A pharmacist intercepted prescribing mix-upswith riboflavin (vitamin B2) and ribavirin. Theprescribers intended to order riboflavin 200 mgbut incorrectly prescribed ribavirin. Both prod-ucts have names that sound and look similarand start with “rib.” There is also an overlapbetween the 200 mg dosage strength of rib-avirin and the 200 mg dose of riboflavin. Someinformation systems may only list riboflavin byits alternative name, vitamin B2. If a prescriberattempts to find riboflavin by typing the firstthree letters, only ribavirin might appear.
Prescribers should include the purpose of themedication with the prescription as most look-and sound-alike name pairs have differentindications. Also, including “vitamin B2” in theprescription can help pharmacists and otherpractitioners correctly identify the intendedmedication. Pharmacists should confirm adiagnosis of hepatitis C for any patient takingribavirin and educate patients on new pre-scriptions. Consider adding this name pair toyour internal list of look- and sound-alike drugnames.
Don’t cover manufacturer’s barcode
11/15 XARELTO (rivaroxaban) 10 mg was dispensedinstead of VESICARE (solifenacin succinate)10 mg. The barcode on the manufacturer’slabel was covered by a pharmacy-applied labeland was not available to be scanned during thechecking procedure.
Ensure stickers, labels, or markings do notobscure the manufacturer’s barcode. Reviewinventories periodically to check that manufac-turer’s barcodes are not covered. Review com-pliance with barcode scanning to ensure staffcomplies with this safety step.
ISMPAmbulatoryCare ActionAgendaOne of the most important ways to prevent medication errors is to learn about problems that have occurred in other organizations and to use that information to prevent similar problems at your practice site. To
promote such a process, the following selected agenda items have been prepared for you and your staff to stimulate discussion and collaborative action to reduce the risk of medication errors. These agenda topics appearedin the ISMP Medication Safety Alert! Community/Ambulatory Care Edition between September 2015 and December 2015. Each item includes a brief description of the medication safety problem, recommendations to reducethe risk of errors, and the issue to locate additional information. The Action Agenda is also available for download in a Word format at: www.ismp.org/Newsletters/ambulatory/actionagenda.asp. To learn how to use the ISMPAmbulatory Care Action Agenda at your practice site, visit www.ismp.org/newsletters/ambulatory/How_To_Use_AA.asp.
Key: — ISMP high-alert medication
September-December 2015
©2016 IS
MP

ISMP MedicationSafetyAlert!ÒCommunity/Ambulatory Care Edition
ACAA 2January 2016
September-December 2015
©2016 IS
MP
ISMPAmbulatoryCare ActionAgendaIssue Problem Recommendation Organization Assessment Action Required/Assignment Date
Completed
Keep children safe from accidental medication poisonings
11/15 In the US, approximately 60,000 young childrenare brought to the emergency departmenteach year for accidental medication poisonings.Most medication poisonings happen in thehome. Leaving prescription and over-the-counter (OTC) medications as well as dietarysupplements, including those brought into thehome by visiting friends and family, withinreach of children is a predominant risk associ-ated with medication poisonings.
Avoid the use of dual-purpose prescriptioncontainer caps that can serve as a child-resis-tant cap but can be flipped over for use as anon-child-resistant cap. Remind patients,parents, and caregivers to keep all medica-tions and vitamins up and away and out of achild’s reach and sight. Encourage patients tofollow the recommendations at www.upandaway.org and to program the phone numberto the Poison Help Line (1-800-222-1222) intotheir cell phones so they have ready access inthe event of an emergency.
Human and animal medications may lead to drug name mix-ups
09/15 There is a potential for injury to animals due toconfusion between human and animal drugsthat have look- or sound-alike names.Recently, a dog mistakenly received the humanantidepressant SINEQUAN (doxepin) insteadof the prescribed animal antibiotic ZENIQUIN(marbofloxacin). The dog became ill 24 hoursafter being administered doxepin.
Alert colleagues to the possibility of look- andsound-alike names for human and animalproducts. Consider configuring product selec-tion screens so look-alike drug names are notlisted consecutively. When possible add ascreen or a notes field to provide an alert onpossible look-alike or sound-alike drug names.Pharmacies should ask for the spelling of thedrug name, if receiving the prescription orally,and then read back the order to theprescriber. At the time of dispensing, advisethe owner to call the veterinarian with anyquestions. Call the veterinarian for clarificationof the order if needed.
HealthAlert! TraMADol in children
09/15 In children 17 years or younger there is a rarebut serious risk of slowed or difficultybreathing when taking traMADol. The risk maybe increased in children using traMADol aftersurgery to remove their tonsils and/oradenoids. After a single dose of traMADol a 5-year-old child in France experienced difficultybreathing and required hospitalization. WhiletraMADol is not US Food and DrugAdministration (FDA)-approved for use inchildren, data show it is being used “off-label”in the pediatric population.
Healthcare professionals should be aware ofthis risk and consider prescribing alternativeFDA-approved pain medicines for children.Educate parents and caregivers of childrentaking traMADol on the signs of an adverseevent including, slow or shallow breathing,difficult or noisy breathing, confusion, orunusual sleepiness; instruct them to seekimmediate medical attention if the childexperiences any of these symptoms.

ISMP MedicationSafetyAlert!ÒCommunity/Ambulatory Care Edition
ACAA 3January 2016
September-December 2015
©2016 IS
MP
ISMPAmbulatoryCare ActionAgendaIssue Problem Recommendation Organization Assessment Action Required/Assignment Date
Completed
Decades-long errors still occurring: hydrALAZINE and hydrOXYzine
11/15 ISMP continues to receive reports of mix-upsbetween the blood pressure medicationhydrALAZINE and the antihistaminehydrOXYzine. Recently, a communitypharmacy received a printed prescription forhydrOXYzine but mistakenly entered anddispensed hydrALAZINE. The patientpresented to the emergency department with ablood pressure of 105/57 mmHg, shortness ofbreath, and numbness in his extremities just 3hours after taking the incorrect medication.
Pharmacies should encourage prescribers toinclude the purpose of the medication on theprescription. Differentiate names (e.g., tallman letters, bolding, highlighting) oncomputer screens and storage shelves.Consider storing products with look-alikenames in different locations; use shelf stickersto help locate products that have been moved.Pharmacists should discuss new therapieswith patients to verify that the medication isappropriate to treat the patient’s condition.
ACTIVELLA (estradiol and norethindrone) strength confusion
09/15 Confusion may arise between the two dosagestrengths of Activella due to similar andoverlapping dosage strength numbers. It isavailable in 1 mg/0.5 mg and 0.5 mg/0.1 mgof estradiol and norethindrone respectively.Patients have received the lower strength bymistake.
Alert healthcare practitioners of the mix-ups.Reminders or alerts about the potential forerror should be included in prescriber andpharmacy computer systems. Highlighting thestrengths on the product may help to differ-entiate them. Patients should receive educa-tion about all of their medications.
Serious liver injury with Viekira Pak and Technivie
10/15 The US Food and Drug Administration (FDA)issued a warning that the hepatitis C treat-ments VIEKIRA PAK (dasabuvir, ombitasvir,paritaprevir, and ritonavir) and TECHNIVIE(ombitasvir, paritaprevir, and ritonavir) cancause serious liver injury, mostly in patientswith underlying advanced liver disease. FDAidentified cases of hepatic decompensationand liver failure in patients with liver cirrhosistaking these medications.
Closely monitor patients for signs andsymptoms of worsening liver disease.Educate patients to contact their physician orpharmacist immediately if they develop signsof liver injury (e.g., fatigue, weakness, loss ofappetite, nausea and vomiting, yellow discol-oration of the eyes or skin, or light-coloredstools). Visit www.fda.gov/Drugs/DrugSafety/ucm468634.htm for the complete FDA drugsafety communication.
Opioid mix-ups: HYDROcodone-acetaminophen and oxyCODONE-acetaminophen
11/15 A number of regulatory and product changesthat occurred years ago may still becontributing to mix-ups betweenHYDROcodone-acetaminophen andoxyCODONE-acetaminophen combinationproducts. For example, all approved opioid-acetaminophen combination products are nowlimited to 325 mg of acetaminophen or less.
Avoid storing these next to each other.Consider tall man letters, bolding, orhighlighting to differentiate the drug names.If the prescribed combination product is notavailable, the pharmacist should contact theprescriber. Review the prescription with thepatient at the point-of-sale to help preventmix-ups.