Embed Size (px)
Citation preview

And
January 1, 2020
The Health Care Plan of Jacksonville Police Officers and Fire Fighters
Health Insurance Trust IMPORTANT NOTICES:
Your identification (I.D.) card is a combination card to be presented for both health and prescription benefits.
Providers will send claims to ClaimsBridge HPN (see I.D. card). The address is listed on the back of the I.D.
card. Please be sure to present your I.D. card each time you visit a health provider or pharmacist.
The network for your Health Plan is the UF Health Direct Care Network. You may access a list of UF Health
Direct Care providers available at jpoffhit.claimsbridge.com. This network will provide greater discounts for
health services when utilizing UF Health Direct Care Providers.
The prescription benefit is through Magellan RX Management. If you require a prescription and the pharmacy
is unsuccessful with the transaction, ask the pharmacy to call INTEGRA for verification of benefits.
INTEGRA’s toll-free number, 1-800-959-3518 and is also located on the back of the I.D. card. Mail order is
also part of the prescription benefit thru Magellan RX Management. See your plan sheet for more information,
contact your employer or visit the Magellan RX Management website at https://www.magellanrx.com.
HIPAA’s privacy rules require that you be provided with a “notice of privacy practices,” stating how the health
plan is permitted to use or disclose protected health information. A notice of privacy practice is in your plan
document, and available on the INTEGRA website, www.integratpa.com. A printed copy is available at your
request from your employer or by contacting INTEGRA Administrative Group, Inc. If you have questions about the health or prescription benefit plans, please contact INTEGRA.
INTEGRA’s Customer Service Department will be happy to assist you. We encourage you to visit INTEGRA’s
website and register for access to your personal claims data and plan information. INTEGRA’s website
provides links to your PPO Network and to “Healthwise,” a current health news publication. This and much
more is available to you at the web address below.
110 South Shipley Street
Seaford DE 19973
Phone: 302-629-3518
Toll Free: 800-959-3518
Claims Fax: 302-629-8600
Customer Service Fax: 302-629-8416
Customer Service Hours:
8:30 – 6:00 Monday thru Thursday
8:30 – 4:30 Friday
After Hours Call Center is available
www.integratpa.com
1
JACKSONVILLE POLICE OFFICERS AND FIRE FIGHTERS
HEALTH INSURANCE TRUST
2020 PLAN YEAR
IMPORTANT WEB ADDRESSES
& PHONE NUMBERS
https://www.integratpa.com
- Customer Service 1-800-959-3518
- Personal Medical Information - Links to UF Health Direct Care Network, Healthwise, and More
https://mbaileygroup.com
- Tiney Rahilly, PHR
1200 Plantation Drive S, Suite 210, St. Augustine FL 32080
(904) 417-6006; FAX: (904) 461-1775
jpoffhit.claimsbridge.com
- UF Health Direct Care Network Service Providers and Hospitals 1-888-960-7809
https://www.magellanrx.com
-Prescription Benefit Manager, Mail Order Service/Home Delivery, Specialty Pharmacy
-Customer Service 1-800-424-5973 (Prompt #1 for Member)
https://www.valenzhealth.com
- Pre-Certifications: 1-877-608-2200, Option # 1
- Case Management: 1-877-608-2200, Option # 5
https://www.healthwise.org
- Medical Information Database
2
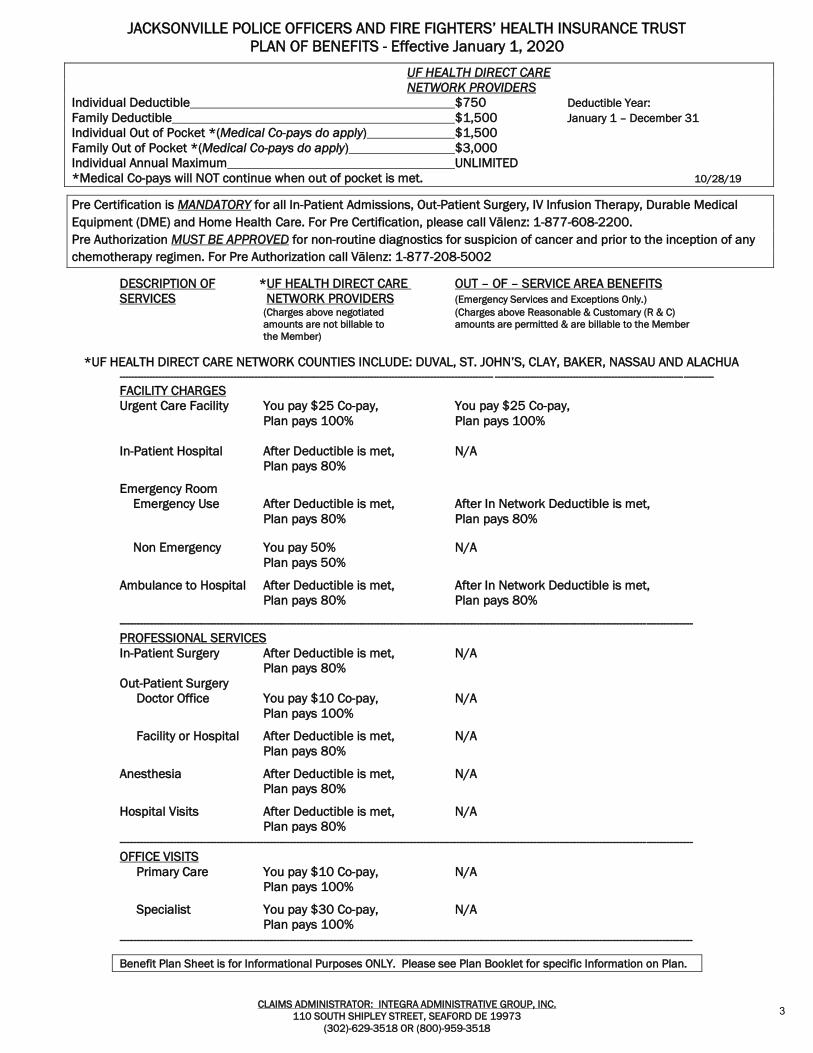
JACKSONVILLE POLICE OFFICERS AND FIRE FIGHTERS’ HEALTH INSURANCE TRUST
PLAN OF BENEFITS - Effective January 1, 2020
CLAIMS ADMINISTRATOR: INTEGRA ADMINISTRATIVE GROUP, INC.
110 SOUTH SHIPLEY STREET, SEAFORD DE 19973
(302)-629-3518 OR (800)-959-3518
UF HEALTH DIRECT CARE
NETWORK PROVIDERS
Individual Deductible $750 Deductible Year:
Family Deductible $1,500 January 1 – December 31
Individual Out of Pocket *(Medical Co-pays do apply) $1,500
Family Out of Pocket *(Medical Co-pays do apply) $3,000
Individual Annual Maximum UNLIMITED
*Medical Co-pays will NOT continue when out of pocket is met. 10/28/19
Pre Certification is MANDATORY for all In-Patient Admissions, Out-Patient Surgery, IV Infusion Therapy, Durable Medical
Equipment (DME) and Home Health Care. For Pre Certification, please call Vālenz: 1-877-608-2200.
Pre Authorization MUST BE APPROVED for non-routine diagnostics for suspicion of cancer and prior to the inception of any
chemotherapy regimen. For Pre Authorization call Vālenz: 1-877-208-5002
DESCRIPTION OF *UF HEALTH DIRECT CARE OUT – OF – SERVICE AREA BENEFITS
SERVICES NETWORK PROVIDERS (Emergency Services and Exceptions Only.) (Charges above negotiated (Charges above Reasonable & Customary (R & C)
amounts are not billable to amounts are permitted & are billable to the Member
the Member)
*UF HEALTH DIRECT CARE NETWORK COUNTIES INCLUDE: DUVAL, ST. JOHN’S, CLAY, BAKER, NASSAU AND ALACHUA
----------------------------------------------------------------------------------------------------------------------------- -------------------------------------------------------------------------
FACILITY CHARGES
Urgent Care Facility You pay $25 Co-pay, You pay $25 Co-pay,
Plan pays 100% Plan pays 100%
In-Patient Hospital After Deductible is met, N/A
Plan pays 80%
Emergency Room
Emergency Use After Deductible is met, After In Network Deductible is met,
Plan pays 80% Plan pays 80%
Non Emergency You pay 50% N/A
Plan pays 50%
Ambulance to Hospital After Deductible is met, After In Network Deductible is met,
Plan pays 80% Plan pays 80%
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------
PROFESSIONAL SERVICES
In-Patient Surgery After Deductible is met, N/A
Plan pays 80%
Out-Patient Surgery
Doctor Office You pay $10 Co-pay, N/A
Plan pays 100%
Facility or Hospital After Deductible is met, N/A
Plan pays 80%
Anesthesia After Deductible is met, N/A
Plan pays 80%
Hospital Visits After Deductible is met, N/A
Plan pays 80%
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------
OFFICE VISITS
Primary Care You pay $10 Co-pay, N/A
Plan pays 100%
Specialist You pay $30 Co-pay, N/A
Plan pays 100%
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Benefit Plan Sheet is for Informational Purposes ONLY. Please see Plan Booklet for specific Information on Plan.
3
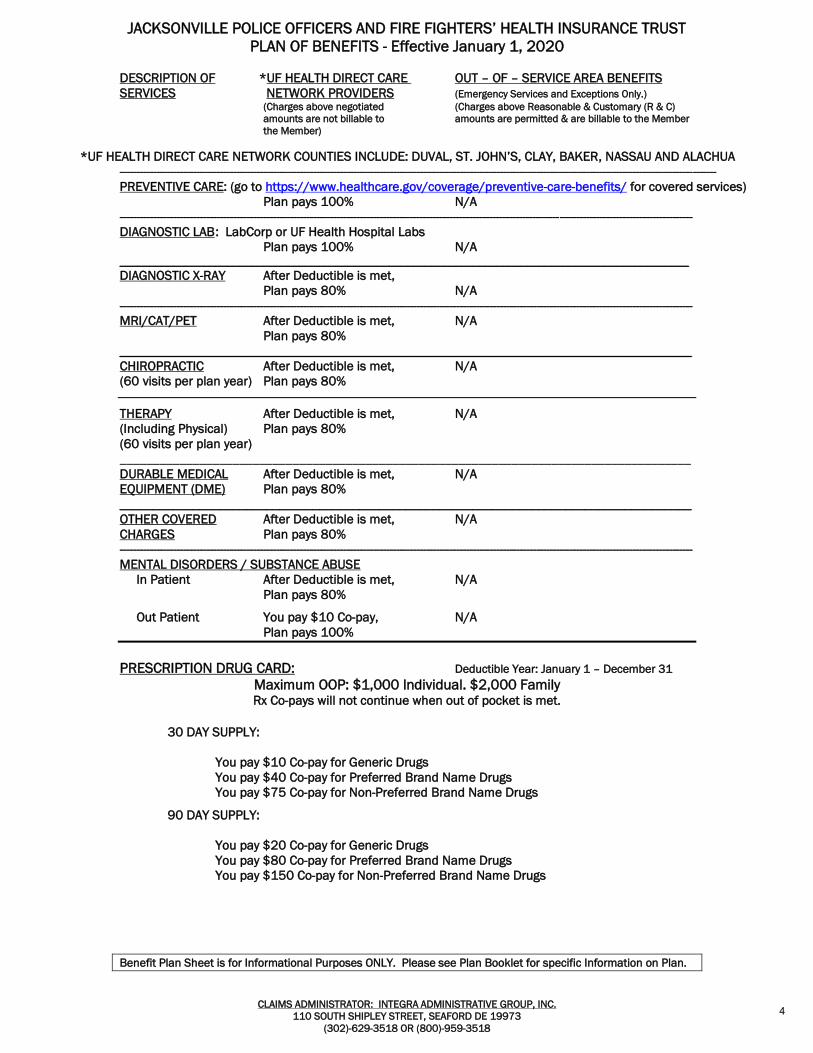
JACKSONVILLE POLICE OFFICERS AND FIRE FIGHTERS’ HEALTH INSURANCE TRUST
PLAN OF BENEFITS - Effective January 1, 2020
CLAIMS ADMINISTRATOR: INTEGRA ADMINISTRATIVE GROUP, INC.
110 SOUTH SHIPLEY STREET, SEAFORD DE 19973
(302)-629-3518 OR (800)-959-3518
DESCRIPTION OF *UF HEALTH DIRECT CARE OUT – OF – SERVICE AREA BENEFITS
SERVICES NETWORK PROVIDERS (Emergency Services and Exceptions Only.) (Charges above negotiated (Charges above Reasonable & Customary (R & C)
amounts are not billable to amounts are permitted & are billable to the Member
the Member)
*UF HEALTH DIRECT CARE NETWORK COUNTIES INCLUDE: DUVAL, ST. JOHN’S, CLAY, BAKER, NASSAU AND ALACHUA
-----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
PREVENTIVE CARE: (go to https://www.healthcare.gov/coverage/preventive-care-benefits/ for covered services)
Plan pays 100% N/A
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------
DIAGNOSTIC LAB : LabCorp or UF Health Hospital Labs
Plan pays 100% N/A _______________________________________________________________________________________________ DIAGNOSTIC X-RAY After Deductible is met,
Plan pays 80% N/A
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------
MRI/CAT/PET After Deductible is met, N/A
Plan pays 80%
______________________________________________________________________________________
CHIROPRACTIC After Deductible is met, N/A
(60 visits per plan year) Plan pays 80%
THERAPY After Deductible is met, N/A
(Including Physical) Plan pays 80%
(60 visits per plan year)
______________________________________________________________________________________
DURABLE MEDICAL After Deductible is met, N/A
EQUIPMENT (DME) Plan pays 80%
______________________________________________________________________________________
OTHER COVERED After Deductible is met, N/A
CHARGES Plan pays 80%
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------
MENTAL DISORDERS / SUBSTANCE ABUSE
In Patient After Deductible is met, N/A
Plan pays 80%
Out Patient You pay $10 Co-pay, N/A
Plan pays 100%
PRESCRIPTION DRUG CARD: Deductible Year: January 1 – December 31
Maximum OOP: $1,000 Individual. $2,000 Family Rx Co-pays will not continue when out of pocket is met.
30 DAY SUPPLY:
You pay $10 Co-pay for Generic Drugs
You pay $40 Co-pay for Preferred Brand Name Drugs
You pay $75 Co-pay for Non-Preferred Brand Name Drugs
90 DAY SUPPLY:
You pay $20 Co-pay for Generic Drugs
You pay $80 Co-pay for Preferred Brand Name Drugs
You pay $150 Co-pay for Non-Preferred Brand Name Drugs
Benefit Plan Sheet is for Informational Purposes ONLY. Please see Plan Booklet for specific Information on Plan.
4
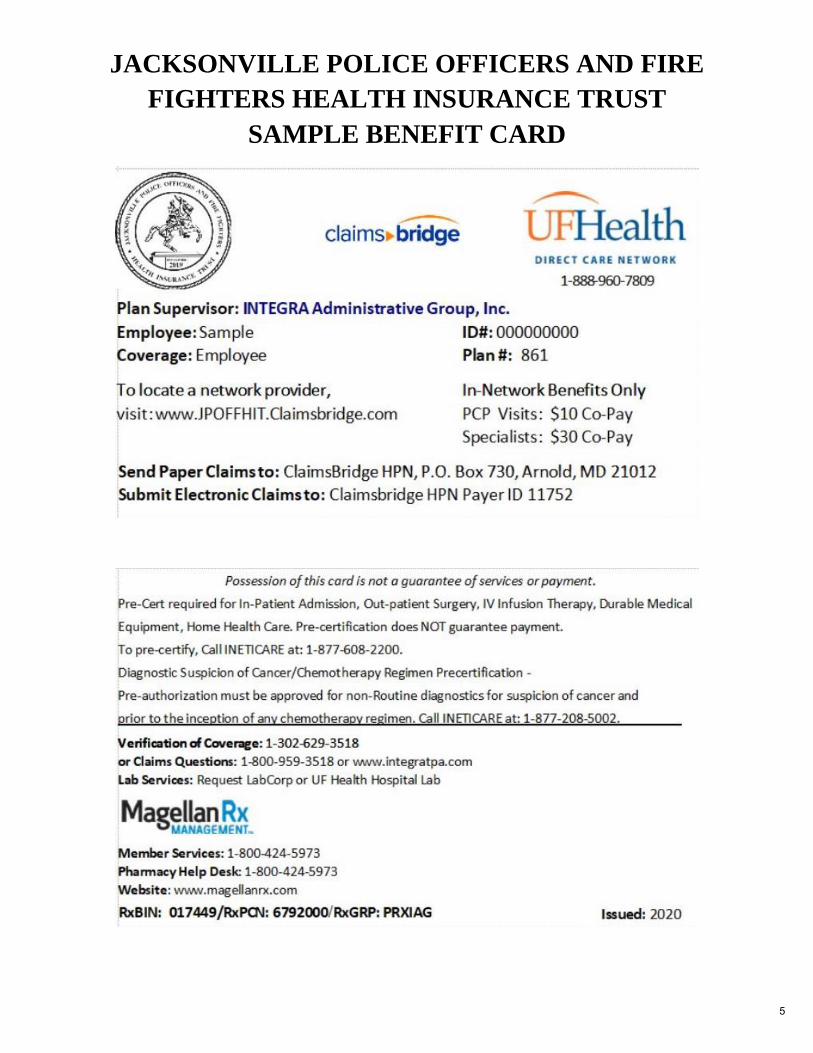
JACKSONVILLE POLICE OFFICERS AND FIRE
FIGHTERS HEALTH INSURANCE TRUST
SAMPLE BENEFIT CARD
5

INTEGRA Administrative Group, Inc.
Web Site Home Page
www.integratpa.com
Click Here to
Log in to the
Web Site
6
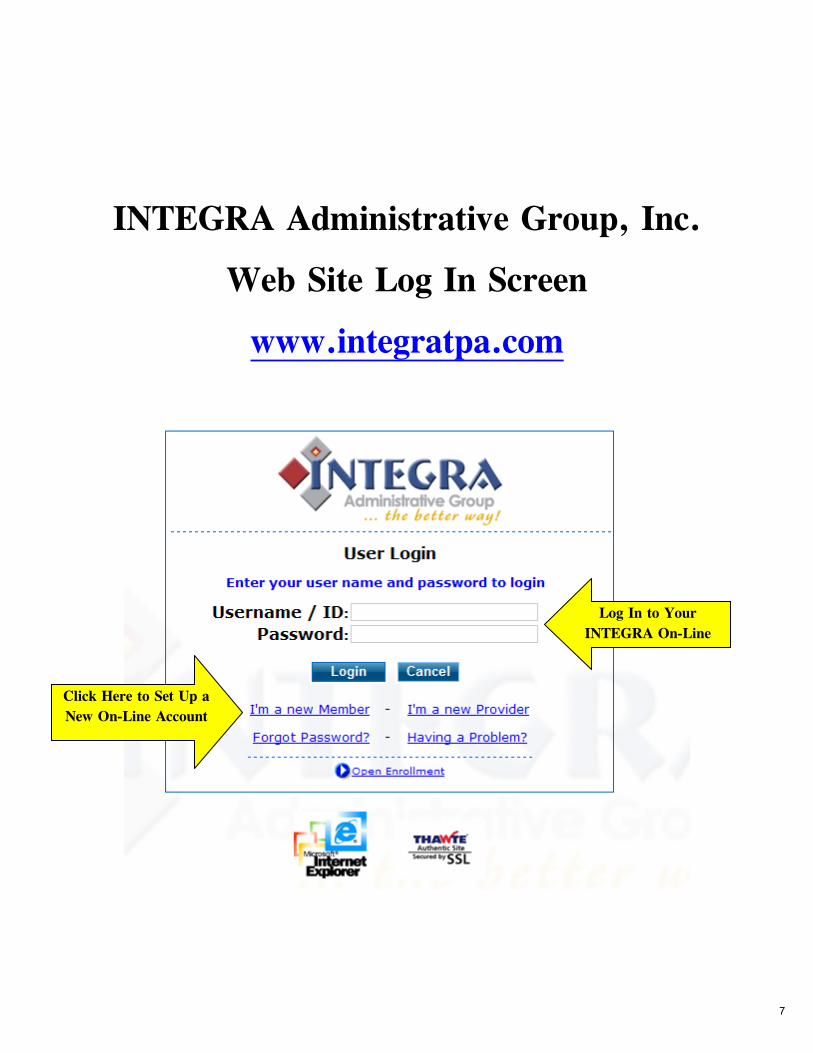
INTEGRA Administrative Group, Inc.
Web Site Log In Screen
www.integratpa.com
Click Here to Set Up a
New On-Line Account
Log In to Your
INTEGRA On-Line
Account Here
7

INTEGRA Administrative Group, Inc.
Web Site Home Page – Vendor Links
www.integratpa.com
Click on any of
these Vendors
to go directly to
their Specific
Websites
Magellan RX is your Mail Order Vendor.
magellanrx.com
8
magellanrx.com2019 Magellan Rx Management, LLC. All rights reserved. MRX0306_0919
Understanding Your Prescription Benefit Program
Your Prescription Benefit Plan through Magellan Rx ManagementMagellan Rx Management is your prescription benefit provider. Magellan Rx is dedicated to giving you the best service and resources to help you and your family make better healthcare decisions to lead more healthy, vibrant lives.
Using Your Prescription Drug Card at Retail PharmaciesYou will receive a prescription card from your employer. Please present your new prescription card along with your prescription to any of our 68,000+ retail pharmacies every time you fill your prescription. You can access a participating pharmacy list at www.magellanrx.com.
Home Delivery by Magellan Rx PharmacyWith home delivery, you may be able to receive up to a 90-day supply of your maintenance medication(s) at a lower price. Just ask your doctor to write two prescriptions: one for a 30-day supply to get you started (to be filled at your local pharmacy), and one for a 90-day supply, plus additional refills (to be filled by mail).
Next, you may either:
• Ask your doctor to e-prescribe or fax your prescription to 1.888.282.1349.
• Faxed prescriptions may only be sent by a doctor’s office and must include patient information and diagnosis.
• Please note: For prompt delivery, please provide your payment information by mailing in your completed order form or by calling 1.800.424.0472.
• Mail us your 90-day prescription and completed order form with payment to Magellan Rx Pharmacy, P.O. Box 620968, Orlando, FL 32862.
Prior Authorization/Step TherapyYour prescription benefit program may have a prior authorization or step therapy process for certain medications.
• Prior authorization is a requirement that your physician obtain approval from your health plan to prescribe a specific medication for you.
• Step therapy is when your prescription benefit requires you to try another medication prior to starting the medication your physician prescribed.
Providing you with the tools and resources to help you make better drug therapy decisions
Online Tools at www.magellanrx.com
Secure online connection, protecting your confidentiality and providing:
• Easy-to-use tools that allow you to view, refill, renew and transfer prescriptions
• Drug formulary and lookup tools
• Trusted drug and health condition information and education
• Real-time benefit information
• Access to view and download pharmacy claims
• A participating pharmacy locator tool
• Downloadable claim and home delivery forms
Questions?Please visit www.magellanrx.com or call customer service at 1.800.424.0472 to determine if any of your medications require prior authorization or are subject to step therapy requirements. Support is available 24 hours a day, 7 days a week.
9
magellanrx.com2020 Magellan Rx Management, LLC. All rights reserved. Standard_MRX0137_1019
ACCU-CHEKACCU-CHECK SOFTCLIXACCU-SOFT TOUCHacetaminophen-codeineacyclovirADVAIR DISKUSADVAIR HFAAIMOVIG*allopurinolALPHAGAN Palprazolamamitriptyline hclamlodipine besylateANDRODERM*ANORO ELLIPTAAPRISOaripiprazoleARNUITY ELLIPTAatenololatorvastatin calciumAZOPTBREO ELLIPTABRILINTAbupropion hcl srbupropion xlbuspirone hclBYDUREON/BCiseBYDUREON PENBYETTABYSTOLICBYVALSONcarvedilolcelecoxibCIPRODEXcitalopram hbrCLIMARA PROclonazepamclonidine hclclopidogrelCOLCRYSCOMBIGANCOMBIVENT
CREONcyclobenzaprine hclDEXILANT*dextroamphetamine- amphetamine erdiazepamDUAVEEduloxetine hclDYMISTAELIQUISEMBEDA*EMGALITY*EMVERM*ENDOMETRINENTRESTOescitalopram oxalateesomeprazole magnesiumestradiolEUCRISA*fenofibrateFLOVENT DISKFLOVENT HFAfluoxetine hclfluticasone propionateFREESTLYE LIBREfurosemidegabapentinglimepirideglipizide erGLUCAGONGLYXAMBIHUMALOGHUMALOG JRHUMALOG KWIKHUMALOG MIXHUMULINHUMULIN NHUMULIN Rhydrochlorothiazidehydrocodone-acetaminophenhydroxyzine hclibuprofen
INCRUSE ELLIPTAINVOKAMETINVOKAMET XRINVOKANAJANUMETJANUMET XRJANUVIAJARDIANCEJENTADUETO/XRlamotrigineLANTUSLANTUS SOLOSTARLEVEMIRlevothyroxine sodiumLINZESS*lisinoprillisinopril-hydrochlorothiazidelorazepamlosartan potassiumlosartan-hydrochlorothiazideLUMIGANmeloxicammetformin hclmetformin hcl ermethocarbamolmethotrexatemethylphenidate ermethylprednisolonemetoprolol succinatemetoprolol tartrateMIRVASOmontelukast sodiumMOVANTIK*MOXEZAMYRBETRIQnaproxenNARCANNATAZIANOVOFINENOVOFINE AUTNOVOFINE PLSNOVOTWISTNOVOLIN
NOVOLIN NNOVOLIN RNOVOLOGNOVOLOG MIXomeprazoleondansetron hclondansetron odtONETOUCHORILISSA*oxycodone hcloxycodone-acetaminophenOZEMPICpantoprazole sodiumparoxetine hclPAZEOpotassium chloridePRADAXApravastatin sodiumPREMARINPREMARIN VAGINAL CREAMPREMPHASEPREMPROPROAIR HFAPROAIR RESPICLICKPROCTOFOAMprogesteronePROLENSApropranolol hclPULMICORT FLEXHALERPYLERA*quetiapine fumarateQVARQVAR REDIHALERRANEXAranitidine hclRAPAFLORESTASIS MULTIDOSE*RESTASIS*RHOPRESSAROCKLATAN*rosuvastatin calciumSEREVENT DISKUSsertraline hcl
sildenafil*SIMBRINZAsimvastatinSOLIQUA*SOOLANTRASPIRIVA/RESPIMATspironolactoneSTIOLTOsumatriptan succinateSYMBICORTSYMPROIC*SYNJARDYSYNJARDY XRtamsulosin hcltestosterone cypionatetizanidine hcltopiramateTOUJEO MAX SOLOSTARTOUJEO SOLOSTARTRADJENTAtramadol hclTRAVATAN Ztrazodone hclTRELEGYTRESIBA FLEXtretinointriamcinolone acetonidetriamterene-hydrochlorothiazideTRULICITYvalacyclovirvenlafaxine hcl erVENTOLIN HFAVICTOZAVYVANSEwarfarin sodiumXARELTOXARELTO STARTER PACKXELPROSXIIDRA*ZENPEPzolpidem tartrateZUBSOLV*
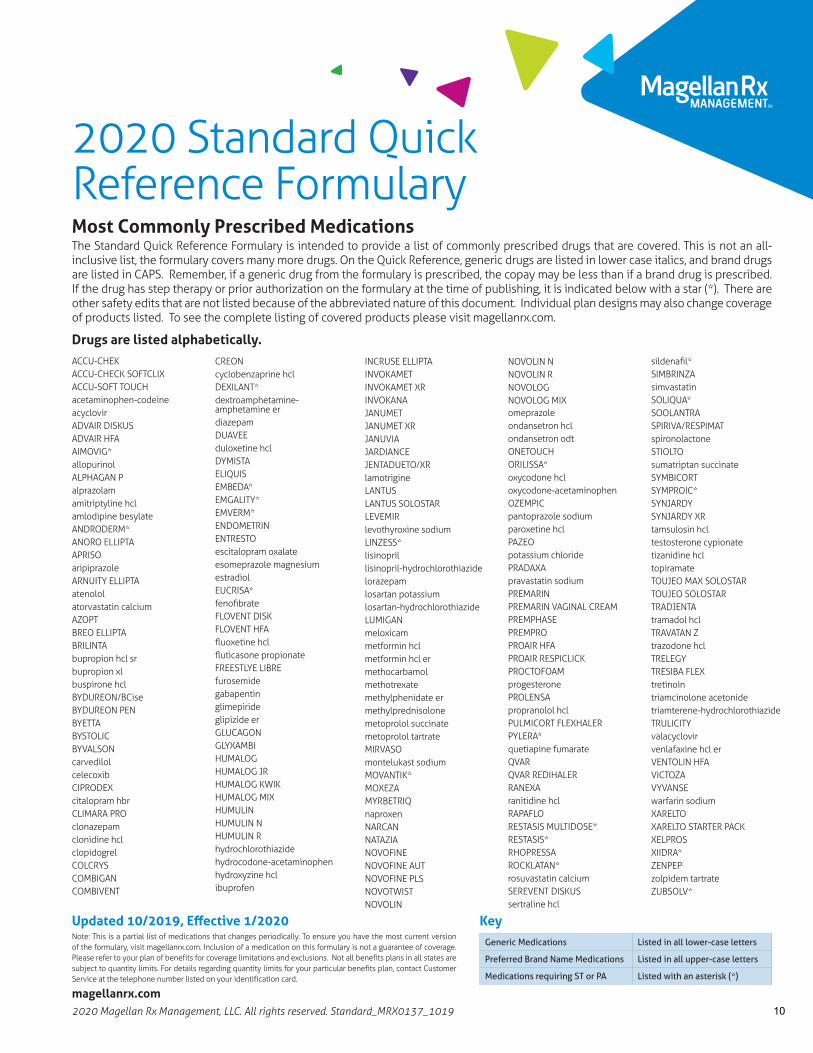
Generic Medications Listed in all lower-case letters
Preferred Brand Name Medications Listed in all upper-case letters
Medications requiring ST or PA Listed with an asterisk (*)
Note: This is a partial list of medications that changes periodically. To ensure you have the most current version of the formulary, visit magellanrx.com. Inclusion of a medication on this formulary is not a guarantee of coverage. Please refer to your plan of benefits for coverage limitations and exclusions. Not all benefits plans in all states are subject to quantity limits. For details regarding quantity limits for your particular benefits plan, contact Customer Service at the telephone number listed on your identification card.
Updated 10/2019, Effective 1/2020 Key
2020 Standard Quick Reference FormularyMost Commonly Prescribed MedicationsThe Standard Quick Reference Formulary is intended to provide a list of commonly prescribed drugs that are covered. This is not an all-inclusive list, the formulary covers many more drugs. On the Quick Reference, generic drugs are listed in lower case italics, and brand drugs are listed in CAPS. Remember, if a generic drug from the formulary is prescribed, the copay may be less than if a brand drug is prescribed. If the drug has step therapy or prior authorization on the formulary at the time of publishing, it is indicated below with a star (*). There are other safety edits that are not listed because of the abbreviated nature of this document. Individual plan designs may also change coverage of products listed. To see the complete listing of covered products please visit magellanrx.com.
Drugs are listed alphabetically.
10
magellanrx.com
As your prescription benefits manager, Magellan Rx Management is dedicated to giving you the best information and resources to help you make better healthcare decisions. Selecting generic medications is one way to help control your health care costs without sacrificing safety and effectiveness. The following are answers to commonly asked questions about generic drugs.
What are generic drugs?Generic drugs are important options that allow greater access to health care for all Americans. They are copies of brand-name drugs and are the same as those brand-name drugs in dosage form, safety, strength, route of administration, quality, performance characteristics and intended use.
Although generic drugs are chemically identical to their branded counterparts, they are typically sold at substantial discounts from the branded price. Generic manufacturers are able to sell their products for lower prices because they are not required to repeat the costly clinical trials of new drugs and generally do not pay for costly advertising, marketing, and promotion. In addition, multiple generic companies are often approved to market a single product; this creates competition in the market place, often resulting in lower prices.
Do generics work just as well as brand-name drugs?A study evaluated the results of 38 published clinical trials that compared cardiovascular generic drugs to their brand-name counterparts. There was no evidence that brand-name heart drugs worked any better than generic heart drugs.
Choose GenericsSave money by choosing quality, cost-effective alternatives to brand medications
11

magellanrx.com2 | 2019 Magellan Rx Management, LLC. All rights reserved. MRX1055_0519
Are generic drugs as effective as brand-name drugs?Yes. A generic drug is the same as a brand-name drug in dosage, safety, strength, quality, the way it works, the way it is taken and the way it should be used. The Food and Drug Administration (FDA) requires generic drugs have the same high quality, strength, purity and stability as brand-name drugs.
Not every brand-name drug has a generic drug. When new drugs are first made they have drug patents. Most drug patents are protected for 20 years. The patent, which protects the company that made the drug first, doesn’t allow anyone else to make and sell the drug. When the patent expires, other drug companies can start selling a generic version of the drug. But first, they must test the drug and the FDA must approve it.
Creating a new drug is expensive. Since generic drug makers do not develop a drug from scratch, the costs to bring the drug to market are less; therefore, generic drugs are usually less expensive than brand-name drugs. However, generic drug makers must show that their product performs in the same way as the brand-name drug.
What standards do generic drugs have to meet?Health professionals and consumers can be assured that FDA-approved generic drugs have met the same rigid standards as the innovator drug. To gain FDA approval, a generic drug must:
• Contain the same active ingredients as the innovator drug (inactive ingredients may vary)• Be identical in strength, dosage form, and route of administration• Have the same use indications• Be bioequivalent• Meet the same batch requirements for identity, strength, purity, and quality• Be manufactured under the same strict standards of FDA’s good manufacturing practice regulations required for innovator products
What if I prefer to take a brand-name drug?To encourage the use of generic drugs, your plan may require that you pay the difference in cost if you choose to take a brand-name prescription medication when a generic version of the same drug is available.
• If your doctor advises you to take a brand over generic, then you may not have to pay the difference, depending on your plan.
• If you elect a brand over a generic without your doctor’s consent, you must pay the difference between the brand and generic drug.
• If there is no generic equivalent, you may receive the brand drug with no penalty.
Is there a generic equivalent for my brand-name drug?To find out if there is a generic equivalent for your brand-name drug, please visit our website at magellanrx.com.
12
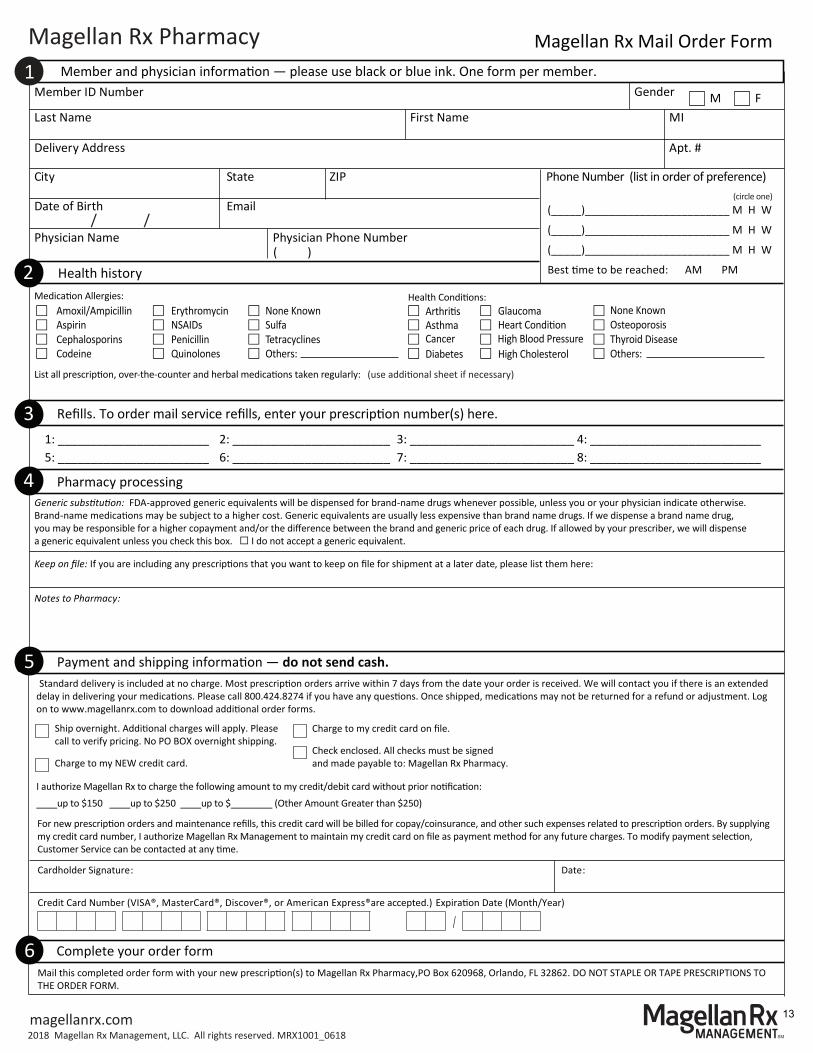
Member and physician informa�on — please use black or blue ink. One form per member.Member ID Number
Last Name First Name MI
Delivery Address Apt. #
City State ZIP
(_____)________________________ M H W
(_____)________________________ M H W
(_____)________________________ M H W
Best �me to be reached: AM PM
Date of Birth
Gender M F
Physician Name Physician Phone Number ( )
Health historyMedica�on Allergies:
None KnownHealth Condi�ons:
None Known
List all prescrip�on, over-the-counter and herbal medica�ons taken regularly:
Amoxil/Ampicillin Aspirin Cephalosporins
Codeine
ErythromycinNSAIDsPenicillinQuinolones
SulfaTetracyclinesOthers:
Arthri�sAsthmaCancerDiabetes
GlaucomaHeart Condi�onHigh Blood PressureHigh Cholesterol
OsteoporosisThyroid DiseaseOthers:
Magellan Rx Mail Order Form1
2
Pharmacy processing
Keep on file: If you are including any prescrip�ons that you want to keep on file for shipment at a later date, please list them here:
Notes to Pharmacy:
Payment and shipping informa�on — do not send cash.
Cardholder Signature: Date:
Credit Card Number (VISA®, MasterCard®, Discover®, or American Express®are accepted.) Expira�on Date (Month/Year)
/
5
Refills. To order mail service refills, enter your prescrip�on number(s) here.
4
3
/ /
Phone Number (list in order of preference)
Standard delivery is included at no charge. Most prescrip�on orders arrive within 7 days from the date your order is received. We will contact you if there is an extended delay in delivering your medica�ons. Please call 800.424.8274 if you have any ques�ons. Once shipped, medica�ons may not be returned for a refund or adjustment. Log on to www.magellanrx.com to download addi�onal order forms.
(circle one)
(use addi�onal sheet if necessary)
Magellan Rx Pharmacy
1: _______________________ 2: ________________________ 3: _________________________ 4: __________________________5: _______________________ 6: ________________________ 7: _________________________ 8: __________________________
magellanrx.com2018 Magellan Rx Management, LLC. All rights reserved. MRX1001_0618
Generic substitution: FDA-approved generic equivalents will be dispensed for brand-name drugs whenever possible, unless you or your physician indicate otherwise. Brand-name medica�ons may be subject to a higher cost. Generic equivalents are usually less expensive than brand name drugs. If we dispense a brand name drug, you may be responsible for a higher copayment and/or the difference between the brand and generic price of each drug. If allowed by your prescriber, we will dispense a generic equivalent unless you check this box. I do not accept a generic equivalent.
For new prescrip�on orders and maintenance refills, this credit card will be billed for copay/coinsurance, and other such expenses related to prescrip�on orders. By supplying my credit card number, I authorize Magellan Rx Management to maintain my credit card on file as payment method for any future charges. To modify payment selec�on, Customer Service can be contacted at any �me.
6Mail this completed order form with your new prescrip�on(s) to Magellan Rx Pharmacy,PO Box 620968, Orlando, FL 32862. DO NOT STAPLE OR TAPE PRESCRIPTIONS TO THE ORDER FORM.
Complete your order form
I authorize Magellan Rx to charge the following amount to my credit/debit card without prior no�fica�on: ____up to $150 ____up to $250 ____up to $________ (Other Amount Greater than $250)
Ship overnight. Addi�onal charges will apply. Please call to verify pricing. No PO BOX overnight shipping.
Charge to my NEW credit card.
Charge to my credit card on file.
Check enclosed. All checks must be signed and made payable to: Magellan Rx Pharmacy.
13
magellanrx.com2018 Magellan Rx Management, LLC. All rights reserved. MRX1122_0718
• Engaging in physical activity regularly
• Maintaining a healthy weight
• Eating a well balanced, nutritious diet
• Limiting alcohol consumption
• Quitting smoking and tobacco use
• Managing stress
Blood Pressure Levels
Normal Systolic: Less than 120 mmHg, andDiastolic: Less than 80 mmHg
Elevated (prehypertension) Systolic: 120–129 mmHg, andDiastolic: Less than 80 mmHg
High (hypertension)Systolic: 130 mmHg or higher, orDiastolic: 80 mmHg or higher
Prevent Health Problems
Learning how to achieve and maintain a healthy body and lifestyle is not always easy, but only you can make changes to improve your health and reduce your risk of developing heart disease and other serious illnesses. Protect your heart today by monitoring and learning about your blood pressure.
Although many of us understand the importance of a healthy body and lifestyle, we don’t always know how to go about achieving and maintaining it. One way to help you stay on top of your health, protect your heart, and prevent many health problems is by regularly monitoring your blood pressure.
Protect Your Heart
Blood Pressure
Blood pressure is determined by two things:
1) The amount of blood your heart pumps and,2) The amount of resistance your blood experiences as it flows through yourarteries.
High blood pressure, or hypertension, occurs when the force of blood pushing against the arteries as the heart pumps blood is elevated.
Blood pressure is written as two numbers:
1) The first or upper (systolic) number represents the pressure in your bloodvessels when your heart beats.
2) The second or lower (diastolic) number represents the pressure in yourvessels when your heart rests between beats.
Risk Factors for High Blood Pressure High blood pressure is often known as the “silent killer”. This is because many times there are no obvious symptoms of high blood pressure. Knowing the risk factors of high blood pressure and managing them appropriately can help increase your quality of life and reduce your risk of serious health problems including heart attack and stroke.
Take charge of your risk factors by:
14
magellanrx.com2019 Magellan Rx Management, LLC. All rights reserved. Low Copay_MRX0335_0719
Brand name drugs like Nexium®, Prevacid®, Prilosec®, Zyrtec®, Claritin® and Zantac® that used to only be available with a prescription are now available over-the-counter (OTC). If the OTC version is available in the same strength as the prescription drug you’re currently taking, then the OTC version could provide additional savings opportunities for you. As a result, your plan has elected to cover select OTC for a low copay. Covered medications include non-sedating antihistamines (NSAs) and ulcer/heartburn treatments packaged as name brands, store brands or generics as long as they are prescribed by your physician and processed using your prescription benefit card at your local pharmacy.
Talk to your physician today to find out if an OTC product is right for you.
Get Started Today
Think OTC for your Ulcer and Allergy MedicationsA smarter way to think. An easier way to save.
Physician Prescription
Take to your In-network Pharmacy
Follow Physician’s Instructions
To take advantage of this low co-pay OTC program, please follow these 3 easy steps once you and your doctor agree that an OTC product is right for you:
1. Ask your physician to write (or telephone in) a prescription for the specific OTC product.
• Make sure your physician writes “OTC” on the prescription.
2. Take the prescription to your local pharmacy (not available through mail service) and ensure that your pharmacist:
• Uses your prescription benefit card to fill the OTC prescription.
• Fills the prescription just like any other prescription medicine, making sure to include your doctor’s name and instructions on the label.
• Charges you a low co-pay as a result of this program.
3. Make sure to follow your doctor’s instructions for use when taking the medication.
It doesn’t make any sense to pay more. Talk to your physician to find out if an OTC product is right for you and start saving today!
Examples of Covered OTC Medications
• ALAVERT
• ALLEGRA
• ALLEGRA-D
• AXID AR
• CETIRIZINE
• CIMETIDINE
• CLARITIN
• CLARITIN-D
• FAMOTIDINE
• FEXOFENADINE
• FEXOFENADINE PSEUDOEPHEDRINE
• LORATADINE
• NEXIUM 24HR OTC
• OMEPRAZOLE
• PEPCID COMPLETE
• PEPCID AC
• PREVACID 24 HR CAP
• PRILOSEC OTC
• RANITIDINE
• TAGAMET HB
• XYZAL OTC
• ZANTAC
• ZEGERID OTC
• ZYRTEC
• ZYRTEC-D
15
INTEGRA Administrative Group, Inc. has partnered with The Phia Group, LLC, a firm
specializing in healthcare cost-containment services to handle your Plan’s subrogation and
reimbursement efforts. As you may be aware, your Plan Document has provisions that entitle
the Plan to be reimbursed for benefits paid if another party is responsible. The Phia Group may
send periodic informational requests, in an effort to uncover the details related to specific claims.
The Phia Group will be undertaking a review of the subrogation and reimbursement matters
opened and trauma-related claims paid. This is to ensure that all potential subrogation and
reimbursement claims have been identified and that the Plan is not paying for claims in which
another party is responsible.
Subrogation is a sure way to reduce Plan costs without reducing your benefits. The Phia Group’s
services will help ease skyrocketing health care costs as money recovered goes back into the
Plan’s general fund and is once again available to pay medical claims.
It may be possible that The Phia Group will request information that you have already responded
to previously. In most cases, The Phia Group’s representatives will be able to close the matter
over the telephone in a few minutes. We apologize for this inconvenience but we assure you that
in the future, The Phia Group will only be requesting information on current claims issues, as the
initial claims review will be completed.
If you have any questions regarding The Phia Group’s services or need assistance, please do not
hesitate to contact The Phia Group toll-free at 888-986-0080. The Phia Group looks forward to
working with you and your Plan.
The Phia Group has recently updated their website to include a “Member Resources” section,
which includes a FAQ section to help alleviate any hesitancy on your part, as it relates to
providing The Phia Group with information.
These options are available in English and Spanish. The URLs are as follows:
Member Information: https://www.phiagroup.com/Members-AreaFAQ's: https://www.phiagroup.com/Members-Area/Frequently-Asked-Questions
CLAIMS ADMINISTRATOR: INTEGRA ADMINISTRATIVE GROUP, INC.
110 SOUTH SHIPLEY STREET, SEAFORD DE 19973
(302)-629-3518 OR (800)-959-3518
16
Federal Law requires the following disclosures:
Women’s Health and Cancer rights Act of 1998
If you have had or are going to have a mastectomy, you may be entitled to certain benefits under
the Women’s Health and Cancer Act of 1998 (WHCRA). For individuals receiving mastectomy-
related benefits, coverage will be provided in a manner determined in consultation with the
attending physician and the patient for:
• All stages of reconstruction of the breast on which the mastectomy was performed;
• Surgery and reconstruction of the other breast to produce a symmetrical appearance;
• Prostheses; and
• Treatment of physical complications of the mastectomy, including lymphedema.
These benefits will be provided subject to the same deductibles and coinsurance applicable to
other medical and surgical benefits provided under this plan.
If you would like more information on WHCRA benefits, please call INTEGRA Administrative
Group, Inc. at (302)-629-3518 or toll free, (800)-959-3518.
Mental Health Parity and Addiction Equity Act (MHPAEA)
Under the federal law called the Mental Health Parity and Addiction Equity Act (MHPAEA),
many health plans and insurers must make sure that there is “parity” between mental health and
substance use disorder benefits, and medical and surgical benefits. This generally means that
treatment limits applied to mental health and substance use disorder benefits must be at least as
generous as the treatment limits applied to medical and surgical benefits. An employee has the
right to request additional information such as process used in respect to medical/surgical
benefits and mental health/substance abuse under the plan utilizing the form listed:
Draft Form – The Department of Labor (DOL) and other federal agencies have released a draft
model disclosure form that participants may use to request information from their health plan
or issuer regarding nonquantitative treatment limitations (NQTLs) that may affect their mental
health and substance use disorder (MH/SUD) benefits, or to obtain documentation after an
adverse benefit determination involving MH/SUD benefits to support a claim appeal.
For more information on this Act, visit https://www.dol.gov/agencies/ebsa/laws-and-regulations/laws/mental-health-and-substance-use-disorder-parity
Continuation of Coverage Notification:
Federal law requires that a copy of the Continuation of Coverage Notification notice be sent,
under a separate cover, to the spouse of an individual covered under a health insurance plan. If
you should have any questions concerning this notice please call our office at (302)-629-3518 or
toll free, 1-800-959-3515.
INTEGRA Administrative Group, Inc.
110 South Shipley Street, Seaford DE 1997
800-959-3518, Local (302)-629-3518, Claims Fax: (302)-629-8600
17
Continuation Coverage Rights Under COBRA
You are receiving this notice because you have recently become covered under a group health plan. This notice
contains important information about your right to COBRA continuation coverage, which is a temporary extension of coverage
under the Plan. This notice generally explains COBRA continuation coverage, when it may become available to you and
your family, and what you need to do to protect the right to receive it. You may have lower cost options such as enrolling in
the Marketplace or enrolling in a spouse’s plan within 30 days under a special enrollment event. The right to COBRA
continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA).
COBRA continuation coverage can become available to you when you would otherwise lose your group health coverage. It can
also become available to other members of your family who are covered under the Plan when they would otherwise lose their
group health coverage. For additional information about your rights and obligations under the Plan and under federal law, you
should review the Plan's Summary Plan Description or contact the Plan Administrator.
What is COBRA Continuation Coverage?
COBRA continuation coverage is a continuation of Plan coverage when coverage would otherwise end because of a life event
known as a "qualifying event." Specific qualifying events are listed later In this notice. After a qualifying event, COBRA
continuation coverage must be offered to each person who is a "qualified beneficiary." You, your spouse, and your dependent
children could become qualified beneficiaries if coverage under the Plan is lost because of the qualifying event. Under the Plan,
qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage.
If you are an employee, you will become a qualified beneficiary if you lose your coverage under the Plan because either one of
the following qualifying events happens:
• Your hours of employment are reduced, or
• Your employment ends for any reason other than your gross misconduct.
If you are the spouse of an employee, you will become a qualified beneficiary if you lose your coverage under the Plan because
any of the following qualifying events happens:
• Your spouse dies;
• Your spouse's hours of employment are reduced;
• Your spouse's employment ends for any reason other than his or her gross misconduct;
• Your spouse becomes entitled to Medicare benefits (under Part A, Part B, or both); or
• You become divorced or legally separated from your spouse.
Your dependent children will become qualified beneficiaries if they lose coverage under the Plan because any of the following
qualifying events happens:
• The parent-employee dies;
• The parent-employee's hours of employment are reduced;
• The parent-employee's employment ends for any reason other than his or her gross misconduct;
• The parent-employee becomes entitled to Medicare benefits (Part A, Part B, or both);
• The parents become divorced or legally separated; or
• The child stops being eligible for coverage under the plan as a "dependent child."
When Is COBRA Coverage Available?
The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator has
been notified that a qualifying event has occurred. When the qualifying event is the end of employment or reduction of hours of
employment, death of the employee, if the plan provides retiree health coverage: commencement of a proceeding In bankruptcy with
respect to the employer, or the employee's becoming entitled to Medicare benefits (under Part A, Part B, or both), the employer
must notify the Plan Administrator of the qualifying event.
(If the Plan provides retiree health coverage: Sometimes, filing a proceeding in bankruptcy under title 11 of the United States
Code can be a qualifying event. If a bankruptcy results in the loss of coverage of any retired employee covered under the Plan,
the retired employee will become a qualified beneficiary with respect to the bankruptcy. The retired
employee's spouse, surviving spouse, and dependent children will also become qualified beneficiaries if bankruptcy
results in the loss of their coverage under the Plan.
The employee must give notice of some qualifying events. For the other qualifying events (divorce or legal separation of
the employee and spouse or a dependent child's losing eligibility for coverage as a dependent child), you must notify
the Plan Administrator within 60 days after the qualifying event occurs. 18
Continuation Coverage Rights Under COBRA
How Is COBRA Coverage Provided?
Once the Plan Administrator receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to
each of the qualified beneficiaries. Each qualified beneficiary will have an independent right to elect COBRA continuation
coverage. Covered employees may elect COBRA continuation coverage on behalf of their spouses, and parents may elect COBRA
continuation coverage on behalf of their children. COBRA continuation coverage is a temporary continuation of coverage that
generally lasts for 18 months due to employment termination. Certain qualifying events or a second qualifying event during the
initial period of coverage may permit a beneficiary to receive a maximum of 36 months such as the death of the employee, the
employee becoming entitled to Medicare benefits (under Part A, Part B, or both), your divorce or legal separation, or a dependent
child's losing eligibility as a dependent child. There are two ways in which this 18-month period of COBRA continuation coverage
can be extended.
Disability extension of 18-month period of continuation coverage
if you or anyone in your family covered under the Plan is determined by the Social Security Administration to be disabled and you
notify the Plan Administrator in a timely fashion, you and your entire family may be entitled to receive up to an additional 11
months of COBRA continuation coverage, for a total maximum of 29 months. The disability would have to have started at some
time before the 60th day of COBRA continuation coverage and must last at least until the end of the 18-month period of
continuation coverage.
Second qualifying event extension of 18-month period of continuation coverage
if your family experiences another qualifying event while receiving 18 months of COBRA continuation coverage, the spouse and dependent
children in your family can get up to 18 additional months of COBRA continuation coverage, for a maximum of 36 months, if
notice of the second qualifying event is properly given to the Plan. This extension may be available to the spouse and any
dependent children receiving continuation coverage if the employee or former employee dies, becomes entitled to Medicare
benefits (under Part A, Part B, or both), or gets divorced or legally separated, or if the dependent child stops being eligible under
the Plan as a dependent child, but only if the event would have caused the spouse or dependent child to lose coverage under the
Plan had the first qualifying event not occurred.
Are there other coverage options besides COBRA?
Yes. There are other possible lower cost options such as enrolling in a spouse’s plan with a special enrollment event
if enrolled within 30 days of loss of coverage. Another option is The Health Insurance Marketplace. You can
compare plan and premium options at www.HealthCare.gov . You may qualify for a rate reduction with a subsidy.
Questions about your rights?
Contact Dept. of Labor: www.dol.gov/ebsa
Marketplace: www.HealthCare.gov
Keep your plan informed of address changes.
19
INTEGRA ADMINISTRATIVE GROUP, INC.
110 SOUTH SHIPLEY STREET, SEAFORD DE 19973
(302)-629-3518 OR (800)-959-3518
Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
You may be eligible for assistance paying your employer health plan premiums. For more information on special enrollment rights, contact either:
U.S. Department of Labor Employee Benefits Security Administration www.dol.gov/ebsa 1-866-444-EBSA (3272)
U.S. Department of Health and Human Services Centers for Medicare & Medicaid Services www.cms.hhs.gov 1-877-267-2323, Menu Option 4, Ext. 61565
20
NOTICE OF PRIVACY PRACTICES AND POLICIES
This provides notice of the privacy practices and policies of INTEGRA Administrative Group, Inc. These
protections have been adopted to ensure that the information that we obtain and maintain for our clients
and customers, which may also include information about the employees, dependents, former employees
and dependents, and other eligible participants on a group health plan for which we are providing services
(“Protected Parties”). The Notice outlines our practices, policies, and legal duties to maintain and protect
against prohibited disclosure of personally-identifiable financial information (as required by the federal
Gramm-Leach-Bliley Financial Modernization Act (“GLB Act”), and the various state laws implementing
those requirements) and protected health information of those Protected Parties (under the privacy
regulations mandated by the Health Insurance Portability and Accountability Act (“HIPAA Privacy”) and
further expanded by the Health Information Technology for Economic and Clinical Health Act
(“HITECH”) provisions in Title XIII of the American Recovery and Reinvestment Act (ARRA).
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT A PROTECTED PARTY
MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
PLEASE REVIEW IT CAREFULLY.
THE PROTECTION OF THE PRIVACY OF THE INFORMATION WE MAINTAIN IS IMPORTANT TO US.
21
1. Statement of Our Duties. We are required by law to
maintain the privacy of non-public personal information
(“NPPI”) and protected health information (“PHI”)
(collectively referred herein as “Protected Information”) of the
Protected Parties and to provide our clients with this notice of
our privacy practices and legal duties. We are required to
abide by the terms of this notice. We reserve the right to
change the terms of this notice and to adopt any new
provisions regarding the Protected Information that we
maintain about the Protected Parties. If we revise this notice,
we will provide each client or customer with whom there is a
current and direct business relationship with a revised notice
by mail, electronic mail, telefacsimile, or hand delivery.
2. Statement of the Client’s Rights under HIPAA
Privacy and HITECH. As our client or customer, you have a
right to know how we may use or disclose the Protected
Information we maintain on those Protected Parties with
whom there is a direct relationship. In the event that our
customer or client is an employer sponsoring a group health
plan, we do not have a direct duty to their employees,
dependents, former employees or dependents or other eligible
participants on the group health plan. Our obligations to not
disclose the Protected Health Information we maintain about
those individuals may arise due to our contractual obligations
as a Business Associate of both the client or customer, as well
as to any other third party who is a Covered Entity under the
HIPAA Privacy Regulations and as revised by HITECH, but
does not create a special legal duty to provide notice to those
individuals of their rights through a Notice of Privacy
Practices.
Primary Uses and Disclosures of Protected Health
Information. We use and disclose protected health information
about Protected Parties for payment and health care
operations. HIPAA Privacy does not generally “preempt” (or
take precedence over) state privacy or other applicable laws
that provide individuals greater privacy protections. As a
result, to the extent state law applies, the privacy laws of a
particular state, or other federal laws, rather than the HIPAA
Privacy, might impose a privacy standard under which we will
be required to operate. For example, where such laws have
been enacted, we will follow more stringent state privacy laws
that relate to uses and disclosures of the protected health
information concerning HIV or AIDS, mental health,
substance abuse/chemical dependency, genetic testing,
reproductive rights.
In addition to these state law requirements, we also may use or
disclose Protected Information in the following situations:
Payment: We might use and disclose your protected
health information for all activities that are included
within the definition of “payment” within the HIPAA
Privacy regulations. For example, we might use and
disclose a Protected Party’s Protected Information to
assist with the payment of claims for services provided to
that Protected Party by doctors, hospitals, pharmacies and
others for services that are covered by a group health
plan. We might also use your information to determine
your eligibility for benefits, to coordinate benefits, to
examine medical necessity, to obtain premiums, and to
issue explanations of benefits to the person who
subscribes to the health plan in which you participate.
Health Care Operations: We might use and disclose a
Protected Party’s Protected Information for all activities
that are included within the definition of “health care
operations” within the HIPAA Privacy regulations. For
example, we might use and disclose the Protected
Information of a Protected Party to an insurer to
determine the premiums for your health plan, to conduct
quality assessment and improvement activities, to engage
in care coordination or case management, and to manage
our business.
Business Associates: In connection with our payment and
health care operations activities, we contract with
individuals and entities (called “Business Associates”) to
perform various functions on our behalf or to provide
certain types of services. To perform these functions or to
provide the services, our business associates will receive,
have access to, create, maintain, use, or disclose protected
health information, but only after we require the business
associates to agree in writing to contract terms designed
to appropriately safeguard your information.
Other Covered Entities: In addition, we might use or
disclose your protected health information to assist health
care providers in connection with their treatment or
payment activities, or to assist other covered entities in
connection with certain of their health care operations.
For example, we might disclose a Protected Party’s
Protected Information to a health care provider when
needed by the provider to render treatment to that party,
and we might disclose protected health information to
another covered entity to conduct health care operations
related to billing, claims payment or enrollment.
For all other uses and disclosures, we first must obtain your
permission.
In addition, you have the following rights:
The right to request that we place additional restrictions
on our uses and disclosures of the personal health
information of Protected Parties. However, we are not
obligated to agree to impose any such additional
restrictions.
22
The right to access, inspect and copy the protected
information pertaining to Protected Parties that we
maintain in our files, and the right to have us correct or
amend any information that we create in error. Requests
to access or amend your health information should be sent
to the contact person and address provided below.
The right to receive an accounting of the disclosures of
the Protected Information we maintain on Protected
Parties that we make for purposes other than activities
related to payment functions or other health care
operations.
The right to request that communications containing a
protected party’s Protected Information are sent in a
confidential manner.
If you received this notice electronically, you also have
the right to obtain a paper copy of this notice from us on
request.
3. Information We Collect About You. We collect the
following categories of information for group and/or
individual policies from the following sources:
a) Information that we obtain directly from you, in
conversations or on applications or other forms that
you or a Protected Party completes.
b) Information regarding current or prospective plan
participants we obtain about them on applications or
other forms.
c) Information about the plan’s transactions with our
affiliates, others or us.
d) Information that we obtain as a result of our
transactions with you.
4. Permissible Uses and Disclosures of Protected
Information. We disclose the information we receive
regarding current or prospective plan participants only in
accordance with the terms and conditions of the various
Business Associate contracts we have entered to with Covered
Entities under HIPAA Privacy Regulations and as permitted
under state and federal laws concerning the privacy of your
insurance and financial information. Those include:
Situations Permitted or Required by Law. We also
may use or disclose your protected health information
without your written permission for other purposes
permitted or required by law, including, but not
limited to the following:
a) As authorized by and to the extent necessary to
comply with workers’ compensation or other no-
fault laws;
b) To an oversight or insurance regulatory agency
for activities including audits or civil, criminal or
administrative actions;
c) To a public health authority for purposes of
public health activities (such as to the Federal
Food and Drug Administration to report
consumer product defects);
d) To a law enforcement official for law
enforcement purposes or in response to a court
order or in the course of any judicial or
administrative proceeding;
e) To organ procurement organizations or other
entities for approved research; or
f) To a governmental authority, including a social
service or protective services agency, authorized
to receive reports of abuse, neglect or domestic
violence.
For any Purposes to Which you have Not Objected.
In certain limited circumstances, we may use or
disclose your protected health information after we
have given you an opportunity to object and you have
not objected. For example, if you do not object, we
may use limited information about you to maintain an
office directory, to notify family members or any
other person identified by you regarding issues
directly related to such person’s involvement with
your care or payment for that care, or in emergency
circumstances.
For Purposes for Which We Have Obtained your
Written Permission. All other uses or disclosures of
your protected health information will be made only
with your written permission, and you may revoke
any permission that you give us at any time.
5. Complaints About Misuse of Health Information. You
may complain either directly to us or to the Secretary of
Health and Human Services if you believe that your rights
with respect to our protection of your health information have
been violated. To file a complaint with us, you may send a
written statement outlining your complaint, the facts and
circumstances surrounding your complaint, including the
names, dates and as many details as possible. You will not be
retaliated against in any way for filing a complaint.
6. Our Practices Regarding Confidentiality and Security.
We restrict access to nonpublic personal and personally-
identifiable health information about you to those employees
and agents who need to know that information in order to
provide products and services to you. We maintain physical,
electronic and procedural safeguards that comply with state
and federal regulations to guard your nonpublic personal
information.
7. Notice of Breach of Protected Health Information. In the
event of any unauthorized acquisition, access, use or
disclosure of Protected Health Information, we shall fully
comply with the breach notification requirements, including
any and all regulations which have been or may be
promulgated, which will include notification to you of any
impact that breach may have had on you, your employees,
dependents or other participants in any plan in which we are
providing services.
8. Our Policy Regarding Dispute Resolution. Any
controversy or claim arising out of or relating to our privacy
policy, or the breach thereof, shall be settled by arbitration in
accordance with the rules of the American Arbitration
Association, and judgment upon the award rendered by the
arbitrator(s) may be entered in any court having jurisdiction
thereof.
23
CMS Form 10182-CC
Important Notice from Jacksonville Police Officers and Fire Fighters Health Insurance Trust
About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your
current prescription drug coverage with Jacksonville Police Officers and Fire Fighters Health Insurance
Trust and about your options under Medicare’s prescription drug coverage. This information can help
you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you
should compare your current coverage, including which drugs are covered at what cost, with the
coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information
about where you can get help to make decisions about your prescription drug coverage is at the end of
this notice.
There are two important things you need to know about your current coverage and Medicare’s
prescription drug coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can getthis coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like anHMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standardlevel of coverage set by Medicare. Some plans may also offer more coverage for a higher monthlypremium.
2. INTEGRA Administrative Group, Inc. has determined that the prescription drug coverage offered by theJacksonville Police Officers and Fire Fighters Health Insurance Trust is, on average for all planparticipants, expected to pay out as much as standard Medicare prescription drug coverage pays and istherefore considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you
can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicaredrug plan.
When Can You Join A Medicare Drug Plan?
You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th to December 7th.
However, if you lose your current creditable prescription drug coverage, through no fault of your own, you
will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan?
If you decide to join a Medicare drug plan your current Jacksonville Police Officers and Fire Fighters
Health Insurance Trust coverage will be affected. For those individuals who elect Part D coverage,
coverage under the entity’s plan will end for the individual and all covered dependents.
See pages 7- 9 of the CMS Disclosure of Creditable Coverage To Medicare Part D Eligible Individuals
Guidance (available at http://www.cms.hhs.gov/CreditableCoverage/), which outlines the prescription drug
plan provisions/options that Medicare eligible individuals may have available to them when they become
eligible for Medicare Part D.
If you do decide to join a Medicare drug plan and drop your current Jacksonville Police Officers and Fire
Fighters Health Insurance Trust coverage, be aware that you and your dependents will not able to get
this coverage back (if you decided to drop your Medicare Part D coverage at a later time).
24
CMS Form 10182-CC
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan?
You should also know that if you drop or lose your current coverage with Jacksonville Police Officers and Fire Fighters Health Insurance Trust and don’t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later.
If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.
For More Information About This Notice Or Your Current Prescription Drug Coverage…
Contact the Jacksonville Police Officers and Fire Fighters Health Insurance Trust personnel office for further information or call INTEGRA Administrative Group at 1-800-959-3518. NOTE: You will get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through Jacksonville Police Officers and Fire Fighters Health Insurance Trust changes. You also may request a copy of this notice at any time.
For More Information About Your Options Under Medicare Prescription Drug Coverage…
More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans.
For more information about Medicare prescription drug coverage:
• Visit www.medicare.gov • Call your State Health Insurance Assistance Program (see the inside back cover of your copy of • the “Medicare & You” handbook for their telephone number) for personalized help • Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you are required to pay a higher premium (a penalty).
Date: January 1, 2020
Name of Entity/Sender: Jacksonville Police Officers and Fire Fighters Health Insurance Trust
Address: 625 Stockton Street, Jacksonville FL 32204
Phone Number: 904-759-7416 or 904-334-8470
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control
number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this information collection is estimated to average 8 hours per response initially, including the time to review instructions, search existing data resources, gather the data needed, and complete and
review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write
to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.
25
Notice of Privacy Practices
Page 1 of 9
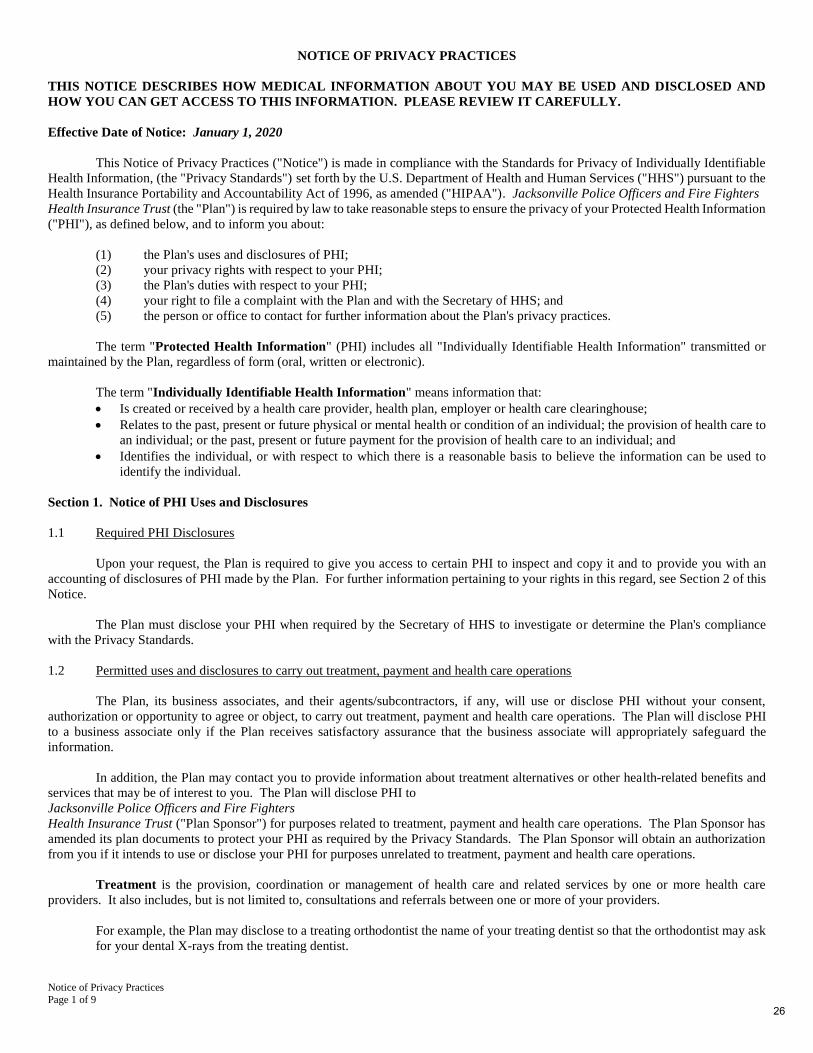
NOTICE OF PRIVACY PRACTICES
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Effective Date of Notice: January 1, 2020
This Notice of Privacy Practices ("Notice") is made in compliance with the Standards for Privacy of Individually Identifiable
Health Information, (the "Privacy Standards") set forth by the U.S. Department of Health and Human Services ("HHS") pursuant to the
Health Insurance Portability and Accountability Act of 1996, as amended ("HIPAA"). Jacksonville Police Officers and Fire Fighters
Health Insurance Trust (the "Plan") is required by law to take reasonable steps to ensure the privacy of your Protected Health Information
("PHI"), as defined below, and to inform you about:
(1) the Plan's uses and disclosures of PHI;
(2) your privacy rights with respect to your PHI;
(3) the Plan's duties with respect to your PHI;
(4) your right to file a complaint with the Plan and with the Secretary of HHS; and
(5) the person or office to contact for further information about the Plan's privacy practices.
The term "Protected Health Information" (PHI) includes all "Individually Identifiable Health Information" transmitted or
maintained by the Plan, regardless of form (oral, written or electronic).
The term "Individually Identifiable Health Information" means information that:
• Is created or received by a health care provider, health plan, employer or health care clearinghouse;
• Relates to the past, present or future physical or mental health or condition of an individual; the provision of health care to
an individual; or the past, present or future payment for the provision of health care to an individual; and
• Identifies the individual, or with respect to which there is a reasonable basis to believe the information can be used to
identify the individual.
Section 1. Notice of PHI Uses and Disclosures
1.1 Required PHI Disclosures
Upon your request, the Plan is required to give you access to certain PHI to inspect and copy it and to provide you with an
accounting of disclosures of PHI made by the Plan. For further information pertaining to your rights in this regard, see Section 2 of this
Notice.
The Plan must disclose your PHI when required by the Secretary of HHS to investigate or determine the Plan's compliance
with the Privacy Standards.
1.2 Permitted uses and disclosures to carry out treatment, payment and health care operations
The Plan, its business associates, and their agents/subcontractors, if any, will use or disclose PHI without your consent,
authorization or opportunity to agree or object, to carry out treatment, payment and health care operations. The Plan will disclose PHI
to a business associate only if the Plan receives satisfactory assurance that the business associate will appropriately safeguard the
information.
In addition, the Plan may contact you to provide information about treatment alternatives or other health-related benefits and
services that may be of interest to you. The Plan will disclose PHI to
Jacksonville Police Officers and Fire Fighters
Health Insurance Trust ("Plan Sponsor") for purposes related to treatment, payment and health care operations. The Plan Sponsor has
amended its plan documents to protect your PHI as required by the Privacy Standards. The Plan Sponsor will obtain an authorization
from you if it intends to use or disclose your PHI for purposes unrelated to treatment, payment and health care operations.
Treatment is the provision, coordination or management of health care and related services by one or more health care
providers. It also includes, but is not limited to, consultations and referrals between one or more of your providers.
For example, the Plan may disclose to a treating orthodontist the name of your treating dentist so that the orthodontist may ask
for your dental X-rays from the treating dentist.
26
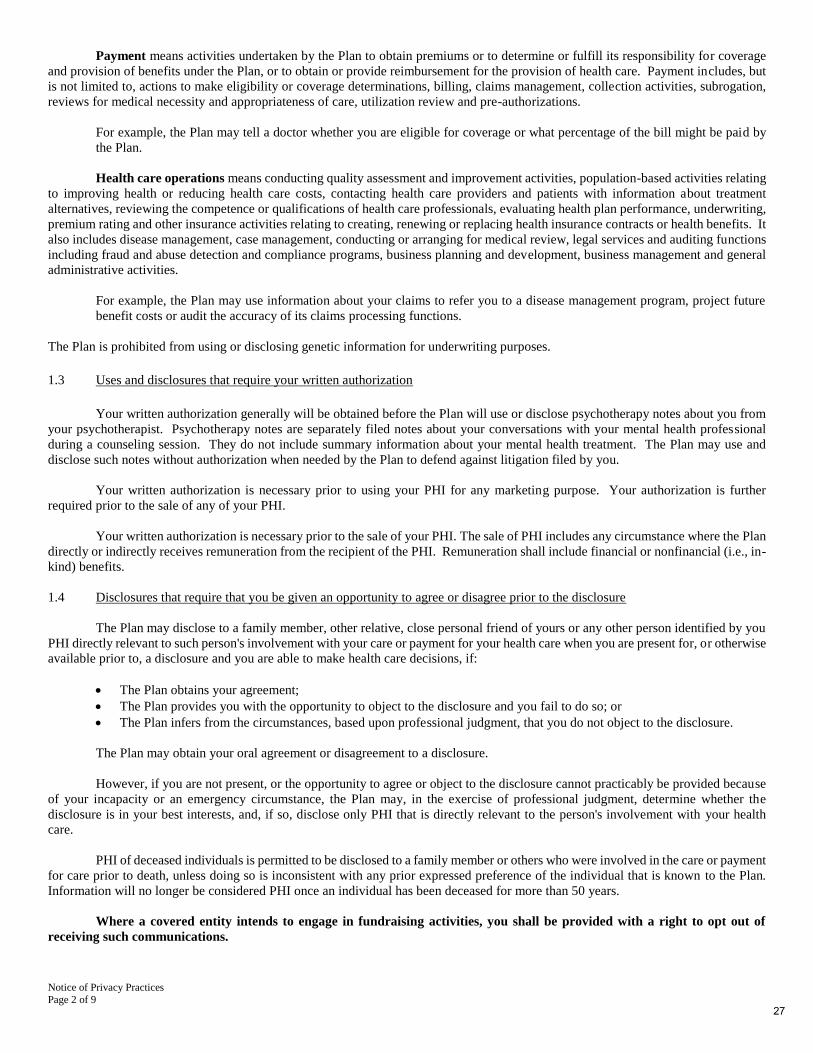
Notice of Privacy Practices
Page 2 of 9
Payment means activities undertaken by the Plan to obtain premiums or to determine or fulfill its responsibility for coverage
and provision of benefits under the Plan, or to obtain or provide reimbursement for the provision of health care. Payment includes, but
is not limited to, actions to make eligibility or coverage determinations, billing, claims management, collection activities, subrogation,
reviews for medical necessity and appropriateness of care, utilization review and pre-authorizations.
For example, the Plan may tell a doctor whether you are eligible for coverage or what percentage of the bill might be paid by
the Plan.
Health care operations means conducting quality assessment and improvement activities, population-based activities relating
to improving health or reducing health care costs, contacting health care providers and patients with information about treatment
alternatives, reviewing the competence or qualifications of health care professionals, evaluating health plan performance, underwriting,
premium rating and other insurance activities relating to creating, renewing or replacing health insurance contracts or health benefits. It
also includes disease management, case management, conducting or arranging for medical review, legal services and auditing functions
including fraud and abuse detection and compliance programs, business planning and development, business management and general
administrative activities.
For example, the Plan may use information about your claims to refer you to a disease management program, project future
benefit costs or audit the accuracy of its claims processing functions.
The Plan is prohibited from using or disclosing genetic information for underwriting purposes.
1.3 Uses and disclosures that require your written authorization
Your written authorization generally will be obtained before the Plan will use or disclose psychotherapy notes about you from
your psychotherapist. Psychotherapy notes are separately filed notes about your conversations with your mental health professional
during a counseling session. They do not include summary information about your mental health treatment. The Plan may use and
disclose such notes without authorization when needed by the Plan to defend against litigation filed by you.
Your written authorization is necessary prior to using your PHI for any marketing purpose. Your authorization is further
required prior to the sale of any of your PHI.
Your written authorization is necessary prior to the sale of your PHI. The sale of PHI includes any circumstance where the Plan
directly or indirectly receives remuneration from the recipient of the PHI. Remuneration shall include financial or nonfinancial (i.e., in-
kind) benefits.
1.4 Disclosures that require that you be given an opportunity to agree or disagree prior to the disclosure
The Plan may disclose to a family member, other relative, close personal friend of yours or any other person identified by you
PHI directly relevant to such person's involvement with your care or payment for your health care when you are present for, or otherwise
available prior to, a disclosure and you are able to make health care decisions, if:
• The Plan obtains your agreement;
• The Plan provides you with the opportunity to object to the disclosure and you fail to do so; or
• The Plan infers from the circumstances, based upon professional judgment, that you do not object to the disclosure.
The Plan may obtain your oral agreement or disagreement to a disclosure.
However, if you are not present, or the opportunity to agree or object to the disclosure cannot practicably be provided because
of your incapacity or an emergency circumstance, the Plan may, in the exercise of professional judgment, determine whether the
disclosure is in your best interests, and, if so, disclose only PHI that is directly relevant to the person's involvement with your health
care.
PHI of deceased individuals is permitted to be disclosed to a family member or others who were involved in the care or payment
for care prior to death, unless doing so is inconsistent with any prior expressed preference of the individual that is known to the Plan.
Information will no longer be considered PHI once an individual has been deceased for more than 50 years.
Where a covered entity intends to engage in fundraising activities, you shall be provided with a right to opt out of
receiving such communications.
27

Notice of Privacy Practices
Page 3 of 9
1.5 Uses and disclosures for which authorization or opportunity to agree or object is not required
Use and disclosure of your PHI is allowed without your authorization or opportunity to agree or object under the following
circumstances:
(a) When required by law, provided that the use or disclosure complies with and is limited to the relevant requirements of
such law.
(b) When permitted for purposes of public health activities, including disclosures to (i) a public health authority or other
appropriate government authority authorized by law to receive reports of child abuse or neglect and (ii) a person subject
to the jurisdiction of the Food and Drug Administration (FDA) regarding an FDA-regulated product or activity for the
purpose of activities related to the quality, safety or effectiveness of such FDA-regulated product or activity, including to
report product defects, to permit product recalls and to conduct post-marketing surveillance. PHI also may be disclosed
to a person who may have been exposed to a communicable disease or may otherwise be at risk of contracting or spreading
a disease or condition, if authorized by law.
(c) Except for reports of child abuse or neglect permitted by part (b) above, when required or authorized by law, or with your
agreement, the Plan may disclose PHI about you to a government authority, including a social service or protective services
agency, if the Plan reasonably believes you to be a victim of abuse, neglect, or domestic violence. In such case, the Plan
will promptly inform you that such a disclosure has been or will be made unless (i) the Plan believes that informing you
would place you at risk of serious harm or (ii) the Plan would be informing your personal representative, and the Plan
believes that your personal representative is responsible for the abuse, neglect or other injury, and that informing such
person would not be in your best interests. For the purposes of reporting child abuse or neglect, it is not necessary to
inform the minor that such a disclosure has been or will be made. Disclosure generally may be made to the minor's parents
or other representatives although there may be circumstances under federal or state law when the parents or other
representatives may not be given access to the minor's PHI.
(d) The Plan may disclose your PHI to a health oversight agency for oversight activities authorized by law. This includes
civil, administrative or criminal investigations; inspections; licensure or disciplinary actions (for example, to investigate
complaints against providers); and other activities necessary for appropriate oversight of: (i) the health care system, (ii)
government benefit programs for which health information is relevant to beneficiary eligibility, (iii) entities subject to
government regulatory programs for which health information is needed to determine compliance with program standards,
or (iv) entities subject to civil rights laws for which health information is needed to determine compliance.
(e) The Plan may disclose your PHI in the course of a judicial or administrative proceeding in response to an order of a court
or administrative tribunal, provided that the Plan discloses only the PHI expressly authorized by such order, or in response
to a subpoena, discovery request, or other lawful process, that is not accompanied by an order of a court of administrative
tribunal if certain conditions are met. One of those conditions is that satisfactory assurances must be given to the Plan that
the requesting party has made a good faith attempt to provide written notice to you, and the notice provided sufficient
information about the proceeding to permit you to raise an objection, and the time to object has expired and either no
objections were raised or any objections were resolved in favor of disclosure by the court or tribunal.
(f) The Plan may disclose your PHI to a law enforcement official when required for law enforcement purposes. The Plan may
disclose PHI as required by law, including laws that require the reporting of certain types of wounds. Also, the Plan may
disclose PHI in compliance with (i) a court order, court-ordered warrant, or a subpoena or summons issued by a judicial
officer, (ii) a grand jury subpoena, or (iii) an administrative request, including an administrative subpoena or summons, a
civil or authorized investigative demand, provided certain conditions are satisfied. PHI may be disclosed for law
enforcement purposes, including for the purpose of identifying or locating a suspect, fugitive, material witness or missing
person. Under certain circumstances, the Plan may disclose your PHI in response to a law enforcement official's request
if you are, or are suspected to be, a victim of a crime. Further, the Plan may disclose your PHI if it believes in good faith
that the PHI constitutes evidence of criminal conduct that occurred on the Plan's premises.
(g) The Plan may disclose PHI to a coroner or medical examiner for the purpose of identifying a deceased person, determining
a cause of death or other duties as authorized by law. Also, disclosure is permitted to funeral directors, consistent with
applicable law, as necessary to carry out their duties with respect to the decedent.
(h) The Plan may use or disclose PHI for research, subject to certain conditions.
(i) When consistent with applicable law and standards of ethical conduct, the Plan may use or disclose PHI if the Plan, in
good faith, believes the use or disclosure: (i) is necessary to prevent or lessen a serious and imminent threat to health or
safety of a person or the public and is to person(s) able to prevent or lessen the threat, including the target of the threat, or
(ii) is needed for law enforcement authorities to identify or apprehend an individual, provided certain requirements are
met.
(j) When authorized by and to the extent necessary to comply with workers' compensation or other similar programs
established by law.
28
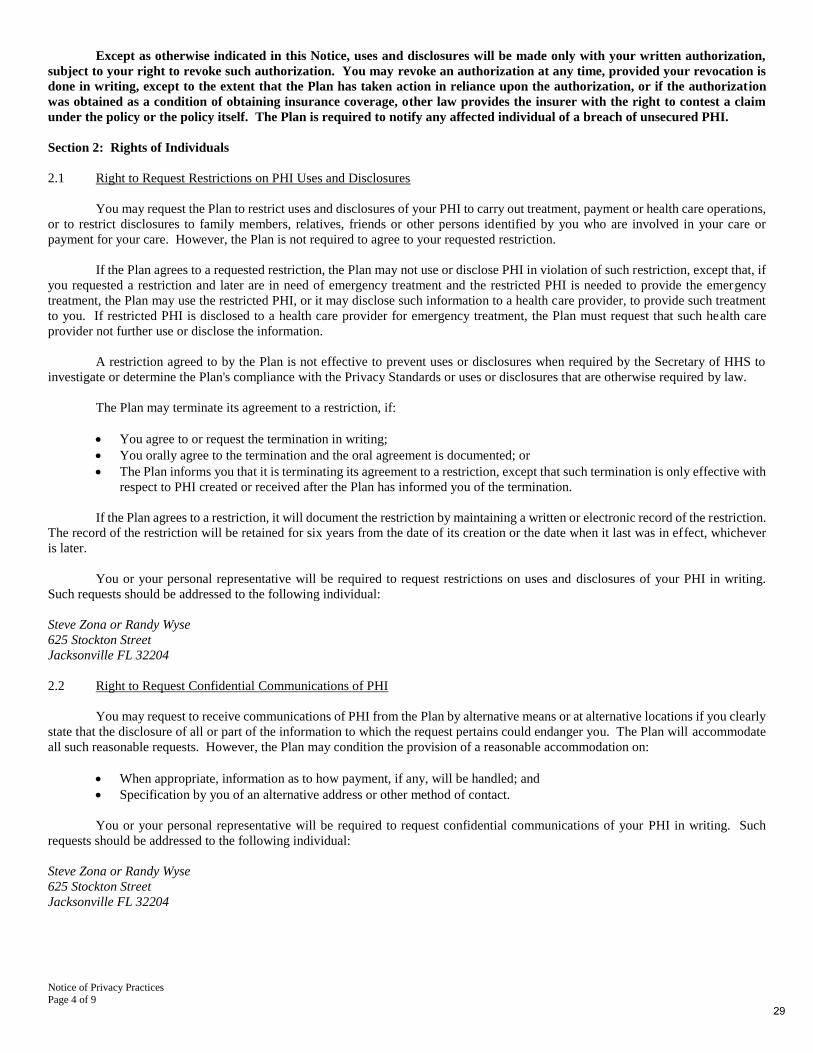
Notice of Privacy Practices
Page 4 of 9
Except as otherwise indicated in this Notice, uses and disclosures will be made only with your written authorization,
subject to your right to revoke such authorization. You may revoke an authorization at any time, provided your revocation is
done in writing, except to the extent that the Plan has taken action in reliance upon the authorization, or if the authorization
was obtained as a condition of obtaining insurance coverage, other law provides the insurer with the right to contest a claim
under the policy or the policy itself. The Plan is required to notify any affected individual of a breach of unsecured PHI.
Section 2: Rights of Individuals
2.1 Right to Request Restrictions on PHI Uses and Disclosures
You may request the Plan to restrict uses and disclosures of your PHI to carry out treatment, payment or health care operations,
or to restrict disclosures to family members, relatives, friends or other persons identified by you who are involved in your care or
payment for your care. However, the Plan is not required to agree to your requested restriction.
If the Plan agrees to a requested restriction, the Plan may not use or disclose PHI in violation of such restriction, except that, if
you requested a restriction and later are in need of emergency treatment and the restricted PHI is needed to provide the emergency
treatment, the Plan may use the restricted PHI, or it may disclose such information to a health care provider, to provide such treatment
to you. If restricted PHI is disclosed to a health care provider for emergency treatment, the Plan must request that such health care
provider not further use or disclose the information.
A restriction agreed to by the Plan is not effective to prevent uses or disclosures when required by the Secretary of HHS to
investigate or determine the Plan's compliance with the Privacy Standards or uses or disclosures that are otherwise required by law.
The Plan may terminate its agreement to a restriction, if:
• You agree to or request the termination in writing;
• You orally agree to the termination and the oral agreement is documented; or
• The Plan informs you that it is terminating its agreement to a restriction, except that such termination is only effective with
respect to PHI created or received after the Plan has informed you of the termination.
If the Plan agrees to a restriction, it will document the restriction by maintaining a written or electronic record of the restriction.
The record of the restriction will be retained for six years from the date of its creation or the date when it last was in effect, whichever
is later.
You or your personal representative will be required to request restrictions on uses and disclosures of your PHI in writing.
Such requests should be addressed to the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
2.2 Right to Request Confidential Communications of PHI
You may request to receive communications of PHI from the Plan by alternative means or at alternative locations if you clearly
state that the disclosure of all or part of the information to which the request pertains could endanger you. The Plan will accommodate
all such reasonable requests. However, the Plan may condition the provision of a reasonable accommodation on:
• When appropriate, information as to how payment, if any, will be handled; and
• Specification by you of an alternative address or other method of contact.
You or your personal representative will be required to request confidential communications of your PHI in writing. Such
requests should be addressed to the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
29
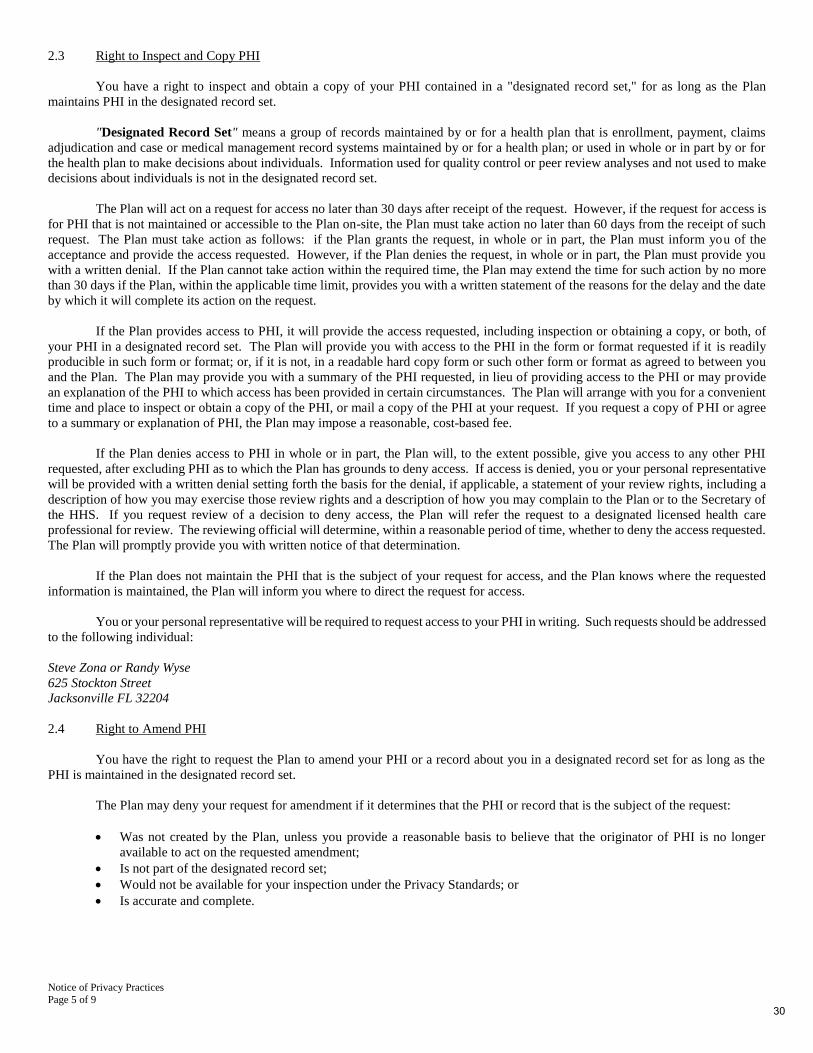
Notice of Privacy Practices
Page 5 of 9
2.3 Right to Inspect and Copy PHI
You have a right to inspect and obtain a copy of your PHI contained in a "designated record set," for as long as the Plan
maintains PHI in the designated record set.
"Designated Record Set" means a group of records maintained by or for a health plan that is enrollment, payment, claims
adjudication and case or medical management record systems maintained by or for a health plan; or used in whole or in part by or for
the health plan to make decisions about individuals. Information used for quality control or peer review analyses and not used to make
decisions about individuals is not in the designated record set.
The Plan will act on a request for access no later than 30 days after receipt of the request. However, if the request for access is
for PHI that is not maintained or accessible to the Plan on-site, the Plan must take action no later than 60 days from the receipt of such
request. The Plan must take action as follows: if the Plan grants the request, in whole or in part, the Plan must inform you of the
acceptance and provide the access requested. However, if the Plan denies the request, in whole or in part, the Plan must provide you
with a written denial. If the Plan cannot take action within the required time, the Plan may extend the time for such action by no more
than 30 days if the Plan, within the applicable time limit, provides you with a written statement of the reasons for the delay and the date
by which it will complete its action on the request.
If the Plan provides access to PHI, it will provide the access requested, including inspection or obtaining a copy, or both, of
your PHI in a designated record set. The Plan will provide you with access to the PHI in the form or format requested if it is readily
producible in such form or format; or, if it is not, in a readable hard copy form or such other form or format as agreed to between you
and the Plan. The Plan may provide you with a summary of the PHI requested, in lieu of providing access to the PHI or may provide
an explanation of the PHI to which access has been provided in certain circumstances. The Plan will arrange with you for a convenient
time and place to inspect or obtain a copy of the PHI, or mail a copy of the PHI at your request. If you request a copy of PHI or agree
to a summary or explanation of PHI, the Plan may impose a reasonable, cost-based fee.
If the Plan denies access to PHI in whole or in part, the Plan will, to the extent possible, give you access to any other PHI
requested, after excluding PHI as to which the Plan has grounds to deny access. If access is denied, you or your personal representative
will be provided with a written denial setting forth the basis for the denial, if applicable, a statement of your review rights, including a
description of how you may exercise those review rights and a description of how you may complain to the Plan or to the Secretary of
the HHS. If you request review of a decision to deny access, the Plan will refer the request to a designated licensed health care
professional for review. The reviewing official will determine, within a reasonable period of time, whether to deny the access requested.
The Plan will promptly provide you with written notice of that determination.
If the Plan does not maintain the PHI that is the subject of your request for access, and the Plan knows where the requested
information is maintained, the Plan will inform you where to direct the request for access.
You or your personal representative will be required to request access to your PHI in writing. Such requests should be addressed
to the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
2.4 Right to Amend PHI
You have the right to request the Plan to amend your PHI or a record about you in a designated record set for as long as the
PHI is maintained in the designated record set.
The Plan may deny your request for amendment if it determines that the PHI or record that is the subject of the request:
• Was not created by the Plan, unless you provide a reasonable basis to believe that the originator of PHI is no longer
available to act on the requested amendment;
• Is not part of the designated record set;
• Would not be available for your inspection under the Privacy Standards; or
• Is accurate and complete.
30
Notice of Privacy Practices
Page 6 of 9
The Plan has 60 days after the request is made to act on the request. A single 30-day extension is allowed if the Plan is unable
to comply within that deadline provided that the Plan, within the original 60-day time period, gives you a written statement of the reasons
for the delay and the date by which it will complete its action on the request. If the Plan accepts the requested amendment, the Plan will
make the appropriate amendment to the PHI or record that is the subject of the request by, at a minimum, identifying the records in the
designated record set that are affected by the amendment and appending or otherwise providing a link to the location of the amendment.
The Plan will timely inform you that the amendment is accepted and obtain your identification of and agreement to have the Plan notify
the relevant persons with which the amendment needs to be shared as provided in the Privacy Standards.
If the request is denied in whole or part, the Plan must provide you with a written denial that (i) explains the basis for the denial,
(ii) sets forth your right to submit a written statement disagreeing with the denial and how to file such a statement, (iii) states that, if you
do not submit a statement of disagreement, you may request that the Plan provide your request for amendment and the denial with any
future disclosures of the PHI that is the subject of the amendment, and (iv) includes a description of how you may complain to the Plan
or to the Secretary of HHS. The Plan may reasonably limit the length of a statement of disagreement. Further, the Plan may prepare a
written rebuttal to a statement of disagreement, which will be provided to you. The Plan must, as appropriate, identify the record or PHI
in the designated record set that is the subject of the disputed amendment and append or otherwise link your request for an amendment,
the Plan's denial of the request, your statement of disagreement, if any, and the Plan's rebuttal, if any, to the designated record set. If a
statement of disagreement has been submitted, the Plan will include the above-referenced material, or, at the Plan's election, an accurate
summary of such information, with any subsequent disclosure of the PHI to which the disagreement relates. If you do not submit a
written statement of disagreement, the Plan must include your request for amendment and its denial, or an accurate summary of such
information with any subsequent disclosure of the PHI only if requested by you.
You or your personal representative will be required to request amendment to your PHI in a designated record set in writing.
Such requests should be addressed to the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
All requests for amendment of PHI must include a reason to support the requested amendment.
2.5 Right to Receive an Accounting of PHI Disclosures
At your request, the Plan will provide you with an accounting of disclosures by the Plan of your PHI during the six years prior
to the date on which the accounting is requested. However, such accounting need not include PHI disclosures made: (a) to carry out
treatment, payment or health care operations; (b) to individuals about their own PHI; (c) incident to a use or disclosure otherwise
permitted or required by the Privacy Standards; (d) pursuant to an authorization; (e) to certain persons involved in your care or payment
for your care; (f) to notify certain persons of your location, general condition or death; (g) as part of a "Limited Data Set" (as defined in
the Privacy Standards), which largely relates to research purposes; or (h) prior to the compliance date of August 14, 2003. You may
request an accounting of disclosures for a period of time less than six years from the date of the request.
The accounting will include disclosures of PHI that occurred during the six years (or such shorter time period, if applicable)
prior to the date of the request for an accounting, including disclosures to or by business associates of the Plan. Except as otherwise
provided below, for each disclosure, the accounting will include:
• The date of the disclosure;
• The name of the entity or person who received the PHI and, if known, the address of such entity or person;
• A brief description of the PHI disclosed; and
• A brief statement of the purpose of the disclosure that reasonably informs you of the basis for the disclosure, or, in lieu of
such statement, a copy of a written request for disclosure.
If during the period covered by the accounting, the Plan has made multiple disclosures of PHI to the same person or entity for
a single purpose, the accounting may, with respect to such multiple disclosures, provide the above-referenced information for the first
disclosure; the frequency, periodicity or number of the disclosures made during the accounting period; and the date of the last disclosure.
If during the period covered by the accounting, the Plan has made disclosures of PHI for a particular research purpose for 50
or more individuals, the accounting may, with respect to such disclosures for which your PHI may have been included, provide certain
information as permitted by the Privacy Standards. If the Plan provides an accounting for such research disclosures, and if it is
reasonably likely that your PHI was disclosed for such research activity, the Plan shall, at your request, assist in contacting the entity
that sponsored the research and the researcher.
31
Notice of Privacy Practices
Page 7 of 9
If the accounting cannot be provided within 60 days after receipt of the request, an additional 30 days is allowed if the individual
is given a written statement of the reasons for the delay and the date by which the accounting will be provided.
If you request more than one accounting within a 12-month period, the Plan will charge a reasonable, cost-based fee for each
subsequent accounting unless you withdraw or modify the request for a subsequent accounting to avoid or reduce the fee.
You or your personal representative will be required to request an accounting of your PHI disclosures in writing. Such requests
should be addressed to the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
2.6 The Right To Receive a Paper Copy of This Notice Upon Request
You have a right to obtain a paper copy of this Notice upon request. To request a paper copy of this Notice, contact the
following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
2.7 A Note About Personal Representatives
You may exercise your rights through a personal representative. Your personal representative will be required to produce
evidence of his/her authority to act on your behalf before that person will be given access to your PHI or allowed to take any action for
you. Proof of such authority may include, but is not limited to, the following:
(a) a power of attorney for health care purposes, notarized by a notary public;
(b) a court order of appointment of the person as the conservator or guardian of the individual; or
(c) an individual who is the parent of a minor child.
The Plan retains discretion to deny access to your PHI to a personal representative to provide protection to those vulnerable
people who depend on others to exercise their rights under these rules and who may be subject to abuse or neglect. This also applies to
personal representatives of minors.
Section 3: The Plan's Duties
3.1 Notice
The Plan is required by law to maintain the privacy of PHI and to provide individuals (participants and beneficiaries) with
notice of its legal duties and privacy practices with respect to PHI.
This Notice is effective beginning on the effective date set forth on Page 1 of this Notice, and the Plan is required to comply
with the terms of this Notice. However, the Plan reserves the right to change the terms of this Notice and to make the new revised notice
provisions effective for all PHI that it maintains, including any PHI created, received or maintained by the Plan prior to the date of the
revised notice. If a privacy practice is changed, a revised version of this Notice will be provided to all individuals then covered by the
Plan. If agreed upon between the Plan and you, the Plan will provide you with a revised Notice electronically. Otherwise, the Plan will
mail a paper copy of the revised Notice to your home address. In addition, the revised Notice will be maintained on any web site
maintained by the Plan to provide information about its benefits.
Any revised version of this Notice will be distributed within 60 days of any material change to the uses or disclosures, the
individual's rights, the duties of the Plan or other privacy practices stated in this Notice. Except when required by law, a material change
to any term of this Notice may not be implemented prior to the effective date of the revised notice in which such material change is
reflected.
32
Notice of Privacy Practices
Page 8 of 9
3.2 Minimum Necessary Standard
When using or disclosing PHI or when requesting PHI from another covered entity, the Plan will make reasonable efforts not
to use, disclose or request more than the minimum amount of PHI necessary to accomplish the intended purpose of the use, disclosure
or request, taking into consideration practical and technological limitations.
However, the minimum necessary standard will not apply in the following situations:
(a) disclosures to or requests by a health care provider for treatment;
(b) uses or disclosures made to the individual;
(c) disclosures made to the Secretary of HHS.
(d) uses or disclosures that are required by law;
(e) uses or disclosures that are required for the Plan's compliance with the Privacy Standards; and
(f) uses or disclosures made pursuant to an authorization.
This Notice does not apply to information that has been de-identified. De-identified information is health information that does
not identify an individual and with respect to which there is no reasonable basis to believe that the information can be used to identify
an individual. It is not individually identifiable health information.
In addition, the Plan may use or disclose "summary health information" to the Plan Sponsor for obtaining premium bids or
modifying, amending or terminating the group health plan. Summary health information summarizes the claims history, claims expenses
or type of claims experienced by individuals for whom a plan sponsor has provided health benefits under a group health plan, and from
which identifying information has been deleted in accordance with the Privacy Standards.
Section 4: Your Right to File a Complaint With the Plan or the HHS Secretary
If you believe that your privacy rights have been violated, you may complain to the Plan. Any complaint must be in writing
and addressed to the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
You also may file a complaint with the Secretary of the U.S. Department of Health and Human Services in its Office of Civil
Rights ("OCR"). Complaints to the Secretary must: (1) be filed in writing, either on paper or electronically; (2) name the entity (i.e.,
the Plan) that is the subject of the complaint and describe the acts or omissions believed to be in violation of the applicable requirements
of the Privacy Standards; and (3) be filed within 180 days of when you knew or should have known that the act or omission complained
of occurred, unless OCR waives this time limit for good cause shown. You may file a written complaint with OCR by mail, fax or e-
mail at the address listed below. Further, you may, but are not required to, use OCR's Health Information Privacy Complaint Form. To
obtain a copy of this form, or for more information about the Privacy Standards or how to file a complaint with OCR, contact any OCR
office or go to www.hhs.gov/ocr/hipaa/.
Complaints may be filed via e-mail at the following e-mail address: [email protected]. Alternatively, written
complaints also may be filed at the following address:
Southeast Region - Atlanta (Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, Tennessee)
Timothy Noonan, Regional Manager
Office for Civil Rights
U.S. Department of Health and Human Services
Sam Nunn Atlanta Federal Center, Suite 16T70
61 Forsyth Street, S.W.
Atlanta, GA 30303-8909
Customer Response Center: (800) 368-1019
Fax: (202) 619-3818
TDD :(800) 537-7697
Email: [email protected]
The Plan will not retaliate against you for filing a complaint.
33
Notice of Privacy Practices
Page 9 of 9
Section 5: Whom to Contact at the Plan for More Information
If you have any questions regarding this Notice or the subjects addressed in it, you may contact the following individual:
Steve Zona or Randy Wyse
625 Stockton Street
Jacksonville FL 32204
904-759-7416 or 904-334-8470
Conclusion
PHI use and disclosure by the Plan is regulated by a federal law known as HIPAA. You may find these rules at 45 Code of
Federal Regulations Parts 160 and 164. This Notice attempts to summarize the Privacy Standards. The Privacy Standards will supersede
any discrepancy between the information in this Notice and the Privacy Standards.
34