Embed Size (px)
DESCRIPTION
Journal of Research and Education in Indian Medicine JREIM was aimed to aid the dissemination of important researches and theoretical works in different areas of common interest to the educators, researchers, specialized and general therapists of Indian Medicine, which includes Ayurveda, Yoga and Naturopathy, Unani, Sidhha, Homeopathy (AYUSH), CAM, Integrative Medicine, and other Traditional / Alternative / Oriental Systems of Medicine in general and Clinical research, researches on Medicinal Plants / Herbs, Spices and Pharmaceutical sciences in particular. The inaugural issue (Jan.-March 1982) of JREIM was released by Dr. Sombhong Kutranon, Regional Director, W.H.O. during International conference on “Role of Practitioners of Indian Medicines in Primary Health Care” at Institute of Medical Sciences, Banaras Hindu University, Varanasi, 20-22 February’ 1982.* JREIM maintained and is enjoying its nonaligned and independent academic status. For JREIM; the sole criterion for publishing i
Citation preview

Pretic Effect of Herbomineral Unani Formulation ( Dolabi )
Analysis of the Effect of Laksha Guggulu(An Ayurvedic Formulation) on Fracture Healing in a Rat Model
Ramesh Kaundal, Suman Sharma,Sanjeev Sharma and V.K. Gupta
Therapeutic Potentials of Minerals in Ancient India:A Review Through Charaka Samhita
Chandrashekhar Jagtap, Galib Ruknuddin,Prashant Bedarkar, Biswajyoti Patgiri and P.K. Prajapati
Evaluation of Eclectic Therapy on Fasting Blood Sugarin patients of Type-2 Diabetes Mellitus
Roohallah Bay, Sujata Vaydia andFatemeh Bay
Memory Loss in Geriatric Age and its Prevention Through Yogic LifestyleHetal Amin, Rohit Sharma,M.K. Vyas and R.R. Dwivedi
Clinical Evaluation of Varadi Kwatha in the Management ofMadhumeha (Type-2 Diabetes Mellitus) - An attempt to provide evidence baseddata to the classical therapeutic claims
Gyaneshwarsing Guddoye,B.K. Dwibedy and O.P. Singh
Immediate Hypoglycaemic Effect of Two Selective HydrotherapeuticProcedures in Non Insulin Dependent Patients of Diabetes Mellitus
Sujatha Dinesh and Gangadhara VarmaA Critical Understanding of Nutraceutical Aspects of Curd in Ayurveda
Priyanka B.V. and Mallika Kurat JayavarmaImpact of Shodhana on Physico-chemical and Chromatographical Profilesof Gunja (Abrus precatorius Linn.) Seeds
Sudipta Roy, Rabinarayan Acharya and V.J. Shukla
Volume XX : 1 eVersion Jan. - March, 2014
THE JOURNAL OFRESEARCH AND EDUCATION
IN INDIAN MEDICINE
ISSN 0970-7700

THE JOURNAL OF RESERCH AND EDUCATION IN INDIAN MEDICINE EDITORIAL ADVISORY BOARD
Editor-in-Chief Prof. R. H. Singh Distinguished Professor (Kayachikitsa) Formerly: Vice Chancellor, Rajasthan Ayurveda University, Jodhpur Professor and Head, Department of Kayachikitsa Dean, Faculty of Ayurveda, Institute of Medical Sciences Banaras Hindu University, Varanasi (India)
Founding Editor Prof. Suresh Kumar Formerly: Principal, Administrator and OSD, HP Inst. of PG Educ. & Res. in Ayurveda ( RGGPGAC-Paprola), Dean, Faculty of Ayurveda, H.P. University, Shimla Director, Indian Institute of Panchakarma (CCRAS, GoI), Karala OSD (Ay.), Department of Ayurveda, HP Government, Shimla (India).
Chief Editors
Prof. Rana Gopal Singh Director, Institute of Medical Sciences Banaras Hindu University, Varanasi
Prof. P.V.Tewari Formerly Professor and Head Dept of Prasuti Tantra, Dean, Faculty of Ayurveda, IMS, BHU, Varanasi
Prof. U.N. Dwivedi Professor of Biochemistry Ex-Vice Chancellor, University of Lucknow UP
Prof. Abhimanyu Kumar Director, All India Institute of Ayurveda, Delhi DG Incharge, C.C.R.A.S, New Delhi
Prof. Rabinarayan Acharya Professor of Dravyaguna, Institute for PG Teaching & Research in Ayurveda, GAU, Jamnagar, Gujarat
Prof. Anand Chaudhary Professor and HOD Department of Rasa Shastra & BK Faculty of Ayurveda, IMS, BHU, Varanasi, UP
Speciality Editors Panchakarma Prof. Girish K.J. (Hassan, Karnataka) Research & Education Prof. G.S. Lavekar (Delhi) Pharma. Sciences Prof. R.G. Mali (Ahmedabad) Shalakya Tantra Dr. Manoj Kumar (BHU, Varanasi) Kriya Sharira Dr. Kishor Patwardhan (BHU, Varanasi)
Shalya Tantra Prof. Manoranjan Sahu (BHU, Varanasi) Rasa Shastra & BK Dr Mukund Sabnis (Aurangabad, M.S.) Dravyaguna Prof. V.V. Prasad (RAV, Delhi) Kayachikitsa and CAM Dr. D.C. Katoch (AYUSH, Delhi) Sangyaharan Dr. K. K. Pandey (BHU, Varanasi)
Balroga Prof. Abhimanyu Kumar (AIIA, Delhi) Kayachikitsa Prof. Y.K. Sharma (Paprola, H.P.) Prasuti Tantra Prof. Eena Sharma (Paprola, HP) Shalya-Ortho Prof. Sanjeev Sharma (Paprola, H.P.) Vikriti Vigyan & Rog Nidan Dr. P.S. Byadgi (BHU, Varanasi)
Associate Editors Dr. Sanjeev Ojha (CDRI, Lucknow) Dr. K.Narasimha Murthy (BHU,Varanasi) Dr. Galib R. (GAU, Jamnagar)
Consultant Editors Prof. M. S. Baghel (GAU, Jamnagar) Prof. Subhash Ranade (Pune) Prof. A. Douglas Kinghorn (USA) Dr. Shrikant Mishra (USA)
Prof. K. R. Kohli (Mumbai) Prof. V. K. Joshi (BHU, Varanasi) Dr. Fred J. Evans (London) Dr. Shinji Funayama (Japan)
Dr. Jagat Kanwar (Australia) Dr. S. K. Sharma (Delhi) Dr. V. N. Pandey (Delhi) Dr. Marc Halpern (California)
Scientific Advisory Committee
Prof. N. P. Rai (BHU, Varanasi) Prof. Sanjay Gupta (BHU, Varanasi) Dr. G. S. Badesha (Raipur, Chhattisgarh) Dr. Sudhir Kumar (Chandigarh) Dr. Ramniwas Prasher (Delhi) Dr. Baldev Kumar (NIA, Jaipur)
Prof. Manjari Dwivedi (BHU, Varanasi) Prof. P. K. Devnath (Kolkata) Dr. S. K. Mishra (Delhi) Dr. K. S. Varier (Coimbatore) Dr. L. Kohout (Czechoslovakia) Dr. Anirudh Tripathi (Mumbai)
Prof. Y. B. Tripathi (BHU, Varanasi) Prof. S. I. Nagral (Mumbai) Dr. H. S. Kasture (Ahmedabad) Dr. Ashwinikumar Raut (Mumbai) Dr. Sudhakar Powar (Mumbai) Dr. Kuldeep Singh Panwar (Jalandhar)
Assistant Editors Dr. Anagha Ranade (GAU, Jamnagar) Dr. Samita Puri (Delhi) Dr. Shweta Dewan (NIA, Jaipur) Dr. Neetu Singh (BHU,Varanasi)
Dr. Rasika Kolhe (GAU, Jamnagar) Dr. Pravesh Puri (BHU, Varanasi) Dr. Gangadhar Varma (Karnataka) Dr. Rohit A.Gokarn (Jamnagar)
Dr. Aditya Puri (Hamirpur, H.P.) Dr. Garish Mishra (Varanasi) Dr. Davinder Singh (Hoshirpur) Dr. Vinamra Sharma (BHU, Varanasi)
Executive Editor: Dr.(Mrs.) Laxmi Bhargava, Ph.D. (BHU) Admin. Office: B 29/19 Lanka, Sankat Mochan Road, PO: BHU, Varanasi -221005 UP (India) E-mail: [email protected] Mob. 09305180763, 09418458257 and 09816043362
Annual Subscription Libraries and Institutions: Rs. 3000/- (India ) US$ 275/- (Foreign)* Individuals: Rs. 2000/- (India ) US$ 100/- (Foreign)*
UG/PG/PhD Students and JREIM Authors: Rs. 1600/- (India only) * Subscription rates are exclusive of postage.
*Please add Rs.200/ extra (Registered postage and packing in India) * US Dollars 75/ (Air Mail Registered delivery outside India)
The Bank draft drawn in name of “The Journal of Research and Education in Indian Medicine” with covering letter be posted under Registered/ Speed Post to Manager, Admin. Office, The Journal of Research and Education in Indian Medicine, B.29/19, Lanka, SM Road, P.O.: BHU, Varanasi-221005 (India)
Online PaymentPayment through Electronic Fund transfer - Subscription can be deposited directly in Journal’s Bank Account
MCA Current A/C No 10654902251 - IFS Code: SBIN0000211 - MICR: 221002003 Branch Code: 00211 State Bank of India (00211), BHU Branch. The copy of deposit receipt be posted with subscription order to Manager, at above JREIM Admin. Office address at Varanasi (India)
For more details visit http://www.jreim.com and register via Online Management System of ScopeMed.org on http://www.my.ejmanager.com/jreim

NLM ID : 8602438 (NlmId) ISSN : 0970-7700 (Print) 0970-7700 (Linking)
THE JOURNAL OF RESEARCH & EDUCATION IN INDIAN MEDICINEJournal of Research and Education in Ayurveda, Yoga, Naturopathy, Unani, Siddha, Homeopathy,Complementary and Alternative Medicine, Integrative Medicine, Medicinal and Aromatic Plants,
Pharmaceutical Sciences …… An International Quarterly
Call for Authors
The Editorial Board of The Journal of Research and Education in Indian Medicine (JREIM)(Website: www.jreim.com/aboutus.htm ) is interested in receiving and reviewing manuscripts in all areas of Researchand Education in Ayurveda, Yoga, Naturopathy, Unani, Siddha, Homeopathy, CAM, Integrative Medicine, Medicinalplants and Pharmaceutical Sciences in general and on education of AYUSH sector in particular.
Papers submitted for consideration for publication in The Journal of Research and Education in Indian Medicine(JREIM) will be reviewed by at least two expert members of the Editorial Review Board with appropriate credentialsand expertise in the specific topic covered. On our web site click on the links under the “Information for Authors” sectionfor complete guidelines for authors and submission requirements. Manuscripts can be electronically submitted by e-mailto [email protected] or any Subject Editor
The Journal of Research and Education in Indian Medicine (JREIM) invites submission of Review articlesand research papers in all areas of Research & Education in Ayurveda, Yoga, Naturopathy, Unani, Siddha, Homeopathyand other Traditional/Alternative/Oriental Systems of Medicine. The sole criterion for publishing is academic andscientific accuracy.
We invite anyone who is involved in research in any relevant area to submit his or her manuscript for considerationof publication. The Journal of Research and Education in Indian Medicine (JREIM) is committed to rapid review andpublication. Your manuscript will be published, once accepted, within 90 days of acceptance.
An Invitation to Subscribe the JournalWe hope that after examination of our Journal and other JREIM publications, you will decide that some or all
of these publication merit being recommended to your main or departmental library for current subscription and foracquisition of Special Issues of some of the back volumes.
If you have any questions, please submit them through our website: www.jreim.com/aboutus.htm or e-mail [email protected]
Prof. Suresh Kumar Prof. Em. R.H. SinghFounder Editor Editor-in-Chief
* The manuscripts submitted in proper JREIM format/typesetting/style are only Registered for publication and assigned Manuscript Number and Reviewers


EDITOR-IN-CHIEFProf. R.H. SINGH ABMS, Ph.D, D.Sc.Distinguished Professor-KayachikitsaFormerly Vice Chancellor,Rajasthan Ayurveda University;Dean, Faculty of Ayurveda,Institute of Medical Sciences,BHU, Varanasi - 221005 UP (India)CHIEF EDITOR (SPECIAL ISSUES)Prof. Rana Gopal Singh MD, DM (BHU)DirectorInstitute of Medical Sciences,B.H.U. Varanasi 221005 UP (India)E-mail : [email protected] EDITOR (DRAVYAGUNA)Prof. Rabinarayan Acharya Ph.D. (GAU)Professor of DravyagunaMember Secretary, National Pharmaco-vigilance programme for ASU drugsInstitute for PG Teaching & Research inAyurveda, Gujarat Ayurved University,Jamnagar-361 008, Gujarat, IndiaFOUNDING EditorProf. Suresh Kumar M.D.(Ay), Ph.D (BHU)Formerly Dean, Faculty of Ayurveda,Himachal Pradesh University, ShimlaDirector, Indian Institute of Panchakarma,CCRAS (AYUSH, MoH&FW, GoI) (Kerala)CONSULTANT SUBJECT EDITORSDr. Manoj Kumar M.S.(Ay.),Ph.D (BHU)Assistant Professor-Shalakya TantraInstitute of Medical Sciences,BHU, Varanasi - 221005 (India)Prof. Ravindra G. Mali M.Pharm, DHMM,Principal, Shree Swaminarayan College ofPharmacy, Kalol, Gandhinagar (Gujarat)
ADVISORY-EDITORS (INTERNATIONAL)Dr. Jagat Kanwar M.Sc., Ph.D.Asso.Professor, Immunology & CellBiology, Institute for Technology &Research Innovation (ITRI), DeakinUniversity, Victoria - 3217 (Australia)Dr. Marc HalpernPresident, California College of AyurvedaE-mail: [email protected] EDITORSDr. Anagha Ranade (GAU, Jamnagar)Dr. Neetu Singh (BHU,Varanasi)Dr. Rasika Kolhe (GAU, Jamnagar)Dr. Samita Puri (CBPCAS, Delhi)Dr. Shweta Dewan (NIA, Jaipur)Dr. Vinamra Sharma (BHU, Varanasi)
JREIM ADMIN. OFFICE:Dr. (Mrs.) Laxmi Bhargava Ph.D. (BHU)Executive EditorE-mail: [email protected]
Standard International ISO Abbreviation of JREIM is: J. Res. Educ. Indian. Med.
J Res Educ Indian Med, Jan.-March 2014; XX (1): 1-66 ISSN 0970-7700 (Linking)
CONTENTS
Our Guru ji - Acarya Dr. Rama Nath DwivediSuresh Kumar and R.G. Singh ... ii
Analysis of the Effect of Laksha Guggulu(An Ayurvedic Formulation) on Fracture Healingin a Rat Model
Ramesh Kaundal, Suman Sharma,Sanjeev Sharma and V.K. Gupta ... 01-08
Therapeutic Potentials of Minerals in Ancient India:A Review Through Charaka Samhita
Chandrashekhar Jagtap, Galib Ruknuddin,Prashant Bedarkar, Biswajyoti Patgiriand P.K. Prajapati ... 09-20
Evaluation of Eclectic Therapy on Fasting Blood Sugarin Patients of Type-2 Diabetes Mellitus
Roohallah Bay, Sujata Vaydia andFatemeh Bay ... 21-27
Memory Loss in Geriatric Age and its Prevention ThroughYogic Lifestyle
Hetal Amin, Rohit Sharma,M.K. Vyas and R.R. Dwivedi ... 29-35
Clinical Evaluation of Varadi Kwatha in theManagement of Madhumeha (Type-2 Diabetes Mellitus)- An attempt to provide evidence based data to theclassical therapeutic claims
Gyaneshwarsing Guddoye,B.K. Dwibedy and O.P. Singh ... 37-44
Immediate Hypoglycaemic Effect of Two SelectiveHydrotherapeutic Procedures in Non Insulin DependentPatients of Diabetes Mellitus
Sujatha Dinesh and Gangadhara Varma ... 45-50A Critical Understanding of Nutraceutical Aspectsof Curd in Ayurveda
Priyanka B.V. & Mallika Kurat Jayavarma ... 51-57Impact of Shodhana on Physico-chemical andChromatographical Profiles of Gunja(Abrus precatorius Linn.) Seeds
Sudipta Roy, Rabinarayan Acharyaand V.J. Shukla ... 59-65
Conferences and Fourth coming Events ... 66

Acharya Dr. Rama Nath Dwivedi M.A., A.M.S. (BHU), Ph.D., D.Sc.Former Head, Department of Ayurveda,Institute of Medical Sciences, BHU, Varanasi UP (India)
Founder Managing EditorThe Journal of Research and Education inIndian Medicine - An International Quarterly
Our Guru JiAcharya Dr. Rama Nath Dwivedi, who
left his earthly abode on January 11, 2014 (PaushShukla Ekadashi, an auspicious day as per Indiancalendar) at the age of around 96 years – wasa prime source of inspiration for all of us.
“It is eternal victory for the sacredone, from whose hands flows ‘Nectar’, whohas patience, who is learned and whose famousform has no fear of aging and death.”
He was born in the second decade of thetwentieth century in village ‘Arati Dube kaChhapara’ (Ojhavalia, Balia, U. P.) as the secondson of father Pandit Anmol Dubey and motherParamajyoti Devi. After initial education in aneighbourhood school at ‘Basarikapur’, he movedalong with his elder brother Acharya Dr. HazariPrasad Dwivedi to ‘Shantiniketan’, where hestudied for about two years in the inspiringpresence of ‘Gurudev Rabindranath Tagore’.
He pursued further education at ‘Kashi’(Varanasi) including ‘Ayurvedacharya in Medicineand Surgery (A. M. S.) Degree at B.H.U., hejoined service in Hindu University during regimeof ‘Dr. S. Radhakrisnan’ Vice-Chancellor. From1940 to 1980 (till his retirement), he taught‘Ayurveda’ to the students and treated a largenumber of patients in SS Hosptial at BHU by theconventional wisdom of our ancient Rishis, inthe true spirit of compliance to the wishes of‘Mahamana Pandit Madan Mohan Malaviya’,the founder of the Banaras Hindu University.
Recognized as ‘Ayurveda Brihaspati’at young age, our Guru ji , during his self-disciplined, hard and devoted life, gave knowledge
to thousands of disciples and gift of life tohundreds of thousands people.
His day started with early morning bathingin the Ganges (well before the sunrise) followedby daily worship and recitation of ‘Shrimad-Bhagavata’. He was mostly the first Doctor/Professor to reach the Hospital or the College.Timely meals and going to bed early, were thefeatures of his daily routine. He authored morethan thirty books on Ayurveda, many of whichare included in the syllabus of Ayurvedic Colleges.
“Pandit Rama Nath Dwivedi is famousas a Doctor with unfailing diagnosis, a prescriberof exactly right medicine and a selfless giver. Amuch talked about Ayurvedic physician, he is alegend who is the subject of many popular storiestold in the region.
Guru Ji, always lived the life of a sage andthe hardest obstacles in his life used to surrenderagainst his strong will-power. Bathing in theGanges in the early morning every day at ‘KedarGhat’, stepping down and up the steep stairs atthe Ghat, visiting the ‘Kedareshwar Mahadev’temple over there, which he did right from theearly age of 19 years to the ripe old age of 90years, is hardly possible for anyone else.
Finally he, with eternal ‘Bhakti-Bhava’, merged into the infinite glow of the Almighty.
Prof. Rana Gopal SinghDirector, IMS,Banaras Hindu University,Varanasi UP (India)Chief Editor JREIM
Prof. Suresh KumarFormer Dean, Ayurveda,Himachal University,Shimla HP (India)Founder Editor JREIM
J Res Educ Indian Med. Vol. XX (1) Jan.- March 2014 ii

J Res Educ Indian Med, Jan.-March 2014; Vol.XX (1): 1-8 ISSN 0970-7700
ANALYSIS OF THE EFFECT OF LAKSHA GUGGULU(AN AYURVEDIC FORMULATION) ON FRACTURE HEALINGIN A RAT MODELRAMESH KAUNDAL,1 SUMAN SHARMA,2 SANJEEV SHARMA3 AND V.K. GUPTA4
P. G. Department of Shalya Tantra 1,2,3
Rajiv Gandhi Govt. P. G. Ayurvedic College, Paprola - 176115 H.P. (India)Department of Veterinary Pathology 4Dr. G. C. Negi College of Veterinary and Animal Sciences, Palampur - 176062 H.P. (India)
Abstract: Objectives: Laksha Guggulu, an Ayurvedic formulation advocated to enhance thefracture healing in ancient Indian texts, was selected to validate its effect on fracture healing oncertain scientific parameters like Radiological, Serological and Histopathological studies in anexperimental rat model. Methods: Eighteen Wistar rats (Rattus norvegicus) were taken to createidentical fractures by a transverse osteotomy of Radial bone of their left fore limb under Ketamineand Xylazine anesthesia (intraperitoneally). Intact ulna acted as an internal splint hence, no otherexternal or internal support to the fractures was given. Post operatively injectable antibiotic(Gentamicin) was given. These osteotomised rats were divided into three groups of six each. GroupI rats were given 13.5mg/100gm body weight of the trial drug (Laksha Guggulu) twice daily throughoral route. Group II rats were given half of the Group I dose of the trial drug whereas in GroupIII, no drug was given (Control group). The drug was given oraly with Cow’s milk. Total durationof trial was of four weeks. Healing was assessed Radiologically, Biochemically and Histopathologically.Results: Assessment of results was done according to pre-designed protocol and data analysis donestatistically. Histopathological and Serological studies revealed significant results in Group I animalsas compared to Group II and Group III. Radiologically the difference between the groups wasnot detectable. Conclusion: Laksha Guggulu has got a definite role in the enhancement of fracturehealing by forming early and improved quality of the callus. However, further studies on largesample size, with more advanced investigations like Histomorphometery, Bone turnover markersand Micro CT scanning are required.
Keywords: Fracture healing, Histopathology, Laksha Guggulu, Rat model.
IntroductionA cursory glance of the available medical
treatise reveals that Ayurveda has spread enoughthought to the care of injured (Sushruta Samhita).Treatment of skeletal injuries has been givenprime importance. As without proper treatmentthese injuries can disable a person for rest oflife. Since Vedic period, surgeons are ponderingover skeletal injuries and are trying to overcometheir complications. Acharya Sushruta hasdescribed detailed etiology, classification,management and prognosis of bone and jointinjuries. He has also described various measuresincluding drugs to hasten the healing process.
For the management of fracture, reduction andimmobilization are universally required and to bedone accordingly (Sushruta Samhita). Butattention also be paid to avoid or minimize theforthcoming complications due to fracture itselfor immobilization. Reduction in fracture healingtime, when achieved will reduce complications.
The healing is a natural process and itoccurs spontaneously. But sometimes, healing isdelayed or bone ends fail to unite because offactors like improper immobilization, deficiencyconditions, reduced blood supply to the fracturedpart, severe soft tissue damage (Abdelhamid H.Elgazzae, 2004), smoking (Mara L. Schenker
1. P.G. Scholar 2. Sr. Lecturer 3. Professor, Shalya Tantra 4. Professor, Department of Veterinary Pathology

Kaundal et al.2
et al., 2013), endocrinal disorders and continuousnerve irritation (Henery Turner, 1936).
To overcome this problem and to minimizethe healing period, various drugs or formulationsfor local, oral use have been advocated inAyurvedic literature (Sushruta Samhita,Chakradatta and Yogratnakara). These drugsare claimed to enhance fracture healing process.Laksha Guggulu (Yogratnakara) is one of themwhich is advocated to promote fracture healing.
Laksha Guggulu is a classical Ayurvedicformulation containing Laksha Churna (Shellacpowder), Asthishrinkhla (Cissus quadrangularisLinn.), Arjun Twak Churna (Bark powder ofTerminalia arjuna), Ashwagandha Churna (Rootpowder of Withania somnifera), Nagbala MoolChurna (Root powder of Grewia hirsuta) andGuggulu (gum resin of Commiphora mukul).Among these ingredients Cissus quadrangularisLinn. is of utmost importance. Cissusquadrangularis alone is also used as a singledrug for promoting fracture healing since ancienttimes. Its fracture healing potential has alsobeen scientifically validated earlier by Udupa,1962; Udupa and Prasad, 1964; Chopra etal.,1976.
In this study, the scientific evaluation ofLaksha Guggulu formulation, as fracture healingdrug in a rat model on parameters likeradiography, serum alkaline phosphatase andhistopathology of fracture callus was planned.
Materials and MethodsMethod of Drug Preparation
Well identified ingredients were taken inequal quantity and fine powder of each wasprepared separately except Guggulu. All thesepowered contents were mixed properly. Further,purified Guggulu of equal weight was addedand mixed. Laksha Guggulu was prepared inthe College Pharmacy as per the AyurvedicFormulary of India (AFI).
Experimental AnimalsEighteen Wistar rats (Rattus norvegicus)
of either sex more than three months of age,
weighing between 150-250 gm were procuredfrom reliable source. Animals were fed oncommercially available standard balanced rat feed.All the animals were acclimatized to laboratoryconditions for one week prior to the trial. Theywere maintained at 12 hrs light cycle with roomtemperature at 15oC + 5oC in well ventilatedanimal house.
Experimental ProtocolFor osteotomy purpose, rats were shifted
to operation theatre of the department and all theoperative works were done under asepticconditions. Rats were anaesthetized with inj.Ketamine (60mg/kg) and inj. Xylazine (8mg./kgbody weight) intraperitoneally.
A cranio-medial incision was applied overthe left fore-limb and open transverse osteotomyof left radial bone was done. As only radial boneof fore limb was osteotomised (fractured) andulna acted as a splint. Hence, no external splintwas applied. Post operative antibiotic(Inj. Gentamicin by I. M. route 12 hourly) forseventy-two hours of post operative period wasgiven. All doses including antibiotic and trial drugwere calculated by using conversion factor i.e. adose for a rat of 200gm weight = 0.018 × Humanadult dose.
After creating similar fractures on similarbones in all 18 animals, they were divided intothree groups (six animals in each group). Toidentify each animal they were marked on tailwith code number. The cages were also labeledas group I, group II and group III respectively.
Group I: This group was fed with LakshaGuggulu dissolved in 1ml of cow’s milk in doseof 13.5 mg per 100gm body weight. The drugwas given through intragastric route 12 hourlywith the help of soft baby feeding tube of No.10 size.
Group II: Second group was fed withhalf of the dose of group I, dissolved in 1ml ofcow’s milk, given through intragastric route 12hourly with the help of soft baby feeding tube ofNo. 10 size.
Effect of Laksha Guggulu on Fracture Healing 3
Group III: Only 1ml of cow’s milk wasgiven through intragastric route 12 hourly. Thisgroup was kept as a control group.
Total duration of trial was Four weeks.Investigations used were:
1. X-rays of operated limb.2. Serum alkaline phosphatase study.3. Histopathology of the callus.
As the operated limb needed to bedisarticulated for histopathology, so euthanasiaof the animals was inevitable and done accordingto international guidelines. Inhalation agentHalothane was used in high doses for euthanasia.
After euthanizing, blood samples werecollected from all the animals, directly from heartfor serum alkaline phosphatase study. Cranio-caudal and lateral radiographs of osteotomisedanimal limbs of all the three groups were takenfor radiological assessment. Operated limbs weredisarticulated and histopathological study of thecallus done.
The segments were placed in bufferedneutral 10% formalin for three days, followedby decalcification with Stewart and Gooding fluid.Specimens were processed for making paraffinblocks and 5-6 micro meter thick tissue sectionswere stained with Hematoxylene Eosin (H & E)and Masson’s trichrome stains. An eleven pointscale based on the amount of fibrous tissue,cartilaginous tissue and woven bone in callusformation was used to evaluate the degree ofhealing process.
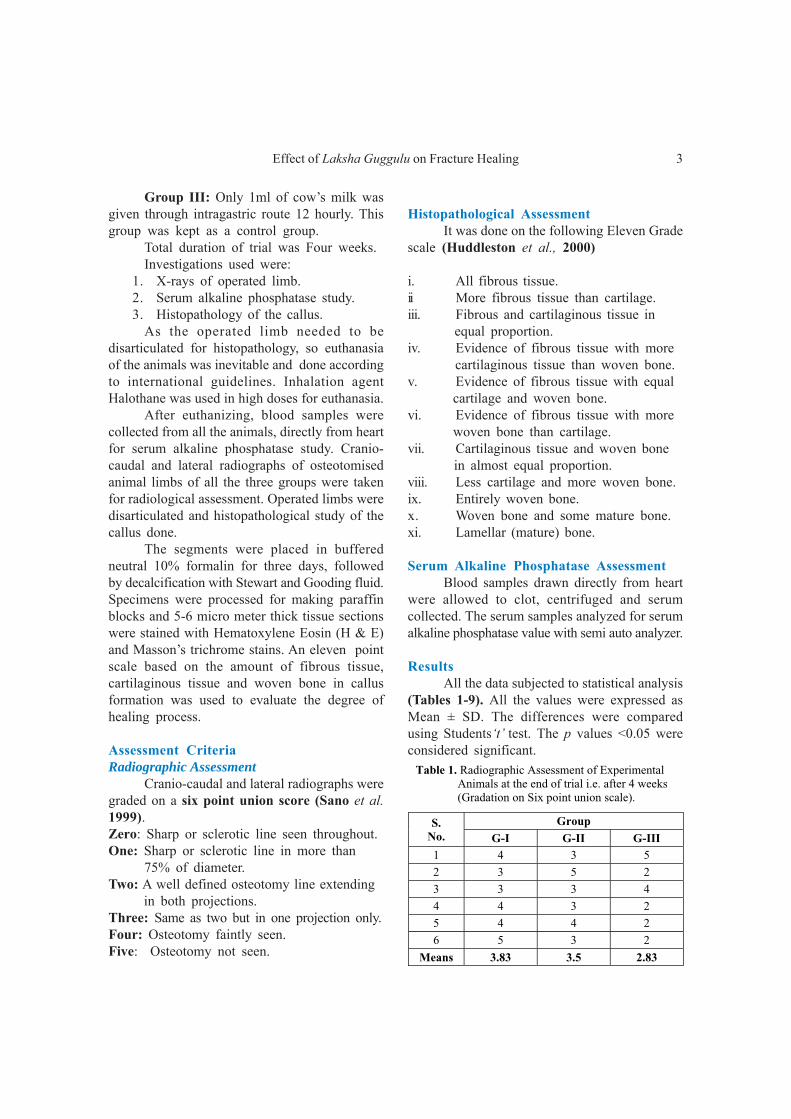
Assessment CriteriaRadiographic Assessment
Cranio-caudal and lateral radiographs weregraded on a six point union score (Sano et al.1999).Zero: Sharp or sclerotic line seen throughout.One: Sharp or sclerotic line in more than 75% of diameter.Two: A well defined osteotomy line extending in both projections.Three: Same as two but in one projection only.Four: Osteotomy faintly seen.Five: Osteotomy not seen.
Table 1. Radiographic Assessment of Experimental Animals at the end of trial i.e. after 4 weeks (Gradation on Six point union scale).
S. No.
Group
G-I G-II G-III 1 4 3 5
2 3 5 2
3 3 3 4
4 4 3 2
5 4 4 2
6 5 3 2
Means 3.83 3.5 2.83
Histopathological AssessmentIt was done on the following Eleven Grade
scale (Huddleston et al., 2000)
i. All fibrous tissue.ii More fibrous tissue than cartilage.iii. Fibrous and cartilaginous tissue in equal proportion.iv. Evidence of fibrous tissue with more cartilaginous tissue than woven bone.v. Evidence of fibrous tissue with equal cartilage and woven bone.vi. Evidence of fibrous tissue with more woven bone than cartilage.vii. Cartilaginous tissue and woven bone in almost equal proportion.viii. Less cartilage and more woven bone.ix. Entirely woven bone.x. Woven bone and some mature bone.xi. Lamellar (mature) bone.
Serum Alkaline Phosphatase AssessmentBlood samples drawn directly from heart
were allowed to clot, centrifuged and serumcollected. The serum samples analyzed for serumalkaline phosphatase value with semi auto analyzer.
ResultsAll the data subjected to statistical analysis
(Tables 1-9). All the values were expressed asMean ± SD. The differences were comparedusing Students‘t’ test. The p values <0.05 wereconsidered significant.

Kaundal et al.4
Table 2. Comparison of groups for Radiographic assessment at the end of 4 weeks.
S. No.
Group. Number Mean S.D. SEM
1 I 6 3.83 0.97 0.3960
2 II 6 3.5 0.8366 0.3416
3 III 6 2.83 1.328 0.542
Table 3. Inter group Comparison
Group Group ‘t’ value
D.F. P value
I II 0.629 10 P> 0.05
I III 1.041 10 P> 0.05
II III 1.047 10 P> 0.05
Table 4. Histopathological Assessment of Calluses - after 4 weeks.$
S. No. G-I G-II G-III 1 6 - 4
2 6 6 -
3 6 4 4
4 6 - 4
5 5 5 -
6 5 6 5
Means 5.66 5.25 4.25 Indicates that sample couldn’t be obtained for study
$ Gradation on 11 point Histopathological Assessment Scale
Table 5. Comparison of Histopathological assessment of Callus at end of 4 weeks.
S. No.
Group n Mean S.D. SEM
1 I 6 5.66 0.5164 0.2108
2 II 4 5.25 0.9573 0.4786
3 III 4 4.25 0.5 0.25
Table 6. Inter Group Comparison
Group Group ‘t’ value
D.F. P value
I II 0.888 8 P >0.05
I III 4.36 8 P <0.01
II III 1.852 6 P >0.05
Table 7. Alkaline phosphatase values of experimental animals after 4weeks (all values are in u/l).
S. No. Group-I Group-II Group-III
(Control) 1 270 319 117.42
2 390.4 230.7 186.6
3 420.2 162.2 252.3
4 396.4 270 172.08
5 170 180 144.16
6 370 300 137.2
Means 336.16 243.65 168.29
Figure 1. Graphical presentation of mean ofRadiographic Gradation of all Groups.
DiscussionPresent study is an effort to assess the
effect of Laksha Guggulu in fracture healing ina rat model. Statistical analysis of the resultsobtained shows that Laksha Guggulu enhances
Table 8. Comparison of Groups for Serum Alkaline Phosphatase values of all Groups after 4 weeks.
No. G n Mean S.D. SEM 1 I 6 336.1667 96.7109 39.48
2 II 6 243.65 63.875 26.078
3 III 6 168.293 48.049 19.616
the fracture healing process. The comparison ofGroup-I with other groups shows statisticalsignificant results (Tables 1-9).
In radiographic assessment the resultsobtained are non significant in all groups incomparison to the control group. Inter group
Table 9. Inter Group Comparison
Group Group ‘t’ value D.F. P value 1 2 1.95 10 P <0.05
1 3 3.81 10 P< 0.01
2 3 2.31 10 P <0.05

Effect of Laksha Guggulu on Fracture Healing 5
2.a 2.b
3.a 3.b
4.a 4.b

Kaundal et al.6
comparison also shows no significant results(Tables 1-3, Fig. 1). The cause of non significantresults might be poorly defined shadow of calluson radiographs. It is hypothesized that the callusso formed has not casted its shadow very well.The analysis of serum alkaline phosphatase valueand histopathology of calluses proved the efficacyof appropriate dose of Laksha Guggulu on bonehealing.
The histopathological study (conducted atCollege of Veterinary and Animal SciencesPalampur, H.P.) of all groups reveals that thecalluses of group-I were containing more part ofwoven bone (immature bone) than cartilage andfibrous tissue (Fig. 2 a,b). Group-II specimensrevealed equal amount of cartilage and wovenbone (Fig. 3 a,b). Whereas, group-III showedmore amount of fibrous and cartilaginous tissuethan woven bone (Fig. 4 a,b). Statistically resultswere also significant in Group-I than Groups IIand III (Tables 4-6, Fig. 5). Hence, it is clearthat the drug Laksha Guggulu accelerates fracturehealing.
The serum alkaline phosphatase iscomposed of a group of iso-enzymes whichoriginate from liver, bone and to a minor extentfrom the intestine and placenta. It functionsprincipally at the site of absorption, depositionand excretion of calcium and also phosphorus.In bones it is concentrated at the main points ofossification (i.e. the epiphyseal line and the sub-periosteal area). During the active bonedestruction (as in fracture) a compensatorystimulation of osteoblasts to replace bone isreflected in an increased intra cellular content ofalkaline phosphatase and increased levels in bloodstream. During fracture repair, osteoblasts try tofill up the gap and cause increased serum alkalinephosphatase value. The increased serum alkalinephosphatase is also found in patients with certaindiseases like Paget’s disease, hyperparathyroidism,rickets, osteoblastic osteogenic sarcoma anddiseases of liver. Because, animals used werehealthy and screened out for any disease, so thepossibility of alkaline phosphatase rise due toany such pathology was ruled out. Hence, the
Fig. 6. Diagram of Mean of Alkaline Phosphatase values.
Fig. 5. Diagram of Mean of Histopathological Assessmentof Callus as per 11 scale grading.
increase in serum alkaline phosphatase value ingroup-I was due to Laksha Guggulu. The resultsfound were statistically highly significant (Tables7-9, Fig. 6).
Formulation Laksha Guggulu containsGuggulu as a main ingredient. Guggulu is gumresin of a shrub named Commiphora mukulEngl. This resin is having anti-inflammatory,analgesic (Jain and Gupta 2006) as well asbone healing properties (Bhavaprakasha).Another important ingredient of this formulationis Cissus quandrangularis which has beenadvocated to promote the fracture healing inAyurvedic classics (Bhava Prakasha). This plantis found to contain vitamins and steroid likevarious versatile constituents such as flavonoids,

Effect of Laksha Guggulu on Fracture Healing 7
triterpenoids, vitamin C, stilbene derivatives andmany others. (Adsenya et al., 1999). Out of theseascorbic acid, triterpene, α-sitosterol, ketosteroids,triterpenoids and calcium were found to havespecific effect on the bone healing (Chopra et al.,1975, 1976: Udupa and Prasad 1963 and 1964,).Cissus quandrangularis also contains anti-oxidantand anti microbial properties (Murthy et al., 2003:Deka and Lohan 1994). Arjuna (Terminalia arjunaRoxb.) however, is having cardio-protectiveproperties but the methanol extract also containsanalgesic and anti-inflammatory properties(Moulisha Biswas et al., 2011). Studies have alsorevealed bone healing potential of this plant (SinghH., 1992). Ashwagandha (Withania somnifera (L)Dunal) is mainly an immunomodulator andimmunoprotective drug but is also having analgesicproperties (Sahni and Srivastava 2011) and somegood effect on bone healing (Jaiswal et al., 2004).Grewia hirsuta is a general and nervine tonic (BhavaPrakasha) whereas Laksha (Shellac powder) isalso having healing effect upon Kshata (tissueinjuries) (Bhava Prakasha). On the basis of theproperties of individual ingredients of theformulation under study (Laksha Guggulu) it canbe well assumed that this should be helpful inenhancing the bone healing process. This studyalso revealed that Laksha Guggulu potentiatesthe bone healing process in rats.
ConclusionOn the basis of this experimental work it
can be concluded that the drug Laksha Gugguluenhanced the fracture healing process and canbe used as an adjuvant therapy to promote thefracture healing. However, further studies on largesample size, with more advanced investigationslike histomorphometery, Bone turnover markersand Micro CT scanning are required.
References1. Abdelhamid H. Elgazzae. Orthopedic Nuclear
Medicine, Germany, Springer - Verlag Heidlberg,2004;107.
2. Adesanya, Saburi A., Rene N., Martin M.Therese, Boukamcha, N., Montagnac, A. andPais M. Stilbene derivatives from Medicinal Plant
-Cissus quadrangularis. J. Nat. Prod.1999;62:1694-95.
3. Bhavaprakasha Nighantu. Translator andcommentator Pandit Shri Vishwanath DwivediShastri, 9th edition.Varanasi, Moti Lal BanarsiDass,1977.
4. Chakaradatta. Commentary and translation byProf. P.V. Sharma. (Bhagna Chikitsa 49-12/13).Varanasi, Chaukhambha Subharti Prakashan, 1994.
5. Chopra, S. S., Patel, M. R. and Awadhiya. R.P. Studies of Cissus quadrangularis inexperimental fracture repair: a histopathologicalstudy. Indian J Med Res 1976;64:1365-68.
6. D.K. Deka and L.C. Lahon. Effect of Cissusquandrangularis in accelerating healing process ofexperimentally fractured Radius-Ulna of Dog, Apreliminary study. Indian Journal of Pharmacology1994;26:44-45.
7. Henery Turner. Some thoughts on the probablecauses of non-union of fractures. J Bone JointSurg Am 1936;18(3):581-93.
8. Huddleston P.M., Steckelberg J.M., HansenA.D., Rouse M.S., Bolander M.E. and Patel R.Ciprofloxacin in inhalation of experimental fracturehealing. JBJS Am 2000;82:161-73.
9. Jain Anurekha and Gupta V. B. Chemistry andPhrmacological profile of Guggul – a review: IndianJournal of Traditional Knowledge 2006;5(4):18.
10. K.N.Udupa and Gurucharan Prasad. Bio-mechanical and calcium 45 studies on the effect ofCissus quandrangularis in fracture repair. IndJour Med Res 1964;52.
11. K.N. Udupa and Gurucharan Prasad. Effect ofCissus quadrangularis on the healing of Cortisonetreated fractures. Ind Jour Med Res 1963;51.
12. K.N. Udupa and Gurucharan Prasad. Furtherstudies on the effect of Cissus quandrangularisin accelerating fracture healing. Ind Jour Med Res1964;52.
13. K.N. Udupa. Cissus quandrangularis in fracturehealing of fractures a clinical study, Indian MedicalAssociation 1962;38.
14. Mara L. Schenker, John A. Scolaro, Sarah M.Yannascoli, Keith D. Balwin, Samir Mehtaand Jaimo Ahn. Smoking Associated withFracture Non union, Longer Healing times,Presented in AAOS annual meeting on Friday,Mar 22, 2013, Organized by J Bone Joint SurgAm 2013.
15. Moulisha Biswas, Kaushik Biswas, Tarun K.Karan, Sanjib Bhattacharya, Ashok K. Ghosh

Kaundal et al.8
and Pallab K. Haldar. Evaluation of Analgesicand anti-inflammatory activities of Terminaliaarjuna leaf. J of Phytology 2011;3(1):33-38.
16. Murthy, K. N. C., Vanitha, A., Swami, M. M.and Ravishankar G. A. Antioxidant andantimicrobial activity of Cissus quadrangularisLinn. J Med Food 2003;6:99-105.
17. Sano H., Unthoff H.K., Backman D.S. andYeadong A. Correlation of radiographicmeasurements with biomechanical test results. ClinOrthop 1999;368:271-78.
18. S. Jaiswal, S.V. Singh, Bhoopendra Singh and H. N.Singh. Plants used for tissue healing of animals.Natural Product Radiance 2004;3(4):284-90.
19. S.S. Chopra, M.R.Patel, L.P.Gupta and I.C.Datta. Studies on Cissus quadrangularis inExperimental fracture repair: Effect on ChemicalParameters in blood. Ind J Med Res 1975;63.
20. Sahni Y.P. and Srivastva D.M. Analgesic activityof Withania somnifera – A possible mode of action.Indian Vet Med J 2011;25(2):153-55.
21. Singh H. Terminalia and Coelogyne crista in therepair of canine fracture, Ph. D. Thesis- G.B. PantUniversity of Agri. & Technology, Pantnagar, 1992.
22. Sushruta Samhita. Nibandhasamgraha (NidanSthana 15 and Chikitsa Sthana 3) Dalhancommentary. Varanasi, Chaukhambha SubhartiPrakashan 1994.
23. The Ayurvedic Formulary of India. Govt. ofIndia Dept. of AYUSH, Part–I, 2nd revised editionGroup no. 5 Guggulu. 2000; pg 70.
24. Yogaratnakara. Translator and Commentator(Hindi) Vaidya Shree Laxmipati Shastri, EditorBhishagratna Shree Brahmshankar Shastri,4th edition. (Uttraardh - Bhagnachikitsa),Varanasi,Chaukhambha Sanskrit Sansthan, 2004; pg 191.
Address for correspondence: Prof. (Dr.) Sanjeev Sharma, Professor, P.G. Department of Shalya Tantra, RajeevGandhi Govt. P.G. Ayurvedic College, Paprola - 176115 Kangra, H.P. (India) E-mail: [email protected]

1. Ph.D. Scholar 2. Assistant Professor 3. Associate Professor 4. Professor
IntroductionAyurvedic system of medicine is of great
antiquity and dates back to about 5000 yearsBC. Materia Medica of Ayurveda contains drugsbelonging to plant, animal and mineral in origin.1In addition to the single drug recipes, poly-herbaland herbo-mineral formulations have also beenincorporated by seers of ancient India who havedocumented their clinical experiences for passingon to future generations.
During the medieval period, with the adventof Rasashastra, certain heavy metals and mineralswere incorporated into Ayurvedic therapeutics.Rasashastra, an integral part of Ayurveda, dealswith drugs of mineral and metallic origin, theirvarieties, characteristics, processing techniques,properties, therapeutic uses, possibilities ofdeveloping adverse effects and their managementetc. in a comprehensive way. Actual developmentof Rasashastra as an independent branch oflearning and therapy started from 8th AD andonwards. Though, the utility of metals and
minerals in therapeutics became more evidentfrom 8th AD, a good deal on the description ofmetals and minerals, their processing techniques,therapeutic utility etc. can be observed in classicslike Charaka Samhita, Sushruta Samhita etc., whichbelongs to the era much earlier since 8th AD.
In due course of time, herbo-mineral andmetallic preparations occupied a significant placein Ayurvedic treatment and are now routinelybeing practiced in different parts of India. Thepreparations are said to be safe, efficacious evenat minute doses and never develop any significantuntoward effects2 when manufactured and usedas specified in classical texts.
Ayurvedic scholars use the metallicpreparations frequently in their routine practicesand these preparations have been reported to besafe through well designed experimental3 andclinical trials. However, the past decade haswitnessed concerns regarding the safety ofAyurvedic herbal, herbo-mineral and metallicpreparations by the western medical circles, and
J Res Educ Indian Med, Jan.-March 2014; Vol.XX (1): 9-20 ISSN 0970-7700
THERAPEUTIC POTENTIALS OF MINERALS IN ANCIENT INDIA:A REVIEW THROUGH CHARAKA SAMHITACHANDRASHEKHAR JAGTAP,1 GALIB RUKNUDDIN,2 PRASHANT BEDARKAR,2BISWAJYOTI PATGIRI3 AND P.K. PRAJAPATI4
Department of Rasa Shastra and Bhaishajya Kalpana,Institute for Post Graduate Teaching and Research in Ayurveda,Gujarat Ayurved University, Jamnagar - 361 008 Gujarat (India)
Abstract: Ayurvedic system of medicine has stood the test of time for four millennia or more.Ancient seers found that the drugs from different origin (herbal, metal or animal) are the mostsuitable tools in maintaining health in the healthy and eradicating diseases in the diseased. The useof metallo-mineral preparations in healthcare is a unique characteristic feature in this system.Processed metals and minerals including Mercury, Lead, Arsenic, Copper etc. were found to be usedvery frequently by the seers of Indian tradition in different disease conditions with great conviction.It is generally claimed that these metals / minerals gets detoxified during the manufacturingprocesses, if followed specified guidelines as emphasized in the scriptures of Ayurveda, especiallyRasashastra texts. Charaka Samhita, one of the scheduled books of Ayurveda also holds amplereferences regarding the use of minerals for different purposes, as reflected in this paper.
Keywords: Arsenic, Ayurveda, Charaka Samhita, Copper, Minerals.

Jagtap et al.10
this has damaged the reputation of the age-oldAyurvedic heritage.4
The need of the hour is to allay suchfears, by creating greater awareness and placingin proper perspective, the context in which thesedrugs are recommended for use and the methodsby which they were used as medicines.
The present paper is a simple compilationfocusing on the uses of minerals mentioned inCharaka Samhita. This review is expected togive an insight to assume the frequency of usageof minerals during the period of Charaka.
MakshikaMakshika has been placed under the group
of Maharasas in the texts of Rasa Shastra.5 Theuse of Makshika in therapeutics can be tracedback to the period of Samhitas, where Charakaadvocated its utility in different disorders likeKusta (skin disorders), Pandu (anaemia) etc. Thismineral is mentioned as an esteemed Rasayana,6possibly because of supplementing some of thevital elements to the body.
Makshika is a copper containingchalcopyrite (CuFeS2), is a combination ofCopper (>5%), Iron (>20%) and Sulphur(>12%),7 whereas the Makshika Satva is acombination8 of Cu, Ferric Oxide, Ferrous Oxide,Ca, Na, K, Phosphates and Silica. It is evidentfrom this unique combination of elements that,Makshika is the best Rasayana.
Formulations of Makshika have beenadvocated to be used in different conditions likePandu (anaemia), Arsha (haemorrhoides), Meha(diabetes), Shopha (inflammation) etc. and alsoas a useful rejuvenating drug.9 The normal dosementioned for Makshika Bhasma is 65-250 mg.10
The formulations mentioned in Charaka Samhita,which contain Makshika as one of thecomponents along with indications for whichrecommended are given in Table 1.
Screening through Charaka Samhitareveals the below important points:
Terms like Makshika Dhatu (Chikitsa 7/70 and 16/73), Suvarna Makshika (Chikitsa 7/71), Makshika (Chikitsa 16/82), Tapi (Chikitsa16/78) and Tapya (Chikitsa 26/250) were usedby Charaka for this mineral. The term Makshikaused in few other places has been clarified asMadhu (honey) by the commentator (Chikitsa 7/70 and 16/83).
Makshika has been defined by commentatorChakrapani as the Dhatu, which is found availableon the river banks of Tapi (Charaka Chikitsa26/250).
The version at Charaka Chikitsa 16/82 may be emphasizing on the adoption ofShodhana procedure of the minerals, includingMakshika etc. prior to their utilization intherapeutics.
ShilajatuShilajatu another drug from Maharasa
group is the most important drug in Ayurvedaand is used in treating a wide range of diseases.Charaka recognized this drug as vital forRasayana purposes and says that there is nodisease on earth, which cannot be cured withShilajatu. Further, he goes on emphasizing thatthe administration of Shilajatu in proper timewill impart strength in an individual.11
Classics speak about its origin as anexcretion due to heat of sun from the gold andother mineral ores in the mountains and is of thenature of lac.12 Further, Rasa Vagbhata narratesthat a sample of Shilajatu which forms into
Table 1. References of Makshika in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 7/70 Lelitaka Yoga Kusta
2 Chikitsa 7/71 Gandhaka Yoga Kusta
3 Chikitsa 16/73 Mandura Vataka
Pandu
4 Chikitsa 16/78 Leha Yoga Pandu
5 Chikitsa 16/82 Yogaraja Pandu
Utilization in therapeutics : External Application
6 Chikitsa 21/130 Lepa Yoga Granthi, Visarpa
7 Chikitsa 26/250 Varti Yoga Netra Roga

Minerals in Charaka Samhita - A Review 11
Lingakara on fire is genuine. Few other classicssay that, a good sample of this element whendropped into pure water from the tip of grasswill produce thin fibrils and dissolves completely,emitting the odour of Gomutra.13 As this elementis attributed with all the qualities of Rasa,Uparasa, Ratna and Loha, it is used as a greatalterative and useful alternative for conqueringpremature old age.14
Charaka, while classifying the Dravyasdepending on the source of origin, has used theterm Samala.15 While commenting on this verse,Chakrapani opines that Samala can beconsidered as slag of Lohas i.e. Shilajatu. Theseer used terms like Shilodbheda (Chikitsa 15/
113, 30/90), Adrijatu (Chikitsa 16/78),Raupyamala (Chikitsa 16/81), Shailasya Jatu(Chikitsa 28/242), Girija (Chikitsa 1-3/64, 21/130, 30/148), Shilahvaya (Chikitsa 1-3/65, 26/99) etc. for Shilajatu and its types.
Formulations of Shilajatu are goodantiseptics, pain relievers, expectorants anduseful in a wide range of diseases likeinflammations, skin diseases, urinary tractinfections, renal calculi, diabetes and associatedcomplications etc.
The normal dose mentioned for Shilajatuis 250-1000mg.16 The herbo-mineral formulationsmentioned in Charaka Samhita, which holdShilajatu as an ingredient, are placed at Table 2.
Table 2. References of Shilajatu in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Sutra 21/24 Shilajatu Yoga Sthaulya
2 Sutra 24/56 Shilajatu Yoga Murccha, Mada
3 Chikitsa 1 - 3/64 Shilajatu Rasayana Rasayana
4 Chikitsa 5/97 Shilajatu Prayoga Vataja Gulma
5 Chikitsa 12/49 Shilajatu Prayoga Tridoshaja Shotha
6 Chikitsa 13/152 Shilajatu Prayoga Sannipataja Udara Roga
7 Chikitsa 15/113 Yavagu Yoga Grahani
8 Chikitsa 16/78 Leha Yoga Pandu
9 Chikitsa 16/81 Yogaraja Pandu, Kasa, Vishama Jwara
10 Chikitsa 16/88 Shilajatu Vataka Pandu, Kusta
11 Chikitsa 26/99 Shilajatu Yoga Kaphaja Hridroga
12 Chikitsa 28/242 Shilajatu Yoga Avrita Vata
13 Chikitsa 29/159 Shilajatu Prayoga Vata Rakta
14 Chikitsa 30/90 Pushyanuga Churna Rajo Dosha
15 Chikitsa 30/148 Shilajatu Prayoga Reto Dosha
Utilization in therapeutics : External Application
16 Chikitsa 7/72 Lelitaka Yoga Kusta
17 Chikitsa 21/130 Lepa Yoga Granthi, Visarpa
18 Chikitsa 23/213 Pancha Shirisha Agada Visha
Other References
19 Sutra 1/70 Referred as ‘Samalaah’ Classification of Parthiva Dravya
20 Chikitsa 1 - 3/48 Classification Types and qualities of Shilajatu

Jagtap et al.12
Sasyaka / TutthaThe mineral Sasyaka also known as Tuttha
is a popular drug for external application sinceancient times. Tuttha bhasma is useful for internaladministration. In modern science, it is equatedwith copper sulphate (CuSO45H2O) familiar asblue Vitriol.17 The aqueous solution is useful toirrigate lesions of Kusta (skin diseases), Arshas(haemorrhoides), Dusta Vrana (non-healingulcers) etc. The solutions of Sasyaka are alsouseful in various Netra rogas (eye diseases) asAschyotana (eye drops).18 The normal dosementioned for the Bhasma is 15-30mg.19
Screening through the classic reveals that,formulations with Sasyaka have often beenpreferred for topical application. Brief details areplaced at Table 3.
The term Sasyaka is not available inCharaka Samhita. The Seer has used terms likeAmritasanga and Tuttha while referring to thismineral. Commentator, Chakrapani quoted otherterms like Karparika Tuttha (Chikitsa 25/117),Kharparika Tuttha (Chikitsa 7/114), MayuraTuttha (Chikitsa 14/55) and Tuttha (Sutra 3/10)while providing clarification to the termAmritasanga. Probably, these terms aresynonymous with each other. But the version ofthe same commentator as “Dwe Tutthe iti MayuraTuttham Kharparika Tuttham Cha” (Chikitsa 7/108) clarifies that Mayura and Kharparika Tutthaare different from each other.
GandhakaA pale yellowish mineral of great
importance, known as Gandhaka in Ayurveda isthe most important Rasa Dravya after Parada(mercury). It is known for its vast range oftherapeutic applications since ancient times andthere are hardly any preparation in Rasashastra,which does not have Gandhaka or its compoundas an ingredient. Thus, it can be said that, it isthe most essential element of Rasashastra placedunder the group of Uparasa. Because of thepeculiar odour of the element, it is described asGandhaka. The English equivalent for thiselement sulphur is probably derived from theSanskrit term Sulbari (antagonistic to copper).
When combined with Parada it forms acompound - Kajjali 20 (a fine, black, lusterlesspowder) which is a basic compound in preparinga number of herbo-mineral / mineral / metallicpreparations. Normal dose mentioned for theShuddha Gandhaka Churna (powder) is125 to 1000mg.21
Though it is an important mineral fromRasashastra point of view, formulations withSulphur as a component are rarely foundmentioned in Charaka Samhita. On scrutiny,only four references were found in the classicthat are placed at Table 4.
Terms like Gandha, Saugandhika,Lelitaka are used to refer this mineral. For theterm Saugandhika, the commentator, Chakrapani
Table 3. References of Sasyaka in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : External Application
1 Sutra 3/10 Avachurna Yoga Kusta
2 Sutra 3/12 Lepa Yoga Kusta
3 Chikitsa 7/114 Kanakaksiri Taila Krimi, Kandu, Kusta
4 Chikitsa 7/108 Tikta Ikshwakvadi Taila Kandu, Kusta
5 Chikitsa 7/120 Yamaka Yoga Vipadika
6 Chikitsa 14/55 Lepa Yoga Arshahara
7 Chikitsa 25/117 Varnakara Yoga Varnakara
8 Chikitsa 26/250 Sukhavati Varti Timira Netra Roga

Minerals in Charaka Samhita - A Review 13
opined that, it may be Gandhatrina (variety ofgrass) (Sutra 3/10), Gandhaka (Sutra 3/10),Manikya Bheda (type of gem) (Chikitsa 17/126).
GairikaAnother mineral in the group of Uparasa
of Rasashastra is Gairika,22 which is familiarfor its therapeutic purposes since ages. Charakaclassified this mineral under Parthiva Dravyaand grouped under Shonitasthapana Gana, whileSushruta used this drug in formulating MahaSugandhi Agada,23 which is a potent Vishahara(anti-poisonous) agent.
Rasa Vagbhata classified Gairika into twobasic varieties viz. Swarna and Pashana, theformer being the acceptable one. Swarna Gairikais smooth to touch (Snigdha / Masruna),extreme red in color (Atyanta Shonitam), whilethe latter variety is hard (Kathina) and copperyred (Tamra varna) in color.24
The term Lohitamrit (Chikitsa 23/101) hasbeen interpreted as Gairika by the commentatorChakrapani. In addition, another term KanchanaGairika was also found mentioned in the classicat Chikitsa 20/32. The cherry red colored mineralis identified as Red Oxide of Iron (Fe2O3) orHematite, which contains Iron (>16%) as principalconstituent,25 because of which the element maybe a proven remedy in cases of anaemia. Thenormal dose mentioned for the Shuddha Gairikais 250-500 mg.26 The formulations mentioned inCharaka Samhita, which hold Gairika as aningredient are placed at Table 5.Kasisa
Kasisa, another mineral mentioned in Rasaclassics under Uparasa Varga was frequently
preferred by Charaka for external purposes inconditions like Switra (leucoderma), Khalitya(alopecia), Kusta (skin disorders), Arshas(haemorrhoides) etc. Sushruta classified thiselement under Ushakadi Gana and advised itsuse in cases of Ashmari (renal calculi),Mutrakrchra (dysurea) etc.27 Terms likeSalomasho (Sutra 3/4), Romasham (Chikitsa 29/152) have been used by Charaka, which havebeen clarified as Dhatu Kasisam and Kasisamrespectively by Chakrapani.
It is identified as Green Vitreol (FeSO47H2O) or Ferrous Sulphate and a genuine samplecontains Iron (>25%) and Sulphur (>15%).28
Kasisa Bhasma is useful in cases of Jwara(pyrexia), Mutrakricchra (dysuria), Ashmari(calculi), Pandu (anaemia) , Pliharoga(spleenomegaly), Vrana (ulcers), Switra(leucoderma / vitiligo) etc.29 As the mineral hasa good amount of Iron in its composition, itmay be proven as a promising remedy in casesof anaemia. The normal dose mentioned forKasisa Bhasma is 65-250 mg.30 The formulationsmentioned in Charaka Samhita, which holdKasisa as an ingredient are placed at Table 6.
KankshiKankshi, another familiar mineral in
Ayurveda is well recognized with synonyms likeSaurashtri, Sphatika, Shubhra etc. AstangaHridaya advised the internal administration ofKankshi in cases of Hikka, Shwasa etc.31
Conventionally, this drug is used for dressing ofbleeding wounds and as a gargling agent indisorders of oral cavity. The sample withcharacters like slight yellowish (ishat pita) in
Table 4: References of Gandhaka in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 17/125 Muktadya Churna Hikka, Shwasa
Utilization in therapeutics : External Application
2 Sutra 3/10 Avachurna Yoga Kusta
3 Chikitsa 7/70 Lelitaka Prayoga Kusta
4 Chikitsa 7/71 Gandhaka Yoga Kusta

Jagtap et al.14
color, heavy (guru) and shiny (snigdha) shouldbe considered as a genuine variety.32
It is identified as Alum [K2SO4 Al2 (SO4)3
24H2O]33 and is a useful element with widetherapeutic attributes like Vranaghna (woundhealing), Chakshushya (helpful in eye diseases),Visarpa (erysipelas), Switra (vitiligo), VishamaJwara (viral fevers), Mukha Roga (diseases oforal cavity)34 etc. The normal dose of ShuddhaKankshi is 125 - 250 mg.35 The formulationsmentioned in Charaka Samhita, which holdKankshi as an ingredient are placed at Table 7.
Charaka used both the terms i.e. Kankshi(Chikitsa 23/54 and 30/121) and Saurashtri(Chikitsa 7/114, 15/138, 30/79 and 30/98) torefer this mineral. Commentator, Chakrapaniclarified that, both these terms are synonymouswith each other (Chikitsa 23/54). In addition,
he used another term Tuvari Mrittika (Chikitsa30/79) considering which, it can be said that,these three terms are synonymous.
HaritalaHaritala is one of the ancient minerals
known for its therapeutic properties, which wasused externally as well as internally since theperiod of Samhitas. This mineral is mentionedas Alam in Charaka Samhita and grouped underParthiva Dravyas. Sushruta classified it underSthavara (dhatu) Visha.36 Rasa Vagbhataclassified this mineral into two types viz. PatraTala and Pinda Tala, the former one being theacceptable variety. Patra Tala should be goldenyellow in color (swarna varnam), heavy (guru),shiny (snigdha), lustrous (bhasuram) with thinand innumerable flakes (tanu and bahu patram).
Table 5. References of Gairika in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 4/73 Pana Yoga Raktapitta
2 Chikitsa 4/79 Pana Yoga Raktapitta
3 Chikitsa 20/32 Pana Yoga Pittaja Chhardi
4 Chikitsa 20/33 Pana Yoga Pittaja Chhardi
5 Chikitsa 20/33 Pana Yoga Pittaja Chhardi
6 Chikitsa 23/46 Pana Yoga Visha
7 Chikitsa 23/101 Ksharagada Sarva Visa
8 Chikitsa 26/210 Khadiradi Gutika Mukha Roga
9 Chikitsa 30/91 Pushyanuga Churna Rajo Dosha
Utilization in therapeutics : External Application
10 Sutra 3/5 Pradeha Yoga Kusta, Kilasa, Dadru
11 Chikitsa 4/99 Avapidana Nasya Raktapitta
12 Chikitsa 21/82 Pradeha Yoga Visarpa
13 Chikitsa 23/220 Lepa Yoga Nakha, Danta Visha
14 Chikitsa 25/117 Varnakara Lepa Savarnikarana
15 Chikitsa 26/232 Netra Varti Netra Roga
16 Chikitsa 26/235 Netra Varti Netra Roga
Other References
17 Sutra 1/70 Classified under Parthiva Dravya
18 Sutra 4/18 Grouped under Shonita Sthapana Gana

Minerals in Charaka Samhita - A Review 15
The second variety i.e. Pinda Tala should bedevoid of flakes (nishpatram), appears like amass (pinda sadrusham), heavy (guru) withinferior degree of qualities and on administration,it causes infertility (pushpa haranam) infemales.37 Chemically it is identified as Orpiment(As2S3),38 probably derived from latin term AuricPigmentorum, which means Gold Paint.39
Being an arsenical mineral, it should beadministered with great caution.
Haritala Bhasma is beneficial in Kustha(skin diseases), Vishama Jwara (viral fever),Vrana (ulcers), Arsha (haemorrhoids),Bhagandara (fistula-in-ano), Apasmara(epilepsy), Visarpa (erysipelas) etc.40
Table 6. References of Kasisa in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 26/271 Mahanila Taila Palita
2 Chikitsa 29/152 Kalka Yoga Vatarakta
Utilization in therapeutics : External Application
3 Sutra 3/4 Pradeha Yoga Kusta
4 Sutra 3/5 Pradeha Yoga Kusta
5 Sutra 3/10 Avachurna Yoga Kusta
6 Sutra 3/15 Lepa Yoga Kusta
7 Chikitsa 7/102 Kustadi Taila Kusta
8 Chikitsa 7/109 Tikta Ikshwakvadi Taila Kandu, Kusta
9 Chikitsa 7/114 Kanaka Kshiri Taila Krimi, Kandu, Kusta
10 Chikitsa 7/117 Lepa Yoga Sidhma
11 Chikitsa 7/167 Shamana Lepa Yoga Switra
12 Chikitsa 21/126 Lepa Yoga Granthi, Visarpa
13 Chikitsa 25/115 Lepa Yoga Twak Janana
14 Chikitsa 25/117 Varnakara Lepa Savarnikarana
15 Chikitsa 26/254 Dristiprada Varti Dristiprada
16 Chikitsa 30/79 Dhatakyadi Taila Yoni Roga
17 Chikitsa 30/121 Yoni Varti Yoni Roga
Table 7. References of Kankshi in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 15/138 Kiratadya Churna Grahani
2 Chikitsa 23/54 Mrita Sanjivani Agada Sarva Visha
3 Chikitsa 30/98 Pana Yoga Pittaja Asrigdhara
Utilization in therapeutics : External Application
4 Chikitsa 7/114 Kanaka Kshiri Taila Krimi, Kandu, Kusta
5 Chikitsa 30/79 Dhatakyadi Taila Yoni Roga
6 Chikitsa 30/121 Yoni Varti Picchila Yoni

Jagtap et al.16
The therapeutic dose mentioned forHaritala Bhasma is 30-60 mg.41 The formulationsmentioned in Charaka Samhita, which holdHaritala as one of the components, are as shownin Table 8.
Charaka used both the terms i.e. Alamand Haritala to refer this mineral. Most of theformulations were mentioned for external useand only two formulations for internal use.
ManahshilaManahshila is mineral containing Arsenic
and grouped under Uparasa in Rasa classics.42
Charaka extensively used this mineral informulating compounds for external applicationas reflected in Sutra Sthana. Rasa Vagbhataclassified this mineral into three types viz.Shyamangi, Kanaviraka and Khandakhya, thelast variety being the best and acceptable one.Shyamangi is heavy (bharadhya) and availablein different colors like Shyama, Rakta and Pita.Kanaviraka is coppery red in color (tamrabha),
lustrous (tejaswini), devoid of yellowish tinge(nirgaura), while Khandakhya variety can beeasily broken into powder form (churnibhuta),bright red in color (ati raktangi) and heavy(bhara).43
Chemically it is identified as Realgar - RedOrpiment (As2S2)44 probably derived from Arabicterm Rehj - Alghar, which means powder of thecaves.45 Because of it being an arsenical mineral,it should be administered with great caution. Itis beneficial in Swasa (breathlessness), Kasa(cough), Agnimandya (loss of appetite), Kusta(skin diseases), Jwara (fever) etc.46 The normaldose mentioned for Manahshila is 4-8 mg.47
The formulations mentioned in Charaka Samhita,which hold Manahshila as one of thecomponents, are tabulated in Table 9.
Charaka used only one term i.e.Manahshila throughout the classic to refer thismineral. This mineral is frequently preferred bythe seer for administration through differentroutes of drug administration.
Table 8. References of Haritala in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 17/78 Dhooma Yoga Hikka, Swasa
2 Chikitsa 23/54 Mrita Sanjivani Agada Sarva Visha
Utilization in therapeutics : External Application
3 Sutra 3/5 Pradeha Yoga Kusta
4 Sutra 3/10 Avachurna Yoga Kusta
5 Sutra 3/12 Pradeha Yoga Kusta
6 Sutra 5/26 Dhooma Yoga Shiro Virechana
7 Chikitsa 7/114 Kanaka Ksiri Taila Krimi, Kandu, Kusta
8 Chikitsa 9/66 Varti Yoga Apasmara, Unmada
9 Chikitsa 14/56 Lepa Yoga Arsa
10 Chikitsa 18/69 Dhooma Yoga Vataja Kasa
11 Chikitsa 18/74 Dhooma Yoga Vataja Kasa
12 Chikitsa 25/114 Lepa Yoga Twak Janana
13 Chikitsa 26/196 Pitaka Curna Mukha Roga
Other References
14 Sutra 1/70 Referred as ‘Alam’ Classification of Parthiva Dravya

Minerals in Charaka Samhita - A Review 17
Table 9. References of Manahshila in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic Uses
Utilization in therapeutics : Internal Administration
1 Chikitsa 17/77 Dhooma Yoga Hikka, Swasa
2 Chikitsa 17/145 Manahshiladi Ghrta Hika, Swasa
3 Chikitsa 18/52 Leha Yoga Kasa, Hikka, Swasa
4 Chikitsa 18/69 Dhooma Yoga Vataja Kasa
5 Chikitsa 18/71 Dhooma Yoga Vataja Kasa
6 Chikitsa 18/73 Dhooma Yoga Vataja Kasa
7 Chikitsa 18/74 Dhooma Yoga Vataja Kasa
8 Chikitsa 18/75 Dhooma Yoga Vataja Kasa
9 Chikitsa 18/130 Dhooma Yoga Vataja Kasa
10 Chikitsa 18/146 Dhooma Yoga Kshataja Kasa
11 Chikitsa 18/147 Dhooma Yoga Kshataja Kasa
12 Chikitsa 18/169 Haritaki Leha Swasa, Kasa
13 Chikitsa 20/39 Leha Yoga Chardi
14 Chikitsa 23/55 Mrita Sanjivani Agada Visha
15 Chikitsa 23/78 Maha Gandha Hasti Visha
16 Chikitsa 26/152 Pradhamana Nasya Yoga Pinasa
Utilization in therapeutics : External Application
17 Sutra 3/5 Pradeha Yoga Kusta
18 Sutra 3/10 Avachurna Yoga Kusta
19 Sutra 3/12 Pradeha Yoga Kusta
20 Sutra 3/12 Pradeha Yoga Kusta
21 Sutra 3/15 Lepa Yoga Kusta
22 Sutra 5/26 Dhooma Yoga Shiro Virechana
23 Chikitsa 3/306 Anjana Yoga Vishama Jwara
24 Chikitsa 7/117 Lepa Yoga Sidhma
25 Chikitsa 7/167 Shamana Lepa Shwitra
26 Chikitsa 7/170 Lepa Yoga Kilasa
27 Chikitsa 23/190 Lepa Yoga Sarva Shotha, Visha
28 Chikitsa 23/192 Lepa Yoga Sarva Visha
29 Chikitsa 23/213 Pancha Shirisha Agada Visha hara
30 Chikitsa 25/114 Lepa Yoga Twak Janana
31 Chikitsa 26/196 Pitaka Churna Mukha Roga
32 Chikitsa 26/235 Varti Yoga Netra Roga
33 Chikitsa 26/250 Anjana Yoga Netra Roga
34 Chikitsa 26/252 Sukhavati Varti Netra Roga
Other References
35 Sutra 1/70 Classified under Parthiva Dravya

Jagtap et al.18
AnjanaAnjana Dravyas are those, which are
employed as collyrium in eye diseases orotherwise. The importance of Anjana in dailyroutine has been recognized since vedic times.Anjana is an important part of Dinacharya(Charaka).48 Rasavagbhata mentioned fivedifferent types of Anjanas.49 Detailed descriptionsof these five are not found available in CharakaSamhita except information on very few.Sauveeranjana is a lead containing mineral witha chemical formula of PbS with Pb (> 50%).50
This mineral has been equated with Stibnite byfew other scholars.51 This mineral has beenpreferred occasionally in therapeutics (Table 10).
The screening reveals that, Anjana Yogasare very rarely mentioned in Charaka Samhita.Anjana has been clarified as Sauveeranjana byChakrapani at Sutra 1/70. It has also beenmentioned that, Suveeraanadibhavam Sauveerami.e. the one found on the river banks of Suveerashould be considered as Sauveeranjana (Sutra5/15).
In addition to Sauveeranjana; other formsof Anjanas like Srotonjana (Chikitsa 20/29),Rasanjana (Sutra 5/15), Pushpanjana (Chikitsa26/250) are also found mentioned in this classic.
Maharasas (Makshika, Shilajatu and Sasyaka)and all eight Uparasas (Kankushta)52 in hisclassic. Interestingly, information on Sadharanarasas was not found in the classic. In additionto these minerals; information on certain salts(lavana dravya), alkaline substances (ksaradravyas) and calcium containing material (jantavadravya) etc. are also found available in CharakaSamhita. These groups were not screened inthe current attempt.
Charaka advocated utilization of thesepreparations with great conviction. In recent past,most of the western scientists focus on the toxicnature of metals and minerals like Mercury, Lead,Arsenic etc. A review of Ayurvedic literaturereveals that the ancient scholars were aware ofthis fact and devised various methods such asShodhana to rid them of their adverse effects,if any.
References1. Charaka Samhita. Ayurveda Dipika
Commentary by Chakrapanidutta, ChaukhambhaSurbharati Prakashan, Varanasi, Reprint,Sutra Sthana 1/68, pp 20 (2000).
2. Rasendra Sara Samgraha, Satyartha Prakashikacommentary by Satyartha Prakasha, KrishnadasAcademy, Varanasi, 1st Ed., 1/4, pp 5 (1994).
3. Anonymous, Safety / Toxicity study report ofsome Ayurvedic Drugs, Central Council forResearch in Ayurveda and Siddha, Dept. ofAYUSH, Ministry of Health & Family Welfare,New Delhi (2009).
4. Saper RS, Kales SN et al. Heavy Metal Contentof Ayurvedic Herbal Medicine Products, JAMA2004;292(23):2868-73.
5. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas publications, New Delhi, Reprint,2/1, pp 18 (2010).
6. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas publications, New Delhi, Reprint,2/80, pp 29 (2010).
7. The Ayurvedic Pharmacopoeia of India. 1stEd., Ministry of Health & Family Welfare, Dept.of AYUSH, Delhi, Part-I, Vol-VII (Minerals &Metals), pp 36-7 (2008).
8. Ayurvediya Rasashastra. Jha CB, ChaukhambaSurabharati Prakashan, Reprint Ed., Varanasi, pp223 (2003).
ConclusionThe screening reveals that mineral
preparations occupied a significant place inAyurvedic therapy since antiquity. Overall, it isfound that, Acharya Charaka mentioned three
Table 10. References of Anjana in Charaka Samhita
Sr. No.
Reference Formulation Therapeutic
Uses
Utilization in therapeutics : External Application
1 Sutra 3/5 Pradeha Yoga Kusta, Kilasa, Dadru
2 Sutra 5/15 Anjana Yoga Netra Roga
3 Chikitsa 26/250 Sukhavati Varti
Timira Netra Roga
Other References
4 Sutra 1/70 Classified under Parthiva Dravya

Minerals in Charaka Samhita - A Review 19
9. Ayurveda Prakasha. Suspashtartha PrakashiniHindi commentary by Gularaj Sharma Mishra,Chaukhamba Bharati Academy, Varanasi, 4/9-10,pp 410 (2007).
10. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 21/29, pp 525 (2000).
11. Charaka Samhita. Ayurveda DipikaCommentary by Chakrapanidutta, ChaukhambhaSurbharati Prakashan, Varanasi, Reprint,Chikitsa Sthana 1/3/65, pp 386 (2000).
12. Charaka Samhita. Ayurveda DipikaCommentary by Chakrapanidutta, ChaukhambhaSurbharati Prakashan, Varanasi, Reprint,Chikitsa Sthana 1/3/56, pp 386 (2000).
13. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulkarni DA, MeharchandLachhmandas publications, New Delhi, Reprint,2/114, pp 33-4 (2010).
14. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulkarni DA, MeharchandLachhmandas publications, New Delhi, Reprint,2/116, pp 34 (2010).
15. Charaka Samhita. Ayurveda DipikaCommentary by Chakrapanidutta, ChaukhambhaSurbharati Prakashan, Varanasi, Reprint,Sutra Sthana 1/70, pp 20 (2000).
16. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 22/87, pp 591 (2000).
17. The Ayurvedic Pharmacopoeia of India. 1stEd., Ministry of Health and Family Welfare,Dept. of AYUSH, Delhi, Part-I, Vol-VII (Minerals& Metals), pp 45 (2008).
18. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 21/80-3, pp 535 (2000).
19. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 21/130, pp 543 (2000).
20. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 2/27, pp 16 (2000).
21. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 8/39, pp 182 (2000).
22. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/1, pp 42 (2010).
23. Sushruta Samhita. Chaukhambha Orientalia,Varanasi, 7th Ed., Kalpa Sthana 6/16, pp 581(2002).
24. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/46, pp 48 (2010).
25. The Ayurvedic Pharmacopoeia of India. 1stEd., Ministry of Health & Family Welfare, Dept.of AYUSH, Delhi, Part-I, Vol-VII (Minerals &Metals), pp 5-6 (2008).
26. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 22/119, pp 597 (2000).
27. Sushruta Samhita. Chaukhambha Orientalia,Varanasi, 7th Ed., Sutra Sthana 38/37-38, pp 167(2002).
28. The Ayurvedic Pharmacopoeia of India. 1stEd., Ministry of Health & Family Welfare, Dept.of AYUSH, Delhi, Part-I, Vol-VII (Minerals &Metals), pp 19-20 (2008).
29. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 21/231-33, pp 564 (2000).
30. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Ed. Kashinath Shastri, MotilalBanarasidas, New Delhi, 11th Ed., Reprint, 22/242, pp 566 (2000).
31. Ashtanga Hridayam. Collated by AnnaMorshwar Kunte, Krishnadas Academy, Varanasi,Reprint Edition, Chikitsa Sthana 4 (2000).
32. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/61, pp 51 (2010).
33. Ayurvediya Rasashastra. Jha CB, ChaukhambaSurabharati Prakashan, Reprint Ed., Varanasi, pp254 (2003).
34. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 11/181-3, pp 274-5 (2000).
35. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Edited by Kashinath Shastri,Motilal Banarasidas, New Delhi, 11th Ed.,Reprint, 11/200-1, pp 276 (2000).

Jagtap et al.20
Address for correspondence: Dr. Galib Ruknuddin, Assistant Professor, Department of Rasa Shastra &Bhaishajya Kalpana, IPGT & RA,Gujarat Ayurved University, Jamnagar - 361008 Gujarat (India) E-mail: [email protected] Mns No: JREIM-2012-09-034
45. http://en.wikipedia.org/wiki/Realgar (last accessedon 19.12.2011 at 10.12 AM)
46. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Ed. Kashinath Shastri, MotilalBanarasidas, New Delhi, 11th Ed., Reprint, 11/116, pp 263 (2000).
47. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Ed. Kashinath Shastri, MotilalBanarasidas, New Delhi, 11th Ed., Reprint, 11/117, pp 263 (2000).
48. Charaka Samhita. Ayurveda DipikaCommentary by Chakrapanidutta, ChaukhambhaSurbharati Prakashan, Varanasi, Reprint, SutraSthana 5/15, pp 39 (2000).
49. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/97-8, pp 58 (2010).
50. The Ayurvedic Pharmacopoeia of India.1st edition., Ministry of Health & Family Welfare,Dept. of AYUSH, Delhi, Part-I, Vol-VII (Minerals& Metals), pp 32 (2008).
51. Ayurvediya Rasashastra. Jha CB, ChaukhambaSurabharati Prakashan, Reprint Ed., Varanasi, pp268 (2003).
52. Charaka Samhita.Ayurveda Dipika Commentaryby Chakrapanidutta, Chaukhambha SurbharatiPrakashan, Varanasi, Chikitsa Sthana 7/111pp 456 (2000).
36. Sushruta Samhita. Chaukhambha Orientalia,Varanasi, 7th Ed., Kalpa Sthana 2/5, pp 564(2002).
37. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/66-7, pp 53 (2010).
38. Ayurvediya Rasashastra. Jha CB, ChaukhambaSurabharati Prakashan, Reprint Ed., Varanasi, pp257 (2003).
39. http://en.wikipedia.org/wiki/Orpiment (lastaccessed on 19.12.2011 at 10.15 AM)
40. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Ed. Kashinath Shastri, MotilalBanarasidas, New Delhi, 11th Ed., Reprint, 11/52-5, pp 252 (2000).
41. Rasatarangini. Prasadani Commentary byHaridutta Shastri, Ed. Kashinath Shastri, MotilalBanarasidas, New Delhi, 11th Ed., Reprint, 11/56, pp 253 (2000).
42. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/1, pp 42 (2010).
43. Rasaratnasamuccaya. VigyanabodhiniCommentary by Kulakarni DA, MeharchandLachhmandas Publications, New Delhi, Reprint,3/88-90, pp 57 (2010).
44. Ayurvediya Rasashastra. Jha CB, ChaukhambaSurabharati Prakashan, Varanasi, pp 263 (2003).

J. Res. Educ. Indian Med., Jan.-March 2014; Vol. XX (1): 21-27 ISSN 0970-7700
EVALUATION OF ECLECTIC THERAPY ON FASTING BLOOD SUGARIN PATIENTS OF TYPE-2 DIABETES MELLITUSROOHALLAH BAY,1* SUJATA VAYDIA2 AND FATEMEH BAY3
Behavioral Sciences Research Center1, Baqiyatallah University of Medical Sciences, Tehran, IranDepartment of Alternative Therapy,2 Zoroastrian College,International University for Complementary Medicine, Mumbai, IndiaDepartment of Education and Psychology,3 Kharazmi University, Tehran, Iran
Abstract : Diabetes mellitus is one of the most dangerous diseases in the world. This reportpresents exploratory research designed and performed at diabetes clinics in Iran. The main aim ofthe research was to evaluate the effect of Eclectic therapy conducted through Hypnotherapy,Acupressure therapy and Transcendental meditation (TM) on Fasting Blood Sugar (FBS) incomparison with placebo treatment in patients of type-2 diabetes mellitus (DM-II). ‘Conveniencesampling’ for the selection of patients who suffered from type-2 diabetes and who were willingto cooperate in this research was used. 20 patients were employed as a sample group. For thecollection of data, the identical quasi-experimental design called ‘non-equivalent control group’system was used. Therapy sessions were carried out for 10 successive days. Each sessioncomprised of 60 to 90 minutes. Prescription included 2 capsules (containing 3 grams of wheatflour each) twice a day for members of the placebo group. The pre-tests, post-tests and follow-up tests were conducted in a medical laboratory recognized by the Ministry of Health and MedicalEducation of Iran. The data of this research showed that the mean FBS level in the post-tests andthe follow-up tests for the experimental group had been reduced significantly in comparison withthe pre-tests, and this result was different from that of the placebo group. The results of thisresearch revealed that eclectic therapy including acupressure therapy, hypnotherapy and transcendentalmeditation had an effect on the FBS level in patients of DM-II and that eclectic therapy was moreeffective than the placebo treatment in reducing the FBS level in diabetes mellitus.
Keywords: Alternative therapy, Diabetes, Eclectic therapy, Transcendental meditation.
Introduction Diabetes Mellitus is one of the most
problematic diseases. Type-2 diabetes mellitus(DM-II) is more severe among patients aged 40to 60. It usually progresses with age. Diabeticpatients must receive great care; otherwise, theywill encounter many complications including heartattacks and strokes.
The pancreas is a gland that is partlyexocrine and partly endocrine. The exocrinepart secretes the digestive pancreatic juice andthe endocrine part secretes hormones, e.g.insulin.1 Insulin is a polypeptide that is secretedby beta-cells in the Islets of Langerhans of thepancreas.2
Type-2 Diabetes accounts for at least80% to 90% of all diabetic patients. Diabetes
causes a decrease in the ability to absorbinsulin, which is referred as insulin resistance.Due to this insulin resistance, the food metabolismand proper utilization of glucose by the body isbadly effected.3
According to Gordon, cancer patientspracticing meditation reported relief from the sideeffects of radiation and chemotherapy associatedwith conventional therapies and enhanced bodyimmune response.4
Williams et al. reported that the currentapproved treatment for hypertension includedtranscendental meditation (TM) as a treatmentmodality.5 Since the early 1980s, the use ofpsychotherapy as a treatment modality has grownrapidly and this has led to a better and morecomplete treatment model.6
* Corresponding Author

Roohallah Bay, Sujata Vaydia and Fatemeh Bay22
In this research, investigations on theefficacy of a treatment modality combiningacupressure therapy with hypnotherapy and TMwere conducted (eclectic therapy). Measuringand comparison of the effect of this eclectictherapy on the fasting blood sugar (FBS) level intype-2 diabetic patients with that of a placebogroup of patients was done and analyzed.
In this research, answer to the followingquestions were attempted:
Does eclectic therapy have an effect onthe FBS level in diabetic patients?
Is there a difference between the effectsof eclectic therapy and placebo treatment on theFBS level in diabetic patients?
Do moderator variables (gender, durationof disease and age of patients) have any effecton the FBS level of diabetic patients?
This research has addressed two mainhypotheses and three minor hypotheses.
The main hypotheses of this research areeclectic therapy has an effect on the FBS levelof type-2 diabetic patients and there should be adifference between the effects of eclectic therapyand a placebo treatment on the FBS level oftype-2 diabetic patients.
The minor hypotheses are:-That differences exist between the effects
of Eclectic therapy and Placebo treatment onthe FBS level of type-2 diabetic patients when
(1) gender,(2) duration of disease and(3) the age of the patients are considered
either individually or as a whole.
In this research, the independent variablesare ‘Eclectic therapy’ and ‘Placebo treatment’.The dependent variable is the ‘FBS’ level ofdiabetic patients under study. The rate of ‘studies,social, economic and cultural factors’ the‘location and the environment of therapy’ andthe ‘therapist’ are control variables.
Moderator variables are(1) gender,(2) duration of disease suffering and(3) age of the patient.
2. Materials and Methods2.1. Therapy Methods
Following procedures-systems wereemployed :
- TM for relaxation,- Hypnotherapy for relaxation and
suggestion (in order to stimulate beta cells) and- Acupressure therapy for the stimulation
of the beta cells in the Islets of Langerhans inthe pancreas.
Diabetic neuropathy is also caused due toliver weakness. If the liver is nomalized byactivation with acupuncture (point stimulation),not only does overall digestion improve but diabeticneuropathy and retinopathy can also be avoided.
Even though the sugar level is kept undercontrol, side effects are seen in diabetic patientsmainly due to continuous stimulation of thepancreas with external medicines. The point ofemphasis was to bring the digestive system to itsoptimum level with acupuncture. For a diagnosedtype-2 diabetic patient, initially, the spleen pointSp-3 or Sp-6 is stimulated to influence thepancreas. Along with this, the liver is chargedby stimulating Liv-1 point.
Once the liver starts functioning at itsoptimum level, pain in any part of the bodydiminishes and the bowel movement improves.Along with the liver-1, the lung point Lu-7 isactivated to take care of energy circulation in thebody. Finally, the brain meridian and the spleencontrol point P-7 are activated with aim toimprove the functioning of the pancreas.
Since the stimulation mechanism iscontrolled by one’s subconscious mind, self-helptechniques, such as generating positive thoughtsand being sincere, may help to overcome diabetes.
2.2. Materials and Research MethodologyTwenty patients were selected from
volunteers who were registered at diabetes clinicsof Gorgan Panjomeazar Policlinic (Iran). Thepatients ranged in age from 25 to 60 years. Fordata collection, we used quasi-experimentaldesigns called “non-equivalent control group.” Aplacebo group was used instead of a control

Evaluation of Eclectic Therapy on FBS in Diabetes 23
group. Pre-tests were done on both groupsbefore treatment began, post-tests were doneafter completion of treatment. Follow-up testswere done two weeks after the last session.
Male and female patients were included inboth groups, because one of the moderatorvariables of this research was gender. Treatmentwas conducted at a room in diabetes clinics ofPanjomeazar Policlinic of Golestan MedicalSciences University. For the experimental group(ten patients), 60 to 90 minute meetings, onconsecutive days were conducted, while for theplacebo group, two placebo capsule containing3 grams each of wheat flour were used per day(one in the morning and one in the evening).We conducted this program for ten sessions andhad one treatment session every day.
To measure the effects of therapy, weused pre-tests, post-tests and follow-up tests.The medical tests were done in a laboratoryrelated to the medical organization of Iran andmeasured the FBS level. In addition, we usedthe AccueCheck machine to monitor patients.We recorded the daily BS level of patients beforeand after therapy sessions in both groups.
Complete check-ups for the patients wereprovided one day before starting the first sessionand one day after the last session. Followupcheckup was conducted two weeks after thelast session. The tests were done at medicallaboratories certified by Golestan MedicalSciences University. Results of these tests wereused to compare the placebo and the experimentalgroups.
In this research, statistical methods wereused at two descriptive and inferential levels. Indescriptive statistics, we used the mean, variance,standard deviation (SD) and also quarter andcharts. In inferential statistics, in order tocompare the data, we used student’s “t” testand variance analyses.
Because of the small sample numbers inthis research, the patients in the groups had to berepresentative of the general population and thegroups had to be equal in size. To determine if thegroups were representative of the general
population, we used the Kolmogorov-Smirnov Test.To check the equality of variances, we used the‘Leven Test’, and to survey the quality ofchanges between the three tests, pre-test, post-test and follow-up test, we used the ‘DuncanTest’. For the survey on the effects of differentvariables, as well as the passage of time andbecause the tests were done at different times,we used the repeated measures method. In orderto do that, equality of co-variances had to beestablished, so we used the ‘box test’ and the‘covariate test’. For the non-existent equality ofvariances, we used the ‘Huynh-Feldt’, the‘Greenhouse-Geisse’ and the ‘lower-bound tests’.The data was computarized and statisticallyanalysed using SPSS software.
2.3. ProcedureWe announced this research at all hospitals,
well-being organizations and clinics of Golestanprovince (Iran). Then, the volunteers for thisresearch were asked to complete a form to getinformation about the volunteer’s age, gender,duration of disease, drugs used, education levels,other illnesses that they suffered etc. Thisinformation was necessary, both to form similargroups to prevent obstructive variable effectsand to manage the control and the moderatorvariables, as well as the obstructive factors.
Initially, 252 volunteer diabetic patientswere enrolled. Then, by paying attention to thecontrol and moderator variables and for trying todecrease obstructive variables, we invited 49 outof enrolled 252 patients for interviews andcheckups. At the time of the interviews,researcher obtained information on the patient’sbackground, duration of disease, kinds ofmedicines used and nutrition with lists of dailymeals. Then, according to the research design(unequal control groups), experimental group andone placebo group were made.
Ultimately, out of 49 patients, 20 volunteersin both groups, were placed while trying to makethe two groups similar. Also, according toacupressure therapy principles, physical condition,pulse rates, etc. were checked.

Roohallah Bay, Sujata Vaydia and Fatemeh Bay24
In this research, we placed male andfemale patients in both groups because one ofthe moderator variables of this research wasgender. The duration for all therapy sessions wasaround 60 to 90 minutes and 10 therapy sessionswere conducted for each of the patients in theexperimental group. It is important to note thatbefore starting the therapy sessions, all of thepatients (both the placebo and the experimentalgroups) went to the medical laboratory on aspecified day (one day before starting the firstsession of therapy) to take the pre-test. Then,while the experimental group was undergoingtherapy, simultaneously the patients of the placebogroup were taking placebo capsules.
For the experimental group’s patients,eclectic therapy was performed during eachsession on consecutive days. At the end oftherapy for the experimental group’s patients,the patients in the placebo group simultaneously
stopped taking the placebo capsules. Then, on aspecified day, all patients of both groups weresent to a medical laboratory for the post-test. Inaddition, around one week after finishing thetherapy sessions, on a specified day, all patientsof both groups were sent to the medicallaboratory for the follow-up test.
3. ResultsThe data for the FBS levels are as follows:
placebo group: FBS 1: 218, FBS 2: 224 and FBS3: 224 and experimental group: FBS 1: 254, FBS2: 155 and FBS 3: 166), where FBS 1, 2, and 3are the mean FBS levels at the pre-test, the post-test and the follow-up test, respectively (Table 1).The effect of time within each group is significant(Table 2). Thus, we can conclude that the FBSlevel experiences different changes with passingtime if we disregard the effects of othermoderator variables on the results and if we
Table 1. Data for FBS levels at different times (1, 2 & 3) for different groups and genders.
Group Gender Mean Std. Deviation
F.B.S.1(pre-test) experiment Male 205.8000 48.56645
Female 303.0000 75.77269
Total 254.4000 78.89543
Placebo Male 207.0000 39.25557
Female 230.2000 44.26850
Total 218.6000 41.29622
F.B.S.2(post-test) experiment Male 115.8000 42.13312
Female 196.0000 72.14915
Total 155.9000 69.92289
Placebo Male 212.2000 27.68935
Female 237.4000 52.91314
Total 224.8000 41.97036
F.B.S.3(follow-up test) experiment Male 119.0000 41.50904
Female 214.0000 68.99638
Total 166.5000 73.40640
Placebo Male 211.0000 32.89377
Female 237.2000 45.83339
Total 224.1000 40.06509

Evaluation of Eclectic Therapy on FBS in Diabetes 25
survey the results for only the placebo or theexperimental group.
Table 1 shows that the FBS levels in bothgroups varied with time. The minimum FBSlevel in both groups occurred at the time of thepost-test. At the follow-up test, a slight increasewas noted, but it was not significant. The pre-test FBS level is the highest among the threetests. These results show that eclectic therapy isable to decrease the FBS levels of patients.
Table 3 (F=25.21 & P=0.000) indicatesdifferent changes in the FBS levels of patients atdifferent times. However, when we surveyed eachmoderator variable individually after deleting theeffects of other variables, we saw that all
significance levels were greater than 0.05. Thus,we could conclude that neither gender nor theage of the patient had a significant effect on thedecrease or the increase in the FBS level atdifferent times. Thus, the data indicate that bothmain hypotheses of this research are correct.
4. Discussion and ConclusionHypnosis has been successfully used for
the treatment of several disorders. In 1996, theNational Institutes of Health judged hypnosis tobe helpful for the treatment of pain from cancerand other chronic conditions. Several studies haveindicated that it can ameliorate acute pain in burnpatients, children experiencing bone marrowaspirations, and women in labor. It has also beeneffective intervention analgesia for the treatmentof invasive medical procedures.7
The research findings about meditationresults include increased happiness, reducedstress, increased intelligence, increased creativity,improved memory, improved health, reduced highblood pressure, improved relationships, increased
Table 3. Factors and moderator variables.
Source df F Sig.
Factor 1 – time Greenhouse-Geisser 1.077 0.029 0.882
Factor 2 – group Greenhouse-Geisser 1.077 25.218 0.000
Factor 3 – gender Greenhouse-Geisser 1.077 0.185 0.691
Factor 4 – age Greenhouse-Geisser 1.077 0.142 0.730
Factor 5 - duration of disease Greenhouse-Geisser 1.077 0.112 0.761
Table 2. FBS levels between groups and within groups.
df F Sig.
Between Groups 2 5.315 .011
Within Groups 27
Total 29
energy, reduced insomnia, reversal of biologicalaging, reduced crime and improved quality oflife in society.
The research has been published in majorscientific journals, such as Science, the AmericanJournal of Physiology, Scientific American, Lancet,the Journal of Counseling Psychology, theInternational Journal of Neuroscience, the Journalof the Canadian Medical Association, the BritishJournal of Educational Psychology and the Journalof Conflict Resolution.8
Sommer reports that 2000 regularpractitioners of transcendental meditation, whencompared with 600,000 non-meditators over a
5-year period, had 30.6% fewer mentaldisorders, 30.4% fewer infectious diseases andgreater than 50% less overall health systemusage.9
Benson conducted a series ofinvestigations involving men and women in orderto examine the effect of transcendentalmeditation on physiological functions of thebody and reported marked physiological changes,including reductions in heart rate, breathing rate,oxygen consumption, blood lactate levels andblood pressure.10
Researchers at the New Mexico StateUniversity’s Social Work Department observed a

Roohallah Bay, Sujata Vaydia and Fatemeh Bay26
high incidence of diabetes among Mexican-Americans in southern New Mexico. Theybelieved that the use of a short relaxation programcould have beneficial effects on the health ofthose with diabetes and their families. They foundthat a combination of acupressure and breathawareness help people with diabetes. The studyshowed that a short stress-relief programincluding touch therapy could lower blood sugarand improve health in diabetic patients.11
According to Redfield, currently, manyhumans integrate meditation practices in theirprograms for health promotion and illnessprevention. Over many centuries, Meditation asa method to integrate the concept of mind andbody, has been recorded as effective in the formof either practical or religious practices. Theprocedure of meditation involves the concept ofinner stillness and celebrates nature as a reveredpath to self-knowledge and spiritualenlightenment, leading the person on a satisfyingmental journey. The goal of meditation is to emptythe mind of thought and let go of thepreoccupations that make up the mind’s chatter.12
According to Bricklin, approximately 40%of the U.S. population is using alternative therapiesfor better health.13
Our study showed different results for theexperimental and the placebo groups. Theeclectic therapy had a more significant effectthan the placebo treatment and this result wasindependent of gender, duration of disease andage. Thus, our study supports a link betweenalternative healing therapies and decrease in meantype-2 diabetes.
This creates a need for structuredprograms teaching lifestyle change, non-pharmacologic interventions and alternativetherapies in conjunction with conventionaltreatment.14
The psychological role has always beenone of patient’s advocate. If lifestyle changesand alternative healing such as hypnotherapy,transcendental meditation and acupressure therapyare taught to patients, the risk of stroke, heartattack, other disabling side effects of diabetes
and most other diseases will decrease thepharmacological treament.
However, there can be adverse side effectswith medication. By implementing and teachingholistic healing, the therapist can give patientsthe foundation to reduce stress in their lives,thereby reducing the need for conventionalmedical treatment. Therapist can also experienceboth the benefits and the limitations of theseapproaches and find ways to use them with theirpatients. By embarking on these extended coursesof study, the clinical results may justify theinvestment of time and energy.15
The findings of our study have implicationsfor advanced psychological practice, educationand health care of diabetic patients and for otherswho suffer from disease. The implementation ofhypnotherapy, acupressure therapy andtranscendental meditation classes taught by apsycho-physiologist in the outpatient clinic shouldbe considered at the patient’s first clinic visit.
A shift in emphasis from treating toimparting teaching the patient these therapieshighlights the psychological function as a guideand teacher; and makes patient care a morefulfilling partnership. All psychologists shouldhave knowledge of holistic healing andimplementation of hypnotherapy, transcendentalmeditation and acupressure therapy. Thesesystems should be taught in the classes atschools of psychology to introduce the conceptof alternative healing therapies.14
Our study established eclectic psycho-physiological therapy (acupressure therapy,hypnotherapy and transcendental meditation) asimportant to the type-2 diabetic patient populationsas it provides the patient with the power todecrease the FBS Level and to enhance the body’sown capacity for healing. Integration ofacupressure therapy, hypnotherapy andtranscendental meditation in treatment plans allowsa collaborative and democratic relationship betweenthe advanced psycho-physiological practitioner,other health providers and the patient, who thenreaps the psychological and physiological rewardsof feeling more in control of their own health.

Evaluation of Eclectic Therapy on FBS in Diabetes 27
Limitations of the studyThe following limitations prohibit
generalizations of study to target populations: Thestudy involved a cross section of 20 participants.The sample size may serve to limit generalizabilityof the findings. Sample size may not berepresentative, as samples would only be fromGolestan state (Iran) and within limited timeframe. Also the sample consisted of volunteeringsample of convenience. All ethnicities may nothave been represented.
AcknowledgmentsThis study was conducted with the
approval of the Medical Sciences University ofGolestan (Iran) and Zoroastrian College ofMumbai (India).
References1. Chaurasias B G. Human Anatomy: New Delhi,
India, CBS Publishers and Distributors, 2003.2. Sembulingam K, Sembulingam P. Essentials
of Medical Physiology. New Dehli, India, JaypeeBrothers, Medical Publishers (P) LTD, 2008.
3. Guyton C, Hall JE. Text book of MedicalPhysiology. Tehran, Teimorzadeh Publishers, 2000.
4. Gordon J. Alternative medicine and the familyphysician. American Family Physician. 1996;54:2205-22.
5. Williams J, Park L, Kline J. Reducing distressassociated with pelvic examinations: A stimulus
control intervention. Women & Health 1992;18(2):41-53.
6. Goldfried MR, Cstonguay LG. The future ofpsychotherapy. Integration Psychotherapy 1992;29:4-10.
7. Lang EV, Benotsch E, Fick LJ, Lutgendorf S,Berbaum ML, Berbaum KS, Logan H,Spiegel D. Surgery:Complications andTreatment. Lancet 2000;355:1486.
8. Orme-Johnson D. Summary of ScientificResearch on the Transcendental Meditation andTM-SIDHI Programs. Maharishi InternationalUniversity, Maharishi Vedic EducationDevelopment Corporation. Available at http://www.tm.org/research/summary.html, June 14, 2009.
9. Sommer SJ. Mind-body medicine and holisticapproaches. Australian Family Physician 1996;25:1233-41.
10. Benson H. The Relaxation Response, New York,William Morrow, 1975.
11. Gerald W. Acupressure, Breath Awareness HelpsDiabetes Patients. Originally published inHealth & Social Work. Vest, New Mexico, 1997;22:95-100.
12. Redfield SM. The Joy of Meditating, NewYork,Time-Warner, 1995.
13. Bricklin M. Positive Living and Health.Pennsylvania, PA. Rodale Press, 1990.
14. Bay R. Alternative and Psycho-PhysiologicalComplementary Therapies. Pune, India, SuchakCreations Publication, 2009.
15. Bay R. Explanatory Dictionary of Type 2 Diabeteswith Psycho –Physiological Treatments. Pune, India,Suchak Creations Publication, 2009.
Address for correspondence: Dr. Roohallah Bay, Behavioral Sciences Research Center, Baqiyatallah Universityof Medical Sciences, Tehran, Iran. E-mail: [email protected] Bay, M.A; M.Phil; Ph.D; Post Doctoral Fellow, Sexual and Family Therapy Group, Department ofFamily Medicine, School of Medical Sciences, University Sians Malaysia.

28

J. Res. Educ. Indian Med., Jan.-March 2014; Vol. XX (1): 29-35 ISSN 0970-7700
MEMORY LOSS IN GERIATRIC AGE AND ITS PREVENTIONTHROUGH YOGIC LIFESTYLEHETAL AMIN,1 ROHIT SHARMA,2 M.K. VYAS3 AND R.R. DWIVEDI4
Departments of Basic Principles,1,3,4
Department of Rasashastra and Bhaishajya Kalpana,2 I.P.G.T.& R.A.,Gujarat Ayurved University, Jamnagar - 361008 Gujarat (India)
Abstract: India is the second largest country in the world with 76 million elderly personsabove 60 years of age as of the 2011 Indian census. The elderly population (70 years and above)are projected to increase five fold from 2001-2051. Condition like Alzheimer’s disease, anotherdisorder that causes dementia or a condition that mimics dementia disrupts work, hobbies, socialactivities and family relationships. Yoga is the ancient science aimed to get eternal happinessthrough eight limbs that include Yama, Niyama, Asana, Pranayama, Pratyahara, Dharana, Dhyanaand Samadhi. All these stimulate and enhance the functioning of the various internal organs andalso in boosting overall health. Ageing can be improved with yoga, which prevents accumulationof stress metabolites and keeps the physiology supple. This paper emphasis on memory loss andsuggests preventive yogic practices for memory loss in geriatric age.
Keywords: Asana, Geriatrics, Memory loss, Yogic lifestyle.
IntroductionMemory loss and age-related problems are
major issues in Geriatrics. Projections made bythe United Nations has indicated that India willhave 198 million persons of 60+ in 2030 and326 million by 2050. In 2016, there will be anestimated 57 million males and 56 million femalesof 60 plus (1986-90 to 2011-16) (http:/socialjustice.nic.in/npopcomplete.php).
Mild memory impairment is a common,even normal, consequence of the ageing process.It becomes abnormal when it affects an abilityof an individual to function normally on a day-to-day basis. The reduced capacity of older peopleto learn and remember may be caused by stemcells in the brain dividing less frequently, ratherthan a shortage of neural stem cells as waspreviously thought (Gunther et al., 2001).Longitudinal studies in the elderly have revealeda gradual decline in the cognitive abilities of olderpeople, but differences between individuals inthe rate of decline suggest that at least some ofthe age-related deterioration is due to the inclusionof subjects with incipient dementia. The elderly
people may demonstrate an incipient phase forAlzheimer’s disease (AD) is supported by studiesin the elderly which have shown evidences ofAlzheimer’s disease years before clinicalsymptoms are evident and this is more commonin individuals with memory impairment in oldage (Alzheimer’s Association, 2004).
ObjectivesThe purpose of this study was to examine
directly the relationship between the practice ofyoga and its impact on memory loss in geriatricage. The attempt of the study was to identifydisease dictated by memory loss and preventionby yogic practices.
Major findings of Research studies onMemory loss
Some of the early symptoms of manydiseases consist of memory loss, confusionregarding time and place, problems with wordsin speaking or writing as well as changes inmood and personality. Age associated cognitiveimpairment can be accompanied by depression
1. Ph.D Scholar 2. Ph.D. Scholar 3. Associate Professor 4. Professor and HOD

Hetal et al.30
and changes in mood (Ownby RL et al., 2006;Rinck and Becker, 2003) and the data suggestthat mood disorders can aggravate the processes ofcognitive decline (Gualtieri CT et al., 2008).The effect of aging and memory loss onspirituality is less clear, although individuals withearly memory loss have often turned tospirituality as an important coping mechanism(Beuscher L et al., 2008). In fact, higher levelsof spirituality have been associated with a slowerrate of cognitive decline in patients with memoryloss (Kaufman Y et al., 2007).
Till now not many options in treatmentof age-associated memory loss and cognitiveimpairment are available especially with associatedmood-related problems. It may be possible totreat degenerative disorders including Alzheimer’sdisease, dementia and depression by stimulatingthe stem cells’ ability to divide and produce newnerve cells (Anonymous, 2006). According toWorld Health Organization, 25% of the worldpopulation is suffering from mental illnesses. Butonly 40% of such cases are diagnosed andtreated. One million annual suicides are the resultof these undiagnosed or missed cases(Anonymous, 2007). Most common causes forthese suicides are depression, dementia, anxietyand schizophrenia. These health issues arecharacterized by memory loss, confusion anddisorientation.
Prevention of Memory loss through YogaYoga is viewed as a physical, mental and
spiritual discipline that confers a sound bodyand mind (Mohan et al., 2002). Two of thephysical aims of yoga are Pranayama (breathingtechniques) and Asana (posture), while one ofthe mental aims is the ability to maintain cognitivecontrol, specifically in the areas of attention,memory and arousal control. One general claimis that yoga helps clear the mind and this mayhave an effect on the ability to attend to relevantstimuli and recall information subsequently(Heriza et al., 2004). Inverted yoga positionshave been associated with claims of increasedmemory and attention due to increased blood
flow to the brain. Yoga can prevent memorylapses by calming person and enhancingconcentration. It can also improve powers ofrecall by increasing circulation to brain.Specifically, two inverted poses are suggested,the Open-Legged Forward Bend and Threadingthe Needle (Schaeffer et al.,2006). Moreinverted poses including the headstand and child’spose are cited as ways to nourish the brain byincreasing circulation of blood and oxygen (http://www.womenfitness.net/yoga_ad.htm). A studyused both meaningful words and nonsensesyllables to test immediate (short-term) verbalmemory abilities before and after a one-monthperiod of yoga training for college-aged (15 to25 years) males and females. The results thoughincomplete, suggested that yoga did smooth theprogress of immediate memory presentation morethan the absence of yoga and that the advantagewas greater for males than females (Kocher etal.,1979).
Elementary school children who engagedin 30 minutes of yogic practices (by following avideotaped yoga session) twice a week for threeweeks increased their time on task (payingattention to the teacher or task at hand) duringthree weeks period and at a later follow-up date,while their classmates’ time on task remainedessentially unchanged (Peck et al., 2005). Similarwork studied the performance scores of childrenaged 11 to 16 years on verbal and spatial memorytests for two groups, one attending a yoga campand the other, a fine arts camp. Both groupswere tested initially and after 10 days of theirrespective interventions. At the final assessment,the yoga group showed a significant increase(43%) in spatial memory while the fine arts and(control group) showed no change. The resultssuggest that yoga practice, including Asana andPranayama improve delayed recall of spatialinformation (Manjunath et al., 2004). Memoryspan and attention measured before and afteryoga training changed positively as a result ofyoga training in primary school children(Anantharaman et al.,1984). Yoga has alsobeen utilized with limited positive results in

Prevention of Memory Loss through Yogic Lifestyle 31
rehabilitation with mentally retarded individuals(Pathak et al., 1984) and in training visualperceptual sensitivity (Manjunath et al.,1999).
The effect of yoga shows positive effecton the attention and behavior of boys withAttention-Deficit Hyperactivity Disorder (ADHD)(Jensen et al., 2004). Boys diagnosed withADHD were assigned to Yoga and Control group.Yoga group includes 20 yoga sessions and co-operative activities, respectively. Both groupswere assessed pre and post intervention on theConners’ Parent and Teacher Scale (Revised)(Conners et al., 1997) and the test of variablesof attention (Greenberg et al., 1997). Significantimprovements from pre-test to post-test werefound for the control group, but not the yogagroup on several subscales of the Conners’Teacher Rating Scales, while the opposite effectwas present on several subscales of the Conners’Parents Rating Scales. Some of the results ofthis study suggest that yoga may have merit asa complementary treatment for boys with ADHDalready stabilized on medication particularly forits evening effect when medication effects wereabsent. Five cognitive tests (color cancellation,digit forward, digit backward, recognition andvisual retention) were done to study the effectsof yoga over the time span of an academic yearfor 12 year old participants.
Results showed improvement on most testsfrom the beginning to the end of the school yearin both, a group that regularly participated inyoga and a group that did not. However, thestatistical analysis did not directly evaluate thecontrol and yoga groups, stating that the meanscore of the yoga group was slightly higher thanthe control group (Sahasi et al., 1984).
Similarly, Anuloma Viloma Pranayama(uninostril breathing) as part of a yoga techniqueincreased spatial memory scores by 84% butdid not cause an increase in verbal memoryscores (Naveen et al., 1997).
Literature review on Memory and YogaMemory is the capacity to retain and recall
information about past and present incidents. It
is the ability to analyze and synthesize theassimilated information and not for storage alone.In Sanskrit, the word ‘memory’ is called as‘Smriti’. The Yoga Sutra of Patanjali describesSmriti as ‘an experienced object not being lostfrom the mind’ (Mahaprabhulal Goswami,2009). Throughout the day, the mind is floodedwith many informations, data and newhappenings/developments/facts. Thus, mind hasits natural way to sieve out only the informationthat is pertinent or useful. Thus, it is essential totrain mind accordingly and ensure a healthy stateof functioning. Memory is the latent capacity toretain and recall information, yoga assists inimproving memory power through yogictechniques of Asana, Pranayama, Pratyaharaetc. The brain functions of attention, cognition,processing of sensory information and visualperception are honed with yogic practices.Patanjali has classified mental functions in tofive categories viz. Pramana (means of validknowledge), Viparyaya (illusion), Vikalpa(imagination), Nidra (sleep) and Smriti (memory)(Mahaprabhulal, 2009). Here, Smriti is recallingof our previously recorded experiences.Perception, illusion, imagination and sleep areregistered to find out whether it is matched withany previously stored information. Sometimesthis stimulus is generated in the Chitta itself inthe form of thoughts. This also triggers therecollection of the past memory.
Hatha Yoga emphasizes ‘Chitta Vishranti’i.e. the tranquility at the level of consciousness(Chamanlal, 1997). Yogic practices like Asana,Pranayama, Dhyana, Om chanting increase thecirculation of blood to the brain. It is directlyrelated to awareness and aims at release oftensions working at the level of consciousness(Chitta). This helps calm the mind and enhancesconcentration skills. Memory lapses can also beprevented through yogic practices that enhancethe power of recall. One can draw upon theimmense power of the mind with consistent yogicendeavor.
Two of the physical steps in yoga practiceare Pranayama and Asana while one of the mental
Figure 7

Hetal et al.32
aims is the ability to maintain cognitive control,specifically in the areas of attention, memoryand arousal control. One common claim is thatyoga helps to clear the mind and this may havean effect on the ability to attend to relevant stimuliand recall information subsequently (Heriza etal., 2004).
Findings based on Literature reviewYoga can help reduce and in some cases
eliminate drug dosage and dependence in patientssuffering from memory loss, diabetes mellitus,hypertension, epilepsy, anxiety, bronchial asthma,constipation, dyspepsia, insomnia, arthritis,sinusitis and dermatological disorders (http://health.yahoo.com/health/ency/adam/000760/_overview). Pranayama and Pratyahara areextremely efficient techniques to divert individual’sattention from the objects of outer environment,to increase every person’s energy potentials andinteriorize them, to achieve control of one’s innerfunctioning. Memory span and attention,measured before and after Yoga training, changedpositively (Anantharaman et al., 1984). Omkarmeditation increases the efficiency of cells andorgans. Omkar recitation is an important andwell known yogic practice. It is generallyprescribed before and/or after every session ofyogic practices (Vishwas et al., 1995).
ImplicationsThere are many yogic techniques that
stimulate the brain and nervous system to improvememory and concentration. Yoga provides anexcellent tool for improving memory power andfighting forgetfulness. Hatha yoga is a gentleform of yoga that consists of Asana, Pranayama,Dhyana and Om chanting, to achieve clarity ofthe mind that translates into all round good health.Memory power is given a boost while alsoimproving the ability to maintain focus andconcentration.
The Five steps of yogic lifestyle for overallwell being
1. Right posture - Asana
2. Right breathing - Pranayama3. Right cleansing - Shuddhi kriya4. Right diet - Satvika ahara5. Right mindset - DhyanaThere are some yogic techniques that
exclusively stimulate the brain and nervous systemto improve memory and concentration.
AsanaInverted postures nourish the brain by
increasing circulation of blood and oxygen.Abundant blood is supplied to the brain duringpractice of Shirshasana. This is to improvememory and for increasing intellectual powers.Exercise boosts circulation, including blood flowto the brain which uses a full 25 percent of theoxygen that enters our lungs(www.yogapoint.com). It also boost brain-nurturing chemicals and reduces stress, whichhas been shown to damage the brain. Physicalactivity can also ease depression and delay theonset of Alzheimer’s disease. The Asanas usinga Drishti (gazing point) especially during balancingpostures improves mental concentration. Spinelengthening postures, the forward and backbending poses, activate the spinal column andstimulate the nervous system.
Types of AsanaAsana are not aimed at mere toning of the
physical body. They are designed to activateenergy channels thereby empowering the bodyfrom within.
During Asana practice, it is important tofocus the eyes at the point between the eyebrowswhich promotes memory power (Udupaet al.,1978). One must gently do away withrestless thoughts and be aware of the movementsof the body. Following Asana are useful for thesepurposes which can easily done by senior citizens.
1. Vrikshasana 2. Natarajasana 3. Sarvangasana 4. Matsyasana 5. Bhujangasana 6. Bhadrasana

Prevention of Memory Loss through Yogic Lifestyle 33
7. Shavasana 8. Padmasana 9. Siddhasana10. Vajrasana11. Ustrasana12. Tadasana etc.
PranayamaIn Pranayama, the mind is focused on
breath as it flows in and out of the body. Oxygenand Prana (energy) levels in mind and body alsoelevate due to the regulation of breath. Anyactivity which requires a total concentration ofmind will control the breath also. Pranayamaaims primarily on the control of mind. Anuloma-Viloma, Bhastrika, Kapalbhati and BhramariPranayama are the best. Pranayama increasesconcentration as well as nourishes the brain. Yogicbreath or Pranayama is an excellent way torevitalize Prana and to train the mind to bepresent and alert. Pranayama cleanses andstrengthens the physical body while calming andclearing the mind (M.M. Gore, 1991).
Shuddhi KriyaTratak Kriya: Improves concentration,
memory and mental power (Gheranda Samhita,1999). It also increases working efficiency andthe ability to read other’s mind.
Kapalbhati Kriya: Kapalbhati kriyadecreases Kapha dosha responsible for the Tamasavarana of the Chitta. After this Kriya the doshais removed and the Satva guna is elevatedresulting improvement in memory (GherandaSamhita, 1999).
This Pranayama supplies pure life energyto the brain. It increases the blood circulation inthe brain and removes blood clots therebyimproving the memory power. Other than this,the toxic and foreign substances from the bodyare evacuated (http://yousigma.com/health/yogaandbenefitssummary.html).
Sattvika AharaA yogic diet ideally follows a Sattvika or
pure vegetarian food. A balance of fresh fruit,
vegetables, whole grains, milk, nuts and seedsin combination of both raw and cooked foodscan be balanced yogic diet. These foods increasesSattva in the body because they are light, simpleand full of necessary nutrients. Such yoga dietand lifestyle increases physical and mental vitalitymaking anybody easier to experience clarity,lightness and peace of mind.
DharanaDeshah Bandhah Chittasya Dharana.
(Patanjali Yoga Sutra, 2009). It is the practiceof fixing the mind to an object for concentration.Daily practice of Dharana reduces the waveringattitude of mind and different kind of peace canbe observed throughout the day (Riyaz et al.,2007). Routine practice of Dharana improvesmemory by controlling fluctuation of thoughts.
Dhyana (Meditation)Tatra Pratyaya-Ekatanata Dhyanam
(Patanjali Yoga Sutra, 2009). When the mindremains without distraction on an object for along time, it is called meditation.
Dhyana is a state of mind where no sensualthoughts or no contents occupying the mind. Itis a step beyond Dharana, requiring even moremental focus and concentration. This practicecontrols the mind and make it more consciousto pay attention on selected subject which furtherleads to increase Smriti power by decreasingChittavritti.
Yogic Mudra (Posture)Mudra stimulate Agya Chakra by making
concentration on this Chakra which is situatedat the centre of the brain and therefore brainstarts working speedily and increase memory(Asana Pranayama Mudra Bandha, 2005).
Sukshma Vyayama (Light exercise)Memory can also be improved by some
light exercise i.e Buddhi and Dhriti vikasaka,Samaran shakati vikasaka and Medha Shaktivikasaka. Types of Sukshma vyayama, reducethe Kapha avarna and balance the Vata Nadi to
Hetal et al.34
increase memory and intellectual power (YogicSukshma Vyayama, 1906) .
ConclusionEffectiveness of yoga therapy to improve
memory, healing of psychosomatic and stress-related conditions is world wide accepted factand same stands true in geriatrics also. Thepositive effect of this therapy is obtained bybridging positive co-ordination between body andmind. Traditional yoga was primarily concernedwith spiritual transcendence, yoga therapy aimsat holistic treatment of a variety of psychosomaticdisorders ranging from memory loss to cognitivedisability. The best feature about yoga, whichmakes it ideal as a tool for enhancing memory isthat it utilizes various components to increaseoverall body and brain function.
References1. Alzheimer’s Association. Alzheimer’s Disease
Statistics. Retrieved November 2, 2004 from thehttp: //search.alz.org/Resources/FactSheets/FSAlzheimerStats.pdf accessed on 11th Oct. 2012.
2. Anantharaman et al. A study of Yoga. Journalof Psychological Researches 1984; 28(2):97-101.
3. Anonymous, Dementia: Supporting people withdementia and their health and social care, NICEClinical Guideline 2006; 102.
4. Anonymous, Memory assessment service for theearly identification and care of people with dementia,NICE Commissioning Guide 2007; 609.
5. Beuscher L et al. A literature review of spiritualityin coping with early-stage Alzheimer’s disease. JClin Nurs 2008; 17:88–97.
6. Chamanlal Gautam. Gheranda Samhita, 2ndchapter, Samskriti Samsthana, Nava Jyoti Press,Mathura (1999).
7. Chamanlal Gautam. Hath Yoga Pradipika, 2ndUpadesha 2/14, Samskriti Samsthana, Nava JyotiPress, Mathura (1997).
8. Conners et al. Conners’ rating scales-revised.Toronto, Canada: Multi-Health Systems 1997;
9. Dhirendra Bhrahmachari. Yogic SukshmaVyayama, Vishvayatana Yogashrama, Jammu(1906).
10. Greenberg et al. Test of Variables of Attention(TOVA) visual continuous performance test. LosAlamitos, CA: Universal Attention Disorders1997; 23-34.
11. Gualtieri CT et al. Age related cognitive declinein patients with mood disorders. Prog NeuroPsychopharmacol Biol Psychiatry 2008; 32:962–67.
12. Gunther, S. and Weber-Mack. The experienceof Alzheimer’s Disease: The family’s perspective.Alzheimer’s Care Quarterly 2001; 2(3):1-4.
13. h t t p : / / y o u s i g m a . c o m / h e a l th /yogaandbenefitssummary.html assessed on 29-7-2013.
14. Heriza et al. Yoga: A complete guide to the medicalbenefits of yoga (yoga for health). Los Angeles,CA:Tarcher 2004; 32(3):57-81.
15. http://health.yahoo.com/health/ency/adam/000760/_overview accessed on 1/9/2010
16. http: //socialjustice.nic.in/npopcomplete.phpAccessed on 11th Oct. 2012.
17. Jensen et al. The effects of Yoga on the attentionand behavior of boys with Attention-Deficit/hyperactivity Disorder (ADHD). Journal ofAttention Disorder 2004; 7(4):205-16.
18. Kaufman Y et al. Cognitive decline in Alzheimerdisease: Impact of spirituality, religiosity, andQOL. Neurology 2007; 68:1509-14.
19. Kocher et al. Effect of yogic practices onimmediate memory. Society for the NationalInstitutes of Physical Education and Sports Journal1979; 2(2):36-38.
20. M.M. Gore. Anatomy and Physiology of YogicPractices. Kanchan Prakashan, Pune 1991;111-12.
21. Mahaprabhulal Goswami. Patanjala Yoga Sutra:Samadhi Pada ½, Chaukhambha SanskritSamsthana, Varanasi (2009).
22. Manjunath et al. Improvement in visualperceptual sensitivity in children following yogatraining. Journal of Indian Psychology 1999;17(2):41-45
23. Manjunath et al. Spatial and verbal memory testscores following yoga and fine arts camps forschool children. Indian Journal of Physiology andPharmocology 2004; 48(3):353-6
24. Mohan et al. Yoga for body, breath, and mind: Aguide to personal reintegration. Boston,MA:Shambala 2009; 209.
25. Naveen et al. Yoga breathing through a particularnostril increases spatial memory scores withoutlateralized effects. Psychological Reports 1997;81(2):555-61.
26. Ownby RL et al. Depression and risk forAlzheimer disease: systematic review, meta-analysis and meta-regression analysis. Arch GenPsychiatry 2006; 63:530-38

Prevention of Memory Loss through Yogic Lifestyle 35
27. Pathak et al. Rehabilitation of mentally retardedthrough yoga therapy. Child Psychiatry Quarterly1984; 17(4):153-58
28. Peck et al. Yoga as an intervention for childrenwith attention problems. School Psychology Review2005; 34(3):415-24.
29. Rinck M, Becker E. Selective memory andmemory deficits in depressed inpatients. DepressAnxiety 2003; 17:197–206
30. Sahasi et al. A replicated study on the effects ofyoga on cognitive functions. Indian PsychologicalReview 1984; 33-35.
Address for correspondence: Dr. Hetal Amin, Ph.D Scholar, Department of Basic Principles, IPGT & RA,Gujarat Ayurved University, Jamnagar -361008 Gujarat (India). E-mail: [email protected]
82-1356596424 of 2013
31. Satyanand Saraswati. Asana Pranayama MudraBandha, Bihar Yoga Vidhyalaya, Munger (Bihar),2005; 116
32. Schaeffer et al. Sharpen your memory with yoga.Natural Health 2006; 40(6):14.
33. Udupa KN. Disorders of stress and theirmanagement by yoga. Banaras Hindu university,Varanasi, 1978.
34. Vishwas et al. Effect of Omkar Chanting onConcentration, Memory and Level of Fatigue1995; 45.
35. www.yogapoint.com accessed on 1/9/2010.

36

J Res Educ Indian Med, Jan.-March 2014; Vol. XX (1): 37-44 ISSN 0970-7700
CLINICAL EVALUATION OF VARADI KWATHA IN THE MANAGEMENTOF MADHUMEHA (TYPE-2 DIABETES MELLITUS) - AN ATTEMPT TO PROVIDE
EVIDENCE BASED DATA TO THE CLASSICAL THERAPEUTIC CLAIMS
GYANESHWARSING GUDDOYE,1 B.K. DWIBEDY2 AND O.P. SINGH3
Department of Siddhant Darshan,1,2 Department of Kayachikitsa,3 Faculty of Ayurveda,Institute of Medical Sciences, Banaras Hindu University, Varanasi- 221005 U.P. (India)
Abstract: The Madhumeha (DM-II) treatment in general all over the world has been primarilyfocusing on blood glucose control (hypoglycemic effect). In the classical textbooks of Ayurveda,several important subjective signs and symptoms of Madhumeha have been described. However,there are only a few studies that have explored the effectiveness of various formulations on thesesubjective parameters. Therefore, the present work was planned to evaluate the effect of Varadikwatha (VK) on both objective and subjective parameters. The VK was chosen because it waseconomical and hence, accessible to the poor people. It also contains the ingredients mostly withTikta (bitter) and Kashaya (astringent) Rasa (tastes). 23 diagnosed patients having signs andsymptoms of DM-II as per WHO guidelines were enrolled in the study. The patients were givenVaradi Kwatha containing the following herbal ingredients: (1) Vatsak (Holarrhena antidysenterica)(2) Triphala (Terminalia chebula, Embelica officinalis, Terminalia belerica) (3) Darvi (Cosciniumfenestratum) (4) Mustaka (Cyperus rotundus (5) Beejaka (Pterocarpus marsupium). The patientswere given VK in a dose of 24 ml twice a day for 8 weeks. A highly significant improvement wasobserved in most of the subjective parameters. All the 23 patients showed a good improvementof more than 75% in cardinal symptoms like Prabhuta mutrata, Avila mutrata, Galatalushosha,Daurbalya and Pipasadhikya etc. In terms of biochemical objective parameters, the mean FBS of207.65±78.43 mg/dl showed a decrease to 162.86 ±72.66 mg/dl and the mean PPBS showed adecrease from 278.89±131.96 mg/dl to 223.30±106.04 mg/dl.
Keyword: Ayurvedic treatment, Diabetes mellitus Type-2, Madhumeha, Medicinal plants,Varadi kwatha.
IntroductionThe management of Madhumeha (Diabetes
mellitus Type-2) (DM-II) is generally focusedon blood glucose control and it is commonlyobserved in our day to day practice that most ofthe modern oral hypoglycemic drugs have sideeffect such as constipation. It has also beenobserved that these drugs have only a minimaleffect in the management of subjectiveparameters. In this context, World HealthOrganization has stated that: 1. 347 million peopleworldwide have diabetes. 2. In 2004, anestimated 3.4 million people died fromconsequences of high fasting blood sugar.3. More than 80% of diabetes deaths occur inlow and middle income countries.4. WHO projects that diabetes will be the 7th
leading cause of death in 2030. [http://www.who.int/mediacentre/factsheets/fs312/en/]
Considering these facts, the present studywas designed with special attention to observethe therapeutical effect of Varadi Kwatha(Sarangadhara Samhita, 2000) on Madhumeha(DM-II). This formulation is predominantly Tikta(bitter) and Kashaya (astringent) and has Laghu(light) and Ruksha (dry) properties.
Tables 1 and 2 summarise the ingredientsof this formulation, along with their Rasa, Guna,Virya, Vipaka indications and active principles.
The test formulation contains the followingherbal ingredients:
(1) Vatsak (Holarrhena antidysenterica)which is commonly known as Kutaj. It is bitterand pungent in taste having drying property.
1. Ph.D. Scholar 2. Professor and HOD 3. Assistant Professor

Guddoye, Dwibedy and Singh38
It reduces Kaphapitta in the body and hasactive principles such as conessine, kurchine etc.
(2) Haritaki (Terminalia chebula) ispredominantly astringent in taste. It is light anddry in properties with a hot potency. It hastannin, chebulinic acid and gallic acid as activeprinciples.
(3) Amlaki (Embelica officinalis) is sourin taste predominantly having light, dry and coolproperties. It is Tridoshahara and Pitta Shamaka.It has vitamin C, tannic acid and gallic acid asmain active principles.
(4) Vibhitaki (Terminalia belerica) isastringent in taste predominantly having light anddry properties. It reduces Kapha. It has tannicacid and allic acid as main active principles.
(5) Darvi (Coscinium fenestratum) is bitterpredominantly having light and dry properties. Itreduces Kaphapitta. It has barberine, oleric acidand saponin. Also it is noted that “serum glucosecould be significantly reduced by saponin” [http://www.ncbi.nlm.nih.gov/pubmed/12583337]accessed on 14.7. 2013 at 2125 hrs which helpto reduce DM.
(6) Mustaka (Cyperus rotundus) is bitter,pungent and astringent predominantly. It reducesKaphapitta. It has an aromatic oil as activeprinciple which aphrodisiac property.
(7) Beejaka (Pterocarpus marsupium) isbitter, astringent predominantly having light, dryproperties and a hot potency. It reduces Kaphaand Vata. It has kinotannin, gallic acid andpyrocatechin as main active principles.
Taking the above facts into considerationthe present study was carried out with specialattention to the therapeutic effect of Varadikwatha on the objective parameters mentionedin Table 5 as well as the subjective parametersmentioned in Table 4 of Madhumeha (DM-II).
Aim and ObjectiveThe aim and objective of the present study
was to evaluate the effect of Varadi kwatha inMadhumeha (DM-II) on subjective and objectiveparameters.
Materials and MethodsThis study was cleared by the Institute
ethical committee with clearance letter no. Dean/2013-14 EC/273 dated 10.05. 2013 andregistration number IC/Ph.D.11/SF/IMS/SD (Ay)/401/4853.
1. Patients: For the present study Twentythree diagnosed patients of Madhumeha (DM-II)were registered from out-patient department ofKayachikitsa, SS Hospital, Institute of MedicalSciences, Banaras Hindu University, Varanasibetween January 2012 and July 2012.
They were assessed on the basis of signsand symptoms of Madhumeha as per Ayurvedicclassics and modern medical science. The patientswho were already on allopathic hypoglycemicdrugs were excluded and not registered for thestudy.
All the patients were only kept on Varadikwatha (decoction) during 8 weeks of trial.
2. Drugs: The raw herbs listed in Table 1were procured from the authentic suppliers fromthe market. The drugs were further authenticatedby the experts from the department ofDravyaguna. Varadi yavkuta (coarse powder)was prepared in the Institute’s AyurvedicPharmacy, Faculty of Ayurveda, I.M.S, BanarasHindu University, Varanasi.
3. Inclusion criteria: Patients of eithersex in the age groups between 30 to 65 yearswith classical symptoms of Madhumeha and whowere not taking allopathic hypoglycemic medicine,
Table 1. Contents of Varadi kwatha (decoction).
Sr. No.
Sanskrit Name
Botanical name Part Used
Propor-tion
1. Vatsaka / Kutaja
Holarrhena antidysenterica
Bark
Skin 1 part
2.
Triphala Haritaki Amalaki Vibhitaki
Terminalia chebula Embelica officinalis Terminalia belerica
Fruits
1/3rd
part
each
3. Darvi / Daruhridra
Coscinium fenestratum
Stem
Arial 1 part
4. Mustaka / Nagarmotha
Cyperus rotundus Rhi-
zome 1 part
5. Beejaka / Vijayasara
Pterocarpus marsupium
Heart
Wood 1 part

Varadi Kwatha in Management of Type-2 Diabetes Mellitus 39
provided they fulfilled other diagnostic criteriafor DM-II, were included in the study.
4. Diagnostic criteria: Standard criteriaof National Diabetes Data Group and WHO forDM-II was adopted (Adopted by American DiabeticAssociation) (Dennis L. Kasper et al., 2005).Symptoms of diabetes + random blood glucose200 mg/dl till 500 mg/dl or fasting blood glucose126 mg/dl till 375 mg/dl or two hours bloodglucose 200 mg/dl (during an oral glucosetolerance test). Along with above criteria, thefollowing subjective signs and symptoms werealso considered while registering the patients.
Patents showing at least 8 or more signsor symptoms were included in the study:1. Prabhuta mutrata (M Ni-36/6)2. Avila mutrata (M Ni-36/6)3. Pipasadhikya (SS Ni-6/5)4. Alasya with Utsahahani (CS-Ni-4/47)5. Kshudhadhikya/Mahashanam (CS Ni-4/51)6. Pindikodveshthan (SS Ni-6/5)7. Karapadatala dah (SS Ni-6/6)8. Karapadatala suptata (CS Ni-4/47)9. Swedadhikya (M Ni-34/3)10. Gala talu shosha (CS Ni-4/47)11. Daurbalya (CS Ni-4/48)12. Shrama shwasa (M Ni-34/3)13. Shula (CS Anubhuta base on Ni-4/48)14. Alasya / Utsahahani (SS Ni-6/6)15. Klaibya (M Ni-34/3)16. Nidradhikya (SS-6/5)17. Purishabadhdhata (SS-6/5)
5. Exclusion criteria: As per AmericanDiabetic Association - accepted by WHO.(Dennis L. Kasper et al., 2005)(a) Patients with juvenile diabetes.(b) Age of patient less than 30 years and more than 65 years.(c) Patients having IDDM and receiving insulin (type 1).(d) Excessive blood glucose (FBS) > 375 mg/dl and (PPBS)>500 mg/dl.(e) Chronic complications [micro vascular and macro vascular] were discarded.
6. Investigations: Biochemical exami-nations like Blood sugar: Fasting and postprandial,
Lipid profile and Serum creatinine were done inorder to assess the functional status of kidney,blood glucose and blood lipid status. Theseinvestigations were carried out in the VikritiVigyan laboratory of SS Hospital, IMS, BHU,Varanasi.
7. Study design: The present study wasa drug interventional study. On the basis ofvarious objective and subjective parameterspatients were compared before and afterintervention of Varadi kwatha (decoction drug).
Management of the PatientsGrouping, drug dosage, duration and
method of administration, Pathya-apathya.
1. Dose and duration: The patients wereprovided with the air-tight packets of coarselypowdered dry herbs in a dose of 12 g per packetand were advised to prepare Kwatha in thefollowing manner: For preparing a single doseof Varadi kwatha (decoction), 12g of Varadiyavkuta (course drug) and 240 ml of water wereto be taken in a vessel. Then the water wasto be boiled and reduced till 24 ml at mediumflame. The decoction was then to be filtered andgiven for 8 weeks in a dose of 24 ml twice a day.2. Method of administration: All the patientswere advised to consume Varadi kwatha(decoction) in a fixed dose of 24 ml twice a dayat morning and evening hours in empty stomach(before food) for 8 weeks.3. Pathya-apathya: Patients were advised torestrict carbohydrate diet and to correct theirdietary habits. Mild to moderate exercise as pertheir capacity was suggested. Also they wereadvised not to take milk and curd in their diet.4. Criteria for assessment: Coarsely powderedVaradi drugs were given to the patients everyweek after recording all the laboratoryinvestigations and noting the changes insubjective parameters like Prabhuta mutrata,Avila mutrata, Pipasadhikya, Alasya withUtsahahani etc.using the specific rating scaleat weekly interval.

Guddoye, Dwibedy and Singh40
Grading of Subjective parameters
Table 3. Criteria for assessment of therapy.
Description Grading
Control of the disease 100% relief
Marked improvement 75% relief
Moderate improvement 50% to74% relief
Mild improvement 25% to 49% relief
No improvement 25% relief
Statistical analysisMean, percentage relief, S.D, S.E, t and p
values have been calculated. Paired ‘t’ test has
After completion of treatment al linvestigations data were taken again and allobjective parameters like FBS, PPBS, Fastingurine sugar, Serum triglyceride, Serumcholesterol, HDL cholesterol, Serum creatinine,LDL, VLDL were utilized for statistical analysis.
The patients were asssessed as:- Control(when relief is 100%), Marked improvement(whenrelief is 75 %), Moderate improvement (when reliefis 50-74%), Mild improvement (when relief is25-49%) and No improvement <25 %) (Table 3)as per percentage relief based on grading.
Symptom Grading 1. Prabhuta Mutrata (Polyuria) :
1.50 to 2.00 liters / 24 hrs. 0 >2.00 to 2.50 liters / 24 hrs 1 >2.50 to 3.00 liters / 24 hrs 2 >3.00 liters / 24 hrs. 3
2. Avila Mutrata (Turbidity in urine) : Crystal clear fluid 0 Faintly cloudy or hazy with slight turbidity. 1 Turbidity clearly present and newsprint easily read through test tube.
2
Newsprint not easily read through test tube. 3 Newsprint cannot be visualized through test tube. 4
3. Pipasaadhika (Polydypsia) : Feeling of thirst 7 – 9 times/24 hours, either/or Intake of water 5 – 7 times/24 hours with quantity 1.5 – 2.0 liter/24 hours. 0
Feeling of thirst 9 - 11 times/24 hours, either/or Intake of water 7 - 9 times/24 hours with quantity 2.0 - 2.50 liter/24 hours 1
Feeling of thirst 11 – 13 times/24 hours, either/or Intake of water 9 – 11 times/24 hours with quantity 2.50 -3.00 liter/24 hours
2
Feeling of thirst >13 times/24 hours, either/or Intake of water >11 times/24 hours with quantity >3.00 liter/24 hours 3
4. Bahavashi -Kshudha- Adhika (Increase in appetite) : As usual / routine. 0 Slightly increased (1 – 2 meals) 1 Moderately increased (3 – 4 meals) 2 Markedly increased (5 – 6 meals) 3
5. Bahavashi -Abhyavaharana Shakti (Excess intake of food) :
Taking food in normal quantity twice /a day 0 Taking food in excessive quantity twice/ day 1 Taking food in moderate quantity twice in a day 2 Person taking food in less quantity twice in a day 3 Person taking food in less quantity once in a day 4 Person not at all taking food 5
6. Pindikodveshtana (Cramps) : No cramps 0 Cramps after walking more than 1 km. 1 Cramps after walking ½ km 2 Inability in walking even ½ km 3
7. Karapadataladaha (Burning sensation in palm and foot) : No suptata 0 Kara-Pada daha incontinuous 1 Kara-Pada daha continuous but bearable and not severe 2 Kara-Pada daha continuous and severe and unbearable 3
8. Karapadasuptata (Numbness in palm and foot) : No suptata 0 Kara-Pada Suptata incontinuous 1 Kara-Pada Suptata continuous but bearable and not severe 2 Kara-Pada Suptata continuous and severe and unbearable 3
9. Swedadhikya (Excess perspiration) : Sweating after some strenuous work or in hot and humidity 0 Profuse sweating after moderate work and movement 1 Sweating after little extra work than routine and movement 2 Profuse sweating after routine work 3 Sweating even at rest or in cold climate 4
Symptom Grading 10. Gala talu shosha (Dryness in mouth) :
Feeling of mouth dryness 0 time/24 hours 0 Feeling of mouth dryness 1 time/24 hours 1 Feeling of mouth dryness 2 times/24 hours 2 Feeling of mouth dryness >3 times/24 hours 3
11. Daurbalya (Weakness) : Can do routine exercise/work 0 Can do moderate exercise with hesitancy 1 Can do mild exercise only, with difficulty 2 Cannot do mild exercise too 3
12. Shrama Shwasa (Dyspnoea) : Dyspnoea after heavy work and walking 0 Dyspnoea after moderate work and walking 1 Dyspnoea after mild work 2 Dyspnoea even at resting condition 3
13. Shula (Pain) : No pain 0 Pain in joint, routine movements normal 1 Pain in joint, slight limitations of movements 2 Pain in joint, limitations of movements with much reduced activity.
3
14. Alasya/Utsahahani (General Debility) : No Alasya (doing satisfactory work with proper vigor and in time
0
Doing satisfactory work with late initiation, likes to stand in comparison to walk
1
Doing unsatisfactory work with late initiation, likes to sit in comparison to stand
2
Doing unsatisfactory work with very late initiation, likes to lie down in comparison to sit.
3
Does not want to do work with no initiation, likes to sleep in comparison to lie down
4
15. Klaibya (Loss of libido) : Normal 0 Decreased frequency with normal performance 1 Decrease frequency with insufficiency 2 No sexual stimulation at all 3
16. Nidradhikya (Excess of sleep) : Normal and sound sleep for 6 – 8 hrs. /24 hrs. with feeling of lightness and relaxation in the body and mind
0
Sleep> 8 -9 hrs. /24 hrs. with slight heaviness in the body. 1 Sleep >9-10 hrs. /24 hrs. With heaviness in the body associated with Jrimbha.
2
Sleep >10 hrs. /24 hrs. With heaviness in the body associated with Jrimbha and Tandra.
3
17. Purishabadhdhata/Malaupathijatila bhava (Constipation): Stool passes as per normal schedule 0 Passes stool with strain, sometimes takes purgative 1 Passes stool after more than 24 hours, frequently takes purgative
2
Passes stool after gap of one day, normal purgatives does not work
3

Varadi Kwatha in Management of Type-2 Diabetes Mellitus 41
been used for calculating the ‘t’ value in thepaired data.
For the assessment of the effect of thetherapy following chief complaints andbiochemical parameters have been selected:-1. Prabhutamutrata 2.Avila mutrata 3. Pipasaadhika 4. Kshudha adhika 5. Hastapadataladaha 6. Kara-pada suptata 7. Fasting bloodsugar 8. Postprandial blood sugar and 9. Serumcholesterol. The overall percentage improvementof each patient was calculated by the followingformula:
Nidradhikya, Purisha-badhdhata, Kara-padataladaha, Karapadatalasuptata,Swedadhikya.
Table 5 shows the effect of Varadi kwathaas follows:- a highly significant (p<0. 001)reduction were observed in FBS and PPBS whilesignificant fall (p<0.05) was observed in fastingurine sugar, serum triglyceride, serumcholesterol, LDL, VLDL and non significant(p>0.05) were observed in serum creatinine andHDL cholesterol.
Table 6 shows the %age of improvementof Varadi kwatha in 23 patients where 17 patients(74%) got moderately improved, 6 patients (26%)got improved mildly, No patient (0%) reportedcontrol of the disease. No side effect wasreported in any of the patients.
DiscussionExplanation of the claimed effect of Varadikwatha in Madhumeha (DM-II) treatment.
There was a significant reduction inPrabhuta mutrata (polyurea), Pipasaadhikya(polydypsia) and Galatalushosha (dryness inmouth) (p<0.001). Varadi kwatha has helped toclear the Ama (toxic substances) which was
The result thus obtained from individualpatient was categorized as mentioned above.
ResultsTable 4 shows the effect of Varadi kwatha
as follows: - A highly significant (p<0.001)reduction was observed in Prabhuta mutrata,Avil mutrata, Klaibya, Pipasadhikya,Pindikovestana, Galatalushosha, Daurbalya,Shramashwasa, Kshudhadhikya, Abhya-varanashakti shula, Alasya / utsahahani,
Table 2. Showing literary review of medicinal plants contained in Varadi kwatha.
Characteristics / Medicinal plants name
Properties Haritak* Amalaki * Vibhitaki* Darvi/
Kasthadaru Mustaka/
Nagarmotha Beejaka/ Vijaysara
Rasa Tikta, Katu Kashaya** Amla# Kashaya Tikta Tikta, Katu, Kashaya
Kashaya, Tikta
Guna Ruksha Laghu Ruksha
Laghu, Ruksha, Shita
Laghu, Ruksha
Laghu, Ruksha
Laghu, Ruksha
Laghu, Ruksha
Virya Shita Ushna Shita Ushna Ushna Shita Ushna
Vipaka Katu Madhura Madhura Madhura Katu Katu Katu
Doshakarm Kaphapitta shamaka
Tridoshahar & Vata shamaka
Tridosha, har Pitta shamaka
Kapha & Tridosha-ghna
Kaphapitta shamaka
Kaphapitta shamaka
Vata kapha shamaka
Prabhava Nil Nil Nil Nil Nil Nil Nil
Roga Prameha etc
Prameha etc
Prameha Caksusya Daurbalya, Agnimandya & Ajirna
Daurbalya, kasaswasa, Aruchi
Prameha, Mutra basti-vikara
Active principles
Conessine
Kurchine etc
Tannin,
Chebulinic
acid etc
Vit C,
Tanicacid
gallic acid
Tennin,
Gallo-
tanic acid
Berberine,
oleic acid,
saponin
Aromatic oil
0. 5-0. 9%,
Aphrodisiac
Kinotannin,
galic acid,
pyrocatechin
Referances ***
P 373
Vol.2
P 749
Vol.1
P 103
Vol.1
P 368
Vol.1
P 201
Vol.2
P 640
Vol.2
P 395
Vol.1
*=in-Triphala ** = Kashaya main & pancha-rasa with lavana varjita # = main & Madhura, Katu, Tikta, Kashaya
***=Reference: Dravyaguna Vigyana by Gynendra Panday, Edition 2004
X 100Total BT - Total AT Total BT

Guddoye, Dwibedy and Singh42
accumulated in body as hypergltcemia (referFBS, PPBS and fasting urine sugar in Table 5).Thus Varadi kwatha could also help in regulatingthe water balance of the Mutra vaha srotas(urinary system) and mouth dryness. A decreasein FBS, PPBS (p<0.001) and (p<0.05) in fastingurine sugar were noted. The treatment probablyhas enhanced the metabolism of glucose.Presence of substances like tannic (Table 2)created an acidic PH which helped in reductionof Kapha (unctuous particles) qualities such as
Guruta and Snigdhata in patients. This resulteda proper functioning of Vayu and enhancementof Agni bala finally leading to a reduction(p<0.05) in serum triglyceride, serum cholesterol,LDL and VLDL.
As regards to post treatment improvementin Klaibya (loss of libido) (p<0.001), this is effectof Mustaka (Cyperus rotundus) a constituent ofVaradi kwatha having aphrodisiac quality(Table 2). Varadi kwatha could also rectify theSrotorodha (blocked channels) and thus can
Table 4. Effect of therapy on Ayurvedic symptoms (subjective parameters) in 23 patients.
Sr. No.
Symptoms (Subjective parameters) n
BT Mean ± SD
AT Mean ± SD
% Change
Diff. BT-AT Mean ± SD
t p
1. Prabhuta Mutrata (Polyuria)
17 1.82
± 0.81
0.35
± 0.49 80.65
1.47
± 0.62 9.71
<.001
HS
2. Avil Mutrata
(Turbidity in urine) 15
1.4
± 0.83
0.2
± 0.41 85.71
± 1.2
0.77 6.00
<0.001
HS
3. Pipasaadhikya (Polydypsia)
19 2.67
± 0.84
0.39
± 0.61 84.31
± 2.28
0.96 10.08
<0.001
HS
4. Kshudhadhikya (Increase in appetite)
16 1.50
± 0.63
0.13
± 0.34 92
± 1.38
0.72 7.65
<0.001
HS
5. Abhyavarana shakti (Excess food intake )
15 1.47
± 0.64
0.13
± 0.35 91
± 1.33
0.72 7 . 1 4
<0.001
HS
6. Pindikovestana (Cramps)
17 2.06
± 0.66
0.53
± 0.62 71.42
± 1.47
0.80 7 . 5 8
<0.001
HS
7. Karapadataladaha (Burning sensation in
palm and foot)
12 2.00
± 0.74
0.5
± 0.52 75.00
± 1.5
0.52 9.95
<0.001
HS
8. Karapadatala suptata
(Numbness in palm and
foot)
17 1.88
± 0.70
0.35
± 0.49 81.25
± 1.53
0.80 7.88
<0.001
HS
9. Swedadhikya (Excess perspiration)
17 2.18
±0.81
0.29
± 0.59 86.49
± 1.88
1.00 7.82
<0.001
HS
10 Gala talu shosha (Dryness in mouth)
15 1.67
± 0.90
0.33
± 0.62 76.00
± 1.27
0.96 5.10
<0.001
HS
11. Daurbalya (Weakness)
22 2.09
± 0.87
0.40
± 0.59 78.26
± 1.64
0.90 8.51
<0.001
HS
12. Shrama shwasa (Dyspnoea)
8 1.63
± 0.52
0.38
± 0.52 76.92
± 1.25
0.46 7.64
<0.001
HS
13. Shula (Pain)
15 2.07
± 0.80
0.53
± 0.52 74.19
± 1.53
0.92 6.49
<0.001
HS
14. Alasya/utsahahani (General debility)
21 2.43
± 0.87
0.38
± 0.59 84.31
± 2.05
0.80 11.6
<0.001
HS
15. Klaibya (Loss of libido)
21 2.14
± 0.73
0.66
± 0.80 75.56
± 1.62
0.80 9.22
<0.001
HS
16. Nidradhikya (Excess sleep)
13 1.62
± 1.12
0.23
± 0.44 85.71
± 1.38
1.19 4.18
<0.01
HS
17. Purishabadhdhata (Constipation)
9 1.78
± 0.83
0
± 0 100
± 1.78
0.83 6.4
<0.01
HS
Abbreviation: HS means Highly significant, S means Significant and NS means Non significant.

Varadi Kwatha in Management of Type-2 Diabetes Mellitus 43
having Shita virya (cooling potency) (Table 2).A reduction in Karapadatala suptata (numbnessin palms and feet) (p<0.001) appears to be dueto relieving of the Srotorodha resulting abetter supply of nutrition and oxygen to thenerves.
A reduction in Shrama shavasa (dyspnoea)(p<0.001) is credited to Tikta and Kashayarasa predominance and Kaphaghna property ofVaradi kwatha (Table 2) which helped to clearthe Pranavahasrotas (respiratory channel) thushelped in improvement in the respiratoryfunctions. A reduction in Shula (pain) (p<0.001)was also noted. Varadi kwatha cleared theSrotasas (channels) as mentioned above. Varadikwatha also facilitated increased utilization ofglucose (nutrition) to generate Bala (energy) andtissue repair thus curbs Shula (pain).
A relief in Alasya with Utsahahani (generalweakness) (p<0.001) was also observed. TheTikta and Kashaya Rasa with Laghu and RukshaGunas (Table 2) of the decoction has helped innormalization of vitiated Kapha.
Thus could channelize the Vayu (energyforce) and rectified the Alasya (lethargyi.e.abnornal lack of energy) resulting in a senceof well being.
generate Ruchi, Utsaha and energy. Also adecrease in symptoms like Kshudhadhikya(increase in appetite), Abhyavaranashakti (excessintake of food), Daurbalya (weakness) werenoted (p<0.001) (Table 4). Varadi kwatha ispresumed to enhance the power of Agni. It alsohelped in increased utilization of gulucose torelease energy. The decoction could have relievedthe accumulated Kapha (unctuous particles) dueto its Tikta rasa and Kashaya rasa (Table 2).Thus Varadi kwatha helped in increasing theAgni and Prana (bio-energy) and generated Bala(over all strength) in the body.
A decrease in Karapadataladaha (burningsensation in palm and foot) (p<0.001) could becredited to Triphala in Varadi kwatha. Triphalahas Pitta rechana property. Amalaki (Embelicaofficinalis) and Mustaka (Cyperus rotundus) are
Table 5. Effect of therapy on biochemical (objective parameters) in 23 patients.
Sr. No.
Biochemical tests (Objective parameters)
n BT
Mean ± SD AT
Mean ±SD %
Change Diff BT-AT Mean ± SD
t p
1. FBS 23 207.65
± 78.43
162.86
± 72.66 21.57
± 44.78
42.05 5.11
<0. 001
HS
2. PPBS 23 278.89
± 131.96
223.30
±106.04 19.92
± 55.57
80.32 3.32
<0. 01
HS
3. Fasting Urine sugar 13 2.38
± 1. 19
1.23
± 1.42 48.39
±1.15
2.08 2.00
<0.05
S
4. Serum triglyceride 23 184.30
± 102.37
156.35
± 57.33 15 .69
± 28.91
70.84 1 . 9 6
>0.05
S
5. Serum cholesterol 23 199
± 47.53
188.35
± 41.84 6 .61
± 14.13
27.18 2 . 4 9
<0.05
S
6. HDL cholesterol 23 37.52
± 11.17
36.78
± 10.03 1 .97
± 0.74
6.89 0 . 5 1
>0.05
NS
7. Serum creatinine 23 1.03
± 0.19
1.00
± 0.20 2 .95
± 0.03
0.13 1 . 1 3
>0.05
NS
8. LDL 23 124.64
± 39.68
116.23
± 34. 80 675
± 8.41
22.67 1 . 7 8
<0.05
S
9. VLDL 23 36.86
± 20.47
31.11
± 11.38 19 .18
± 7.07
13.92 2 . 4 4
<0.05
S
Abbreviation: HS means Highly significant, S means Significant and NS means Non significant.
Table 6. Overall effect of therapy in 23 patients.
Result Patients (n=23)
No of Patients % relief
Control of the disease 00 00
Marked improvement 00 00
Moderately improved 17 74
Mildly improved 06 26
No improvement 00 00
Total 23 100

Guddoye, Dwibedy and Singh44
The Triphala in Varadi kwatha relievedthe Purishabadhdhata (constipation) (Table 2).This is mainly due to Anulomaka property ofHaritaki (Terminalia chebula) (Table 2) whichfacilitated the bowel evacuation and relieve ofconstipation.
Limitations of the studyThe following limitations prohibit
generalizations of study to target populations.The study involved a cross section of 23participants only. The sample size may serve tolimit generalization of the findings.
Sample size may not be representative, assamples was only from the Kayachikitsa O.P.D.of S.S Hospital within ‘limited time frame ofauthor’s Ph.D. programme. Also the sampleconsisted of volunteering sample of convenience.All ethnicities may not have been represented.
ConclusionVaradi kwatha is an economic Ayurvedic
medicine. This herbal medicine has benefited theType-2 diabetic patients in just 8 weeks oftreatment. The medical community can lookforward for further scientific evaluation of thisherbal drug for improvement of subjective andobjective parameters in Madhumeha (Type-2Diabetes mellitus).
References1. Charaka Samhita. by Agnivesha edited by Jadavaji
Trikamji Aacharya. Nidanasthana (4:47),5th edition.Varanasi, Chaukhambha SanskritSansthan, 2001.
2. Charaka Samhita. by Agnivesha edited by VaidyaJadavaji Trikamji Aacharya. Nidanasthana (4:48), 5th edition.Varanasi, Chaukhambha Sanskrit Sansthan, 2001.
3. Charaka Samhita. Agnivesha edited by JadavajiTrikamji Aacharya. Nidanasthana (4:51), Varanasi,Chaukhambha Sanskrit Sansthan, 2001.
4. Health India. http://health.india.com/diseases-conditions/common-queries-about-cholesterol-lipid-profile-vldl-hdl-triglycerides (26.6.2013)
5. Dennis L. Kasper, Stephen Hauser, DanLongo, J. Larry Jameson, Anthony S. Fauci:Harrison’s Principles of Internal Medicine.16th edition. 2005.
6. Madhava Nidana. by Madhukosa, withcommentary of Sri Vijayarakshita andSrikanthadatta. Chapter (33:6), 31st edition.Varanasi, Chaukhambha Sanskrit Sansthan,2002.
7. Madhava Nidana. by Madhukosa , withcommentary of Sri Vijayarakshita andSrikanthadatta. Chapter (34:3), 31st editionVaranasi. Chaukhambha Sanskrit Sansthan,2002.
8. Sarangadhara Samhita. by Sarangadharacommentated by Adhamalla’s Dipika andKasirama’s Gudhartha Dipika. Madhyakhanda,Sloka-108, 4th edition. Varanasi. ChaukhambhaOrientalia, 2000.
9. Sushruta Samhita. by Sushruta commentated byKaviraja Ambikadatta Shastri (Part I and II)Nidanasthana (6:5), 4th edition. Varanasi,Chaukhambha Sanskrit Sansthan, 2001.
10. Sushruta Samhita. by Sushruta commentated byKaviraja Ambikadatta Shastri (Part I and II)Nidanasthana (6:6), 14th edition. Varanasi,Chaukhambha Sanskrit Sansthan, 2001
11. World Health Organization http://www.who. int/mediacentre/factsheets/fs312/en/ (25.6.2013)
12. National Center for Biotechnology Information,U.S. NLM http://www.ncbi.nlm.nih.gov/pubmed/12583337 (14.7.2013)
13. Dravyaguna Vijnana. Materia Medica, Vegetabledrugs. Gyanendra Pandey. Varanasi, ChaukhambhaKrishnadas Academy, 2004.
Address for correspondence: Dr. Gyaneshwarsing Guddoye, Ph.D. Scholar, Department of Siddhant Darshan,Institute of Medical Sciences, Faculty of Ayurveda, Banaras Hindu University, Varanasi - 221005 (India).E-mail: [email protected], [email protected] JREIM-2013-07-020 UID: 82-1372786878

J Res Educ Indian Med, Jan.-March, 2014; Vol. XX (1):45-49 ISSN 0970-7700
IMMEDIATE HYPOGLYCAEMIC EFFECT OF TWO SELECTIVEHYDROTHERAPEUTIC PROCEDURES IN NON INSULIN DEPENDENTPATIENTS OF DIABETES MELLITUSSUJATHA DINESH1 AND GANGADHARA VARMA B.R2
Division of Natural Therapeutics,1 S.D.M College of Naturopathy and Yogic Sciences,2Ujire - 574240 Karnataka (India)
Abstract: Background and Objectives: Non-Insulin Dependent Diabetes Mellitus (NIDDM)is a costly, complex and chronic disease that is expected to increase in prevalence in the comingdecades. Recent population based studies shows the prevalence of NIDDM in south India to be12.4% in Bengaluru in 2001,16.6% in Hyderabad in 2001,14.3% in Chennai in 2006 and 19.6%in Ernakulum in 2006. Complementary and Alternative Medicine (CAM) modalities are found tobe effective in the management of NIDDM. Hydrotherapy is a part of CAM, used in themanagement of NIDDM. Hence, the present study is planned to evaluate which of the hydrotherapeutic treatments has the best immediate hypoglycaemic effect between Gastrohepatic packand Neutral douche in NIDDM patients. Methods: The patients were selected from S.D.M. Yogaand Nature cure Hospital, Shanthivana, Dharmastala, Karnataka. They were randomly divided intotwo groups. According to the order in which they were recruited, they were allotted alternativelyinto two groups. Group-1: The Gastrohepatic pack group of 20 patients and Group-2: The Neutraldouche group of 20 patients. Patients were assessed on day 1 and day 2 during which they receivedGastrohepatic pack and Neutral douche respectively. Results: The results have shown statisticallysignificant changes in fasting blood glucose levels in Gastrohepatic pack subjects (p=0.02) and postprandial blood glucose levels in Neutral douche subjects (p=0.03) after the intervention period.Conclusion: The present study suggests that Neutral douche and Gastrohepatic pack can play amajor role in lowering the raised blood glucose levels in patients with NIDDM. Gastrohepatic packis relatively better for lowering the blood glucose levels as compared to Neutral douche.
Keywords: Complimentary and Alternative Medicine, Hydrotherapy, Naturopathy, NIDDM,Non-insulin dependent diabetes mellitus.
IntroductionNon-insulin dependent diabetes mellitus
(NIDDM) is a complex and chronic disease thatis expected to increase in prevalence in thecoming decades.1 The global prevalence ofdiabetes mellitus is projected to rise from 171million in 2000 to 366 million in 2030.2 A majorpart of diabetes burden (75%) will be borne bydeveloping countries3 and India has the secondlargest number (>61 million) of individuals withNIDDM in the world.4
Surveys on diabetic patients in Indiaestimate that, by the year 2000 India will behome to 32 million diabetics and the numbersmay increase to 40.9 million by 2006, 69.9 million
by 2025 and 80 million by 2030.5,6 Recentpopulation based studies shown the prevalenceof NIDDM in south India to be 12.4% inBengaluru in 2001,7 16.6% in Hyderabad in 2001,714.3% in Chennai in 20068 and 19.6% inErnakulum in 2006.9
Cardiovascular complications are theleading cause of morbidity and mortality amongpatients with NIDDM and cardiovascular disease(CVD) risk is 2 to 8 fold higher in the diabeticpopulation than in non-diabetic individuals of asimilar age, sex and ethnicity.10,11 Microalbuminuria and retinopathy are indicators ofmicro vascular dysfunction, and both predict apoorer outcome in patients with diabetes.12-14
1. Dean 2. P.G. Scholar

Sujatha Dinesh and Gangadhara Varma46
Naturopathic medicine is of greatestinterest as it is a whole-system of CAM mostclosely resembling conventional primary care inscope of practice, but with greater delivery ofhealthy lifestyle counselling.15 Naturopathy is asystem of man building in harmony with theconstructive principles of nature on physical,mental, moral and spiritual planes of living andconsists of non-invasive treatment modalities likediet therapy, fasting therapy, mud therapy,hydrotherapy, massage therapy, acupressure,acupuncture, chromo therapy, air therapy andmagnet therapy.16
Retrospective observational studies alsosuggest that Naturopathy care and treatment mayreduce risk for NIDDM and hypertension,including improved glucose control and reducedblood pressure respectively.18
Hydro therapy is one of the important partsof Naturopathy treatment, which has beenproven beneficial in cardiovascular,hemodynamic, cellular immunity, psychologicalparameters and neonatal growth.19-22
The first line of Naturopathic managementin treating NIDDM are Gastrohepatic pack,Neutral douche to whole body, cold hip bathand partial massage to abdomen. Gastrohepaticpack is a treatment modality in hydrotherapythat uses combination of hot and cold treatment.
The hot and cold treatment modality hasopposite effects on tissue metabolism, blood flow,inflammation, edema and connective tissueextensibility.23 The Neutral douche is a procedurewhere warm water is given to body with mildpressure, which increases peripheral circulation.
Hence, the present study was planned toevaluate the immediate hypoglycemic effect ofhydrotherapeutic treatments and to compareGastrohepatic pack and Neutral douche in patientsof NIDDM. Both Fasting blood glucose andPost prandial blood glucose levels were studied.
Materials and MethodsSubjects: The patients were selected and
registered for study from S.D.M Yoga and NatureCure Hospital, Shanthivana, Dharmastala,Karnataka (India).
They were randomly divided into twogroups.
1. The Gastrohepatic pack group of 20 patients and2. Neutral douche group of 20 patients.
The institutional ethical committee approvalwas obtained for conducting the study. Patientswere assessed on day 1 and day 2 during whichthey received 3 times Neutral douche and 3 timesGastrohepatic pack. Both groups also receivedtheir standard treatment regimen of drugs withyoga and dietary prescription.
Inclusion criteria1. Diagnosed subjects of type-2 diabetesmellitus, who have been on oralhypoglycaemic drugs for the past two years.2. Above the age of 35 years and below theage of 85 years.3. Both genders were included.
Exclusion criteria1. Patients of Diabetes mellitus on Insulin therapy.2. Diabetes associated with systemic complications.3. Females patients during menstruation period.
Study design: The study adopts a pre-post design. Patients were assessed on day 1and day 2 during which they received Neutraldouche or Gastrohepatic pack with the same diet,exercise and environment.
Consent: Signed voluntary informedconsent forms were obtained from all subjectsbefore their participation.
Trial profile (Flow chart)Assessments: The primary outcome
measure was Fasting blood glucose (FBG) and
Effect of GH pack and Neutral douche in Type-2 Diabetes Mellitus 47
Post prandial blood glucose (PPBG) before andafter the trial period.
InterventionGastrohepatic pack: The hot water bag
is kept on the abdominal region, covering theepigastric region, left and right hypogastric region,left and right lumbar region and umbilical region.The ice bag covers the region of lumbar vertebraeL2, L3, L4 and L5.
The treatment is administered in supinelying position, where the hot fomentation bag iskept over the abdominal region and then the icebag on lower back region. The pateients arethen covered with cotton cloth and wrapped with
woollen blanket. The duration of treatment is 20minutes.
Neutral douche: Water at a temperatureof 45 degree Celsius is made to flow in a pipewith mild pressure. The water is then sprayed onwhole body at controlled temperature and pressure.
Data analysisStatistical analysis was performed using
SPSS version 20.0 for windows. Data wereexpressed as mean ± SD. Data were tested fornormality. Paired sample ‘t’ test and independentsample ‘t’ tests were used to measure the withingroup difference and between groups differencesrespectively. Levels of significance were set to 0.05.
ResultsThe results have shown statistically
significant changes in fasting blood glucose levelsin Gastrohepatic pack subjects (p=0.02) and postprandial blood glucose levels in Neutral douchesubjects (p=0.03) after the intervention period.(Table 1). In other cases results are statisticallyinsignificant but have shown reduction in FBSand PPBS levels. Though Gastrohepatic packhas shown relatively better glycemic control ascompared to Neutral douche, there is nostatistically significant difference between (across)the groups for Fasting blood glucose (FBG) andPost prandial blood glucose (PPBG).
DiscussionThe results of present study suggest that
both the gastrohepatic pack and neutral douchehave shown significant (p<0.05) effect onglycemic control on Fasting blood glucose and
Figure 7
Trial Profile:
Randomly assessed patients for
eligibility (n = 42)
The subjects
who did not
meet the
inclusion
criteria (n = 2)
The number of subjects selected
for study (n = 40)
Assessments of FPG and PPPG
Neutral Douche
group (n = 20)
Gastrohepatic Pack
group (n = 20)
Drop outs (n = 0) Drop outs (n = 0)
1 Day 1 Day
Assessments of FPG and PPPG
Table 1. The data comparison within subjects and between subjects
Variable
Within subjects Between subjects
Baseline
Mean ± SD
Post interventional
Mean ± SD Mean diff ± SE diff.
Gastro hepatic Pack FBSN=20 129.5 ± 41.05 114.4 ± 27.5* 0.06 ± 7.1
Neutral Douche FBSN=20 129.9 ± 35.5 114.7 ± 24.9
Gastro hepatic Pack PPBSN=20 171.2 ± 52.4 157.45 ± 53.25 2.7 ± 14.1
Neutral Douche PPBSN=20 153.85 ± 41.2 137.4 ± 38.43*
*=P<0.05
.
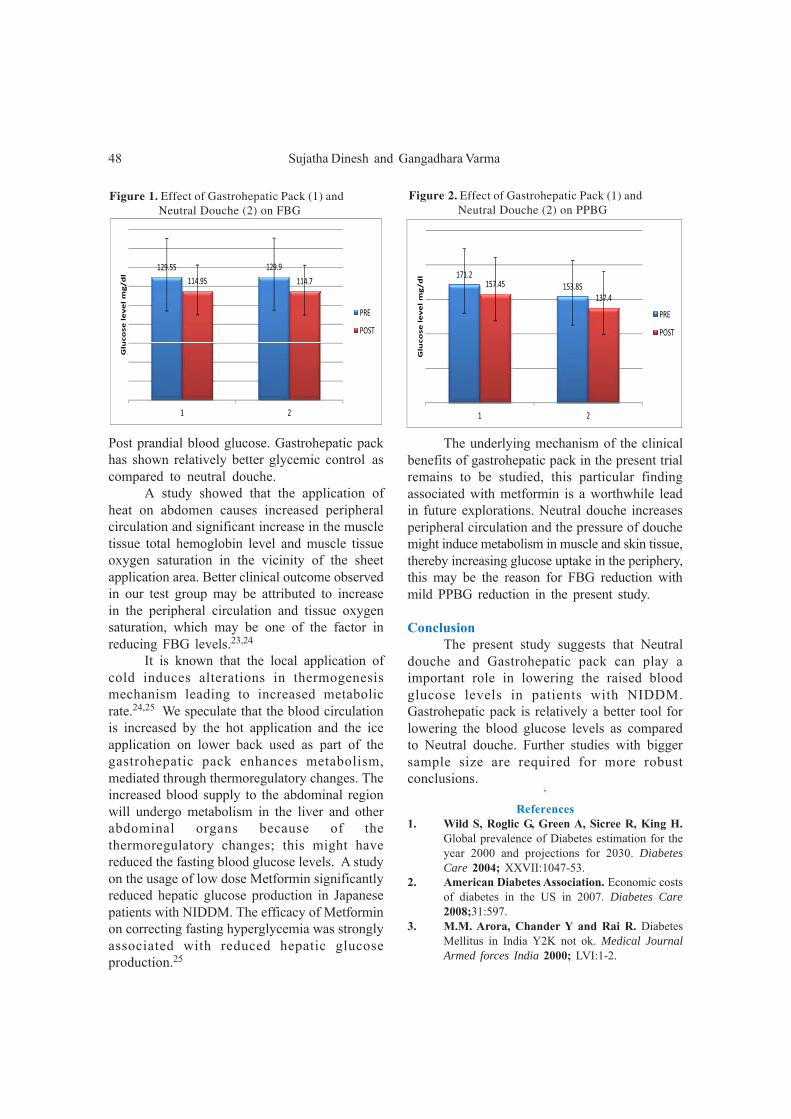
Sujatha Dinesh and Gangadhara Varma48
Post prandial blood glucose. Gastrohepatic packhas shown relatively better glycemic control ascompared to neutral douche.
A study showed that the application ofheat on abdomen causes increased peripheralcirculation and significant increase in the muscletissue total hemoglobin level and muscle tissueoxygen saturation in the vicinity of the sheetapplication area. Better clinical outcome observedin our test group may be attributed to increasein the peripheral circulation and tissue oxygensaturation, which may be one of the factor inreducing FBG levels.23,24
It is known that the local application ofcold induces alterations in thermogenesismechanism leading to increased metabolicrate.24,25 We speculate that the blood circulationis increased by the hot application and the iceapplication on lower back used as part of thegastrohepatic pack enhances metabolism,mediated through thermoregulatory changes. Theincreased blood supply to the abdominal regionwill undergo metabolism in the liver and otherabdominal organs because of thethermoregulatory changes; this might havereduced the fasting blood glucose levels. A studyon the usage of low dose Metformin significantlyreduced hepatic glucose production in Japanesepatients with NIDDM. The efficacy of Metforminon correcting fasting hyperglycemia was stronglyassociated with reduced hepatic glucoseproduction.25
The underlying mechanism of the clinicalbenefits of gastrohepatic pack in the present trialremains to be studied, this particular findingassociated with metformin is a worthwhile leadin future explorations. Neutral douche increasesperipheral circulation and the pressure of douchemight induce metabolism in muscle and skin tissue,thereby increasing glucose uptake in the periphery,this may be the reason for FBG reduction withmild PPBG reduction in the present study.
ConclusionThe present study suggests that Neutral
douche and Gastrohepatic pack can play aimportant role in lowering the raised bloodglucose levels in patients with NIDDM.Gastrohepatic pack is relatively a better tool forlowering the blood glucose levels as comparedto Neutral douche. Further studies with biggersample size are required for more robustconclusions.
`References
1. Wild S, Roglic G, Green A, Sicree R, King H.Global prevalence of Diabetes estimation for theyear 2000 and projections for 2030. DiabetesCare 2004; XXVII:1047-53.
2. American Diabetes Association. Economic costsof diabetes in the US in 2007. Diabetes Care2008;31:597.
3. M.M. Arora, Chander Y and Rai R. DiabetesMellitus in India Y2K not ok. Medical JournalArmed forces India 2000; LVI:1-2.
129.55 129.9
114.95 114.7
ucoselevelmg/dl
PRE
POST
1 2
Glu
171.2
153.85157.45
137.4
ucoselevelmg/dl
PRE
POST
1 2Glu
Figure 1. Effect of Gastrohepatic Pack (1) and Neutral Douche (2) on FBG
Figure 2. Effect of Gastrohepatic Pack (1) and Neutral Douche (2) on PPBG

Effect of GH pack and Neutral douche in Type-2 Diabetes Mellitus 49
4. International Diabetes Federation. DiabetesAtlas, 5th edition. Brussels, Belgium. InternationalDiabetes Federation. 2011.
5. Wild S, Roglic G, Green A, Sicree R, King H.Global prevalence of Diabetes estimation andprojections for 2030. Diabetes Care 2004.
6. Sicree R, Shaw J and Zimmet P. Diabetes andimpaired glucose tolerance. Diabetes Atlas.International Diabetes Federation, 3rd edition. Belgium,International Diabetes Federation. 2006;15-103.
7. Ramachandran A, Snehalatha C, Kapur A,Vijay V, Mohan V, A.K. Das, et al. Highprevalence of diabetes and impaired glucosetolerance in India: National Urban Diabetes Survey.Diabetologia 2001;XLIV:1094-101.
8. V.U. Menon, K.V. Kumar, Gilchrist A, T.N.Sugathan, K.R. Sundaram, Nair V, et al.Prevalence of known and undetected diabetes andassociated risk factors in central Kerala ADEPS.Diabetes Res Clin Pract 2006;LXXVII:289-94.
9. Mohan V, Deepa M, Deepa R, C.S. Shantirani,Farooq S, Ganesan A. Secular trends in theprevalence of diabetes and glucose tolerance inurban South India - the Chennai Urban RuralEpidemiology Study (CURES-17). Diabetologia2006;49:1175-8.
10. S.M. Haffner, Lehto S, Ronnemaa T, PyoralaK, Laakso M. Mortality from coronary heart diseasein patients with type-2 diabetes and in nondiabeticpatients with and without prior myocardialinfarction. N Engl J Med 1999;339:229-34.
11. Brun E, Nelson N, Bennett P, Imperatore G,Zoppini G, Verlato G. Diabetes duration andcause-specific mortality in the Verona DiabetesStudy. Diabetes Care 2000;23:1119–23.
12. American Diabetes Association. Economic costsof diabetes in the U.S. in 2007. Diabetes Care2008;31(3):596–615.
13. The Diabetes Control and Complications Trialresearch group. The effect of intensive treatmentof diabetes on the development and progression oflong-term complications in insulin-dependent diabetesmellitus. N Engl J Med 1993;329:977–86.
14. Rajala U, Pajunpaa H, Koskela P, Keinanen-Kiukaanniemi S. High cardiovascular disease mortalityin patients with visual impairment caused by diabeticretinopathy. Diabetes Care 2000;23:957- 61.
15. Klein R, B.E. Klein, S.E. Moss, K.J.Cruickshanks. Association of ocular diseaseand mortali ty in a diabetic population.Arch Ophthalmol 1999;117:1487-95.
16. Bradley R, Kozura E, Buckle H,Kaltunas J,Tais S, Standish L. Description of clinical riskfactor changes during naturopathic care for type 2diabetes. J Altern Complement Med 2009;15:633-38.
17. Digiesi V, Cerchiai G, Mannini L, Masi F,Nassi F. Hemorheologic& blood cell changes inhumans during partial immersion with a therapeuticmethod in 38oC water. Minerva Med 1986;77(30-31):1407-11.
18. Blazickova S, Rovensky J, Koska J, Vigas M.Effect of hyperthermic water bath on parameterson cellular immunity. Int J Clin Pharmacol Res2000;20(1-2):41-6.
19. W.N. Robiner. Psychological & physical reactionsto whirlpool baths. J Behav Med 1990;13(12):157-73
20. Zhao S, Xie L, Hu H, Xia J, Zhang W, Ye N,Chen B. A study of neonatal swimming (watertherapy) applied in clinical obstetrics. J MaternFetal Neonatal Med 2005;17(1):59-62.
21. Scott Nadler F, Kurt Weingand, Roger Kruse J.The Physiologic Basis and Clinical Applicationsof Cryotherapy and Thermotherapy for the PainPractitioner. Pain Physician 2004;(7):395-99.
22. Ryan Bradley, Karen J Sherman, Sheryl Catz,Carlo Calabrese, Erica B Oberg, Luesa Jordan,Lou Grothaus, Dan Cherkin. Adjunctive naturo-pathic care for type-2 diabetes: patient reported andclinical outcomes after one year. BMC Complementaryand Alternative Medicine 2012;12:44.
23. YoshinaoNagashima, MichihitoIgaki, Atsushi Suzuki,Shuichi Tsuchiya, Yoshimi Yamazaki, MichikoHishinuma, Sachiko Oh-ishi, MasatakaMajima.Application of a Heat- and Steam-Generating SheetIncreases Peripheral Blood Flow and InducesParasympathetic Predominance. Evidence-BasedComplementary and Alternative Medicine 2011;(13):1-13.
24. Arthur Guyton, John Hall. Text book of MedicalPhysiology. Elsevier Inc. 2006.
25. Mitsuyoshi Takahara, Hideaki Kaneto, NaotoKatakami, MunehideMatsuhisa, IichiroShimomura. Effect of metformin on hepatic glucoseproduction in Japanese patients with type-2 diabetesmellitus. Endocrine Journal 2012;59 (9):845-47.
Address for correspondence: Dr. Sujatha Dinesh, Dean, Division of Natural Therapeutics, S.D.M Collegeof Naturopathy and Yogic Sciences, Ujire-574240 Karnataka (India). E-mail: [email protected]
82-1373107667_RVZ-4

50

J Res Educ Indian Med, Jan.-March 2014; Vol. XX (1): 51-57 ISSN 0970-7700
A CRITICAL UNDERSTANDING OF NUTRACEUTICALASPECTS OF CURD IN AYURVEDAPRIYANKA B.V.1 AND MALLIKA KURAT JAYAVARMA2
Department of Samhita and Siddhanta,S.D.M. College of Ayurveda and Hospital, Hassan - 573201 Karnataka (India)
Abstract: Background: Curd is a popular milk product prepared indigenously in mosthousehold and is widely available commercially. It has high nutraceutical values and finds a veryprominent position in Indian culture, food habits and religious ethos. Curd by its nature has;Madhuraamlarasa (sweetish sour taste), Amlavipaka (sour post digestion taste), Guru (heavy todigest), Ushnavirya (hot in potency) and is Abhishyandi (coats over the channels carrying Dosha,Dhatu and Mala). Ayurveda proposes certain rules for its consumption and specify some adjuvantto contradict its ill effects. It is enumerated as etiology for Kleda (dampness) predominant diseases.On the other hand it is also useful as Pathya (diet) in diseases as well as, an ingredient in medicinalpreparations. Research throws light on yogurt, saying it is endowed with large variety of bacteriathat provide a number of health benefits such as lowering the low density lipid, hypertension andpreventing certain disorders. Aims: To critically understand the nutraceutical aspects of curd basedon available literature in Ayurveda and biomedical researches. Settings and Design: Conceptualcritical review. Methods and Materials: Literature search of authoritative texts of Ayurveda andprobable hypothesis is framed; conclusion is drawn based on current research. Results: Availableresearch on yogurt provides evidence of its health benefits based on its calcium content andprobiotic value. Some studies have established the medicinal properties of curd, but detrimentalconsequences which are repeatedly avowed in Ayurveda have not been taken up yet. Conclusion:Owing to the nutraceutical value of curd its use has been recommended as diet in chronic disease.
Keywords: Ayurveda, Curd, Nutraceutical value of curd.
1. Post Graduate Scholar, Department of Samhita and Siddhanta 2. Professor and Dean Academics
IntroductionThe science nutraceuticals deals with food
or constituents of food that provide medical orhealth benefits including the prevention andtreatment of disease.[1] Curd possessing numberof medicinal values, holds a primary position inIndian diet and culture, which is also evident inVedic literature, gives an idea that the techniquesof curd preparation and its health benefits werewell-known to people.
In present era, curd and yogurt areconsidered as the best source of probioticproducts. In this article an attempt is made toanalyze the nutraceutical value of different typesof curd based on its source, taste and its usageeither in external, internal medicine or purificatorytherapy with due respect to researches incontemporary sciences.
Curd by its nature is sweetish sour in taste,hot in potency, sour in post digestive taste andheavy to digest.[2] The attributes of curd variesaccording to type and nature of milk and itsinoculation time for fermentation. Attributes ofmilk like Snigdha (unctuousness) varies inaccordance with the habitat of animals and timeof milking, for instance, milk of low altitudeanimal or that which is collected during morningis heavy. These specifications are also applicableto curd as it is a byproduct of milk itself. Thoughboth possess similar properties curd is moreAbhishyandi and Guru (heavy), which is provedby gastric emptying time (liquid phase is shorterfor milk [35min] than curd [60min]).[3]
Curd prepared from boiled milk possessesqualities like relishing, promotes Dhatu, digestivepower, strength and also pacifies Vata and Pitta.

Priyanka B .V. and Mallika Kurat Jayavarma52
This is re-established by percentage of totalnitrogen and ammonia found less in curd preparedout of boiled milk than of unboiled milk[4]
(Table 2). Whereas the curd which is filtered(Parisrita) reduces Vata, increases Kapha, alsocreates interest in food and produces nourishingaction.[5]
Properties based on rate of fermentationVarious types of curd are cited such as
Mandaka (unfermented curd), Madhura (sweet),Madhura amla (sweetish sour), Amla (sour) andAtyamla (sourer). Sweet curd by its hot potency,sweet taste during post digestion and unctuousquality mitigates Vata. However it aggravatesKapha, Meda and Shukra by its unctuousnessand heaviness qualities.[6] Sour curd aggravatesPitta, and possesses Grahi (water absorbingaction) by its hot potency (Virya) and sour postdigestive effect (Vipaka).
A study carried out shows that the nitrogenpercentage, dialyzable nitrogen and ammoniarespectively increase to 0.144, 0.060 and 9.74%on 7th day of fermentation. When it wascompared with buffalo curd on 7th day it showedsignificantly high values of nitrogen. This provessourer curd is more detrimental to health incomparison with sweet or sour curd (1st day)(Table 1 and 2).[4]
Usefulness in multiple formsAction of curd again differs according to
its part used, as with cream (Sara), curd mitigatesVata, increases Kapha and Shukra, therebyproduces Vrushya action through increasedproduction and improved ejaculation of semen.However in general the entity which increasesShukra is heavy and possesses Brumhana action.Whereas curd without cream possessesproperties like astringent preceding taste(Anurasa), dry, light ; improves taste and digestivefire; performs Grahi (absorbs water) andVistambikarma (constipated).
The supernatant layer of curd (Mastu) alsoknown as Manda is sour, sweet and astringentin taste, clears the channel, produces nourishment,strength, creates interest in food, relishing innature and breaks the stool. It can be preparedwith properly formed curd, whose qualityresembles butter milk.[7]
Nutraceutical value based on sourceBased on the source of milk there are eight
types of curd viz. cow, buffalo, goat, camel,sheep, mare, human and she-elephant. Goat curdreduces all three humors and stimulates digestion;being light than cow’s curd possesses softer andsmaller casein molecules. Hence it helps toovercome the conditions like hemorrhoids,dyspnoea, tuberculosis and cough etc. Moreoverseveral studies proved that, it stimulates themucosal immune system and improves thedefense mechanism against intestinal andrespiratory infections in a mouse immunesuppression model.[8,9] Also some studiesestablished that it is beneficial in producing GABAand ACE-inhibitor to counteract high bloodpressure.[10]
Buffalo curd is Snigdhatama, it increasesKapha to a larger extent, and thereby reducesVata. Hence, it is also useful in insomnia whichis caused by aggravation of Vata. Supportive tothis, a study proved that it consists of casein andfat, double the quantity of cow curd (Table 2).
Camel’s curd is alkali in taste, hot inpotency and pungent post digestive taste, but
Table 1. Nitrogen percentage in curd on 1st and
7th day of fermentation
Product Total N
%
NPN % Protein
%
Dialisable
Nitrogen
%
Amonia
Nitrogen
mg%
Cow milk @ 0.56 0.048 0.512 0.017 0.24
Curd 1st day 0.57 0.073 0.497 0.027 9.79
Curd 7th day 0.55 0.144 0.406 0.060 x
Buffalo milk @ 0.65 0.038 0.612 0.021 0.16
Curd 1st day 0.65 0.052 0.598 0.22 12.20
Curd 7th day 0.66 0.081 0.579 0.034 9.74
Buffalo milk# 0.64 0.040 0.600 0.023 0.36
Curd 1st day 0.65 0.059 0.591 0.026 13.86
Curd 7th day 0.63 0.057 0.573 0.029 12.45
@- Unboiled #-Boiled, x- not observed

A Conceptual Review on Curd 53
Table 2. Quality of boiled and unboiled buffalo milk curd
on 1st and 7th Day of Fermentation
Product Sp.gr Total
solid
(Protein
& Fat)
Acidity Volatile
acid
(mk.OIN
NaoH *)
Alcohol
(%
by vol)
Buffalo milk @ 0.65 0.038 0.612 0.021 00.16
Curd 1st day 0.65 0.052 0.598 0.220 12.20
Curd 7th day 0.66 0.081 0.579 0.034 09.74
Buffalo milk # 0.64 0.040 0.600 0.023 00.36
Curd 1st day 0.65 0.059 0.591 0.026 13.86
Curd7th day 0.63 0.057 0.573 0.029 12.45
@- unboiled #-Boiled * for 100gm
reduces Vata thereby overcomes the diseases likepiles, skin disease, worm and ascitis. Now adays camel milk is used to treat diabetes (as itcontains insulin like molecules) and to strengthencellular immune response, antimicrobial activity.[11]
However regarding camel curd no research isevident to prove its beneficial effect.
Sheep curd is sweet in both taste and postdigestive effect, accordingly increases all Dosha,but is considered as wholesome for diseases likehematological disorders, inflammatory diseases,wound and gouty arthritis. On the other hand itis comprehensively established to contain excessof total solids and major nutrients than the milkof goat and cow.
There are no researches to prove thenutraceutical aspect of other curd, butauthoritative texts of Ayurveda provideinformation regarding their attributes as follows.
Mare’s curd is astringent in taste, hot inpotency, pungent in post digestive effect, inaddition possesses attributes like rough, light andAbhishyandhi, thereby it increases Vata. Humanmilk curd is sweet in taste and post digestiveeffect; heavy thereby reduces Vata, Pitta,considered best for eyes. Whereas elephant curdis astringent in taste and pungent in post digestiveeffect, hot in potency, light in quality there byreduces Kapha.
Among eight types, cow’s curd beingcommon diet and ingredient in medicaments, thisarticle contains explanations regardingnutraceutical value of the same. However yogurtis artificially prepared curd, thus which is usedas a substitute in diet and medicine.
In internal medicamentsIn Antarparimarjanachikitsa (internal
treatment), curd is useful as diet, adjuvant andas ingredient in various therapeutic formulations.It is useful in diseases of vitiated Vata, Amashaya(pathogenesis involving stomach), Rasavahasrotos(channels which carry Rasa) and in Jeerna orPakvaavasta (chronic) (Table 3). If it is usedjudiciously cures conditions like anorexia,intermittent fever, diarrhoea, emaciation,rhinitis,[12] vomiting,[13] dry cough,[14] irritablebowel syndrome[15] and haemorrhoids.[16] Furtherlogical interpretation of the curd usage in aboveillustrated diseases is explained as follows.
Taste enhancing (Rochishnu) and salivapromoting (Praseka due to Kaphavruddhi)property is appreciated with curd, which iscomprehensively attributed to its acidic taste,sodium and calcium ions.[17]
Curd is indicated in intermittent fever(Vishamajvara), caused by Vata, Kapha orVatakapha. Based on its nature of presentationdifferent febrile conditions like typhoid can alsobe included under Vishamajvara. An in vitrostudy claims that, certain probiotic strains presentin yogurt can inhibit the growth and adhesion ofa range of entero-pathogens like Salmonella.[18]
Curd by its hot potency does the digestionof Ama,[19] there by relieves the condition Pinasa(acute and chronic rhinitis). A similar approachis found in naturopathy and other systems ofmedicine attribute the beneficial effect ofdecreasing intensity of allergy to increasedimmunoglobulin. But impact of curd on longterm usage is not yet evaluated.
In diseases of gastrointestinal tract likediarrhoea, irritable bowel syndrome andhemorrhoids curd is widely indicated. A studyhas established its beneficial effect in preventingand treating the acute diarrhoea caused byrotaviruse in children, curd is also useful as adiet in lactose intolerance.[20]
Improper functioning of Medodhatvagniwhich is a part of pathogenesis inhypercholesterolemia (Apacitameda), curd canbe a choice, as it influences Dhatvagni.

Priyanka B .V. and Mallika Kurat Jayavarma54
A research study illustrates that, the healthybacteria present in yogurt (L. acidophilus)assimilates cholesterol by enzymatic de-conjugation, consequently decreases the lowdensity lipid.[21]
In individuals who are lean by nature(Sahaja) or emaciated due to chronic disease,curd improves metabolic process. It is proved tobe beneficial in protein energy malnutrition. Theabove mentioned explanations have been proposedand proved by Ayurveda and other science.
However in addition to this, advancedstudies prove yogurt (with Lactobacillusacidophilus) as effective in decreasing candidalcolonization on daily ingestion of eight ounce,[22]
thereby prevents bacterial vaginosis.[23]
Curd is found effective in relievinghypertension as it shows antioxidative effect byinhibiting angiotensin.[24]
In Rasayana and VajeekaranaCurd is attributed with rejuvenating
property, hence used in preparations as ingredientand adjuvant. However it is also considered asApathya (unwholesome) during administration ofLashuna (Allium sativum). As curd is knownfor action of enhancing taste and adds flavor tofood, also a good aphrodisiac, thus it is useful inpreparations of Vajeekarana.
In external medicamentsCurd is useful in Bahirparimarjana chikitsa
(external treatment) as adjuvant for Lepa (externalapplication),[25] Seka (pouring)[26] and Prakshalana(washing)[27] in diseases like gouty arthritis,Urusthamba etc.
The main reason for its usage may be asa base for preparations and also providescoolness.
Table 3. Therapeutic usage of curd
Disease Method of curd usage
Vatikapravahika (dysentery due to Vata) Curd along with sour pomegranate fruit and ghee (Bahusneha).
Sapravahikaatisara (dysentery with diarrhea) Curd, oil, ghee and milk in equal quantity.
Varchakshaya (decreased stool quantity) Black gram, barley and sour fruit juice processed with ghee, oil and curd.
Vatajachardhi (vomiting due to Vata) Coriander decoction is prepared with curd, then with equal part of water or milk.
Vatajahridroga (heart disease due to Vata) Oil prepared with Rasna, Jeevaka etc. with four parts of curd.
Katina pureeshayuktaarshas (hard stool in hemorrhoids)
Ghee and oil processed with asafoetida and mixed with upper layer of curd.
Urusthambha (stiffness of thigh) Liquid portion of curd is used as adjuvant for Gunja, Madana, Danti.
Pureeshajakrimi (worms) Liquid portion of curd with Trapu.
Raktapitta (bleeding disorder) Karanjabeeja and salt with liquid portion of curd.
Raktatisara (blood mixed diarrhea) Bastamamsa with curd or gruel prepared with curd or creamy curd with honey.
Rajayakshma (tuberculosis) Creamy curd along with pomegranate juice and large amount of ghee.
Udara (ascitis associated with constipation) Narayanachurna with liquid portion of curd.
Arshas (haemorrhoids) Curd with cream.
Vatajaasrugdhara (menorrhagia due to Vata) Curd with honey or sugar.
Vatapradhanakasa (dry cough ) Curd.
Shvasa (bronchial asthma ) Ghee prepared out of liquid portion of curd and Dashamoola.

A Conceptual Review on Curd 55
In PanchakarmaIn Panchakarma (five purificatory therapy)
various medicated curd preparations arementioned for conducting emesis and purgationlike Jeemutakalpa,[28] Iksvakukalpa,[29]
Aragwadakalpa,[30] Tilvakakalpa,[31]
Saptalashankhinikalpa,[32] Sudhakalpa [33] andDantidravantikalpa.[34] It is also used as aprocessing agent for Madana [35] (Randiadumetorum). It is one of the ingredients forenema preparation iin both Niruha (decoctionenema) like Prasrutayougika basti [36] andAnuvasana (oil enema).
Supernatant portion of curd possessesVidbeda and Vatanulomana property; hence it isuseful in most of purgative formulation. Similarlyuseful in the formulations of emesis as it increasesKapha by its Abhishyanda, Guru and Snigdhaproperties.
As an ingredient in various formulationsCurd is used in various preparations like
Cangerighrita, [37] Pancagavyaghrita,[38]
Dashamoolaghrita,[39] Mulakadyataila,[40]
Agurvaditaila, [41] Balataila [42] and Takrarista.[43]
In many of the oil/ghee preparations, thecombination of curd and milk used is an exceptionto Viruddha, as it aims at relieving the disease byacting against the Dosha.
Harmful effects of curdThough curd is found beneficial in many
ways, still it should not be consumed daily (Nityaasevanadravya),[44] as it alters the digestion andleads to different ailments like herpes, bleedingdisorder, skin disease, anemia, giddiness,jaundice,[45] edema and diabetes.[46] It is alsocontraindicated in diseases like gouty arthritis[47]
and disorders of oral cavity. Hence there arespecifications for addition of adjuvant to curdlike ghee, honey, sugar, Indian gooseberry, greengram soup as a diet and medicine, which supportsAghrutasharkaraihi (without adjuvant curd shouldnot be consumed). However their is no scientificresearch data to support the same.
ConclusionHistorical review reveals that curd has been
used as a diet. Its usage was popularized whenthere was need for preserving milk in differentforms for obtaining certain therapeutic valueswhich were originally absent in milk. Curd whichis sweet in taste and prepared out of boiled cow’smilk is considered best as compared to its othervarieties. It is useful as diet, medicine, adjuvantand processing agent in many disorders, ifadministered judiciously.
Key Message: Curd is a common dietarysupplement used habitually by people across theworld. It endows wide spectrum of applicationin preparing medicaments and treating aliments.
References1. Stephen Defelice. Foundation for Innovation in
Medicine, Cited on [18 Jan 2013]. Available from:h t t p : / / w w w . c l e m s o n . e d u / N N C /what_are_nutra.html
2. Sushruta Samhita. Sushruta, Dalhana Sanskritcommentary, Acharya YT, Sutra Sthana,Drava Dravyavidhi Adhyaya (45:81-3),Varanasi.Chaukhambha Surbharati Prakashana, 2007.
3. Mahe S, Marteau P, Huneau JF, Thuillier Fet al. Intestinal nitrogen and electrolyte movementsfollowing fermented milk ingestion in man. Br JNutr 1994;71(2):169-80.
4. Asha K V. The toxicity study on Dadhi (Curd),(3:71-3), Trivendrum, Govt. Ayurvedic College,Kerala University, Thiruvananthapuram, 1989.
5. Rajanigantu, Tripathi Indradeo Vishvanatha.Ksheeradi Varga, 1st edition. Varanasi, KrishnadasaAcademy, 1982: pg 513.
6. Sushruta Samhita. Sushruta, Dalhana Sanskritcommentary, Acharya YT, Sutra Sthana,Drava Dravyavidhi Adhyaya (45: 81-82),Varanasi.Chaukhambha Surbharati Prakashan, 2007.
7. Astanga Hrudayam. Vagbhata. Srvangasundaraof Arunadatta & Ayurveda Rasayana of HemadriSanskrit commentary, Paradakara HS, Sutra Sthana,Drava Dravyavijnaniya Adhyaya (5:29-32),Varanasi.Choukhambha Orientalia, reprint 2005.
8. Astanga Hrudayam. Vagbhata, Srvangasundaraof Arunadatta & Ayurveda Rasayana of HemadriSanskrit commentary, Paradakara HS, Sutra Sthana,Drava Dravyavijnaniya Adhyaya (Commentary

Priyanka B .V. and Mallika Kurat Jayavarma56
on 5:29-32),Varanasi, Choukhambha Orientalia,reprint 2005.
9. Salva S, Nunez M, Villena J, Ramon A, FontG, Alvarez S. Development of a fermented goats’milk containing Lactobacillus rhamnosus: in vivostudy of health benefits. Sci Food Agric 2011;91:2355-62.
10. Minervini F, Bilancia MT, Siragusa S,Gobbetti M, Caponio F. Fermented goats’ milkproduced with selected multiple starters is apotentially functional food. Food Microbiol2009;26:559-64.
11. Ahmed Ali Al-Alawi, Louis C. Laleye.Characterization of Camel Milk Protein Isolatesas Nutraceutical and Functional Ingredients,Collaborative Research Project SQU/UAEU CL/SQU-UAEU/01/08 SQU/UAEU 01-06-60/08,Available from http://www.squ.edu.om/ committee/report/ Characterization of Camel M ilk ProteinIsolates as Nutraceutical and%20 FunctionalIngredientsU
12. Sushruta Samhita. Sushruta, Dalhana Sanskritcommentary, Acharya YT, Sutra Sthana,Drava Dravyavidhi Adhyaya (45:65), Varanasi,Chaukhambha Surbharati Prakashana, 2007.
13. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,ChardiChikitsa Adhyaya (20:24),Varanasi,Chaukhambha Surbharati Prakashana,2007.
14. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana, KasaChikitsa Adhyaya (18:82), Varanasi, ChaukhambhaSurbharati Prakashana,2007.
15. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Grahani Chikitsa Adhyaya (15:114), Varanasi,Chaukhambha Surbharati Prakashan, 2007.
16. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana, ArshaChikitsa Adhyaya (14:47), Varanasi, ChaukhambhaSurbharati Prakashan, 2007.
17. Sushruta Samhita. Sushruta, Dalhana Sanskritcommentary, Acharya YT, Sutra Sthana,Drava Dravyavidhi Adhyaya (45:65),Varanasi,Chaukhambha Surbharati Prakashan, 2007.
18. Babaee N, Atefeh G, Samir Z et al. Effects ofmilk curd on saliva secretion in healthy volunteercompared to baseline, 2% pilocarpine andequivalent pH adjusted acetic acid solutions.IndianJournal of Dental Research 2013; cited on 18 Jan2013.
19. Morita H. Preliminary human study for possiblealteration of serum immunoglobulin E productionin perennial allergic rhinitis with fermented milkprepared with Lactobacillus gasseri, TMCO356.Microbiol Immunol 2006; 50(9):70-76.Cited on[18 Jan 2013]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16985291
20. Labayen I, Forga L, Gonzalez A, Lenoir-Wijnkoop I, Nutr R, Martinez JA. Relationshipbetween lactose digestion, gastrointestinal transittime and symptoms in lactose malabsorbers afterdairy consumption. Ailment Pharmacol Therapy.2001;15:543-49.
21. Ataie-Jafari A, Larijani B, AlaviMajd H, TahbazF. Cholesterol-lowering effect of probiotic yogurtin comparison with ordinary yogurt in mildly tomoderately hypercholesterolemic subjects. Citedon [18 Jan 2013].Available from http://www.ncbi.nlm.nih.gov/pubmed/19229114.
22. Hilton E, Isenberg HD, Alperstein P et al.Ingestion of yogurt containing Lactobacillusacidophilus as prophylaxis for candidal vaginitis.Ann Intern Med. 1992;116(5):353-7. Cited on [18Jan 2013]. Available from http://www.ncbi.nlm.nih.gov/pubmed/1736766
23. Robert S, Uwe-Thomas D, Lactobacillusacidophilus and Yogurt in the Prevention andTherapy of Bacterial Vaginosis on [18 Jan 2013].Available from http://www.sciencedirect.com/science/article/pii/S095869469800096X
24. Effect of Administration of Fermented MilkContaining Whey Protein Concentrate to Ratsand Healthy Men on Serum Lipids and BloodPressure. Cited on [18 Jan 2013]. Available fromhttp://www.sciencedirect.com/science/article/pii/S0300908498800229
25. Astanga Hrudayam. Vagbhata , Srvangasundaraof Arunadatta & Ayurveda Rasayana of HemadriSanskrit commentary, Paradakara HS,Uttara Sthana, Vranapratisheda Adhyaya (25:36),Varanasi, Choukhambha Orientalia, reprint 2005.
26. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Vatarakta Chikitsa Adhyaya (29:127), Varanasi,Chaukhambha Surbharati Prakashana, 2007.
27. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Madatyaya Chikitsa Adhyaya ( 24:114), Varanasi,Chaukhambha Surbharati Prakashana, 2007.
28. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana,Jeemutakalpa Adhyaya (2:6),Varanasi,Chaukhambha Surbharati Prakashan, 2007.

A Conceptual Review on Curd 57
29. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana, IkshvakuAdhyaya (3:8), pg.657, Varanasi, ChaukhambhaSurbharati Prakashan, 2007;
30. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana,Aragvadha Adhyaya (8:9-10), pg.666, Varanasi,Chaukhambha Surbharati Prakashan, 2007;
31. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana, TilvakaAdhyaya (9:6),pg.667, Varanasi, ChaukhambhaSurbharati Prakashan, 2007;
32. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana,Sudhakalpa Adhyaya (10:11-2),pg.668, Varanasi,Chaukhambha Surbharati Prakashan, 2007;
33. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana,Saptalashankini Adhyaya (11:9-10), pg.669, Varanasi,Chaukhambha Surbharati Prakashan, 2007;
34. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana,DantidravantiAdhyaya(12:36),pg.671,Varanasi,Chaukhambha Surbharati Prakashan, 2007;
35. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Kalpa Sthana,MadanakalpaAdhyaya(1:14),pg.654,Varanasi,Chaukhambha Surbharati Prakashan, 2007;
36. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Siddhi Sthana,Prasrutayogiyamsiddhi Adhyaya 8:41), pg.715,Varanasi, Chaukhambha Surbharati Prakashan, 2007;
37. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana, AtisaraChikitsa Adhyaya (19:42-3), pg.551, Varanasi,Chaukhambha Surbharati Prakashan, 2007;
38. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,
Address for correspondence: Dr. Mallika Kurat Jayavarma, Professor & Dean Academics, Department ofSamhita and Siddhanta, S.D.M. College of Ayurveda and Hospital, Hassan, Karnataka (India).E-mail: [email protected]
Apasmara Cikitsa Adhyaya (10:18-24), pg.475,Varanasi, Chaukhambha Surbharati Prakashan, 2007;
39. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Grahani Cikitsa Adhyaya (15:82-6),pg.518,Varanasi, Chaukhambha Surbharati Prakashan, 2007;
40. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Vatavyadhi Adhyaya (28:136),Varanasi,Chaukhambha Surbharati Prakashan, 2007.
41. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Jvarachikitsa Adhyaya (3:267),Varanasi,Chaukhambha Surbharati Prakashan, 2007.
42. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Vatavyadhi Adhyaya (28:149),Varanasi,Chaukhambha Surbharati Prakashan, 2007.
43. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Chikitsa Sthana,Grahani Chikitsa Adhyaya (15:112-6),Varanasi,Chaukhambha Surbharati Prakashan, 2007.
44. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Sutra Sthana, MatrashitiyaAdhyaya (5:10-1),Varanasi, Chaukhambha SurbharatiPrakashan, 2007.
45. Charaka Samhita. Agnivesha, Cakrapani Sanskritcommentary, Acharya YT, Sutra Sthana,Navegandharaniya Adhyaya (7:62), Varanasi,Chaukhambha Surbharati Prakashan, 2007.
46. Astanga Hrudayam, Vagbhata, Srvangasundaraof arunadatta & Ayurveda Rasayana of HemadriSanskrit commentary, Paradakara HS, Sutra Sthana,Dravadravya Vijnaneeya Adhyaya (5:30), Varanasi,Choukhambha Orientalia, reprint 2005.
47. Charaka Samhita. Agnivesha, Sanskritcommentary, Acharya YT, Cikitsa Sthana,VatashonitacikitsaAdhyaya (29:6), Varanasi,Chaukhambha Surbharati Prakashan, 2007.
JREIM UID 82-1375946427

58

J Res Educ Indian Med Jan.-March 2014;Vol. XX (1):59-65 ISSN 0970-7700
IMPACT OF SHODHANA ON PHYSICO-CHEMICAL ANDCHROMATOGRAPHICAL PROFILES OF GUNJA(Abrus precatorius Linn.) SEEDSSUDIPTA ROY,1 RABINARAYAN ACHARYA2 AND V. J. SHUKLA3
Department of Dravyaguna,1,2 and Pharmaceutical Laboratory,3Institute for Post Graduate Teaching and Research in Ayurveda,Gujarat Ayurved University, Jamnagar - 361008 Gujarat (India).
Abstract: Gunja (Abrus precatorius Linn.) has been described under the category of Upavisha(semi poisonous) in Ayurveda. Certain compound formulations, containing Gunja as an ingredientlike Gunjaditaila, Kanakakshiritaila, Siddharthakaghrita, Kakadanighrita, Agnigarbha Rasa,Karpuragunja Rasa, Garudagad Rasa and Gunjagarbha Rasa are well practiced in Ayurveda.Seeds of Gunja are frequently used and strictly recommended to be used after proper Shodhana(processing) in presence of specified liquid media like Godugdha, Goghrita, Kanji etc. GunjaShodhana in this study has been carried by following the standard methods explained in AyurvedicFormulary of India (AFI). The study reveals that purified samples in presence of Kanji (sourgruel) and water showed changes in physico-chemical parameters in comparison to raw drugs.In HPTLC analysis, different Rf values were detected before and after purification indicating changein the nature of the shodhita drugs.
Keywords: Abrus precatorius Linn, Gunja, Kanji, Poisonous plants, Shodhana.
1 M. Pharma Scholar 2. Associate Professor 3. Head, Pharmaceutical Laboratory
IntroductionThe use of poisons in therapeutics has been
recorded in ancient Ayurvedic classical texts.Acharya Charaka has elaborately mentionedvarious poisoning symptoms and theirmanagement (Charaka).[1]
Acharya Sushruta has classifiedcategorically various sources of poison anddescribed accordingly (Sushruta).[2] Even today,these poisonous plants, after purification are inpractice widely as a medicament in a number ofdiseases.
Description of Gunja, one of the Upavisha,can be traced in Samhita, Nighantu as well as inRasagranthas. In few Ayurvedic texts, it hasbeen said that, white seeds of Gunja are morepotent (Rasatarangini)[3] and recommended incases of gonorrhea, stiffness of shoulder joints,sciatica and paralysis.
It is also used as an emetic and abortificientagent (Anand R. Attal, Kishor V).[4]
Though Gunja is described under theUpavisha its seeds have been used successfullyin different Ayurvedic formulations after properSamskara known as Shodhana (Rasa-tarangini,[3] Gogte VM).[5] Effect of shodhitaGunja seed kernels with cow’s milk or kanjihas been reported in previous works (GautamDS et al.).[6]
Literature revealed that specific mediai s u s e d f o r S h o d h a n a o f s p e c i f i csubstances (Ilanchezhian R. et al.).[7] Certainstudies have also shown that the toxicsubstances present in the plant drugs arereduced (Swarnendu Mitra et al,)[8] PatelYogesh et al.)[9] and transferred into themedia during the Shodhana process, renderingthe drug non toxic (Sarkar PK).[10]
Though a specific Shodhana method ofGunja seed has been recommended by theAyurvedic Formulary of India (AFI),[11] butpublished data related with the impact of this

60
Shodhana process on different physico-chemicaland chromatographical parameter is lacking.Hence, a study has been planned to evaluate theimpact of Shodhana of Gunja through kanjiand water and develop physico-chemical andHPTLC profile.
Materials and Methods- Shodhana procedure: A.F.I[11]
- Principle: Swedana (boiling)- Ingredients: Ashuddha Gunja seeds (KR): 300g (100g for each batch)- Kanji: 16.5 litres (5.5 litres for each batch).
Collection of DrugGunja (Abrus precatorius Linn.) was
identified by medicinal plants taxonomist.Different flora and its mature seed werepersonally collected from surrounding area ofJamnagar, in their natural habitat, during themonth of November-January, 2012.
Selection of SeedDamaged (broken) and discolored (faded)
seeds were rejected from the study. Remainingseeds were dropped into a beaker containingwater. The seeds that floated on the surface ofwater were also rejected. Only the seeds thatsettled in water at the bottom of the beakerwere dried in air. The dried seeds wereconsidered as Raw Gunja Seeds (RGS) andsubjected to the process of Shodhana.
Preparation of MediaKanji was prepared in the departmental
laboratory, following standard procedure asdescribed in Ayurvedic Pharmacopoeia of India(API).[15]
Equipment for Shodhana (Purification)Stainless steel vessel (20cm x 30cm);
capacity of 7l, used as Dolayantra (vessel forthe purification procedure), Stainless steel rod(28cm), Stainless steel vessel (48cm x 30cm x7cm); capacity of 3l, Cotton threads 30cm inlength, Measuring cylinder (capacity of 1l),Muslin cloth (45cm x 45cm), Digital weighing
machine, Digital induction cooker, stainless steelspatula (length: 30cm) and measuring cylinder(10ml, 25ml).
Procedure100g of raw Gunja seeds (RGS) were kept
in a muslin cloth and made into a pottali,suspended in a steel vessel and kanji was filledup to complete immersion of pottali. Swedanaprocedure was followed as described in theclassics (Rasatarangini).[3] The procedure wascarried-out over an induction cooker, for threehours at 100οC. Total 5.5 litres of kanji wereutilized for one batch. After boiling for threehours, the seeds were taken out from pottali andwashed with lukewarm water. After washing withlukewarm water seed coat was removed carefullyand kept on a paper sheet, for shade drying.Same procedure was carried out for all the threebatches. After proper drying, the seeds werecollected and stored in air tight container andlabelled as ‘Kanji Shodhita Gunja Seeds’ (KSGS).
Same procedure of Swedana was followedin another group of seeds in presence of ROwater and that product (seeds) was labelled as‘Water Shodhita Gunja Seeds’ (WSGS).
Preparation of SampleAll the three samples (RGS, KSGS and
WSGS) were powdered separately withmechanical grinder and passed through 60#.
Physico-chemical ParametersAssessment of the parameters such as
foreign matter, moisture content, ash value, acidinsoluble ash, pH, water soluble extractive, alcoholsoluble extractive, foaming index and swelling indexwere carried out by following standard proceduresrecommended by Ayurvedic pharmacopoeia ofIndia (Ayurvedic Pharmacopoeia of India (API),[15] D.R.Lohar).[16]
HPTLC studyEquipments for HPTLC
A CAMAG (Switzerland) HPTLC systemequipped with a sample applicator Linomat Vsample applicator was used for application of
Roy, Acharya and Shukla

61
samples. CAMAG Scanner III, Reprostar andWincats 4.02 were used for scanning the plates.CAMAG twin through glass chamber was usedfor developing the plates.
ChemicalsPre-coated silica gel 60 F254 TLC
aluminium plates (10×10cm, 0.2mm thick), ARgrade toluene, ethyl acetate, glacial acetic acid,methanol were obtained from M/S Merck Ltd.Mumbai, India (Anonymous, PlannerChromatography).[12]
Samples for HPTLCThe extract of all three samples (RGS,
KSGS and WSGS) for HPTLC, were made insame process as mentioned below.
Methanolic extract - 2g of sample wasmacerated with 20ml methanol for 24 hrs. andfiltered. Filtrate was concentrated to 5ml andused for spotting. The samples were titled asTrack-1, Track-2 and Track-3.
Track-1 : Methanolic extract of RGS.Track-2 : Methanolic extract of KSGS.Track-3 : Methanolic extract of WSGS.
Mobile phase:Toluene: Ethyl acetate: Glacial acetic acid (6.5: 3.5: 0.2)Detection: Spray with Vanilline-H2SO4.
Chromatographic ConditionsDetection: Deuterium lamp,
Tungsten lamp.Data System: Win cats software. The developed plate was scanned to
obtain densitogram in visible range from600nm to 800nm with 100 nm interval.
The developed plate was scanned to obtaindensitogram in visible range from 600 nm to 800nm with 100 nm interval.
Results and DiscussionThe toxic principles present in the plant
drugs are also reported as their active
constituents (Swarnendu Mitra et al.)[8] PatelYogesh et al.)[9] Therefore, it is not desirableto expel them out completely from the drugs.The main aim of Shodhana process is to reducethe toxic constituents to some extent or bypotentiating their chemical transformation to non-toxic or relatively less toxic substances. Theremay be some new principles added duringshodhana process to the drugs, which areresponsible for enhancing their biological efficacy.Hence, maximum beneficial effect can be obtainedby administering the shodhita drugs within theirtherapeutic dosage limit.
In this study, Shodhana of Gunja seed wascarried out by standard method as mentioned inAyurvedic Pharmacopoeia of India.[15]
Each Shodhana procedure was repeated for threetimes to establish the validation of thepharmaceutical processing. Shodhana of Gunjawas performed by the process of Swedana (boiling)in Kanji, for three hours. Same process wasfollowed for Swedana in water (as a control).
Principles of Swedana methods are theextraction process where the solvent entersthrough the pores into the cells resulting in theswelling of the tissues and solution of the solubleconstituents takes place within the cells, thenthere is escape of dissolved material through thesolvent boundary layer by the process ofdiffusion - finally separation of the solution fromthe drug occurs. The rate of extraction dependsmainly on the temperature and concentrationgradient across the cell membrane. The rate ofextraction and solubility is increased by elevationof temperature. Rising temperature increase theconcentration gradient across the cell membranethereby increase mass transfer of activeprinciples from solid material to the solvent(Carter SJ, et.al.).[13]
During Shodhana of Gunja, change incolour of the liquid media was noticed (Table 1)and it might be due to the removal of colourcontaining materials from the endosperm of theseeds. Changes in organoleptic characters ofGunja seeds were also noticed and the percentageof final weight obtained and the percentage of
Physico-chemical and Chromatographical profiles of Abrus precatorius Linn.

62
Track-1 HPTLC for Methanolic extract of RGS.Track-2 HPTLC for Methanolic extract of KSGS.Track-3 HPTLC for Methanolic extract of WSGS.
Fig-1. Track 1 ( 366nm ) Fig-2. Track 2 ( 366nm )Fig-3. Track 3 ( 366nm ) Fig-4. Track 1 ( 254nm )Fig-5. Track 2 ( 254nm ) Fig-6. Track 3 ( 254nm )
Roy, Acharya and Shukla

63
and Ash colour in case of water shodhita Gunjaseed after processing (Table 1). In case ofphysico-chemical study, it was observed that,after purification, the colour of all samples waschanged (Table 3). The moisture content of Kanjishodhita Gunja seed was comparatively lowerthan the raw and water shodhita Gunja seed(Table 3). Ash value was decreased in case ofall samples after purification. Ash values in Kanjipurified seeds were comparatively less than thatof the water shodhita and raw Gunja
weight lost during each batch of Shodhanaprocesses are duly calculated and presentedaccordingly. Greater yield (91.66%) and minimumweight loss (8.34%) were found after Shodhanawith water, whereas, lesser yield (88.2%) andgreater weight loss (11.8%) were found afterShodhana with Kanji. It might be due to theextraction of more soluble mass from the seedsby Kanji (Table 2). The reddish cream colouredpowder of raw seeds turned into yellowish brownin colour in case of Kanji shodhita Gunja seed
Fig-07. Multiple tracks ( 254nm ) Fig-08. Multiple Tracks (366nm)Fig-09. U.V.Spectral comparison Rf 0.28 T-1,2,3 Fig-10. U.V.Spectral comparison Rf 0.32 T-1,2,3Fig-11. U.V.Spectral comparison Rf 0.92 T-1,2,3
Table 1. Organoleptic characters of raw & Kanji sodhita and water sodhita Gunja seeds powder
Sample Colour Odour Taste Appearence
1 RGS Reddish cream Typical Bitter Smooth and shiny
2 KSGS Yellowish brown Characteristic of Kanji Sour and bitter Dull
3 WSGS Ash colour Typical Bitter Dull
RGS= Raw gunja seed; KSGS= Kanji sodhita Gunja seed; WSGS= Water shodhita Gunja seed
Physico-chemical and Chromatographical profiles of Abrus precatorius Linn.

64
seed (Table 3). Water soluble extractive in Kanjishodhita Gunja seed was comparatively lowerthan raw Gunja seed but higher than the watershodhita Gunja seed. pH value of all sampleswas found in between 5 to 5.5 (Table 3).According to some experts the, acidic pHindicates Ushnavirya (Shiva Charan Dhyani).[14]
Lower pH value indicates more acidic in nature,which is more capable to inhibit microbes.
In HPTLC study, at short UV (254nm),Raw Gunja seed, Kanji shodhita Gunja seedand water shodhita Gunja seed showed 8, 7 and4 spots respectively.(Table-4) (Fig.-4,Fig.-5,Fig.-6 & Fig.-7). Among which same Rf value(0.01) was found in all the three samples,indicating the presence of one similar componentin all three samples.
At long UV (366nm), Kanji shodhita Gunjaseed showed maximum number of spots (10spots), indicating presence of more number ofcomponents in comparison to the other twosamples (RGS and WSGS). One same Rf value(0.01) was found in all three samples.(Table-5)(Fig.-1, Fig.-2, Fig.-3 & Fig.-8).
From the spectral comparison (Fig.-9, Fig.-10 & Fig.-11) same Rf values were found in allthree samples (0.28, 0.32 & 0.92).
After spraying with vanillin-H2SO4, RGS,KSGS and WSGS showed 2(0.71, 0.94), 4(0.15,0.60, 0.67, 0.94) and 3(0.60, 0.69, 0.94) spots,respectively
ConclusionThe present work highlights the impact of
Shodhana on Gunja seed with different liquidswith special focus on physico-chemical andchromatographical profiles. From the study, itcan be concluded that Kanji is a better Shodhanamedia than water.
The observed different Rf values in HPTLCstudy reveals that, different components arepresent in all different samples. Besides this, sameRf values also found in all three samples whichindicates the presence of similar components inall three samples.
Table 2. Effect of Shodhana on yield of final product
after shodhana with kanji and water.
Sample Initial
Quantity(G)
Final Weight
(Avg.)(G)
Percentage
of Weight
Loss(% )
KSGS 100 88.2 11.8%
WSGS 100 91.66 8.34%
KSGS= Kanji sodhita Gunja seed; WSGS= Water sodhita Gunja
Table 3. Physicochemical parameters of raw and
purified Gunja seeds
Test Parameters RGS KSGS WSGS
Description Outer
coat
Red with
Yellowish
brown
Ash
colour
Foreign matter Nil Nil Nil
Moisture content 9.5% 7.726% 9.49%
Ash value 4.944% 1.971% 4.096%
Acid insoluble ash 1.5% 0.19% 0.54%
pH (pH paper) 5.5 5.5 5.5
Water soluble
extractive value
10.35% 6.27% 6.087%
Alcohol soluble
extractive value
1.5% 0.89% 0.39%
Foaming index <100 <100 <100
Swelling index 3 ml 3ml 3.5ml RGS= Raw gunja seed; KSGS= Kanji sodhita Gunja seed;
WSGS= Water shodhita Gunja seed
Table 4. Rf value in Short UV 254 nm of all samples
Sample
No. of
Spots Rf Value
1 RGS 8 0.01, 0.04, 0.11,0.20, 0.24,0.27,
0.46, 0.90
2 KSGS 7 0.01, 0.03, 0.25, 0.40, 0.55, 0.70,
0.88
3 WSGS 4 0.01, 0.26, 0.88, 0.91
RGS= Raw gunja seed; KSGS= Kanji sodhita Gunja seed;
WSGS= Water shodhita Gunja seed
Table 5. Rf value in long UV 366nm of all three samples
Sample
No. of
Spots Rf Value
1 RGS 6 0.01, 0.05, 0.08, 0.25, 0.41, 0.91
2 KSGS 10 0.01, 0.03, 0.09, 0.25, 0.31,
0.40,0.55, 0.69, 0.88, 0.91
3 WSGS 5 0.01, 0.40, 0.47, 0.87, 0.93
RGS= Raw gunja seed; KSGS= Kanji sodhita Gunja seed;
WSGS= Water shodhita Gunja seed
Roy, Acharya and Shukla

65
Further, higher studies using sophisticatedtechnologies are needed to evaluate thecharacterization of different components indifferent samples and their utility in therapeutics.
AcknowledgementsThe authors are thankful to the Director,
Institute for Post Graduate Teaching & Researchin Ayurveda for providing facilities to carry outthe research work. They are also thankful tothe staff of pharmaceutical laboratory for helpand guidance.
References1. Charaka Samhita. Sutra Sthana 1/53. Ed.
Dwivedi L., 1st edition. Varanasi, ChowkhambhaSanskrit Series Office, 2007.
2. Susruta Samhita. Sutra Sthana 15/47. Ed.Dwivedi. L, 3rd edition. Varanasi, ChowkhambhaSanskrit Series Office, 2003.
3. Rasatarangini. by Pranacharja Shri SadanandaSharma, Pandit Kashinath Shastri, Delhi, MotilalBanarasidas, 2009; pg 727-733.
4. Anand R. Attal, Kishor V. Otari, Rajkumar V.Shete, Chandrashekhar. D. Upasani, TanajiD. Nandgude. Abrusprecatorius Linnaeus: APhytopharmacological Review. Journal ofPharmacy Research 2010; 3(11): 2585-87.
5. Gogte VM. Ayurvedic Pharmacology &Therapeutic Uses of Medicinal Plants. 1st edition.Mumbai, Bharatiya Vidya Bhavan, 2000.
6. Davnath Singh Gautam, R. Banerji, S. Mahrotra.Effect of shodhana on the toxicity of Abrusprecatorius. Ancient Science of Life 1998; 18:2.
7. Ilanchezhian R, Roshy Joseph C, RabinarayanAcharya. Importance of media in shodhana
(Purification/Processing), Ancient Science of Life2010; 30(2):27-30.
8. Swarnendu Mitra, V. J. Shukla, RabinarayanAcharya. Effect of Shodhana (processing) onKupeelu (Strychnos nux-vomica Linn.) with specialreference to strychnine and brucine content. AYU2011;(3) July Sept. www.ayujournal.org.
9. Patel Yogesh, Bhat Savitha D, AcharyaRabinarayan, B.K.Ashok and Shukla V.J. Roleof Shodhana on analytical parameters of Dhaturainnoxia Mill. and Dhatura metel Linn. seeds. IJRAP2010;1(2):249-54.
10. Sarkar PK. Evaluation of Shodhana Process andAntidotal Study on Vatsanabha. Gujarat AyurvedUniversity, Jamnagar, Ph.D. Thesis 2008.
11. The Ayurvedic Formulary of India. 1st edition.New Delhi, Government of India. Department ofAYUSH, 1978; pg172.
12. Anonymous. Planner Chromatography, ModernThin layer Chromatography, Switzerland. 1999;pg 2-16.
13. Carter SJ. Cooper and Gunn’s.TutorialPharmacy, 6th edition. Delhi, CBS Publishers &Distributers, 2000.
14. Shiva Charan Dhyani, Dravyaguna Sidhanta,1st edition. Varanasi, India, Krishnadas Academy,1986.
15. Ayurvedic Pharmacopoeia of India (API). Part-II, Vol-II, Appendices-2, First edition. New Delhi,Government of India, Ministry of Health andFamily Welfare, Department of AYUSH, 2008;pg159-61.
16. Lohar D.R. Protocol for Testing, Ayurvedic,Siddha, Unani medicines, government of India,Depertment of AYUSH, Ministry of Health& Fami ly Wel fa re , Pharmacopoe ia lLaboratory for Indian Medicines, Ghaziabad,30th March 2007.
Address for correspondence: Dr. R.N.Acharya, Professor, Department of Dravyaguna, Institute for Post GraduateTeaching and Research in Ayurveda, Gujarat Ayurved University, Jamnagar (India).E-mail: [email protected] UID JREIM-2012-06-029
Physico-chemical and Chromatographical profiles of Abrus precatorius Linn.

J. Res. Educ. Indian Med., 2014; Vol. XX (1):66
For more information and to submit a proposal visit:http://agingandsociety.com/manchester-2014
Enquiries: [email protected] address: http://agingandsociety.com/manchester-2014
Sponsored by: Aging &Society / Common Ground Publishing
Presenters also have the option to submitcompleted papers to one of fully peer-reviewedjournals in The International Journal of Agingand Society. If you are unable to attend theconference, you may still join the communityand submit your article for peer review andpossible publication, upload an onlinepresentation, and enjoy subscriber access tothe journal.
Proposals are reviewed on rolling deadlines.The final proposal submission deadline to qualifyfor regular registration is 7 October 2014 (titleand short abstract). Proposals submitted afterthis day will be accommodated in non-themedsessions at the conference or are eligible forcommunity membership registrations (noattendance at conference required withcommunity membership presentations).
On behalf of the Organizing Committeeand the International Advisory Board, we arepleased to announce the Call for Papers forthe Aging and Society: Fourth InterdisciplinaryConference and the Call for Submissions toThe International Journal of Aging and Society.
The 2014 Aging and Society Conferencewill be held at the Manchester ConferenceCentre in Manchester, UK from 7 - 8November. Proposals for paper presentations,poster sessions, workshops, roundtables orcolloquia are invited to the conference,addressing the aging and society through oneof the following themes:.
Economic and DemographicPerspectives on Aging
Theme 1: Public Policy and PublicPerspectives on AgingTheme 2: Medical Perspectives on Aging,Health, WellnessTheme 3: Social and Cultural Perspectiveson AgingTheme 4: Diversity and Aging (Special Focusfor 2014)
Final Proposal SubmissionDeadline to Qualify for
Regular Registration:7 October 2014
CONFERENCES AND FORTHCOMMING EVENTS Announcement
A
Manchester Conference Centre, Manchester, UK7 - 8 November 2014
AGING AND SOCIETYFOURTH
INTERDISCIPLINARY CONFERENCE

For further details - kindly visit http://www.jreim.com/instructions_authors.htm
Download Authors templates from www.jreim.com
(Visit http://www.jreim.com/instructions_authors.htm)
*(Authors to draft references as per modified JREIM style: visit http:// www.jreim.com/how-to-draft-references-for-JREIM)
via www.jreim.com (Submit Manuscript) or via direct ScopeMed link http://my.ejmanager.com/jreim/ (Author Login)Authors can also upload articles online
(Optional pre-submission Copyeditng Servce is avialable. For further details visit www.jreim.com/copyediting)
d
*
(One orignal and two pho-copies)