Embed Size (px)
Citation preview

James S. Gammie, MDJames S. Gammie, MD
Professor and Chief, Division of Cardiac Surgery
Chief Medical Officer, Harpoon Medical
The Houston Aortic Symposium
February 23-25, 2017

Disclosure Statement of Financial InterestDisclosure Statement of Financial Interest
Within the past 12 months, I or my spouse/partner have had afinancial interest/arrangement or affiliation with the organization(s)financial interest/arrangement or affiliation with the organization(s)listed below.
Affiliation/Financial Relationship Company
• Consulting Fees/Honoraria • Edwards Lifesciences• Correx
• Ownership/Founder • Harpoon Medical
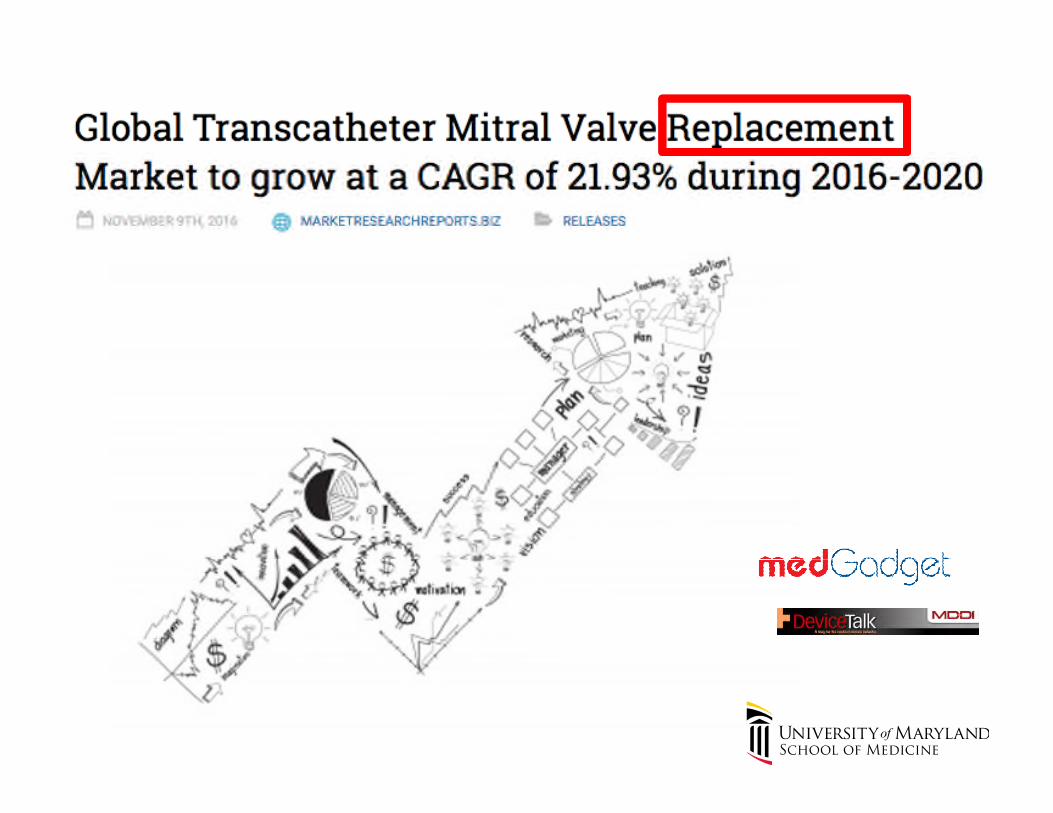
Surgery for Mitral Regurgitation:Who Are We Operating on Today?Who Are We Operating on Today?
DegenerativeDiseaseDisease
N = 13,154 Society of Thoracic Surgeons Adult CardiacN = 13,154 Society of Thoracic Surgeons Adult CardiacDatabase; 2011

FOR DEGENERATIVE MR:
REPAIR BEATS REPLACEMENT EVERY TIMEREPAIR BEATS REPLACEMENT EVERY TIME
REPAIR
Advantages of Repair Compared to Replacement
Lower operative mortality Lower operative mortality Improved left ventricular function Lower risk of stroke Lower risk of infection Lower risk of infection Freedom from anticoagulation and reoperation Superior long-term survival
Mitral Valve Repair or ReplacementMitral Valve Repair or Replacement
“A Patient with a Mitral Prosthesis…“A Patient with a Mitral Prosthesis…
Is a Patient for Life”Is a Patient for Life”
Robert W.M. Frater, MDRobert W.M. Frater, MD
Advantages of Mitral Valve RepairCompared to ReplacementCompared to Replacement
2000 – 2007
N = 58,370 Mitral Operations
Trends in Mitral Valve Surgery in the United States: Resultsfrom the Society of Thoracic Surgeons Adult Cardiac
Ann Thorac Surg 2009;87:1431-1439
from the Society of Thoracic Surgeons Adult CardiacDatabase
Ann Thorac Surg 2009;87:1431-1439

Procedure N # ofdeaths
ObservedMortality
Odds ratio (95% CI) (MVrepair vs MV
Riskstandardizeddeaths Mortality repair vs MV
replacement)standardizedmortality %
(95 % CI)**
MV 30811 414 1.34 Unadjusted Adjusted 1.65MV
Repair
30811 414 1.34 Unadjusted Adjusted 1.65
(1.49, 1.80)0.34
(.30, .39)
0.52(.45,.59)
MV 17007 651 3.83 (reference) (reference) 2.96
Replace (2.72, 3.20)
* Adjusted for 25 risk factors plus year of surgery; p < 0.0001 repair compared toreplacement
** Directly adjusted across 10 propensity groups; p < 0.001

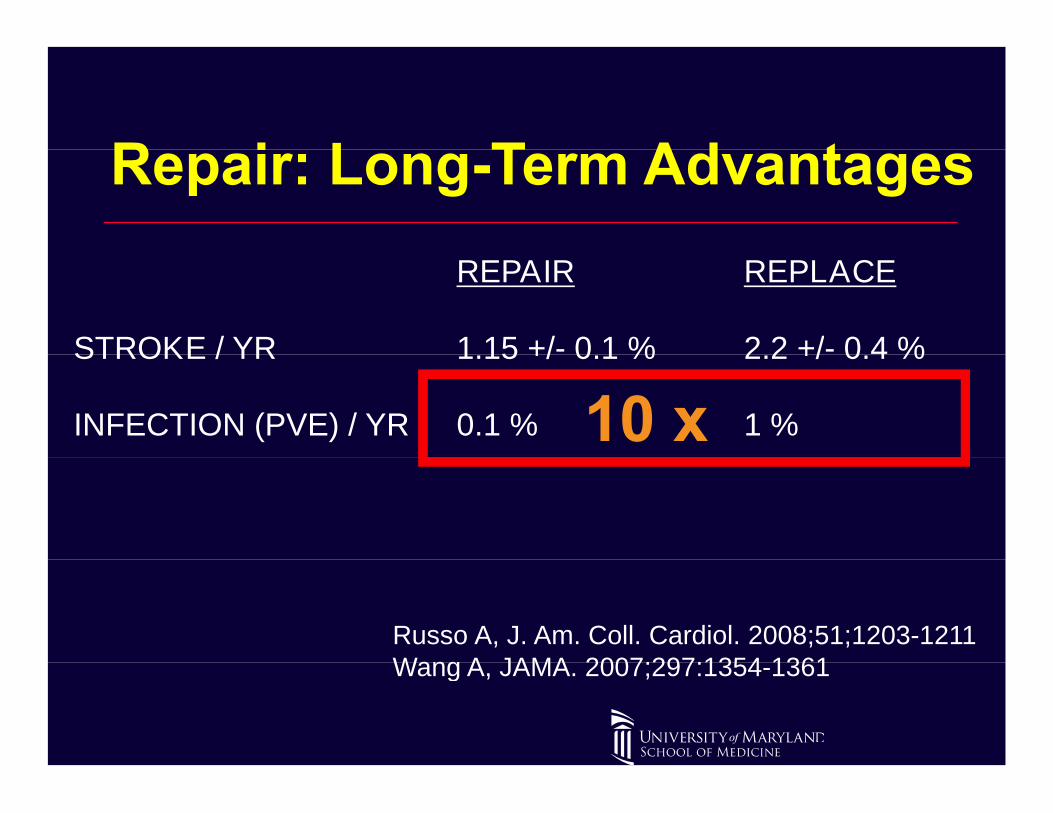
REPAIR REPLACE
STROKE / YR 1.15 +/- 0.1 % 2.2 +/- 0.4 %STROKE / YR 1.15 +/- 0.1 % 2.2 +/- 0.4 %
INFECTION (PVE) / YR 0.1 % 1 %
Russo A, J. Am. Coll. Cardiol. 2008;51;1203-1211Wang A, JAMA. 2007;297:1354-1361Wang A, JAMA. 2007;297:1354-1361

REPAIR REPLACE
STROKE / YR 1.15 +/- 0.1 % 2.2 +/- 0.4 %STROKE / YR 1.15 +/- 0.1 % 2.2 +/- 0.4 %
INFECTION (PVE) / YR 0.1 % 1 %
Russo A, J. Am. Coll. Cardiol. 2008;51;1203-1211Wang A, JAMA. 2007;297:1354-1361Wang A, JAMA. 2007;297:1354-1361
REPAIR REPLACE
STROKE / YR 1.15 +/- 0.1 % 2.2 +/- 0.4 %STROKE / YR 1.15 +/- 0.1 % 2.2 +/- 0.4 %
INFECTION (PVE) / YR 0.1 % 1 %
Russo A, J. Am. Coll. Cardiol. 2008;51;1203-1211Wang A, JAMA. 2007;297:1354-1361Wang A, JAMA. 2007;297:1354-1361

Advantages of Mitral Valve Repair

Mitral Valve Disease Segmentation
Primary (Degenerative) Functional
Percent of Total MR population*: 50 % 50%
Indications for Intervention: Well Established Not Clear (IIB) –Indications for Intervention: Well Established Not Clear (IIB) –COAPT?
Operative Therapy: Repair Replacement
Good Operative Therapy? YES NO
Is Therapy Applied Consistently? NO (replacement) NO
Patients with Severe MR USA*: 800,000 800,000
Annual Mitral Valve Surgery Rate: 5% 0.75 %Annual Mitral Valve Surgery Rate: 5% 0.75 %
*Canaccord Genuity 2016

Future of Catheter-Based Mitral Intervention
Near Future:
TMVR: BIG HURDLES: Access, Thrombosis,Paravalvular leak, LVOT obstruction, etc.BIG Investment – BIG EngineeringBIG Investment – BIG EngineeringWhen it works… IT IS STILL A MITRAL REPLACEMENT!
Repair for Degenerative Disease:Mitraclip: suboptimal (lessons from surgery)Goal:
Replicate ePTFE Non-Resectional MV Repair
*Canaccord Genuity 2016
Replicate ePTFE Non-Resectional MV Repair
Transapical, Beating-Heart*Canaccord Genuity 2016
Evolution of Repair for Degenerative Disease

Evolution of Repair for Degenerative DiseaseUniversity of Maryland ExperienceUniversity of Maryland Experience
100Leaflet resection Neochordal Insertion
80
40
60
20
40
0
20
2004 2005 2006 2007 2008 2009 2010 2011 2012
Year
2004 2005 2006 2007 2008 2009 2010 2011 2012

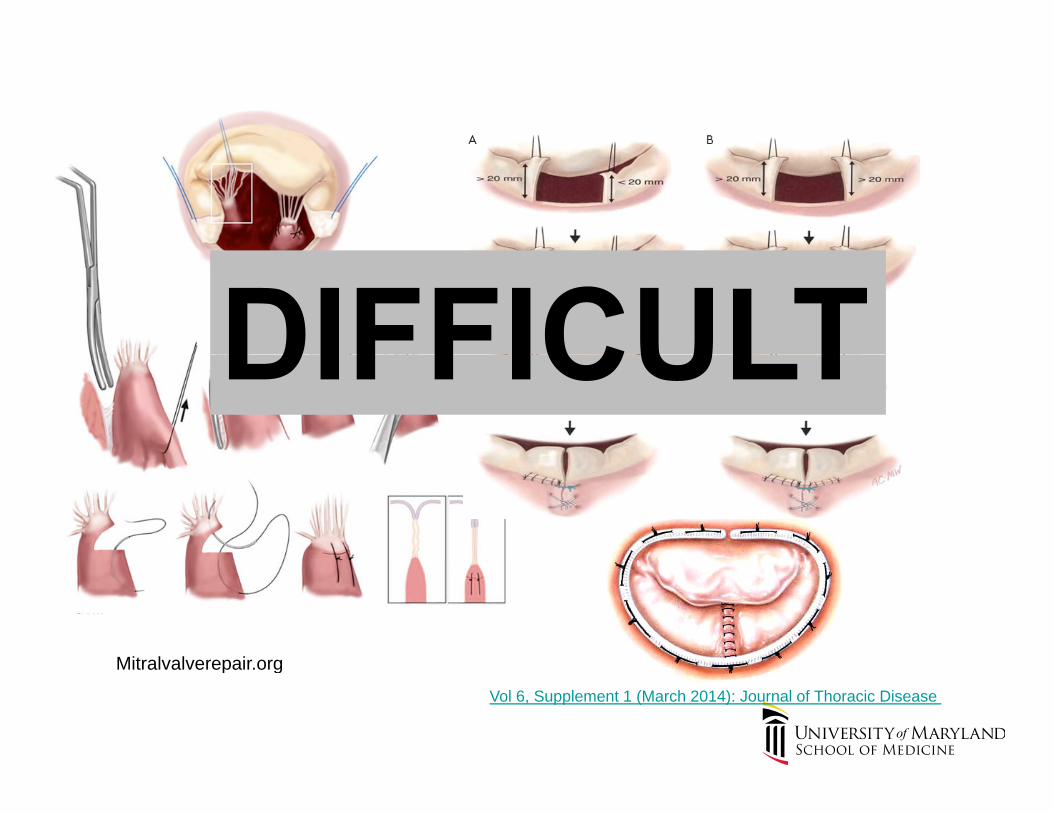
Mitralvalverepair.org
Vol 6, Supplement 1 (March 2014): Journal of Thoracic Disease
Mitralvalverepair.org
Mitralvalverepair.org
Vol 6, Supplement 1 (March 2014): Journal of Thoracic Disease
Mitralvalverepair.org

Courtesy A. M. Gillinov, MD
CONFIDENTIAL Slide 23 2/23/2017

http://www.visibleheart.com

Image-Guided Trans-Apical Mitral Valve Repair:A Better WayA Better Way
J.S. Gammie
COMPREHENSIVE HEART CENTER
J.S. Gammie

Harpoon: Fast Simple Procedure


Real-Time Titration of ePTFE Cordal Length
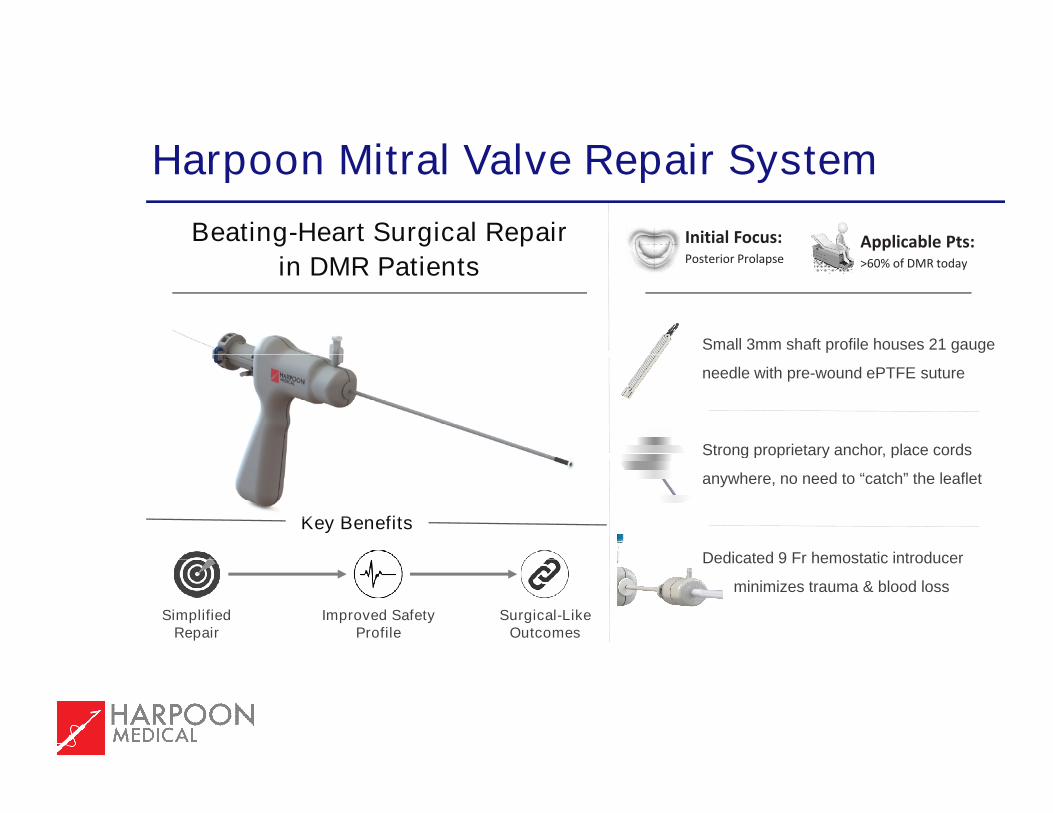
Harpoon Mitral Valve Repair System
Beating-Heart Surgical Repair
in DMR PatientsInitial Focus:Posterior Prolapse
Applicable Pts:
Harpoon Mitral Valve Repair System
in DMR Patients Posterior ProlapseApplicable Pts:>60% of DMR today
Small 3mm shaft profile houses 21 gauge
Strong proprietary anchor, place cords
needle with pre-wound ePTFE suture
Key Benefits
Strong proprietary anchor, place cords
anywhere, no need to “catch” the leaflet
Dedicated 9 Fr hemostatic introducer
Improved SafetyProfile
Surgical-LikeOutcomes
SimplifiedRepair
Dedicated 9 Fr hemostatic introducer
minimizes trauma & blood loss
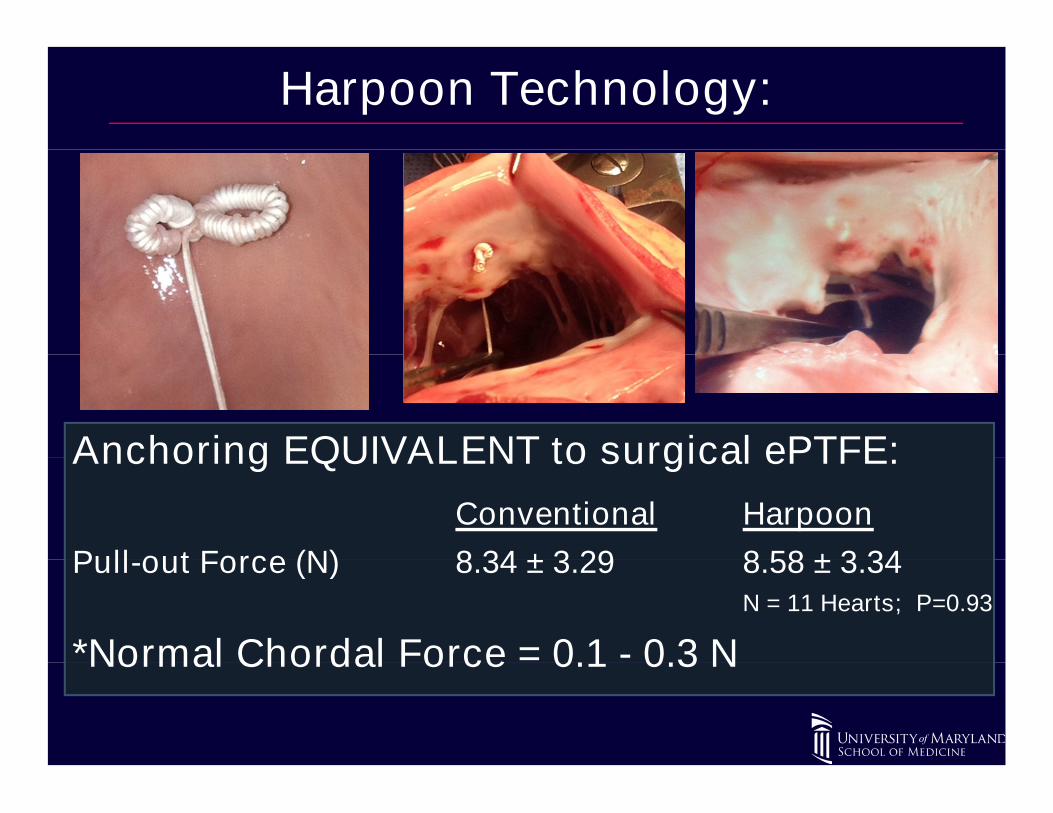
Harpoon Technology:
Anchoring EQUIVALENT to surgical ePTFE:Anchoring EQUIVALENT to surgical ePTFE:
Conventional Harpoon
Pull-out Force (N) 8.34 ± 3.29 8.58 ± 3.34Pull-out Force (N) 8.34 ± 3.29 8.58 ± 3.34N = 11 Hearts; P=0.93
*Normal Chordal Force = 0.1 - 0.3 N*Normal Chordal Force = 0.1 - 0.3 N
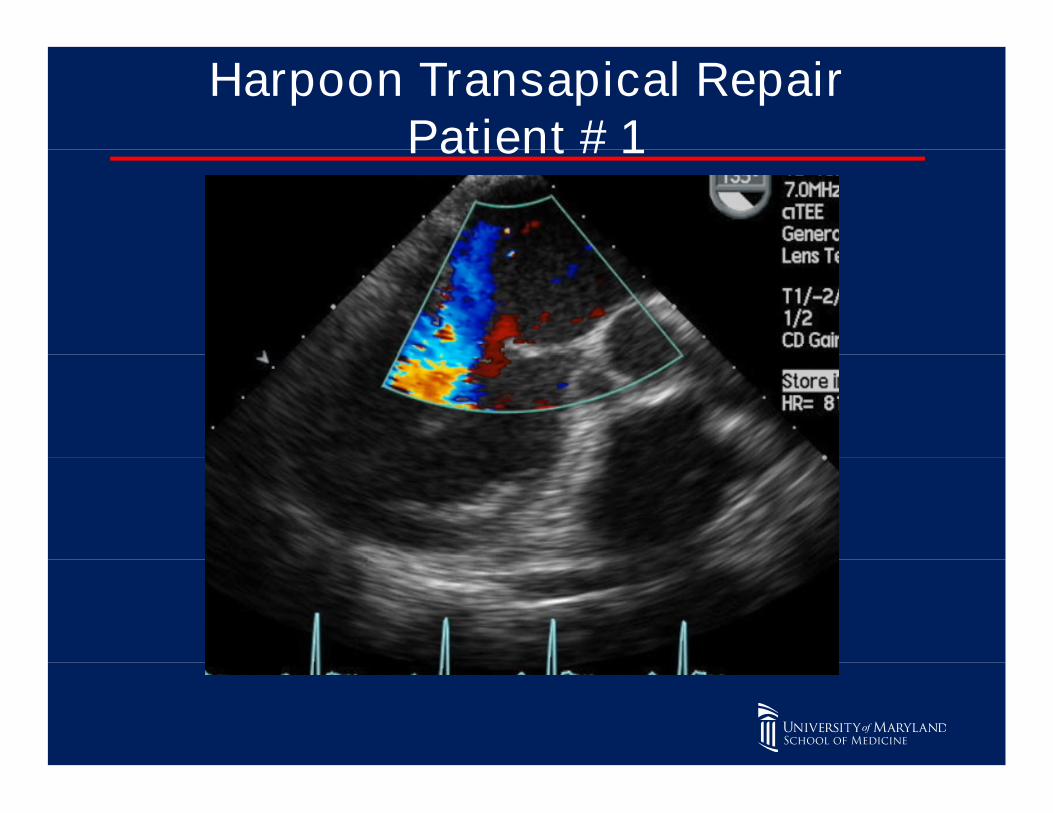
Harpoon Transapical RepairPatient # 1Patient # 1

Intraprocedural TEE (Knot deployment)

Intraprocedural TEE (ePTFE artificial cords tightened)
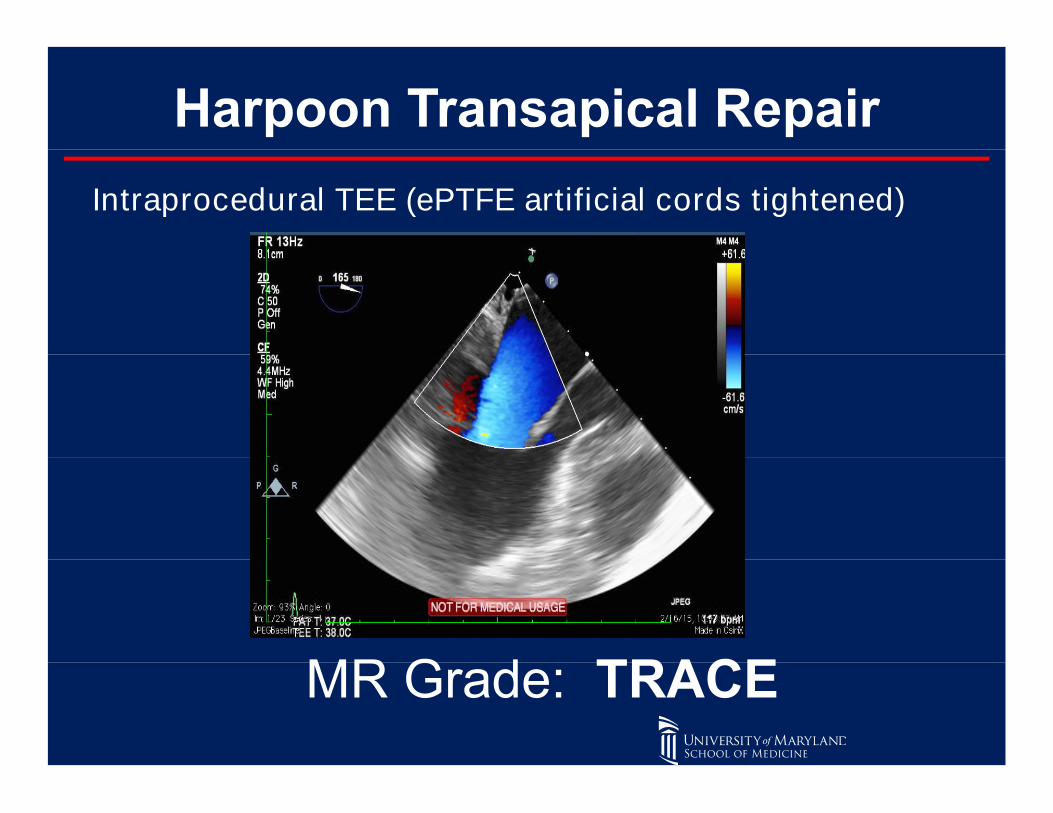
Intraprocedural TEE (ePTFE artificial cords tightened)

6 MONTH TTE
MR Grade: NONE/TRACE
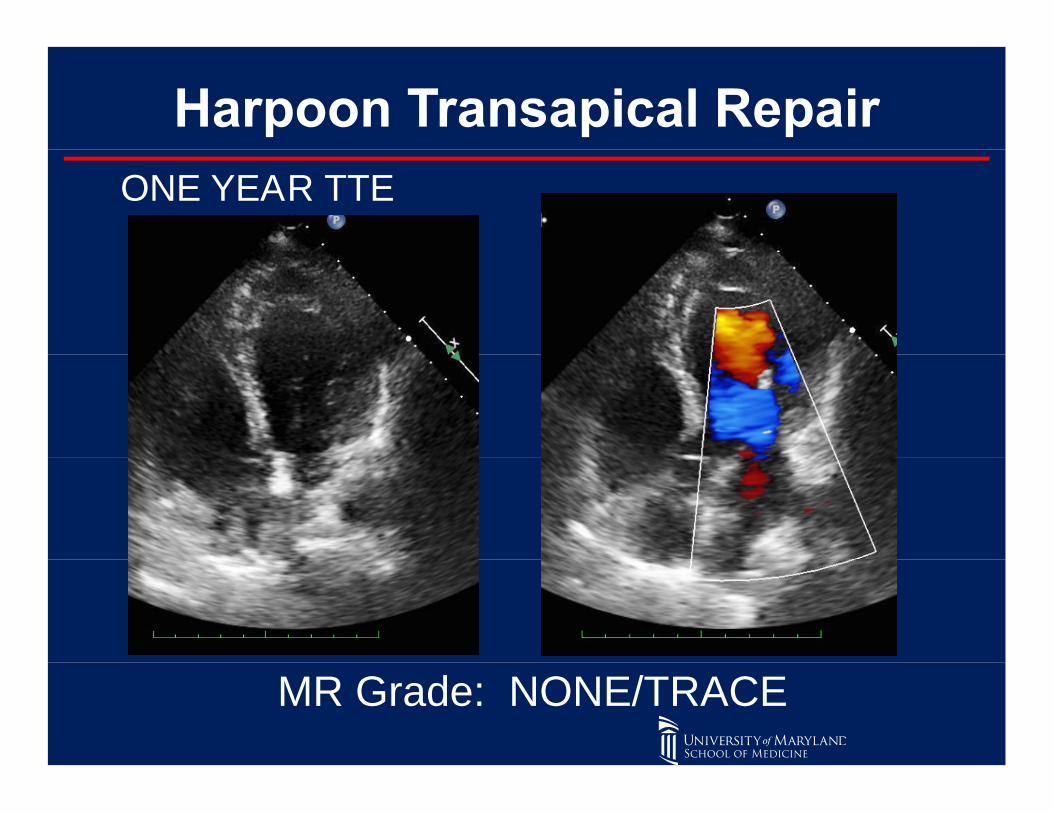
ONE YEAR TTE
MR Grade: NONE/TRACE
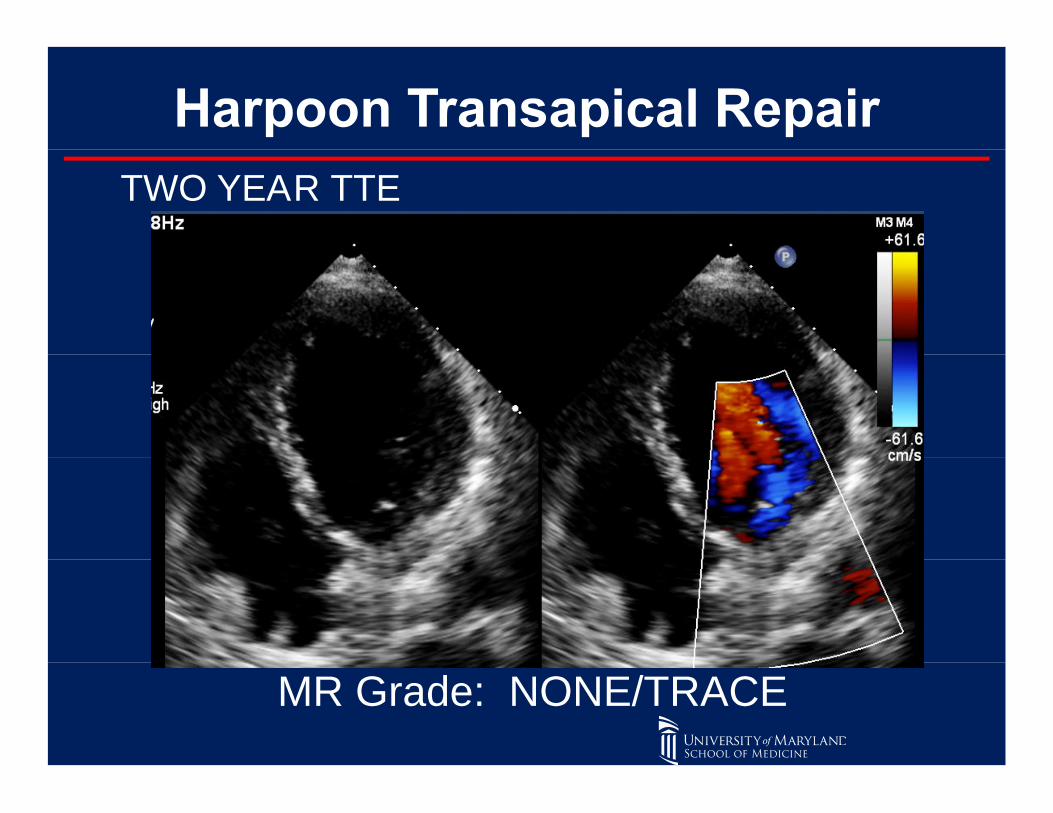
TWO YEAR TTE
MR Grade: NONE/TRACE
Clinical Results: Early Feasibility Study
Two Study Centers:• Jagellonian University John Paul II Hospital,
KrakowKrakow• Institute of Cardiology, Warsaw
Enrollment Complete:Enrollment Complete:• 13 patients enrolled with follow-up ongoing• February 2015 – February 2016• February 2015 – February 2016
Echocardiography Core Lab:• Massachusetts General Hospital (J. Hung, MD)• ASE Grading of MR• ASE Grading of MR
• None/Trace• Mild• Moderate• Moderate• Severe

Study Objective: Evaluate Safety and Performance of the HarpoonDevice
Primary Endpoints:• Harpoon Device Performs as Designed, Successfully Implant 1 or more
ePTFE CordsePTFE Cords• Demonstrate MR Reduction from Severe to </= Moderate MR• Measure of adverse events in accordance with MVARC
Inclusion Criteria:Inclusion Criteria:• Severe Degenerative Mitral Regurgitation• Isolated Posterior Leaflet Prolapse• Good Predicted Surface of Coaptation• Good Predicted Surface of Coaptation
Exclusion Criteria:• STS PROM Risk > 6• STS PROM Risk > 6• EF < 40 %
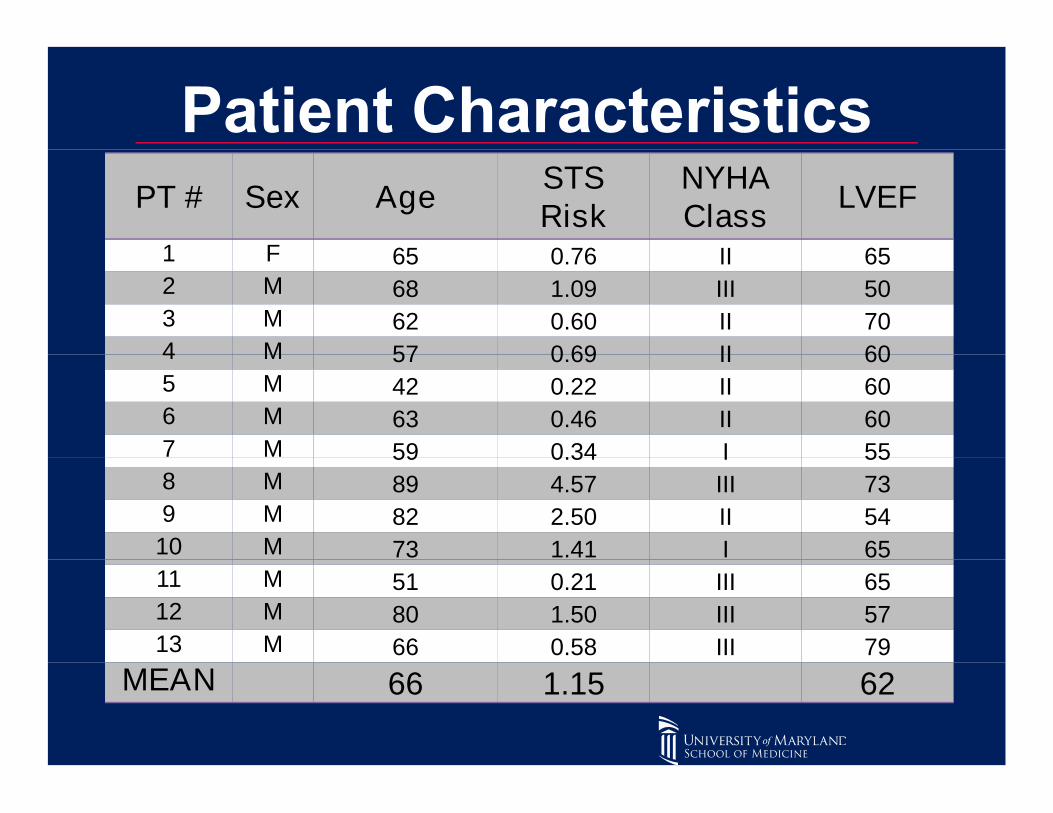
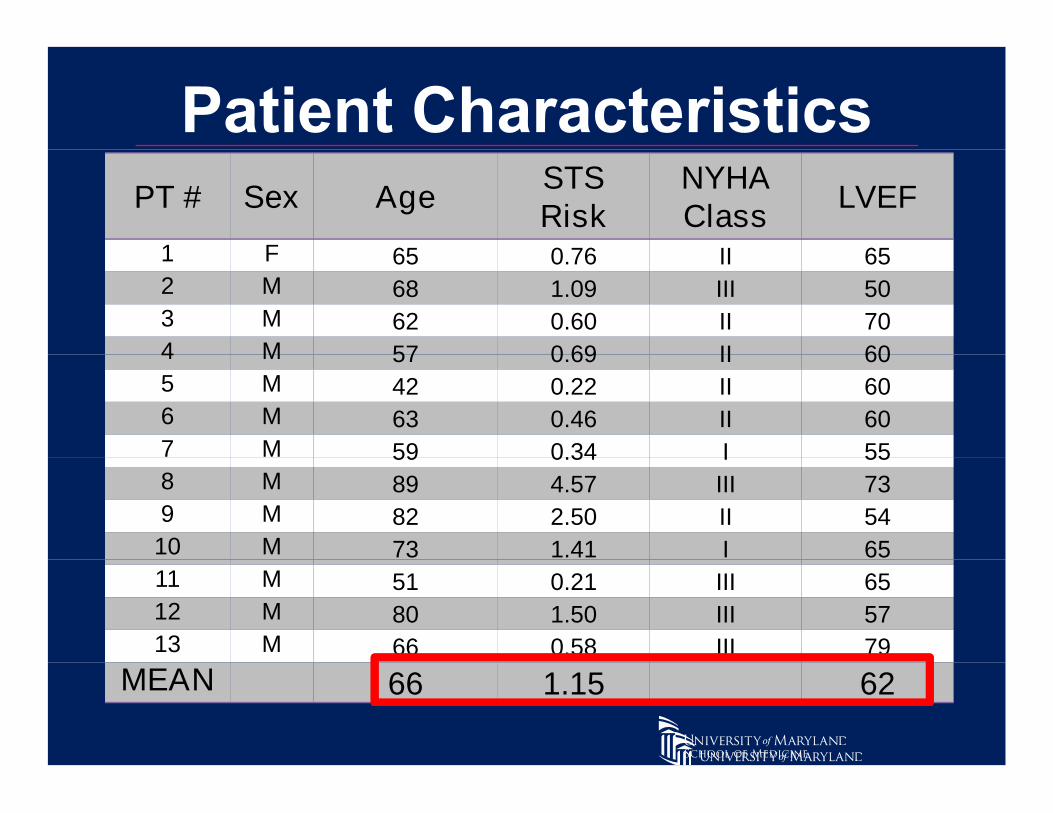
PT # Sex AgeSTSRisk
NYHAClass
LVEF
1 F 65 0.76 II 651 F 65 0.76 II 652 M 68 1.09 III 503 M 62 0.60 II 704 M 57 0.69 II 604 M 57 0.69 II 605 M 42 0.22 II 606 M 63 0.46 II 607 M 59 0.34 I 557 M 59 0.34 I 558 M 89 4.57 III 739 M 82 2.50 II 54
10 M 73 1.41 I 6573 1.41 I 6511 M 51 0.21 III 6512 M 80 1.50 III 5713 M 66 0.58 III 79
MEANMEAN 66 1.15 62
PT # Sex AgeSTSRisk
NYHAClass
LVEF
1 F 65 0.76 II 651 F 65 0.76 II 652 M 68 1.09 III 503 M 62 0.60 II 704 M 57 0.69 II 604 M 57 0.69 II 605 M 42 0.22 II 606 M 63 0.46 II 607 M 59 0.34 I 557 M 59 0.34 I 558 M 89 4.57 III 739 M 82 2.50 II 5410 M 73 1.41 I 6573 1.41 I 6511 M 51 0.21 III 6512 M 80 1.50 III 5713 M 66 0.58 III 79
MEANMEAN 66 1.15 62
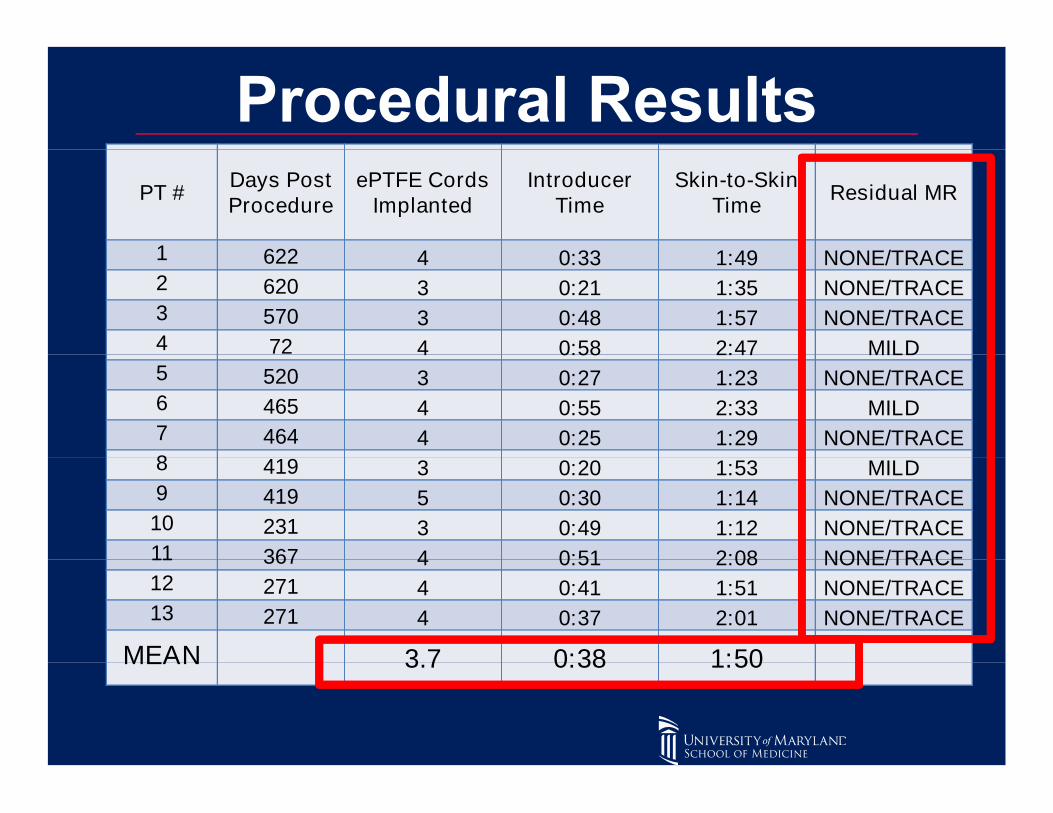
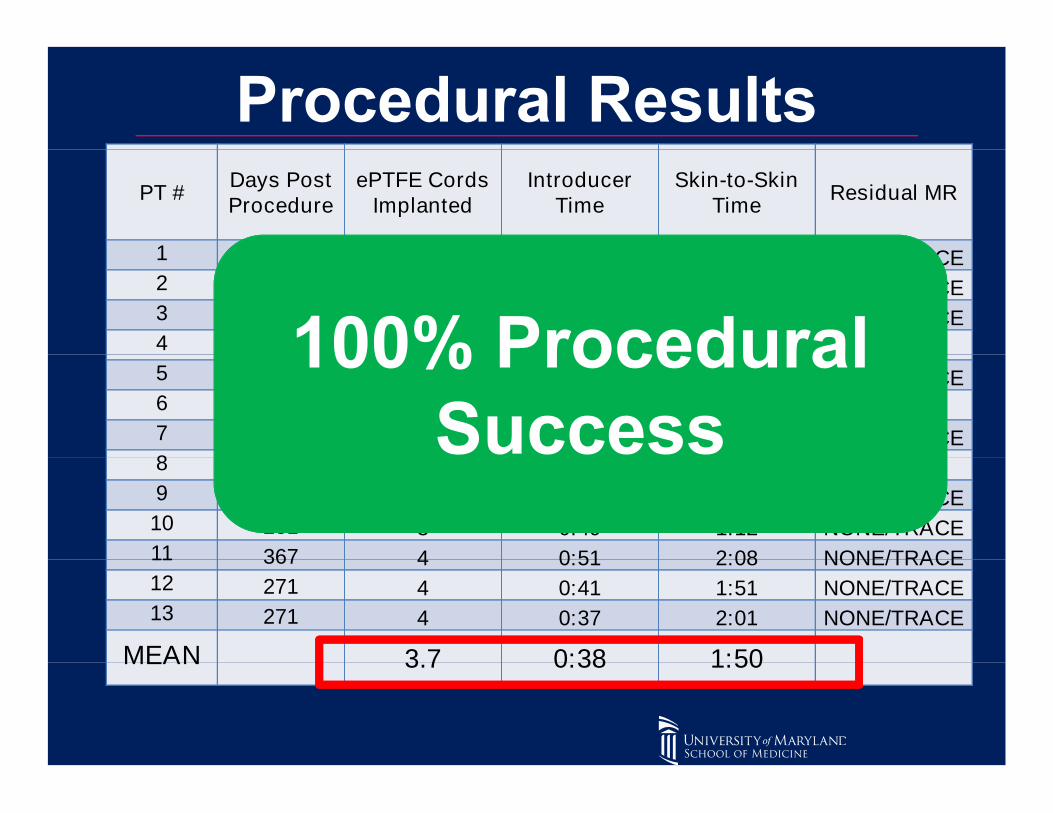
PT #Days PostProcedure
ePTFE CordsImplanted
IntroducerTime
Skin-to-SkinTime
Residual MR
1 622 4 0:33 1:49 NONE/TRACE1 622 4 0:33 1:49 NONE/TRACE2 620 3 0:21 1:35 NONE/TRACE3 570 3 0:48 1:57 NONE/TRACE4 72 4 0:58 2:47 MILD4 72 4 0:58 2:47 MILD5 520 3 0:27 1:23 NONE/TRACE6 465 4 0:55 2:33 MILD7 464 4 0:25 1:29 NONE/TRACE8 419 3 0:20 1:53 MILD8 419 3 0:20 1:53 MILD9 419 5 0:30 1:14 NONE/TRACE10 231 3 0:49 1:12 NONE/TRACE11 367 4 0:51 2:08 NONE/TRACE11 367 4 0:51 2:08 NONE/TRACE12 271 4 0:41 1:51 NONE/TRACE13 271 4 0:37 2:01 NONE/TRACE
MEAN 3.7 0:38 1:50MEAN 3.7 0:38 1:50
PT #Days PostProcedure
ePTFE CordsImplanted
IntroducerTime
Skin-to-SkinTime
Residual MR
1 622 4 0:33 1:49 NONE/TRACE1 622 4 0:33 1:49 NONE/TRACE2 620 3 0:21 1:35 NONE/TRACE3 570 3 0:48 1:57 NONE/TRACE4 72 4 0:58 2:47 MILD4 72 4 0:58 2:47 MILD5 520 3 0:27 1:23 NONE/TRACE6 465 4 0:55 2:33 MILD7 464 4 0:25 1:29 NONE/TRACE8 419 3 0:20 1:53 MILD8 419 3 0:20 1:53 MILD9 419 5 0:30 1:14 NONE/TRACE10 231 3 0:49 1:12 NONE/TRACE11 367 4 0:51 2:08 NONE/TRACE11 367 4 0:51 2:08 NONE/TRACE12 271 4 0:41 1:51 NONE/TRACE13 271 4 0:37 2:01 NONE/TRACE
MEAN 3.7 0:38 1:50MEAN 3.7 0:38 1:50

• No Mortality• No Mortality
• No Stroke
• No Renal Failure• No Renal Failure
• No Myocardial Infarction
• No Blood Transfusion• No Blood Transfusion
• No Conversion to Open Heart Surgery• No Conversion to Open Heart Surgery

• Two Reoperations for PericardialEffusions (POD 5, 13)
• Two Reoperations for Recurrent MR (POD72, 231)72, 231)
– 1st Patient ePTFE cord untied at apical pledget
– 2nd Patient native anterior chord ruptured– 2 Patient native anterior chord ruptured
– Both patients received successful re-operations, are alive and doing well
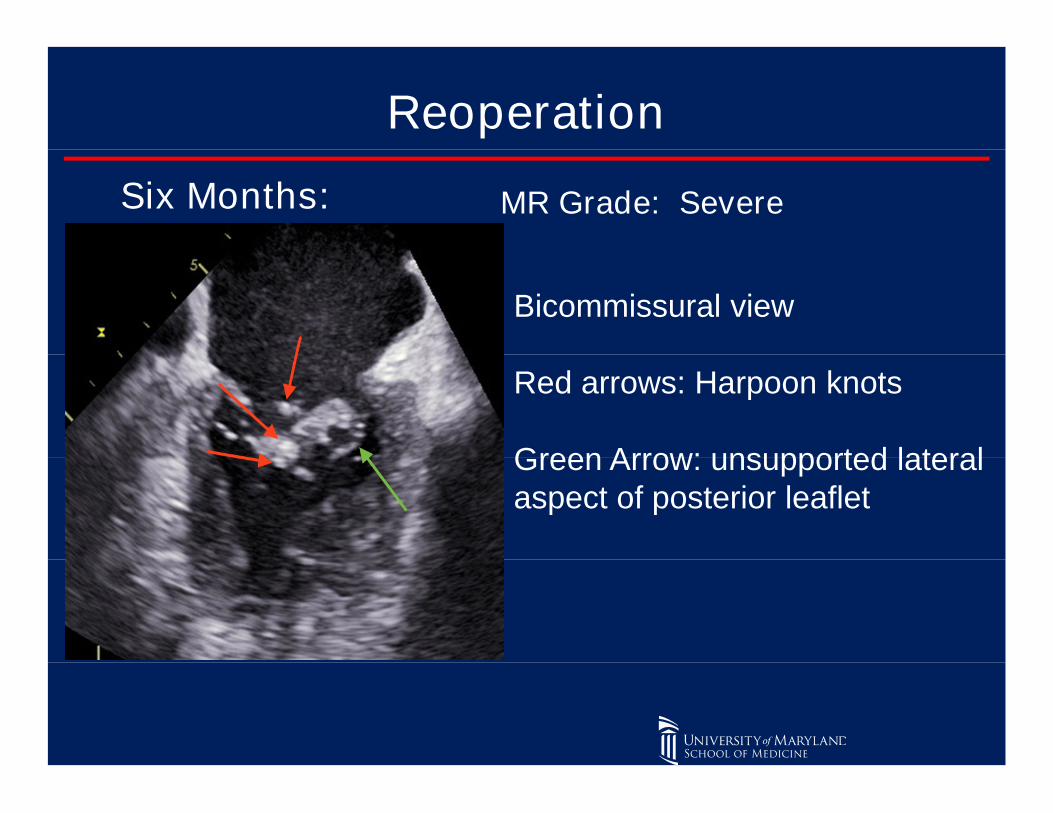
Reoperation
Six Months: MR Grade: Severe
Bicommissural view
Red arrows: Harpoon knots
Green Arrow: unsupported lateralGreen Arrow: unsupported lateralaspect of posterior leaflet
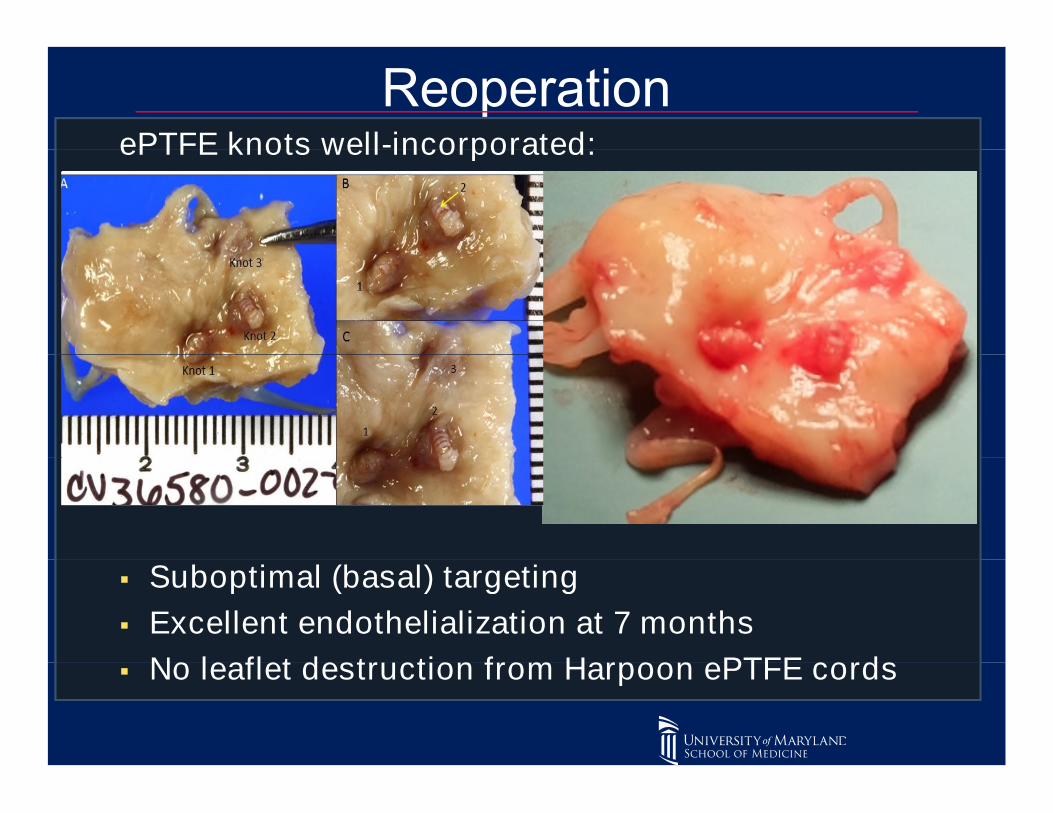
ePTFE knots well-incorporated:ePTFE knots well-incorporated:
Suboptimal (basal) targeting Suboptimal (basal) targeting
Excellent endothelialization at 7 months
No leaflet destruction from Harpoon ePTFE cords No leaflet destruction from Harpoon ePTFE cords

Transapical Artificial ePTFE Cordal Repair DoesNOT Preclude Subsequent Conventional RepairNOT Preclude Subsequent Conventional Repair
Mitraclip
Harpoon
Geidel S et al Submitted for Publication
Mitraclip
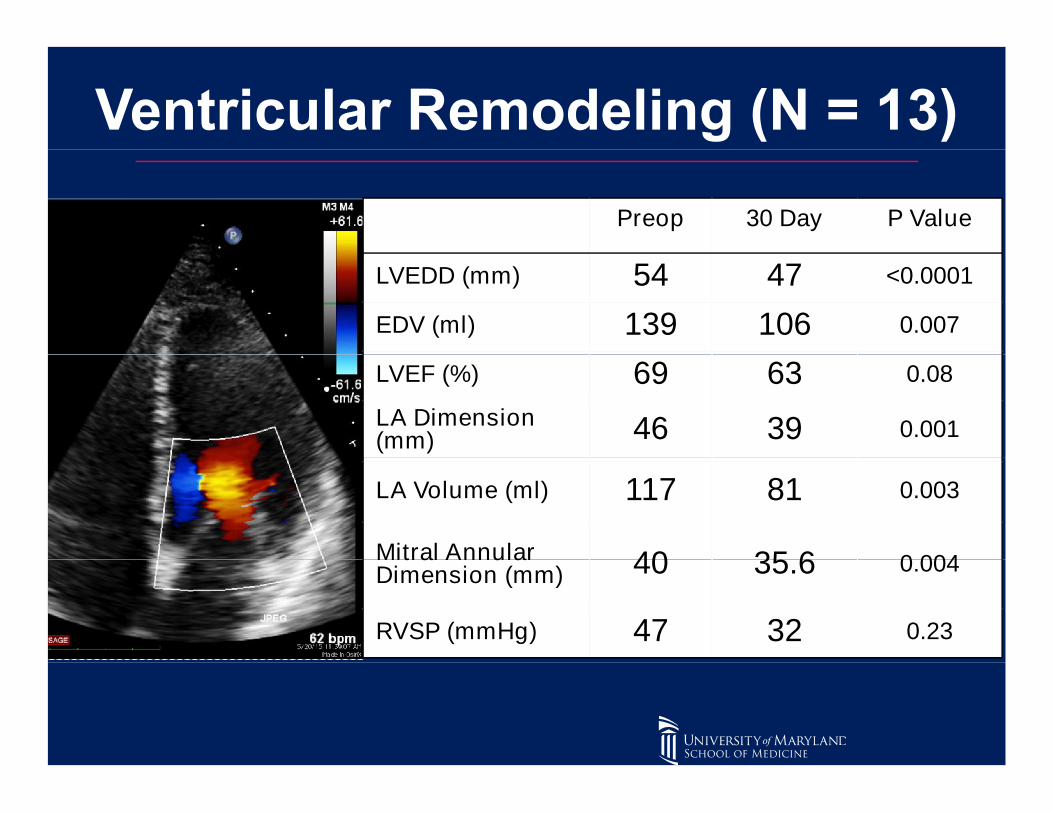
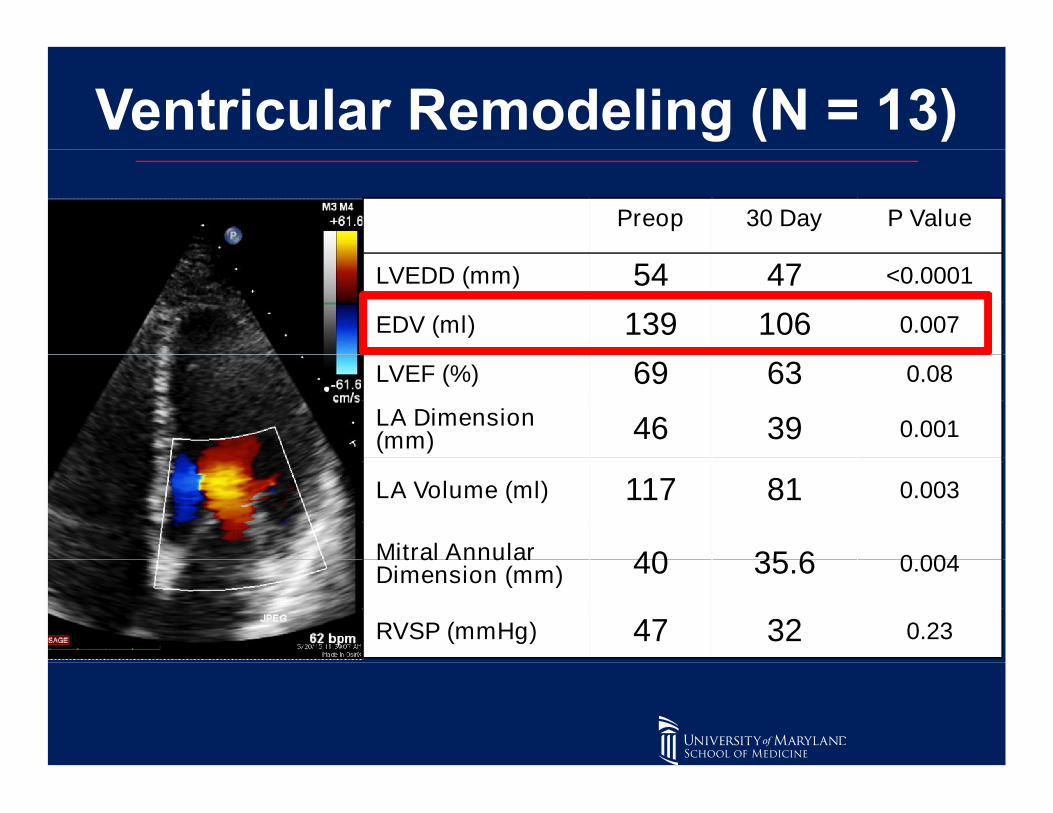
Preop 30 Day P Value
LVEDD (mm) 54 47 <0.0001
EDV (ml) 139 106 0.007
LVEF (%) 69 63 0.08
LA Dimension(mm) 46 39 0.001
LA Volume (ml) 117 81 0.003
Mitral Annular 40 35.6 0.004Mitral AnnularDimension (mm) 40 35.6 0.004
RVSP (mmHg) 47 32 0.23
Preop 30 Day P Value
LVEDD (mm) 54 47 <0.0001
EDV (ml) 139 106 0.007
LVEF (%) 69 63 0.08
LA Dimension(mm) 46 39 0.001
LA Volume (ml) 117 81 0.003
Mitral Annular 40 35.6 0.004Mitral AnnularDimension (mm) 40 35.6 0.004
RVSP (mmHg) 47 32 0.23

Preop 30 Day P Value
LVEDD (mm) 54 47 <0.0001
EDV (ml) 139 106 0.007
LVEF (%) 69 63 0.08
LA Dimension(mm) 46 39 0.001
LA Volume (ml) 117 81 0.003
Mitral Annular 40 35.6 0.004Mitral AnnularDimension (mm) 40 35.6 0.004
RVSP (mmHg) 47 32 0.23
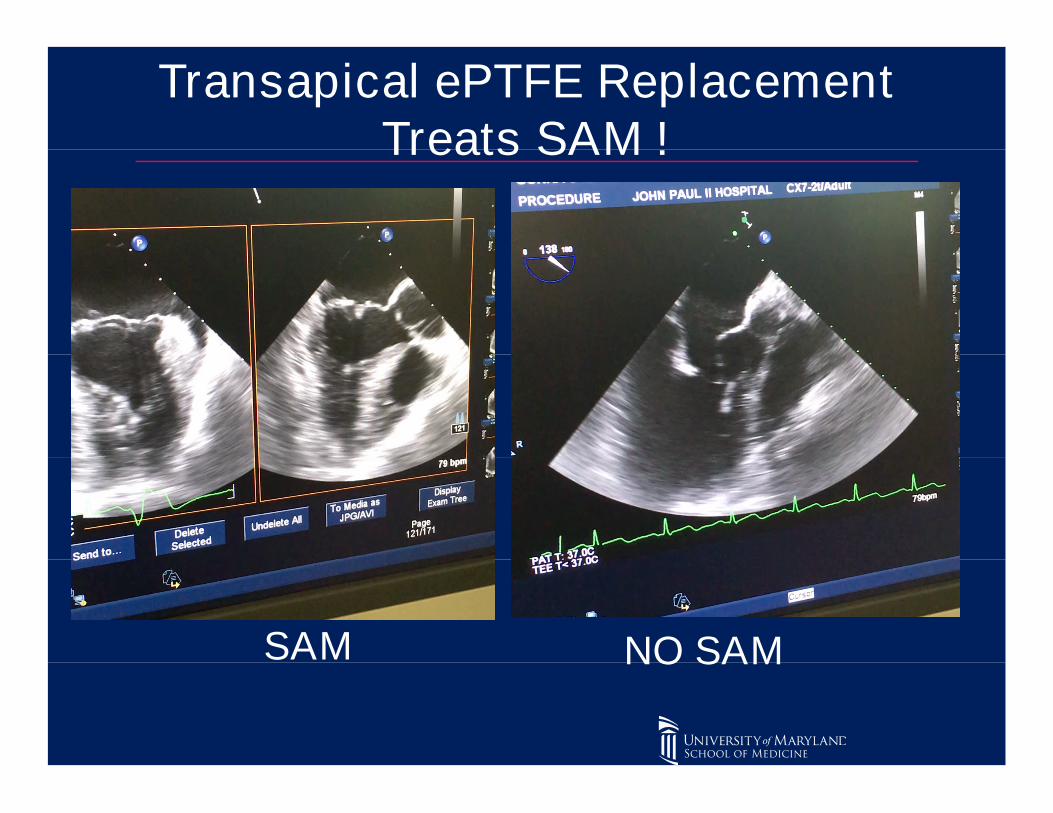
Transapical ePTFE ReplacementTreats SAM !Treats SAM !
SAM NO SAMSAM NO SAM
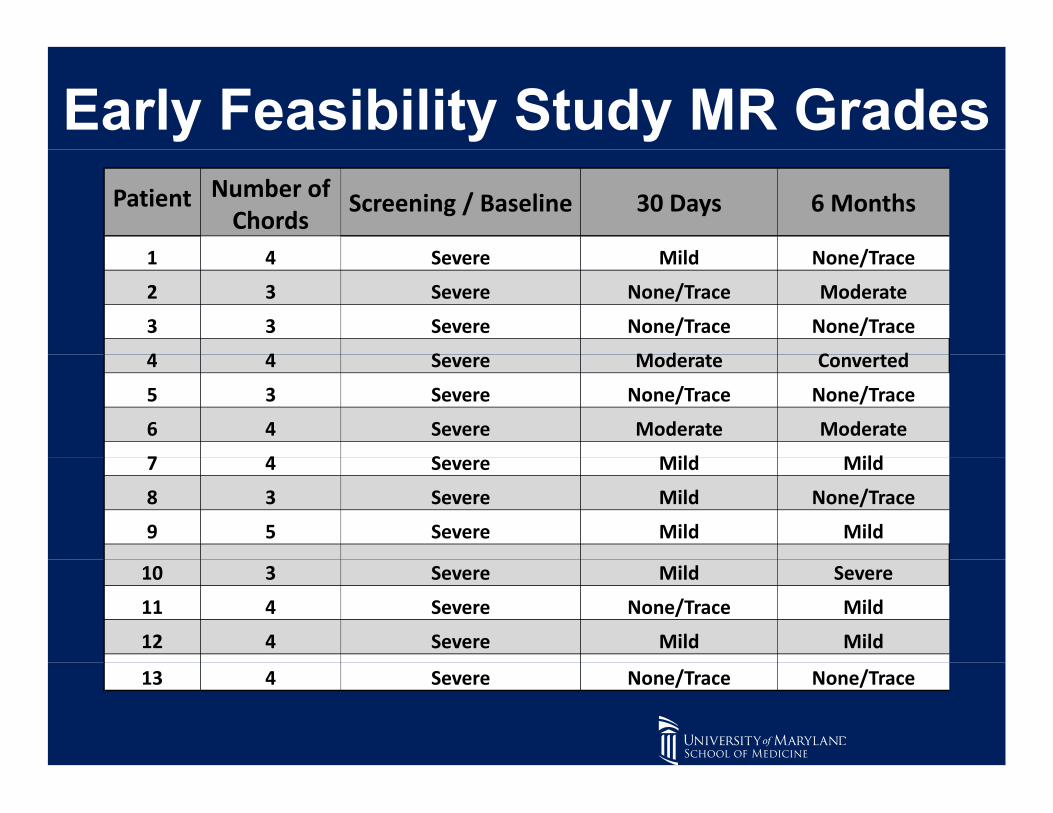
Patient0
Number ofChords
Screening / Baseline 30 Days 6 Months
1 4 Severe Mild None/Trace1 4 Severe Mild None/Trace
2 3 Severe None/Trace Moderate
3 3 Severe None/Trace None/Trace
4 4 Severe Moderate Converted4 4 Severe Moderate Converted
5 3 Severe None/Trace None/Trace
6 4 Severe Moderate Moderate
7 4 Severe Mild Mild7 4 Severe Mild Mild
8 3 Severe Mild None/Trace
9 5 Severe Mild Mild
10 3 Severe Mild Severe10 3 Severe Mild Severe
11 4 Severe None/Trace Mild
12 4 Severe Mild Mild
13 4 Severe None/Trace None/Trace

Patient0
Number ofChords
Screening / Baseline 30 Days 6 Months
1 4 Severe Mild None/Trace1 4 Severe Mild None/Trace
2 3 Severe None/Trace Moderate
3 3 Severe None/Trace None/Trace
4 4 Severe Moderate Converted4 4 Severe Moderate Converted
5 3 Severe None/Trace None/Trace
6 4 Severe Moderate Moderate
7 4 Severe Mild Mild7 4 Severe Mild Mild
8 3 Severe Mild None/Trace
9 5 Severe Mild Mild
10 3 Severe Mild Severe10 3 Severe Mild Severe
11 4 Severe None/Trace Mild
12 4 Severe Mild Mild
13 4 Severe None/Trace None/Trace

Patient0
Number ofChords
Screening / Baseline 30 Days 6 Months
1 4 Severe Mild None/Trace1 4 Severe Mild None/Trace
2 3 Severe None/Trace Moderate
3 3 Severe None/Trace None/Trace
4 4 Severe Moderate Converted4 4 Severe Moderate Converted
5 3 Severe None/Trace None/Trace
6 4 Severe Moderate Moderate
7 4 Severe Mild Mild7 4 Severe Mild Mild
8 3 Severe Mild None/Trace
9 5 Severe Mild Mild
10 3 Severe Mild Severe10 3 Severe Mild Severe
11 4 Severe None/Trace Mild
12 4 Severe Mild Mild
13 4 Severe None/Trace None/Trace
Median Follow-Up 580 Days (386-787)Median Follow-Up 580 Days (386-787)
• 100% Survival
• No Late Stroke• No Late Stroke
• No Thromboembolism
• No Repaired Valve InfectiveEndocarditisEndocarditis
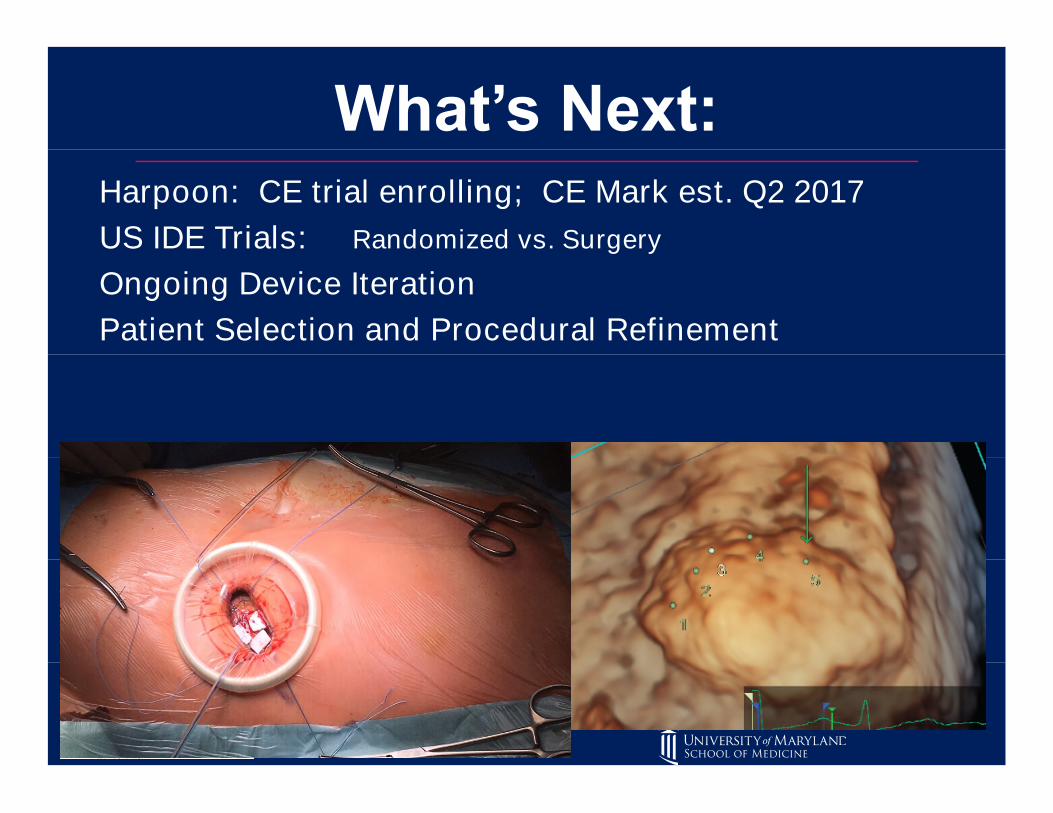
Harpoon: CE trial enrolling; CE Mark est. Q2 2017
US IDE Trials: Randomized vs. SurgeryUS IDE Trials: Randomized vs. Surgery
Ongoing Device Iteration
Patient Selection and Procedural Refinement

CONCLUSIONSINITIAL CLINICAL EXPERIENCEINITIAL CLINICAL EXPERIENCE
BEATING-HEART, IMAGE-GUIDED,TRANSAPICAL MITRAL VALVE REPAIR:TRANSAPICAL MITRAL VALVE REPAIR:
Safe
100 % Procedural Success 100 % Procedural Success
Effective and Durable MR Reduction
Adoptable Adoptable
Does Not Preclude Subsequent Open Mitral ValveRepairRepair
Can Address the Large Majority of Degenerative MitralValve PathologyValve Pathology
Favorable Reverse Remodeling
CONCLUSIONSINITIAL CLINICAL EXPERIENCEINITIAL CLINICAL EXPERIENCE
BEATING-HEART, IMAGE-GUIDED,TRANSAPICAL MITRAL VALVE REPAIR:TRANSAPICAL MITRAL VALVE REPAIR:
Real-time Titration of ePTFE Cords on Beating Real-time Titration of ePTFE Cords on BeatingHeart
Provides tactile / haptic feedback to operator Provides tactile / haptic feedback to operator
Maximize Coaptation
Only Implant = ePTFE Suture
NO: sternotomy, cross clamp, cardioplegia, or NO: sternotomy, cross clamp, cardioplegia, orbypass

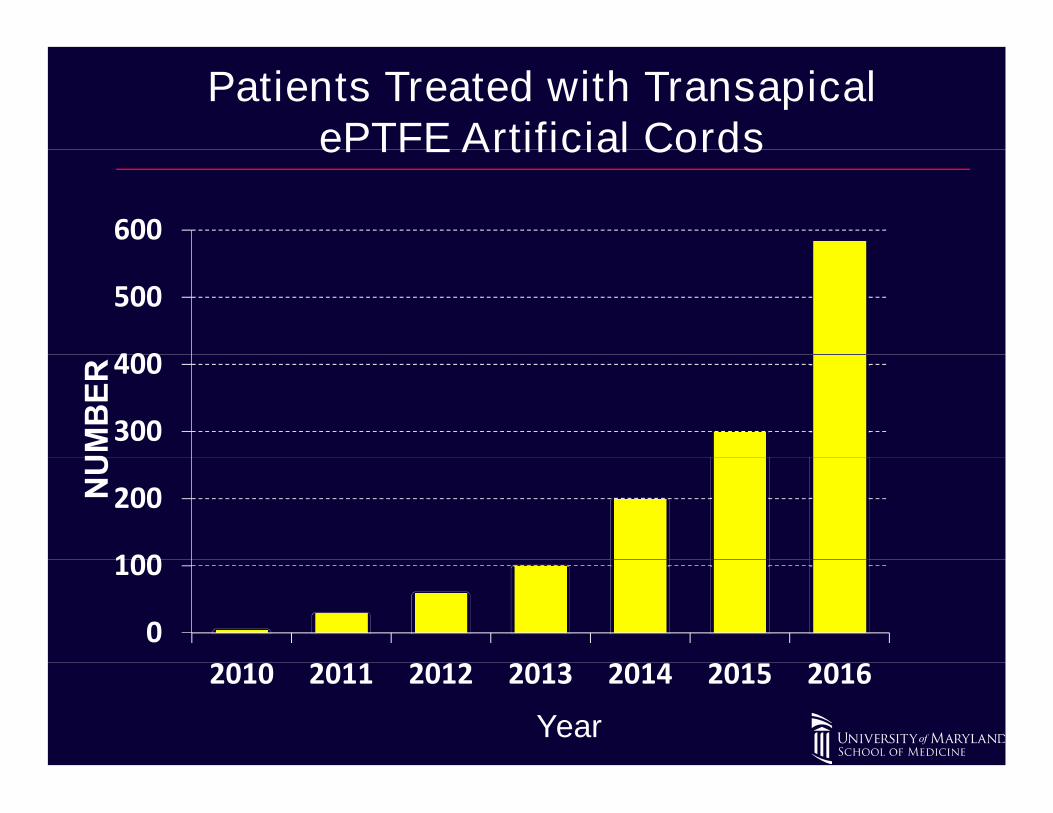
Patients Treated with TransapicalePTFE Artificial CordsePTFE Artificial Cords
600
400
500
300
400
100
200
0
100
2010 2011 2012 2013 2014 2015 2016
Year
2010 2011 2012 2013 2014 2015 2016

Transapical ePTFE Cordal Mitral Repair Conclusions
Key Advantages:
• Sole Implant = ePTFE Suture• Beating-Heart, Less Invasive• Beating-Heart, Less Invasive• NO: sternotomy, cross clamp, cardioplegia, or
bypass• Outstanding Safety Profile• Outstanding Safety Profile• No Fluoroscopy/Radiation• Provides Haptic Feedback to Operator• Provides Haptic Feedback to Operator• Easy to Learn; “Reference-quality” Repair
Accessible to All

Transapical ePTFE Cordal Mitral Repair Conclusions
Key Advantages:
• Real-time Titration of ePTFE Cordal Lengthon Loaded Heart: Maximize Coaptationand Repair Qualityand Repair Quality
• Encourage Earlier Intervention In MR• SAM is easily treatable• SAM is easily treatable• Favorable Reverse Ventricular Remodeling• Does NOT Preclude Subsequent
Conventional RepairConventional Repair• Effective, Durable MR Reduction