Embed Size (px)
DESCRIPTION
Chronic Illness in a Complex Health Economy: The Perils & Promises of Downstream & Upstream Reforms. Jack Homer, Gary Hirsch, and Bobby Milstein International System Dynamics Conference Boston, Massachusetts July 29 – August 2, 2007. The U.S. Health Care Quandary. A puzzle: - PowerPoint PPT Presentation
Citation preview

Chronic Illness in a Complex Health Economy: The Perils & Promises of Downstream & Upstream Reforms
Jack Homer, Gary Hirsch, and Bobby Milstein
International System Dynamics ConferenceBoston, Massachusetts
July 29 – August 2, 2007

The U.S. Health Care Quandary• A puzzle:
– U.S. has world’s highest healthcare costs
– But our health and longevity are only mediocre for a developed country
– How did this happen?
• Some preliminary thinking (causal loops) – CDC’s Health Systems Workgroup 2003
– SD Society’s Health Policy Special Interest Group 2005
• To build a solid theory, need to look at data series– Healthcare spending & price inflation
– Disease & risk prevalence and deaths
– Health insurance coverage
– Health care assets & investments

Data sources
Source Data Topics
National Health Expenditures Audit(NHEA), 1960-2004
- Health care spending by type- Investments in structures & equipment - Public health spending
US Census- Population growth (1960-2010)- Health insurance coverage (1987-2005)
Bureau of Labor Statistics (BLS), 1960-2005
- Overall & medical consumer price index- GDP and GDP deflator
National Health Interview Survey (NHIS), 1982-2004
- Self-reported health status
Behavioral Risk Factor Surveillance System (BRFSS), 1991-1999
- Prevalence of cardiovascular risk factors
National Vital Statistics Records (NVSR), 1960-2003
- Deaths
Nat’l Institute for Health Care Mgmt (NIHCM) & proprietary sources
- Spending on drugs for hypertension (1980-2004) and cholesterol (1987-2004)

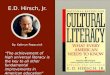
Health Care Spending and Self-reported Prevalence of Impaired Health 1982-2004
(National Health Expenditure Accounts, National Health Interview Survey)
0%
10%
20%
30%
40%
50%
60%
200420022000199819961994199219901988198619841982
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
Self-reported health (NHIS) good, fair, or poor (not excellent or very good)
Health consumption (NHEA) per capita in year 2000 dollars
Sources: National Health Expenditure Accounts (NHEA), US Census; National Health Interview Survey (NHIS), CDC

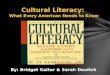
Health Population Stocks and Flows
Populationwith disease
Population atrisk
RiskmanagementAdverse behaviors &
living conditions
Disease cureand recovery
Diseaseincidence
Populationnot at risk
Risk onset
Risk reduction
Populationnet inflow
Disease relateddeaths
Injury & violencedeath rate
Complications(urgent episodes)
Diseasemanagement
Urgent care

Disease Care (Downstream) Loops
Diseaseprevalence
Healthcareassets
Insurancecoverage
Extent ofdisease care
Complications& Deaths
-
-
Diseaseincidence
Personalhealthcarespending Reimbursement and
coverage restrictions
-
Investment innew assets -
Healthcareprices
R1
B1
R2
B2
B3
Provideradaptation
R3
(Disease management,Urgent care)
R1. Revenues reinvested
B1. Dis Mgmt reducescomplications
R2. Care prolongslife, increases demand
B2. High costs lead to less reimbursement, inhibiting investment
B3. High costs lead to less insurance,inhibiting disease mgmt
R3. “Tug of war” leading toprice inflation

Downstream What-Ifs (1960-2010)
• What if employers didn’t cut insurance? Extent of care improved, but health care costs increased.
• What if providers didn’t raise their fees? Costs reduced, insurance increased, so greater extent of care.
– However, a fixed-price policy threatens provider autonomy, and may trigger a decline in supply of providers
• What if payers didn’t restrict reimbursements? Investments and assets increased, so greater extent of care. Also, providers don’t feel need to raise their fees, so costs reduced and insurance increased, so even greater extent of care.
– However, private payers may not trust providers to “play fair”, and will fear an explosion in wasteful spending and investment
• Conclusion: In U.S. system, hard to find a politically acceptable way to limit costs but also encourage beneficial investments.

Risk & Disease Prevention (Upstream) Loops
Diseaseprevalence
Healthcareassets
Insurancecoverage
Extent ofdisease care
Complications& Deaths
-
-
Riskprevalence
Diseaseincidence
Riskmanagement
-
Health protectionfunding andorganizing-
Personalhealthcarespending
Reimbursement andcoverage restrictions
-
Investment innew assets -
Healthcareprices
R1
B1
R2
B2
B3
B4
B5
Provideradaptation
R3
Adverse behaviors& living conditions
B6
(Disease management,Urgent care)
B4. Risk mgmt $ linked to downstream $
B5. Health protection $ linked to downstream $
B6. Health protection $ linked to risk prevalence (“sin taxes”)

Upstream What-Ifs (1960-2010)
• What if the risk management portion of non-urgent care were doubled? Less onset of disease and lower downstream costs, with a payback time of 15 years.
• What if (starting 1980) $5 were spent on health protection for every $100 of downstream spending? Even greater reduction in disease onset and downstream costs, but with a payback time of 22 years.
– A longer payback time because health protection acts further upstream than risk management
– But cost data reflect only direct costs of care, not productivity losses; Whatcom County models (SDR 2004) show payback time much shorter when productivity losses taken into account
• Conclusion: Even in the dysfunctional U.S. system, progress to reduce costs and improve health through upstream measures is possible…but will require commitment and political will.

ADDITIONAL SLIDES



Source: Centers for Disease Control and Prevention. Health-related quality of life: prevalence data. National Center for Chronic Disease Prevention and Health Promotion, 2003. Accessed March 21 at <http://apps.nccd.cdc.gov/HRQOL/>.
But health-related quality of life has worsened
14% increase

Upstream work is a very small fraction of health spending
Upstream Prevention and Protection-----------------------------------Total 3%
Downstream Care and Management--------------------------------Total 97%
Brown R, Elixhauser A, Corea J, Luce B, Sheingod S. National expenditures for health promotion and disease prevention activities in the United States. Washington, DC: Battelle; Medical Technology Assessment and Policy Research Center; 1991. Report No.: BHARC-013/91-019.

Upstream and Downstream in the Health System
GeneralPopulation
Becomingvulnerable
Becoming no longervulnerable
VulnerablePopulation
BecomingAfflicted
Afflictedwithout
Complications DevelopingComplications
Afflicted withComplications
Dying fromComplications
CENTERS FOR DISEASE CONTROL & PREVENTION
Gerberding JL. Protecting health—the new research imperative. JAMA 2005; 294(11): 1403-1406.
Levins R, Lopez C. Toward an ecosocial view of health. Intl J Health Svcs 1999; 29(2):261-293.
SAFER • HEALTHIER • PEOPLE ™

Health Policy Reform Loops (ISDC 2005)
Containingcosts
Improving insurancecoverage & distribution
of care
Improvingquality
Protectinghealth
Safer,HealthierPeople
People atRisk
People withDiseaseBecoming
at riskDeveloping
diseaseDying from
disease
Adverse livingconditions
Insurance coverage &Reimbursement rates
-
Acute cases
High-tech acute carecapacity & utilization
Health carecosts
Funds available forimproving living
conditions
-
-
Costs of managingrisk and disease
Costs of acute care
Recovering orgetting cured
Becoming safer,healthier
-
Administrativeoverhead of
providers
Efforts to improveliving conditions
-
-
-
Adequacy of providers inless wealthy & more
remote areas
Effectively managedrisk and disease
Effective acute care
People withdisease and at
risk
High-tech risk &disease mgmt capacity
& utilization
-
Variety of payer feeschedules andarrangements
-
-
-
Inappropriate anddefensive use of
high-tech acute care-
Costs of regulationand qualityassurance

0%
20%
40%
60%
80%
200019981996199419921990
>1
>2
Risk factors include high blood pressure, high cholesterol, diabetes, obesity, smoking
Fraction with specified # of risk factors (source: NHIS)
Prevalence of cardiovascular risk factors 1991-1999
(National Health Interview Survey)

60%
65%
70%
75%
80%
85%
90%
200420022000199819961994199219901988
0%
5%
10%
15%
20%
25%
30%
Total insured
Private insured
Gov't-only
Medicaid
Health insurance coverage 1987-2004(US Census)

$0
$200
$400
$600
$800
200420001996199219881984198019761972196819641960
$0
$1,000
$2,000
$3,000
$4,000
Estimation of structure & equipment (S&E) assets assumes depreciation rate of 5%/year, and assets initially equal to 12 years of investment. The average age of S&E assets remains in the 8-12 year range, settling around 11 years by the 1990s.
S&E investment per capita in year 2000 dollars per year
S&E assets per capita in year 2000 dollars
Healthcare structures & equipment investment and estimated asset value
1960-2004 (in year 2000 dollars per capita)

0
200
400
600
800
2004200019961992198819841980
Thousands of MDs (source: AMA)
Total active
Office-based
Primary care
Medical doctors 1980-2004 (in thousands)
Healthcare assets also include human capital, in the form of doctors, nurses, and other trained personnel. The number of MDs grew somewhat more slowly than did S&E assets, helping to explain why a shortage of medical personnel has developed.

$0
$20
$40
$60
$80
$100
2004200019961992198819841980
Anti-hypertensive
Anti-cholesterol
Anti-hyp + Anti-chol
Spending per capita in year 2000 dollars (sources: various)
Anti-hypertensive & anti-cholesterol drug spending per capita 1980-2004

Population death rate from coronary heart disease, 1950–1998
0.6%
0.5%
0.4%
0.2%
0.1%
0%1950 1960 1970 1980 1990 2000
Age-a
dju
sted D
eath
Rate
0.3%
Year
Marks JS. The burden of chronic disease and the future of public health. CDC Information Sharing Meeting. Atlanta, GA: National Center for Chronic Disease Prevention and Health Promotion; 2003.
1950

0
4
8
12
16
200420001996199219881984198019761972196819641960
Consumer price index (CPI-U) relative to 1960
Total economy
Healthcare
Consumer Price Indices for Health Care andthe General Economy 1960-2004 (1960=1)

Key Calibration Assumptions Allowing a Good Fit to History (1960-2004)
• Revenue reinvestment rate started at 13-14% in the 1960s, but in reaction to higher costs declined to 10% in 1980, and 6% by 2004.
• Government-insured fraction of those not privately insured rose from 18% in 1960, to 37% in 1970, to 45% in 1975, to 48% in 1990, to 50% in 2000.
• Reduction in care due to no insurance coverage is 60% for urgent/rehab care and 85% for disease management.
• Risk onset rate due to adverse behaviors and living conditions increased by 30% from 1980 to 1995, and by another 5% through 2005.
– This pattern corresponds well to apparent pattern of caloric intake driving the rise in U.S. obesity since late 1970s. See Homer/CDC obesity model presented at ISDC 2006.

Insured fraction of population
1
0.9
0.8
0.7
0.6
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Healthcare consumption fraction of GDP
0.2
0.15
0.1
0.05
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Healthcare price index vs general economy (1960=1)
3
2
1
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Healthcare consumption and investments per capita ($/yr)
6,000 1,200
4,000 800
2,000 400
0 0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Simulation versus Historical Data (1)
Consumption-sim
Consumption-data (1)
Investment-sim
Investment-data (2)
Total-sim
Total-data (5)
Private-sim
Private-data (6)
Sim
Data (3)
Sim
Data (4)

Deaths per population per year
0.01
0.009
0.008
0.007
0.006
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Fraction of population with disease or at-risk
0.8
0.6
0.4
0.2
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Simulation versus Historical Data (2)
Sim
Data (9)Risk-sim
Risk-data (7)
Disease-sim
Disease-data (8)
Data sources:
(1 & 3) Consumption: NHEA personal health care spending, 1960-2004 annual, divided by pop and by GDP deflator (2000=1);
(2) Investment: NHEA investments in structures and equipment, 1960-2004 annual, divided by pop and by GDP deflator;
(4) Price: BLS medical care CPI (1960=1) divided by general economy CPI (1960=1), 1960-2005 annual;
(5 & 6) Insured: Census fraction of pop all ages covered by private or govt health insurance, 1987-2005 annual;
(7) Risk prevalence: BRFSS fraction adults report at least one of five cardiovascular risk factors, 1991-1999 odd years;
(8) Disease prevalence: NHIS fraction pop all ages report health as good, fair, or poor (i.e., not excellent or very good), 1982-2004 annual;
(9) Deaths: NVSR total deaths per year divided by pop, 1960-1980 every 5 years, 1980-2003 annual.

Test Results for Downstream What-ifs
Base
No price up
No reimburse down
No coverage down
Base
No price up
No reimburse down
No coverage down
Base
No price up
No reimburse down
No coverage down
Base
No price up
No reimb. down
Healthcare assets per capita
6,000
4,500
3,000
1,500
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Insured fraction of popn
1
0.95
0.9
0.85
0.8
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Healthcare costs per capita
8,000
6,000
4,000
2,000
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Urgent episodes per capita
0.18
0.16
0.14
0.12
0.1
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
No cover down

Test Results for Upstream What-Ifs
More risk mgmt
Base
More health protection
No obesity up
Base
More risk mgmt
More health protection
No obesity up
Base
More risk mgmt
More health protection
No obesity up
Base
More risk mgmt
More health protection
No obesity up
Upstream spending per capita
400
300
200
100
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Fraction of popn with disease
0.4
0.35
0.3
0.25
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Healthcare costs per capita
8,000
6,000
4,000
2,000
0
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)
Urgent episodes per capita
0.18
0.16
0.14
0.12
0.1
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010Time (year)