Embed Size (px)
DESCRIPTION
Jab Mein Thaa , Tab Guru Nahin ‚ Aub Guru Hai , Mein Nahin Sab Andhiyara Mit Gaya‚ Jab Deepak Dekhya Mahin - PowerPoint PPT Presentation
Citation preview
Jab Mein Thaa, Tab Guru Nahin‚
Aub Guru Hai, Mein Nahin
Sab Andhiyara Mit Gaya‚
Jab Deepak Dekhya Mahin
When "I“, the Ego, was with me, then I couldn’t
realize the almighty within; Now, the Almighty "is"
ever with me and there is no place for this Ego.
All the darkness (illusion) within me is mitigated,
on realizing the light (illumination) within.
SK
www.drsarma.in
Diabetic HypertensionDiabetic Hypertension
The Two TerroristsThe Two Terrorists
THE ENORMITY OF THE
PROBLEM - COMPOUNDED
THE ENORMITY OF THE
PROBLEM - COMPOUNDED
How Common is this Duo?How Common is this Duo?
HTN is twice as common in DMHTN is twice as common in DM
New onset DM is 2.5 times in HTNNew onset DM is 2.5 times in HTN
20 to 40% of IGT pts have HTN20 to 40% of IGT pts have HTN
40 to 50% of Type 2 DM have HTN40 to 50% of Type 2 DM have HTN
Only 1/4 of HTN in DM is controlledOnly 1/4 of HTN in DM is controlled
DM + HTN – CV Risk 3 foldDM + HTN – CV Risk 3 fold
What Causes HTN in DMWhat Causes HTN in DM
• Metabolic Syndrome – Mainly IR, ED,
BG
• Excessive RAAS activity is the main
mechanism
• HTN due to nephropathy in T2DM – GS -
KWL
• Renal scarring - Recurrent pyelonephritis
• Endocrine causes for both HTN & DM– Cushing’s, Conn’s, Pheochromo,
Acromegaly
• Coincidental – DM on existing HTN
• Diabetogenic antihypertensive drugs (D
and B)
• Drugs causing both HTN & DM – OCP, CS
Each Perpetuates the OtherEach Perpetuates the Other
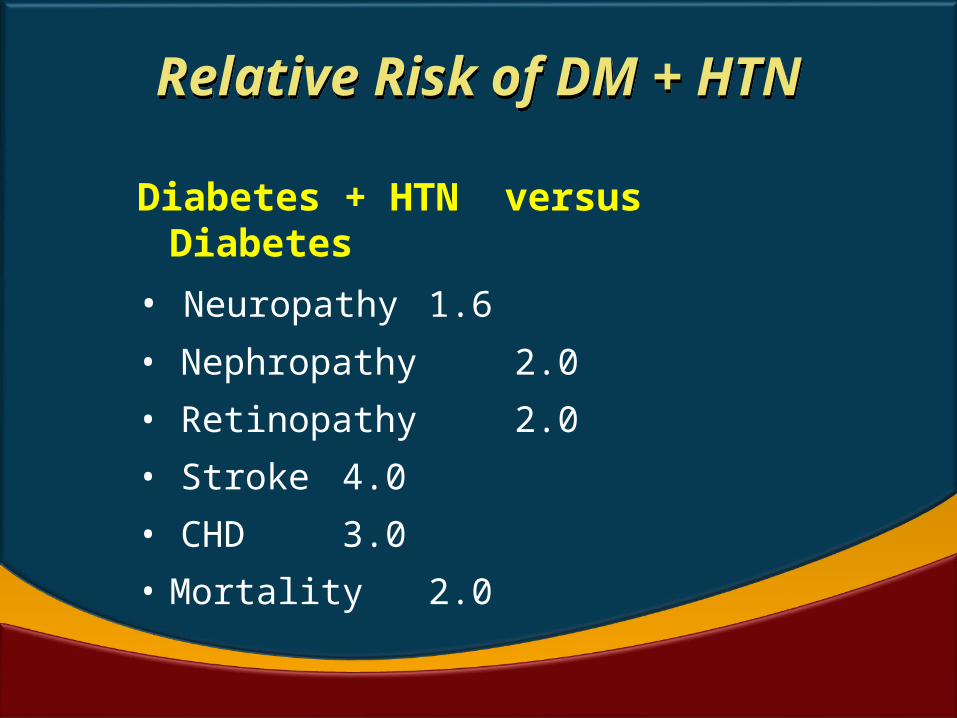
Relative Risk of DM + HTNRelative Risk of DM + HTN
Diabetes + HTN versus Diabetes
• Neuropathy 1.6
• Nephropathy 2.0
• Retinopathy 2.0
• Stroke 4.0
• CHD 3.0
• Mortality 2.0
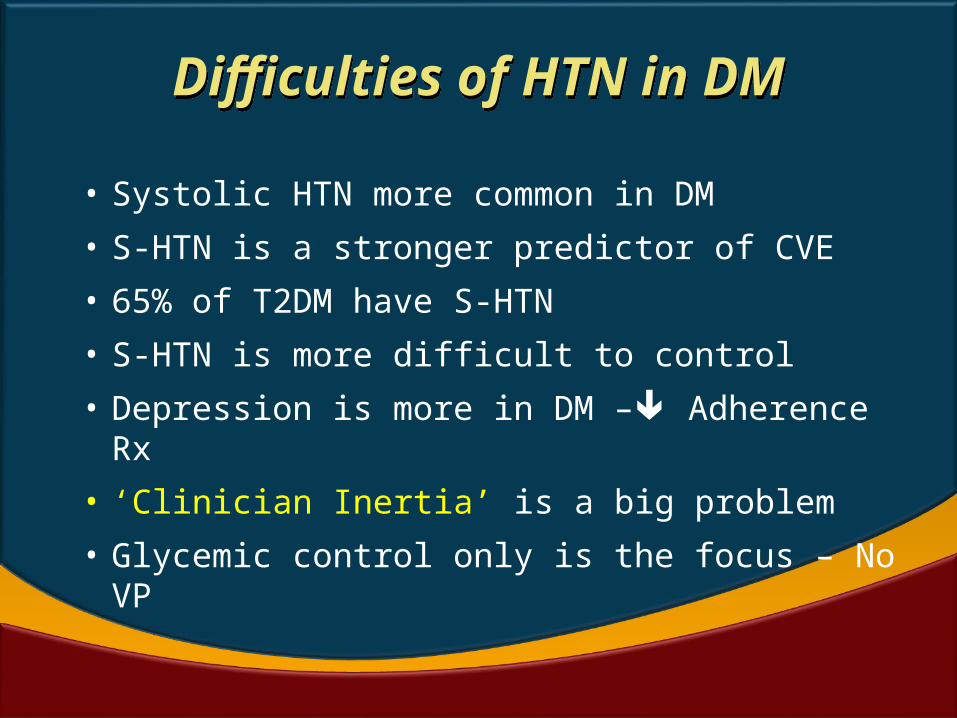
Difficulties of HTN in DMDifficulties of HTN in DM
• Systolic HTN more common in DM
• S-HTN is a stronger predictor of CVE
• 65% of T2DM have S-HTN
• S-HTN is more difficult to control
• Depression is more in DM – Adherence Rx
• ‘Clinician Inertia’ is a big problem
• Glycemic control only is the focus – No VP
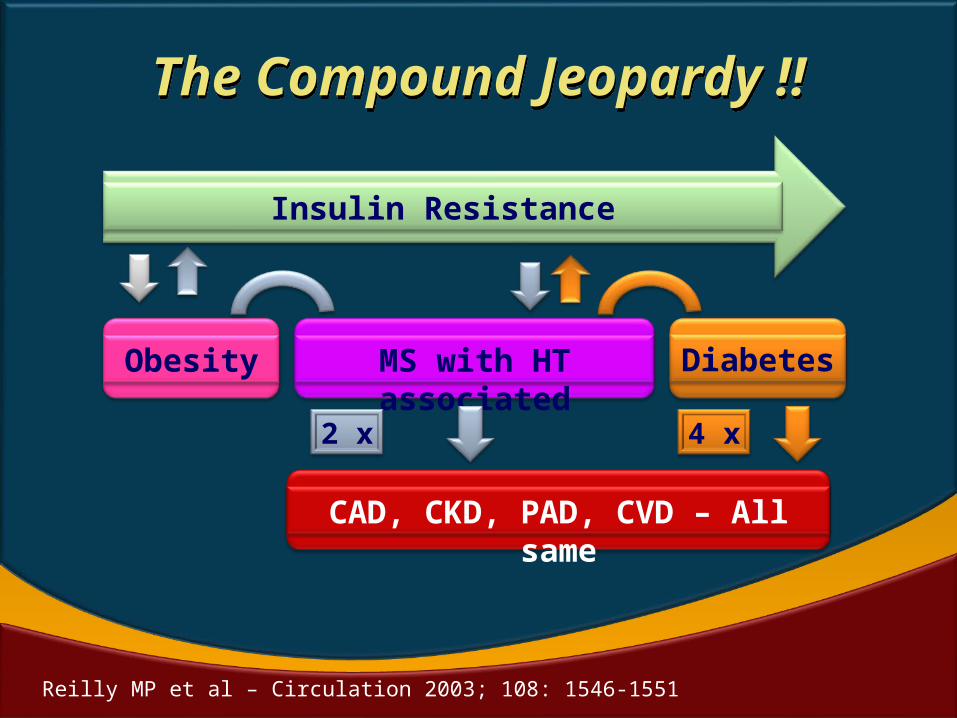
The Compound Jeopardy !!The Compound Jeopardy !!
Insulin Resistance
Obesity Diabetes
MS with HT associated
CAD, CKD, PAD, CVD – All same
2 x 4 x
Reilly MP et al – Circulation 2003; 108: 1546-1551
THE DASAVATARAM AND
THE VISWA ROOPAM
THE DASAVATARAM AND
THE VISWA ROOPAM
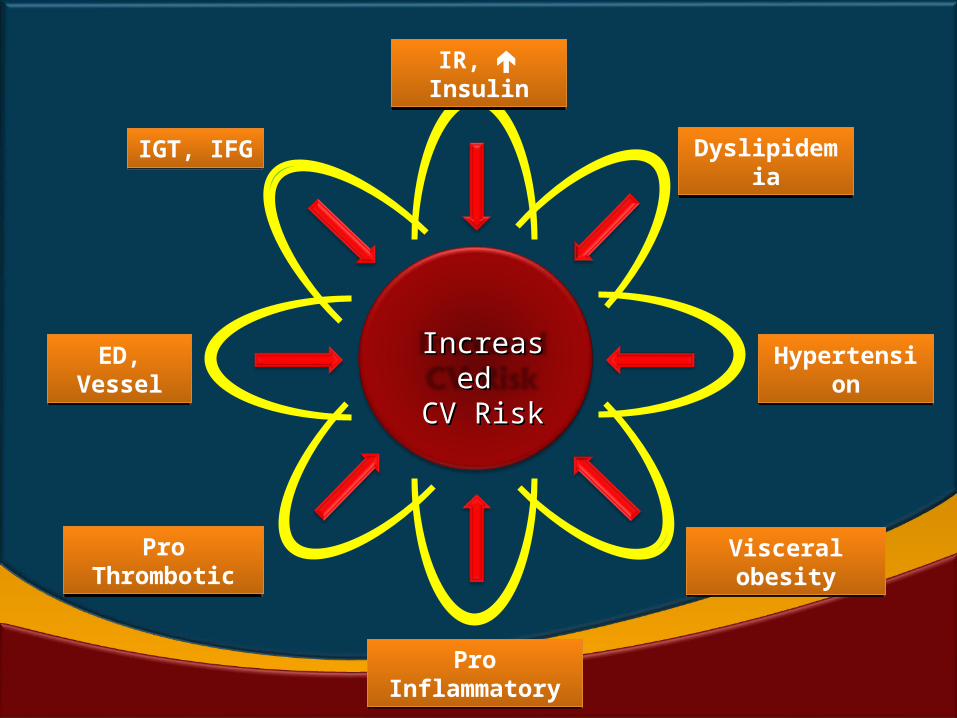
IGT, IFGIGT, IFG
IR, InsulinIR,
Insulin
Dyslipidemia
Dyslipidemia
Hypertension
Hypertension
ED, Vessel
ED, Vessel
Visceral obesityVisceral obesity
Pro Inflammatory
Pro Inflammatory
Pro Thrombotic
Pro Thrombotic
IncreaseIncreased d
CV RiskCV Risk
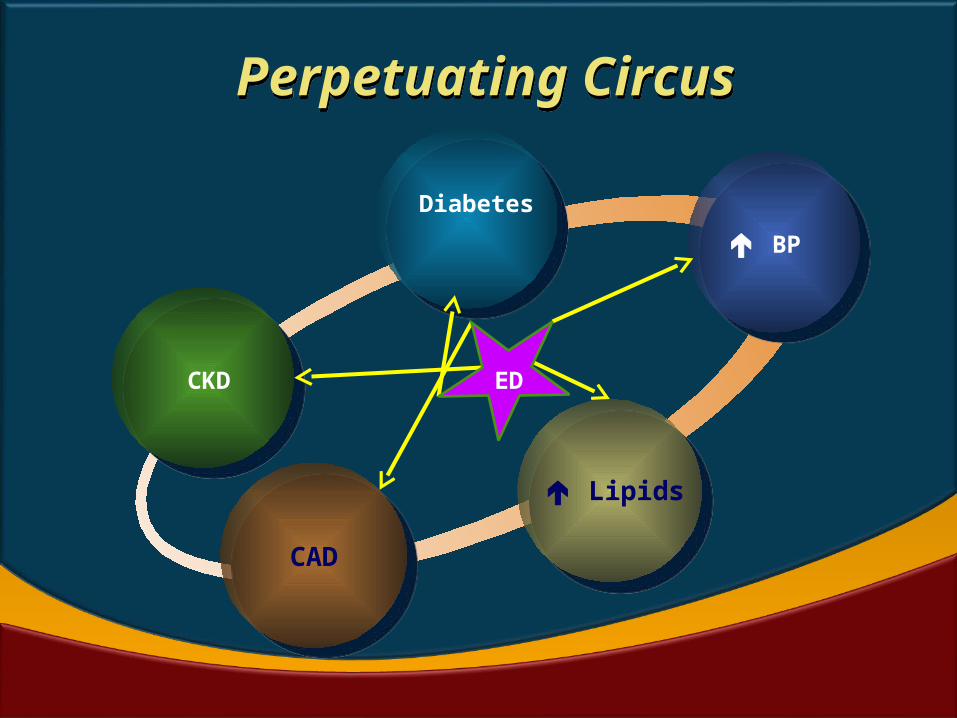
Perpetuating Circus Perpetuating Circus
CKD
Diabetes
BP
Lipids
CAD
ED
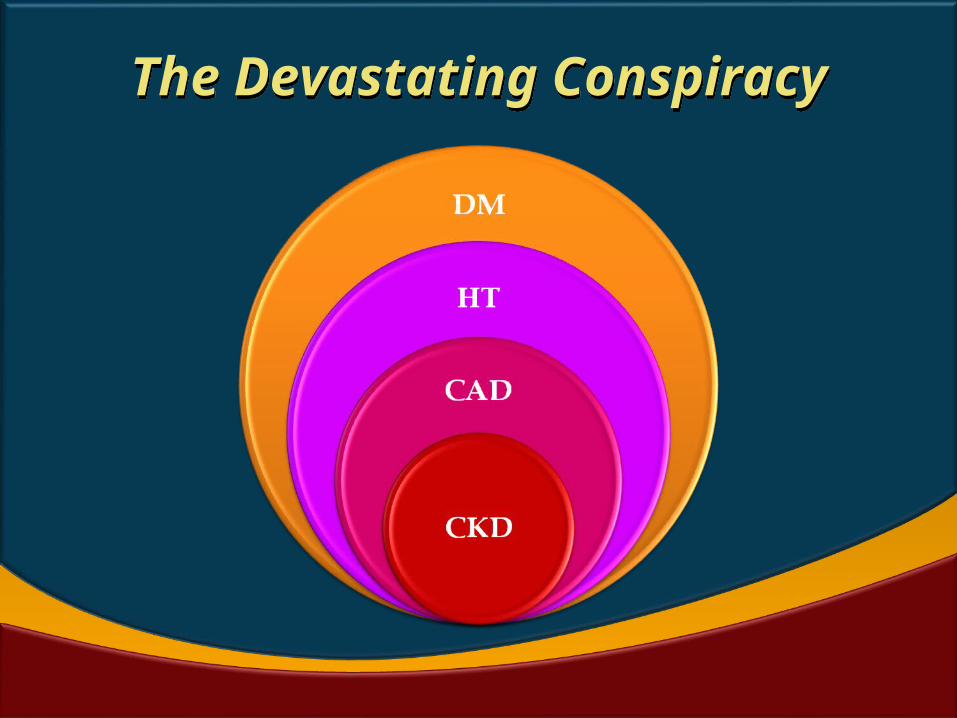
The Devastating ConspiracyThe Devastating Conspiracy
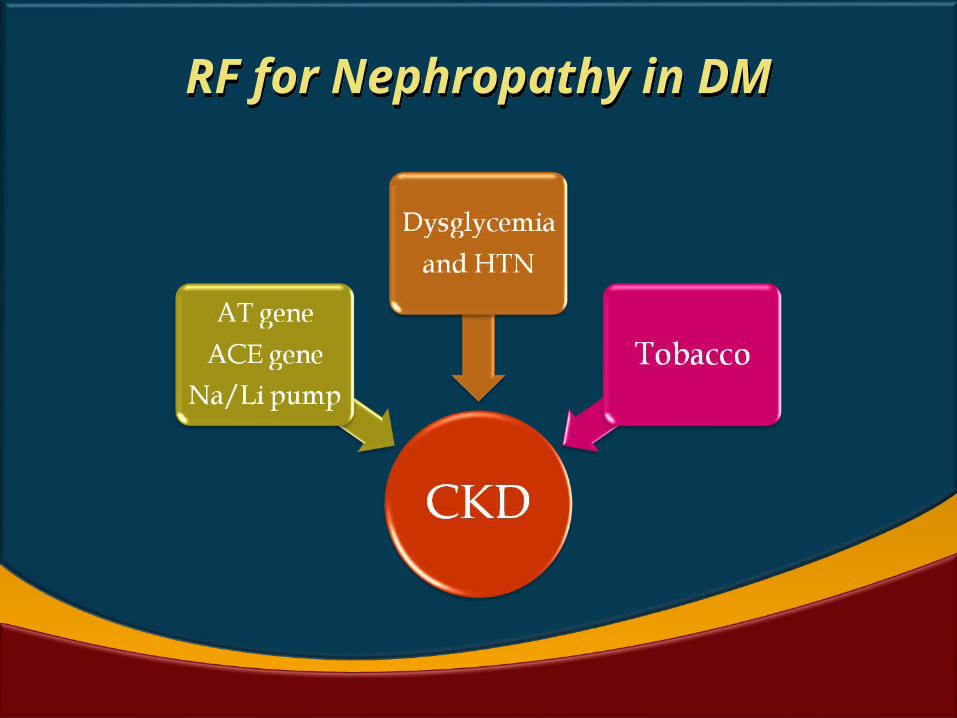
RF for Nephropathy in DMRF for Nephropathy in DM
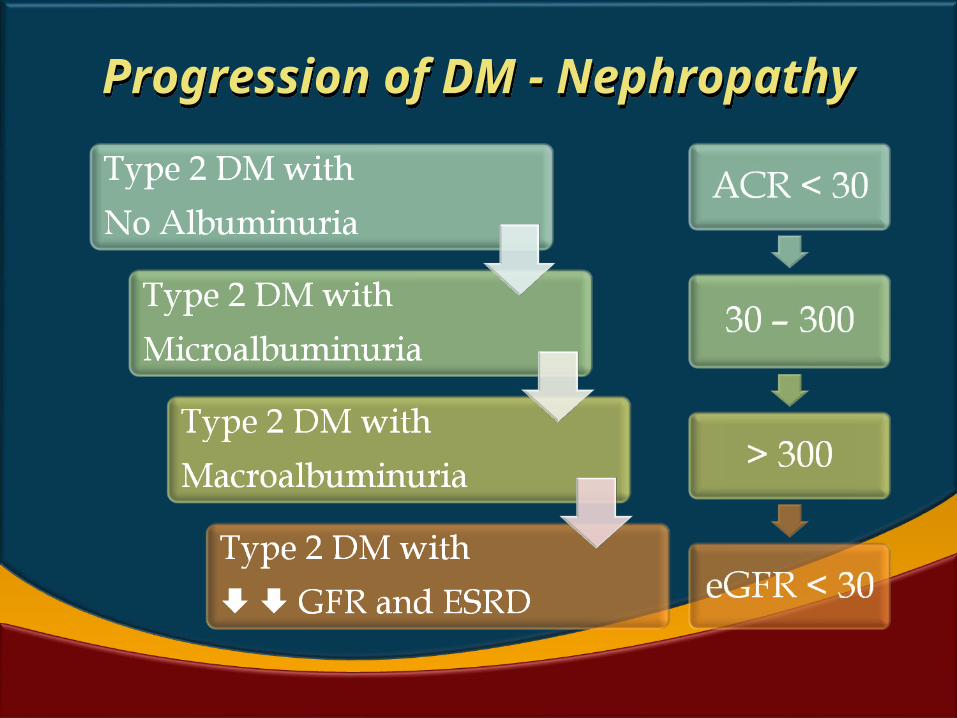
Progression of DM - Nephropathy
Progression of DM - Nephropathy
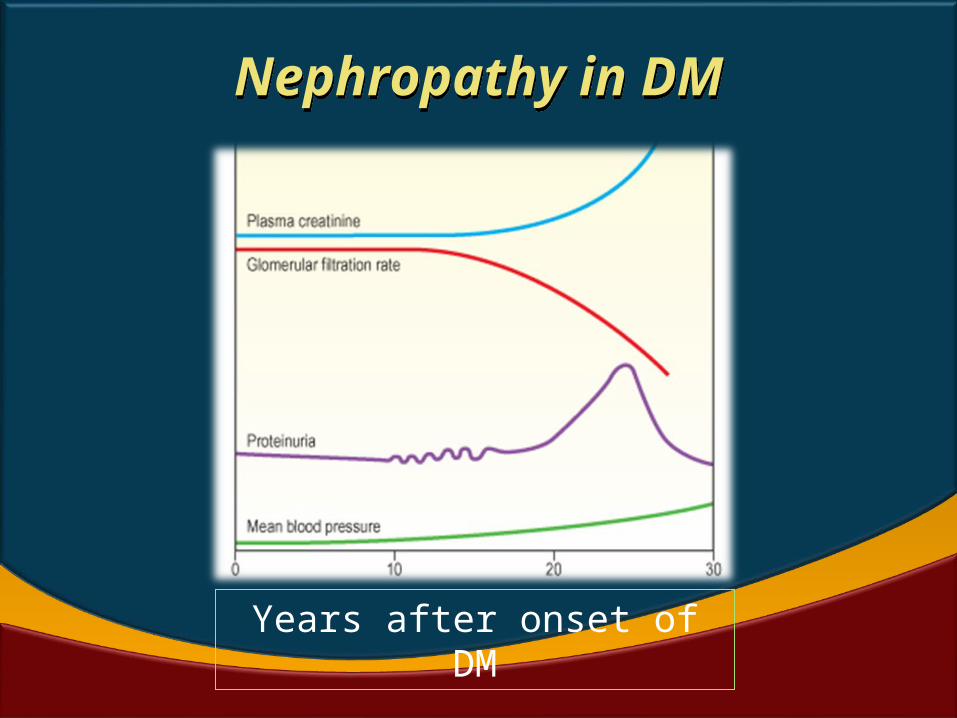
Nephropathy in DMNephropathy in DM
Years after onset of DM
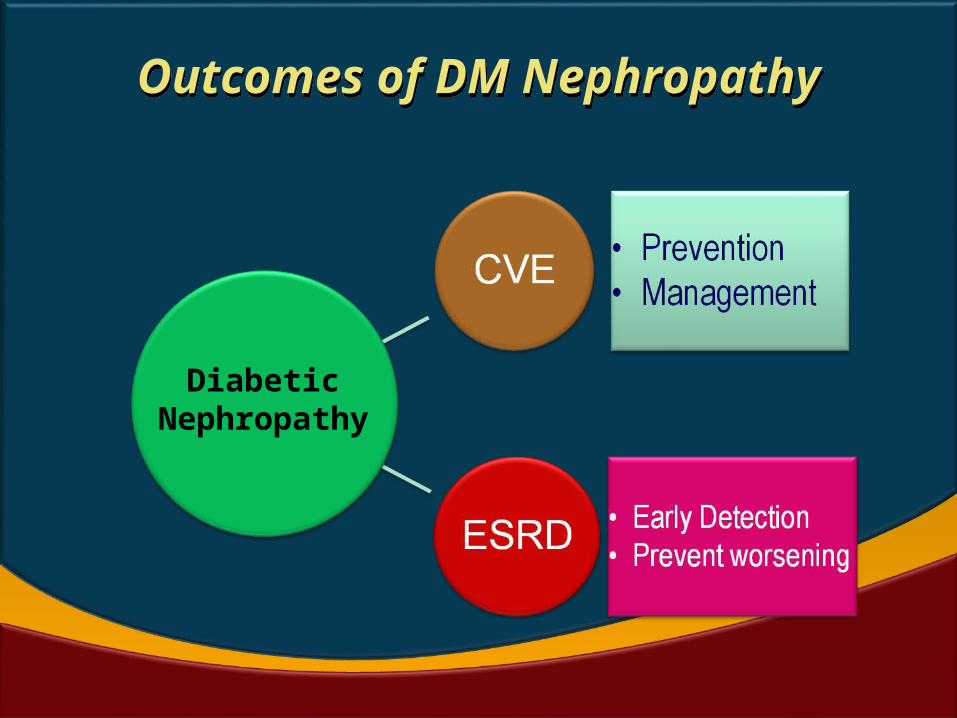
Outcomes of DM NephropathyOutcomes of DM Nephropathy
Diabetic Nephropathy
THE EVIDENCE BASE
DM + HT IS DANGEROUS
THE EVIDENCE BASE
DM + HT IS DANGEROUS
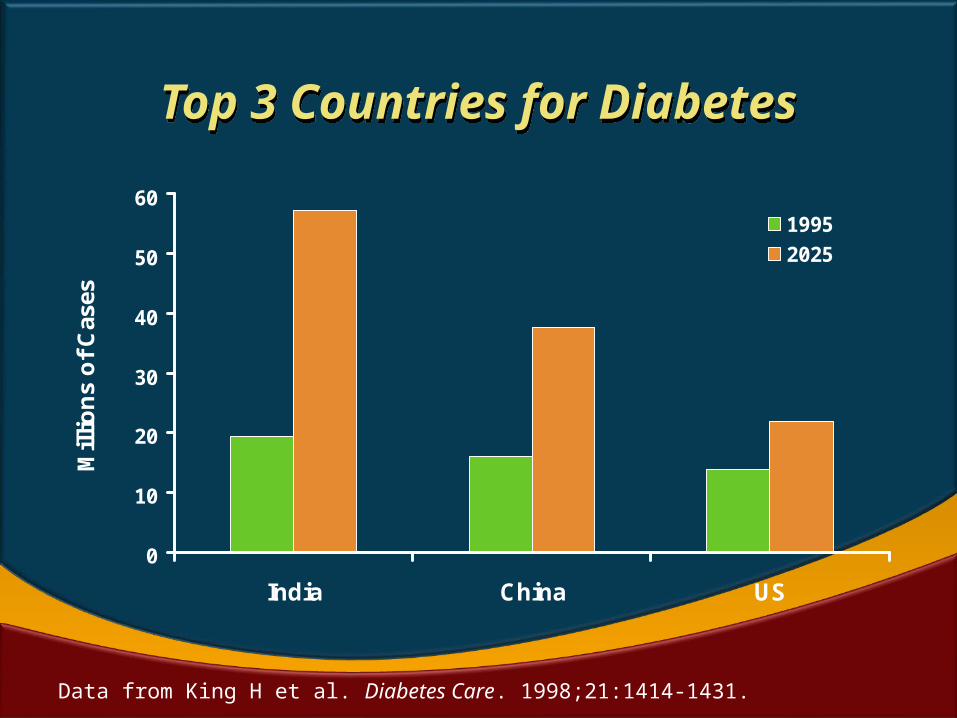
Data from King H et al. Diabetes Care. 1998;21:1414-1431.
Top 3 Countries for DiabetesTop 3 Countries for Diabetes
0
10
20
30
40
50
60
India China US
Mil
lio
ns
of
Cas
es
1995
2025
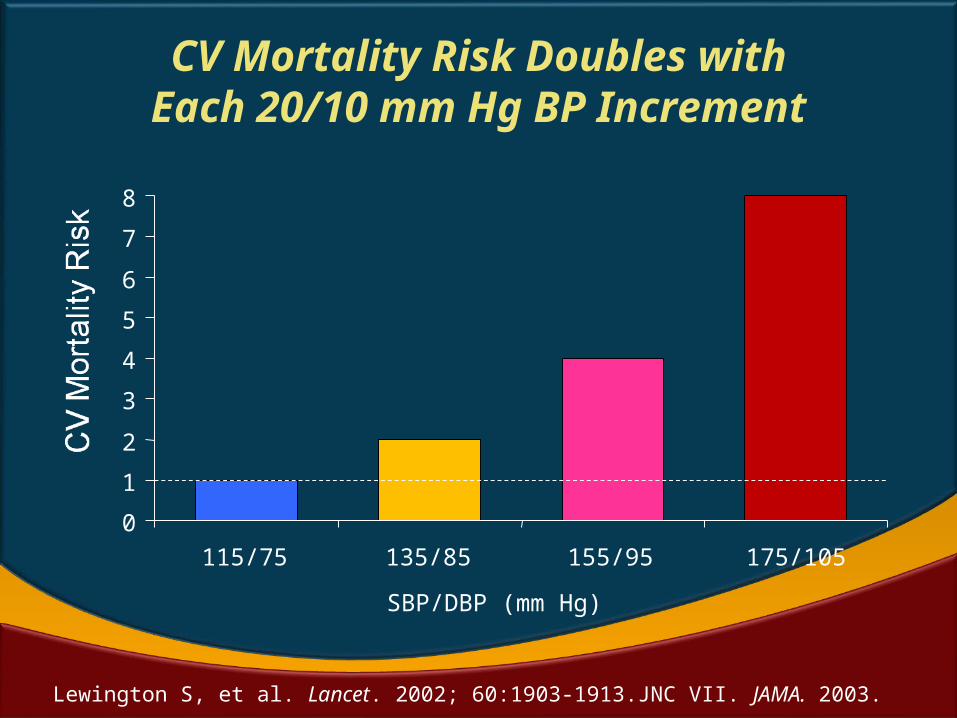
CV Mortality Risk Doubles withEach 20/10 mm Hg BP Increment
Lewington S, et al. Lancet. 2002; 60:1903-1913.JNC VII. JAMA. 2003.
SBP/DBP (mm Hg)
0
1
2
3
4
5
6
7
8
115/75 135/85 155/95 175/105
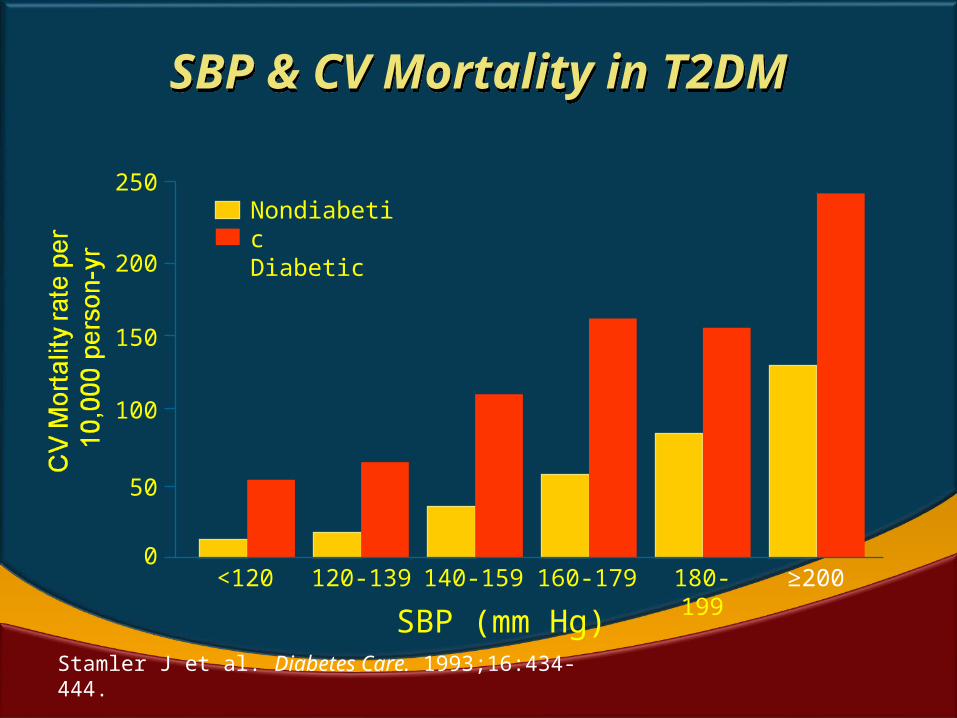
SBP & CV Mortality in T2DMSBP & CV Mortality in T2DM
250
200
150
100
50
0<120 120-139 140-159 160-179 180-199
SBP (mm Hg)
NondiabeticDiabetic
Stamler J et al. Diabetes Care. 1993;16:434-444.
≥200
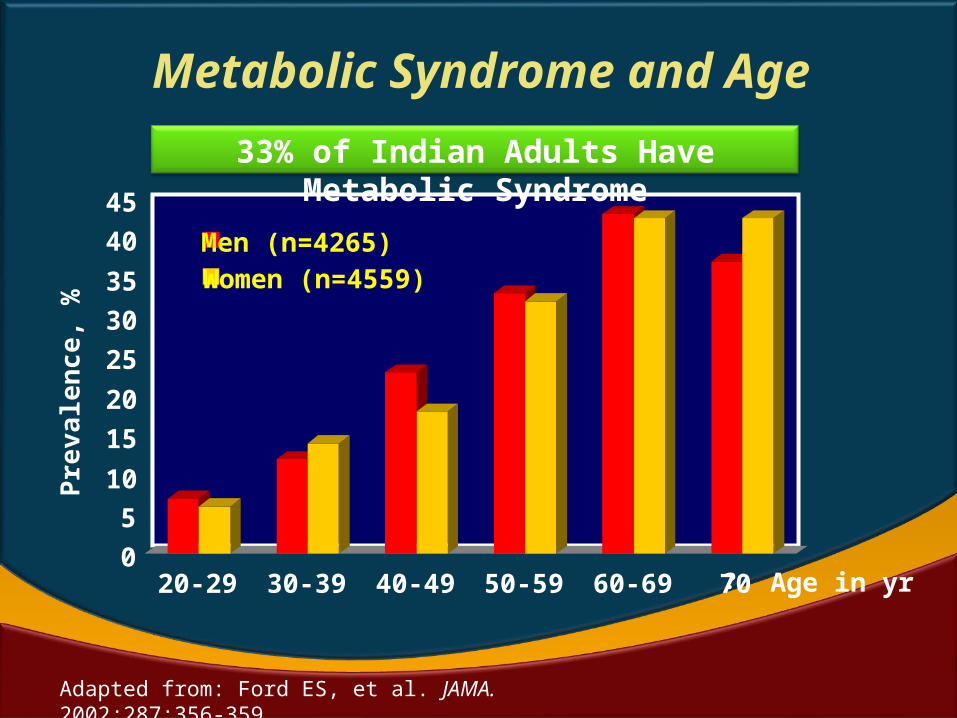
Metabolic Syndrome and AgeP r
e va l
e nc e
, %
Age in yr
Adapted from: Ford ES, et al. JAMA. 2002;287:356-359.
33% of Indian Adults Have Metabolic Syndrome
0
5
10
15
20
25
30
35
40
45
20-29 30-39 40-49 50-59 60-69 ?70
Men (n=4265)Women (n=4559)
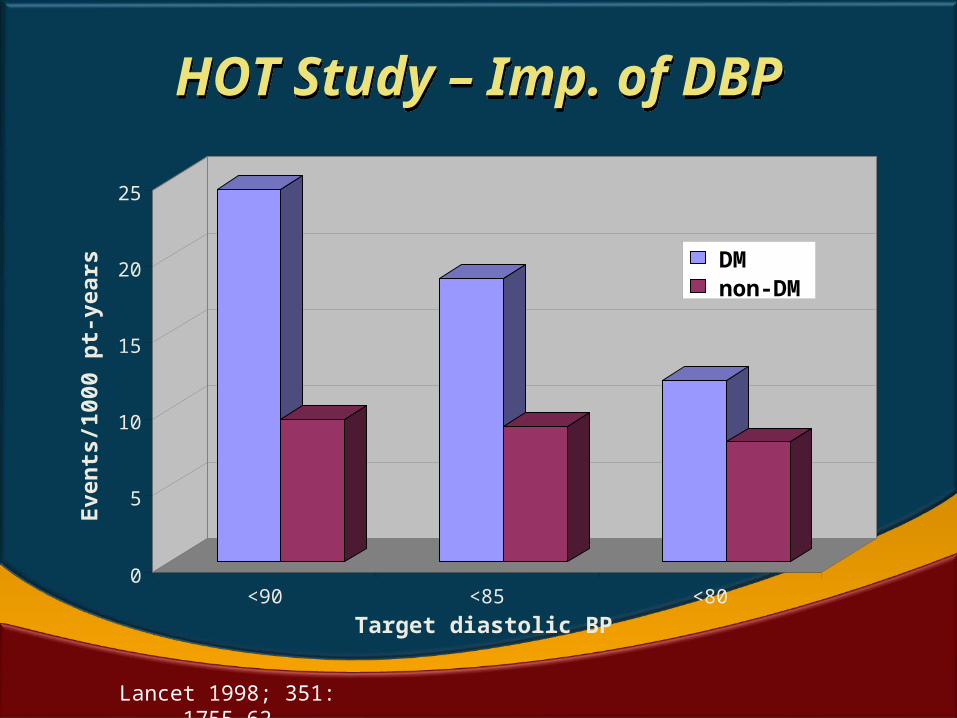
HOT Study – Imp. of DBPHOT Study – Imp. of DBP
0
5
10
15
20
25
Ev
ents
/10
00 p
t-y
ears
<90 <85 <80
Target diastolic BP
DMnon-DM
Lancet 1998; 351: 1755–62
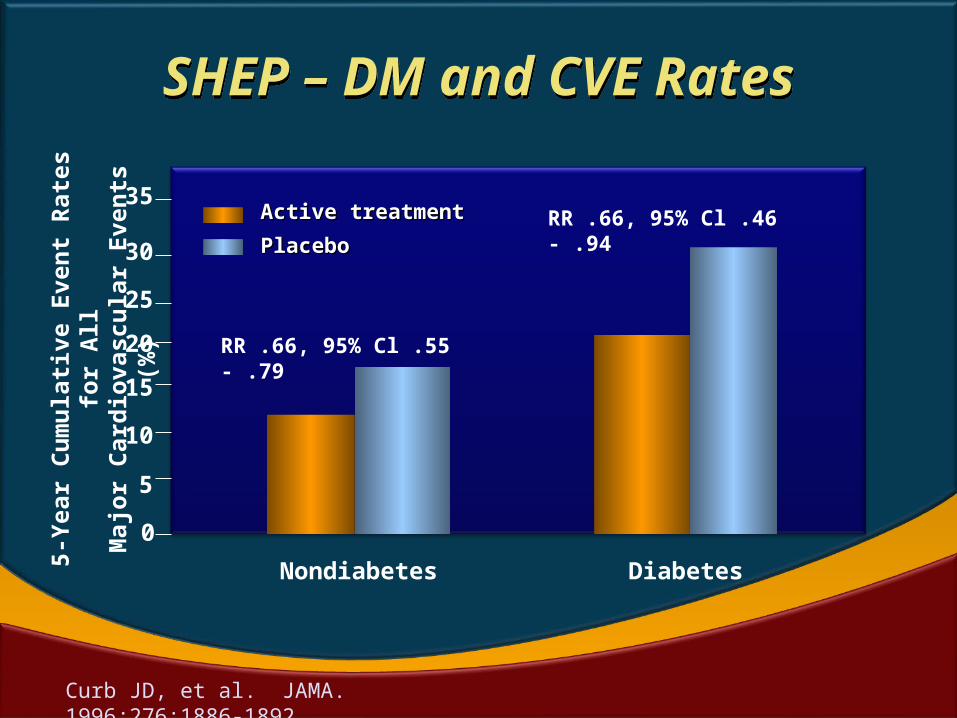
RR .66, 95% Cl .46 - .94
RR .66, 95% Cl .55 - .79
DiabetesNondiabetes
Curb JD, et al. JAMA. 1996;276:1886-1892.
35
15
30
25
20
5
0
10
5-Ye
ar C
umul
ativ
e Ev
ent R
ates
for A
llM
ajor
Car
diov
ascu
lar E
vent
s (%
) Active treatmentActive treatment
PlaceboPlacebo
SHEP – DM and CVE RatesSHEP – DM and CVE Rates
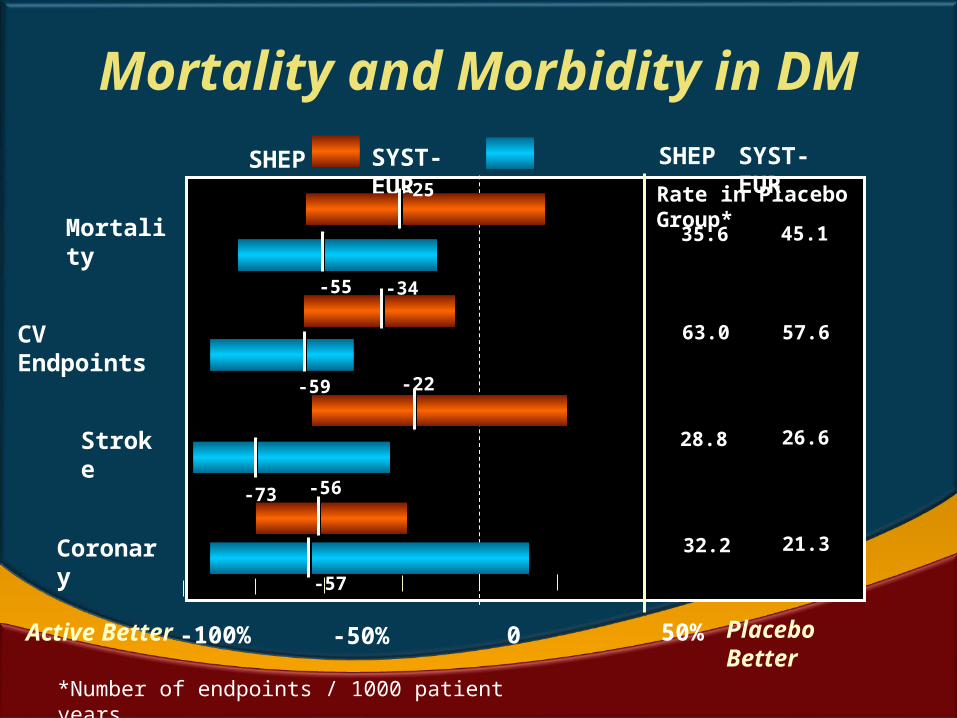
Mortality
CV Endpoints
Stroke
Coronary
Active Better
SHEP SYST-EUR
Rate in Placebo Group*
SHEP SYST-EUR
35.6 45.1
63.0 57.6
28.8 26.6
32.2 21.3
-100% -50% 0 50% Placebo Better
*Number of endpoints / 1000 patient years
-25
-55 -34
-59 -22
-73 -56
-57
Mortality and Morbidity in DM
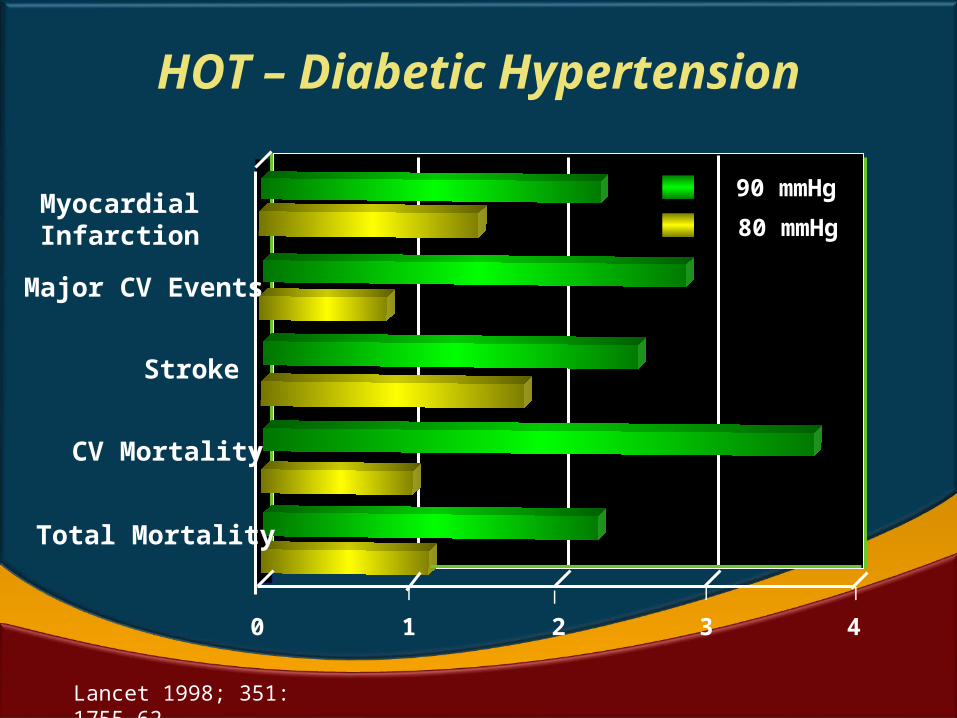
Myocardial Infarction
Major CV Events
Stroke
CV Mortality
Total Mortality
90 mmHg
80 mmHg
0 1 2 3 4
| | | |
HOT – Diabetic Hypertension
Lancet 1998; 351: 1755–62
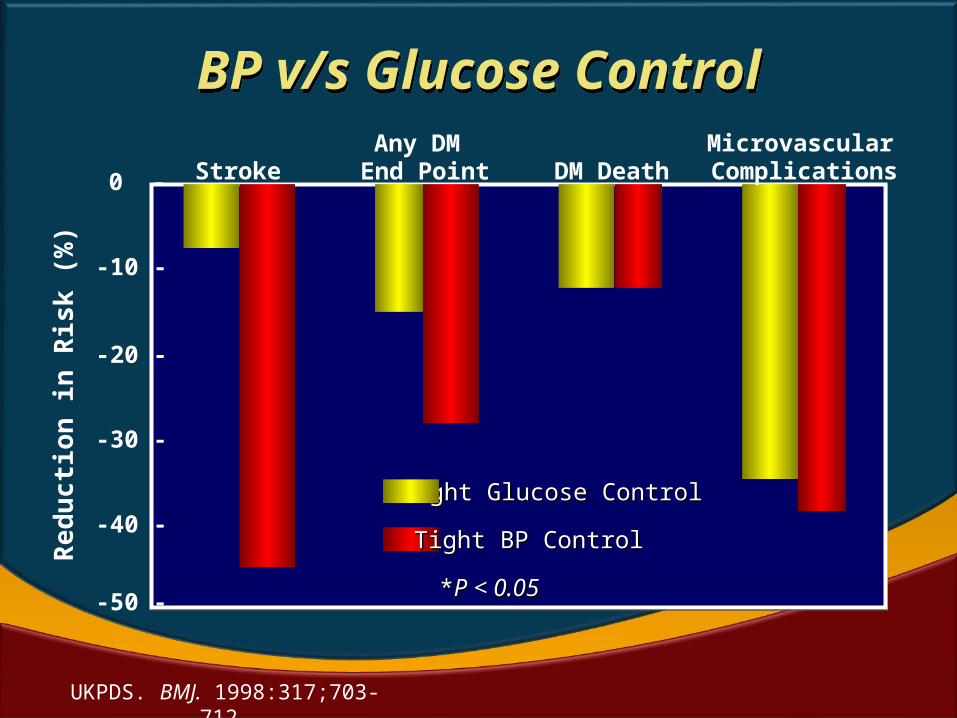
Tight Glucose ControlTight Glucose Control
Tight BP ControlTight BP Control
**P < 0.05P < 0.05-50 -
-40 -
-30 -
0 - StrokeAny DM
End Point DM DeathMicrovascular
Complications
Red
uctio
n in
Ris
k (%
)
UKPDS. BMJ. 1998:317;703-712.
-20 -
-10 -
BP v/s Glucose ControlBP v/s Glucose Control
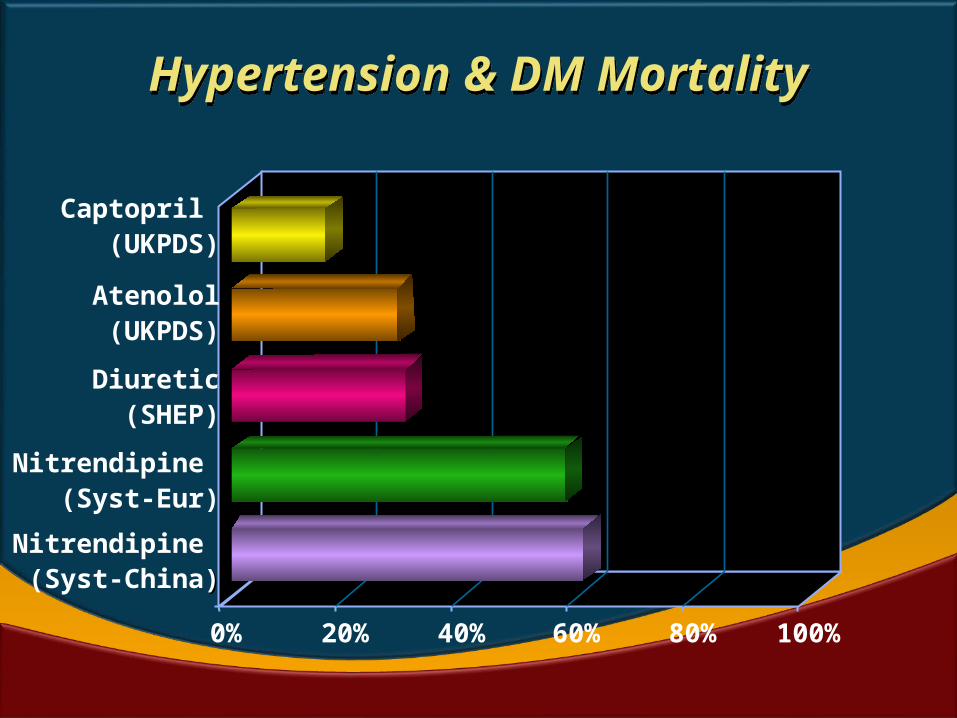
Hypertension & DM MortalityHypertension & DM Mortality
0% 20% 40% 60% 80% 100%
Captopril (UKPDS)
Atenolol
(UKPDS)
Diuretic(SHEP)
Nitrendipine (Syst-Eur)
Nitrendipine (Syst-China))
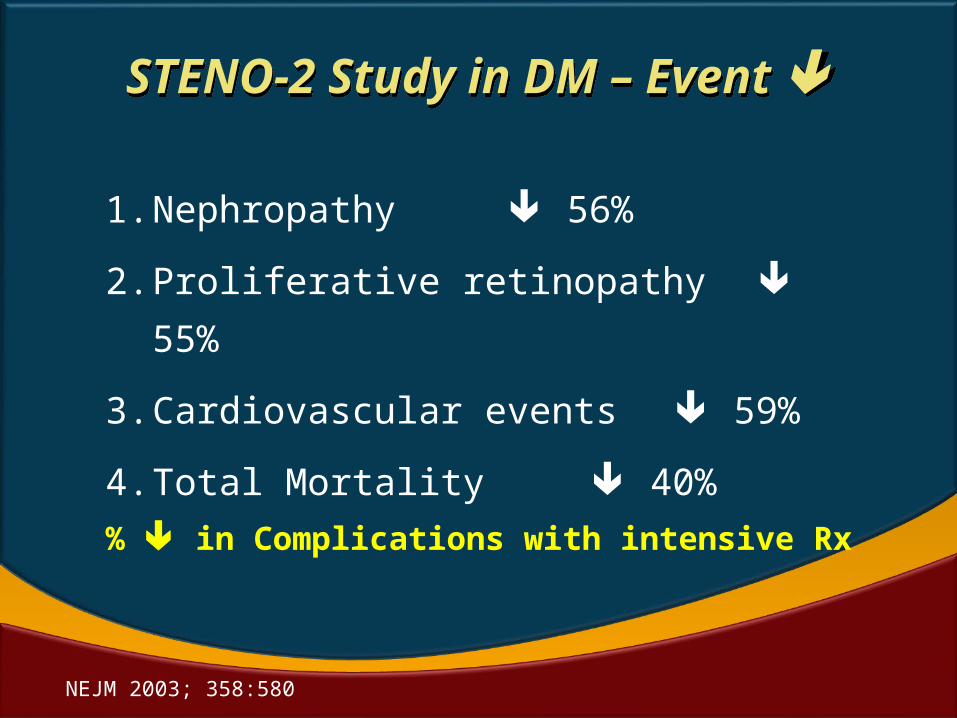
STENO-2 Study in DM – Event
STENO-2 Study in DM – Event
1. Nephropathy 56%
2. Proliferative retinopathy 55%
3. Cardiovascular events 59%
4. Total Mortality 40%
% in Complications with intensive Rx
NEJM 2003; 358:580
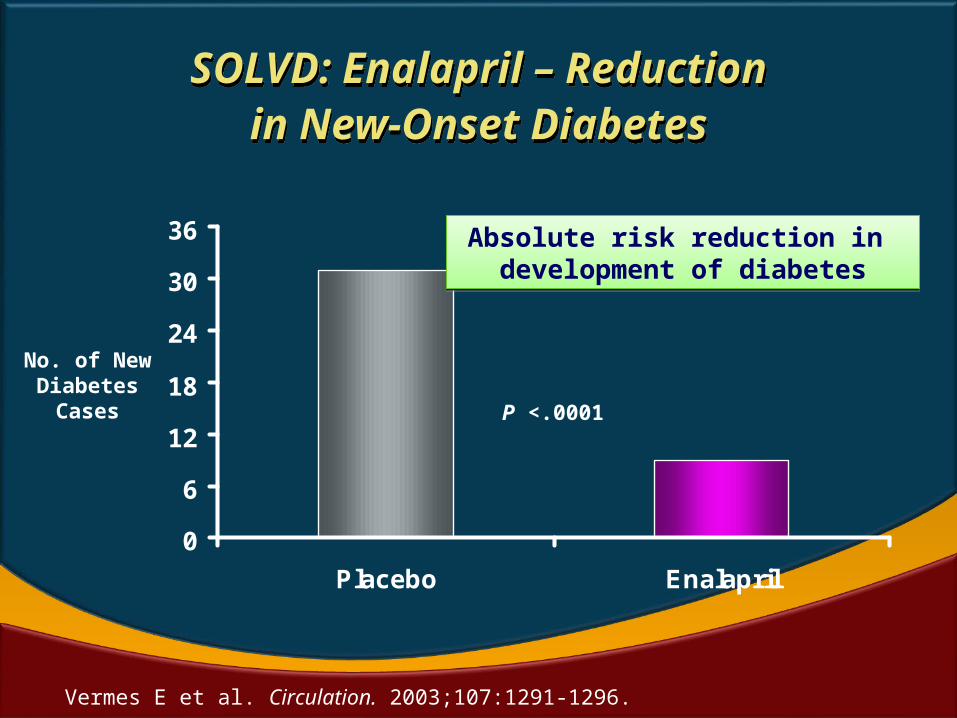
SOLVD: Enalapril – Reductionin New-Onset Diabetes
SOLVD: Enalapril – Reductionin New-Onset Diabetes
0
6
12
18
24
30
36
Placebo Enalapril
P <.0001
Absolute risk reduction in development of diabetes
Absolute risk reduction in development of diabetes
No. of New Diabetes
Cases
Vermes E et al. Circulation. 2003;107:1291-1296.
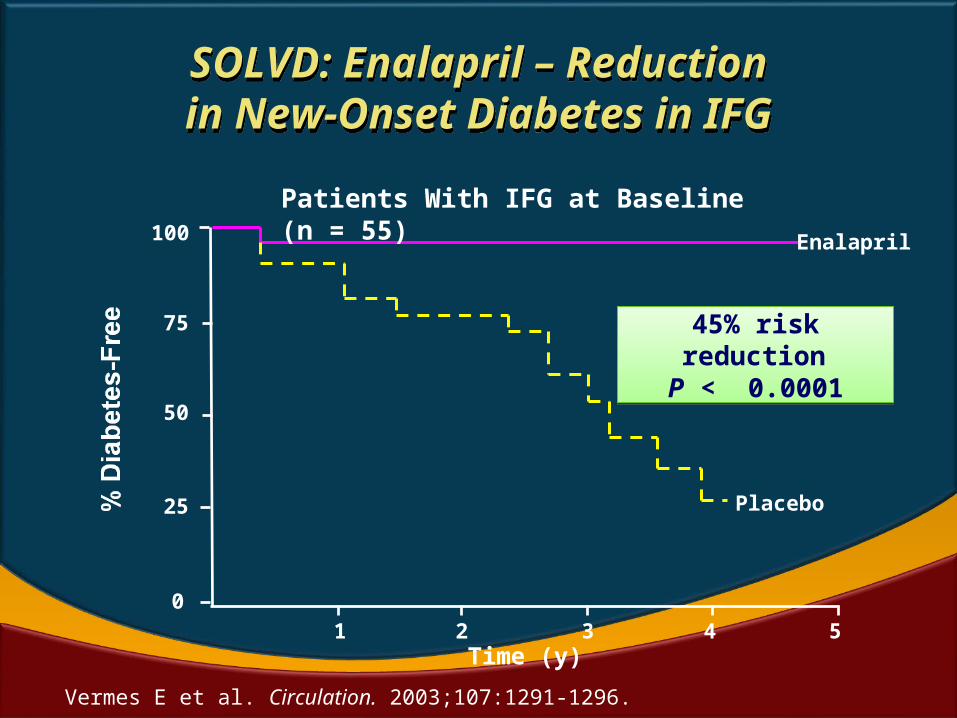
1 2 3 4 5Time (y)
Vermes E et al. Circulation. 2003;107:1291-1296.
25
50
75
100
0
Enalapril
Placebo
45% risk reduction
P < 0.0001
45% risk reduction
P < 0.0001
Patients With IFG at Baseline (n = 55)
SOLVD: Enalapril – Reductionin New-Onset Diabetes in IFGSOLVD: Enalapril – Reductionin New-Onset Diabetes in IFG
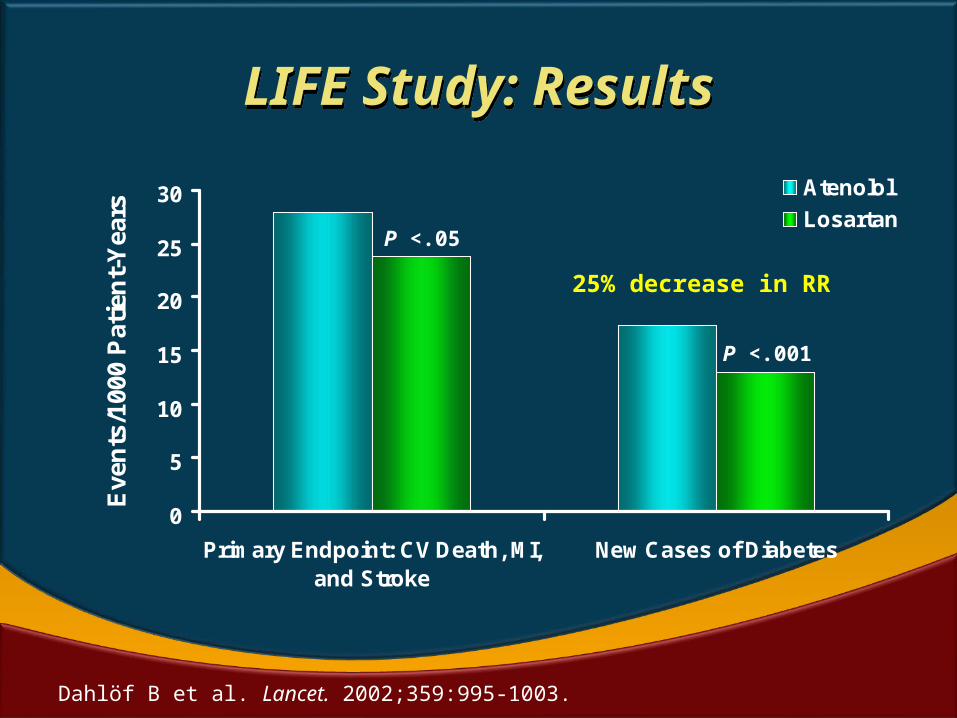
LIFE Study: ResultsLIFE Study: Results
0
5
10
15
20
25
30
Primary Endpoint: CV Death, MI,and Stroke
New Cases of Diabetes
Eve
nts
/100
0 P
atie
nt-
Yea
rs
Atenolol
Losartan
P <.001
P <.05
Dahlöf B et al. Lancet. 2002;359:995-1003.
25% decrease in RR
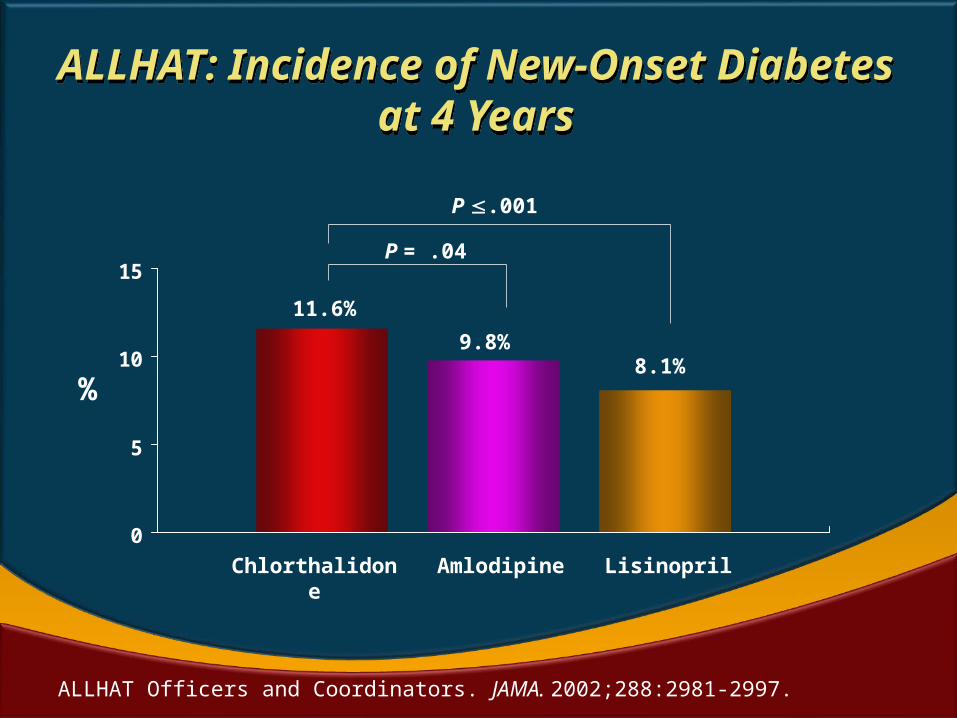
ALLHAT: Incidence of New-Onset Diabetes at 4 Years
ALLHAT: Incidence of New-Onset Diabetes at 4 Years
ALLHAT Officers and Coordinators. JAMA. 2002;288:2981-2997.
0
5
10
15
Chlorthalidone Amlodipine Lisinopril
P .001
P = .04
11.6%
9.8%8.1%
%
THE EVIDENCE BASE
MANAGEMENT GUIDE
THE EVIDENCE BASE
MANAGEMENT GUIDE
Hypertension Dyslipidemia
Dysglycemia
Risk Reduction for CAD and CKD
Risk Reduction for CAD and CKD
Na & K SFA
UFA
CHO GL
Risk Reduction for CAD and CKD
Risk Reduction for CAD and CKD
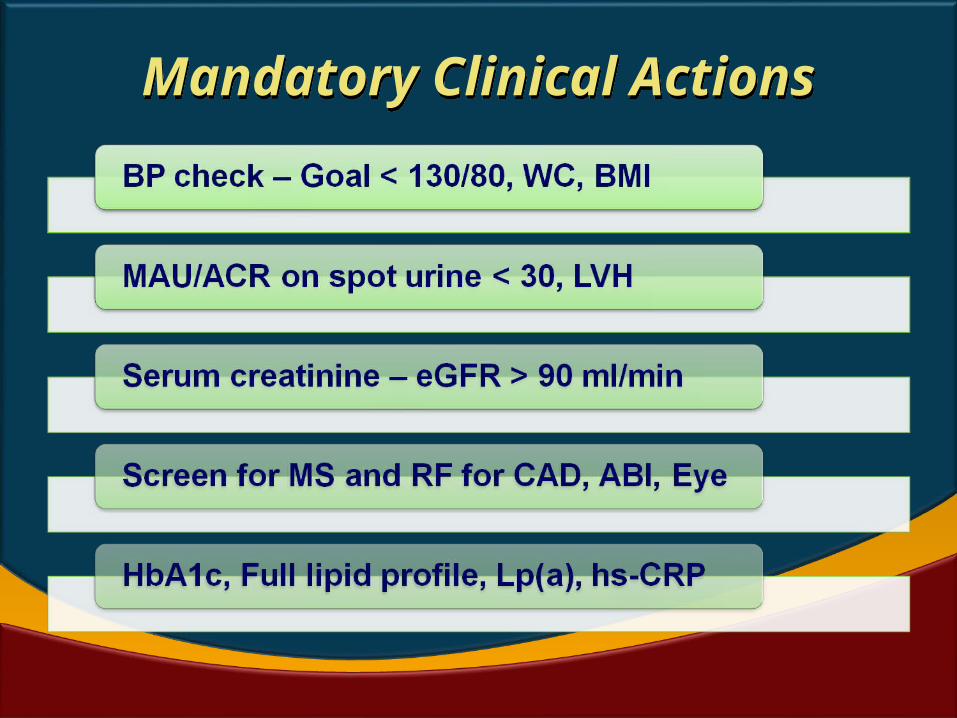
Mandatory Clinical ActionsMandatory Clinical Actions
HTN – Lifestyle modificationsHTN – Lifestyle modifications
• Regular 30’ of moderately intense exercise
• No tobacco and minimizing alcohol
• Na restriction to < 6 g of Nacl per day
• Avoiding high salt foods – pickles, savouries
• Four adult family – 6 x 30 x 4 = 720 g (500 g)
• Use of K containing foods – fruits, vegetables
• Weight reduction – goal ideal weight
• Reducing coffee consumption
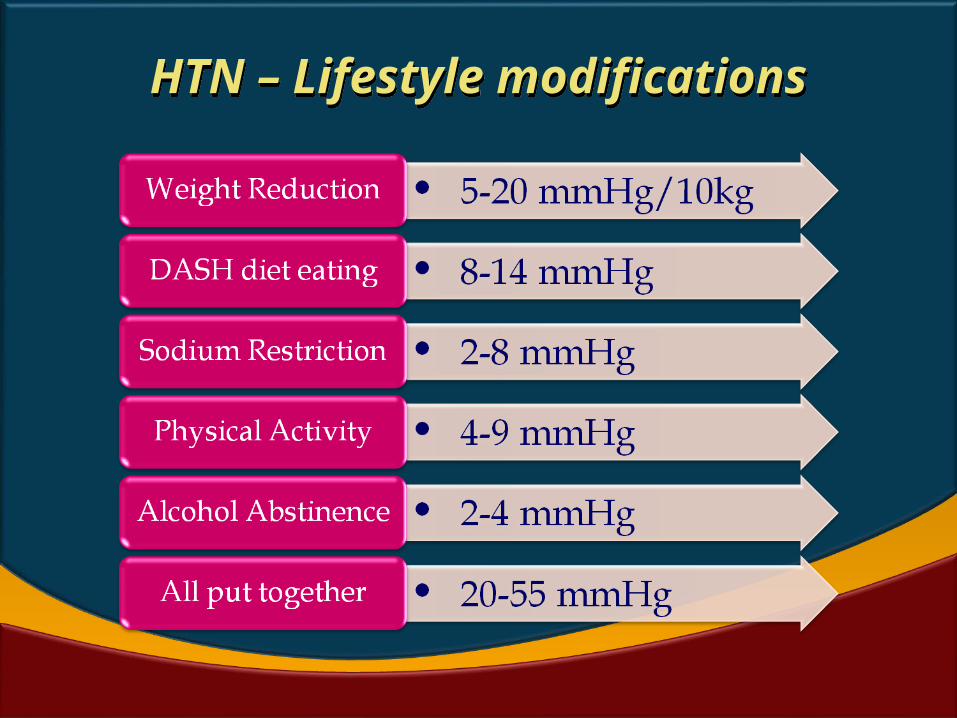
HTN – Lifestyle modificationsHTN – Lifestyle modifications
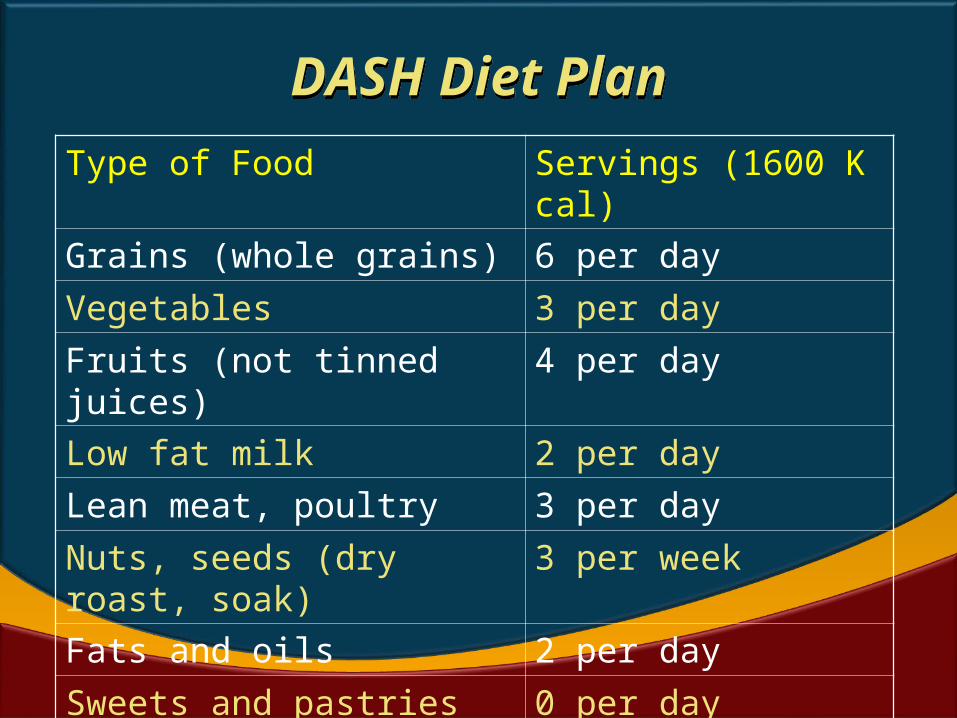
DASH Diet PlanDASH Diet Plan
Type of Food Servings (1600 K cal)
Grains (whole grains) 6 per day
Vegetables 3 per day
Fruits (not tinned juices) 4 per day
Low fat milk 2 per day
Lean meat, poultry 3 per day
Nuts, seeds (dry roast, soak)
3 per week
Fats and oils 2 per day
Sweets and pastries 0 per day
Salt at table & salted foods
None
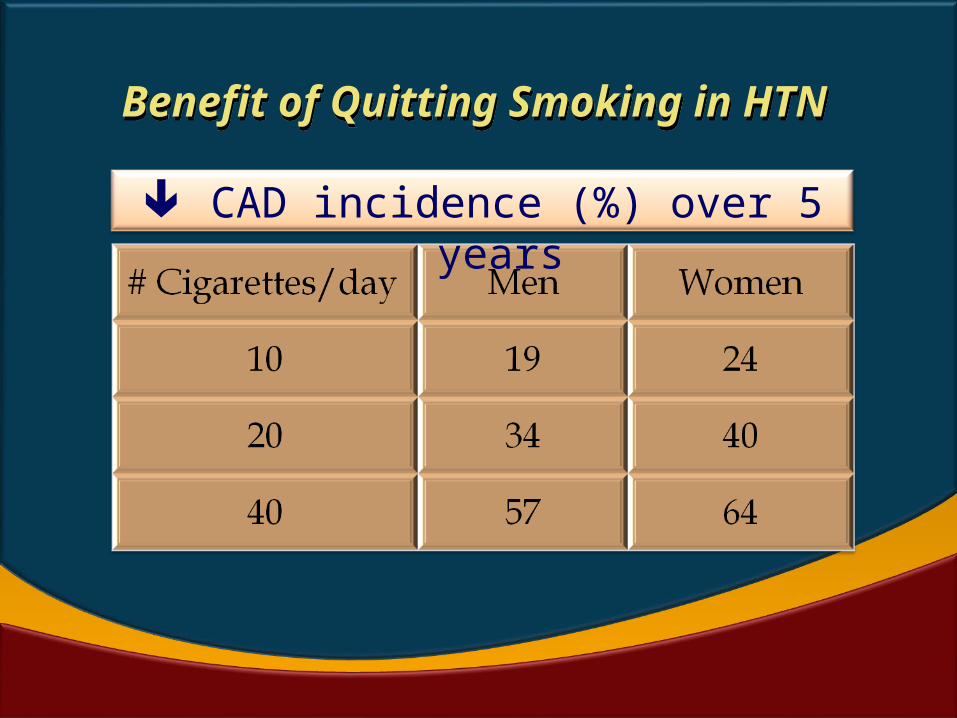
Benefit of Quitting Smoking in HTN
Benefit of Quitting Smoking in HTN
CAD incidence (%) over 5 years
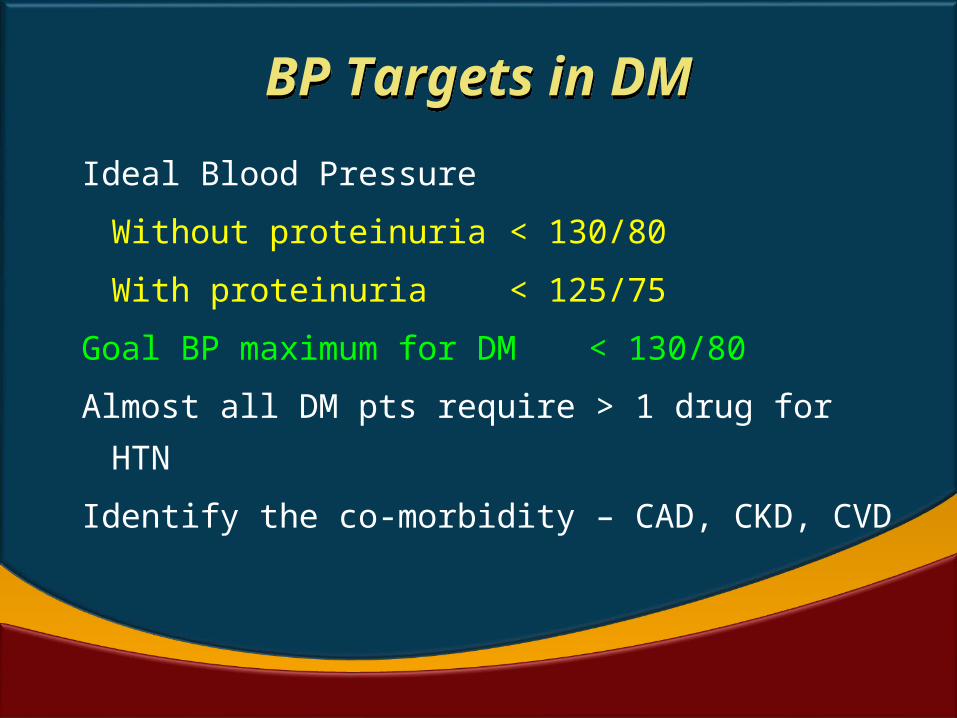
BP Targets in DMBP Targets in DM
Ideal Blood Pressure
Without proteinuria < 130/80
With proteinuria < 125/75
Goal BP maximum for DM < 130/80
Almost all DM pts require > 1 drug for HTN
Identify the co-morbidity – CAD, CKD, CVD
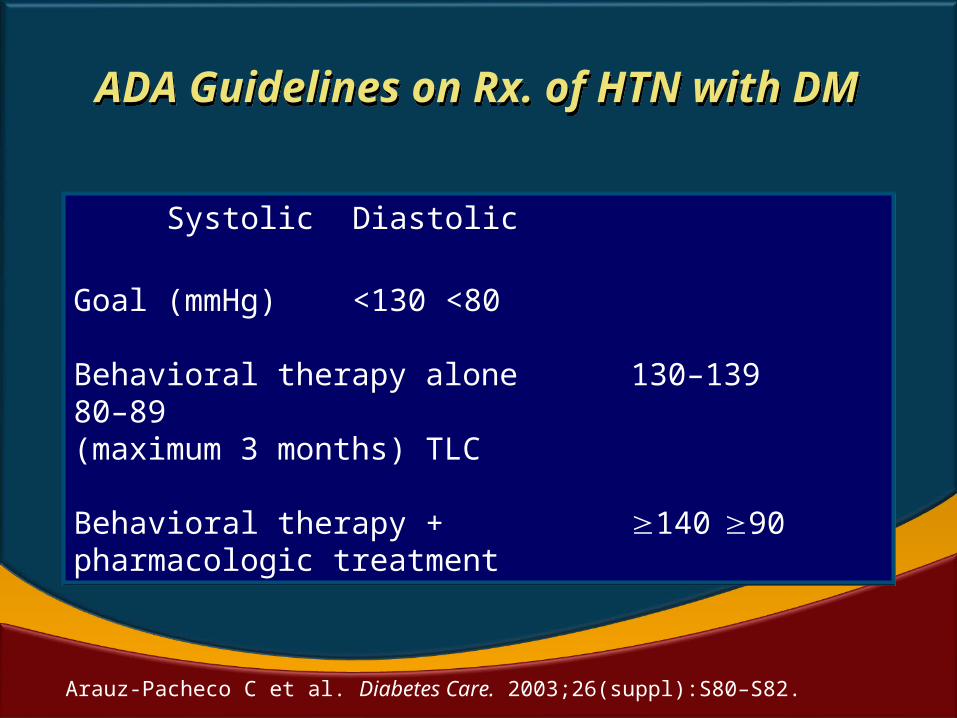
ADA Guidelines on Rx. of HTN with DM
ADA Guidelines on Rx. of HTN with DM
Systolic Diastolic
Goal (mmHg) <130 <80
Behavioral therapy alone 130–139 80–89(maximum 3 months) TLC
Behavioral therapy + 140 90pharmacologic treatment
Systolic Diastolic
Goal (mmHg) <130 <80
Behavioral therapy alone 130–139 80–89(maximum 3 months) TLC
Behavioral therapy + 140 90pharmacologic treatment
Arauz-Pacheco C et al. Diabetes Care. 2003;26(suppl):S80–S82.
THE EVIDENCE BASE FOR
MANAGEMENT OPTIONS
THE EVIDENCE BASE FOR
MANAGEMENT OPTIONS
Management OptionsManagement Options
Diuretics
NDHP - CCBs
MNT
ExerciseNew BB
ACEi, ARB
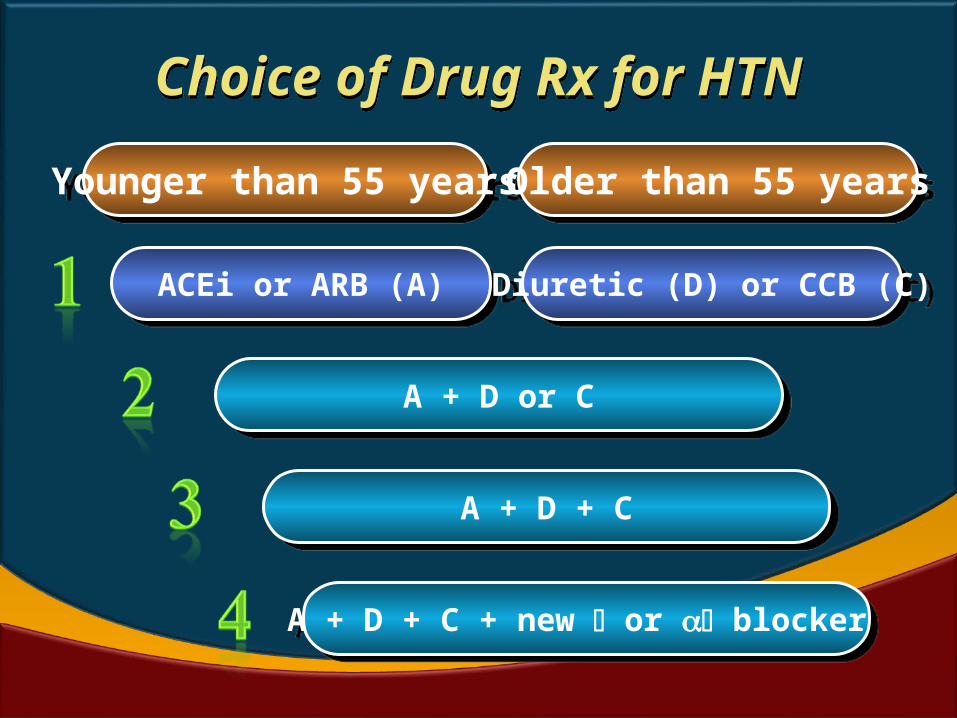
Choice of Drug Rx for HTNChoice of Drug Rx for HTN
Younger than 55 yearsYounger than 55 years Older than 55 yearsOlder than 55 years
ACEi or ARB (A)ACEi or ARB (A) Diuretic (D) or CCB (C)Diuretic (D) or CCB (C)
A + D or CA + D or C
A + D + CA + D + C
A + D + C + new or blocker A + D + C + new or blocker
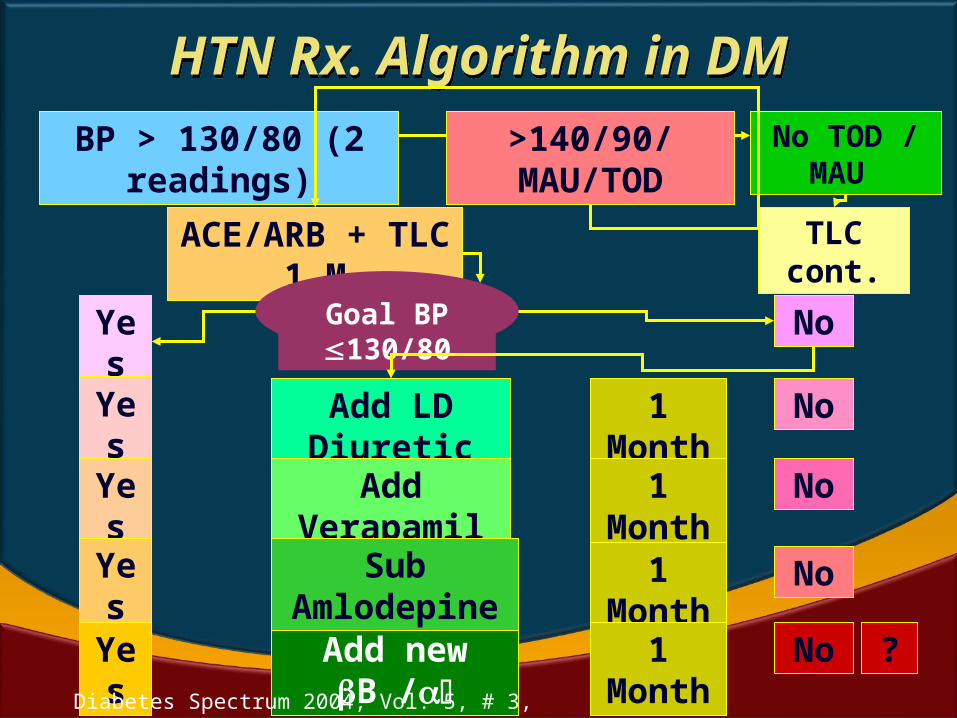
HTN Rx. Algorithm in DMHTN Rx. Algorithm in DMBP > 130/80 (2 readings) No TOD / MAU
ACE/ARB + TLC 1 M
Goal BP 130/80Yes No
Add LD Diuretic
Add Verapamil
Add new B /
Yes
Yes
No
TLC cont.
>140/90/MAU/TOD
1 Month
Sub Amlodepine
No
No
No
Yes
Yes
1 Month
1 Month
1 Month ?Diabetes Spectrum 2004, Vol. 5, # 3, 103-108
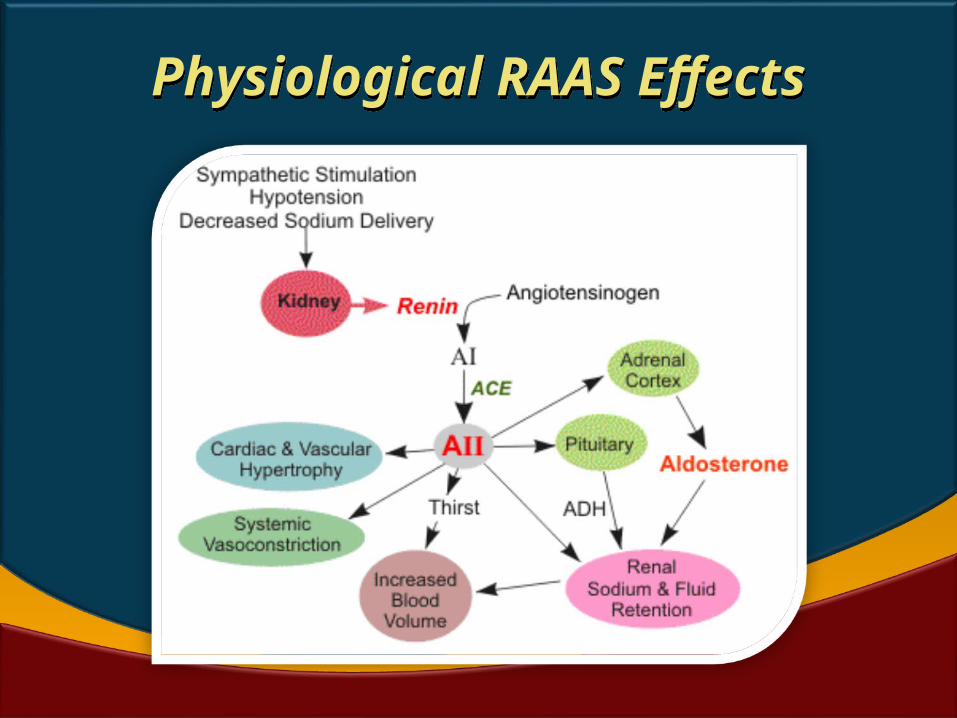
Physiological RAAS EffectsPhysiological RAAS Effects
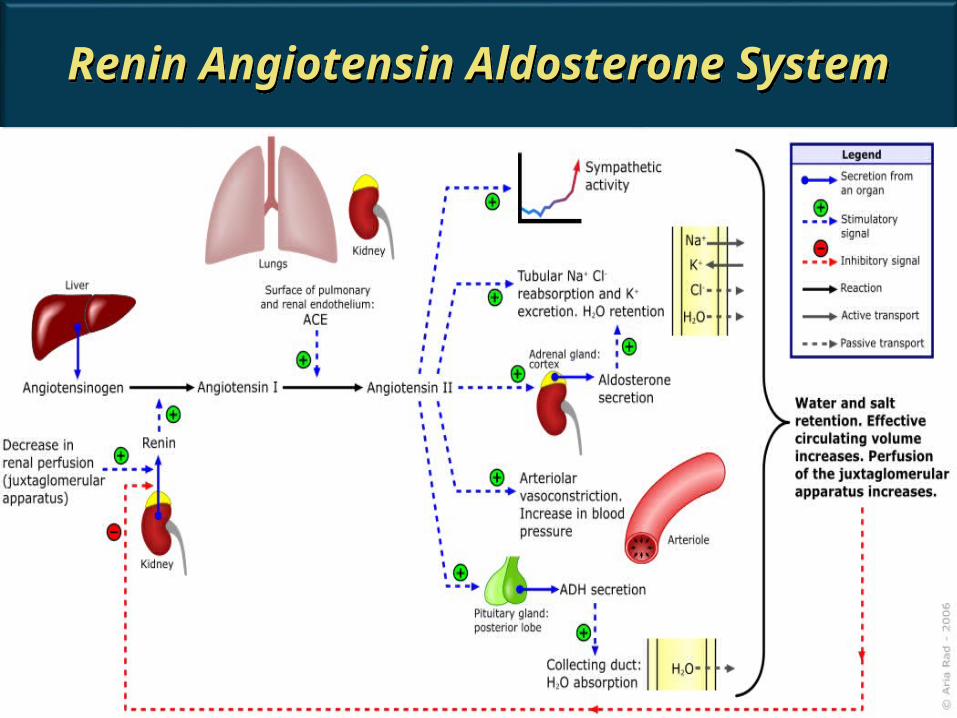
Renin Angiotensin Aldosterone System
Renin Angiotensin Aldosterone System
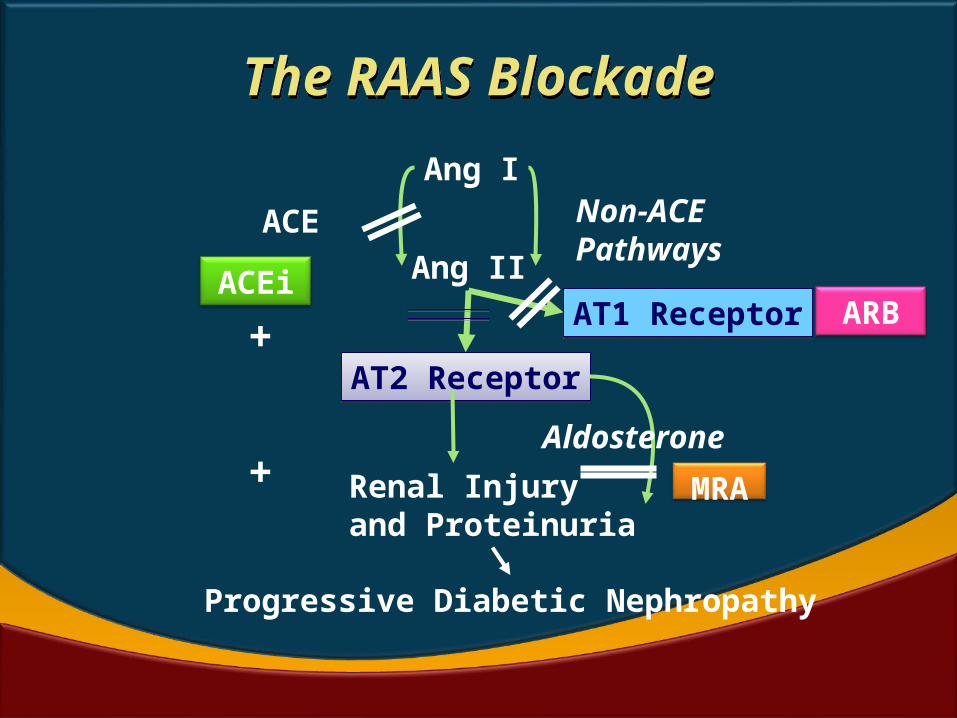
The RAAS BlockadeThe RAAS Blockade
Ang I
Ang II
Progressive Diabetic Nephropathy
ACE
Renal Injury and Proteinuria
ACEi
AT2 ReceptorAT2 Receptor
Non-ACEPathways
Aldosterone
MRA
AT1 ReceptorAT1 Receptor+
+
ARB
Adverse Renal and CVEffects of AldosteroneAdverse Renal and CVEffects of Aldosterone
•Glomerulosclerosis•Interstitial Fibrosis•Proteinuria•Renal Failure
•LVH•Cardiac Fibrosis•LV Dysfunction•Heart Failure
•Endothelial
Dysfunction•Inflammation•Oxidative Stress
Aldosterone
MRA – EplerenoneBrand name: Eplirestat
ACEi or ARB – A must for VPACEi or ARB – A must for VP
• Antihypertensive, vasoprotective,
anti-thrombotic and anti-inflammatory
• Inevitable in DM more so in DM + HT/CVD
• Reduce CV events, Reduce atherosclerosis
• Reduce renal disease - a strong CV risk factor
• Metabolically ‘friendly’ drugs in DM
• They prevent new onset DM, Nephropathy
• Well-tolerated with few side effects
ACE inhibitor or ARBACE inhibitor or ARB
• Renal impairment – These improve
e-GFR, microalbuminuria or proteinuria
• LV dysfunction (along with new blocker)
• Previous MI (along with new blocker)
• Contraindicated in pregnancy
• Relative contraindications
- Bilateral renal artery stenosis
- Severe renal impairment (Cr > 3.0)
- Monitor renal function
- Angioedema, ACEi cough
Vascular Protection in DMVascular Protection in DM
1. Atorvastatin (Lipid management)2. ASA (Acetyl Salicylic Acid) – (enteric
coated)3. ACE inhibitors or ARBs4. A1c control (Glycemic control)5. Blood pressure goal (<130/80)6. Control of Nephropathy, Proteinuria
(MAU)7. Cigarette smoking cessation8. Weight and waist management9. Physical Activity – at least 2 km/d x 5 d
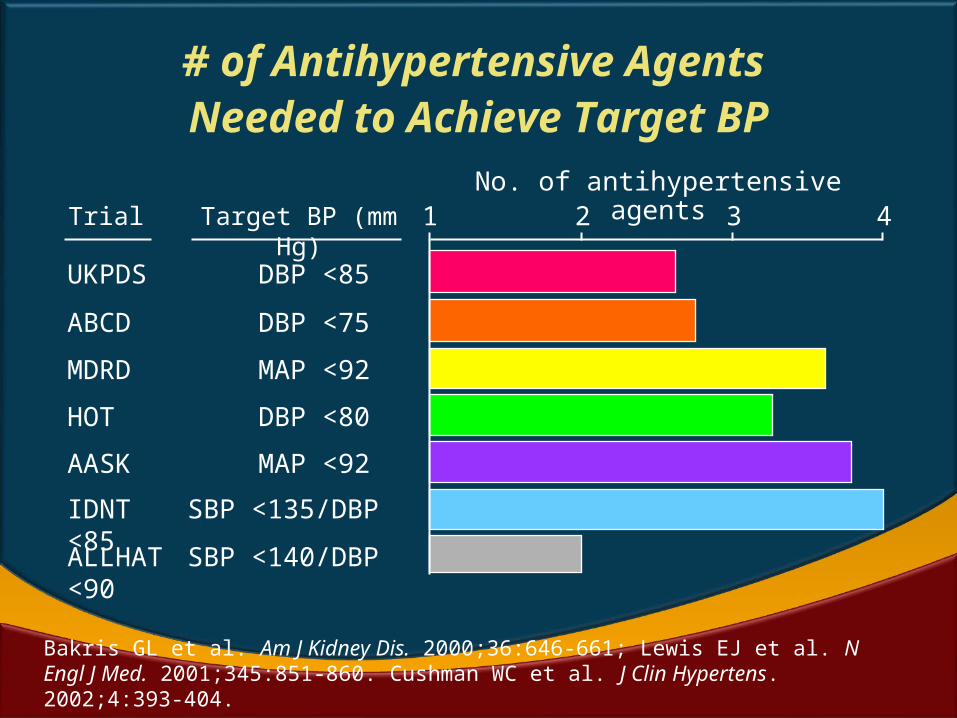
AASK MAP <92
Target BP (mm Hg)
# of Antihypertensive Agents Needed to Achieve Target BP
No. of antihypertensive agents1
UKPDS DBP <85
ABCD DBP <75
MDRD MAP <92
HOT DBP <80
Trial 2 3 4
Bakris GL et al. Am J Kidney Dis. 2000;36:646-661; Lewis EJ et al. N Engl J Med. 2001;345:851-860. Cushman WC et al. J Clin Hypertens. 2002;4:393-404.
IDNT SBP <135/DBP <85
ALLHAT SBP <140/DBP <90
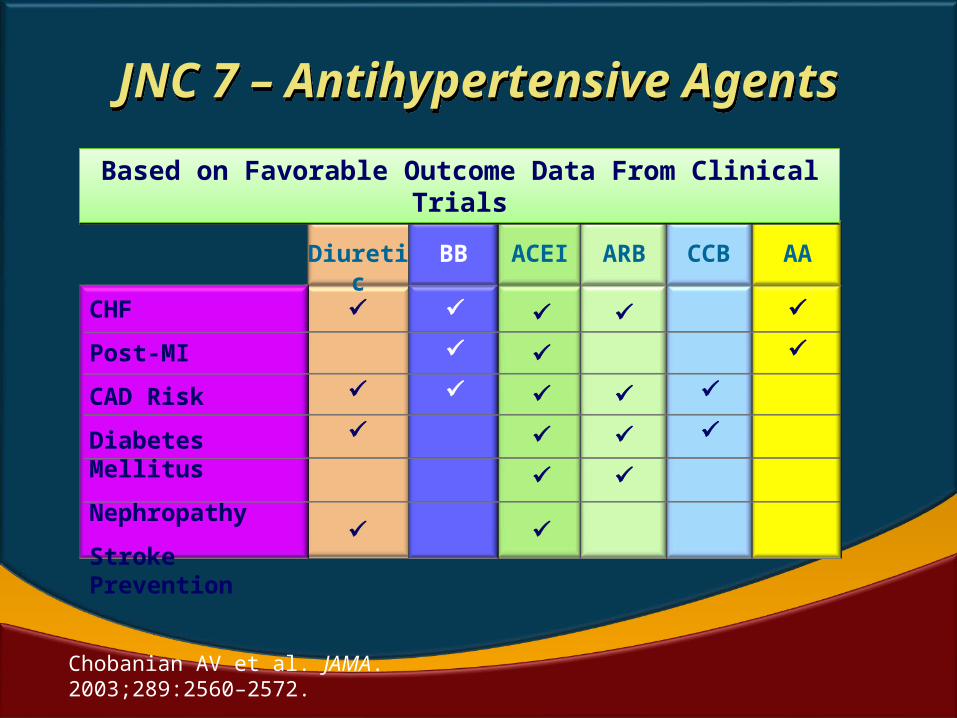
Chobanian AV et al. JAMA. 2003;289:2560–2572.
CHF
Post-MI
CAD Risk
Diabetes Mellitus
Nephropathy
Stroke Prevention
BB
ACEI
ARB
CCB
AADiuretic
JNC 7 – Antihypertensive Agents
JNC 7 – Antihypertensive Agents
Based on Favorable Outcome Data From Clinical Trials
Based on Favorable Outcome Data From Clinical Trials
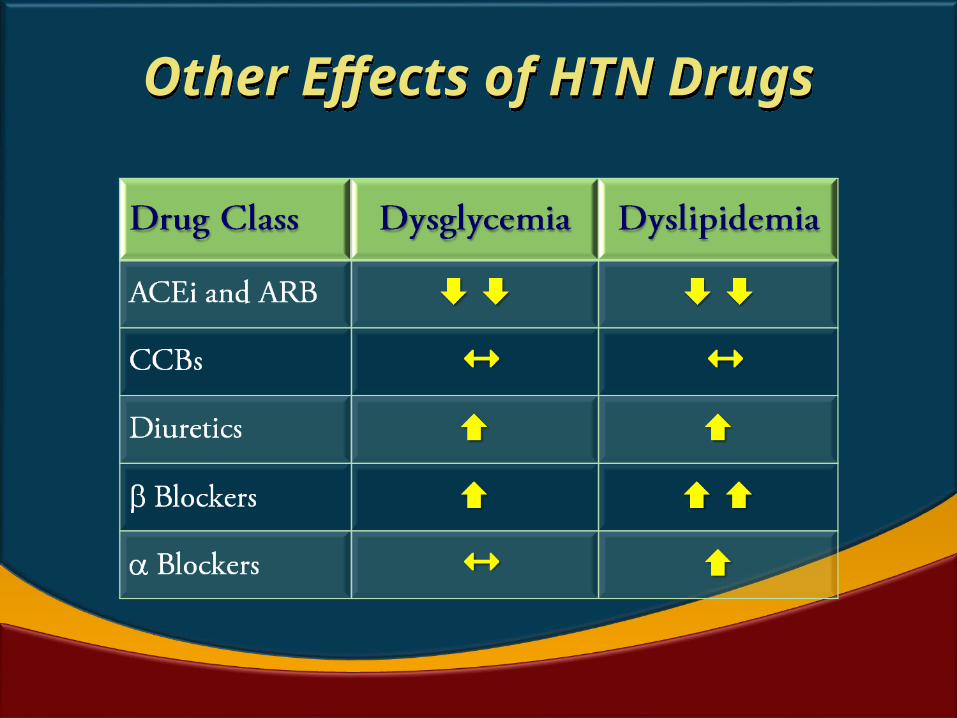
Other Effects of HTN DrugsOther Effects of HTN Drugs
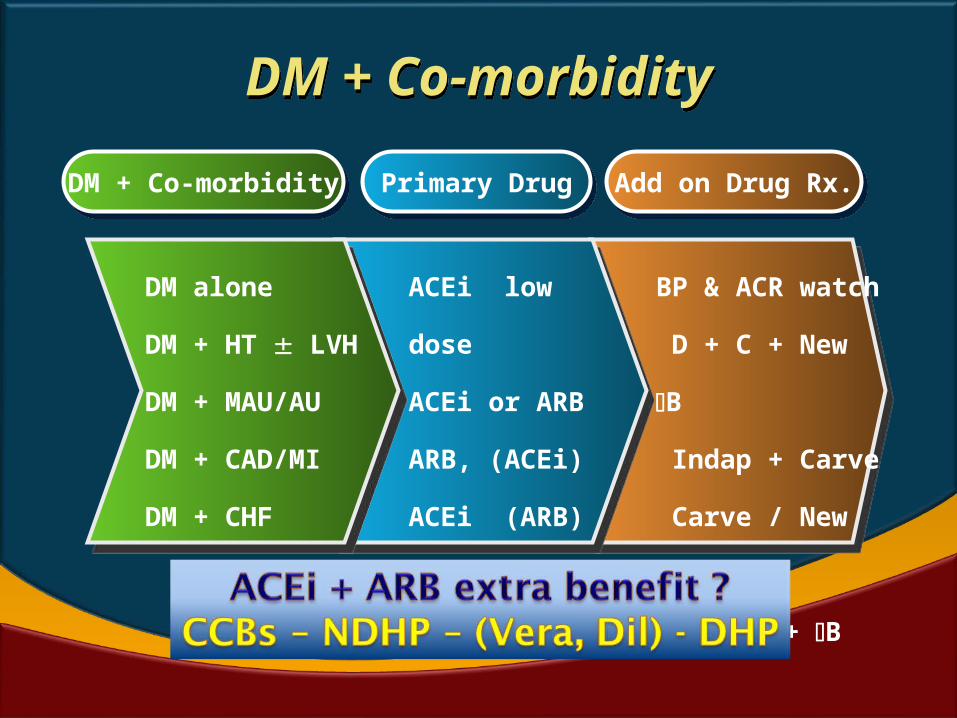
DM + Co-morbidityDM + Co-morbidity
DM + Co-morbidityDM + Co-morbidity Primary DrugPrimary Drug Add on Drug Rx.Add on Drug Rx.
DM alone
DM + HT
LVH
DM + MAU/AU
DM + CAD/MI
DM + CHF
ACEi low dose
ACEi or ARB
ARB, (ACEi)
ACEi (ARB)
ACEi or ARB
BP & ACR
watch
D + C + New
B
Indap + Carve
Carve / New B
D + AA + B
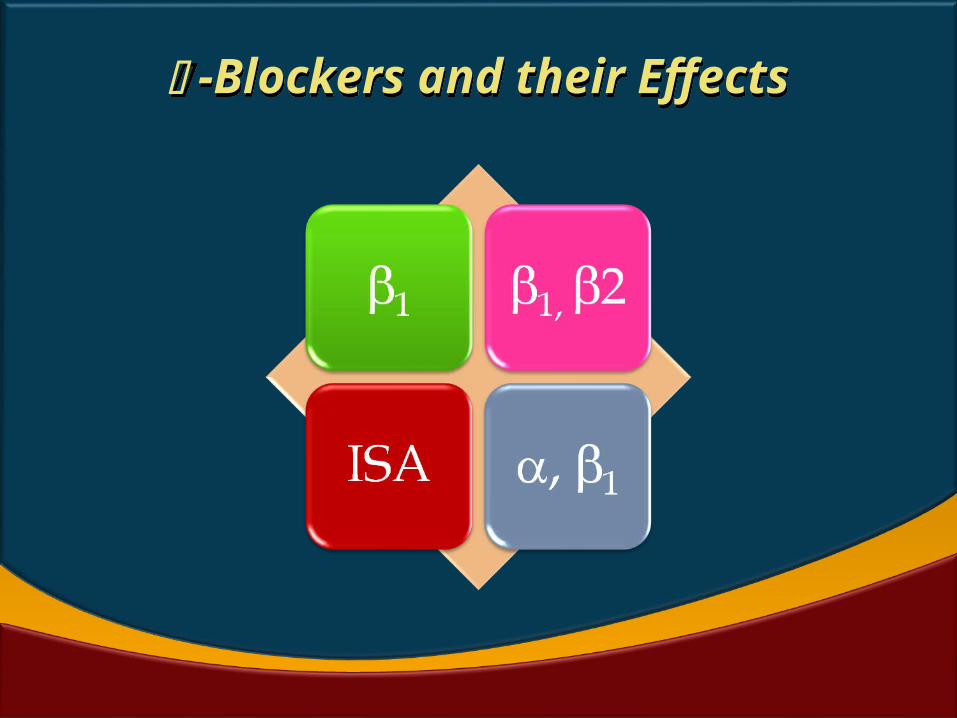
-Blockers and their Effects -Blockers and their Effects
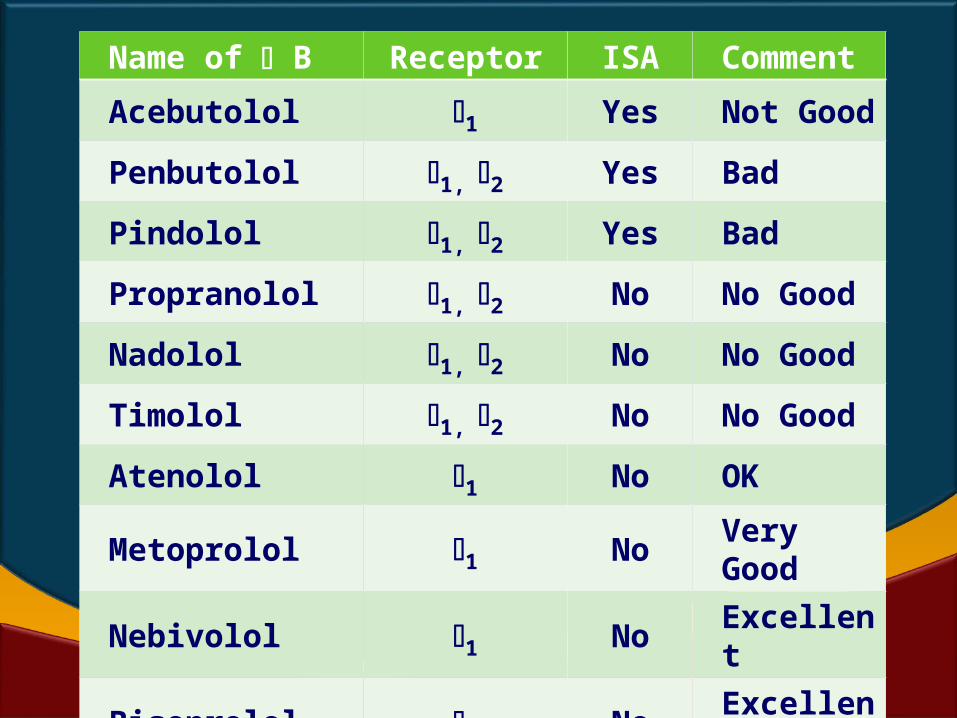
Name of B Receptor ISA Comment
Acebutolol 1 Yes Not Good
Penbutolol 1, 2 Yes Bad
Pindolol 1, 2 Yes Bad
Propranolol 1, 2 No No Good
Nadolol 1, 2 No No Good
Timolol 1, 2 No No Good
Atenolol 1 No OK
Metoprolol 1 No Very Good
Nebivolol 1 No Excellent
Bisoprolol 1 No Excellent
Labetalol , 1, 2 No Emergency
Carvedilol , 1, 2 No CHF, IHD
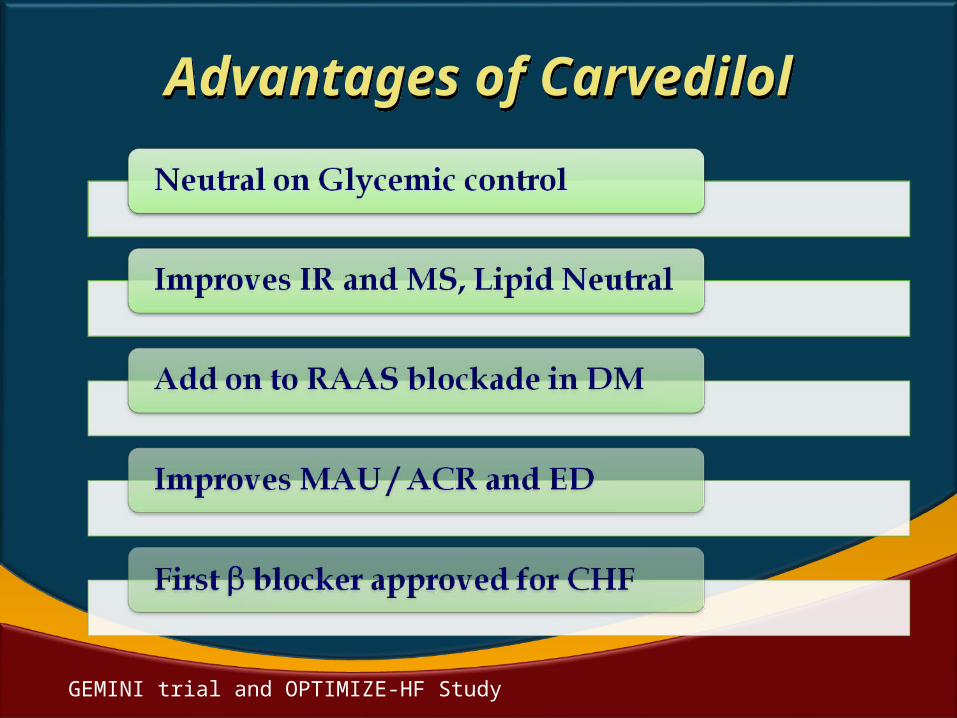
Advantages of CarvedilolAdvantages of Carvedilol
GEMINI trial and OPTIMIZE-HF Study
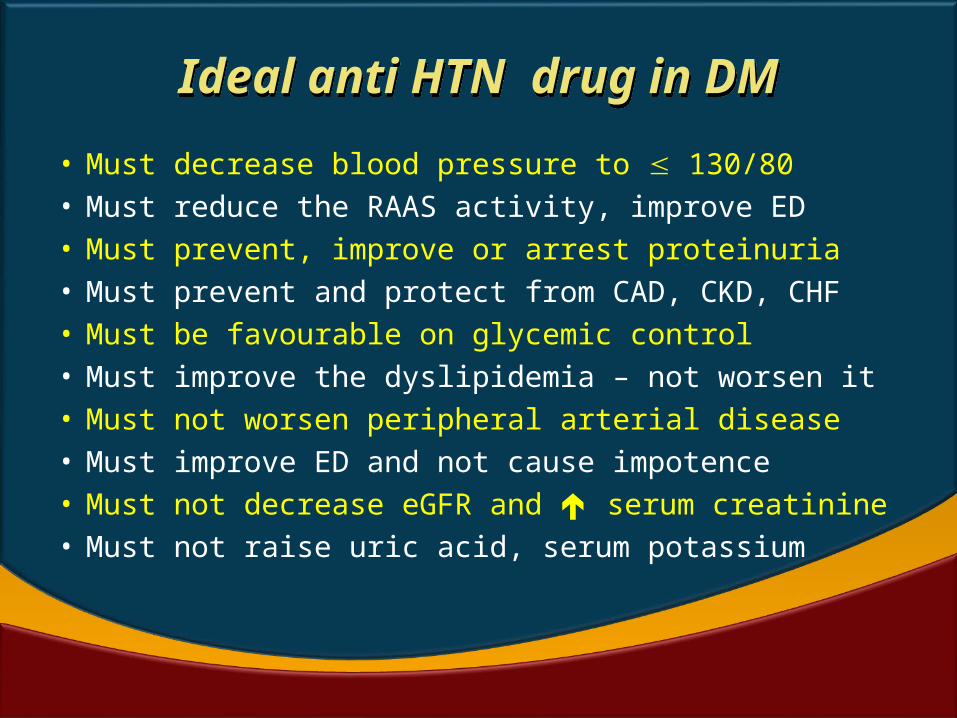
Ideal anti HTN drug in DMIdeal anti HTN drug in DM
• Must decrease blood pressure to 130/80• Must reduce the RAAS activity, improve ED • Must prevent, improve or arrest proteinuria• Must prevent and protect from CAD, CKD, CHF• Must be favourable on glycemic control• Must improve the dyslipidemia – not worsen it• Must not worsen peripheral arterial disease• Must improve ED and not cause impotence• Must not decrease eGFR and serum
creatinine• Must not raise uric acid, serum potassium
What should We take home ?
What should We take home ?
‘Clinician Inertia’ for HTN in DM must be overcome
HTN in DM is serious; So manage aggressively
TLC, Lipid control, Glycemic targets – VP is a must
HTN Rx. delays or arrests CVD, CKD, PAD, CVD
ACEi or ARBs are the main stay of Rx - RAAS
Postural hypotension, DAN are important in Rx
MAU/ACR must for all DM – Predict CAD, CKD
Typically 2 or more drugs are needed for HTN Rx.
New B, Carvedilol, CCBs are add-on drugs
Amaedhya poornam, krimi raasi
samkulam,
Swaabhava gandham, asaucham,
adhruvam |
Sareeram, mootra pureesha bhaajanam
Ramanti moodha, viramanti pandithaa |
Full of filth, ridden with all bacteria and worms,
Naturally stinking, unclean to the core & perishable,
This body of ours, is drenched in excreta & secreta,
Only the fools engross in it, but the wise shun it. VC by ASA