Embed Size (px)
Citation preview

1
MANAGING MANAGING MEDICAREMEDICARE
California Society of Pathologists San
Francisco California December 4 2009
2
WE WILL DISCUSSWE WILL DISCUSSbull National and Local Lab Policiesbull Requesting Reconsiderationsbull Referral Rulesbull Enrollment PECOS
ndash Revalidationndash Reporting any Changes
bull HIGLASSmdashDecember Payment Changesbull On-Line Viewing of Claimsmdashsoon a realitybull Signature Rulesbull Coverage for New Lab Tests
ndash National Versus Local Coveragendash Meet with CMDs amp Othersndash Thoughts on Pricing amp Codingndash Time Factors for Decisions
bull Some 2010 Reimbursement Changesbull Questions and answers
3
NATIONAL COVERAGE DECISIONS
bull National NCDs come from CMSNational NCDs come from CMSndash Based on scientific studies amp data collectedBased on scientific studies amp data collectedndash Presented often at MCAC-open meetingsPresented often at MCAC-open meetingsndash Notice and comment welcomeNotice and comment welcomendash Reconsiderations always possibleReconsiderations always possible
bull NCDs cover entire countryNCDs cover entire countryndash May specify services May specify services alwaysalways covered covered ndash May specify services May specify services nevernever covered coveredndash Published in CMS Coverage ManualPublished in CMS Coverage Manualndash May change as science changes new May change as science changes new
studies emerge or as laws changestudies emerge or as laws change
ndash Reconsiderations always possible
4
NATIONAL COVERAGE DECISIONS
bull Examples of NCDs (over 300 currently)Examples of NCDs (over 300 currently)ndash Alpha-fetoproteinAlpha-fetoproteinndash Collagen crosslinks any methodCollagen crosslinks any methodndash Cytogenic studiesCytogenic studiesndash Digoxin therapeutic drug assayDigoxin therapeutic drug assayndash Fecal occult blood testingFecal occult blood testingndash Genetic testing for warfarin Genetic testing for warfarin ndash HIV testingHIV testingndash Prostate cancer screening testsProstate cancer screening testsndash Sweat testSweat test
bull National Laboratory Coverage Determinations National Laboratory Coverage Determinations (23 currently)(23 currently)
5
LOCAL COVERAGE DECISIONS
bull Local LCDs from 1 or more statesareasLocal LCDs from 1 or more statesareasndash Written by local CMDs about situations that are Written by local CMDs about situations that are
data based amp need control or instructiondata based amp need control or instructionndash Presented at state CACs open to medical and Presented at state CACs open to medical and
specialty societies representativesspecialty societies representativesndash Notice and comment always welcome Notice and comment always welcome ndash Reconsiderations always possibleReconsiderations always possible
bull LCDs cover a Medicare Jurisdiction (eg J-1)LCDs cover a Medicare Jurisdiction (eg J-1)ndash Discuss and describe medical necessityDiscuss and describe medical necessityndash Usually give codes amp conditions for paymentUsually give codes amp conditions for paymentndash May state frequency of service and diagnoses May state frequency of service and diagnoses
and always published locally and nationallyand always published locally and nationally
ndash Reconsiderations always possible
6
LOCAL COVERAGE DECISIONS
bull Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)ndash Category III codes ndash temporary or trackingCategory III codes ndash temporary or trackingndash Cytogenic studiesCytogenic studiesndash Free PSAFree PSAndash MammaprintMammaprintndash Oncologic in-vitro chemoresponse assaysOncologic in-vitro chemoresponse assaysndash Oncotype DX Oncotype DX ndash Flow cytometry and immunohistochemistry Flow cytometry and immunohistochemistry
(article) ndash soon to be policy(article) ndash soon to be policybull Some Part A LCDs may also applySome Part A LCDs may also applybull Local articles may also specify lab use or Local articles may also specify lab use or
instruct in billingcodinginstruct in billingcoding
7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
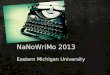
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

2
WE WILL DISCUSSWE WILL DISCUSSbull National and Local Lab Policiesbull Requesting Reconsiderationsbull Referral Rulesbull Enrollment PECOS
ndash Revalidationndash Reporting any Changes
bull HIGLASSmdashDecember Payment Changesbull On-Line Viewing of Claimsmdashsoon a realitybull Signature Rulesbull Coverage for New Lab Tests
ndash National Versus Local Coveragendash Meet with CMDs amp Othersndash Thoughts on Pricing amp Codingndash Time Factors for Decisions
bull Some 2010 Reimbursement Changesbull Questions and answers
3
NATIONAL COVERAGE DECISIONS
bull National NCDs come from CMSNational NCDs come from CMSndash Based on scientific studies amp data collectedBased on scientific studies amp data collectedndash Presented often at MCAC-open meetingsPresented often at MCAC-open meetingsndash Notice and comment welcomeNotice and comment welcomendash Reconsiderations always possibleReconsiderations always possible
bull NCDs cover entire countryNCDs cover entire countryndash May specify services May specify services alwaysalways covered covered ndash May specify services May specify services nevernever covered coveredndash Published in CMS Coverage ManualPublished in CMS Coverage Manualndash May change as science changes new May change as science changes new
studies emerge or as laws changestudies emerge or as laws change
ndash Reconsiderations always possible
4
NATIONAL COVERAGE DECISIONS
bull Examples of NCDs (over 300 currently)Examples of NCDs (over 300 currently)ndash Alpha-fetoproteinAlpha-fetoproteinndash Collagen crosslinks any methodCollagen crosslinks any methodndash Cytogenic studiesCytogenic studiesndash Digoxin therapeutic drug assayDigoxin therapeutic drug assayndash Fecal occult blood testingFecal occult blood testingndash Genetic testing for warfarin Genetic testing for warfarin ndash HIV testingHIV testingndash Prostate cancer screening testsProstate cancer screening testsndash Sweat testSweat test
bull National Laboratory Coverage Determinations National Laboratory Coverage Determinations (23 currently)(23 currently)
5
LOCAL COVERAGE DECISIONS
bull Local LCDs from 1 or more statesareasLocal LCDs from 1 or more statesareasndash Written by local CMDs about situations that are Written by local CMDs about situations that are
data based amp need control or instructiondata based amp need control or instructionndash Presented at state CACs open to medical and Presented at state CACs open to medical and
specialty societies representativesspecialty societies representativesndash Notice and comment always welcome Notice and comment always welcome ndash Reconsiderations always possibleReconsiderations always possible
bull LCDs cover a Medicare Jurisdiction (eg J-1)LCDs cover a Medicare Jurisdiction (eg J-1)ndash Discuss and describe medical necessityDiscuss and describe medical necessityndash Usually give codes amp conditions for paymentUsually give codes amp conditions for paymentndash May state frequency of service and diagnoses May state frequency of service and diagnoses
and always published locally and nationallyand always published locally and nationally
ndash Reconsiderations always possible
6
LOCAL COVERAGE DECISIONS
bull Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)ndash Category III codes ndash temporary or trackingCategory III codes ndash temporary or trackingndash Cytogenic studiesCytogenic studiesndash Free PSAFree PSAndash MammaprintMammaprintndash Oncologic in-vitro chemoresponse assaysOncologic in-vitro chemoresponse assaysndash Oncotype DX Oncotype DX ndash Flow cytometry and immunohistochemistry Flow cytometry and immunohistochemistry
(article) ndash soon to be policy(article) ndash soon to be policybull Some Part A LCDs may also applySome Part A LCDs may also applybull Local articles may also specify lab use or Local articles may also specify lab use or
instruct in billingcodinginstruct in billingcoding
7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

3
NATIONAL COVERAGE DECISIONS
bull National NCDs come from CMSNational NCDs come from CMSndash Based on scientific studies amp data collectedBased on scientific studies amp data collectedndash Presented often at MCAC-open meetingsPresented often at MCAC-open meetingsndash Notice and comment welcomeNotice and comment welcomendash Reconsiderations always possibleReconsiderations always possible
bull NCDs cover entire countryNCDs cover entire countryndash May specify services May specify services alwaysalways covered covered ndash May specify services May specify services nevernever covered coveredndash Published in CMS Coverage ManualPublished in CMS Coverage Manualndash May change as science changes new May change as science changes new
studies emerge or as laws changestudies emerge or as laws change
ndash Reconsiderations always possible
4
NATIONAL COVERAGE DECISIONS
bull Examples of NCDs (over 300 currently)Examples of NCDs (over 300 currently)ndash Alpha-fetoproteinAlpha-fetoproteinndash Collagen crosslinks any methodCollagen crosslinks any methodndash Cytogenic studiesCytogenic studiesndash Digoxin therapeutic drug assayDigoxin therapeutic drug assayndash Fecal occult blood testingFecal occult blood testingndash Genetic testing for warfarin Genetic testing for warfarin ndash HIV testingHIV testingndash Prostate cancer screening testsProstate cancer screening testsndash Sweat testSweat test
bull National Laboratory Coverage Determinations National Laboratory Coverage Determinations (23 currently)(23 currently)
5
LOCAL COVERAGE DECISIONS
bull Local LCDs from 1 or more statesareasLocal LCDs from 1 or more statesareasndash Written by local CMDs about situations that are Written by local CMDs about situations that are
data based amp need control or instructiondata based amp need control or instructionndash Presented at state CACs open to medical and Presented at state CACs open to medical and
specialty societies representativesspecialty societies representativesndash Notice and comment always welcome Notice and comment always welcome ndash Reconsiderations always possibleReconsiderations always possible
bull LCDs cover a Medicare Jurisdiction (eg J-1)LCDs cover a Medicare Jurisdiction (eg J-1)ndash Discuss and describe medical necessityDiscuss and describe medical necessityndash Usually give codes amp conditions for paymentUsually give codes amp conditions for paymentndash May state frequency of service and diagnoses May state frequency of service and diagnoses
and always published locally and nationallyand always published locally and nationally
ndash Reconsiderations always possible
6
LOCAL COVERAGE DECISIONS
bull Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)ndash Category III codes ndash temporary or trackingCategory III codes ndash temporary or trackingndash Cytogenic studiesCytogenic studiesndash Free PSAFree PSAndash MammaprintMammaprintndash Oncologic in-vitro chemoresponse assaysOncologic in-vitro chemoresponse assaysndash Oncotype DX Oncotype DX ndash Flow cytometry and immunohistochemistry Flow cytometry and immunohistochemistry
(article) ndash soon to be policy(article) ndash soon to be policybull Some Part A LCDs may also applySome Part A LCDs may also applybull Local articles may also specify lab use or Local articles may also specify lab use or
instruct in billingcodinginstruct in billingcoding
7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

4
NATIONAL COVERAGE DECISIONS
bull Examples of NCDs (over 300 currently)Examples of NCDs (over 300 currently)ndash Alpha-fetoproteinAlpha-fetoproteinndash Collagen crosslinks any methodCollagen crosslinks any methodndash Cytogenic studiesCytogenic studiesndash Digoxin therapeutic drug assayDigoxin therapeutic drug assayndash Fecal occult blood testingFecal occult blood testingndash Genetic testing for warfarin Genetic testing for warfarin ndash HIV testingHIV testingndash Prostate cancer screening testsProstate cancer screening testsndash Sweat testSweat test
bull National Laboratory Coverage Determinations National Laboratory Coverage Determinations (23 currently)(23 currently)
5
LOCAL COVERAGE DECISIONS
bull Local LCDs from 1 or more statesareasLocal LCDs from 1 or more statesareasndash Written by local CMDs about situations that are Written by local CMDs about situations that are
data based amp need control or instructiondata based amp need control or instructionndash Presented at state CACs open to medical and Presented at state CACs open to medical and
specialty societies representativesspecialty societies representativesndash Notice and comment always welcome Notice and comment always welcome ndash Reconsiderations always possibleReconsiderations always possible
bull LCDs cover a Medicare Jurisdiction (eg J-1)LCDs cover a Medicare Jurisdiction (eg J-1)ndash Discuss and describe medical necessityDiscuss and describe medical necessityndash Usually give codes amp conditions for paymentUsually give codes amp conditions for paymentndash May state frequency of service and diagnoses May state frequency of service and diagnoses
and always published locally and nationallyand always published locally and nationally
ndash Reconsiderations always possible
6
LOCAL COVERAGE DECISIONS
bull Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)ndash Category III codes ndash temporary or trackingCategory III codes ndash temporary or trackingndash Cytogenic studiesCytogenic studiesndash Free PSAFree PSAndash MammaprintMammaprintndash Oncologic in-vitro chemoresponse assaysOncologic in-vitro chemoresponse assaysndash Oncotype DX Oncotype DX ndash Flow cytometry and immunohistochemistry Flow cytometry and immunohistochemistry
(article) ndash soon to be policy(article) ndash soon to be policybull Some Part A LCDs may also applySome Part A LCDs may also applybull Local articles may also specify lab use or Local articles may also specify lab use or
instruct in billingcodinginstruct in billingcoding
7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

5
LOCAL COVERAGE DECISIONS
bull Local LCDs from 1 or more statesareasLocal LCDs from 1 or more statesareasndash Written by local CMDs about situations that are Written by local CMDs about situations that are
data based amp need control or instructiondata based amp need control or instructionndash Presented at state CACs open to medical and Presented at state CACs open to medical and
specialty societies representativesspecialty societies representativesndash Notice and comment always welcome Notice and comment always welcome ndash Reconsiderations always possibleReconsiderations always possible
bull LCDs cover a Medicare Jurisdiction (eg J-1)LCDs cover a Medicare Jurisdiction (eg J-1)ndash Discuss and describe medical necessityDiscuss and describe medical necessityndash Usually give codes amp conditions for paymentUsually give codes amp conditions for paymentndash May state frequency of service and diagnoses May state frequency of service and diagnoses
and always published locally and nationallyand always published locally and nationally
ndash Reconsiderations always possible
6
LOCAL COVERAGE DECISIONS
bull Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)ndash Category III codes ndash temporary or trackingCategory III codes ndash temporary or trackingndash Cytogenic studiesCytogenic studiesndash Free PSAFree PSAndash MammaprintMammaprintndash Oncologic in-vitro chemoresponse assaysOncologic in-vitro chemoresponse assaysndash Oncotype DX Oncotype DX ndash Flow cytometry and immunohistochemistry Flow cytometry and immunohistochemistry
(article) ndash soon to be policy(article) ndash soon to be policybull Some Part A LCDs may also applySome Part A LCDs may also applybull Local articles may also specify lab use or Local articles may also specify lab use or
instruct in billingcodinginstruct in billingcoding
7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

6
LOCAL COVERAGE DECISIONS
bull Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)Example of J-1 LCDs (Currently 80+ ldquoBrdquo LCDs)ndash Category III codes ndash temporary or trackingCategory III codes ndash temporary or trackingndash Cytogenic studiesCytogenic studiesndash Free PSAFree PSAndash MammaprintMammaprintndash Oncologic in-vitro chemoresponse assaysOncologic in-vitro chemoresponse assaysndash Oncotype DX Oncotype DX ndash Flow cytometry and immunohistochemistry Flow cytometry and immunohistochemistry
(article) ndash soon to be policy(article) ndash soon to be policybull Some Part A LCDs may also applySome Part A LCDs may also applybull Local articles may also specify lab use or Local articles may also specify lab use or
instruct in billingcodinginstruct in billingcoding
7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

7
FINDING LCDs amp NCDsFINDING LCDs amp NCDsbull wwwcmshhsgovMCDoverviewasp
ndash Click ldquoindexesrdquo from left boxndash Click ldquonationalrdquo or ldquolocalrdquo coveragendash For local coverage click LCDs by
contractor (We are MACsmdashPart A or Part B---Palmetto)
ndash For articles we are MACs---Part A or Part B---Palmetto
8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

8
REQUESTING LCD RECONSIDERATIONS
bull Send in writing to local ContractorSend in writing to local Contractorndash Specific address for reconsiderations on our web siteSpecific address for reconsiderations on our web sitendash Specific address of CMDsSpecific address of CMDs
bull Add supporting scientific evidenceAdd supporting scientific evidencendash Literature in peer reviewed journalsLiterature in peer reviewed journalsndash Expert opinion from credible sourcesExpert opinion from credible sourcesndash Guidelinesstatements from specialty societiesGuidelinesstatements from specialty societiesndash Results of medium or long term studiesResults of medium or long term studies
bull Be specific in requestsBe specific in requestsndash CPT ICD-9 organ systems or special circumstancesCPT ICD-9 organ systems or special circumstances
bull Be conscious of vested interestsBe conscious of vested interestsbull Contractor must respond in 30 days to valid Contractor must respond in 30 days to valid
reconsideration requestsreconsideration requests
9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

9
ORDERING-REFERRING DOCS
bull MD Clin Nurse Specialist
bull DO Clin Psychologistbull Dental Surgery Nurse Midwifebull Dental Medicine Clin Social Workerbull Podiartist Nurse Practitionerbull Optometrist Chiropractorbull Physician Assistant
10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

10
ORDERING PHYSICIANS
bull Claims ordered referred mustndash NPI of ordering providerndash Name in PECOS or MAC system ndash Specialty as listed
bull Grace Periodndash Phase 1 10509 to 33110 warning
message on remittancendash Phase2 40110 and after claim
rejected if referring individual not in Pecos or MAC list
40110 and after
11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

11
OTHER ENROLLMENTOTHER ENROLLMENTbull Revalidation of older
physicians not in PECOSbull Revalidation of some labsbull Need to update any changes
within 30 daysndash Address phone suitendash New members in groupndash Other changes
bull If no claims to Medicare in one yearmdashphysician is disenrolled in Medicare
12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

12
HIGLASS-FINANCIAL CHANGEHIGLASS-FINANCIAL CHANGE
bull Healthcare Integrated General Ledger Accounting System (HIGLASS)
bull Change CMS accounting systemndash More accurate timely consistent
paymentsndash More CMS direct oversight
bull Dec 9th ndash Payment floor to 0ndash All claims approved are paid
bull Dec 14 ndash Payment floor returnsndash 14 days for electronic claimsndash 28 days for paper claims
13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

13
CHANGE IN CHANGE IN PAYMENT FLOORCHANGE IN PAYMENT FLOOR
14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

14
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull On-line provider servicendash Claims statusndash Eligibility statusndash Remittance Statusndash Financial Status
bull In real time updated dailybull Must have EDI enrollment
agreement signed with Palmetto
15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

15
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Register on OPS home page
bull Get user ID and PasswordGet user ID and PasswordbullAnswer security questionAnswer security question
16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

16
ON-LINE CLAIMS ON-LINE CLAIMS MANAGEMENTMANAGEMENT
bull Log inbullClaim status claim status claim lines
bullRemits online list of remits e-remits
bullEligibility Inquiry deductibles caps MSP more
bullFinancial Tools payment floor cash flow more
bullAdministration control who can use tool
17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

17
SIGNATURES bull Handwritten signatures or initialsHandwritten signatures or initials
ndash Must be legibleMust be legible bull Electronic signatures Electronic signatures
ndash Digitized-Digitized- an electronic image of an an electronic image of an individualrsquos handwritten signature reproduced individualrsquos handwritten signature reproduced in its identical form using a pen tablet in its identical form using a pen tablet
ndash ElectronicElectronic signatures usually contain date amp signatures usually contain date amp timestamps and include printed statements timestamps and include printed statements eg electronically signed by or verified eg electronically signed by or verified reviewed by followed by physicianrsquos name amp reviewed by followed by physicianrsquos name amp preferably a professional designation Note preferably a professional designation Note The responsibility and authorship related to The responsibility and authorship related to the signature should be clearly defined in the the signature should be clearly defined in the record record
ndash Digital signatureDigital signature - an electronic method of a - an electronic method of a written signature typically generated by written signature typically generated by encrypted software that allows for sole usage encrypted software that allows for sole usage
18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

18
SIGNATURESChart Accepted By with providerrsquos nameChart Accepted By with providerrsquos name
Electronically signed by with providerrsquos name Electronically signed by with providerrsquos name Verified by with providerrsquos name Verified by with providerrsquos name Reviewed by with providerrsquos name Reviewed by with providerrsquos name Released by with providerrsquos name Released by with providerrsquos name Signed by with providerrsquos name Signed by with providerrsquos name Signed before import by with providerrsquos name Signed before import by with providerrsquos name Signed John Smith MD with providerrsquos name Signed John Smith MD with providerrsquos name Digitalized signature Handwritten amp scanned into the Digitalized signature Handwritten amp scanned into the
compute compute This is an electronically verified report by John Smith This is an electronically verified report by John Smith
MD MD Authenticated by John Smith MD Authenticated by John Smith MD Authorized by John Smith MD Authorized by John Smith MD Digital Signature John Smith MD Digital Signature John Smith MD Confirmed by with providerrsquos name Confirmed by with providerrsquos name Closed by with providerrsquos name Closed by with providerrsquos name Finalized by with providerrsquos name Finalized by with providerrsquos name Electronically approved by with providerrsquos nameElectronically approved by with providerrsquos name
19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

19
Unacceptable Signaturesbull See unacceptable signature examples See unacceptable signature examples bull Signing physician when Signing physician when providers name is typedproviders name is typed
Example Signing physician ______________________Example Signing physician ______________________ John Smith MD John Smith MD
bull Confirmed by when a Confirmed by when a providers name is typedproviders name is typedExample Confirmed by ______________________Example Confirmed by ______________________ John Smith MD John Smith MD
bull Signed by providers name typed and the signing Signed by providers name typed and the signing line above but line above but done as part as the transcriptiondone as part as the transcription
bull This document has been electronically signed in This document has been electronically signed in the surgery department the surgery department with no provider namewith no provider name
bull Dictated by when Dictated by when providers name is typedproviders name is typedExample Dictated by ______________________Example Dictated by ______________________ John Smith MD John Smith MD
bull Signature stamp Signature stamp bull Signature On FileSignature On File
20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

20
SIGNATURES WHAT WE FIND
bull Illegible unrecognizable Illegible unrecognizable handwritten signatures or initials handwritten signatures or initials
bull Unsigned ldquotypewrittenrdquo progress Unsigned ldquotypewrittenrdquo progress notes with a typed name only notes with a typed name only
bull Unverified or unauthorized Unverified or unauthorized electronic signatureselectronic signatures
bull No indication of the rendering No indication of the rendering physicianpractitionerphysicianpractitioner
bull Required for all labs progress Required for all labs progress notes orders and the likenotes orders and the like
21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

21
IF SIGNATURE IS AN ILLEGIBLE IF SIGNATURE IS AN ILLEGIBLE SCRAWLhellipSCRAWLhellip
bull Have an official Have an official signature page with signature page with name and signature name and signature OROR
bull Send an attestation Send an attestation statement certifying statement certifying that physician saw that physician saw patient and wrote note patient and wrote note on that dateon that date
22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

22
MAC OVERVIEW-15 AREAS
bull 15 MACs 4 DMACs 4RHHIsbull Companies may have gt 1MACbull MAC may have gt1 CMDbull CMDs work together
ndash Within MACsndash Within Companiesndash Across MACsndash Within CMS Committees Workgroups
bull Many MAC Contracts in Dispute
23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

23
NATIONAL VS LOCAL LAB COVERAGE
bull Advantages ndash Policies coverage coding and pricing
same everywhere ndash More publicity fewer local hasslesndash More likely private insurance accepts
bull Disadvantages of Nationalndash Requires more evidence studiesndash Longer time frame for acceptancendash Usually requires FDA clearancendash Increased marketing costs required ndash Access across all statesterritories
when lab not large enough for tests
24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

24
NATIONAL VS LOCAL COVERAGE
bull Advantages of Localndash Home brew possible without FDA
approval neededndash Quicker less intensive reviewsndash Easier to convince CMDsndash Can select areas for introductionndash Can use 1-2 MACs to influence others
bull Disadvantages of Localndash Less uniform coding coverage pricingndash Variation in payment acceptancendash Private insurance may not go alongndash Have to repeat work with each MAC
25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

25
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull CMDs are very busy
ndash Policies articles coveragendash Med Review and chart adjudicationndash Education outreach to societies groupsndash Contact with CMS amp other organizations
bull Most CMDs will find time for meetingndash In Person office hotel other locationndash Telephone Web etc may be more efficient
bull Time is always a considerationndash Send info data literature in advancendash Allows CMDs to be prepared shortens
meeting allows quicker resolutionndash Must fit between CMDs travel outreach
teleconferences with CMS and home office
ndashSend info data literature in advance
26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

26
MEETING WITH LOCAL CMDMEETING WITH LOCAL CMDbull Show us the data
ndash Published peer reviewed datandash Statistically significant differencesndash Demonstrate effect on patient
diagnosis or patient therapy
bull Bottom Linendash Does it work amp affect patient carendash Sensitivity specificity amp relatedndash Outcomes for patientsndash Cost (and more important pricing)
- Demonstrate effect on patient diagnosis or patient therapy
27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

27
HELP US WITH PRICINGHELP US WITH PRICINGbull Show us the pricingShow us the pricing
ndash Prefer single pricing vs code stackingPrefer single pricing vs code stackingndash Reality versus imaginationReality versus imagination
bull What is included in pricingWhat is included in pricingbull What should not be includedWhat should not be included
bull Can it be cross walked to existing Can it be cross walked to existing CPT codesCPT codesndash Easier to determine prices Easier to determine prices ndash May use NOC codes at first to May use NOC codes at first to
describe its usedescribe its usendash Remember least costly alternative Remember least costly alternative
situationssituations
28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

28
SELECTING CPT CODES
bull Stacking codes problematicndash Donrsquot define test to usndash May give inaccurate prices--- too
high or too lowbull Use NOC code (eg 84999)
ndash Use with name of test (eg ldquoWonderTestrdquo)
ndash We can assign specific pricendash We can follow use of test for policyndash Less confusing for ordering MD
bull We can consider development costs or small quantity costs
29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

29
LONGER TERM CODING
bull Real CPT Code Helps Define Testndash Can take yearsndash Usually associated with national
coverage and national pricingbull Consider HCPCS or Category III
ndash HCPCS comes from CMSndash Category III easy to obtain
bull Allows national tracking of databull Can allow for payment alsobull Category III can progress to regular CPT
bull Consider Coverage With Evidence Developmentndash Obtained from CMS
30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

30
GENETIC TESTINGbull Consider the science
ndash Same proof amp science as other tests
ndash Same clinical validityndash Same peer reviewed data
bull Consider the ethicsndash Who gets testedndash Under what circumstancesndash When tests done
bull Consider the costsndash Once per lifetime
31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

31
GENETIC TESTINGbull Consider if the test is
screening-amp not coveredndash Each screening test requires
new law from Congressndash When is screening not
screening but disease management ndash gray area
bull Future CMS amp legal issues dealing with genetic testing
32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

32
OTHER ASPECTS OF NEW TESTSOTHER ASPECTS OF NEW TESTSbull Coverage for a new test (service)
may be positively influenced byndash Requests from physicians in
practicendash Clinical society white papers or
guidelinesndash Technical Advisory Committeesndash Other Medicare MACs or insurers
bull Coverage for a new test (service) may be negatively influenced byndash Over-marketing by manufacturer ndash Inadequate data with ldquospinrdquo by
consultantsndash Ridiculous pricing demandsndash Use of stacking codes when other
coding more appropriate
33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

33
TIME FACTORS FOR DECISIONS
bull Review (re-review) literaturebull Discuss with staffbull Review other Contractors for like policiesbull Add as article 3-6 weeks
ndash Includes code decision price decisionndash Claims personnel education
bull Formal Policy due to restrictions of use or diagnoses 3-6 monthsndash Write amp review policyndash Draft on web for public reviewndash CAC and open meetings requiredndash Open for comments from anyonendash Notice of final policy before effect date
34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

34
Welcome to The ACP Advocate
Our second story as promised is an analysis of the Medicare Fee Schedule for next year ACPrsquos Advocacy Web Site also has answers to your frequently asked questions about the new rule While the new schedule is considered final we still expect that Congress will step in to stop the 21 percent overall fee cut that is supposed to start Jan 1 On Thursday afternoon the House passed HR 3961 a bill that would fix the problems in Medicare payments caused by the sustainable growth rate formula If they manage to work with the Senate to pass similar legislation this would provide a fix for not only the 21 percent cut it would pave the way for the long-term fix wersquove been waiting for
35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

35
MAJOR PRICING CHANGES 2010
bull PPIS (AMA Physician Practice Information Survey) data
bull Change in utilization ratebull Medicare Consultations
eliminated ndash some other CPT changesbull 5 year review of malpractice RVUsbull Implementation of MIPPA provisionsbull Not many changes for routine lab
36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

36
PPIS SURVEY FOR PRACTICE PPIS SURVEY FOR PRACTICE EXPENSE INFORMATIONEXPENSE INFORMATION
bull PPIS is multispecialty survey of physicians and NPPs ndash Used consistent survey instrumentndash 3656 across 51 specialties and
professional groupsbull New survey conducted by AMA
ndash Expanded to include NPPsndash CMS purchased updated specialty
specific PE hr data for PE RVUsbull Most consistent source of
practice expense survey information to date
37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

37
PPIS SURVEY FOR PEPPIS SURVEY FOR PEbull PPIS data has effects of redistribution
with negative aspects to some groupsndash Cardiologyndash Radiologyndash Oncologyndash Urology
bull Positive aspects for primary carebull PPIS data transitioned over 4 yearsbull Supplemental survey data also used
ndash Clinical labsndash IDTFsndash Oncology and Drug Administration
38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

38
bull Contract Language
bull Ethics Forum
bull In the Courts
bull Practice Management
bull Technically Speaking
bull raquo More BROWSE
bull Issue dates bull Regions bull Health
plans bull Sections bull News briefs bull Columns bull Editorials bull Letters bull Writers bull Other years
HELP
bull Search tips bull E-mail alert bull Radio bull RSS bull Mobile bull Subscribe bull Institutions bull Staff
directory bull Advertising bull Permissions bull Reprints bull News
media bull Site guide bull Useful links bull About bull Premium bull Contact
Specialty Average change
Ophthalmology 5
Family medicine 4
General practice 3
Geriatrics 3
Internal medicine 2
Interventional radiology -3
Urology -4
Radiology -5
Cardiology -8
Nuclear medicine -18
Source Centers for Medicare amp Medicaid Services Payment Policies Under the Physician Fee Schedule and Other Revisions
to Part B for CY 2010 Federal Register Oct 30 (wwwfederalregistergovofruploadofrdata2009-26502_pipdf)
CHANGES
FOR
2010
WINNERS
AND
LOSERS
39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

39
40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

40
41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

41
42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

42
CMS ACTION (not final) from AMA Meeting
bull Eliminated use of all consultation codes Eliminated use of all consultation codes (except for telehealth consult G-codes)(except for telehealth consult G-codes)
bull Increased work RVUs for new amp Increased work RVUs for new amp established office visits established office visits
bull Increased work RVUs for initial hospital Increased work RVUs for initial hospital and initial nursing facility visitsand initial nursing facility visits
bull Incorporated the increased use of these Incorporated the increased use of these visits into PE and malpractice RVU visits into PE and malpractice RVU calculations calculations
bull Increased incremental work RVUs for Increased incremental work RVUs for EampM codes built into the 10-day and 90-EampM codes built into the 10-day and 90-day global surgical codesday global surgical codes
43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

43
CONSULTATION Decision not CONSULTATION Decision not FinalFinal
bull Per AMA-CPT Meeting Consultations no Per AMA-CPT Meeting Consultations no longer reimbursed for Medicarelonger reimbursed for Medicarendash Effective 1-1-10 unless rules changeEffective 1-1-10 unless rules changendash Regular initial EampM codes for initial inpatient Regular initial EampM codes for initial inpatient
hospital amp nursing facilitieshospital amp nursing facilitiesndash Regular follow up codes for hosp SNF-NFRegular follow up codes for hosp SNF-NFndash Regular office initial amp follow up codesRegular office initial amp follow up codes
bull Principal physician of record uses a Principal physician of record uses a modifier to be listedmodifier to be listed
bull CPT still lists consult codes for non-CPT still lists consult codes for non-Medicare patientsMedicare patients
44
QUESTIONS

44
QUESTIONS