-
8/11/2019 j.1444-0938.2003.tb03058.x
1/6
OPTOMETRY
I CASEREPORT
Sub retinal neovascular membrane in exudative
macular degeneration
Clin Exp Optom
2003; 86: 1: 51-56
Sandra
HarrisB
Optom PgDipAdvClinOpt
Victorian College of Optometry, The
University of Melbourne
Age-related macular degeneration is a major cause of serious
vision loss. The earliest
stages of age-related maculopathy may be defined by the size of
the drusen present in
the macula and the effects on vision. Further manifestations may
include soft drusen,
Received: 18 March 2002
Revised: 28 October 2002
choroidal neovascularisation, macular haemorrhage and
cicatricial or disciform degen-
eration
of
the macula.
This report describes a patient with a macular haemorrhage, a
choroidal neovascular
Accepted for publication: 18 November
2002
membrane and serious loss
of
vision. In addition, the pathogenesis, diagnosis and treat-
ment options of macular degeneration are reviewed.
Key words: age-related maculopathy, macular degeneration,
neovascular membrane
Age-related macular degeneration AMD)
is the leading cause of vision loss in the
developed world and
i t
is predicted that
the incidence of this condition will rise as
the population ages.l Studies show a fur-
ther increase in the incidence and preva-
lence of
AMD
independent of the aging
factor.2 The Blue Mountains Eye Study
showed the prevalence of
AMD
in an Aus-
tralian population to be 1.9 per cent. The
overall prevalence of
AMD
is estimated to
be approximately
two
per cent, depend-
ing on the classification system used, with
a significant increase in prevalence over
65 years of age. Wolffsohn4 tudied a Mel-
bourne low-vision population and found
that
AMD
was by far the most common
cause
of
visual impairment in those over
the age of 60 years. The percentage of this
age group whose visual impairment was
primarily due to
AMD
rose from about 40
per cent in 1976 to
70
per cent in 1998.
The initial form of AMD, prior to signifi-
cant vision loss, is termed age-related
maculopathy
ARM).
t is defined as a
degenerative disorder in patients older
than 50 years of age with abnormalities in
the macular region, including one or more
drusen greater than 63 microns in diam-
eter.5 The grading circle
of
63 microns is
used in the Wisconsin grading system6 o
differentiate the small hard drusen that are
associated with the normal aging process
from the larger soft drusen that are indica-
tive of ARM. It can be compared to the
average optic disc diameter, which
is
esti-
mated to be between 1,500 and 1,900
microns.6
Retinal pigment epithelium (W E) dis-
ruption also may be evident as atrophy,
hyperpigmentation,
or
hypopigmentation
with associated neurosensory detachment.
The prevalence ofARM in the Blue Moun-
tains Eye Study population, based o n the
Wisconsin classification system, was
7.2
per
cent and rose with age from 1.3 per cent
in those under 55 years to 28 per cent in
those aged
85
years or older. AMD is the
progression of
ARM
and has
two
clinical
forms, commonly known
as
dry (atrophic)
AMD and wet (exudative) AMD. The divi-
sion of the disease into dry and wet forms
is representative of the presence or ab-
sence of choroidal neovascularisation
(CNV). Subfoveal choroidal neovascular-
isation provokes sudden, severe central
vision loss. Only 10 to 15 per cent of
affected patients progress to exudative
AMD, however, this form of the condition
is responsible for up to 90 per cent of the
associated severe vision loss. In more than
40
per cent of patients with exudative
AMD,
the condition becomes bilateral
within five ye ax 8
Currently, there are no available thera-
pies for exudative AMD that aim to restore
the patients visual acuity. The
two
estab-
lished treatments that stabilise vision and
limit severe vision loss in selected patients
Clinical and Experimental Optometry
86.1
January 2003
51
-
8/11/2019 j.1444-0938.2003.tb03058.x
2/6
Sub-retinal neovascular membrane Hum's
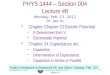
Figure 1. A
50
degree digital fundus photograph of the patient s
right eye in April 1999. Evident at the macula is a dark,
slightly
raised area of approximately onequarter disc diameter.
are laser photocoagulation, which was
widely used in the 199Os, and verteporfin
photodynamic t reatment, which has been
introduced in the past t w o years.
Fluorescein angiography is used to diag-
nose CNV and to direct treatment. The
composition of a choroidal neovascular
lesion is classified as either classic (show-
ing a well-demarcated hyperfluorescence
in the early phase)
or
occult (poorly de-
marcated boundaries) depending on the
fluorescein angiography appearance, and
this has implications for ~e a t m e n t . ~ther
imaging techniques such as Indocyanine
Green angiography are not required
to
decide whether treatment is needed, but
may further assist the retinal specialist to
localise the lesion.9It is estimated that only
13 to 26 per cent of patients would benefit
from laser photocoagulation compared
with no treatment.' The recent introduc-
tion of verteporfin photodynamic treat-
ment
PDT)
has the potential
to
increase
the proportion of patients eligible for treat-
ment to between 25 and 40 per cent.
However, even with treatment, there is a
high risk of the recurrence of membrane
growth and the need for retreatments.
This report illustrates the natural course
of exudativeAMD with ocular fundus pho-
tographs and fluorescein angiography at
several stages. It discusses the identifica-
Figure
2.
Fluorescein angiography of the patient s right eye in
May 1999 revealed a classic subfoveal choroidal neovascular
membrane. Image courtesy of
Dr
A Harper (Fitzroy, Victoria,
Australia).
tion of early symptoms and retinal signs
that may suggest the need for fluorescein
angiography and risk factors that may
prompt more frequent review of the sus-
ceptible patient.
CASE
REPORT
A 73-year-old man presented for optomet-
ric examination to the Melbourne Optom-
etry Clinic of the Victorian College of
Optometry on 30 April 1999, having noted
for about
two
months reduced vision in
his right eye compared with the left. He
reported that straight edges appeared wavy
when viewed with his right eye only. Apart
from having high cholesterol, he was in
good health and was not taking any medi-
cations.
Visual acuities were
R
6/12 and
L
6/7.5
with
R t1.00 DS
and
L
-0.25/-0.50 x 90.
Testing with an Amsler chart showed cen-
tral distortion in the right eye. Slitlamp
examination showed early crystalline lens
changes in both eyes consistent with age.
Intraocular pressures were within normal
limits. Mydriatic ocular fundus examina-
tion showed a dark, slightly raised area at
the macula in the right
eye
(Figure
1)
and
a faint 'dot' haemorrhage was evident one
quarter of a disc diameter superior to the
right macula. Scattered hard drusen were
present in right and left eyes. N o soft
drusen were noted. Exudative
AMD
was
suspected in the right eye and the patient
was referred for assessment and possible
treatmen
t.
At a previous examination in the clinic in
March 1998, visual acuities had been R 6/6
and
L
6/7.5 with
R
+0.25
DS
and
L
-0.25/
-0.50 x 135. Both internal mydriatic and
external eye examinations had appeared
unremarkable, with some subtle macular
pigment changes noted in the left eye.
At ophthalmological examination on 19
May 1999, right eye visual acuity was 6/18.
Fluorescein angiography showed a classic
choroidal neovascular membrane approxi-
mately 500 microns in diameter extend-
ing benea th the fovea (Figure 2) , with
overlying subretinal fluid. Fluorescein
angiography for the left eye was relatively
normal with some macular hard drusen
but n o soft drusen evident. The option of
immediate laser treatment
of
the right eye
was discussed with the patient, however,
the probability of further reduction in
central visual acuity with therapy was con-
sidered unacceptable. The ophthalmolo-
gist recommended observation over a
period of weeks with the possibility of
subfoveal laser treatment at
a
later date to
limit final scotoma size.
In March 2000,ophthalmological review
Clinical and Experimental
Optometry
86.1 January 2003
52
-
8/11/2019 j.1444-0938.2003.tb03058.x
3/6
Sub-retinal neovascular membrane
Harris
Figure 3a. A red-free fundus photograph of the patients
right
eye in March
2000
shows sensory retinal detachment.
Haemorrhages are indicated by arrowheads. Image courtesy of
Dr A
Harper (Fitmoy, Victoria, Australia).
Figure 3b. Fluorescein angiography in March 2000 illustrates
the
underlying choroidal neovascular membrane. Image courtesy of
Dr A Harper (Fitzroy, Victoria, Australia).
Figure 5. The photograph of October 2001 shows resolution of
the superior haemorrhage. Flame haemorrhagesare evident
along
the inferior arcade (arrowheads).
Figure 4 Red-free fundus photograph in April 2001. A macular
choroidal scar is noted, with superior haemorrhage and
exudate.
Clinical and Experimental Optometry
86.1
January
2003
53
-
8/11/2019 j.1444-0938.2003.tb03058.x
4/6
Subretinal neovascular membrane
Hums
gave a visual acuity of
6/60
in the right
eye. The left eye was unchanged at
6/7.5.
Ophthalmoscopy and fluorescein angiog-
raphy showed a classic choroidal neovas-
cular membrane of at least four disc
diameters in size with minimal late leak-
age (Figure 3a, 3b). Options including
central laser photocoagulation were dis-
cussed with the patient, however, given the
further loss of acuity associated with treat-
ment, observation alone
was
the chosen
course of action. With the expectation of
further deterioration in the right eye, the
patient was asked to report any changes
in the vision of the left eye.
Regular optometric review was insti-
gated and in November
2000,
the patient
could define a black scotoma centrally in
the right eye. Visual acuities were
R
less
than 6/120 and
L 6/9.
A large superior
subretinal haemorrhage was noted in the
right eye. In April2001,visual acuities were
R 6/380 part and L6/7.5 with refraction
unchanged from
1999.
There was a
chorioretinal scar at the right macula and
a one disc diameter flame haemorrhage
along the superior arcade (Figure4 . Hard
exudate was noted in the inferior arcade.
At
review in October
2001,
the patient
reported a recent diagnosis of diabetes
mellitus. Visual acuities were still
R
6/380
part and
L 6/7.5.
Right fundus assessment
showed small flame haemorrhages along
the inferior arcade (Figure
5).
The appear-
ance of the left fundus was relatively nor-
mal, with hard drusen at the macula but
no soft drusen or significant RPE changes
evident. Optometric review
was
scheduled
for six months.
An
Amsler chart was pro-
vided for home monitoring and the pa-
tient was asked to report immediately any
signs
of
distor tion with the left eye.
COMMENT
This case illustrates the natural course of
exudativeAMD over a two and a half year
period in an older man. He was able to
observe monocular vision disruption,
which prompted presentation and diagno-
sis. The signs displayed were typical of this
condition, along with the severe monocu-
lar vision loss, which is often a portent of
devastating binocular loss. Up to 70 per
cent of eyes with subfoveal
CNV
second-
ary to
AMD
have visual acuity
of 6/60
or
worse within
two
years of diagnosisI2and
12
per cent of patients who present with
the unilateral form of the disease are
legally blind within two years1
The patient had reported reduced
vision in one eye and metamorphopsia of
relatively recent onset. These symptoms of
painless vision loss are typical of early
AMD.Other conditions that display uni-
lateral painless vision loss include cataract,
glaucoma, ischaemic optic neuropathy,
central serous retinopathy, retinal artery
or
vein occlusion and retinal detachment.
The majority of these conditions can be
ruled out following initial optometric
assessment. The exception is central
serous retinopathy, which can be excluded
with fluorescein angiography, although it
typically occurs in younger patients, and
would be expected to display a pale rather
than dark raised macula as only the sen-
sory retina is detached.I3 n addition to re-
duced or distorted vision inAMD atients
may describe the visual disruption as a
shadow, discolouration
or
loss of contrast.
Rarely, floaters may be experienced if pre-
retinal haemorrhage occurs. Given the age
group of patients with
AMD
t is possible
for early symptoms to be masked by cata-
ract
or
posterior vitreous detachment.
Because people rarely compare the vision
between their two eyes in everyday life,
unilateral AMD often escapes detection
initially and although the patient is more
sensitive to vision changes in the fellow
eye, there may be a delay in presenting if
the patient is unaware that earlier assess-
ment maximises treatment options.
The role of the eye care practitioner is
vital in emphasising to patients who are
observed to have signs of earlyARM, hat
same-day presentation is important with
symptoms of visual disturbance. Without
this caution, many patients seem content
to wait for an appointment across a few
weeks, if the waiting list demands. The
patient in this case waited up to two
months after noticing the initial visual
disruption before attending for an eye
examination.
n
Amsler grid used at home
can be a valuable patient education tool
for patients at risk. Unfortunately, some
patients such as the above case show few
ocular warning signs to alert the practi-
tioner. As more effective treatments for
AMD
become available, public awareness
campaigns may be of advantage in encour-
aging patients to attend
an
eye care practi-
tioner immediately when symptoms occur.
Histopathologic evaluation of the retina
has shown that deterioration occurs in all
eyes with advancing age and AMD s the
acceleration of this process to a level where
vision loss O C C U ~ S . ~ he degenerative proc-
ess is manifested primarily
as
damage to
the
RPE
cells. It is thought that the
affected RPE cells are unable to digest
some elements of damaged photorecep-
tor membranes, resulting in the formation
of lipofuscinor bodies within the RPE cells
that are filled with debris. The accumula-
tion of these bodies is associated with ex-
trusion by the
WE
cells of a waste prod-
uct between the plasma membrane and
the basement membrane of the
RPE
(ba-
sal laminar deposit)
I5
These deposits may
further impair the function of the RPE by
blocking nutrient intake from the chorio-
capillaris. Formation of soft drusen occurs
with localised detachments when larger
areas of the RPE become dysfunctional
and secrete debris in vesicles through the
basal lamina to coalesce on Bruchs mem-
brane (basal linear deposits).
Loss
of vision
in AMD occurs with the atrophy of the
photoreceptor cells associated with the
damaged
WE
or by neovascular invasion
of the region, A neovascular membrane
forms when choroidal vessels are able to
breach Bruchs membrane and spread
beneath the basal laminar and basal lin-
ear deposits within the soft drusen. Haem-
orrhaging from the new vessels can cause
RPE detachment from Bruchs membrane
and subsequent neural retinal detachment
as
serous exudate leaks through the dam-
aged RPE (Figure
6).
Th e early clinical app earan ce of a
subretinal choroidal neovascular mem-
brane is illustrated in Figure
1.
Ophthalm-
oscopy at this stage shows subtle darken-
ing of the affected macular region that can
be seen more distinctly with a red-free fil-
ter. Although it was difficult to determine
the extent
to
which the retina was elevated
with ophthalmoscopy alone, a hyperopic
Clinical and Experimental Optometry 86 1 January2003
54
-
8/11/2019 j.1444-0938.2003.tb03058.x
5/6
Sub-retinal neovascular membrane
Harris
Figure 6.
Redrawn after Young
RW.
Schematic diagram of a disciform lesion. Choroidal
vessels have penetrated Bruch s membrane (BM) and have spread
laterally in the plane of a
large, soft druse (D). One of the peripheral arcades
of
the neovascular membrane
(NV)
has
ruptured, producing a haemorrhagic detachment
H)
of
the retinal pigment epithelium (WE)
from Bruch s membrane. The haemorrhage is located in the same
plane as the new vessels,
that is between the basal lamina (BL) of the RPE and the
remainder of Bruch s membrane.
Fluidhas penetrated the damaged WE, producing a
serous
detachment
(S)
of the overlying
neural retina (of which only the inner and outer segments of
the
v isua l
cells are shown).
shift of t0.75 D was noted in the right eye
across the period March 1998 o April 1999
and this gives an objective indication of
retinal elevation. Other conditions such
as myopic degeneration, angioid streaks
and ocular histoplasmosis syndrome need
to be ruled out where neovascularisation
is suspected, particularly in the absence
of other obvious signs of AMD, as in this
case.13Of interest in the later stages of the
observation period (Figures 4 and 5) is the
fact that despite the central chorioretinal
scar, retinal haemorrhages were noted up
to twoyears following the initial detection
of the neovascular membrane. Given their
peripheral location,
i t
is possible that the
haemorrhages seen in Figure 5 were a
result of the patient's diabetes rather than
AMD.
Established risk factors forARM include
age, systemic hypertension, a history of
smoking, coronary artery disease, race,
light exposure, genetic predisposition and
iris co lo ~r .~ ~ ' ' ~recent study found that
cigarette smoking for longer than 40 years
caused 14 per cent of AMD cases and that
smoking was the primary modifiable risk
factor for ARM and AMD.I6 The only risk
factors displayed by the patient in this case
at the time of diagnosis were a high cho-
lesterol level and the fact that he was 73
years of age. The patient did not display
any ocular risk factors in the right eye prior
to diagnosis of the subfoveal neovascular
membrane in 1999. It is likely that basal
laminar and basal linear deposits were
present in 1998 and contributed to the
process of neovascularisation in this pa-
tient. Ocular risk factors for the fellow eye
include presence of large drusen, soft
drusen and focal hyperpigmentation of
the RPE (Table 1) .The Macular Photoco-
agulation Study Group (MPS)* reported
that where all of these ocular risk factors
are evident, the risk to the fellow eye across
five years is 87 per cent compared with
seven per cent, where none of them is
present. In this case the fellow eye re-
mained free of these ocular risk factors
throughout the period of observation, with
both ophthalmoscopy and fluorescein
angiography. Some mild pigment mottling
was noted at the left macula in 1998 that
may account for the reduction of visual
acuity to 6/7.5, although the fluorescein
angiography was normal. However, this
slight reduction may be accredited also to
early crystalline lens changes or patient
motivation. Although no specific ocular
risk
factors were identified in the fellow
eye, regular review was indicated.
As
well
as ocular fundus assessment, regular re-
view provides an opportunity to reinforce
patient instruction in the use of an Amsler
chart and in prompt attendance for assess-
ment on noticing symptoms.
Of patients who fit the MPS criteria for
laser photocoagulation, treatment reduces
the risk of severe vision loss by ha1f.I The
MPS data show that the patients who do
best with this treatment have poor initial
visual acuity or a CN V membrane that
appears on fluorescein angiography to
cover an area less than one disc diameter.
Laser photocoagulation is applicable to
about 13 o 26 per cent of cases'O and many
experience persistent
or
recurrent
CNV
following treatment .
Verteporfin photodynamic treatment
(PDT) is relatively new and has been avail-
able in Australia only since early 2000. It
was not available when this patient initially
presented. It involves the treatment of
CNV through a two-step process. A photo-
sensitive dye that binds selectively on new
blood vessels is injected intravenously and
later activated with a 689 nm (non-
thermal) laser. It appears to cause less
damage to the overlying retina than laser
photocoagulation, allowing the treatment
of more central lesions. The percentage
of patients who may be suitable for PDT is
limited by the classification of CNV based
on the fluorescein angiography appear-
Ocular
risk
factors for the fellow eye
One or more large drusen at the macula
Soft drusen at the macula
Focal hyperpigmentation
of
the
RPE
Five or more drusen
Confluent drusen
Table
1.
Risk
factors for the fellow eye in
exudative AMD.The Macular Photocoag-
ulat ion Study Group reports that a
combination of these risk factors in the
fellow eye increases
the risk of
progression
to AMD to
87
per cent across five years
compared to seven per cent, where none is
present.
Clinical and Experimental Optom etry 86 1 January 2003
55
-
8/11/2019 j.1444-0938.2003.tb03058.x
6/6
Sub-retinal neovascular membrane Harris
ance. Currently, the greatest benefit occurs
for m embrane s with a predo minan tly clas-
sic profile (as above) . The percentage of
AMD patients match ing the t rea tme nt cri-
teria who will benefit from
PDT
remains
unclear. Estimates
range
from
20
to 30 per
cent to as few as five
per
cent.' There may
be a substantial cost involved to the pa-
tient and it is necessary to reinforce the
fact that visual improvement is unlikely
and that the therapy needs to be repeated.
Finel' estimates that at least
75
per cent
o f pa t ien t s r ece iv ing PDT requ i re
retreatment in the first year alone. Th e
cost
of
the treatments a nd side effects in-
cludi ng transient visual distu rbance s an d
transient photosensitivity reactions need
to be taken into account.
Oth er therapy options currently under-
going trials include submacular surgery
and external beam radiation. A recent
study proposes that a high-dose vitamin
supplement including antioxidants and
zinc may be protective for patients with
inter medi ate and advanced AMD. Patients
given a combination of both antioxi dants
and zinc had a probability of progression
to advanced AMD of
20
per cent across
five years compared with 28 per cent in
the placebo group.lyJampolzo autions that
one of the antioxidants, beta carotene,
should not be used in smokers
or
recent
former-smokers, as it may be associated
with a great er risk of lu ng cancer. Preven-
tion of the condition is anoth er research
goal, however, evidence remai ns inconclu-
sive with respect to the benefits of such
treatments as angioinhibitory drugs.
CONCLUSION
Th e earliest signs of exudative AMD may
be detected with routine retinal examina-
tion of patients with environmental and
ocular risk factors. These patients nee d to
be impressed with the i mport ance of hom e
monitoring and prompt attendance fol-
lowing the appearance of symptoms. Be-
cause current treatment options aim to
prevent vision loss rather than restore
vision, expedience of referral to a retinal
specialist while visual acuity is high allows
maximisation of treatment options and
reduct ion of severe visual acuity
loss.
More
patients are potentially treatable if th e
symptoms have been present less than two
weeks.g Knowledge
of
risk factors, likely
progression an d prognosis allows appro -
priate schedulingof reviews following oph-
thalmological assessment. Provision
of
appropriate low vision rehabilitation is
often required once a stabl e level of vision
is reached.
10.
Ciulla TA, Danis RP, Harris A. Age-related
macular degeneration: A review
of
experi-
mental treatments. Sun Ophthalmol 1998;
43: 134146.
11. Fine SL. Editorial. Photodynamic therapy
with verteporfin
is
effective for selected
patients with neovascular age-related macu-
lar degeneration.
Arch Ophthalmol 1999;
117: 1400-1402.
12. Bressler SB, Bressler NM, Fine SL, HillisA,
Murphy RP Olk RJ et al. Natural course of
choroidal neovascular membrdnes within
the foveal avascular zone in senile macular
degneration. AmJOphthalmol1982; 93: 157-
ACKNOWLEDGEMENTS
I would like to thank
D r
Adrian Bruce for
editorial comm ent a nd assistance with
photographs.
I
would also l ike to thank Dr
Alex Harper fo r contributin g Figures 2,3 a
and
3b.
REFERENCES
1
Soubrane
G,
Bressler
NM.
Treatment of
subfoveal choroidal neovascularisation in
age-related macular degeneration: focus on
clinical application of verteporfin photo-
dynamic therapy.
BrJ Ophthalmol2001;85:
483-495.
Evans J, Wormald R. Is the incidence of
registrable age-related macular degenera-
tion increasing? Br Ophthalmol 1996; 80:
9-14.
Mitchell P, Smith W, Attebo K, Wang JJ
Prevalence of age-related maculopathy in
Australia. The Blue Mountains Eye Study.
O#hthalmology 1995; 102: 1450-1460.
4.
Wolffsohn
J.
The changing face of the visu-
ally impaired: The Kooyong low vision clin-
ic's past, present and future. Optom Vis ci
1999; 76: 747-754.
5.
Bird AC, Bressler N M , Bressler SB,
Chisholm
IH,
Coscas
G,
Davis MD et al. An
international classification and grading sys-
tem for age-related maculopathy and age-
related macular degeneration.
S u r u
Ophthalmol 1995; 39: 367-374.
Klein R, Davis MD, MagliYL, Segal P, Klein
BEK, Hubbard L. The Wisconsin age-
related maculopathy grading system. Oph-
thalmology 1991; 98: 1128-1134.
Ferris
111
FL,
Fine
SL
Hyman L. Age-related
macular degeneration and blindness due to
neovascular maculopathy. Arrh Ophthalmol
1984; 102: 1640-1642.
8.
Macular Photocoagulation Study Group.
Five-year follow up of fellow eyes of pa-
tients with age-related macular degenera-
tion and unilateral extrafoveal choroidal
neovascularisation. Arch Ophthalmol 1993;
9. Sickenberg M. Early detect ion, diagnosis
and management of choroidal neovas-
cularisation in age related macular degen-
eration: The role of ophthalmologists.
Ophthalmologica 2001; 215: 247-253.
2.
3.
6.
7.
111: 189-199.
163.
13. Rhee DJ, Pyfer MF, eds. T he Wills Eye
Manual-Office and emergency room diag-
nosis and treatment of eye disease, 3rd ed.
Philadelphia: Lillincott, Williams and
Wilkins; 1999.
14. Young RW. Pathophysiologyof age-related
macular degeneration.
Suru
Ophthalmol
15. Green WR, Enger C. Age-related macular
degeneration histopathologic studies. Oph-
thalmology 1993; 100: 1519-1535.
16. McCarty
CA
Mukesh BN,
Fu
CL, Mitchell
P, WangJ, Taylor HR. Risk factors for age-
related maculopathy. The Visual lmpair-
ment Project.
Arch Ophthalmol 2001; 119:
17. Schwartz SD. Age-related maculopathy and
age-related macular degeneration. In:
Silverston B, Rosenthal BP, Lang MA, Faye
EE, eds. The Lighthouse Handbook on
Vi-
sion Impairment andvision Rehabilitation:
Vol 1 Vision Impairment. Oxford: Oxford
University Press; 2000:
85101
18.
Mandal N, Chisholm
IH.
Identifying the
proportion of age related macular degen-
eration patients who would benefit from
photodynamic therapy with verteporfin
(Visudyne).
Rr @hthalmol2002; 86: 118-
119.
19. The Age-Related Eye Disease Study Group.
A randomized, placebo-controlled, clinical
trial of high dose supplementation with
vitamins C and E, beta carotene, and zinc
for age-related macular degeneration and
vision
loss:
AREDS report No.
1.
Arch
Ophthalmol2001; 119: 1417-1436.
20. Jampol LM. Editorial. Antioxidants, zinc
and age-related macular degeneration.
Arch Ophthalmol2001; 119: 15331534.
1987; 31: 291-306.
1455-1462.
Author's address:
Sandra Harris
Victorian College of Optometry
374 Cardigan Street
Carlton VIC 3053
AUSTRALIA
Clinical and Experimental Optom etry
86.1
January 2003
56