J Clin Pathol 1993;46:177-179
Lymph node disease with lymphocyticabnormal chromatin clumping
in amyelodysplastic/myeloproliferative syndromeJ Gardais
AbstractA case of abnormal chromatin clumping(ACC) which arose
during the course of amyelodysplastic/myeloproliferative syn-drome
is described in a 61 year old womanwho died ofhaemorrhage 43 months
afterdiagnosis. Mature granulocytes exhibitedthe same nuclear
abnormality describedin other patients reported. Unusually,
shepresented with advanced splenomegalyand lymphadenopathy. This
case was thethird example ofACC in lymphocytes, thefirst with
clinically confirmed lymphade-nopathy.Diagnosis of this subset can
be based
on: older age; short duration of symp-toms; no specific
karyotypic damage;non-rearranged bcr; proliferative growthpattern
in vitro; numerous circulatingmyelocytes; profound
thrombocytopenia.
(7 Clin Pathol 1993;46:177-179)
A new variant ofmyelodysplastic syndrome hasrecently been
described. It comprises concom-itant cytopenias, proliferative
features, and, inparticular, abnormal clumping of chromatin(ACC) of
certain mature granulocytes. Thismorphological characteristic has
also beenobserved in medullary or circulating lympho-cytes in only
two patients.' We report anadditional case with the same
abnormality inlymphocytes within a lymphadenopathy, ararely
reported complication.
Laboratoire deCyto-h6matologie,Centre Departementalde
TransfusionSanguine d'Angers, 16boulevard Mirault, BP2208, F-49022,
AngersCedex 22 FranceJ GardaisCorrespondence to:Dr J
GardaisAccepted for publication7 August 1992
Case reportA 61 year old woman presented in March 1987with the
following peripheral blood picturehaemoglobin: 96 g/l mean
corpuscular volume(MCV) 93.9 fl, reticulocytes 37.5 x
109/1,anisocytosis, poikilocytosis, a white cell countof 3-3 x
109/1 with a normal differential, and aplatelet count of 51 x
109/l. She was other-wise entirely well and there were no
relevantmedical or family histories.
Physical examination indicated no abnor-mality apart from
pallor. Serum B,2, serumand red cell folate, and serum iron
concentra-tions were all normal as were a biochemicalscreen and
neoplastic markers. There was apolyclonal increase in
immunoglobulin con-centrations. A bone marrow aspirate
showederythroid hyperplasia without sideroblastosiswith increased
cellularity and 15% blasts. Itwas considered to be morphologically
con-sistent with non-sideroblastic refractory anae-mia with excess
of blasts. She received low
dose aracytine treatment which was discon-tinued after only four
days because of thesudden appearance of a severe throm-bocytopenia
and a fall in haemoglobin concen-tration to 60 g/l. It was felt
that simplesupportive treatment would be appropriateand she was
maintained on regular bloodtransfusions. In July 1987 a further
bonemarrow aspirate showed a reduced blastosis.She was admitted
again in February 1988
with 10% blasts in the peripheral blood. Arepeat bone marrow
examination showed 24%blasts. Seven days of intravenous
aclacinomy-cin and oral thioguanine was started. Despiteclinical
improvement she did not achievecomplete remission. Hydroxyurea 500
mg/dayand thioguanine 50 mg/day, then 25 mg/daywere given. During
follow up, however, heranaemia and thrombocytopenia
persisteddespite deferred chemotherapy; the white cellcount rose to
14-7 x 109/1 with 6-5% blasts,6-5% promyelocytes, 31% myelocytes,
18%metamyelocytes, 10-5% monocytes, 12-5%neutrophils and 15%
lymphocytes in April1988. Chronic myelomonocytic leukaemia(CMML)
was diagnosed. The haematologicalpicture over the subsequent period
was charac-terised by a slow progressive increase in whitecells and
the persistence of monocytosis,immature granulocytic cells, and
blastosis inthe peripheral blood.
In October 1989 a repeat bone marrowaspirate disclosed an
increase in blast cells to37% with abnormalities of mature
gran-ulocytes (fig 1). Neutrophils and metamyelo-cytes were
characterised by chromatinclumping into large blocks separated
byclear zones, mimicking nuclear fragmentationand nuclear membrane
disruption. Theseabnormalities were not seen in myelocytesand
promyelocytes. Degranulation was alsoobserved in mature forms.
Moderate dyseryth-ropoiesis was observed but megakaryocyteswere
absent. A slight monocytosis suggestedthe diagosis of CMML in
transformation.Chromosomal analysis of bone marrow cells,using
synchronisation and R banding, showeda 46XX karyotype in five
metaphases exam-ined. Profound thrombocytopenia persisted,and
between January 1990 and July-August1990 the white cell counts
fluctuated from 44to 68-7-116 x 109/1 with 6, 18, and 23%blasts and
4, 23, and 9% monocytes, respec-tively. There was no perceptible
response todanazol. Meanwhile, the patient developed aprogressive
splenomegaly and cervical lympha-denopathies. A cytogram of the
latter exhibitedthe same abnormal mature granulocytes found
177
on July 2, 2021 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.46.2.177 on 1 F
ebruary 1993. Dow
nloaded from
http://jcp.bmj.com/
Gardias
.. ...0
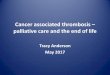
Figure 1 Mature granulocytes in peripheral blood presenting
large blocks of chromatinseparated by clear zones
(May-Griunwald-Giemsa).
..
,
.,~ ~ ~ ~... ...c
.:
.} ...:.......::
Figure 2 Metaplasia of lymph node with lymphocytes exhibiting
the same ACC as inmature granulocytes (May-Grainwald-Giemsa).
in bone marrow; the lymphocytes were charac-terised by the
similar ACC (fig 2). Because ofsevere thrombocytopenia and allogen
immuni-sation to platelet concentrates, chemotherapywas deferred.
However, her spleen increased insize, repeated bleedings required
numerousblood transfusions and, in October 1990, shedied 43 months
after diagnosis with signs ofdigestive haemorrhage. Death occurred
onlyone year after the diagnosis of ACC had beenmade. Postmortem
examination was not per-formed.
DiscussionThe nature ofACC has been discussed before.DNA
analysis failed to reveal any hyperploidclone in two previous
cases. Therefore, forFelman,' this clumping does not correspond
tochromatin increase, but is probably related toan abnormal
distribution within the nucleusand a modification of the
heterochromatin:euchromatin ratio. No systemic
karyotypicabnormality was found in the same study. Inanother report
the karyotype was also normaland no consistent rearrangement of the
bcr wasidentified after isolation of high molecularweight DNA and
Southern blotting analysis
from the patient's peripheral blood.2 Aspointed out by Brizard,3
we cannot argueagainst a case of "atypical chronic
myelocyticleukemia (CML)" where non-rearranged bcridentification
was obviously demonstrated.4The case reported here resembles all
the
other 19 described to date in severalrespects."2 5 ACC was seen
mainly in neu-trophils, band forms and
metamyelocytes.Myelodysplastic features were also evident.ACC was
absent at diagnosis and examinationof lymphocytes contrasted with
later abnor-malities. However, ACC appeared withinlymphadenopathy
during the course of thedisease. Such a clinical complication
hasalready been reported in CMML.' l" Lym-phadenopathy was rarely
recognised in CMLmany years ago. 2 Until now, ACC in leuco-cytes
had been identified from haematologicalcriteria among either
myelodysplastic syn-dromes (MDS), or "atypical CML", closelyrelated
to true CML and CMML. That thisfeature has been reported in an
acute phase ofCML7 and that the well known CMML hasbeen included in
MDS by the FAB group" isconfusing. In one of the two cases
previouslydescribed by Gustke,6 where lymphocytes hadno abnormal
chromatin, metaplasia of thespleen, liver, and lymph nodes at the
time of asplenectomy was observed.
Evidence of the underlying clonality ofhaematopoiesis in MDS has
been establishedby cytogenetic, glucose 6-phosphate dehydro-genase
(G6PD), or, more recently, restrictionfragment length analysis.'4
8. Prchal et alpostulated that the clonal abnormality
inmyelodysplasia involves a stem cell precursorof both myeloid and
lymphoid cell lines. 5 Thisis supported by investigation of a
patient withmyelodysplasia who was heterozygous forG6PD; the same
isoenzyme was present in allhaematopoietic cells, including
lymphocytes.Nowadays, there is a general agreement con-cerning the
clonal nature of all malignantblood disorders, resulting from
neoplastictransformation of a pluripotent stem cell,regardless of
morphological subtypes. Conse-quently, it raises the possibility of
lymphoidlineage involvement. This "unitary theory" issustained by a
spectrum of several remarkablestudies, clinical observations, or
unique asso-ciations: Wallis and Joyner described a patientwith
chronic lymphocytic leukaemia (CLL)untreated for five years who
subsequentlydeveloped acute myeloid leukaemia.'0 Theseauthors
pointed out that this secondary diseasemay occur as a result of
reduced immunecompetence consequent on CLL. Severalexamples of
associations between myeloid dis-turbances, as observed in MDS, and
immunedysfunction have been published. Acute lym-phoblastic
leukaemia following MDS,20 21association of lymphoma,22 or
immunologicalabnormalities23 24 with MDS support the con-cept of
lymphocyte down-regulation of a myo-loid clone. Bastion et al also
described a patientin whom MDS coexisted with CLL for morethan nine
years.25 The patient's serum inhib-ited the patient's own
granulocyte-macrophagecolony forming units. Furthermore, T cell
178
on July 2, 2021 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.46.2.177 on 1 F
ebruary 1993. Dow
nloaded from
http://jcp.bmj.com/
Lymph node disease with lymphocytic abnormal chromatin clumping
in MDS
receptor 5 gene rearrangement has been shownin CMML.26 On the
other hand, unstable andreversible (to myeloid cells)
differentiation hasbeen found in mature T lymphoid
leukaemiacells.27 In our case ACC in lymphocytes withina
lymphadenopathy would provide an addi-tional argument supporting
the fact that, inMDS or related disorders, progenitor cells
arecapable of clonal differentiation along avariety of pathways.
The recombination eventsrequired for gene rearrangement demand
thatthe chromatin be "open" and accessible torecombinant enzymes"
at the appropriatephase of the developmental cycle. Thus
animbalance in the distribution of the two chro-matins could
sometimes exceptionally befound at microscopic level, as in our
caseand other ACC examples. Lymphadenopathywith lymphocytes
exhibiting ACC is a newcharacteristic which contributes to support
theview that this particular myelodysplastic/myeloproliferative
syndrome is a homogenousgroup of disorders with, overall, poor
prog-nosis" among heterogeneous subsets of multi-potent stem cell
derived blood diseases. Thissyndrome is placed precisely between
myelo-dysplastic and myeloproliferative ones and ischaracterised by
the coexistence of somemixed features suggesting both. It
representsan atypical and rare expression of a lingeringmultiphasic
panmyelopathy that involves allproducts of the marrow stem cell.30
It perhapsindicates that the same marrow insult canmanifest itself
in several ways and that an initialoncogenic event selects a clone
of stem cells,which retain the capacity to differentiate intoboth
lineages, these being marked by func-tional abnormalities. One of
them exhibitschromatin disturbance, accounting for a newevidence of
a common lymphoid and myeloidprogenitor cell. However, whether ACC
inlymphoid cells in lymphadenopathy in ourpatient rather represents
proof of the commonstem cell origin of two myeloid and
lymphoidhaematological manifestations or a morpho-logical
consequence of immune dysregualtionremains to be determined.
In conclusion, our patient's clinical courseand haematological
symptoms complete thedefinition of this newly described subset.
Fin-ally, the diagnosis of this syndrome is based onthe following:
older age; short duration; nospecific karyotypic damage;
non-rearrangedbcr; proliferative growth pattern in vitro;numerous
circulating myelocytes; profoundthrombocytopenia preventing
chemotherapy,dysplastic features associated with ACC of
allleucocytes, chiefly mature granulocytes; possi-bility of
hepatosplenomegaly and, hereafter,lymphadenopathy with ACC of
lymphocyteseventually appearing in the course of thedisease.
We are grateful to Sylvie Maillard for typing the manuscript
andRobert Perry for reviewing the English text.
1 Felman P, Bryon PA, Gentilhomme 0, et al. The syndromeof
abnormal chromatin clumping in leucocytes: a myelo-dysplastic
disorder with proliferative features? Br J Hae-matol
1988;70:49-54.
2 Invernizzi R, Custodi P, De Fazio P, et al. The syndrome
ofabnormal chromatin clumping in leucocytes: clinical andbiological
study of a case. Haematologica 1990;75:532-6.
3 Brizard A, Huret JL, Lamotte F, et al. Three cases
ofmyelodysplastic-myeloproliferative disorder with abnor-mal
chromatin clumping in granulocytes. Br Jf
Haematol1989;72:294-5.
4 Wiedermann LM, Karchi KK, Shivi MKK, et al. Thecorrelation of
breakpoint cluster region rearrangementand p21OPhl/abl expression
with morphological analysisof Ph-negative chronic myeloid leukemia
and othermyeloproliferative diseases. Blood 1988;71:349-55.
5 Morel P, Bryon PA, Guyon JM, et al. Hemopathie malignede type
aplastique avec anomalies nucleairs majeures desgranulocytes. Sem
H6p (Paris) 1968;49:3026-8.
6 Gustke SS, Becker GA, Garancis JC, et al. Chromatinclumping in
mature leucocytes: an hitherto unrecognizedabnormality. Blood
1970;35:637-58.
7 Winter JN, Variakojis D, Gaynor ER, et al. Low-dosecytosine
arabinoside (Ara-C) therapy in themyelodysplastic syndromes and
acute leukemia. Cancer1985;56:443-9.
8 Weil SC, RoseVL. A variant myelodysplastic syndrome
withmultilineage pelgeroid chromatin. Am Jf Clin Pathol1986;85:
176-9.
9 Jaen A, Irriguible D, Milla F, et al. Abnormal
chromatinclumping in leucocytes: a clue to a new subtype
ofmyelodysplastic syndrome. Eur Jf Haematol 1990;45:209-14.
10 Bizet M, Callat MP, Goasguen J, et al. Chronic myelomon-cytic
leukemia (CMML) with lymphodenopathy. F. In:Schmalz F, Muffi GJ,
eds. Myelodysplastic syndromes.Berlin: Springer Verlag,
1992:140-6.
11 Tefferi A, Hoagland HC, Therneau TM, et al.
Chronicmyelomonocytic leukemia: natural history and
prognosticdeterminants. Mayo Clin Proc 1989;64:1246-54.
12 Scott RB. Leukaemia (chronic myeloid leukaemia).
Lancet1957;i: 1099-103.
13 Bennett JM, Catovsky D, Daniel MT, et al. Proposals for
theclassification of the myelodysplastic syndromes. Br JHaematol
1982;51:189-99.
14 Nowell PC. Cytogenetics of preleukemia. Cancer GenetCywogenet
1982;5:265-78.
15 Prchal JT, Throckmorton DW, Carrol AJ, et al. A
commonprogenitor for human myeloid and lymphoid cells.
Nature1978;274:590-1.
16 Raskind WH, Tirumali N, Jacobson R, et al. Evidence for
amultistep pathogenesis of a myelodysplastic syndrome.Blood
1984;63:1318-23.
17 Abkowitz JL, Fialkow PJ, Niebruge DJ, et al.
Pan-cytocytopenia as a a clonal disorder of a
multipotenthematopoietic stem cell. J Clin Invest
1984;73:258-61.
18 Kere J, Ruutu T, de la Chapelle A. Monosomy 7 ingranulocytes
and monocytes in myelodysplastic syn-drome. N Engl J Med
1987;316:499-503.
19 Wallis JP, Joyner MV. Acute myeloid leukaemia developingin a
patient with longstanding untreated chronic lym-phocytic leukaemia.
Acta Haematol 1986;75:229-31.
20 Inoshita T. Acute lymphoblastic leukemia following
myelo-dysplastic syndrome. Am J Clin Pathol 1985;84:233-7.
21 Stark AN, Scott CS, Bhatt B, et al. Myelodysplasticsyndrome
coexisting with acute lymphoblastic leukaemia.J Clin Pathol
1986;39:728-30.
22 Wajima T, Mukhopadhyay M. Co-existing myelodysplasticsyndrome
and malignant lymphoma with IgA monoclonalgammopathy terminated in
acute myeloid leukemia shor-tly after treatment of malignant
lymphoma and prostatecancer. Blood 1991;78(suppl 1):462a.
23 Copplestone JA, Mufti GJ, Hamblin TJ, et al. Immun-ological
abnormalities in myelodysplastic syndromes. BrJHaematol 1989;63:
149-59.
24 Colombat PH, Renoux M, Lamaguere JP, et al. Immun-ologic
indices in myelodysplastic syndromes. Cancer1988;61:1075-81.
25 Bastion Y, Thomas X, Felman P, et al. High risk
myelodys-plastic syndrome coexistent with chronic
lymphocyticleukemia for more than 9 years: inhibition of the
myeloidclone by the lymphoid clone? Leukemia 1991;5:1006-9.
26 Provan AB, Majer RV, Smith AG, et al. Chronic myelomon-ocytic
leukamia associated with T cell receptor £5 generearrangement. J
Clin Pathol 199 1;44:344-5.
27 Griesinger F, Jansen B, Kersey JH. Differentiation inmature T
lymphoid leukemia cells is unstable andreversible to myeloid cells,
without the involvement of acommon stem cell. I Immunol
1991;147:3336-41.
28 Boehm T, Rabbitts TH. A chromosomal basis of
lymphoidmalignancy in man. EurJ7 Biochem 1989;185:1-17.
29 Varma N, Dash S, Marwaha N, et al. A case ofmyelodysplastic
syndrome with abnormal chromatinclumping in leucocytes. Brj
Haematol 1989;73:135.
30 Uinman JW, Bagby GC. The preleukemic syndrome (hemo-poietic
dysplasia). Cancer 1978;42:854-64.
179
on July 2, 2021 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.46.2.177 on 1 F
ebruary 1993. Dow
nloaded from
http://jcp.bmj.com/