Embed Size (px)
Citation preview

IV./5. Chapter: Shoulder dislocation
Fundamental information of the epidemiology, diagnosis, workupand therapy of shoulder dislocation is given in the present chapter.
IV./5.1.: DefinitionShoulder dislocation occurs as the humeral head leaves completely theglenoid fossa. Anterior or antero-inferior dislocation is the most commonform reaching about 97 % of all cases. Posterior luxation can be found in 2%, leaving the remaining 1 % to inferior (luxatio erecta), superior orintrathoracic dislocation.
IV./5.2.: EpidemiologyThe shoulder has the largest range of movement (ROM), but it pays theprice by being the most commonly dislocating joint at the same time. Dueto different studies, shoulder dislocation affects 1.7-2% of the population.
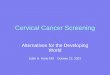
IV./5.3.: EtiologyDepending on the direction of the dislocation, the mechanism of the injuryis different. Antero-inferior dislocation usually occurs when the patient fallsdown with the arm in abduction and external rotation, or by throwingsomething as the shoulder is held in the same position. Luxation generallytears off the antero-inferior part of the capsule from its glenoid origintogerther with the labrum. This type of labral tear is called Bankart laesion(1. Figure). The younger is the patient at the time of the first dislocation, thebigger the chance for a recurrent doslocation. After reccurent luxation thejoint can become instable, so it generally dislocates without sufferring amajor trauma, or without any major force. In fact, luxation can occur bythrowing an object, putting on a coat or by any other movement that forcesthe joint in abduction and external rotation. Posterior dislocation occursusually as the patient falls down with the arm in internal rotation andadduction, or it can develop – sometimes also bilaterally - during epilepticseizures. The very rare inferior luxation (luxatio erecta) is caused by anaxial load affecting the arm while held in an extremely abducted position.This type is commonly associated with traffic injuries.
Figure 1.: Arthroscopic image of a right shoulder viewed from the back can be seen. Thearthroscopic probe holds the labrum as it is torn off of the glenoid rim. (L-labrum, G-glenoid,
H-humeral head)

IV./5.4.: PresentationPatients complain about shoulder pain, that develops after a traumatic event(fall, throwing, sudden abduction and external rotation, epileptic seizure,etc.). Decreased and painful ROM is always presented, numbness aroundthe shoulder or in the hand is not uncommon. The clinical occurence of theleast common type of dislocation is the most characteristic: in case of aninferior shoulder dislocation the arm is in total adduction, while the elbowis held flexed behind the head. In case of an atero-inferior dislocation theglenoid fossa is empty, the axis of the arm points towards the armpit, thearm is held in slight external rotation and abduction. Posterior dislocation isgeneraly featured by adduction and internal rotation, sometimes thehumeral head can be palpated posteriorly under the acromion. If the patientis presented after reduction, instead of dislocation only the type ofinstability can be diagnosed. Antero-inferior instability is characterized bythe patients’ apprehension of the externaly rotated and adbucted position ofthe arm – this is called the anterior apprehension test. If the patient hassimilar complaint in internal rotation and adduction (posterior apprehensiontest), it is a sign of posterior instability.
IV./5.5.: WorkupPlain radiographs should be performed (AP, Y and axillary views) wherethe empty glenoid fossa, the dislocated humeral head and any possiblefractures can be detected. (2. Figure) The most common fracture iscompression of the postero-superior part of the head (Hill-Sachs laesion),caused by the glenoid rim as the head is in the antero-inferior dislocatedposition. In case of a posterior dislocation, the same mechanism causesantero-superior comression (reverse Hill-Sachs laesion) on the head. (3.Figure) Depending on the patients’ age, rotator cuff injury occurs in 40-80% of dislocations. The best way to evaluate the cuff is MRI, that should beperformed after dislocation. MRI also provides information about thelabrum and the capsule. If neurological or vascular injury is suspected,electromyography or angiography may be necessary.
Figure 2.: Acute antero-inferior dislocationcan be seen on the AP radiograph. The
humeral head is located anteroinferiorly tothe glenoid, which is empty.
Figure 3.: Axillary view of a posteriorly dislocatedshoulder. The humeral head is behind the glenoid,the glenoid rim causes compression fracture on the
posterior articular surface of the head.
IV./5.6.: DiagnosisBased on the history, physical signs and imaging studies.

IV./5.6.1.: Differential diagnosis
Acromioclavicular injury, clavicule fracture, humeral fracture, rotator cufftear
IV./5.7.: TreatmentIn case of acute dislocation:
Closed reduction: If necessary performed in general anesthesia.The arm is held in a splint for 3 weeks, afterwards most preferablyin 90 degrees of external rotation. After 3 weeks physiotherapy ismandatory.
Open reduction: In neglected cases closed reduction usually is notpossible, therefore open reduction is needed
In case of instability
Arthroscopic stabilization: Refixation of the Bankart injury isusually carried out by arthroscopic procedure. Inferior capsularshift also can be performed during the surgery.
Open stabilization: In case of a recurrent dislocation, or arecurrence after previous surgery, open stabilization is the methodof choice. The labrum and the capsule is reattached to the glenoidduring the procedure, commonly together with bone transplantation(iliac crest, coracoid process). Posterior instability is also treated byopen surgery. Postoperative immobilization by a sling andphysiotherapy is necessary.
ReferencesObligatory:
- Szendrői Miklós: Orthopedics 25.6. chapter
Optional:
- http://emedicine.medscape.com/article/823843-overview



![TO BE PUBLISHED IN THE UNITED STATES DISTRICT … · The prognosis for this gentleman was really poor mainly ... dislocating shoulder was a problem[] ... hospital early because it](https://img.pdfslide.us/doc/110x75/5afba4897f8b9a32348f5267/to-be-published-in-the-united-states-district-prognosis-for-this-gentleman-was.jpg)