Embed Size (px)
Citation preview

“It’s all in your head”
“It’s all in your head”
Kyle McLaughlinSept. 1, 2005
Diagnostic Imaging Rounds
Kyle McLaughlinSept. 1, 2005
Diagnostic Imaging Rounds

Case of R.M.Case of R.M.
• 28 M, 3 mos Hx of Headache• Headache: diffuse, constant, 4-10/10• No previous Hx of H/A• Tx for HTN and migraine with no
success• Booked for H/A clinic by Family MD
• 28 M, 3 mos Hx of Headache• Headache: diffuse, constant, 4-10/10• No previous Hx of H/A• Tx for HTN and migraine with no
success• Booked for H/A clinic by Family MD

Case of R.M.Case of R.M.
• What else do you want to know?• What else do you want to know?

Case of R.M.Case of R.M.
• H/A worse with lying down, late at night and early a.m.
• Assoc. Sx– Nausea– Dizziness– Vague diplopia– Word finding
difficulties– Mild personality
change
• H/A worse with lying down, late at night and early a.m.
• Assoc. Sx– Nausea– Dizziness– Vague diplopia– Word finding
difficulties– Mild personality
change
• PMHx- healthy• Meds- none, NKDA• FHx- unremarkable• P/E:
– Unremarkable except poor R sided Upper Extremity Cerebellar testing
• PMHx- healthy• Meds- none, NKDA• FHx- unremarkable• P/E:
– Unremarkable except poor R sided Upper Extremity Cerebellar testing

What next?What next?
• DDx?• Investigations?• Imaging?
– Why?
• DDx?• Investigations?• Imaging?
– Why?



What now?What now?
• DDx?• Disposition and Management?
• DDx?• Disposition and Management?

Case of R.M.Case of R.M.
• Diagnostic Imaging:– CT head- Dx with astocytoma– MRI- low grade glioma
• Diagnostic Imaging:– CT head- Dx with astocytoma– MRI- low grade glioma

Case of R.M.Case of R.M.
• Transferred to Neurosurgery, started on Dexamethasone
• Craniotomy for excision of brain tumour 3 days later
• Negative culture• Biopsy result: primitive
neuroepithelial tumour
• Transferred to Neurosurgery, started on Dexamethasone
• Craniotomy for excision of brain tumour 3 days later
• Negative culture• Biopsy result: primitive
neuroepithelial tumour

Headaches and Brain Tumours
Headaches and Brain Tumours
• Headache present in 50-60% of brain tumours
• Pain secondary to:– Vessel traction, distention and dilation– Direct pressure on CN with pain
afferents– Inflammation around pain sensitive
structures (venous sinuses, portion of the dura, dural arteries, cerebral arteries)
• Headache present in 50-60% of brain tumours
• Pain secondary to:– Vessel traction, distention and dilation– Direct pressure on CN with pain
afferents– Inflammation around pain sensitive
structures (venous sinuses, portion of the dura, dural arteries, cerebral arteries)

Headache Red FlagsHeadache Red Flags

Headache Red FlagsHeadache Red Flags• New or changed • Exertional• Onset at night or early a.m.• Progressive in nature• Fever or systemic Sx• Meningismus• Neuro Sx• Valsalva maneuver worsens• Age: New onset >50 y.o. or in children
• New or changed • Exertional• Onset at night or early a.m.• Progressive in nature• Fever or systemic Sx• Meningismus• Neuro Sx• Valsalva maneuver worsens• Age: New onset >50 y.o. or in children

Conditions to Rule OutConditions to Rule Out• Space occupying lesion• Meningitis, encephalitis• Stroke• Subarachnoid hemorrhage• Systemic illness (thyroid, HTN,
pheochromocytoma, etc.)• Temporal arteritis• Traumatic head injuries• Serious ophthalmologic and otolaryngologic
etiologyPurdy, A., Kirby, S. Headaches and brain tumours. Neuro Clin Am 22 (2004) 39-53.
• Space occupying lesion• Meningitis, encephalitis• Stroke• Subarachnoid hemorrhage• Systemic illness (thyroid, HTN,
pheochromocytoma, etc.)• Temporal arteritis• Traumatic head injuries• Serious ophthalmologic and otolaryngologic
etiologyPurdy, A., Kirby, S. Headaches and brain tumours. Neuro Clin Am 22 (2004) 39-53.

DDx of brain lesionDDx of brain lesion
• Tumour• Pus• Blood
• Tumour• Pus• Blood

TumourTumour
• Adults– Infratentorial:
• Mets (20-30%)• Schwannoma (6%)
– Supratentorial:• Astrocytoma (40-50%)• Mets (20-30%)• Meningioma (15%)• Oligodendroglioma (5%)
• Adults– Infratentorial:
• Mets (20-30%)• Schwannoma (6%)
– Supratentorial:• Astrocytoma (40-50%)• Mets (20-30%)• Meningioma (15%)• Oligodendroglioma (5%)

AstrocytomaAstrocytoma

MeningiomaMeningioma

PusPus
• Brain abscess– Local spread (i.e. OM, mastoiditis,
sinusitis)– Hematogenous spread (i.e.
immunosuppressed, lung abscess, empyema)
– Dural disruption – Granuloma (TB, sarcoid)
• Brain abscess– Local spread (i.e. OM, mastoiditis,
sinusitis)– Hematogenous spread (i.e.
immunosuppressed, lung abscess, empyema)
– Dural disruption – Granuloma (TB, sarcoid)

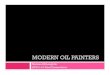
Brain Abscess (CT with contrast)
Brain Abscess (CT with contrast)

BloodBlood
• Hematoma/hemorrhage– Epidural, subdural, SAH, etc.
• Vascular Abnormality– Aneurysm, AV malformation
• Ischemic cerebral infarction
• Hematoma/hemorrhage– Epidural, subdural, SAH, etc.
• Vascular Abnormality– Aneurysm, AV malformation
• Ischemic cerebral infarction





Indications for imaging in headache
Indications for imaging in headache
• Sudden onset of “worst h/a of life”• New h/a in HIV +• A h/a that:
– Worsens with exertion– Assoc with decreased alertness or mental status
change– Awakens from sleep– Changes in pattern over time– Assoc with papilledema– Assoc with focal neurological deficit Mettler: Essentials of Radiology, 2nd ed, 2005
• Sudden onset of “worst h/a of life”• New h/a in HIV +• A h/a that:
– Worsens with exertion– Assoc with decreased alertness or mental status
change– Awakens from sleep– Changes in pattern over time– Assoc with papilledema– Assoc with focal neurological deficit Mettler: Essentials of Radiology, 2nd ed, 2005

Imaging choicesImaging choices
• CT– More accessible, quicker– Good initial scan in ruling out many
etiologies (i.e.hemorrhage)
• MRI– Superior soft tissue contrast– Good for further differentiation of:
• Brain tumour• Undiagnosed intracranial lesions
• CT– More accessible, quicker– Good initial scan in ruling out many
etiologies (i.e.hemorrhage)
• MRI– Superior soft tissue contrast– Good for further differentiation of:
• Brain tumour• Undiagnosed intracranial lesions