-
It’s Not Just Drug Addiction!
Howard Wetsman MD DFASAMChief Medical Officer
Townsend Treatment Centers@addictiondocMD
[email protected]
-
Let’s Start With Why
• What I want• Can it happen?
-
We Don’t Remember
-
How Will We Do It
• The Goal• “To make more recovering people now
and in the future”
• But why hasn’t this happened already?
• “Our problems, we think, are of our own making.”
-
Words And Names Are Important
• Imagine you’re a congressman– “Substance abuse”– “Addiction
to…”– “Illness”
• Imagine you are an insurance company
• Imagine you are a patient
-
How Many Addictions Are There?
• DSM5 lists 10 SUDs and Gambling• The problem of “Addiction
to…”• The DSM paradigm invented in 1981• ASAM’s Definition in
2011
-
ASAM’s Definition
• Addiction is a primary, chronic disease of brain reward,
motivation, memory and related circuitry. Dysfunction in these
circuits leads to characteristic biological, psychological, social
and spiritual manifestations. This is reflected in an individual
pathologically pursuing reward and/or relief by substance use and
other behaviors.
• ASAM Apr, 2011
-
A New System
• We need a new system based on this illness as it is in nature,
not as we wish it to be
• What are the questions this new system should answer
-
Questions• If addiction is a disease, where’s the
broken bone?
• If addiction isn’t limited to drugs, how do we stay sober?
• If addiction is chronic, when does treatment end?
• If addiction is progressive, what hope do we have?
-
What’s the Drug?
0
5
10
15
20
25
30
1900 1915 1930 1945 1960 1975 1990 2005
Gall
on
s p
er
10 P
eople
Alcohol Consumption Over Time
-
What’s the Drug?
0
5
10
15
20
25
30
35
40
45
50
1900 1920 1940 1960 1980 2000Hun
dre
ds o
f C
igare
ttes p
er
Pers
on
Nicotine Consumption Over Time
-
What’s the Drug?
0
5
10
15
20
25
1900 1905 1910 1915 1920 1925 1930 1935 1940 1945 1950
Abstr
act
Num
bers
On
ly f
or
Scale
Nic-ETOH Dopamine Load Over Time
-
What’s a Drug?
0
5
10
15
20
25
1940 1950 1960 1970 1980 1990 2000 2010
Nic
-ET
OH
Dopam
ine L
oad
Year
Nic-ETOH Dopamine Load
-
What’s a Reward?
0
5
10
15
20
25
30
35
40
45
1960 1970 1980 1990 2000
Comparison of Calories and Nic-ETOH Dopamine Load Over Time
Dopamine Load
1000 Cal per Person
-
Let’s Play Whack-a-Mole
0
200
400
600
800
1000
1200
0
10
20
30
40
50
60
7019
50
195
2
195
4
195
6
195
8
196
0
196
2
196
4
196
6
196
8
1970
1972
1974
1976
1978
198
0
198
2
198
4
198
6
198
8
199
0
199
2
199
4
199
6
199
8
20
00
20
02
20
04
20
06
20
08
20
10
Opioid Prescriptions Dispensed by US Retail Pharmacies IMS
Health, Vector One: National, years 1991-1996, Data Extracted 2011.
IMS Health, National Prescription Audit, years 1997-2013, Data
Extracted 2014. Nicotine, EtOH, HFCS data from USDA data
tables.
-
Let’s Play Whack-a-Mole
0
200
400
600
800
1000
1200
0
20
40
60
80
100
1201950
1952
1954
1956
1958
1960
1962
1964
1966
1968
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
Opioid Prescriptions Dispensed by US Retail Pharmacies IMS
Health, Vector One: National, years 1991-1996, Data Extracted 2011.
IMS Health, National Prescription Audit, years 1997-2013, Data
Extracted 2014. Nicotine, EtOH, HFCS data from USDA data
tables.
-
From NIDA
-
Shift Gears
• Back to the future
-
Silkworth - Allergy
• Allergy - “We believe, and so suggested a few years ago, that
the action of alcohol on these chronic
alcoholics is a manifestation of an allergy; that the
phenomenon of craving is limited to this class and
never occurs in the average temperate drinker.”• Alcoholics
Anonymous page XXVIII
-
Silkworth – Base State
• Base State - “They are restless, irritable, and discontented,
unless they can again experience the
sense of ease and comfort which comes at once by
taking a few drinks – drinks which they see others
taking with impunity.”• Alcoholics Anonymous page XXVIII
-
Feedback Loop
-
Cue Induced Craving
GL
U
Amygdala
-
Dopamine Tone
• Factors– Dopamine Release– Dopamine Receptor number and
function– Time
-
What Medications Can Do
• Increase Dopamine Release• Increase Time• But we have no
medication for
increasing receptors
-
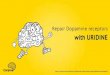
Stress and Dopamine Receptors
Social Dominance in Monkeys: Dopamine Receptors and Cocaine
Self-Administration Morgan et al, Nature Neuroscience 2002
Coincidentally, what do you get from an AA meeting?
Socially Housed
Housed in Isolation
Socially Housed
-
Attachment From the Spike
• Dangerous or risky behavior• Staying up late or sleeping in•
Being the center of attention• Being liked• Making someone smile•
Completion of a hard task• Sexual climax• Taking in food
Laviola G, et al. Risk-taking behavior in adolescent mice:
psychobiological determinants and early epigenetic influence.
NeuroSci and Biobehav Rev 27 (1-2): 19-31.Volkow ND, et al. Sleep
Deprivation Decreases Binding of [11C]Raclopride to Dopamine D2/D3
Receptors in the Human Brain. Journal of Neuroscience 28(34):
8454-8461.Martinez D, et al. Dopamine Type 2/3 receptor
availability in the Striatum and Social Status in Hjman Volunteers.
Bio Psych 67 (3): 275-278.Hsu DT, et al. Response of the mu-opioid
system to social rejection and acceptance. Mol Psych (20 August
2013) doi:10.1038/mp.2013.96Iwase M et al. Neural substrates of
human facial expression of pleasant emotion induced by comic films:
A PET study. NeuroImage, 17:758-768. Wassum KM, et al. Phasic
mesolimbic dopamine signaling precedes and predicts performance of
a self-initiated action sequence task. Bio Psych
71(10):846-54.Komisaruk BR and Whipple B. Functional MRI of the
Brain During Orgasm in Women. Brain Research 1024.1 (2004):
77-88.Wang GJ, et al. Enhanced striatal dopamine release during
food stimulation in binge eating disorder. Obesity
19(8):1601-8.
-
How Do We Stay Sober
• With brain definition we stop looking outside and start
looking inside
• With midbrain localization we stop looking to our cortex for a
solution
• Good news is, that part of the system already exists in
12-step and other recovery cultures
-
Outside vs Inside
• Is it about alcohol, cocaine, opiates, or is it about my
seeking to feel better?
• Less focus on what I’m doing and more focus on why
• Less focus on an absolute and more focus on progress
-
Cortex vs Midbrain• Historically, we’ve sought ways to have
the cortex override the midbrain
• But now that we understand that the midbrain feeds the cortex
we need to refocus
• Less about conscious thought and more about behavioral change
to induce conscious change
• More about behaviors that keep dopamine tone normal
-
But We Already Knew That
• “You can’t think your way into new behaviors but you can
behave your way into new thinking.”
• “Meeting makers make it.”• “We all have 24 hours”
-
What Never Ends?
• The goal of inpatient treatment is to create an outpatient
• The goal of outpatient treatment is to create a person in
recovery
• The goal of recovery is to live long enough to die of
something else
-
The Role of the Professional
• Intensive treatment phase• Monitoring recovery, not just drug
use• Quickly step back in when needed
-
The Disease Progresses
• As we age we lose VTA cells and DA receptors
• If we live long enough we’ll all get addiction
• So what hope do we have?
-
A Lot
• Yes it progresses but so does recovery– Peeling the onion–
Growing in spirit
• Give old-timers permission to get treatment
• There’s a lot we can do medically for people with good
recovery and older brains
-
The Future
• Genetics• Microbiome• Non-medical biological brain
treatments
-
Peek at Genetics
The medical goal is to normalize hedonic function and suppress
symptoms enough
so that the patient can hear the message of the
non-pharmacologic part of
treatment
5HTNIC
-
The Mission
• To end addiction as a problem in America in my life time (30
years)
-
How to Achieve the Mission• Can’t cure it today• Get everyone
with addiction into
recovery from addiction
• But 10-20% of the country has addiction which is up to 66
million people
• We aren’t going to get them all in recovery with the cottage
industry we have
-
So We Need a New System
• Industrial in scale• Replicable• Easily taught• Addresses
treatment and prevention
on both individual and societal levels
• Efficient in execution in that it doesn’t take sustained
effort
-
The Goal
• To create more recovering people now and in the future.
– Safety– Courtesy and respect– Excellent care– Tell the world–
Expand the system
-
Safety
• Addiction is a dangerous place to be. People have their guards
up, and they need to know that they can safely let their guard
down
• That means that we have to take responsibility for safety at
every level of care
-
Courtesy and Respect
• A patient isn’t going to get as much out of treatment if they
have a lowered dopamine tone. When we treat someone with less than
full respect and courtesy we lower their dopamine tone
• There are enough places in the world where our patients can
get their DA tone lowered
-
Excellent Care
• Cutting edge, state of the art, focused, individualized care
in collaboration with the patient at all levels of care
-
Tell The World
• Why do we have accreditation?• Why not just expose our
outcomes?• Tell the world what we’re doing to
attract more people who need our help as well as the interest of
others who currently don’t know they can help
-
Expand The System
• To get more recovering people we’ll need greater ability to
treat more people as they are attracted to treatment
• Between 10-20% of the population has addiction. Only about 10%
of them ever get care
• What about the rest?
-
The Goal
• To create more recovering people now and in the future.
– Safety– Courtesy and respect– Excellent care– Tell the world–
Expand the system
-
Our Current Challenges
• How to get people in
• How to get people to stay• How to get people to change• How to
get people to accept help of
others