Embed Size (px)
Citation preview

Kristin Remm
Kaitlynn Ayers

Page 1
I. Statement of the Problem
While there are many problems that constitute to foodborne illnesses post disaster, the
main issues recognized in research as being the most prominent in nearly all studies were a lack
of awareness, preparation, and education. The issue is not that information is lacking, but rather
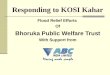
that it is not being made easily accessible for the public. Figure 1 illustrates the weighted
percentage of respondents in a study instigated in 2012 (Kosa, Cates, Karns, Godwin, &
Coppings, 2012). While such recommendations found on the left side of this table are detailed
specifically on the CDC’s webpage, it has been made obvious by this data that the public is
either unaware of the recommendations or decide not to heed the suggestions.
Along with food safety, food aid and the customs and regulations implemented in providing
relief to victims is another problem. In the same way that food safety policies need to be
implemented according to the specific circumstances of each disaster, so does food aid and relief
policies. This proposal is aimed at addressing the problems surrounding the risk of foodborne
illnesses after a disaster as well as how food aid customs and regulations play a role in food
insecurity post disaster.
Figure 1

Page 2
I. Overview
According to a report published in 2007, there needs to be a difference in food aid
policies according to the type of disaster, either being a sudden-impact disaster or a slow-onset
disaster. “Sudden impact disasters are urgent but temporary, whereas in slow-impact
disasters…food needs develop gradually and tend to be longer-lasting” (Fisher, 2007). Studies
have shown that assessments of victim’s needs after a disaster fail to adapt to the changing nature
of a disaster and tend to focus only on the current, one-time response. For example, research and
projects are most commonly concentrated on “short-term, commodity focused interventions,
usually of less than a year in duration…” (Flores, Khwaja, & White, 2005). The needs after a
disaster have the potential to change; to increase or decrease, or vary in appearance, so naturally,
relief policies should have the potential for change as well.
Studies have shown that there is a lack in providing easily accessed information for
public use on food safety. There is a rather large policy gap in developing programs for relief
efforts during an emergency situation. A common problem in policy making for food insecurity
and food safety following a disaster is that policies are often restrictive in nature. There is a
failure to maintain a multidimensional point of view when addressing food insecurity after a
disaster. This multidimensional view would include factors such as the magnitude of the
disaster, whether short-term relief is needed or long-term, politics, social relations, ethnicity,
religion, and economics. In the past, relief organizations have used a standardized set of
responses in reacting to emergencies. This is proving to be deficient in certain situations that call
for a different set of actions.
Specific details regarding the type of disaster in particular need to be taken into account
when planning relief efforts and food aid. For instance, according to an article published in
2011, environmental factors should be considered. “Cold conditions favor airborne pathogens
and warm conditions favor waterborne pathogens. In temperate climates, the winter is associated
with influenza, while summer is a time for enterovirus infections. Similarly,
rainfall…contributes to malaria, while drought leads to malnutrition-related disease” (Lemonick,
2011). When environmental conditions are better understood as well as the types of diseases and
viruses that can manifest from these conditions, proper food aid and relief can be provided
without increasing the risk of disease spread.

Page 3
When considering the recent devastation in Nepal, other concerns present themselves in
regards to food aid and food safety policies. Research shows that geographical locations of
natural disasters also play a significant role in the increase and spread of epidemics by isolating
victims from needed resources (Lemonick, 2011). A recent report given by The New York
Times on April 27, 2015, show that “outside [Nepal’s] capital, many of the worst-hit villages in
the ridges around Katmandu remain a black hole, surrounded by landslides that make them
inaccessible even to the country’s armed forces (Fuller & Barry, 2015).
A lack of educational programs on food safety constitute a huge problem in encouraging
safe behaviors when dealing with food products, resulting in an increased rate of foodborne
illnesses during and following a disaster. While most airborne, foodborne, waterborne, and
vector diseases are seen primarily in the post-impact phase of a disaster, diseases with long
incubation periods, such as vector borne and chronic diseases manifest in the recovery phase
(Lemonick, 2011). The correlation between increased rates of diseases and natural disasters is
present, though often overstated. However “according to the CDC, an estimated 76 million cases
of foodborne illness occur each year in the United States” (Finch & Daniel, 2005). Figure 2
demonstrates the increase in hospitalizations due to foodborne illnesses from 2010 to 2012.
Along with this data, information was retrieved from the National Weather Service showing that
there was an increase in natural disasters, which in this case can be determined by the number of
fatalities, from 490 deaths in 2010 to 528 deaths in 2012.
Figure 2

Page 4
Pre-Disaster
Foodborne Illness/Food
Safety
Food Aid
Post-Disaster
Foodborne Illness/Food
Safety
Food Aid
Recovery
Foodborne Illness/Food
Safety
Food Aid
As shown from the data, 2012 experienced higher rates of hospitalizations and cases of
foodborne illnesses in relation to the year of 2010. These results can be correlated to the increase
in natural disasters in the year of 2012 when compared to 2010. While this correlation are not
present in all cases, there are aspects specifically related to natural disasters that increase the risk
of disease spread. David Lemonick states in his article Epidemics After Natural Disaster, “the
primary driver of disease spread after natural disasters is population displacement and crowding
and its interplay with endemic disease and with a breakdown in infrastructure” (Lemonick,
2011).
II. Literature Review
Introduction
Data from the UN International Strategy for Disaster Reduction indicates that natural
disasters are causing incredible economic and human impact. However, the question must be
asked. What are the leading causes of death in a disaster? The World Health Organization states
that “the most common causes of death in a disaster are diarrhea, acute respiratory infections,
measles, malaria, and malnutrition.” For example, after Hurricane Katrina, there was an increase
in deaths reported by the CDC from Vibrio soft tissue infections. “Sixty percent of cases were
wound infections and 40% resulted from eating raw shellfish” (Lemonick, 2011).
Our research was directed
toward addressing the top factors
regarding the correlation between food
aid/safety and natural disasters. In
analyzing our information, we were
able to categorize our research into
three classifications; pre-disaster, post-
disaster, and recovery. While sorting
the research into these categories, we
were also able to divide the research into two different themes. The first theme involves research
regarding foodborne illnesses and food safety. The second theme includes all research found on
food aid, both from the receiving end and giving end.

Page 5
Pre-Disaster
According to a study done in 2012, “only 17% of respondents reported they are fully
prepared to keep food safe during an extended power outage” (Kosa, Cates, Karns, Godwin, &
Coppings, 2012). Lack of awareness, preparation, and education was a common theme in nearly
every article that was reviewed for this proposal. As mentioned before, while there is
information available, it is either ignored by the general public or seen as unnecessary. Studies
have shown that individuals often do not heed the recommendations given by CDC and other
similar organizations. The CDC reports that about “48 million people (1 in 6 Americans) get
sick, 128,000 are hospitalized, and 3,000 die each year as a result of foodborne disease” (Kosa,
Cates, Karns, Godwin, & Coppings, 2012). Along with the lack of education, which results in
insufficient preparedness, there is also a lack of concern when it comes to food safety. A study
aimed at identifying those who have the most concern about radiation, food safety, and natural
disasters was conducted and showed that “people living with their child, college graduates, and
homemakers were more concerned about food safety than participants who did not live with their
child…” (Sugimoto, Shinozaki, Naruse, & Miyamoto, 2014).
Prior to a disaster, individuals need to have action plans in place for when a natural
disaster strikes. An adequate amount of perishable foods, water, and shelter needs to be
accounted for. Along with having an action plan in place, individuals need to educate
themselves on food safety. Food education is not being taught in our schools anymore, and food
safety courses are not being mandated for food workers (Finch, Food Safety Knowledge and
Behavior of Emergency Food Relief Organization Workers: Effects of Food Safety Training
Intervention, 2005). These factors play a significant role in the diminishing rate of individuals
who feel well educated, prepared and aware of the risks that arise after a natural disaster.
Post-Disaster
While during the immediate impact phase of a natural disaster certain ailments may
occur, such as hypothermia, heat, illness, and dehydration, it is during the post-disaster phase
when the risk of becoming ill increases. The post-impact phase lasts roughly between 4 days to
4 weeks after the disaster. It is during this phase that airborne, foodborne, waterborne, and
vector diseases are most often seen. Findings from our literature point to multiple causes for this
increase in disease in the post-disaster stage. While some of these causes may not be
characteristic of all natural disasters, they are still very prevalent.

Page 6
In regards to epidemics after a natural disaster, causes can be divided into four categories;
environmental factors, population factors, pre-disaster variables, and type of disaster variables.
As mentioned in the overview section of this paper, the climate of the effected region should be
taken into consideration as certain bacteria and viruses arise in specific climates. For example,
flooding increases the risk of malaria, aspiration pneumonia, “Tsunami Lung”, diarrhea,
hepatitis, leptospirosis, and illnesses carried by mosquitos, such as the West Nile Virus
(Lemonick, 2011). Often what causes these illnesses in individuals is near-drowning incidents.
While individuals are inhaling water, they are also inhaling the bacteria in the water, such as
fecal matter, soil-contaminated salt water, or sand. Reports show that “diarrheal diseases…are
the most lethal public health threat to refugees overall” (Lemonick, 2011). Standing water also
attracts insects, especially mosquitos. This is very dangerous to the public health because
mosquitoes transport blood, causing the spread of disease to intensify. While flooding is a
sudden-impact disaster, and requires immediate, but short-term assistance, other disasters such as
droughts require alternative responses. Droughts imply summer heat, which is associated with
enterovirus infections, which often impacts the respiratory system and cause mild cold
symptoms, or severe breathing difficulties. This is often due to the dry air common during a
drought. As the air is filled with particles, sand, and dust, individuals are breathing in
contaminated air, which causes pneumonia-like symptoms. Obviously, relief efforts should be
tailored to the type of disaster. Aid that is commonly given for a flood should not be given
during a drought. Not only are there different food and shelter needs, but also different medical
needs, since the types of diseases associated with different disaster are diverse.
Now that we have addressed some environmental issues pertaining to post-disaster issues,
let us now look at some of the population factors found after impact. There are three overarching
characteristics of the population after a natural disaster. These characteristics include the density
of the victimized population, the age, and the dominance of chronic disease (Lemonick, 2011).
The young and the elderly are commonly considered high risk individuals following a natural
disaster. Their immune systems are either on a decline or not at full capacity yet, therefore
leaving them prone to illness. Along with age, current diseases among victims prior to the
disaster play a large role in how they will cope after the disaster. If malnutrition, diabetes, and
heart disease are quite common within the victim population, then they are also much more
susceptible to infection, as their immune system is deficient. Finally, one of the most influential

Page 7
factors in the spread of disease after a natural disaster is the density of the population. Since
most natural disasters are destructive in nature, victims often have to relocate, or stay at a shelter
for some time. Outbreaks can become explosive in relief settings, as they often involve hundreds
of refugees in a makeshift, often unsanitary location. Epidemics after natural disasters are often
the result of “disrupted public water and sewage system, crowded living conditions, airborne
transmission, lack of immunization, and injury-related infection due to exposure to debris”
(Lemonick, 2011).
When considering the population factors of disease spread after a natural disaster, one
must also bear in mind relief workers and volunteers. Data shows that “approximately three-
quarters of the estimated 76 million cases of foodborne illness are thought to be the result of
mishandling by food workers” (Finch & Daniel, Food Safety Knowledge and Behavior of
Emergency Food Relief Organization Workers: Effects of Food Safety Training Intervention,
2005). Education on food safety is not mandated for relief workers or volunteers, thus unsafe
habits and behaviors are common in shelters, soup kitchens, and relief centers. Food education
needs to include topics such as proper sanitation, food temperature, and hygiene. Along with
those working directly with the victims after a natural disaster, we must also consider the
international donation supply and the
quality of the food coming in. Common
problems found in regards to food aid and
donations are first, donated food is
culturally insensitive. For example,
canned pork was donated to a population
of Muslim victims after a tsunami
(Fisher, 2007). Second, the quality of the
food is often very poor. Researchers found
that after the 2004 tsunami in Indonesia, “officials measured the amounts of expired foods they
had received – some with expiration dates over a year old – by the truckload” (Fisher, 2007). In
some regards, this is the donors fault. However, further research has shown that due to the
complex customs and regulations system for donated food aid, perfectly good food is found
wasting away in customs. According to a recent report, aid customs is currently hampering with
relief efforts in Nepal after the recent earthquake that has already taken 6,600 lives. “They
Figure 3

Page 8
should not be using peacetime customs methodology,” he [Jamie McGoldrick] said, adding that
material was piling up at Kathmandu airport instead of being ferried out to victims (Ratcliffe,
2015). Figure 4 is an image received from the quoted article and shows food aid being held in
customs1.
In explaining the issues surrounding post-disaster disease and food insecurity, one must
look at pre-disaster preparedness. As mentioned earlier is the report, “sanitation, primary health
care and nutrition, medical infrastructure, equipment and medications, disaster preparedness,
disease surveillance, and roads and transportation” are all factors that play into post-disaster
conditions (Lemonick, 2011). If prior to the disaster these factors are well under control and
have been reinforced with adequate education, awareness, and action plans regarding their
destruction due to a natural disaster, post-disaster conditions would be much less severe due to
this increased level of preparation.
As discussed before, the type of disaster and following climate are huge factors in post-
disaster circumstances. A study done on epidemics following natural disasters states that
“earthquakes, hurricanes, and tsunamis can lead to crush injuries and other penetrating injuries.
Tsunamis and floods can lead to near-drowning (and all the diseases linked to near-drowning)
and electrocution” (Lemonick, 2011). The post-impact phase is understood to be the most
dangerous phase. Disease runs rampant, structures are lacking, food supplies are diminished,
and the population is entirely displaced. All of these factors play a role in the increased death
rates after a natural disaster and should be equally considered when planning relief efforts.
Recovery
While most diseases proliferate during the post-disaster phase, there is a significant
amount of disease and illness that show up in the recovery phase. Most of these diseases have
long incubation periods and often arise more than 4 weeks after the initial impact. Examples of
organisms that have long incubation periods and are commonly found in the recovery stages after
natural disasters are malaria, western/Saint Louis encephalitis, dengue, yellow fever, and West
Nile virus (Lemonick, 2011). Along with the newly introduced diseases that have long
incubation periods, problems often seen in post-disaster phases are still present during the
following recovery stage. Food is often still trapped in customs during the recovery period and
is also seen to be culturally insensitive to the victims in need. Overcrowding is still an issue
1 Prakash, J. (2015). Nepal customs holding up earthquake relief efforts, says United Nations. Retrieved from URL.

Page 9
during recovery because due to a lack of urgent request and response efforts, infrastructures have
yet to be deemed secure. Both on the giving and receiving end of relief efforts, alternative
motives are recognized. “Both donors and humanitarian actors have frequently succumbed to the
temptation to compete for recognition as the first to respond to a particular disaster” (Fisher,
2007). Not only that, but “both political and administrative factors can complicate the initiation
of international relief. It is often difficult for a government to admit that it requires international
assistance for fear of appearing weak and damaging national pride” (Fisher, 2007). Though
these factors are understandable and very human, there should be a sole focus on assisting
survivors, containing the spread of disease and further death, and rebuilding the lives these
victims once knew.
Conclusion
By understanding all of the factors that contribute to a rise in disease after a natural
disaster, potential victims, relief workers and volunteers, as well as government officials world-
wide can begin to tailor relief efforts to specific conditions, disasters, populations, and
environments. It is necessary to provide long-term relief as a disaster still has its effects years
after the initial impact. As data has shown, diseases may not even present themselves until after
considerable time following the disaster. No one disaster is the same, and therefore they should
all be treated differently.
III. Stakeholder Groups
In conducting research pertaining to the spread of diseases, particularly foodborne illness,
after a natural disaster, many stakeholders presented themselves. First and foremost, the victims
of natural disasters are the largest stakeholder group. While their lives, their homes, families,
and livelihood have been destroyed by a natural disaster, their health is also on the verge of being
destroyed. Victims are at high risk of developing disease post-impact because of overcrowding
and unsanitary living conditions. Exposure to the elements may also be considered a risk factor
for individuals who do not have access to shelter after a disaster. Specifically within the
population of victims, the elderly and the young are at high risk of disease because of their
diminishing immune system or their growing immune system that has not reached full capacity.
Food workers and volunteers who assist victims after a natural disaster are also considered
stakeholder groups because they are also exposed to the dangers of post-impact conditions.
While food workers and volunteers are indeed there to help, they are under scrutiny because they

Page 10
are coming from other locations bringing foreign illness or disease with them. Food safety
education is at an all-time low so while they are trying to help, they are also increasing the risk of
disease spread.
Finally, governments and administration on both the receiving and giving end of aid and
relief have a lot at stake. Receiving governments have their pride at stake. By asking for
international relief, they are admitting that they cannot do it on their own and need alternative
assistance. Especially when thousands of people are dying due to a natural disaster and its
aftereffects, this could be seen as a positive quality in a government. However, it is still a
humiliating thing to do asking for help, even on a personal level. When the entire world is
watching, the humiliation might propel a government to avoid asking for much needed help.
International relief organization are also at risk of a bad name if they provide poor quality food
and aid. Recent reports have found that international relief for the Nepal earthquake victims is
incredibly gender-blind. Materials for women in particular, such as pads and tampons, are not
being made available. International relief could be to blame for this, making them a stakeholder
group as well.
IV. Proposed Solutions
In addressing relief policies and processes made available through the Federal Emergency
Management Agency (FEMA), we recognized some ways that resources could be better used.
FEMA uses their funding to respond to disasters and emergencies. While this is a positive
action, and one that should certainly be continued, we must propose that an amount of the
funding FEMA receives should be utilized in readiness efforts. According to Figure 5, accessed
from the FEMA Disaster Relief Fund: Monthly Report, the Federal Emergency Management
Agency spent nearly thirteen times the amount on public assistance than on mitigation efforts
during Hurricane Sandy through the fiscal year of 2015 (Federal Emergency Management
Agency, 2015)..
We propose that disaster relief organizations like that of FEMA should focus more of their
assets and funding on mitigation and preparedness efforts. If only half of what was used on
public assistance were to be used toward mitigation efforts, the amount spent on relief efforts
after a disaster would be much less. This drop in public assistance spending would be due to the
higher levels of preparation in communities, thus decreasing the amount of assistance needed
post-impact.

Page 11
Micro level emergency response agencies, like the American Red Cross for example, appear
to coordinate their resources efficiently. With multiple locations gathering small amounts of
funding, volunteers, and resources, they tend to accumulate to a rather large impact on local and
international disasters. This is a common characteristic of small organizations and should be
replicated in the macro level of emergency response. According to the 2012 fiscal year report by
the American Red Cross, donations made to the American Red Cross assisted in:
Response to nearly 70,000 disasters
Education in first aid, water safety, and other lifesaving skills for more than 4 million
people
More than 50,000 relief items being provided via international disaster response
operations
400,000 services for military members, veterans and civilians
Education for more than 53,000 people in International Humanitarian Law
Disaster assistance internationally for more than 7 million people
Reconnecting nearly 1,000 families separated by war or disaster
Vaccination of an estimated 146 million children through the Measles Initiative
campaign
Briefing more than 1 million people by local chapter through the “Get to Know us”
program
Providing disaster education presentations to nearly 2.5 million people
Figure 5

Page 12
Reaching more than 335,000 people with HIV/AIDS prevention, care and support
activities
Distributing nearly 9 million blood products to patients across the country
(The American Red Cross, 2012)
These two separate reports indicate that the American Red Cross is doing more to prevent severe
conditions after a natural disaster with only donated money than government programs like
FEMA are doing with their own funding. We would suggest that organizations at a macro level,
like that of FEMA, start adapting the policies and procedures similar to micro organizations, like
the American Red Cross. We understand that this solution is theoretical, and a rather large step
to take in enhancing both response and readiness actions. If this is a step that we are unable to
take as a nation, we would then suggest giving more money to micro level organizations.
After analyzing research and gaining a new perspective on response and relief efforts after a
natural disaster, one must consider the difference between a reaction and a response. Often,
efforts by local organizations and international relief establishments reflect a reaction to natural
disasters. Poor quality food, culturally insensitive materials, and gender-blind supplies are just a
few examples of the result of reaction-based replies to a natural disaster. On the other hand
however, a response indicates a plan; a set of actions that local, governmental, and international
relief organizations are prepared to and educated in how to implement. By changing relief
efforts to well thought out, prepared action steps that are sensitive to not only all ways of life, but
to the type of disaster, climate, and environment, victims of natural disasters will experience
quicker and more effective responses, allowing them to once again find normalcy.
V. Implementing the Solution(s)
In order to address problems regarding the use and distribution of funding toward disaster
response organizations, there needs to be a change in priority. While the process of going from a
response geared organization to a readiness focused organization will be prolonged and difficult,
it has the potential to decrease overall, long-term costs to local, state, and government programs.
A program focused on changing the distribution of funding to better assist mitigation efforts
rather than being nearly 75% financially focused on response and relief will include policy
makers and many government departments, agencies, and councils. Introducing a policy or
changing policies can be influenced by political parties or individual politicians, lobbyists,
voluntary organizations, community groups, public opinions, public consultants, and the media

Page 13
(nidirect government services, 2014). With all of these influences in policy, it would be
unreasonable to think that results and changes will be seen anytime soon, because policy has
many avenues it must go through to get approved and implemented. In general, United States
has applied a process in approving policies. This process includes recognizing a problem, setting
an agenda for addressing the problem, formulating a policy regarding the problem, adopting the
policy, implementing the policy, then reviewing the effectiveness of the policy (Policy Making:
Political Interactions, 2014).
The first thing that must happen in implementing a change in how large government
organizations use their funding toward disaster mitigation, response, and relief is to recognize the
problem of unequal distribution of assets. As we have seen in this proposal, organizations that
are solely reliant on donations spread their assets into many different areas of preparedness
programs, response actions, and relief efforts. If this kind of approach were to be translated into
large relief organizations, then imagine what kind of impact these organizations could have. Not
only would resources be better distributed to address all areas of disaster resiliency and response,
but they would also have government funding to put toward these efforts rather than just
donations.
Along with this change in perspective and policy of government funded relief organizations,
there must also be attention put toward the type of reply that we have when faced with a disaster.
Changing from reaction-based replies to a response-based reply will require more focus on pre-
impact efforts to prepare and educate individuals on action steps that must be taken during and
after a disaster. This type of action would guarantee a plan, and therefore a better developed
response to a disaster, with factors such as race, class, ethnicity, religion, age, and gender in
mind and accounted for in response materials and resources. Certain implementations would
need to take place, like starting at the community level by encouraging educational programs on
the conditions that often present themselves after a natural disaster. We should start by
encouraging community action and response kits, which should include a large location for
shelter stocked with cots, blankets, and pillows. There should be a community stock of food,
water, and clothing. Along with these basic needs, other specific materials should be included,
such as sanitary items, toiletries, cell phone chargers, first aid items, flashlights, batteries, and
basic pharmaceuticals, just to name a few. Simply by putting together community action and

Page 14
response kits prior to a disaster, we have succeeded in avoiding the reaction reply, which would
be panicked and random. Instead, we now have a planned for and prepared purposeful response.
VI. Conclusion
In the face of a disaster, there are many factors that contribute to the severity of post-disaster
conditions. While often the main focus of response and relief organizations is to react post-
disaster, we propose that more effort needs to be put in the pre-disaster phase to educate, prepare,
and boost awareness among potential victims, relief workers, and volunteers.
Studies have shown that education and preparedness are lacking in communities, especially
when it comes to food safety. In order to make a significant impact on the post-disaster
conditions, organizations need to focus more energy, resources, and assets on pre-disaster
mitigation efforts. An increase in awareness among communities and a growth in educational
programs on disaster response and food safety will significantly impact the post-disaster results
by decreasing the spread of disease and having relief materials already on hand. Often we see
that the reaction to a natural disaster is just that, a reaction. A reaction is an urgent impulse.
Individuals, communities, states, and governments need to shift the focus from reaction to
preparedness, because then after a disaster there would be a well thought out, planned, and
educated response to assess the needs of the victimized community.
Not only do the potential victims need to be educated in food safety and response techniques,
but so do relief workers, volunteers, and relief organizations. We have seen how food aid is
often culturally insensitive, gender-blind, and inadequate for the specific climate and condition
post-impact. Education on what kinds of foods are culturally acceptable for certain areas should
be included in food safety programs. Also, certain types of disasters and climates call for
different food supplies. This is why we propose having multiple response plans and procedures
in order to adapt to unique circumstances. Every disaster is different in its impact and following
conditions, so why are relief programs not just as different? Finally, materials and supplies that
are sent should accommodate all types of people; young, elderly, men, women, etc. This will not
only help reach every affected group, but it will also assist in sanitary efforts, cleanliness, and
diminishing occurrences of disease spread.
By initiating a change in how relief organizations approach disaster relief, mitigation will be
significantly increased and therefore post-impact conditions would be much less severe. By
simply having community relief kits prepared prior to a disaster filled with materials for all

Page 15
groups within a community, response efforts, though still very important, would be much less
urgent. Please consider the following changes:
1. Budget shifts to better finance mitigation efforts
2. Policy alterations to support multiple adaptation of relief processes
3. Increased education programs
4. Financing food safety awareness and education program in particular
5. Support for community aid and relief kits
6. Increased collaboration among relief organizations
By implementing some of these changes, our nation’s relief organizations will immediately shift
from reaction-based efforts to a response-based effort. Collaboration among relief organizations,
planned, well thought out action response plans, and educated individuals, not only those who
are responding, but those who were also victimized, will significantly decrease the urgency of
responding to a natural disaster. Spread of disease would diminish, death rates are likely to
decline, and the time between impact and getting back to normalcy would be much quicker.

Page 16
References
Federal Emergency Management Agency. (2015). Disaster Relief Fund: Montly Report. Homeland
Security.
Finch, C. (2005). Food Safety Knowledge and Behavior of Emergency Food Relief Organization
Workers: Effects of Food Safety Training Intervention. Journal of Environmental Health, 30.
Finch, C., & Daniel, E. (2005). Food Safety Knowledge and Behavior of Emergency Food Relief
Organization Workers: Effects of Food Safety Training Intervention. Journal of Environmental
Health, 30.
Fisher, D. (2007). Fast Food: Regulating Emergency Food Aid in Sudden-Impact Disasters. Vanderbilt
Journal of Transnational Law, 1130.
Flores, M., Khwaja, Y., & White, P. (2005). Food security in protracted crises: building more effective
policy frameworks. Food and Agriculture Organization of the United Nations, 531.
Fuller, T., & Barry, E. (2015). Nepal Villages Cut Off by Earthquake Wait for Aid as Death Toll Passes
4,000. New York City: The New York Times .
Kosa, K. M., Cates, S. C., Karns, S., Godwin, S. L., & Coppings, R. J. (2012). Are Older Adults Prepared
to Ensure Food Safety During Extended Power Outages and Other Emergencies?: Findings from
a National Survey. Educational Gerontology, 769.
Lemonick, D. M. (2011). Epidemics After Natural Disasters. American Journal of Clinical Medicine .
nidirect government services. (2014). What is government policy? Retrieved May 7, 2015, from nidirect
government services: http://www.nidirect.gov.uk/what-is-government-policy
Policy Making: Political Interactions. (2014). Retrieved May 7, 2015, from American Government:
http://www.ushistory.org/gov/11.asp
Ratcliffe, R. (2015, May 2). Nepal customs holding up earthquake relief efforts, says United Nations.
Retrieved May 6, 2015, from thegardian :
http://www.theguardian.com/world/2015/may/02/nepal-customs-holding-up-relief-jamie-
mcgoldrick-united-nations
Sugimoto, T., Shinozaki, T., Naruse, T., & Miyamoto, Y. (2014). Who Was Concerned about Radiation,
Food Safety, and Natural Disasters after the Great East Japan Earthquake and Fukushima
Catastrophe? A Nationwide Cross-Sectional Survey in 2012. PLOS One, 3.
The American Red Cross. (2012). Where Your Money Goes. Retrieved May 7, 2015, from The American
Red Cross: http://www.redcross.org/support/donating-fundraising/where-your-money-goes