Embed Size (px)
Citation preview

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
1 | P a g e
What is MAT?
Medication Assisted Treatment
(MAT) is an evidence-based
practice in which a client is
treated for a Substance Use Dis-
order through the combined use
of medications and counseling.
While MAT has been proven
effective in treating depend-
ence to tobacco, alcohol, and
opiates, this Spotlight will pri-
marily focus on the use of MAT
to treat individuals addicted to
opioids.
Opioids have such a powerful
impact on brain chemistry that
medications are often required
to assist the individual in reach-
ing a manageable state. Bene-
fits related to medication in-
clude diminishing cravings, pre-
venting withdrawal symptoms,
and reestablishing brain func-
tion. These positive effects al-
low an individual to regain the
control necessary to shift focus
from maintaining addiction to
achieving recovery.
Historically speaking, treatment
for substance use disorders was
derived solely from the absti-
nence-only framework. The in-
clusion of medication into treat-
ment for dependence was
frowned upon, as many be-
lieved the prescribed medica-
tion replaced one addiction with
another. Today, much more is
known about the science behind
addiction and MAT is widely
seen as the standard in effective
treatment.
The Hazelden Betty Ford Foun-
dation is considered a pioneer in
the field of addiction treatment.
Best Practice Spotlight
In This Issue
What is Medication Assist-ed Treatment?
Medications used by MAT
programs Key Components of MAT
Programs Federal and Kentucky Re-
sponse to Opioid Epidemic Q&A with Allen Brenzel,
M.D. Medical Director for DBHDID
Issue Number 4: Medication Assisted Treatment (MAT) for Opioid Dependence
MAT has been found to reduce morbidity and mortality, decrease overdose deaths, reduce transmission of infec-tious diseases, increase treatment retention, improve so-cial functioning, and reduce criminal activity. SAMHSA—2016.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
2 | P a g e
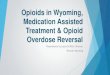
Hazelden sought to develop a program that would success-fully treat new clients after wit-nessing a significant rise in their treatment of opioid de-pendence. According to their statistics, Hazelden’s facility for young adults and adoles-cents in Plymouth, Minnesota charted an increase for clients seeking opioid addiction treat-ment from 15 percent in 2001 to 41 in 2011. The national sta-tistics concerning opioids are more staggering. (See Figures 1 and 2) Centers for Disease Control reports that the death toll from prescription painkiller overdose increased more than fivefold in the past decade in the U.S.
Overdose Deaths (total vs. heroin) Over Time
1020 1032979
1034
43
132204 224
0
200
400
600
800
1000
1200
2011 2012 2013 2014
Total OD Deaths
Heroin OD Deaths
Figure 1. Overdose Deaths in Kentucky from Heroin versus all Opi-ates, 2011-2014.
Figure 2. Drug Overdose Death Rates in Kentucky Counties, 2013.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
3 | P a g e
FIGURE 4. Opioid Dependence: How Does it Work? www.hazeldenbettyford.org
Marvin D. Seppala, MD, Chief Medical Officer of the Hazelden Betty Ford Foundation
Initiation and
Addiction
Opioid molecules travel through the brain and attach to receptors, specialized proteins on the
surface of certain brain cells. The binding of these molecules with their target receptors triggers
the same chemical response in the brain’s reward center that occurs with anything that causes
intense pleasure or is intended to be reinforcing to survival itself. Rewarding and survival-based
activities result in release of dopamine in the brain’s reward center and opioids trigger the release
of dopamine in excess amounts. The brain recognizes this as something that needs to be repeat-
ed.
Maintaining
Addiction;
Increased Doses
Prolonged use of increasingly higher doses of opioids changes the brain so that it functions more
or less normally when the drug is present and abnormally when it is removed. The brain becomes
tolerant and dependent. In addition, the euphoria associated with use tends to diminish with reg-
ular use. The opioid receptors have changed at a cellular level, trying to protect them from over-
stimulation. A user is no longer chasing euphoria, but a sense of normalness.
Withdrawal and
Relapse
Avoiding withdrawal is what typically drives the continuation of use. Withdrawal from opioids
includes agitation, anxiety, itching, irritability, insomnia, goose bumps, rapid heart rate, mild hy-
pertension, vomiting and diarrhea. The withdrawal increases over time and can cause tremors,
intense anxiety, deep bone pain, and other debilitating symptoms. The body is effected long term
as well, resulting in depression, anxiety and cravings for months or years after even while main-
taining sobriety.
Treatment Opioid withdrawal is so intense that many individuals feel as if returning to the drug is their only
option to feel normal again. Most overdoses and deaths occur when a person relapses using the
same dose as when their tolerance was high during active addiction. The use of FDA-approved
medications in treatment provides the sense of “normalcy” needed to begin the healing process.
Figure 3. Depicts the
performance of ago-
nist drugs (e.g., meth-
adone) and antagonist
drugs (e. g. naloxone)
with the receptor
cites in the brain.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
4 | P a g e
Figure 5 Major Treatment Medications
Characteristics Methadone Buprenorphine Naltrexone
Brand Names Dolophine, Methadose Subutex, Suboxone, Zub-solv
Depade, ReVia, Vivitrol
Class
Agonist (fully activates opioid receptors)
Partial agonist (activates opioid receptors but produces a dimin-
ished response even with full occupancy)
Antagonist (blocks the opioid recep-tors and interferes with the reward-ing and analgesic effects of opioids)
Use and Effects
Taken once per day orally to reduce opioid cravings and
withdrawal symptoms
Taken orally or sublingually (usually once a day) to relieve
opioid cravings and withdrawal symptoms
Taken orally or by injection to dimin-ish the reinforcing effects of opioids
(potentially extinguishing the associ-ation between conditioned stimuli
and opioid use)
Advantages High strength and efficiency as long as oral dosing (which
slows brain uptake and reduc-es euphoria) is adhered to;
excellent option for patients who have no response to oth-
er medications
Eligible to be prescribed by cer-tified physicians, which elimi-nates the need to visit special-ized treatment clinics and thus
widens availability
Not addictive or sedating and does not result in physical dependence; a recently approved depot injection
formulation, Vivitrol, eliminates the need for daily dosing
Disadvantages
*Volkow, N.D., Frieden, T.R., Hyde, P.S. & Cha, S.S.
(2014) Medication-assisted therapies – tack-ling the opioid-overdose epidemic. The New Eng-land Journal of Medicine.
Mostly available through ap-proved outpatient treatment
programs, which patients must visit daily
Subutex has measureable abuse liability; Suboxone diminishes this risk by including naloxone,
an antagonist that induces with-drawal if the drug is injected
Poor patient compliance (but Vivitrol should improve compliance); initia-
tion requires attaining prolonged (e.g., 7-day) abstinence, during
which withdrawal, relapse, and early dropout may occur
Methadone has been proven to be a safe and effective option for treating individuals for opioid de-pendence. Maintenance treat-ment typically leads to reduction or cessation of illicit opioid use and its adverse consequences, includ-ing cellulitis, hepatitis, and HIV infection from nonsterile injection
equipment, as well as criminal behavior associated with obtain-ing drugs. Additional positive out-comes include a proven reduction in psychiatric symptoms, unem-ployment, and family or social problems (SAMHSA, TIP 43, 2014).
There are a few health risks relat-
ed to the use of methadone in-
cluding the concern of neonatal
abstinence syndrome (NAS) for
babies exposed to narcotics, such
as methadone, in the womb. The
official definition of NAS as out-
lined by the National Institutes of
Health reads, “Neonatal absti-
nence syndrome (NAS) is a group
of problems that occur in a new-
MEDICATIONS USED IN MEDICATION ASSISTED TREATMENT

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
5 | P a g e
Quick Facts: Neonatal Abstinence Syndrome (NAS)
In the United States, 5.9% of pregnant women 15 to 44 years of age used illicit drugs in the past month (MacMullen, Dulsk & Blobaum, 2014).
Prenatal NAS—due to prenatal maternal use of substances. Abuse may result in withdrawal symptoms in the ne-onate once the placental access to the substance is no longer available.
Opiates can produce a longer and more threatening withdrawal.
The effect of drugs on body systems is also influenced by the type of drug, the combination of drugs, the amount and frequency of use, the trimester in which the drug is used, the timing of withdrawal, and the genetic suscepti-bility of the fetus/neonate (MacMullen, Dulsk & Blobaum, 2014).
The primary recommendation for assisting babies with NAS is to match the drug used to treat withdrawal to the type of drug abused (e.g., opiates are given to the neonate if withdrawing from opiates).
Only 24% of opioid-dependent mother’s breastfeed and 60% stop on the average after 5.9 days
Breastfeeding could potentially decrease the severity of NAS, delay its onset, and decrease the need for pharma-cologic treatment (MacMullen, Dulsk & Blobaum, 2014).
Concentrations of methadone and buprenorphine found in human milk are low (Pritham, Paul & Hayes, 2012); breastfeeding should be permitted and mothers educated on its benefits.
Treatment of co-occurring psychiatric disorders with antidepressants, benzodiazepines, or antipsychotics may
increase the effects of NAS (Pritham, Paul & Hayes, 2012).
born who was exposed to addictive
opiate drugs while in the mother’s
womb.” This condition may also
be referred to as neonatal narcotic
withdrawal syndrome. This is a
major concern for women who are
prescribed methadone while preg-
nant, as the baby is likely to suffer
withdrawal upon birth and experi-
ence intense discomfort. Risks al-
so exist for adults who are exposed
to methadone. The drug has the
potential to affect cardiac electro-
physiology which is linked to seri-
ous heart arrhythmias and sudden
death (Thomas et al., 2014). Risks
are manageable as long as the cli-
ent is using methadone as pre-
scribed and adheres to the guid-
ance of his or her physician. An
alternative to methadone is bu-
prenorphine, a partial agonist,
which has proven to be somewhat
safer than methadone.
Buprenorphine When compared
to methadone, buprenorphine pro-
duced similar rates of treatment
retention, abstinence from illegal
drugs, and proved to substantially
reduce illicit opioid use (SAMHSA,
TIP 43, 2014). The drug has also
been shown to improve self-help
group attendance and to be effec-
tive for both youths and adults
(Hazelden). In addition, Buprenor-
phine does not affect cardiac elec-
trophysiology and therefore, no
risk exists for lethal cardiac ar-
rhythmias. Buprenorphine howev-
er, can cause respiratory depres-
sion if taken in extremely high dos-
es. Studies also indicate that the
risk of NAS is lower for fetuses ex-
posed to buprenorphine than
those exposed to methadone
(Thomas et al., 2014).
Naltrexone When used as di-
rected, naltrexone is highly effec-
tive in reducing cravings and pre-
venting relapse (SAMHSA, TIP 43,
2014). Poorer outcomes have
been linked to clients who were
prescribed a methadone regimen
prior to beginning naltrexone
treatment. Studies also indicate
increased compliance when nal-
trexone therapy is supported with
payment scheduling and vouchers
(SAMSHA, TIP 43, 2014). A major
benefit associated with the pre-
scription of naltrexone is that it
cannot be abused by clients be-
cause an injectable version of nal-
trexone (Vitriol) is available to cli-
ents monthly causing no chance of

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
6 | P a g e
MAT PROGRAMS
The design of MAT programs var-
ies but the basic components re-
main the same: medications bun-
dled with counseling. The follow-
ing section discusses COR-12, Ha-
zelden Betty Ford’s pioneer pro-
gram, and characteristics related
to alternative available MAT pro-
grams based on suggestions from
SAMHSA TIP 43.
COR-12 Hazelden has been in-
strumental in advocating for the
use of these FDA-approved medi-
cations in treatment for opioid de-
pendence. COR-12 was developed
in response to the growing need
for effective opioid treatment and
was fully implemented in 2013.
The official description of COR-12
as provided by Hazelden reads:
“COR-12 is the extended, adjunctive
use of medicines – in combination
with psychological and psychiatric
care; Twelve Step based counseling
and other therapies – to increase
the potential for those who have
the disease of addiction to achieve
long-term recovery.”
– 2013, Hazelden Foundation
COR-12 offers three primary path-
ways to those recovering from opi-
oid dependence: no medication,
buprenorphine/naltrexone, and
extended-release naltrexone. The
client always has a choice as to
how he or she prefers to receive
treatment and the pathways are
clearly outlined. Hazelden utilizes
an interdisciplinary team to en-
gage clients and pinpoint their ex-
act individualized treatment
needs. These teams analyze a cli-
ent’s medical and substance use
history, treatment and recovery
history, co-occurring mental
health issues, recovery environ-
ment and support network, and
risk of relapse to suggest the most
appropriate pathway for each cli-
ent. Hazelden’s individualized ap-
proach also offers a variety of
treatment settings in an effort to
provide the most effective treat-
ment possible. A key characteris-
tic of COR-12 pertains to how it
defines abstinence for clients en-
gaged in a medical pathway op-
tion for treatment. The develop-
ers of COR-12 were greatly influ-
enced by the creators of Over-
eaters Anonymous (OA) and Sex
Addicts Anonymous (SAA) when
formulating a concept of absti-
nence that involves a “drug” that
cannot be completely eliminated.
Participants in OA and SAA recog-
Figure 6 Other Opioid Addiction Treatments
Medication Assisted Treatment uses not only medication to treat opioid dependence but also a combination of counseling, case management, behavioral treatments and psychothera-pies based on the client’s individualized needs. Programs may vary in the services provided however, the following briefly outlines SAMHSA’s suggestions for counseling components in MAT.
Counseling and Case Management Individual Counseling – focus on feelings, coping skills, barriers, etc. Group Counseling – reduces sense of isolation with inclu-sion of peer support Case Management – Assistance pertaining to housing, medical care, etc.
Cognitive and Behavioral Therapies Node-link Mapping Community Reinforcement Approach Contingency Management Motivational Enhancement
Psychotherapy Modify or remove problematic thoughts, feelings, be-haviors; useful for chronic psychological and social prob-lems
Miscellaneous Topics for Treatment Effects of sexual abuse
Living with HIV/AIDS and Hepatitis C
Domestic Violence
From TIP 43: Medication-Assisted Treatment for Opioid Ad-diction in Opioid Treatment Programs, 2014.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
7 | P a g e
nize that food and sex are unavoid-
able, but have grown to under-
stand the choices and behaviors
that classify an action as A key
characteristic of COR-12 pertains
to how it defines abstinence for
clients engaged in a medical path-
way for treatment. The develop-
ers of COR-12 were greatly influ-
enced by the creators of Over-
eaters Anonymous (OA) and Sex
Addicts Anonymous (SAA) when
formulating a concept of absti-
nence that involves a “drug” that
cannot be completely eliminated.
Participants in OA and SAA recog-
nize that food and sex are unavoid-
able, but have grown to under-
stand the choices are behaviors
that classify an action as recovery-
based or relapsing. Recovery for
opioid dependence is achieved
when the individual is using medi-
cation as directed and not for the
use of intoxication, and if the client
is applying new
MAT programs may use alterna-
tive approaches to the application
of counseling without specifically
referring to the twelve-step pro-
cess. SAMHSA summarized the
possible avenues of counseling in
their TIP 43 on medication assisted
treatment. While these are not
requirements for MAT programs, it
provides details on what some pro-
grams offer clients in addition to
their medication. Encouraging cli-
ents to engage in counseling helps
them address psychological needs
that may have been the underlying
motivator of the addiction or a
barrier to recovery. Figure 6 briefly
outlines SAMHSA’s
suggestions for meet-
ing psychological
needs in MAT pro-
grams.
Federal Initiatives
Ample evidence sup-
porting the use of
MAT to treat opioid dependence
motivated the Substance Abuse
and Mental Health Services Ad-
ministration (SAMHSA) to award
grants to 39 states with the high-
est rates of primary treatment ad-
missions for heroin and opioids.
SAMHSA created Targeted Capac-
ity Expansion: Medication Assisted
Treatment – Prescription Drug and
Opioid Addiction (MAT-PDOA) RFA
No. T1-15-007. “The purpose of
this program is to provide funding
to states to enhance or expand
their treatment service systems to
increase capacity and provide ac-
cessible, effective, comprehensive,
coordinated care, and evidence-
based medication assisted treat-
ment (MAT) and recovery support
services to individuals with opioid
use disorders seeking or receiving
MAT (http://www.samhsa.gov/
grants/grant-announcements/ti-15
-007)”. This Funding Opportunity
Announcement (FOA) outlines
three key goals for states who re-
ceive funding:
1. Increase the number of individ-uals receiving MAT through pro-grams offering FDA-approved pharmacotherapies
2. Increase the number of individ-uals receiving integrated care
3. Decrease illicit drug use at 6-month follow-up
Kentucky was one of the states
selected to receive the grant based
on its need for expanded treat-
ment for opioid dependence. The
following section discusses Ken-
tucky’s need for an effective treat-
ment response to opioid addiction,
and outlines the grant and
DBHDID’s implementation of MAT
programs statewide.
MAT in Kentucky
The statistics related to Kentucky’s
opioid epidemic are startling, es-
tablishing the need for a compre-
hensive and effect treatment re-
sponse. Currently, overdose
deaths are more frequent than
motor vehicle deaths in Kentucky
with exceptionally high rates of
OD deaths seen in women of
childbearing age (18-44). (See Fig-
ure 7). In fact, Kentucky’s rates of
overdose deaths for women be-
tween the ages of 18 and 44 great-
ly surpass that of the national aver-
age. In addition, Kentucky has wit-
nessed a dramatic increase in the
number of babies hospitalized for
Figure 7. Source: Kentucky Injury Prevention and
Research Center

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
8 | P a g e
NAS with numbers increasing
from 67 in 2001 to 1,016 in 2014.
Without effective treatments
available, mothers are often una-
ble to reach a state of stabilization
in which critical bonding and at-
tachment may occur between
mother and child. Healthy inter-
actions among mother and child
are critical to a child’s brain devel-
opment. MAT may facilitate at-
tachment between mother and
child as the mother can be posi-
tively engaged in parenting with
treatment.
These findings collectively sup-
ported the drive to expand treat-
ment services and to increase ca-
pacity for evidence-based MAT
and other recovery support ser-
vices to pregnant and parenting
women.
Kentucky’s Response
Kentucky’s program is known as
SMARTS (Supporting Mothers to
Achieve Recovery through Treat-
ment and Supports) INITIATIVE.
The project length is three years
with $1,000,000 being awarded
by SAMHSA every year for a total
of $3,000,000. These programs
treat women through a
partnership with two Community
Mental Health Centers in high-risk
areas of Kentucky: Cumberland
River Behavioral Health in Corbin
and Bluegrass.org in Lexington.
The DBHDID Project Director for
this initiative is Kris Shera, MPA.
Ms. Shera has outlined the
primary components currently
being implemented:
Creating a new system of care with evidence-based, compre-hensive, integrated, communi-ty coordinated service delivery systems for pregnant and par-enting women up to two years post birth with opioid use disor-der that addresses current ser-vices deficits and includes ac-cess to MAT; includes Hazelden Betty Ford Foundation’s Com-prehensive Opioid Response – Twelve-Steps (COR-12) ap-proach; and includes wrapa-round services to assist these clients with meeting medical, social, childcare, housing, edu-cation, and vocational needs that serve as barriers to treat-ment and recovery.
Figure 8. Source: Kentucky Department of Medicaid Services Claims Database

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
9 | P a g e
Quick Facts for SMARTS SMARTS goal is to create a sustainable and comprehensive array of interconnected services.
Target population: pregnant and postpartum women up to 2-years post-birth who have an opioid use
disorder. Each enrolled client should receive services appropriate to her treatment and recovery sup-
port needs for minimum 12 months after delivery, and up to 24 months as needed. Services should in-
clude parenting training and coordination of care for the infant.
Target Numbers: Grant project will serve a total of 500 pregnant and parenting women over three years
of the project.
o Bluegrass – 58 in first year, total 290 over 3 years
o Cumberland – 42 in the first year, total of 210 over the 3 years
Eligibility: Referrals accepted from any source; woman must be pregnant or postpartum 6 months post
birth with an opioid disorder and accept services.
Enrollment: Case managers complete an assessment and enroll the woman; will also identify appropri-
ate level of care through ASAM criteria and develop with the client a service plan. Client is entered into
the Service Point system, MAT is explained and offered as an option, and medication is decided upon
with medical team approval.
Promoting community partner-ships by facilitating meetings and work sessions to examine how to best provide these com-prehensive services promote community education and max-imize efficient use of resources.
Enhancing information sharing through technology infrastruc-ture to support service delivery.
Providing extensive training and workforce development oppor-tunities for both the medical and behavioral health work-force.
Kentucky’s ultimate goal is to cre-
ate a sustainable program that
provides a comprehensive array of
interconnected services that ex-
tends well beyond the life of the
grant. SMARTS has established
five expected outcomes:
1. Increased access to MAT, wrapa-round services and treatment;
2. Increased number of individuals receiving comprehensive, integrat-ed, community coordinated care;
3. Reduction in adverse childhood experiences and intergenerational substance abuse patterns;
4. Decreased illicit drug use among the target population at 6 months follow-up; and
5. Formation of a comprehensive, sustainable system of care that can be replicated throughout the Commonwealth.
When the project officially con-
cludes in late July 2018, the hope is
that the SMARTS will have created
lasting improvement to treatment
access and services for pregnant
and parenting women. While
women constitute a large popula-
tion of underserved individuals
with opioid dependence, many
other individuals are in need of
quality, evidence-based treat-
ments. The next section discusses
Narcotic Treatment Programs
(NTPs), existing treatment pro-
grams which are available to a
wide variety of clients with opioid
dependence.
Narcotic Treatment Programs (NTPs)
Narcotic Treatment Programs
(also known as Opioid Treatment
Programs or OTPs) are in 21 sepa-
rate locations in Kentucky for any-
one struggling with opioid de-
pendence. Ron Easterly, M.D.,
MPH, with BHDID, is the state’s
acting State Opioid Treatment Au-
thority (SOTA) and discussed the
role of NTPs in opioid depend-
ence. The narcotic treatment pro-
grams (NTPs) within the state of
Kentucky’s opioid treatment re-
sponsibility falls under the regula-
tory requirements of 908 KAR
1:340 (narcotic treatment pro-
grams) and 908 KAR 1:370

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
10 | P a g e
(licensing procedures nd stand-
ards for persons and agencies op-
erating nonmedical-based and
nonhospital-based alcohol and
other treatment programs).
There are NTPs spread around
the state, and they each provide
medication-assisted treatment
for individuals whose goal is to
reduce and eliminate an individu-
al’s dependence upon an opioid
substance. (See Figure 9.) The
primary treatment medication
prescribed is methadone, but a
number of programs also are eli-
gible to dispense buprenorphine
in addition to methadone. health
and safety of the clients as well as
ensure the security and control of
the medications. This control in-
volves the regulation, storage,
dosing and administration and to
maintain efficacy and verify ac-
countability.
The NTPs themselves provide
medically monitored drug treat-
ment and related counseling ser-
vices to patients who are physio-
logically dependent upon a nar-
cotic drug such as heroin, mor-
phine and other opioids such as
oxycodone and hydrocodone.
Their mission is to empower per-
sons with Opioid Use Disorder so
they can recover their health and
improve their quality of life. The
goal of NTPS is to provide a safe
environment that includes a com-
prehensive, structured recovery
program of counseling, educa-
tion, medical care and case man-
agement. Patients are required
to abstain from illegal and unap-
proved drug use. Through treat-
ment, patients can reestablish
and recover family and social re-
lationships and pursue or main-
tain meaningful employment.
(See a complete list of NTP’s in
Figure 10.)
In addition to the ongoing over-
sight of the NTPs, the program is
also responsible for the evalua-
tion of requests from the pro-
grams for approval of waivers or
exceptions to the regulations for
individual clients whose particular
circumstances may require an ad-
justment or change in the medi-
cation dosing routine. These re-
quests are examined in accord-
ance with guidelines to assure
compliance with the regulatory
requirements and approved or
denied accordingly. Where ap-
propriate, comments or explana-
tions are provided with the deci-
sion in order to assure there is
complete understanding on the
part of the requesting program.
Information and data relating to
the NTPs is maintained by
DBHDID to evaluate trends, asso-
ciations, or disparities in the oper-
ations of the programs. This also
includes a tracking system and
evaluation checklist that accom-
panies each incoming waiver or
Figure 9. Narcotics Treatment Programs/Opioid Treatment Programs in 19 cities with 21 locations around Kentucky

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
11 | P a g e
Program Name Street City Zip Phone
Ultimate Treatment Center 3655 Winchester Avenue Ashland 41101 (606) 393-4632
Center for Behavioral Health Ky, Inc. 1990 Louisville Road, Suite 110 Bowling Green 42101 (270) 782-2100
BHG XXXIV, LLC 967 South Hwy. 25 West Corbin 40702 (606) 526-9348
NKY Med Clinic, LLC 1717 Madison Avenue Covington 41011 (859) 360-0250
E-Town Addiction Solutions, LCC 2645 Leitchfield Road, Suite 104 Elizabethtown 42701 (270) 234-8180
Center for Behavioral Health Ky, Inc. 2225 Lawrenceburg Rd., Building C Frankfort 40601 (502) 352-2111
BHG XXVI, LLC 48 Independence Drive Hazard 41701 (606) 487-1646
Western KY Medical, LLC 609 Hammond Plaza Hopkinsville 42240 (270) 887-8333
BHG XXXV, LLC 340 Legion Drive, Suites 32 Lexington 40504 (859) 276-0533
Bluegrass Narcotics Addictions Program 3161 Custer Drive Suite 4 Lexington 40517 (859) 977-6080
Methadone Opiate Rehabilitation Ed. Ctr. 1448 South15th St. Louisville 40210 (502) 574-6414
Center for Behavioral Health Kentucky, 1402-A Browns Lane Louisville 40207 (502) 894-0234
BHGXXXIII, LLC 4625 Falcon Crest Paducah 42001 (270) 443-0096
BHG XXIV, LLC 628 Jefferson Ave. Paintsville 41240 (606) 789-6966
BHG XXV, LLC 368 South Mayo Trail Pikeville 41501 (606) 437-0047
Pinnacle Health, Carroll 539 A 11th St. Carrollton 41008 (502 ) 732-3070
Pinnacle Health, Simpson 2714 Nashville Rd. Franklin 42134 (270) 253-3078
Pinnacle Health, Georgetown 105 Eastside Drive Georgetown 40324 (502) 868-0664
Pinnacle Health, Maysville 152 E. 2nd St. Maysville 41056 (606) 564-0303
Pinnacle Health, Daviess 3032 Hwy 60 Owensboro 42303 (270) 685-5029
Center for Behavioral Health Ky, Inc., 1018 Ival James Blvd., Ste C Richmond 40475 (502) 352-2111
Figure 10. Kentucky NTP/OTP Contact Information
exception request in order to en-
sure accuracy and maintain ac-
countability. The information and
data relating to the NTPs is main-
tained by DBHDID as the state
oversight agency in order to as-
sure that the NTP meet the high-
est standards of accountability in
the performance of their NTP ser-
vice responsibilities.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
12 | P a g e
Lockbox Distribution Campaigns – done in
partnership with law enforcement, DCBS,
pain clinics, etc.
Awareness Campaigns – use of brochures,
billboards, social media, radio, and televi-
sion PSAs concerning opioids
Coordinating community and professional
trainings and policy regarding substance
use, opioid addiction, naltrexone, MAT, and
needle exchanges
Conducting trainings with school nurses,
health department staff, parents, coalition
groups, physicians, first responders, and law
enforcement
Assisting community partners in developing
curricula and policy regarding substance us
Holding community forums to discuss the
opioid crisis
FIGURE 11. REGIONAL PREVENTION CENTERS:
RESPONSE TO OPIOID ADDICTION CRISIS
Regional Prevention Centers
The opioid crisis in the state of Kentucky requires
strong prevention. Currently underway are coordi-
nated actions to curb increasing rates of opioid use
and dependence. The Prevention Branch within
DBHDID provides federal and state funding and oth-
er support to the Regional Prevention Centers
throughout Kentucky. The principle funding source
for RPCs is the SAMHSA Substance Abuse Preven-
tion and Treatment (SAPT) Block Grant Regional
Prevention Centers (RPC) work in a variety of set-
tings and with diverse partners to address substance
use in Kentucky. RPCs are regionally based and cov-
er anywhere from five to 17 counties. There are 14
RPCs in Kentucky. RPCs are charged with the respon-
sibility of working with community partners to re-
duce drug use and abuse. The goal is to empower
communities through skills training and technical as-
sistance so that they become mobilized around sub-
stance use prevention. RPC’s work with community
coalitions whose purpose it is to address problems
locally. RPC’s provide support to local Drug Free Co-
alitions (DFCs), Agencies for Substance Abuse Pre-
vention groups (ASAP), faith community, schools,
law enforcement, treatment providers, and the med-
ical community.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
13 | P a g e
Q & A with Dr. Allen J. Brenzel, M.D., MBA
Medical/Clinical Director for Department for Behavior-
al Health, Developmental & Intellectual Disabilities
Medication Assisted Treatment
Q: What is your philosophy concerning Medication Assisted Treat-
ment (MAT)?
Brenzel: MAT is a critical tool in our toolbox of interven-
tions to allow those with opiate dependence to enter and
maintain recovery. Opiate Addiction changes brain chemis-
try in profound ways. For some, medications are the critical
first step in allowing the individual to develop control over
intense cravings and diminish withdrawal symptoms to
manageable levels. It is at this point that healing can begin
and the individual is capable of benefitting from associated
interventions.
Q: There is a great deal of concern about MAT drugs being diverted
for non-prescribed use. Do you see this as a problem and if so what is
DBHDID (the Cabinet) doing about it? Are there any messages that
you think are important related to diversion?
Brenzel: Some of the medications used in MAT have po-
tential for misuse and illegal diversion. Because of this,
Methadone for addiction treatment is prescribed in moni-
tored setting with close monitoring and limited take home
dosing. Buprenorphine can be prescribed for up to 30 day
supplies; however, for it to be prescribed appropriately,
those in treatment should be seen regularly, have random
drug screens, and be required to be in active therapies and
supports such as peer mediated support network. CHFS
has worked with the Kentucky Board of Medical Licensure
to issue revised scope of practice regulations that set expec-
tation for appropriate prescribing and monitoring. The Cab-
inet has worked with Managed Care Organizations to insure
that Managed Care Medicaid plans provide preauthoriza-
tion requirements that specify dosing and monitoring are
occurring and that individuals are in treatment as well re-
ceiving medications. BHDID is working to develop access
to high quality MAT services through increasing provider
networks.
Continued on page 14..

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
14 | P a g e
More of the Interview with Dr. Brenzel
Q: In reality there still appears to be a great deal of stigma within the general public
(and perhaps among providers) about the use of MAT in treating SUD. There also
appears to be a continuing belief that abstinence is the only approach that works.
Do you see any progress on this front?
Brenzel: It must be recognized that addiction is a brain disorder and that especial-
ly opiate addiction involves changes to brain chemistry are so substantial that
medications may be required. Relapse rates in abstinence only based treatment
indicate that many individuals may not be able to directly to abstinence based re-
covery. I do believe we are making progress in recognizing that the best treat-
ment is individualized to the person and that MAT is not “substituting one addic-
tion for another” but a lifesaving and appropriate treatment.
Q: Another long held concern about MAT is the view that it is trading one drug for
another. Do people really ever get off opiate replacement drugs completely? How
long is the maintenance phase on average?
Brenzel: With MAT, the initial goal is tapering and discontinuing the medication
support when clinically appropriate. For some, due to the chronic and relapsing
nature of addiction, medication support may be required on an on—going basis.
Science has not yet determined what percentage of individuals may require long
term medication. It could be as high as 30 percent.
Q: What is the Department of Behavioral Health, Developmental and Intellectual
Disabilities (or the Cabinet) doing to ensure access for individuals who want MAT?
Brenzel: The key will be working to create an adequate network of high quality
providers through education, advocacy for appropriate reimbursement including
considering bundled payment options, and ongoing training and support for pro-
viders.
Q: Despite all the bad news in the press about the spread of heroin and the related
overdose deaths, is there any good news out there related to our efforts to either
reduce the availability of opioids and/or improve treatment for those who are ad-
dicted?
Brenzel: With the addition of Substance Abuse Treatment ser-
vices as a covered benefit in the Medicaid program, and the en-
actment and emerging enforcement of the Mental Health and
Substance Abuse Parity Act, we are beginning to see improved
access to treatment and the development of a more robust and
evidence based provider network.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
15 | P a g e
This Just In… New legislation made possible KRS
217.186 which supports the use of Nalox-
one and protects any person administer-
ing Naloxone in good faith from criminal
and civil liability.
201 KAR 2:360 – pharmacists are permit-
ted to dispense Naloxone if they have
received the required training and have
an agreement with a doctor to dispense.
Some insurance plans may cover the cost
of the kit however; many will have to pay
out-of-pocket. Humana Care Source, a
Medicaid Managed Care Organization,
has agreed to cover the cost. The Ken-
tucky Board of Pharmacy has trained
roughly 500 pharmacists across the state.
Kroger in northern Kentucky has required
all pharmacists to receive training, while
CVS has also proven adamant about in-
creasing the availability of Naloxone. See
Figure 9 for a portrayal of how Nalox-
one reverses the effects of opioids.
Narcan is the trade name for Naloxone;
the FDA has approved a Narcan nasal
product and Adapt Pharma has agreed to
sell kits to the public sector for $75.00.
The Clinton Foundation has teamed up
with Adapt Pharma to fund one kit for
every single high school in the US – Ken-
tucky included. BHDID children’s branch
will be available to teach schools how to
screen and refer youth with substance
use issues for treatment services.
People Advocating Recovery (PAR), KY
Harm Reduction Coalition, UK Hospital,
UofL Hospital, St. Elizabeth Hospital and
UK Adolescent Psychiatry are working
toward distributing naloxone kits.
Figure 12. Demonstrates how an opioid overdose oc-
curs and how Naloxone is able to intervene and reverse
the overdose.

Best Practice Spotlight Issue Number 4: Medication Assisted Treatment
16 | P a g e
References
Fullerton, C.A., Meelee, K., Thomas, C.P., Lyman, D.R., Montejano,
L.B., Dougherty, R.H., … Delphin-Rittmon, M.E. (2014). Medica-
tion-assisted treatment with methadone: Assessing the evidence.
Psychiatric Services, 65(2), 146-157.
MacMullen, N.J., Dulsk, L.A., & Blobaum, P. (2014). Evidence-based
Interventions for neonatal abstinence syndrome: Pediatric Nurs-
ing, 40(4), 165-203 39p.
Pritham, U.A., Paul, J.A., & Hayes, M.J. (2012). Opioid dependency in
Pregnancy and length of stay for neonatal abstinence syndrome.
JOGNN: Journal of Obstetric, Gynecologic & Neonatal Nursing, 41
(2), 180-190 11p. doi:10.1111/j.1552-6909.2011.01330.x
Substance Abuse and Mental Health Services Administration. (2014).
Treatment Improvement Protocol: TIP 43. Rockville, MD: U.S. De-
partment of Health and Human Services.
Thomas, C.P., Fullerton, C.A., Meelee, K., Montejano, L., Lyman,
R.D., Dougherty, R.H., … Delphin-Rittmon, M.E. (2014). Medica-
tion-assisted treatment with buprenorphine: Assessing the evi-
dence. Psychiatric Services, 65(2), 158-170.
Volkow, N.D., Frieden, T.R., Hyde, P.S. & Cha, S.S. (2014) Medication
Assisted therapies – tackling the opioid-overdose epidemic. The
New England Journal of Medicine, 370(22), 2063-2066.
Resources
For more information on COR-12 please visit www.hazeldenbettyford.org
For more information on Medication Assisted Treatment and the evidence
supporting its use visit:
http://www.samhsa.gov/medication-assisted-treatment
https://www.whitehouse.gov/sites/default/files/ondcp/recovery/
medication_assisted_treatment_9-21-20121.pdf
http://attcnetwork.org/about/about.aspx
Institute for Excellence in
Behavioral Health
Louis Kurtz, M.Ed. Interim Director
351 Perkins Hall
Eastern Kentucky University
Office: 859-622-7281
Website: www.iebh.eku.edu
Kentucky Department of Behavioral Health Developmental and Intellectual
Disabilities
KY SMARTS Grant Initiative
Kristopher Shera, MPA MAT-PDOA Pro-ject Director,
502-782-7802
Narcotic Treatment Programs
Ron Easterly, M.D., MPH State Opioid Treatment Authority [email protected]
502-782-6250
Regional Prevention Centers
Phyllis H Millspaugh, M.A. Branch Man-ager, [email protected]
502-782-6234
Printed in part or whole with federal or state funds M/D/F
Contact Information
The Institute for Excellence in Behavioral Health is a contracted initiative of the Department for Behavioral Health, Developmen-tal and Intellectual Disabilities in
partnership with the Training Resource Center.