Embed Size (px)
Citation preview

Issue 39
Dear Readers: Someone said once that if you live here, in our part of the country, you can live anywhere. It seems that every newsletter starts with a comment on the change in the weather and here we go again. What a summer we had! Let’s hope that the beautiful weather we are enjoying now that fall is almost here will last and last. We are lucky though, to be able to enjoy a dramatic and colorful change in seasons. Living here affords us another luxury that we sometimes overlook. We are fortunate to be located within less than 50 miles of the best medical treatment you can find for nearly every condition, but particularly for MG. This was especially evident at our annual membership meeting last Saturday, September 11. Our keynote speaker was Dr. Daniel Drachman, Professor of Neurology at Johns Hopkins. Also attending the meeting were Dr. Charlene Hafer-Macko, Medical Director, Myasthenia Gravis Center and Associate Professor of Neurology at University of Maryland Hospital and Dr. Richard Macko, Professor of Neurology, Baltimore Veterans Affairs Medical Center. The majority of our membership sees one of these excellent doctors for their MG care. Dr. Drachman held us all nearly spellbound with his presentation. We have all heard the familiar story of the nerve ending transmitting the impulse via acetylcholine to the receptor sites many, many times, but not in the way Dr. Drachman presented it to us at this meeting. The information he shared with us about his Genome Study and how it can help with future treatments of MG was very exciting. For those of you who were unable to attend, we will have a DVD available in the near future. A professional videographer taped Dr. Drachman’s presentation for our lending library. The Chairperson of our National Board of Directors, Sam Schulhof, attended our meeting and gave a very nice talk on the benefits of volunteerism. We are very happy that our chapter was first to be selected for a visit by a member of our National Board. It takes up nearly an entire weekend to visit our chapter, so we send Sam a special thank-you. The Annual Meeting of the National Foundation will take place next May, in Baltimore, at the Tremont Hotel. As we announced at the meeting, the board is working to budget as much as we can to allow the greatest attendance possible from our chapter. More details later on this. Thank you, each and everyone, on behalf of the board and myself for your continued support and your generous donations.
September, 2010
MD/DC/DE CHAPTER NEWSLETTER
Marika Bates Chapter Chair
Thank You! & Podcast information Pg 2 Everything you ever wanted to know about Mestinon Pg 10 Support group news Pg 3 The Roles of Insurance Case Manager Latin Corner Pg 4 & Patient Advocate Pg 11 Emily’s Story Pg 5 Abstracts Pg 12 How to prepare for IvIg Pg 6 Hands-only CPR / Medications that MAY worsen MG Pg 13 Free Drug Information Pg 8 Lending Library Pg 14 Infections and MG Pg 9 Holiday Humor Pg 15
MG MATTERS
A quarterly publication of the MD/DC/DE CHAPTER, MGFA
Carol Welty - Founder
Publisher -Lynn Waltz Editor - Dianne Gatton
EXECUTIVE COMMITTEE
Marika Bates, Chair Joe Cservek Bill DeLorenzo Aubrey Hellstrom Bob Howe, Treasurer Carol Roman Marilyn McCloskey Stanley Way Gerry Weinrib
Lifetime Board Member- Emeritus. We welcome your story or article and request that it be submitted by November 1st in order to be considered for the December newsletter. Help us distribute information and continue to create awareness of Myasthenia Gravis. Call or send us the name of your physicians, optometrists, dentists or anyone else you would like to add to our mailing list.
Any advertisement in this newsletter is paid for by the individual and/or company and does not reflect any official endorsement of the MD/DC/DE Chapter or the MGFA.
Restricted Virginia Mistr Vernon Collins in honor of Carol Welty
Unrestricted Lois Smith Brian Stevenson Charles Althoff Joseph Lo Grasso Harry Krewsun Sam & Georgiann Sbona Ted & Antoinette McFadden David & Catherine Fisher If you would like your donation “restricted” (to be used for newsletter, brochures, research, patient assistance, fundraising expenses, etc) please indicate your choice on your check. A big “Thank You” to IgG America & A&M Printing for their constant support of our Annual Meeting.
Dr. Ted Burns from the University of Virginia and a member of the M/SAB is producing a series of patient oriented podcasts for MGFA with information on the diagnosis, treatment, and management of MG. Listen to the first three at http://www.myasthenia.org/podcasts.cfm MGFA has partnered with AANEM (American Association of Neuromuscular & Electrodiagnostic Medicine) to produce a series of podcasts related to myasthenia gravis. To listen to the first one on the safety of the influenza vaccine for patients with myasthenia gravis, go to http://www.myasthenia.org/ and click on the appropriate link. Watch for future podcasts. As always, consult with your physician directly before making any medical decisions. ~~~For those, like myself, who are asking “what is a podcast?”~~~ Definition of: podcast (iPOD broadCAST) An audio broadcast that has been converted to an MP3 file or other audio file format for playback in a digital music player. Although many podcasts are played in a regular computer, the original idea was to listen on a portable device; hence, the "pod" name from "iPod." Although podcasts are mostly verbal, they may contain music, images and video. ~ 2 ~
Remembering “Riley”, our Chapter Mascot.
Dogs can acquire MG too! Read Riley’s’ story on our
webpage.
Any medical views expressed in this
newsletter are those of the
individual author and do not reflect
any official position of the MGFA or the
MD/DC/DE Chapter.
Always contact
your own physician who
knows your situation best.

CONGRATULATIONS!!
Richard & Alma Arnold
64th Wedding Anniversary 7-30-10
We first met Alma, Richard and their family at the Baltimore Support Group quite a few years ago when Alma was recovering from a MG crisis at University of Maryland Hospital. She was also a member of Norberta Parks Perry Hall Support Group. Her fantastic spirit is an inspiration to all of us.
~~ OTHER KINDS OF SUPPORT~~ For those who have asked for information about Plasmapheresis there is a really informative video at www.mgakc.org/myastheniagravis IG Living! Blog Informative blogs on living with a chronic disease and helpful information for those receiving IvIg treatments www.igliving.com/BlogEngine HRS Erase Partners with hospitals to help patients find solutions to pay their medical bills, including helping them apply for benefits through public programs. If you need assistance, ask your hospital if they partner with HRS Erase. www.hrserase.com MDA Quest Products & Services A listing of websites that provide products & services to aid daily living for those who need physical assistance. http://quest.mda.org/products-services
Danielle White is in the process of starting a support group in the Newark, Delaware area. Danielle ran a support group several years ago, so her name may be familiar to some of you. Please email her at [email protected] if you would like more information.
Myasthenia Gravis Foundation of America, Inc. 355 Lexington Avenue, 15th Floor
New York, NY 10017-6603 1-800-541-5454 / www.myasthenia.org
MD/DC/DE CHAPTER
PO Box 186 Pasadena, Md. 21123-0186
410-437-1157 / 1-866-437-2881 www.myasthenia.org
(click on Chapters, Maryland)
WESTERN MD SUPPORT GROUP Dave Miller - 717-597-5107
GLEN BURNIE SUPPORT GROUP 1st Saturday of each month, 10 - noon Baltimore Washington Medical Center
Lynn Waltz - 410-437-3761 / [email protected]
BETHESDA/DC SUPPORT GROUP 3rd Saturday of each month, 10-noon
Suburban Hospital Bill DeLorenzo - 301-384-1229 / [email protected]
BEAR, DELAWARE SUPPORT GROUP Marilyn McCloskey, RN - 302-292-0876
Telephone Buddies
Grace DiGiorgio
301-208-8326 Rockville
Medie McLaughlin 410-284-0647 Dundalk
Thymectomy
Both Angel and Amy have had thymectomies and are doing great. They are willing to share their experience with you. You can reach them at…
Angel - [email protected]
Amy - [email protected]
~ 3 ~
New Local Number

~~EL RINCÓN LATINO~~ (THE LATIN CORNER)
An Argentinean Myasthenic wrote the following “Reflections of a Myasthenic”. She very graciously gave us permission to publish an English version here.
WISH II…. (She also wrote WISH I) by M. Julieta Grande
[email protected] Submitted and translated into English
by Bill De Lorenzo
Who has not dreamed about wishes one might ask for, no matter under whatever circumstance it might be. Possible wishes, impossible wishes (because of one’s lack of belief in miracles), attainable wishes, unattainable wishes, silly wishes (but, non-the-less valid when all is said and done), intelligent and well thought-out wishes, small wishes, BIG wishes, personal wishes, another’s wishes…WISHES, SO MANY WISHES… Thinking about what all of us would like, I’ve compiled the following list: • I wish that all staircases had a “button,” that when pressed, would transform them into ramps… • I wish that they would make glasses and cups lighter, so that we could lift them “easily” when making a toast… • I wish that “gravity” would disappear… • I wish that there were a bench on every street corner, so that one could rest and regain strength… • I wish that people would understand those who are nasal… • I wish that meat were more tender… • I wish that they would sell MESTINON in Kiosks, to help us in case of loss or having forgotten it… • I wish that a SINGLE MESTINON pill would last, at the minimum, for an entire week… • I wish that I could sleep, without having to rely on an alarm clock… • I wish that ring-topped bottles were not so difficult to open… • I wish that there were banisters on EVERY staircase…(and if not, that they would turn into ramps)… • I wish that all chairs would have head rests… • I wish that one could wear high heels (really high), obviously for women, or maybe some men would also want them, one never knows…
• I wish that it were easy to button and unbutton a shirt… • I wish that a “bubble” would form a barrier around every virus and bacteria that might appear… • I wish that buses would stop at the edge of the sidewalk… • I wish that all subway stations had elevators or escalators… • I wish that medications did NOT HAVE CONTRAINDICATIONS… • I wish that dancing would not weaken my legs… • I wish that science would make more advances in the area of autoimmune diseases… • I wish that God would offer some explanations… • I wish that hot showers wouldn’t weaken me… • I wish that massages were not contraindicated… • I wish that drooping eyelids were only for sleeping… • I wish that elevators ALWAYS functioned, or on the contrary, stairs had banisters (if they hadn’t already been transformed into ramps by pressing a button)… • I wish that bathrooms in bars, restaurants, offices, cinemas, theatres, recital halls, and all other public places were not always SO far away…(or at the top of the stairs, that sometimes doesn’t have a banister, or hasn’t even been converted to a ramp)… • I wish that one didn’t have to ask for help with combing one’s hair… • I wish that our guide dogs would learn to bring us MESTINON (it’s a question of teaching them)… • I wish that Winter wouldn’t bring the usual colds, flu’s, anginas, bronchitis, that impede breathing… • I wish that Summer didn’t bring on the similar impediments due to high temperatures… • I wish that ocean waves did not cause one to fall… • I wish that after swimming, one didn’t need a “Tow Truck,” to get out of the water… • I wish that coats weren’t so heavy that they impede our walking… • I wish that purses, backpacks, wallets, suitcases and other objects that are used to carry things, ALL had wheels… • I wish that Intensive Care Rooms had longer visiting hours… • I wish that one’s health could be bought just around the corner… • I wish that wisdom and rationality would reign before any decision… • I wish that everything in life had meaning, and if not, one would seek it… ~ 4 ~

~~Emily's Story ~ A Reason for Hope~~ Written by Emily Wineland, daughter of Sue Wineland, Connecticut "Nutmeg" State Chapter Board Member
The symptoms were puzzling from the beginning: slurred speech; crooked smile; drooping eyelid; double vision; difficulty chewing, and general fatigue. They would suddenly appear, out of nowhere. I recall numerous instances when I was unable to formulate words after a long day of teaching outdoor education, and my students would look at me in confusion. My mysteriously deteriorating health caused me social discomfort and embarrassment on many occasions. Sometimes, it was so difficult for me to smile or to communicate that people would peg me as unfriendly. At times when I talked, the words came out so nasally that I sounded hearing-impaired. Being diagnosed with myasthenia gravis finally gave me an answer to why my body wasn't functioning properly. I was relieved I had an answer, but fearful of the unknown. And I was resentful. Why me? I was 26 and vibrant. I had been a collegiate swimmer and had just completed a marathon. I was devastated to think I would not have the muscle strength to participate in sports anymore. I wanted answers and explanations during office visits but there were still so many unknowns.
I began taking Mestinon, prescribed to me by my doctor to be taken as needed. I habitually took one (60 mg) pill each morning with breakfast and carried an additional pill in my pocket. My symptoms began to improve and I began to focus on my overall wellness. In May 2008, one year after I was diagnosed, I had a thymectomy. I learned how to adapt to and manage my disease by experimenting with nutrition, exercise and acupuncture, and I gradually began to do everything I did before I got sick. I love surfing, swimming and jogging and I am able to do these things when my energy levels are high. It takes me longer to recover and I need more rest than other people, but I have learned to stop comparing myself to others. Last summer I completed my first triathlon; I also stopped taking Mestinon every day. The medication was causing my muscles to twitch and cramp severely while exercising, so after talking to my doctor, I stopped taking it. I have been medication-free ever since. Two months after my thymectomy, I started taking classes full-time to complete prerequisite classes for dental school. This summer I will be applying to dental school and, I hope, entering in the fall of 2011. A friend of mine questioned my desire to go into dentistry because it requires constant neck muscle strength... but I am not about to let any doubts get in the way of fulfilling my dreams! I have found that the most important thing that I can do for my MG symptoms is lessening the stresses in my life to the best of my ability. I have learned to be gentle and understanding with myself, allowing days off to rest and do nothing, without feeling guilty about it. Moderate exercise like yoga keeps me emotionally grounded, helps me sleep soundly, and gives me a healthy appetite. I make sure that I eat nutritious, whole foods, stay positive, and rest, rest, rest! AMPS: The Nutmeg -June 2010
Centenarian Mathilda Karel Spak dies
Although she may be best known for her 2003 write-in campaign for governor of California, Spak's true passion until her very last days was her volunteer work. Until March of this year, when Spak attended and "held court" at the annual gala celebration for the Myasthenia Gravis Foundation of California, the energetic centenarian was the hub of any party. Spak was also very active with the Myasthenia Gravis Foundation, which works to find a cure for the neuromuscular disorder. Spak's mother was diagnosed with MG. Throughout her life, Spak liked to joke that the recipe for longevity was cookies, cake, candy - and no veggies. Another story she liked to tell was of a time she fell at her apartment. When four firefighters arrived to transport her to the hospital, she reportedly said, "Why would I want to go to the hospital, when I can stay here with four handsome guys?" Spak died in her sleep at her home in Long Beach. She was 103.
Our life's a stage, a comedy: either learn to play and take it lightly, or bear its troubles patiently. Palladas Palladas was a Greek poet, who lived in Alexandria, Egypt. ~ 5 ~

~~How to Best Prepare for IVIG Treatments~~ by Jen Walsh
I have a love/hate relationship with IVIG. I love that it has kept me out of the hospital, preserved my muscles that allow me to breathe, and those that I use to swallow. I hate that it takes six hours to infuse every two weeks (*length of time depends on volume and how fast or slow the infusion can be run and tolerated) and that it doesn't always work consistently to manage my other symptoms. I also hate the cost, but love the donors who make it possible for me to receive this life saving treatment. I have an autoimmune neuromuscular disorder called Myasthenia Gravis which takes away my ability to open my eyes, walk, or grip things at its mildest and can literally cause my diaphragm to stop working at it's worst. Fortunately there are treatments, but there is no cure. And so, my physician team decided that I would be a good candidate for IVIG. This is my guide for new patients undergoing IVIG treatment - or those who don't feel their treatment is going so well. I have been receiving IVIG since December 2009 and my current protocol is every two weeks. 1. Hydrate. Hydrate, Hydrate – I don't care if you don't drink water, this is a MUST! You must start hydrating at least 48 hours prior to infusion and for 48 hours after, not to mention during. If you are not well hydrated you are increasing your risk of blood clots, aseptic meningitis (a.k.a. the worlds most excruciatingly painful headache), and an extreme feeling of the flu.
2. Take Benedryl and Tylenol: Most doctors will order this in what they call "pre-meds." Ask your nurse first so you don't double dose. If you aren't getting it in the IV, make sure to take it by mouth. The Benedryl gives you a better chance of not having an allergic reaction which can set off the immune response thus rendering the whole treatment useless. The Tylenol will reduce the achy, flu like feeling as your body processes the high volume of healthy donor immune cells.
* Tylenol & Benedryl can be taken every 6 hours during infusion day to help minimize post infusion side effects.
3. Get a good night's sleep before and after: Anyone with an autoimmune disorder knows a poor night's sleep can worsen their symptoms. Well, I have found that my IVIG works better if I get a good night's sleep the night before and the night of treatment.
4. Ask your doctor if you can receive it in home: Some insurance companies will cover in home treatment. This is such a wonderful option for so many reasons. Most importantly, you don't need to arrange transportation to and from the infusion center and you will not expose yourself to all the germs that are in the hospital or infusion center.
* You are much more relaxed in your own home and are monitored closely by your RN for onset of complications or side effects. 5. Prepare many snacks to eat during treatment: I tend to crave protein based foods but anything healthy is good. It will help stave off a headache or stomach ache. My recommendations include...cheese and crackers, nuts, bananas, Clementines, a bagel with cream cheese and tomato slices. Prepare whatever you like the night before so you don't have to worry about it the day of. 6. Avoid stress at ail costs: Stress sets off the immune response and will render the treatment less effective because your faulty immune system wins the fight so to speak. I have found when there is high stress, my treat-ments do not work so well. Jen Walsh is a Great Lakes Chapter member from Grand Rapids, Michigan who has published multiple articles and blogs on her experiences with myasthenia gravis, as well as a PSA for June is MG Awareness Month 2010. You can read this article in its original location (published May 25, 2010) at:
http://www.associatedcontent.com/article/5412436/how_to_best_prepare_for_ivig_treatments.html AMPS: MG Communicator - Great Lakes Chapter Summer-2010 Issue * Comments added by Jo Monka, RN. Jo is an infusion nurse for IgG America and administers IvIg to some of our Chapter members, myself included. Lynn Waltz
~~What is IvIg?~~
IvIg is intravenous immune globulin. It is also known as pooled human gamma globulin or simply gamma globulin. IvIg has been used for decades in modern medicine in the treatment of a variety of infectious or inflammatory diseases. In patients who are lacking in the antibodies necessary to fight infection, IvIg replaces those lost antibodies. IvIg is used also in the treatment of a variety of autoimmune disorders. Over the past two decades, IvIg has been used extensively in the treatment of some autoimmune neurological disorders, including myasthenia gravis. There are indications that IvIg is an effective treatment for some patients with autoimmune myasthenia gravis. (Copied from the MGFA brochure Intravenous Immunoglobulins)
Life isn't about waiting for the storm to pass it's about learning to dance in the Rain
~ 6 ~

~ 7 ~
~~GET YOUR DRUGS AT 50% OFF OR EVEN FREE ~~
Anyone who regularly takes prescription medication knows how pricey drugs can be. Fortunately, there are places where you can buy your drugs for less—or even get them for free. The key is knowing where to look. Important: Although most low cost drug programs have income eligibility requirements, do not assume that you won't be accepted into a program just because your income is officially too high. Many programs will consider applications on a case-by-case basis. Best resources for finding low-cost or free medications. DRUG DISCOUNT NETWORKS Some groups connect patients to public and private assistance programs that provide discounted or free drugs to eligible patients. These include... Partnership for Prescription Assistance 888-477-2669, www.pparx.org This collaborative network of professional medical organizations, including the American Academy of Family Physicians, and private groups links patients with more than 475 public and private patient assistance programs that offer more than 2.500 drugs at reduced cost or no charge. Income qualifications vary by stale. Together Rx Program 800-444-4106, http://www.togetherrxaccess.com/Tx/jsp/home.jsp Backed by a consortium of pharmaceutical companies, this program provides a 15% to 40% discount on more than 300 brand-name and generic prescription drugs. The program targets people who don't have prescription drug coverage with annual incomes of $30,000 or less for individuals, $40,000 for a family of two...and up to $70,000 for a family of five. PHARMACEUTICAL PATIENT-ASSISTANCE PROGRAMS Major pharmaceutical companies have their own patient-assistance programs that offer many—though not all—drugs at a discount, or even for free, to people who cannot afford them. Eligibility requirements vary—even families earning up to $70,000 a year can qualify. Some companies evaluate applications on a case-by-case basis. To obtain a free copy of Directory of Prescription Drug Patient Assistance Programs, call the Partnership for Prescription Assistance at 800-762-4636. To determine the manufacturer of a particular drug, ask your pharmacist or go http://pdrhealth.com/home/home.aspx (More information is available on the MGFA website at http://www.myasthenia.org/pe_patientresources.cfm)
Among the pharmaceutical companies with programs… AstraZeneca's - AZ & Me Prescription Savings Program 800-292-6363, http://www.astrazeneca-us.com/help-affording-your-medicines/prescription-saving-program/ GlaxoSmithKline 888-825-5249, (IMURAN) http://www.gskforyou.com/ Click on "A Helping Hand" for a list of all GSK drug-assistance programs. Lilly Cares Patient Assistance Program (Eli Lilly) 800-545-6962, http://www.lillycares.com/Pages/index.aspx Merck Patient Assistance Program 800-727-5400, http://www.merck.com/merckhelps/patientassistance/ home.html Novartis Patient Assistance Foundation 800-277-2254 www.pharma.us.novartis.com Pfizer Connection to Care - 866-776-3700 http://www.pfizerhelpfulanswers.com/pages/programs/ProgramDetails.aspx?p=2 Roche Labs Patient Assistant Foundation (CELLCEPT) 877-757-6243 www.rocheusa.com/programs/patientassist.asp Valeant (MESTINON) – 800- 511-2120. http://www.valeant.com/about/programs/patient-assistance-program.jsp Wyeth Pharmaceutical Patient Assistance Program 800-568-9938 http://www.wyeth.com/contact?rid=/wyeth_html/home/shared/footer/Patient/contact_patient_assist.html Some pharmaceutical companies also offer coupons that can be printed from their Web sites, as well as discount card programs offering savings on some products. Check the drug manufacturers Web site for details.
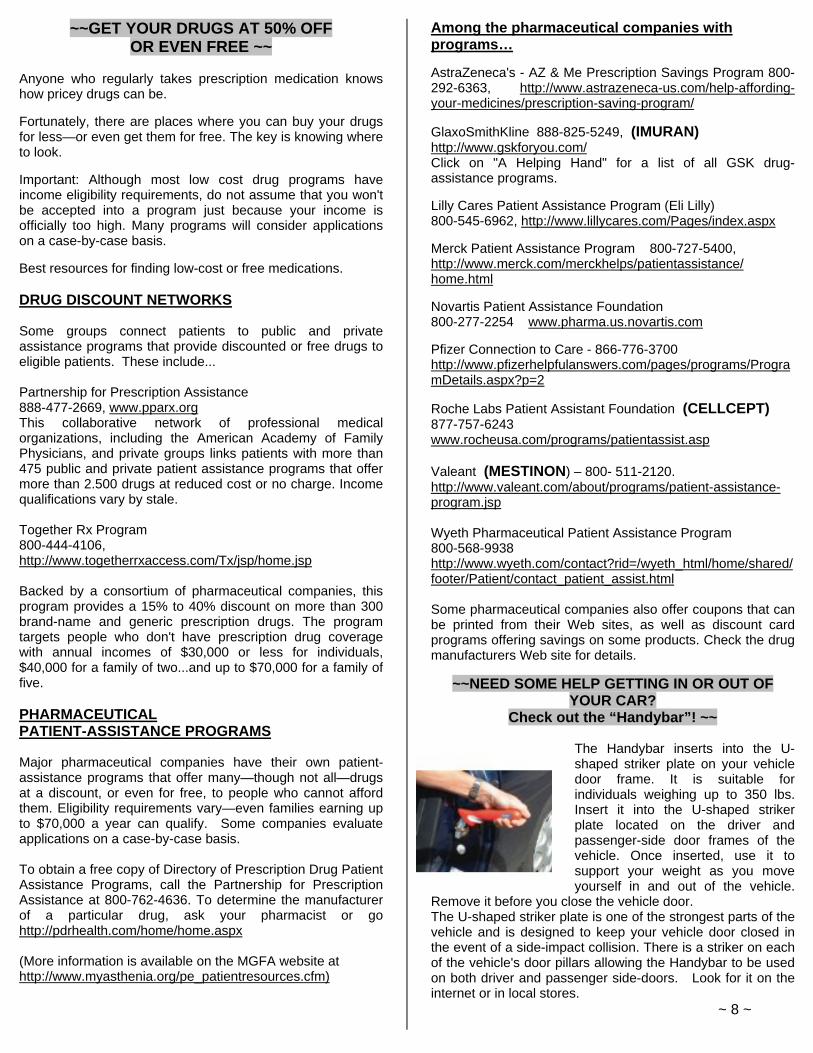
~~NEED SOME HELP GETTING IN OR OUT OF YOUR CAR?
Check out the “Handybar”! ~~
The Handybar inserts into the U-shaped striker plate on your vehicle door frame. It is suitable for individuals weighing up to 350 lbs. Insert it into the U-shaped striker plate located on the driver and passenger-side door frames of the vehicle. Once inserted, use it to support your weight as you move yourself in and out of the vehicle.
Remove it before you close the vehicle door. The U-shaped striker plate is one of the strongest parts of the vehicle and is designed to keep your vehicle door closed in the event of a side-impact collision. There is a striker on each of the vehicle's door pillars allowing the Handybar to be used on both driver and passenger side-doors. Look for it on the internet or in local stores. ~ 8 ~

~~ INFECTIONS AND MG ~~
As you may know, some of the drugs used to treat myasthenia gravis (MG) can make it harder for your body to fight off bacteria or viruses. This may put you at greater risk for infection. Having an infection can cause your MG symptoms to become worse. An important part of managing your condition is to know what to watch for and how to prevent infections. How will I know if I have an infection? One sign of infection is a temperature that is new or higher than normal for you. Sometimes an infection may result in a flare-up of your disease. It is important to speak with your doctor to rule out possible causes of a fever. Some common infections, like pneumonia, involve your respiratory tract. Some of the common symptoms of respiratory infections include: Sore throat - Cough - Sneezing - Runny Nose - Fever - Fatigue - Chills -Shortness of breath What should I do if I think I am sick? Contact your doctor as soon as you notice symptoms of infection. It's best to start treatment before an infection becomes worse. Your doctor can decide which treatment is best for your symptoms and type of infection. Don’t treat infections yourself or use non-prescription products unless directed by your doctor. Your doctor may prescribe medicine for your infection. It is important to take the medicine exactly as prescribed and finish it, even if you start to feel better. Otherwise, the infection may return and be harder to treat. ~ 9 ~
Call Us Today For An Appointment: 410.290.5688
7135 Minstrel Way Suite # 101
Columbia, MD 21045 http://nextgenerationmri.com/
-Watch A 42" Flat-Screen TV While Being Scanned -The Only "TRUE" Open MRI Which Provides -The Most Non-Claustrophobic MRI -0.6 Tesla High-Field Open Scanner -Exceptional Image Quality -Scans Can Be Performed While Sitting, Standing, Or Lying Down -Allows For Weight-Bearing MRI Studies Which Can Detect Certain Problems That Conventional Lie Down MRI Scanners May Overlook
-Fast And Easy Scheduling -Caring And Dedicated Professional Staff -One-On-One Patient Care -Board-Certified Radiologists -Prompt Results For Your Referring Physician -Ample Parking
Now You Can Sit, Relax, And Have Your MRI In A Room With A View...

~~All you ever wanted to know about Mestinon or
“Pyridostigmine bromide, USP” ~~ Mestinon® is an orally ingested cholinesterase inhibitor used as the first source of therapy in treating MG. Acetylcholine is a chemical, one of the main neurotransmitters in the brain that sends nerve impulses to the skeletal (voluntary) muscles. With MG, there is a breakdown of acetylcholine in the neuromuscular receptor sites, responsible for voluntary muscle control. Mestinon® prevents this breakdown of acetylcholine by allowing more acetylcholine to accumulate at the neuromuscular receptor sites, providing more control of voluntary muscle function, such as eye movement, limited strength, swallowing, chewing and breathing. The physician determines the amount of Mestinon® dose and frequency according to the needs of each individual patient. During the initial induction of Mestinon®, the patient should keep a record reflecting the responses of symptoms after each dose. This helps the physician determine the correct dose and frequency for the patient, especially when the patient's MG is unstable. It is very important to follow the physician's instructions pertaining to the patient's Mestinon® dose and frequency. Discuss any change made in your Mestinon® regimen with your physician because too much Mestinon® can induce extreme muscle weakness. Equally important, discuss any instability of Myasthenia Gravis weakness with the physician BEFORE changing the initially prescribed dose and/or frequency. PRECAUTIONS AND SIDE EFFECTS Precaution should be taken in patients with mechanical intestinal and urinary obstruction. Particular precaution should be taken when administering Mestinon® to patients with bronchial asthma. The most common side effects of Mestinon® include nausea, vomiting, diarrhea, abdominal cramps, in-creased tearing, salivation and bronchial secretions. Other side effects are muscle twitching, muscle cramps and weakness. Since Mestinon® is eliminated from the body mainly unchanged by the kidneys; lower doses may be required in patients with renal (kidney) disease. The safety of Mestinon® has not been established during pregnancy and lactation, or in pediatric patients. When taking Mestinon®, failure of improvement of symptoms may be a sign of overdose or underdose. AMPS: MG Ontario Newsletter, May 2010
~~Three forms of MESTINON®~~
1. The conventional 60mg tablets contain pyridostigmine bromide, as well as lactose, silicon dioxide and stearic acid.
2. Mestinon Timespan® tablets contain 60mg of pyridostigmine bromide as well as carnauba wax, corn- derived proteins, magnesium stearate, tribasic calcium phosphate and silica gel. Mestinon Timespan® tablets are the slow-release dosage form. They should not be crushed or broken into pieces as this disturbs the time-release mechanism and could result in IMMEDIATE release instead of slow release of pyridostigmine bromide.
3. Mestinon Syrup® contains 60mg of pyridostigmine bromide. Also included are 5% alcohol, glycerin, lactic acid, sodium benzoate, sorbital, sucrose, FD&C red # 40, FD&C blue # 1, flavors and water. The syrup is raspberry flavored. This formula allows dosage that is more precise for children and people with 'brittle' or fragile MG who may require doses in fractions of the 60mg. It is also more easily swallowed by patients with swallowing difficulties in the morning.
~~Storage of MESTINON® Tablets
and Timespan®~~ MESTINON® Tablets and Timespan® are very hygroscopic (pronounced "hi gro ska pic") which means they readily pick up and retain moisture. Moist MESTINON® Tablets may become mottled or discolored or crumble easily. Moisture affects the appearance of MESTINON® but it does not alter the effectiveness of the drug. Do not store MESTINON® Tablets or TIMESPAN® Tablets in bathrooms or kitchens where there is a higher incidence of moisture in the air. MESTINON® Tablets are packaged in a bottle of 100 or 500 tablets. MESTINON® Timespan® is packaged in a bottle of 30 tablets. Do not remove the desiccant(s) (a small canister containing a drying agent) from any MESTINON® prescription bottle. Source: http://www. valeantcanada.com/
~ 10 ~
Many (not all) people find Mestinon hard on their
stomach. Take Mestinon with food or
even a glass of milk!

~~The Roles of an Insurance Case Manager and Patient Advocate~~
Anyone with a medical condition that requires ongoing care knows well the many frustrations that have nothing to do with medical care itself. Dealing with the insurance company, doctors' staff, pharmacies and other providers can be a headache all its own. And all too often, the many choices — from the treatment plan to selecting a provider for that treatment — can seem overwhelming to patients and their families for whom the entire process is unfamiliar. To streamline the bureaucratic process inherent to medical care, as well as to clarify the choices available to patients and to control costs, a mitigating party can help. This party can be either a case manager or an independent patient advocate, or, in some cases, both. But, before deciding whether to utilize one or both, it will be helpful for patients and their families to understand what roles a case manager and a patient advocate play. The Role of a Case Manager A case manager works for the insurance company. While that individual can help clarify the choices available to a patient, as well as take some of the red tape out of the process, they are paid by and their loyalty is to the insurer. From an insurance company's perspective, a case manager's salary and benefits are another expense to be paid for out of plan members' contributions and deductions. Jose Santoro, director of managed care with NuFACTOR, the specialty pharmacy of FFF Enterprises Inc., says there are good reasons why insurance companies utilize the services of either staff or a contract case manager. For instance, they "ensure appropriate care for a member's disease state, reduce inpatient hospital stays, minimize duplicity of tests and increase utilization of a contracted provider network," he explains. "The insur-ance company can steer the member to the appropriate resources, can have an active role in care coordination and [can] manage cost-effective care." From a patient’s point of view. Having a case manager means having a familiar face or voice to deal with at the insurance company. Rather than calling customer service and having to repeatedly explain their situation to a different company representative, patients can interact with the same person who is familiar with their case history and can provide quick, accurate information about their account.
A case manager is commonly used to help oversee the treatment of people with cancer, HIV and other serious chronic diseases and conditions with high-cost ongoing therapy, such as patients who rely on immune globulin (IG). And, even if they are not automatically assigned a case manager, patients can request one. According to Santoro, assignment of a case manager often occurs when hospitalization is required, particularly when ongoing post-hospitalization treatment or home equipment is also necessary.
Many large companies that are self-insured (i.e., they pay their employees' medical bills out of a pool of money from their profits and hire an insurance company to admin-ister the program) are increasingly relying on case managers to help control costs. A case manager can ensure that the patient isn't receiving duplicate tests, is receiving treatment from in-network providers (thus saving the company money), and is on track with treatment to prevent more serious complications. But, even with a case manager to fully explain all of the options and to act as a regular conduit to the insurance company, it remains important for patients to ask the correct questions so they can get accurate answers. For some families, this is where a patient advocate comes in. The Role of a Patient Advocate Whereas a case manager works for the insurance company, a patient advocate works for the patient. "The patient does not know what they don't know," explains Santoro, which is why they may need a patient advocate to help them map out their treatment options. A patient advocate should have expertise and experience in both medical care and insurance company bureaucracy, making them better equipped than the family to sort out the best course of action. But, while a patient advocate's loyalty is to the patient, that person may not always have the same access to the decision-making process at the insurance company that a case manager would have. And, caution is advised in hiring a patient advocate, since no licensing is required for the profession. In addition, many individuals and firms advertising their patient advocacy services emphasize their ability to negotiate better financial terms with the insurance company and/or care providers — which isn't always what a patient or their family is looking for. When considering whether to hire a patient advocate, some precautions should be taken. For instance, before agreeing to services, patients should find out exactly how much they will be paying and the specifics of what they will get for that money. Those items should be drawn up in a contract so there are no misunderstandings later. In addition, the patient advocate should provide documentation of their expertise that will allow them to assist patients in negotiating the maze of insurance requirements and treatment options. Referrals from previous clients should be requested. Whether a case manager and/or patient advocate is util ized depends upon each patient's needs. However, if a patient advocate is hired, and the patient also has a case manager assigned from their insurer, it's important that the two work as a team. "The advocate would serve the patient better by interacting with the insurer's case manager," says Santoro. "It would not be in lieu of the patient; it would be in conjunction with the patient."
JIM TRAGESER edits the film, religion and books sections for a daily newspaper in the San Diego, Calif., area, and has contributed to two reference books on the blues.
Reprinted with permission grom IGLiving magazine 6-7/10 Issue www.igliving.com ~ 11 ~
Abstracts…….. (A short summary of a speech, report, or other piece of writing) To read the complete paper, click on the links. You may have to register with individual websites.
The MG Composite A valid and reliable outcome measure for MG
Ted M. Burns, MD, Mark Conaway, PhD, Donald B. Sanders, MD On behalf of the MG Composite
and MG-QOL15 Study Group Department of Neurology, University of Virginia
Objective: To study the concurrent and construct validity and test-retest reliability in the practice setting of an outcome measure for myasthenia gravis (MG). Methods: Eleven centers participated in the validation study
of the Myasthenia Gravis Composite (MGC) scale. Patients with MG were evaluated at 2 consecutive visits. Concurrent and construct validities of the MGC were assessed by evaluating MGC scores in the context of other MG-specific outcome measures. We used numerous potential indicators of clinical improvement to assess the sensitivity and specificity of the MGC for detecting clinical improvement. Test-retest reliability was performed on patients at the University of Virginia. Results: A total of 175 patients with MG were enrolled at 11
sites from July 1, 2008, to January 31, 2009. A total of 151
patients were seen in follow-up. Total MGC scores showed excellent concurrent validity with other MG-specific scales. Analyses of sensitivities and specificities of the MGC revealed that a 3-point improvement in total MGC score was optimal for signifying clinical improvement. A 3-point improvement in the MGC also appears to represent a meaningful improvement to most patients, as indicated by improved 15-item myasthenia gravis quality of life scale (MG-QOL15) scores. The psychometric properties were no better for an individualized subscore made up of the 2 functional domains that the patient identified as most important to treat. The test-retest reliability coefficient of the MGC was 98%, with a lower 95% confidence interval of 97%, indicating excellent test-retest reliability.
http://www.neurology.org/cgi/content/abstract/74/18/1434
Update on muscle-specific tyrosine kinase antibody positive myasthenia gravis.
JT Guptill JT & DB Sanders Division of Neurology, Duke University Medical Ctr.
Durham, North Carolina, USA. PURPOSE OF REVIEW: Important concepts regarding the pathogenesis, clinical features, diagnosis and treatment of muscle-specific tyrosine kinase (MuSK) antibody positive myasthenia gravis will be reviewed. Special attention will be paid to clinical phenotypes and treatment, particularly encouraging responses that have been reported to rituximab. RECENT FINDINGS: Worldwide studies confirm three major phenotypes in MuSK antibody positive myasthenia gravis (MMG) patients: indistinguishable from acetylcholine
receptor antibody positive patients, prominent faciopharyngeal weakness, usually with marked muscle atrophy, and relatively isolated neck extensor and respiratory weakness. MMG predominates in women and weakness is typically more severe, with more frequent respiratory crises than non-MuSK myasthenia gravis. Patients with sub-acute bulbar, shoulder, and neck weakness pose unique challenges in terms of differential diagnosis and electrodiagnosis. Electrodiagnostic studies evaluating for disorders of neuromuscular transmission should focus on proximal limb and facial muscles, as well as clinically weak muscles. The response to acetylcholinesterase inhibitors is often disappointing. Long-term outcomes appear favorable though patients typically require more aggressive immunosuppression. Uncontrolled observations report encouraging results with rituximab in the treatment of refractory MMG. The role of thymectomy in the management of these patients remains uncertain. SUMMARY: MuSK antibody positive patients represent a unique subset of myasthenia gravis. Identification of these patients has important diagnostic and disease management implications. http://www.ncbi.nlm.nih.gov/pubmed/20613516
Anesthetic management using remifentanil target controlled infusion without muscle
relaxants in two patients with MG
Abe N, Kunisawa T, Sasakawa T, Takahata O, Iwasaki H. Department of Anesthesia, National Hospital Organization
Hokkaido Cancer Center, Sapporo 003-0804. Japan Two patients with myasthenia gravis were scheduled for surgery. Anesthesia was managed with remifentanil and propofol target-controlled infusion without the use of muscle relaxants. In both cases, we gradually raised the effect-site concentration of remifentanil and performed tracheal intubation at 10 ng x ml(-1). For both patients, the conditions for tracheal intubation were good, and hemodynamics also stabilized during tracheal intubation. Throughout the surgery, muscle relaxants were not required. Thus, the use of these drugs for inducing anesthesia provided good conditions for tracheal intubation and surgery, and it precluded the need for muscle relaxants. http://www.ncbi.nlm.nih.gov/pubmed/20560375
Cytokinetics, Incorporated (Nasdaq: CYTK) announced that the National Institute of Neurological Disorders and Stroke (NINDS) has awarded the company a grant in the amount of $2.9 million to support research and development of CK-2017357, a fast skeletal muscle troponin activator, directed to the potential treatment for myasthenia gravis. The grant was awarded to Cytokinetics under the American Recovery and Reinvestment Act of 2009. ~ 12~

Michael Merlo Managing Director
CAIR Respiratory Services, LLC
11C Gwynns Mill Ct Owings Mills, Md. 21117 410-581-3400
~~WORTH SHARING~~……
Cardiopulmonary resuscitation that consists of only pressing on the chest works about as well and saves as many lives as conventional CPR incorporating both chest compressions and mouth-to-mouth breathing, according to new research. The findings of two studies in which telephone dispatchers instructed bystanders in how to perform CPR suggest that current techniques can be made simpler and less objectionable without harming most patients. "There is inherent appeal to chest compressions alone because of the challenges of doing the rescue breathing," said Thomas D. Rea, a physician at the University of Washington, in Seattle, where one of the studies was done. "If we can simplify the approach, I think we may enable more lay people to perform CPR in cardiac arrests." The American Heart Association, which trained 13 million people in CPR last year, is developing new guidelines for resuscitation that will be released in October. The current guidelines encourage bystanders to at least do chest compressions, also known as hands-only CPR.
New NIH Website offers easy access to
information on Bone Health A new Web resource providing people with the latest science-based information on bone health and bone disease is available through the NIH Osteoporosis and Related Bone Diseases ~ National Resource Center (NRC). The site is www.bones.nih.gov. Strong bones are essential to overall health and quality of life. Visitors to the NRC site will learn about strategies for bone health, such as the prevention and management of osteoporosis, a common bone disease that makes bones weak and prone to fracture. One feature is the Check Up On Your Bones tool, an online interactive bone health assessment that provides personalized information on osteoporosis risk, as well as approaches to enhance bone health.
~~Some Common Medicines That May
Worsen MG Weakness~~
• alpha-interferon • Antibiotics—the aminoglycosides such as
amikacin gentamicin tobramycin (including eye drops) generics that end in "mycin"or"micin"
• Antibiotics—the fluoroquinolones ciprofloxacin generics that end in “floxacin”
• Antibiotics—the macroiides, especially erythromycin azithromycin generics that end in "mycin"or"micin"
• Beta-blockers such as propranolol generics that end in "olol" timolol (including eye drops)
• botulinum toxin • Calcium channel blockers
verapamil felodipine nifedipine
• chloroquine • Contrast dyes or agents that contain iodine • Corticosteroids such as prednisone • d-penicillamine • Magnesium-containing compounds
epsom salts antacids and laxatives such as Gaviscon®, Maalox®, Milk of magnesia, Mylanta
• procainamide • quinidine • quinine • succinylcholine or other neuromuscular-blocking
agents ~ 13 ~
1) You, Me & MG 2) Coping with Prednisone 3) Living with a Gray Disease in a Black and White World 4) The Autoimmune Connection- Essential information for women on diagnosis, treatment and getting on with your life 5) Living well with Autoimmune Disease 6) How Doctors Think 7) Acquired Hope 8) Myasthenia Gravis ~ An Illustrated History 9) A guide to the Diagnosis & Management of MG 10) Beyond the Limits of Myasthenia Gravis 11) The Mystery Guest, MG
12) Don’t drive on the sidewalk – Inspirations through the detours of life 13) You are not your illness – Seven principles for meeting the challenge 14) Just Fine – unmasking concealed chronic illness and pain 15) A Delicate Balance – Living successfully with Chronic Illness 16) I Can't Chew Cookbook 17) Easy-to-Swallow Easy-to-Chew Cookbook *18) Living positively with MG (booklet) *19) Your guide to healthy sleep (booklet)
*20) Breath Easy (booklet) *21) But you LOOK good! (booklet)
~ 14 ~
Myasthenia Gravis Foundation of America, Inc. MD/DC/DE Chapter
~Lending Library~
ONE BOOK per request *THREE BOOKLETS per request
Email Lynn Waltz @ [email protected], supply your home address and make your book request by title name. We will mail the book to you with a self address, stamped label enclosed to make it easy for you to return it. Since we only have one copy of most of our books we ask your cooperation in returning them as soon as you finish it since other members may be waiting to read it. If you do not have access to a computer, circle the book you would like to read and send this page to us at the address below. You may also call us at 410-437-1157 or toll free, in our area, at 1-866-437-2881.
MD/DC/DE CHAPTER, MGFA PO BOX 186
PASADENA, MD. 21123-0186

~ Holiday Humor & Thoughts~
*** Labor Day***
On a Septic Tank Truck sign: "We're #1 in the #2 business."
On a Plumber's truck:
"We repair what your husband fixed."
Pizza Shop Slogan: "7 days without pizza makes one weak."
At a Tire Shop in Milwaukee:
"Invite us to your next blowout."
On a Plastic Surgeon's Office door: "Hello. Can we pick your nose?"
At a Towing company:
"We don't charge an arm and a leg. We want tows."
On an Electrician's truck: "Let us remove your shorts."
In a Nonsmoking Area:
"If we see smoke, we will assume you are on fire and take appropriate action."
At an Optometrist's Office
"If you don't see what you're looking for, you've come to the right place."
On a Taxidermist's window: "We really know our stuff."
In a Podiatrist's office:
"Time wounds all heels."
On a Fence: "Salesmen welcome! Dog food is expensive."
At a Car Dealership:
"The best way to get back on your feet - miss a car payment."
Outside a Muffler Shop:
"No appointment necessary. We hear you coming."
In a Veterinarian's waiting room: "Be back in 5 minutes. Sit! Stay!"
At the Electric Company:
"We would be delighted if you send in your payment. However, if you don't, you will be."
In a Restaurant window:
"Don't stand there and be hungry, Come on in and get fed up."
In the front yard of a Funeral Home: "Drive carefully. We'll wait.."
************************** At a Propane Filling Station, "Tank heaven for little grills."
***Halloween Groaner*** A man was walking home alone one night when he heard a "BUMP....BUMP....BUMP..." behind him. Walking faster, he looked back, making out an image of an upright coffin banging its way down the middle of the street towards him...."BUMP...BUMP...BUMP..."
The man began to run toward his home, and the coffin bounced after him faster....faster...BUMPBUMPBUMP.
He ran up to his door, fumbled with his keys, opened the door, rushed in, and locked it behind him. The coffin crashed through his door, with the lid of the coffin clapping BUMP...BUMP...BUMP... on the heals of the terrified man. The man rushed upstairs to the bathroom and locked himself in, heart pounding.
With a CRASH, the coffin broke down the door, coming slowly toward him. The man while screaming, reached for something, anything....all he can find was a box of cough drops which he hurled at the coffin...and suddenly "the coffin stops." ***Thanksgiving……..Be Thankful***
Be thankful that you don't already have everything you desire. If you did, what would there be to look forward to?
Be thankful when you don't know something, for it gives you the opportunity to learn.
Be thankful for the difficult times. During those times you grow. Be thankful for your limitations, because they give you opportunities for improvement. Be thankful for each new challenge, because it will build your strength and character. Be thankful for your mistakes. They will teach you valuable lessons. Be thankful when you're tired and weary, because it means you've made a difference. It's easy to be thankful for the good things. A life of rich fulfillment comes to those who are also thankful for the setbacks. Gratitude can turn a negative into a positive.
Find a way to be thankful for your troubles, and they can become your blessings.
~ 15 ~
Business Signs and A Few Chuckles
RETURN SERVICE REQUESTED
MD/DC/DE CHAPTER, MGFA PO Box 186 Pasadena, Md. 21123-0186 PRSRTSTD
Nonprofit Org. U.S. Postage Paid Glen Burnie, MD PERMIT No. 498
I want to help realize our vision of a world without Myasthenia Gravis
Enclosed is my $____________________________________TAX DEDUCTIBLE donation
Payable to the MD/DC/DE Chapter, MGFA (address above) A receipt will be mailed to you.
NAME_________________________________________________________________________________________________________ ADDRESS _____________________________________________________________________________________________________ CITY, STATE, ZIP_______________________________________________________________ _______________________________________________________________________________
You may also donate
directly through your place of employment.
THANK YOU, YOUR SUPPORT IS APPRECIATED