Embed Size (px)
Citation preview

ISSN 2522-1310
EUROPEACTIVE
The House of Sport
Avenue des Arts 43 – 7ème étage
1040 Brussels, Belgium
Tel.: +3226499044 www.europeactive.eu
ISSUE 1 - 2017

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
1
Contents
FOREWORD by Rita Santos Rocha & Alfonso Jimenez ................................................ 4
European Journal for Exercise Professionals – SCOPE AND EDITORIAL BOARD .... 6
1 - EXPERT OPINION: The need for Research and Evaluation skills for Exercise
Professionals, a high-value challenge to be addressed [Alfonso Jimenez & Simona
Pajaujiene] ........................................................................................................................ 9
Introduction ................................................................................................................ 10
Physical activity vs inactivity ..................................................................................... 11
Current physical activity policy and challenges for the health and fitness sector ...... 12
Conclusions ................................................................................................................ 15
References .............................................................................................................. 16
2 - EXPERT OPINION: Exercise counselling by general practitioners. Exercise
prescription by exercise specialists [César Chaves Oliveira & Rui Garganta] .............. 18
Promoting Exercise .................................................................................................... 19
Are general practitioners promoting more exercise? .................................................. 20
Are we more active? ................................................................................................... 20
Barriers to exercise prescription by general practitioners .......................................... 21
Why “exercise is NOT medicine” .............................................................................. 24
Conclusion .................................................................................................................. 26
References .............................................................................................................. 27
3 - REVIEW PAPER: Fitness professionals’ pedagogical intervention [Susana Franco
& Vera Simões] .............................................................................................................. 29
Background ................................................................................................................. 30
Discussion ................................................................................................................... 30
Implications for practice ............................................................................................. 35
References .............................................................................................................. 36
4 - ORIGINAL RESEARCH: The transtheoretical model of behaviour change and
strategies for fitness professionals to increase exercise behaviour [Jan Middelkamp] .. 39

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
2
Introduction ................................................................................................................ 40
Transtheoretical Model of Behaviour Change........................................................ 40
Integrative Model ................................................................................................... 44
Practical applications .................................................................................................. 45
Conclusion .................................................................................................................. 47
References .............................................................................................................. 48
5 - ORIGINAL RESEARCH: Health Promotion in Commercial Fitness Gyms. An
analysis of organizational culture as an organization-specific premise for decision-
making. [Thomas Rieger & Michael Pfleger] ................................................................ 50
Introduction ................................................................................................................ 51
State of Research .................................................................................................... 52
Aspects of Organizational Theory .......................................................................... 53
The Organizational Culture as a part of the Social System .................................... 54
The Implementation of a Health Promotion Orientation ........................................ 58
Derivation of Research Questions .......................................................................... 59
Methodological approach ........................................................................................... 59
Qualitative Evaluation ............................................................................................ 60
Document Analysis ................................................................................................ 61
Results ........................................................................................................................ 61
Self-Conception of Commercial Fitness Gyms ...................................................... 61
Organizational Culture and Health Promotion ....................................................... 65
Conclusion .................................................................................................................. 68
References .............................................................................................................. 69
6 - ORIGINAL RESEARCH: How exercising women feel about their bodies and
behave in fitness club environment? [Simona Pajaujiene] ............................................. 71
Introduction ................................................................................................................ 72
Methods ...................................................................................................................... 74
Participants ............................................................................................................. 74
Instrument ............................................................................................................... 74
Results ........................................................................................................................ 74
Discussion ................................................................................................................... 79
Conclusions ................................................................................................................ 82
Practical applications .................................................................................................. 82

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
3
References .............................................................................................................. 83
7 - ORIGINAL RESEARCH: Step-Exercise as a mean of bone health improvement
[Rita Santos Rocha] ........................................................................................................ 84
Introduction ................................................................................................................ 85
Exercise and bone health ........................................................................................ 85
Exercise and ground reaction forces ....................................................................... 87
Step-Exercise and osteogenic potential .................................................................. 88
Purposes .................................................................................................................. 89
Methods ...................................................................................................................... 90
Results ........................................................................................................................ 91
Discussion ................................................................................................................... 94
Implications for practice ............................................................................................. 96
Conclusion .................................................................................................................. 97
References .............................................................................................................. 97
8 - PRACTICE UPDATE: How can we motivate the "unsocial" children in Fitness
classes? [Eljona Spaho] ................................................................................................ 100
Introduction .............................................................................................................. 101
How can we motivate the "unsocial" children/members in fitness classes? ............ 101
How can we motivate the children/student/member?............................................... 102
What should we do as teachers/instructors to motivate the children/members? ...... 105
How can we involve the parents? ............................................................................. 106
How can we adopt our teaching method? ................................................................. 107
Discussion ................................................................................................................. 110
Overall Conclusion ................................................................................................... 111
References ............................................................................................................ 111
European Journal for Exercise Professionals – INSTRUCTIONS FOR AUTHORS
AND SUBMISSION PROCESS .................................................................................. 112
OTHER PUBLICATIONS BY EUROPEACTIVE ..................................................... 115

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
4
FOREWORD by Rita Santos Rocha & Alfonso Jimenez
It is our pleasure to welcome you to the First Issue of the European Journal for
Exercise Professionals. This new publication by EuropeActive is focused on
providing up-to-date information to all exercise professionals, from research to
practice and from practice to research on all topics of interest for the fitness
industry, active leisure, health promotion, and sports fields.
Current literature supports the recommendation to initiate or continue an active
and healthy lifestyle in our perinatal lives and across the lifespan. There are plenty
of evidence-based studies that support the benefits of physical activity and exercise
on the promotion of health and well-being outcomes. Those include, as examples,
the reduction of several disease risks, prevention of hypertension, diabetes, or
musculoskeletal disorders, improvement of weight control, mental health, and
physical fitness, as well as the improvement of several disease treatments.
Moreover, epidemiologic studies prove the positive effect of physical fitness in
terms of a reduced risk of mortality, and improved quality of life.
Exercise professionals are key players in promoting the above benefits, and are the
main actors in planning and delivering exercise programmes, and in assuring
positive fitness outcomes.
Exercise professionals are required to develop and maintain a commitment to the
lifelong learning process in relation to their role, the professional context in which
they operate (including market evolution and development) and any technical and
scientific updates focusing on their particular field of expertise and experience. Our
aim, each year, is to gather relevant materials for exercise professionals, and their
multidisciplinary teams, that will support these requirements and bridge the gap
between science and practice.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
5
This first issue includes a selection of content, from “expert opinion”, “original
articles”, “review articles”, and ”practice updates” coming from authors across
Europe (Germany, The Netherlands, Denmark, Lithuania, United Kingdom, Spain,
and Portugal).
A wide range of content - research and higher education, marketing and
management, vocational education and practice based - will be included in future
editions, and as editors we aim to further involve exercise professionals, employers,
suppliers, students, and researchers in contributing to these editions.
We are pleased to recommend this first issue to all exercise professionals, and to
anyone else who is interested in the fitness industry, and in getting MORE
PEOPLE, MORE ACTIVE, MORE OFTEN.
Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
6
European Journal for Exercise Professionals – SCOPE AND
EDITORIAL BOARD
The European Journal for Exercise Professionals is an on-going peer-reviewed
online journal which publishes articles on important trends and developments in the
fitness industry and related fields.
Journal scope:
The European Journal for Exercise Professionals is an official publication of
EuropeActive, available free to all EREPS members. It aims to provide up-to-date
information to all exercise professionals, from research to practice and from
practice to research on all topics of interest for the active leisure and sports fields.
Topics include exercise prescription & assessment, personal training, group
exercise, outdoor exercise, sports, health & nutrition, lifestyle, injuries prevention,
professional development, special populations (special phases of life, clinical
conditions and disabled people), fitness trends, exercise and health costs, worksite
health & exercise promotion, physiology and biomechanics of exercise, pedagogy
and psychology of sports and exercise, club management, sport law, among others.
Its mission is to promote and distribute accurate, unbiased, and authoritative
information on health and fitness.
The European Journal for Exercise Professionals includes components of
research and higher education, marketing and management, vocational education
and practice based on EuropeActive’s Fitness Standards and European
Qualifications Framework, as well as continuing education opportunities.
Target audience:
Mainly practitioner-focused, the European Journal for Exercise Professionals
will be written for exercise specialists, personal trainers, exercise
Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
7
leaders/instructors, academics and researchers working in the Health & Fitness
field, in-training professionals, graduate students in the field of Health & Fitness,
programme managers, club managers, rehabilitation specialists, exercise-test
technologists, and other professionals related to the Health & Fitness industry.
Publisher:
EuropeActive
House of Sport, Avenue des Arts 43 - 7 ème étage
1040 Bruxelles, Belgium
ISSN 2522-1310
Key title: European journal for exercise professionals
Abbreviated key title: Eur. j. exerc. prof.
URL: http://www.ereps.eu/ejep/ejep
Editors-in-Chief:
Prof. Rita Santos-Rocha, PhD, ESDRM-IPSantarém / EuropeActive (Portugal)
Prof. Alfonso Jimenez, Coventry University (United Kingdom / Spain)
Editorial Board:
Dr. Simona Pajaujiene, PhD, Lithuanian Sports University / Active Training /
EuropeActive (Lithuania)
Dr. Alexis Batrakoulis, MSc, GRAFTS / EuropeActive (Greece)
Dr. László Zopcsak, PhD, International Wellness Institute (Hungary)
Dr. Lou Atkinson, PhD, Aston University (United Kingdom)
Dr. Cedric X. Bryant, PhD, FACSM, American Council on Exercise (United
States)
Prof. Gary Liguori, PhD, University of Rhode Island (United States)
Prof. Thomas Rieger, BiTS University (Germany)
Dr. Jan Middlekamp, HDD Group / BlackBoxFitness (The Netherlands)
Dr. Julian Berriman, MA, Professional Standards Committee, EuropeActive
(United Kingdom)

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
8
External Reviewers:
Dr. Silvano Zanuso, PhD, University of Padova / Technogym Research
Department (Italy)
Dr. Anna Szumilewicz, PhD, Gdansk Sports University (Poland)
Prof. Susana Franco, PhD, ESDRM-IPSantarém (Portugal)
Dr. Antonino Bianco, PhD, University of Palermo (Italy)
Dr. Fernando Naclerio, University of Greenwich (United Kingdom)
Prof. João Brito, ESDRM-IPSantarém (Portugal)
Dr. Adrian Casas, University of La Plata (Argentina)
Dr. Steven Mann, ukactive Research Institute (United Kingdom)

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
9
1 - EXPERT OPINION: The need for Research and Evaluation
skills for Exercise Professionals, a high-value challenge to be
addressed [Alfonso Jimenez & Simona Pajaujiene]
Alfonso Jimenez1 , Simona Pajaujiene2
1Centre for Applied Biological & Exercise Sciences, Coventry University, UK.
E-mail: [email protected]
2Lithuanian Sports University, Lithuania. ActiveTraining – Training provider,
Lithuania. EuropeActive – Professional Standards Committee.
E-mail: [email protected]
1 Alfonso Jimenez, 1970, Madrid, Spain. A truly international scholar, fully involved in the health and fitness industry
since the late 80s, Alfonso has worked as fitness and group exercise instructor, personal trainer, programme director, club manager and senior executive before moving into academia. Former Chairman of the Standards Council at EuropeActive and Honorary Member, he is Professor of Exercise Science & Health and Executive Director of the Centre for Applied Biological and Exercise Sciences at Coventry University; Chair of the Research & Dissemination Commission at the Healthy & Active Living Foundation in Spain. Co-Director of the Healthy & Active Living National Observatory at Universidad Rey Juan Carlos de Madrid (Spain); Scientific Advisory Board member at ukactive Research Institute; Formal member of the “Active Leisure Alliance Task Group” as expert from Academia; and Visiting Professor at ISEAL, Victoria University (Melbourne, Australia), the University of Greenwich (London, UK) and EUSES, University of Girona (Spain). Research interests: active living, exercise prescription, clinical exercise and worksite health promotion. Qualifications: BSc in Sport & Exercise Sciences (1993); PhD in Exercise Physiology (2003), postdoctoral training in Physical Activity & Health Promotion (2007), CSCS, NSCA-CPT. More info: CoventryU ResearchGate LinkedIn 2 Simona Pajaujien, 1970, Kaunas, Lithuania. She has been involved in fitness training, exercise for health and fitness
education for over 25 years and currently works as trainer, group fitness instructor, educator, speaker, author and technical expert. She is a lecturer and coordinator for several study programmes at the Lithuanian Sports University since 2004. Research interest: Health Education; Body Image in Sport and Leisure Physical Activity; Weight Control and Exercising Behaviour. She is a program director and founder of accredited vocational training school - ActiveTraining. Member of Professional Standards Committee – EuropeActive. Qualifications: BSc in Sport Sciences (1995); MSc in Public Health – Health and Fitness (2004); PhD in Social Science – Sports Science and Education (2012). More info: ResearchGate LinkedIn

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
10
“High-quality research and robust evidence are the cornerstones of effective policy, and while we know
that physical activity is one of the most powerful medicines available to society, and we’ve proven that
adding just small amounts of activity improves the health and wellbeing of almost everyone – all the
resources and time spent investigating activity amounts to very little unless we know how to support
more people, to be more active, more often. We have to support the academic community and
physical activity providers to put research at the heart of practice.” (Prof. Greg Whyte, ukactive
Blueprint for an Active Britain, 2015) [1]
Abstract: Despite the known benefits of physical activity, there is a worldwide trend towards less
total daily physical activity, and as a consequence, physical inactivity has become a leading risk factor
for chronic health disorders. The health and fitness sector is expanding very fast, although its overall
impact is only addressing the needs of about 11% of the European population. Exercise professionals
should play a more proactive role model supporting thousands of inactive potential clients. Providing
solid evidence-based information about the benefits of active living could act as a valuable driver for
positive behavioral change. The education and professional development of exercise professionals are
missing a solid training in basic research and evaluation skills. These new skills, integrated into the
formal training and practice of exercise professionals, will allow the whole Physical Activity sector, and
specially the health and fitness industry, to develop new knowledge, transform current professional
practice, inform public policy and expand the innovation capacity of our field.
Key-words: health and fitness sector, physical activity, research, evidence-based, competency,
exercise professionals
Introduction
A sedentary lifestyle is a risk factor for the development of many chronic illnesses,
and a main cause of premature death. Furthermore, living an active life brings
other social and psychological benefits. At the same time, poor nutrition makes an
important contribution to the burden of disease. A diet high in saturated fat and
energy-dense foods, and low in fruit and vegetables – along with a sedentary
lifestyle and smoking – is the major cause of cardiovascular diseases (CVD), cancer
and obesity.
There is significant evidence to show that physical inactivity and over-nutrition are
associated with a substantial economic burden in industrialized countries.
Implementation of specific strategies to modify inactive behavior is critical, but
could be associated with considerable costs if they are not properly evidenced and

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
11
structured. To address large and meaningful public health benefits in improving the
health of adults, the cost-effectiveness of those intervention strategies will be of
major importance in addition to their health/clinical effectiveness. The current level
of evidence is not sufficient [2], and few studies published relate to the
potential positive impact that the health and fitness industry could bring.
From the UN High-level Meeting on NCDs Prevention and Control Political
Declaration (NYC, Sep’11) [3], to the top evidences published at Lancet Series on
Physical Activity (2012, 2016) [4,5], there is a clear message that Physical
Activity and Exercise can play a major role in the Public Health agenda, and
significant funding and resources are being put in place to identify cost-effective
active living models of implementation and delivery.
Physical activity vs inactivity
Physical activity is one of the most basic human functions. It is an important
foundation of health throughout life. Its known health benefits include a reduced
risk of cardiovascular disease, hypertension, diabetes and certain forms of cancer;
it also has an important role in the management of certain chronic conditions. In
addition, it has positive effects on mental health by reducing stress reactions,
anxiety and depression and by possibly delaying the effects of Alzheimer’s disease
and other forms of dementia. Furthermore, physical activity is a key determinant of
energy expenditure and is therefore fundamental to achieving energy balance and
weight control. Throughout childhood and adolescence, physical activity is
necessary for the development of basic motor skills, as well as musculoskeletal
development. Furthermore, physical activity is also embedded in the United Nations
Convention on the Rights of the Child. In adults, physical activity maintains muscle
strength and increases cardiorespiratory fitness and bone health. Among older
people, physical activity helps to maintain health, agility and functional
independence and to enhance social participation and quality of life. It may also
help to prevent falls and assists in chronic disease rehabilitation, becoming a critical
component of a healthy life.
Despite the known benefits of physical activity, there is a worldwide trend towards

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
12
less total daily physical activity. Globally, one-third of adults do not achieve the
recommended levels of physical activity. In Europe, estimates indicate that more
than one-third of adults are insufficiently active [6]. While there are some
continuing challenges in terms of the validity and comparability of data on levels of
physical activity across Europe, recent figures from member States of the European
Union (EU) indicate that six in every 10 people above 15 years of age never or
seldom exercise or play a sport and more than half never or seldom engage in
other kinds of physical activity, such as cycling, dancing or gardening. At the same
time, a high proportion of adults in Europe spends more than four hours a day
sitting, which could be a contributing factor to sedentary lifestyles.
As a consequence, physical inactivity has become a leading risk factor for chronic
health disorders: 1 million deaths (about 10% of the total) and 8.3 million
disability-adjusted life years lost per year in the WHO European Region are
attributable to physical inactivity. It is estimated to cause 5% of the burden of
coronary heart disease, 7% of type 2 diabetes, 9% of breast cancer and 10% of
colon cancer [7]. Rising rates of overweight and obesity have also been reported in
many countries in the Region during the past few decades. The statistics are
disturbing: in 46 countries (accounting for 87% of the Region), more than 50% of
adults are overweight or obese; in several of those countries the rate is close to
70% of the adult population. Overweight and obesity are also highly prevalent
among children and adolescents, particularly in Southern European countries.
Physical inactivity has been identified as contributing to the energy imbalance that
leads to weight gain. Collectively, physical inactivity has not only substantial
consequences for direct health-care costs but also causes high indirect costs due to
increased periods of sick leave, work disabilities and premature deaths. For a
population of 10 million people, where half the population is insufficiently active,
the overall cost is estimated to be €910 million per year [8].
Current physical activity policy and challenges for the health and
fitness sector
The recently launched Physical Activity Strategy for the WHO European

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
13
Region 2016–2025 [9] is building on the commitments of Health 2020 – the
WHO European policy framework for health and well-being – and aligns with
existing WHO frameworks and strategies, such as the Global action plan for the
prevention and control of non-communicable diseases 2013–2020, the Action Plan
for implementation of the European Strategy for the Prevention and Control of Non-
communicable Diseases 2012–2016, the Global Strategy on Diet, Physical Activity
and Health and the WHO Global Recommendations on Physical Activity for Health.
The leadership for promoting health-enhancing physical activity is set out for the
national ministries of health with a formal encouragement to establish coordination
mechanisms between the areas of health, sports, education, transport, urban
planning, environment and social affairs sectors.
The EU-WHO Strategy identifies five priority areas, with Evaluation and Research
as the fifth one (1 – Providing leadership and coordination for the promotion of
physical activity; 2 – Supporting the development of children and adolescents; 3 –
Promoting physical activity for all adults as part of daily life, including during
transport, leisure time, at the workplace and through the health-care system; 4 –
Promoting physical activity among older people; 5 – Supporting action through
monitoring, surveillance, the provision of tools, enabling platforms, evaluation and
research) [9]. With the main goal of supporting the strategy and related actions
(through monitoring, surveillance, and provision of tools, enabling platforms,
evaluation and research), the priority considers that strengthen the evidence
base for physical activity promotion is a key issue to address.
The European health and fitness sector is rapidly developing. It currently serves
over 50 million consumers, generates 26.8 billion Euro in revenues, employs
400,000 people, and consists of 48,000 facilities [10]. The collaboration between
healthcare systems and the health and fitness sector is very important, yet the
interaction between both in Europe is not always sufficient [11, 12].
Getting and staying fit is the result of the integration of both physical activity and
exercise in your lifestyle and the application of solid evidence-based interventions

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
14
will guarantee effective positive results achieved safely and progressively. Science
and applied research are progressing faster than ever, and we, exercise
professionals, should be able to build the bridge between theory and
practice. Exercise professionals should be upskilled based on the current
evidences allowing the public to achieve their exercise goals easier, faster and
safer.
The health and fitness industry, and very specially EuropeActive, have been
actively involved (since 2007) in projects and activities in partnership with
Governments across Europe to promote an active and healthy behaviour, and
significant funding support has been received from the European Commission in
that regard [13]. In fact, the health and fitness sector, represented by
EuropeActive, recognizes its responsibility to work with partners at all levels across
the European Union to create a healthier society, where living an active lifestyle is
the social norm, rather than an exception, and where daily physical activity and
exercise is seen as part of the routine part of the prevention and management of
disease. Its mission is to get more people | more active | more often [14]. But
despite the obvious capacity of the fitness sector across Europe, its willingness to
contribute to increased levels of physical activity, and its track record of positive
performance, the sector is rarely recognized in national governments’
physical activity promotion programmes and campaigns.
The underlying reasons for the interaction between the healthcare system and
health and fitness industry in Europe are not always sufficient identified [11, 12].
And what we consider are the reasons for this? Firstly, exercise professionals have
not historically been considered as an extension of the health care team [12].
Unfortunately, representatives of healthcare systems tend to view the health and
fitness sector to be founded on principles that differ from medical system and
lacking the “credibility” and “authenticity” to partner on NCDs prevention [14]. The
main problem is that the health and fitness sector in some cases is seen as a
private multibillion industry, feeding modern consumerism and making business by
manipulating clients’ concerns similarly as hamburger restaurant chains [15].
Secondly, the healthcare system is not prepared to apply exercise prescription as a

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
15
first-line therapy because of the lack of the specific HEPA related education in the
training of general practitioners [16].
Exercise professionals are the main source to convey exercise-related information
for the general public. They provide information and implement exercise
counselling, exercise prescription, client’s fitness assessment and guidance.
Unfortunately, there is a lack of review studies on the analysis of their education
and professional competencies [17], it is unclear how they obtain evidence–based
information and other issues associated with their education and lifelong learning
[17, 18]. However, it is revealed that exercise professionals with higher level of
education (e.g., graduate degrees) are more likely to use scholarly sources of
evidence compared to those with lower levels of education who are more likely to
rely on mass media, including the internet [19, 20]. Therefore, given exercise
professional's role in advising the general public, their accessibility, and the
emerging evidence-based guidelines on the best practices related to the use of
exercise and nutrition interventions, further research is needed to ensure that
exercise professionals, working with the public, integrate new research knowledge
into their fitness assessment and exercise guidance [17]. One critical element in
this regard is the fact that the Health and Fitness Industry is not investing
resources to provide solid evidences supporting its capacity to deliver
meaningful and sustainable public health outcomes.
Conclusions
As health and fitness sector expands very fast, exercise professionals should play a
proactive role model for thousands of clients. The education and professional
development of exercise professionals are missing a solid training in basic
research and evaluation skills (from critical analysis to data collection, pre- and
post- intervention assessments, data analysis and reporting).
These new skills integrated into the formal training and practice of exercise
professionals will allow the whole Physical Activity sector, and specially the health
and fitness industry, to develop new knowledge, transform current professional
practice, inform public policy and expand the innovation capacity of our field.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
16
Public health commissioners should not only insist on evidence-based practice, but
should insist that ongoing data capture is a feature of all commissioned
interventions. Accordingly, we (practitioners, operators and training providers)
must become adept at embedding data capture and analysis into all relevant
activity. Representative bodies must lobby government, health agencies and
research councils to provide greater funding for effectiveness research [21].
The value of Research and Evaluation for the health and fitness industry will be
immense on delivering solutions and innovative ways of tackling inactivity at
population level, and its broad implementation will become a long lasting legacy for
a different, positive and more active future.
Due to the aforementioned challenges in public health, the healthcare and the
health and fitness sector should review and reformulate their current strategies.
This will be critically important in the light of the implementation of the EU-WHO
Physical Activity Strategy for the European Region 2016-2025. Moreover, it will be
relevant for the recognition of the value of the health and fitness sector as an
effective partner on the public health agenda worldwide.
References
1. ukactive (2015). ukactive’s Blueprint for an Active Britain, Research and Evaluation, 30-34. http://www.ukactive.com/downloads/managed/ukactives_Blueprint_for_an_Active_Britain_-_online.pdf
2. Muller-Riemenschneider, F., Reinhold, T., Willich, S. N. (2009). Cost-effectiveness of interventions promoting physical activity. British Journal of Sports Medicine, 43, 70–76.
3. http://www.ncdalliance.org/sites/default/files/rfiles/Key%20Points%20of%20Political%20Declaration.pdf
4. The Lancet Series on Physical Activity (2012). Physical Activity 2012. http://www.thelancet.com/series/physical-activity
5. The Lancet Series on Physical Activity (2016). Physical Activity 2016: Progress and Challenges. http://www.thelancet.com/series/physical-activity-2016
6. Hallal, P.C., Andersen, L.B., Bull, F.C., Guthold, R., Haskell, W., Ekelund, U. (2012). Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet, 380(9838), 247–257.
7. Lee, I.M., Shiroma, E.J., Lobelo, F., Puska, P., Blair, S.N., Katzmarzyk, P.T. (2012). Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet, 380(9838), 219–229.
8. Word Health Organization (2007). Steps to health: a European framework to promote physical activity for health. Copenhagen: WHO Regional Office for Europe. http://www.euro.who.int/__data/assets/pdf_file/0020/101684/E90191.pdf
9. World Health Organization (2015). Physical activity strategy for the WHO European Region 2016–2025. Copenhagen: WHO Regional Office for Europe. http://www.euro.who.int/__data/assets/pdf_file/0010/282961/65wd09e_PhysicalActivityStrategy_150474.pdf?ua=1

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
17
10. Deloitte & EuropeActive (2016). European Health & Fitness Market Report 2016. Cologne, Germany. Available: http://www.europeactive.eu/blog/europeactive-and-deloitte-publish-european-health-fitness-market-report-2016
11. Sagner, M., Katz, D., Egger, G., Lianov, L., Schulz, K.H., Braman, M., et al. (2014). Lifestyle medicine potential for reversing a world of chronic disease epidemic: from cell to community. Int J Clin Pract, 68(11), 1289-92.
12. Muth, N.D., Vargo, K., Bryant, C.X. (2015). The role of the fitness professional in the clinical setting. Curr Sports Med Rep, 14(4), 301-12.
13. EHFA (2011). Becoming the Hub. The Health and Fitness Sector and the Future of Health Enhancing Physical Activity. Final Report, http://www.ehfa-programmes.eu/sites/ehfa-programmes.eu/files/documents/hub/HUB_THE%20FINAL%20REPORT.pdf
14. Matheson, G.O., Klügl, M., Engebretsen, L., Bendiksen, F., Blair, S.N., Börjesson, M., et al. (2013). Prevention and management of non-communicable disease: the IOC consensus statement, Lausanne. British Journal of Sports Medicine, 47(16), 1003-11.
15. Andreasson, J., Johansson, T. (2014). ‘Doing for group exercise what McDonald's did for hamburgers’: Les Mills, and the fitness professional as global traveler. Sport Educ Soc, 21(2), 148-65.
16. Joy, E., Blair, S.N., McBride, P., Sallis, R. (2013). Physical activity counselling in sports medicine: a call to action. British Journal of Sports Medicine, 47(1), 49-53.
17. Stacey, D., Hopkins, M., Adamo, K.B., Shorr, R., Prud’home, D. (2010). Knowledge translation to fitness trainers: A systematic review. Implementation Science, 5:28.
18. Waryasz, G.R., Daniels, A.H., Gil, J.A., Siric, V., Eberson, C.P. (2016). Personal trainer demographics, current practice trends and common trainee injuries. Orthopedic Reviews, 8:6600.
19. Hare, S.W., Price, J.H., Flynn, M.G., King, K.A. (2000). Attitudes and perceptions of fitness professionals regarding obesity. J Community Health, 25, 5-21.
20. Forsyth, G., Handcock, P., Rose, E., Jenkins, C. (2005). Fitness instructors: How does their knowledge on weight loss measure up? Health Education Journal, 64(2), 154-167.
21. Beedie, C., Mann, S., Jimenez, A., et al. (2016). Death by effectiveness: exercise as medicine caught in the efficacy trap! British Journal of Sports Medicine, 50(6), 323-4.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
18
2 - EXPERT OPINION: Exercise counselling by general
practitioners. Exercise prescription by exercise specialists
[César Chaves Oliveira & Rui Garganta]
César Chaves Oliveira3, Rui Garganta4
3Instituto Politécnico de Viana do Castelo, Escola Superior de Desporto e Lazer,
Portugal.
E-mail: [email protected]
4Faculdade de Desporto, Universidade do Porto, Portugal.
E-mail: [email protected]
Abstract: In 2007, the American College of Sports Medicine (ACSM), with endorsement from the
American Medical Association and the Office of the Surgeon General, launched a global initiative termed
“Exercise is Medicine”, to mobilize physicians, healthcare professionals and providers, and educators to
promote exercise in their practice or activities to prevent, reduce, manage, or treat diseases that impact
health and the quality of life in humans. Since then, physicians are increasingly advising their patients to
exercise, although the number of them that comply with this practice is still generally low. Far more
important, data shows that people are less active than before. Here we discuss the main barriers
physicians face to exercise promotion and highlight the main features of successful interventions, with
an emphasis on the role of exercise specialists. Finally, we argue that exercise prescription should only
be performed by exercise specialists, as only they possess the required deep knowledge of the exercise
techniques, methods, and types most suited for each individual and only they have the time and
commitment to support, supervise and motivate patients before, during and after any kind of physical
activity or exercise programme that is implemented.
Key-words: exercise prescription, personal trainer, medicine, exercise is medicine.
3 César Chaves Oliveira has a PhD in Physical Activity and Health and is currently an assistant teacher at Sports and
Leisure School, of Polytechnic Institute of Viana do Castelo, Portugal. He has worked in the exercise training and fitness
industries for almost 2 decades, addressing both special and healthy populations. He is a scientific writer, consultant
and lecturer in exercise, health and nutrition subjects. 4 Rui Garganta has a PhD in Sports Sciences and is currently a full professor at Oporto Sports Faculty, University of
Porto, Portugal. He has worked in the exercise training and fitness industries for almost 3 decades, addressing both
special and healthy populations. He is a scientific writer, consultant and lecturer in exercise, health and nutrition
subjects.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
19
Promoting Exercise
The protective effects of physical activity and exercise on various chronic diseases
are overwhelmingly well studied and supported in the literature and are comparable
to drug interventions on mortality outcomes [1, 2]. Whether through physical
activity or by exhibiting a higher fitness level or reducing the amount of time one
spends sitting, non-sedentary people can significantly reduce their mortality risks
[3]. Nevertheless, a recent European Report found that the amount of people that
never exercises or play sports raised from the previously 39% in 2009 to 42% four
years later [4]. In the United States, only 21% of the total population met the full
guidelines for both aerobic and muscle-strengthening activity and critically only 3%
met the muscle-strengthening activity guidelines [5]. Furthermore, it may be that
for several health diseases, the recommended minimum amount of physical activity
does not convey special protection. In particular, it was found that individuals with
a total activity level of 600 metabolic equivalents (MET [6]) minutes/week (the
minimum recommended level, corresponding to 150 minutes/week at a moderate
intensity or 75 minutes/week at a vigorous intensity) had only a 2% lower risk of
diabetes compared with those reporting no physical activity. However, an increase
from 600 to 3600 MET minutes/week reduced the risk by an additional 19%. This
means that for significant reductions in the risk of some conditions (this study
addressed breast cancer, colon cancer, diabetes, ischemic heart disease, and
ischemic stroke events), people may actually need to perform several times the
recommended minimum of physical activity [7]. Hence, getting people to be more
active seems to be a vital public health matter. The role and relevance of medical
professionals are evident and pivotal, as they can reach almost all of the total
population of a country and within a relatively short period of time [8]. As such, in
2007, the American College of Sports Medicine (ACSM), with endorsement from the
American Medical Association and the Office of the Surgeon General, launched a
global initiative (termed “Exercise is Medicine - EIM”) to mobilize physicians,
healthcare professionals and providers, and educators to promote exercise in their
practice or activities to prevent, reduce, manage, or treat diseases that impact
health and the quality of life in humans [9, 10]. According to the programme, the
EIM initiative is achieved by: 1 - Assessing physical activity levels of each patient at

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
20
every clinic visit; 2 - Providing patients with an exercise “prescription” that can be
tailored to their specific disease conditions; and 3 - Referring patients to a trusted
network of local evidence-based physical activity programs led by qualified
professionals [11]. In summary, the EIM clinically links all the community in order
to develop and support a physically active lifestyle of all patients involved in this
initiative. So is EIM initiative being successful?
Are general practitioners promoting more exercise?
The first thing one must consider is if general practitioners are actually prescribing
more physical activity to their patients nowadays. By analysing data from the
National Center for Health Statistics, of the Centers for Disease Control and
Prevention, we can observe that in 2010, about one in three adults who had seen a
physician or other health professional in the past year had been advised to begin or
continue to do exercise or physical activity. From the same database we also find
that the percentage of adults who have been advised to exercise increased from
22.6% in 2000 to 32.4% in 2010 [12]. In the UK, it was found that 46% of patients
have reported receiving advice about physical activity and exercise from their
general practitioner [13]. This data seems to confirm that physicians are
increasingly advising their patients to exercise. Nevertheless, these numbers are
still far from optimal and are generally considered to be low [13].
Are we more active?
Although physicians are increasingly recommending physical activity and exercise
for their patients, data from the total population evidences that people are not
getting more active. In fact, trends from 2010 to 2015 reveal that the inactivity
rate changed from 26.8% in 2010 to 27.7% in 2015, which translates to a total of
81,6 million inactive Americans in the past year [14]. In Europe the trend for
physical inactivity is similar, as previously pointed [4]. Not surprisingly, studies
confirm that the effectiveness of physical activity counselling in improving patient’s
physical activity levels is mixed [15]. Simply advising people to take more exercise
seems to be an ineffective means to get them more active, but even adopting a
more personalized approach may not render the intended effects. To highlight this,
we recall the results of a study that compared the effects of direct advice or brief

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
21
negotiation groups to a control group and found no differences in weekly energy
expenditure among them, after the intervention [16]. In fact, exercise advice has
shown multiple times its efficacy (results in a controlled environment) but not its
effectiveness [17].
Barriers to exercise prescription by general practitioners
Physicians meet various barriers to physical activity promotion and these barriers
are at least partially responsible for the mixed results on the physical activity
advice effectiveness. These include the perception that their patients are
uninterested in increasing their physical activity levels and are unlikely to change
their behaviour [18], and the fact that when they do devote time to counselling,
they do not usually receive positive feedback from patients becoming more
physically active [19]. This is not without reasoning, especially when we look at the
best case scenario adopted in a study conducted in Spain [20], where fifty-six
Spanish family physicians were randomized to either the intervention or standard
care arm of the trial. The physicians recruited 4.317 physically inactive patients
(2.248 for intervention and 2.069 for control protocols) from a systematic sample
after assessing their physical activity in routine practice. Intervention physicians
provided advice to all patients and a physical activity prescription to the subgroup
attending an additional appointment (30%). The main outcome measure was the
change in physical activity measured by blinded nurses using the 7-Day Physical
Activity Recall [21]. Secondary outcomes included cardiorespiratory fitness and
health-related quality of life. The results are surprising. At 6 months, intervention
patients increased physical activity more than controls (18 min/wk) but the
proportion of the population achieving minimal physical activity recommendations
was only 3.9% higher in the intervention group. Moreover, no differences were
found in secondary outcomes, despite all patients from the intervention group being
advised to exercise and 30% of them being given a physical activity prescription
[20]. Nevertheless, there are other barriers to exercise promotion, like physician’s
own physical activity habits, as less active physicians are less likely to engage in
such practices with their patients [22]. However, we consider the following two, to
be some of the most important barriers to exercise promotion: the first one is the
physician’s lack of knowledge of physical activity and exercise: more than one-half

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
22
of the physicians trained in the US in 2013 received no formal education in physical
activity and most courses focused on exercise physiology and used a clinical
approach, rendering physicians ill-prepared to assist their patients in a manner
consistent with several national programmes, like Healthy People 2020, the
National Physical Activity Plan, or the EIM initiative [23]. In a study conducted on
UK medical students, on their final year, it was found that: physical inactivity was
incorrectly perceived to be the least important risk factor for global mortality; that
only 36% of students reported they were aware of the current UK physical activity
guidelines, while (by comparison) 94% knew UK alcohol guidelines; and that only
9% were able to adequately define ‘moderate/vigorous exercise intensity’, key
aspects of the UK Chief Medical Office physical activity guidelines (a number of
responses could be considered dangerous to patient’s health) [24]. Despite these
findings, 52% of the students stated they felt adequately trained to give physical
activity advice to the general public. The other notable barrier to physical activity
promotion is physicians’ lack of time [18]: a study designed to compare
determinants of consultation length in six European countries (Belgium,
Switzerland, Germany, Spain, Netherlands, United Kingdom), found that the
average length of a consultation in general practice was just under 11 minutes,
ranging from 7.6 minutes in Germany to 15.6 in Switzerland (20). Since even ‘brief
counselling’ in successful physical activity promotion interventions requires at least
3 to 5 minutes [25], we argue if physicians should devote almost 50% of their
consultation time to accurately evaluate their patient’s fitness levels and to
prescribe exercise according to his condition/illness, while concomitantly neglecting
medical related issues.
Fortunately, physicians do not need to perform extensive counselling to be able to
assist their patients with increasing their physical activity, as they could use their
limited time and resources by referring them to external sources for more
comprehensive community-based support. Exercise referral schemes consist of an
assessment involving a primary care or allied health professional to determine that
someone is inactive, a referral to a physical activity specialist or service, an
assessment to determine what programme of physical activity to recommend and
participation in that programme [26]. These type of schemes show promise in

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
23
conveying better health outcomes than a far simpler exercise advice procedure [26,
27]. Along with exercise adherence, which is defined as successful if participants
complete a prescribed exercise routine for at least two-thirds of the time [28],
exercise maintenance is a key feature for a lifelong healthy physical activity status.
One of the most cited barriers to exercise maintenance after study completion was
the lack of professional support beyond the end of the programme, as found in a
review of 33 UK-relevant studies [26]. Participants who dropped out of exercise
post-completion of referral cited the removal of the exercise professional as the
primary motivating factor [29]. In a recent study, the researchers explored the
experiences of weight management clients in their meetings with registered
dietitians, personal trainers, and health behaviour counsellors in order to explain
how these services are perceived and received by participants. It was found that
the personal trainers received the highest percentage of positive codes (92.1%)
and that the participants tended to highlight the interpersonal experiences and
knowledge acquired and the specific exercise techniques or personalized programs
that were available [30]. Research also suggests that one-on-one personal training
is an effective method for changing attitudes and thereby increasing the amount of
physical activity. In one study, it was found that weekly sessions with a personal
trainer significantly increased clients’ ability to move upward through the stages of
change in regard to physical activity. Overall, 60 percent of study participants
moved up one stage, while 13 percent moved up two stages, demonstrating
evidence of health-behaviour change over a 10-week period [31]. Others
demonstrated more favourable outcomes on cognitive processes of change,
decisional balance, and scheduling self-efficacy of female college students receiving
personal trainer services [32] or higher values for the perception of autonomy
support, relatedness and competence in the same context of personal training [33].
This kind of supervision does not necessarily need to take place at a traditional gym
facility. In fact, researchers at Adelphi University compared in-home and at-the-
gym personal training and found that both were effective in terms of weight loss,
cardiovascular function, adherence and motivation, with little differences between
the two [34]. Although not rich, some research points to less loss to follow-up and
more adherence to exercise with a personal trainer versus unsupervised exercise or
a group exercise modality as BodyPump™ (loss to follow-up and number of

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
24
sessions completed were 17% and 32.2 with a personal trainer, 40% and 26.9 with
unsupervised training and 32% and 21.1 with BodyPump™) [35]. Once being
supervised, patients are expected not only to exhibit lesser drop-out rates but also
a significant improvement on specific and relevant health indicators. It has been
shown that members whose training was directed by well-qualified personal
trainers administering evidence-based training regimens achieved significantly
greater improvements in lean body mass and other dimensions of fitness than
members who direct their own training [36]. Other studies achieved similar results
[37, 38]. This highlights not only the importance of interdisciplinary approaches to
achieving a favourable outcome, but also the specific and unique contribution of
exercise specialists and specifically personal trainers to the promotion and
maintenance of an active lifestyle.
Why “exercise is NOT medicine”
Many people are advocates of the EIM philosophy. We can easily understand why
this happens, as exercise undoubtedly has the ability to boost the health of the
populations.
But “exercise” and “medicine” are actually two very distinct concepts that should
never be confused: we define “medicine” as “the science or practice of the
diagnosis, treatment, and prevention of disease” [39], while the definition of
“exercise” is much more comprehensive and reflects its reach - that is obviously not
constrained to health promotion or management - “something performed or
practiced in order to develop, improve, or display a specific capability or skill”;
“Activity requiring physical effort, carried out to sustain or improve health and
fitness” [39]. As Andy Smith brilliantly puts it, “Exercise is Recreation not Medicine”
[40]. In his article, he further highlights the realms of “exercise is recreation” by
stating its features: (1) a focus on the experience of the user, (2) the promotion of
well-being, (3) the importance of community, (4) embracing inclusivity, (5) sport,
(6) aesthetics, and (7) leisure time [40]. As we can easily find, most of these
characteristics are unique to “exercise” and not to “medicine”. Even if we compare
both terms from a medical point of view, we can see many differences between

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
25
them (table 1).
Table 1 - Comparison of Medicine vs Exercise
MEDICINE EXERCISE
When to use In the need to prevent, manage or treat a diagnosed disease
To improve health, to have fun, to master a skill, to improve body composition, and many others
Target Someone's disease The person
Contraindications Several: See Drug Label Not applicable
How to use According to drug label Endless possibilities
Dosage According to drug label Endless possibilities
Duration of treatment According to drug label Not applicable
Action in case of overdose According to drug label Rest
Interaction with other drugs/forms of exercise
From non-significant to life-threatening
From non-significant to beneficial
If we further indulge ourselves in this kind of comparisons, we can continue to find
significant differences between two of the most well-known forms of administration
of medicine and exercise (table 2).
Nevertheless, there are two major similarities between “medicine” and “exercise”:
1) a bad prescription can strongly affect the beneficial outcomes expected from
both sciences and 2) the best practice is made by those who are trained and have
studied and worked in the related area of expertise.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
26
Table 2 - Comparison of Aspirin vs Walking/running
ASPIRIN [41] WALKING/RUNNING
Minimum dose to promote an effect
50 mg Variable: depends on subject characteristics5
Contraindications Allergy; Reye’s Syndrome None6
Warnings Alcohol, Coagulation Abnormalities, GI side effects, Peptic Ulcer Disease
None
Precautions Renal Failure, Hepatic Insufficiency, Sodium Restricted Diets
None, except those regarding injury prevention and outdoor conditions (e.g. traffic conditions)
Drug/exercise interaction
ACE inhibitors, Acetazolamide, Anticoagulant Therapy, Anticonvulsants, Beta Blockers, Diuretics, Methotrexate, Non-steroidal Anti-inflammatory Drugs, Oral Hypoglycemics, Uricosuric Agents
Interaction with other forms of exercise is generally favourable
Adverse reaction
Dysrhythmias, dyspepsia, coagulopathy, acute anaphylaxis, rhabdomyolysis, pulmonary edema, and many others
Rare, occasional delay onset muscle soreness
Conclusion
In conclusion, we believe that the EIM mantra is reductionist to exercise as exercise
is much more than medicine [42-44]. Exercise presents both treatment AND
preventative benefits, but also many other unique facets that medicine can never
aspire to convey. One in particular is critical for a successful exercise promotion
intervention: enjoyment.
Instead of exercise being prescribed like a drug [45], we feel that the medical staff
should only refer their patient’s to community-based exercise facilities and/or to
exercise professionals as only they possess the required deep knowledge on the
exercise techniques, methods, and types most suited for each individual and only
they have the time and commitment to support, supervise and motivate patients
before, during and after any kind of physical activity or exercise programme that is
implemented. An interdisciplinary approach is needed to augment population’s
physical activity levels but the specificity of each intervention is key. For the results
5 Some subjects can (and do) achieve some kind of “effect” with lower doses than ACSM suggested guidelines.
Conversely, others need higher doses to provoke any measurable effect. 6 The risks of walking or running under a determined medical condition are still lesser than the benefits of walking or
running under those conditions, hence there are no contraindications for these modes of exercise.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
27
we are all aiming for, we believe that general practitioners should only prescribe
medicine and exercise should only be prescribed by exercise specialists.
References
1. Naci H, Ioannidis JPA. Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study. BMJ. 2013;347.
2. Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25 Suppl 3:1-72.
3. Bouchard C, Blair SN, Katzmarzyk PT. Less Sitting, More Physical Activity, or Higher Fitness? Mayo Clinic proceedings. 2015;90(11):1533-40.
4. Commission E. Special Eurobarometer 412 “Sport and physical activity”. 2014. 5. Blackwell D, Lucas J, Clarke T. Summary health statistics for U.S. adults: National Health Interview
Survey, 2012. 2014. 6. Autier P, Pizot C. Meaningless METS: studying the link between physical activity and health. BMJ.
2016;354. 7. Kyu HH, Bachman VF, Alexander LT, Mumford JE, Afshin A, Estep K, et al. Physical activity and risk of
breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ. 2016;354.
8. McPhail S, Schippers M. An evolving perspective on physical activity counselling by medical professionals. BMC Family Practice. 2012;13(1):1-8.
9. Tipton CM. The history of "Exercise Is Medicine" in ancient civilizations. Advances in physiology education. 2014;38(2):109-17.
10. Berryman JW. Exercise is medicine: a historical perspective. Curr Sports Med Rep. 2010;9(4):195-201.
11. Medicine ACoS. What is the EIM solution? http://www.exerciseismedicine.org/support_page.php/the-eim-solution5/2016 [cited 2016 15th of August].
12. Barnes P, Schoenborn C. Trends in adults receiving a recommendation for exercise or other physical activity from a physician or other health professional. Hyattsville, MD: National Center for Health Statistics, 2012.
13. Health. Do. High quality care for all: NHS next stage review final report. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/228836/7432.pdf: 2008.
14. Council PA. 2016 Participation Report. http://www.physicalactivitycouncil.com/PDFs/current.pdf:
2016. 15. Eden KB, Orleans CT, Mulrow CD, Pender NJ, Teutsch SM. Does counseling by clinicians improve
physical activity? A summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137(3):208-15.
16. Hillsdon M, Thorogood M, White I, Foster C. Advising people to take more exercise is ineffective: a randomized controlled trial of physical activity promotion in primary care. International Journal of Epidemiology. 2002;31(4):808-15.
17. Beedie C, Mann S, Jimenez A, Kennedy L, Lane AM, Domone S, et al. Death by effectiveness: exercise as medicine caught in the efficacy trap! Br J Sports Med. 2016;50(6):323-4.
18. Cornuz J, Ghali WA, Di Carlantonio D, Pecoud A, Paccaud F. Physicians' attitudes towards prevention: importance of intervention-specific barriers and physicians' health habits. Fam Pract. 2000;17(6):535-40.
19. Flocke SA, Crabtree BF, Stange KC. Clinician reflections on promotion of healthy behaviors in primary care practice. Health policy (Amsterdam, Netherlands). 2007;84(2-3):277-83.
20. Grandes G, Sanchez A, Sanchez-Pinilla R, et al. Effectiveness of physical activity advice and prescription by physicians in routine primary care: A cluster randomized trial. Archives of Internal Medicine. 2009;169(7):694-701.
21. Sallis JF, Haskell WL, Wood PD, Fortmann SP, Rogers T, Blair SN, et al. Physical activity assessment methodology in the Five-City Project. Am J Epidemiol. 1985;121(1):91-106.
22. Fie S, Norman IJ, While AE. The relationship between physicians’ and nurses’ personal physical activity habits and their health-promotion practice: A systematic review. Health Education Journal. 2013;72(1):102-19.
23. Cardinal BJ, Park EA, Kim M, Cardinal MK. If Exercise is Medicine, Where is Exercise in Medicine? Review of U.S. Medical Education Curricula for Physical Activity-Related Content. J Phys Act Health.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
28
2015;12(9):1336-43. 24. Dunlop M, Murray AD. Major limitations in knowledge of physical activity guidelines among UK
medical students revealed: implications for the undergraduate medical curriculum. Br J Sports Med. 2013;47(11):718-20.
25. Eakin EG, Glasgow RE, Riley KM. Review of primary care-based physical activity intervention studies: effectiveness and implications for practice and future research. The Journal of family practice. 2000;49(2):158-68.
26. Morgan F, Battersby A, Weightman AL, Searchfield L, Turley R, Morgan H, et al. Adherence to exercise referral schemes by participants – what do providers and commissioners need to know? A systematic review of barriers and facilitators. BMC Public Health. 2016;16(1):1-11.
27. Mann S, Jimenez A, Domone S, Beedie C. Comparative effects of three 48-week community-based physical activity and exercise interventions on aerobic capacity, total cholesterol and mean arterial blood pressure. BMJ Open Sport & Exercise Medicine. 2016;2(1).
28. King AC, Kiernan M, Oman RF, Kraemer HC, Hull M, Ahn D. Can we identify who will adhere to long-term physical activity? Signal detection methodology as a potential aid to clinical decision making. Health psychology : official journal of the Division of Health Psychology, American Psychological Association. 1997;16(4):380-9.
29. Cock D. Development of REFERQUAL; an Instrument for Evaluating Service Quality in GP Exercise Referral Schemes. University of Central Lancashire: University of Central Lancashire; 2006.
30. Zizzi S, Kadushin P, Michel J, Abildso C. Client Experiences With Dietary, Exercise, and Behavioral Services in a Community-Based Weight Management Program. Health promotion practice. 2016;17(1):98-106.
31. McClaran SR. The Effectiveness of Personal Training on Changing Attitudes Towards Physical Activity. Journal of sports science & medicine. 2003;2(1):10-4.
32. Fischer DV, Bryant J. Effect of certified personal trainer services on stage of exercise behavior and exercise mediators in female college students. Journal of American college health : J of ACH. 2008;56(4):369-76.
33. Klain IP, de Matos DG, Leitão JC, Cid L, Moutão J. Self-Determination and Physical Exercise Adherence in the Contexts of Fitness Academies and Personal Training. Journal of Human Kinetics. 2015;46:241-9.
34. Sykes D, Probst L, Otto RM, Wygand JW. The Effects of In‐Home versus facility Personal Training:
2009: Board #79 May 31 2:00 PM −3:30 PM. Medicine & Science in Sports & Exercise. 2007;39(5):S349-S50.
35. Rustaden AM, Haakstad LA, Paulsen G, Bo K. Bodypump And Resistance Training With And Without A Personal Trainer - A Randomized Controlled Trial: 2125 Board #277 June 2, 3: 30 PM - 5: 00 PM. Med Sci Sports Exerc. 2016;48(5 Suppl 1):599.
36. Storer TW, Dolezal BA, Berenc MN, Timmins JE, Cooper CB. Effect of supervised, periodized exercise training vs. self-directed training on lean body mass and other fitness variables in health club members. J Strength Cond Res. 2014;28(7):1995-2006.
37. Maloof RM, Zabik RM, Dawson ML. THE EFFECT OF USE OF A PERSONAL TRAINER ON IMPROVEMENT OF HEALTH RELATED FITNESS FOR ADULTS. Medicine & Science in Sports & Exercise. 2001;33(5):S74.
38. Ratamess NA, Faigenbaum AD, Hoffman JR, Kang J. Self-Selected Resistance Training Intensity in Healthy Women: The Influence of a Personal Trainer. The Journal of Strength & Conditioning Research. 2008;22(1):103-11.
39. Dictionaries O. Language matters http://www.oxforddictionaries.com/definition/english/exercise2016 [cited 2016 10th of September].
40. Smith A. Exercise is recreation not medicine. Journal of Sport and Health Science. 2016;5(2):129-34. 41. FDA. Aspirin. Comprehensive Prescribing Information
http://www.fda.gov/ohrms/dockets/ac/03/briefing/4012B1_03_Appd%201-Professional%20Labeling.pdf: FDA; 2016 [cited 2016 10th of September].
42. Swisher AK. Yes, “Exercise is Medicine”….but It Is So Much More! Cardiopulmonary Physical Therapy Journal. 2010;21(4):4-.
43. Nesti MS. Exercise for health: Serious fun for the whole person? Journal of Sport and Health Science. 2016;5(2):135-8.
44. Sjøgaard G, Christensen JR, Justesen JB, Murray M, Dalager T, Fredslund GH, et al. Exercise is more than medicine: The working age population's well-being and productivity. Journal of Sport and Health Science. 2016;5(2):159-65.
45. Nunan D. Doctors should be able to prescribe exercise like a drug. BMJ. 2016;353.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
29
3 - REVIEW PAPER: Fitness professionals’ pedagogical
intervention [Susana Franco & Vera Simões]
Susana Franco7, Vera Simões8
7ESDRM-IPSantarém - Sport Sciences School of Rio Maior, Polytechnic Institute of
Santarém, Portugal.
E-mail: [email protected]
8ESDRM-IPSantarém - Sport Sciences School of Rio Maior, Polytechnic Institute of
Santarém, Portugal.
E-mail: [email protected]
Abstract: It is recognised the importance of fitness professionals’ intervention for fitness centres’
quality and participants’ satisfaction and retention. The objective of this article is to present several
studies that show some particular aspects of pedagogical intervention which must be taken into account
for participants’ satisfaction and retention, namely encouragement, instruction and pay attention to
participants. Some implications for the practice of fitness professionals’ pedagogical intervention are
presented.
Key-words: Pedagogical intervention; Fitness professionals; Quality; Satisfaction
7 PhD Methodological Foundations of Research on Physical Activity and Sport; Master Degree in Exercise and Health;
Bachelor in Sport Sciences – Physical Education and Sport. Associate Professor at ESDRM-IPSantarém, Portugal. Subjects teaching: Fitness; Fitness Assessment and Exercise Prescription; Sport and Fitness Pedagogy; Fitness Internship, Thesis. Fitness Instructor in several Health Clubs. Conferences’ speaker in several events related with Fitness. Participation in several workshops, Conventions, Congress related with Fitness. Research and publication areas: Fitness and Sport Pedagogy. Participation in several European I&D Projects: Sport Physical Education and Coaching in Health (SPEACH), Fitness e-Learning Team Training (FELT2), e-Learning Fitness (e-LF), Physical Activity and Lifestyle Counselling (PALC), European Accreditation – Fitness (EA-Fitness), ECVET-Fitness, Aligning a European Higher Education Structure in Sport Science (AEHESIS). 8 PhD in Sport Sciences; Master Degree in Sport and Exercise Psychology; Post-Graduations in Fitness – Personal
Training and in Groups Fitness Instructor; Bachelor in Sport – Fitness. Assistant Professor at ESDRM-IPSantarém, Portugal. Subjects teaching: Fitness; Fitness Assessment and Exercise Prescription; Sport and Fitness Pedagogy; Exercise for Special Populations; Sport Systematic; Fitness Internship, Thesis. Teacher and coordinator of extracurricular subject, Fitness, in an elementary private school in Lisbon. Fitness Instructor in several Health Clubs. Conferences’ speaker in several events related with Fitness. Participation in several workshops, Conventions, Congress related with Fitness. Research and publication areas: Fitness and Sport Pedagogy. Participation in several European I&D Projects: Fitness e-Learning Team Training (FELT2), e-Learning Fitness (e-LF), Physical Activity and Lifestyle Counselling (PALC).
Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
30
Background
Although known the innumerable benefits of exercise [1,2], according to Sport and
Physical Activity Eurobarometer [3], there is still a large number (42%) of
European Union citizens that never exercised or played sport. One of the concerns
of fitness centres managers is to present a quality service, which, according to
several authors, may provide clients’ satisfaction and consequently clients’
retention [4-12]. Several authors refer the importance of human resources,
particularly fitness professionals, in a quality service of fitness centres and
participants’ satisfaction and retention [12-22]. The adherence to physical activity
in unsupervised program setting is very low [23], which reinforce the importance of
the intervention of fitness professionals. Fitness professionals can be one of the
participant's drop out motives from fitness centres [24], or can be a motive to
choose a fitness centre [25].
Discussion
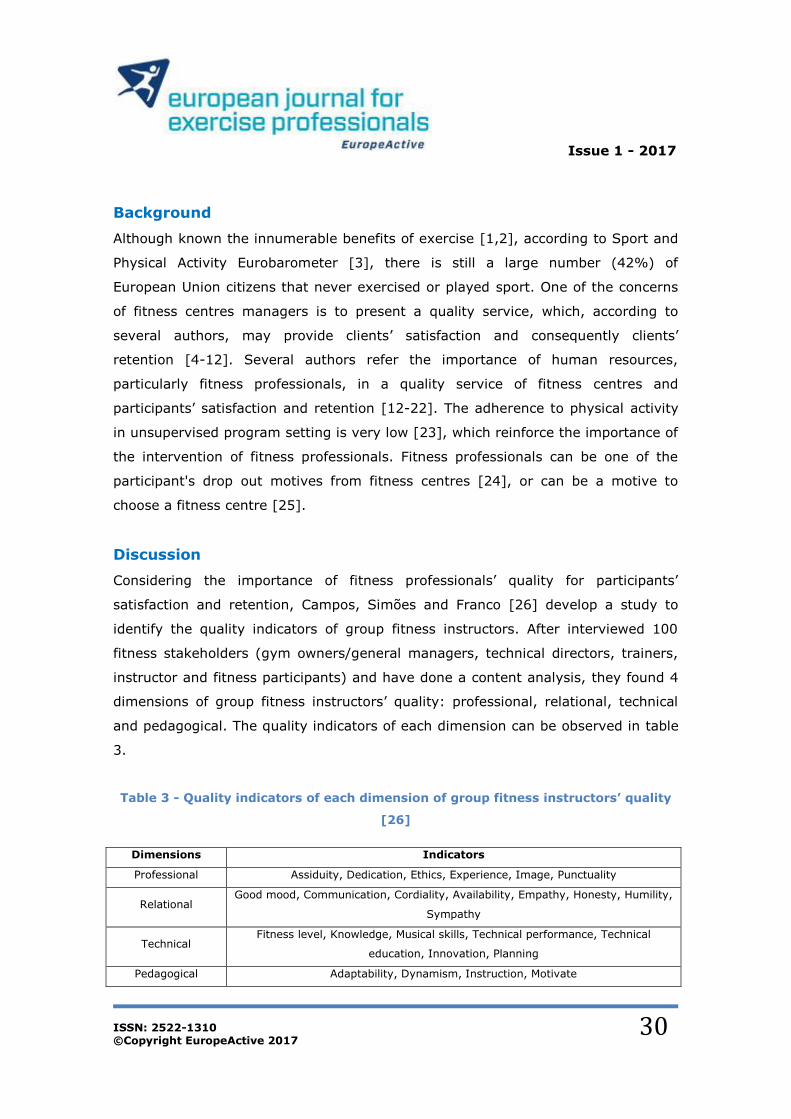
Considering the importance of fitness professionals’ quality for participants’
satisfaction and retention, Campos, Simões and Franco [26] develop a study to
identify the quality indicators of group fitness instructors. After interviewed 100
fitness stakeholders (gym owners/general managers, technical directors, trainers,
instructor and fitness participants) and have done a content analysis, they found 4
dimensions of group fitness instructors’ quality: professional, relational, technical
and pedagogical. The quality indicators of each dimension can be observed in table
3.
Table 3 - Quality indicators of each dimension of group fitness instructors’ quality
[26]
Dimensions Indicators
Professional Assiduity, Dedication, Ethics, Experience, Image, Punctuality
Relational Good mood, Communication, Cordiality, Availability, Empathy, Honesty, Humility,
Sympathy
Technical Fitness level, Knowledge, Musical skills, Technical performance, Technical
education, Innovation, Planning
Pedagogical Adaptability, Dynamism, Instruction, Motivate

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
31
The most cited quality indicators, in Campos et al. study [26], were empathy (from
relational dimension), motivate and instruction (from pedagogical dimension). This
study, like others studies [6,12,27-30], reveal the importance of fitness
professionals’ pedagogical intervention in fitness centres’ quality and participants’
satisfaction and retention.
In fact, there is a positive relation between the participants’ satisfaction and the
fitness professionals’ pedagogical behaviour [31]. Franco et al. [31] studied this
relation, in group fitness classes, and found a significant positive relation between
participants’ satisfaction and the following fitness instructors’ pedagogical
behaviours: encouragement, instruction (information, correction, positive
evaluation, negative evaluation and questioning) and monitoring (observe and pay
attention to what participants do and say). Therefore, behaviours for encouraging,
instruct and for pay attention to participants can contribute to increasing
participants’ satisfaction. Authors also found a significant negative relation between
participants’ satisfaction and the behaviour independent exercise of fitness
instructors, which means that if during a group fitness classes the fitness instructor
performs the exercise with participants but don’t pay attention to them,
participants will be less satisfied.
According to the multidimensional model of sports leadership from Chelladurai [32],
the satisfaction level of participants results from the level of congruence between
required, actual and preferred behaviour. This model also shows that situational
characteristics (e.g., group dimension, activity, objectives, tasks, etc.) and member
characteristics (e.g., age, gender, participant experience, personality, etc.) are
related to required and preferred behaviour. Based on this model, Franco, Cordeiro
and Cabeceiras [33] study participants’ preferences about group fitness instructors
characteristics in different activities, namely: resistance training, hip hop, aqua-
fitness and fitness-combat. They found some similarities in the participants’
preferences about group fitness instructors’ characteristics in different fitness
activities, such as being dynamic and motivator, that are two of the most preferred
characteristics by participants about group fitness instructors. However, authors

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
32
found significant differences between groups in 8 of the 23 characteristics. Authors
also study participants’ preferences of different group ages, about fitness
instructors’ characteristics, and they verify similarities in different group ages about
the most preferred characteristics in group fitness instructors, namely being
dynamic, motivator and imaginative. Nonetheless, they found significant differences
between groups in 14 of the 23 characteristics. Considering these results, it’s
important that fitness professionals adapt their intervention to participants’
characteristics, such as participants’ age, and to situational characteristics, such as
the activity.
Considering the importance, for participants’ satisfaction, of congruence between
required, actual and preferred behaviour about fitness professionals, it’s important
to know what participants prefer for fitness professionals act according to their
preferences. Participants’ preferences about fitness instructors’ pedagogical
behaviour were studied, in different group fitness activities, namely resistance
training [31], indoor cycling [34] and Zumba® [35]. Results are summarized in
table 4.
Table 4 - Participants’ preferences about fitness instructors’ pedagogical
behaviour, in resistance training [31], indoor cycling [34] and Zumba® [35]: most
preferred and less preferred behaviours.
Most preferred behaviours Less preferred behaviours
Resistance training
Encouragement (E, WE), Demonstration with information, Information (E, WE), Participative exercise (with clients as a
participant), Correction (E, WE), Positive evaluation (E), Questioning (E)
Conversations with others (clients or staff out of the class; E, WE), Attention to
interventions of others (clients or staff out of the class; E, WE), Negative affectivity (E, WE), Other behaviours (e.g., drink water or clean the face with a towel
without pay attention to participants), Independent exercise (do exercise without
pay attention to participants), Demonstration without information
Indoor cycling
Encouragement (E, WE), Questioning
(WE), Participative exercise, Positive evaluation (E), Positive affectivity (E, WE),
Correction (WE), Information (E)
Negative affectivity (E, WE), Conversations
with others (E, WE), Attention to interventions of others (E, WE),
Independent exercise, Other behaviours
Zumba® Demonstration with information,
Information (E, WE), Encouragement (E)
Conversations with others (E, WE), Attention to interventions of others (E, WE), Independent exercise, Negative affectivity (E, WE), Other behaviours, Demonstration without information
E: fitness instructor behaviour doing exercise simultaneously; WE: fitness instructor behaviour without
doing exercise simultaneously.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
33
There are some common participants’ preferred fitness professionals’ behaviours in
different activities, such as encourage participants and give information to explain
exercise while performing the exercise with participants (table 4). However, there is
some behaviours specificity that participants prefer in each group fitness activity.
For example, considering that indoor cycling requires fewer changes in the
exercises and consequently less instruction than the others activities, so, probably
for “breaking the ice” during practice, participants like that the instructor interacts
with them to create a good climate. In activities that require more technical skills,
like resistance training or Zumba®, participants prefer that, besides just show
(demonstrate) the model, also explain, with verbal and/or non-verbal instruction,
how to perform the exercises. Franco et al. [35] also found significant differences
between participants’ preference about the following instructional behaviour, which
means that participants don’t want just a model to see during “the Zumba® party”,
but also an explanation of the exercises: give information explaining the exercise,
verbally or non-verbally, while doing exercise; give information explaining the
exercise, verbally or non-verbally; show the model, before participants perform the
exercise, and give information explaining the exercise, verbally or non-verbally;
just show the model before participants perform the exercise (significantly less
preferred, compared with others).
There are also some common less participants’ preferred fitness professionals’
behaviours in different activities, which are related to bad mood or don’t pay
attention to participants, namely: negative affectivity creating a bad class climate;
conversations with people outside of the class (other clients or staff); pay attention
to interventions of people out of the class (other clients or staff); other behaviours,
such as fix the clothes, drink water, clean the sweat; do exercise without pay
attention to participants.
Considering that for a participant have a higher level of satisfaction the perception
and the preferences should be congruent [32], some studies were done to check
this congruence in fitness. Franco and Simões [36] compared participants’
perception and preferences, about pedagogical feedback of Body Pump®
instructors, and found significant differences in 19 of the 24 types of feedback.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
34
These results probably mean that participants are not satisfied with feedback of
Body Pump® instructors, which may be due to, in closed pre-choreographed
program, the obligation to follow the choreography, and perform pedagogical
functions for that, may limit the availability of fitness professional to observe and
correct participants.
In another study [31] group fitness instructors’ observed behaviour, participants’
perception and preferences, about pedagogical intervention, were related. Although
there was no congruence between the observed behaviour of the instructors and
the preference of the participants in various categories (26 of 33), there was
always congruence between perception and preference, which, perhaps, may
contribute to the participants satisfaction with the instructor, considering that
satisfaction results from the level of congruence between preference and
perception. But when authors relate observed behaviour with participants’
perception they only found 15 significant positive relations in the 33 tested
behaviours. Participants’ perception is influenced by their preference and affective
reactions, so the participants’ perception may not reflect reality [37].
Sometimes it is not just the participants who have no sense of reality, but also
fitness professionals. A study [38] that relates self-perception with the observed
behaviour of group fitness instructors, verified that fitness instructors had no idea
about one-third of the behaviours they performed. Considering these results, it is
important that fitness professionals do a self-analysis of their own intervention to
have a better sense of the reality [38].
A systematic process of supervision and self-analysis, through observation, using
for example videos, observation systems or checklists, should be done to collect
information about fitness professionals’ intervention, and give feedback for they
improve their professional performance. There are some observation systems about
fitness professional intervention, validated for fitness context, namely about
general pedagogic intervention [31,39], pedagogic feedback [40], class climate
[41], instruction [42], non-verbal kinetic communication [43], non-verbal
proxemics communication [44].

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
35
There are also instruments to know participants opinion about fitness professionals’
intervention, validated for this context, namely about fitness professional quality
[45], general pedagogic intervention [31,46] and pedagogic feedback [47].
Implications for practice
For participants’ retention and satisfaction, fitness professionals should focus their
pedagogical intervention especially in [31,34,35]:
Encouragement for practice;
Instruction situations: demonstrating and explaining verbally and non-
verbally the exercises, question participants about their physical state and
exercises’ understanding, correct participants’ performance and praise
them;
Pay attention to participants, observing and hear them.
Fitness professionals should adapt their intervention to participants’ characteristics
(e.g., age, gender, participant experience, personality) and to situational
characteristics (e.g., group dimension, activity, objectives, tasks).
For a continuous professional development fitness professionals should often do:
Continuous education [48];
Systematic self-analysis [49,50];
Be supervised by other professionals or coordinators [49,50];
For systematic self-analysis and supervision, observation systems, specific for
fitness context [31,39-44], can be used for this process. Surveys about
participants’ opinion [31,45-47] should sometimes be applied, to know their opinion
and adapt the intervention to preferences of class in general and to each individual
in specific, which can contribute to participants’ satisfaction and retention.
A triangulation of these different perspectives (observed behaviour, participants’
perception and preferences, instructors’ self-perception) can be used for a better
comprehension of the fitness professionals’ intervention, adjusting and improving it
[31,38,51].

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
36
References
1. Physical Activity Guidelines Advisory Committe. Physical Activity Guidelines Advisory Committee Report 2008. Washington, DC: U.S. Department of Health and Human Services; 2008.
2. World Health Organization. Global Recommendation on Physical Activity for Health. Geneve: World Health Organization; 2010.
3. TNS Opinion & Social. Special Eurobarometer 412 / Wave EB80.2 "Sport and Physical Activity". Brussels: TNS Opinion & Social; 2014.
4. Chang K. Understanding Service Quality in Health/Fitness Clubs from a Systems Perspective 1999 [6/1999]. Available from: www.dure.net/~kma/kjm/thesis/1c/KJM1c_4.pdf.
5. Makover B. Examining the Employee-Customer Chain in the Fitness Industry [Doctor Thesis]. Florida: The Florida State University - College of Education; 2003.
6. Papadimitriou DA, Karteroliotis K. The Service Quality Expectations in Private Sport and Fitness Centers: A Reexamination of the Factor Structure. Sport Marketing Quarterly. 2000;9(3):157-64.
7. Theodorakis N, Alexandris K, Rodriguez P, Sarmento PJ. Measuring Customer Satisfaction in the Context of Health Clubs in Portugal. International Sports Journal. 2004;8(1):44-53.
8. Fernández JG, Carrión GC, Ruíz DM. La Satisfacción de Clientes y su Relación con la Percepción de Calidad en Centro de Fitness: Utilización de la Escala CALIDFIT. Revista de Psicología del Deporte. 2012;21(2):309-19.
9. Gonçalves C, Meireles P, Carvalho MJ. Consumer Behaviour in Fitness Club: Study of the Weekly Frequency of Use, Expectations, Satisfaction and Retention. The Open Sports Sciences Journal. 2016;9(Suppl-1, M8):62-70.
10. Pedragosa V, Correia A. Expectations, Satisfaction and Loyalty in Health and Fitness Clubs. International Journal of Sport Management and Marketing. 2009;5(4):450-64.
11. Theodorakis N, Howat G, Ko YJ, Avourdiadou S. A Comparison of Service Evaluation Models in the Context of Sport and Fitness Centres in Greece. Managing Leisure. 2014;19(1):18-35.
12. Avourdiadou S, Theodorakis N. The Development of Loyalty Among Novice and Experienced Customers of Sport and Fitness Centres. Sport Management Review. 2014;17(4):419-31.
13. Gonçalves C, Buchman C, Carvalho MJ. Perceção da Qualidade do Serviço e Satisfação dos Sócios de Fitness: Contribuições para o Papel do Gestor. Revista Intercontinental de Gestão Desportiva. 2013;3(S2):47-58.
14. Albayrak T, Caber M. Symmetric and Asymmetric Influences of Service Attributes: The Case of Fitness Clubs Managing Leisure. 2014;19(5):307-20.
15. Liu Y-D, Hsu H-H. Identifying the Factor Structure of Costumer Satisfaction with Public Leisure Services. International Journal of Leisure and Tourism Marketing. 2010;1(3):288-303.
16. Pedragosa V, Biscaia R, Correia A. The Role of Emotions on Consumers' Satisfaction Within the Fitness Context. Motriz. 2015;21(2):116-24.
17. Argan M, Argan MT, Köse H, Soner A. The Relationship Between Fitness-Related Quality Satisfaction and Intention. International Refereed Academic Journal of Sports, Health and Medical Sciences. 2015;5(16):1-19.
18. Bodet G. Investigating Customer Satisfaction in a Health Club Context by an Application of the Tetraclasse Model. European Sport Management Quarterly. 2006;6(2):149-65.
19. Alexandris K, Palialia E. Measuring Customer Satisfaction in Fitness Centres in Greece: An Exploratory Study. Managing Leisure. 1999;4(4):218-28.
20. Lagrosen S, Lagrosen Y. Exploring Service Quality in the Health and Fitness Industry. Managing
Service Quality. 2007;17(1):41-53. 21. Yildiz SM. An Importance-Performance Analysis of Fitness Center Service Quality: Empirical Results
from Fitness Centers inTurkey. African Journal of Business Management. 2011;5(16):7031-41. 22. Tsitskari E, Antoniadis C, Costa G. Investigating the Relationship Among Service Quality, Customer
Satisfaction and Psychological Commitment in Cyprian Fitness Centres. Journal of Physical Education and Sport. 2014;14(4):514-20.
23. Sperandei S, Vieira MC, Reis AC. Adherence to Physical Activity in an Unsupervised Setting: Explanatory Variables for High Attrition Rates Among Fitness Center Members. Journal of Science and Medicine in Sport. 2016;19:916-20.
24. Franco S, Pereira L, Simões V, editors. Dropout Motives in Exercise. 13th Annual Congress of the European College of Sport Science; 2008; Estoril, Portugal.
25. Szumilewicz A. Multiple Influences Affecting the Women's Choice of a Fitness Club. Baltic Journal of Health and Physical Activity. 2011;3(1):55-64.
26. Campos F, Simões V, Franco S. Characterization and Comparison of the Quality Indicators of the Group Exercise Fitness Instructor, Considering the Intervenient, Gender and Age. International Journal of Sport, Exercise and Training Science. 2016;2(2):50-9.
27. Wininger SR. Instructors' and Classroom Characteristics Associated with Exercise Enjoyment by Females. Perceptual and Motor Skills. 2002;94:395-8.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
37
28. Cloes M, Laraki N, Zatta S, Piéron M, editors. Identification des Critères Associés à la Qualité des Instructeurs d'Aérobic. Comparaison des Avis des Clients et des Intervenants. Colloque L'Intervention dans le Domaine des Activités Physiques et Sportives: Compétence(s) en Mutation?; 2001; Grenoble.
29. Loughead TM, Carron AV. The Mediating Role of Cohesion in the Leader Behavior - Satisfaction Relationship. Psychology of Sport and Exercise. 2004;5:355-71.
30. Collishaw MA, Dyer L, Boies K. The Authenticity of Positive Emotional Displays: Client Responses to Leisure Service Employees. Journal of Leisure Research. 2008;40(1):23-46.
31. Franco S, Rodrigues J, Castañer M. Case Study 6.3: The Behaviour of Fitness Instructors and the Preferences and Satisfaction Levels of Users. In: Camerino O, Castañer M, Anguera MT, editors. Mixed Methods Research in the Movement Sciences. Oxon: Routledge; 2012. p. 202-14.
32. Chelladurai P. Leadership in Sport: A Review. International Journal of Sport Psychology. 1990;21:328-54.
33. Franco S, Cordeiro V, Cabeceiras M, editors. Perception and Preferences of Participants about Fitness Instructors' Profile - Comparison between Age Groups and Different Activities. 9th Annual Congress of the European College of Sport Science; 2004; Clermont-Ferrand, France: European College of Sport Science.
34. Mercê C, Franco S, Alves S, Campos F, Simões V. Preferências dos Praticantes de Indoor-Cycling, relativamente ao Comportamento Pedagógico do Instrutor. Revista da UIIPS. 2014;2(1):59.
35. Franco S, Mercê C, Simões V. Preferência dos Praticantes Acerca do Comportamento Pedagógico dos Instrutores de Zumba. Journal of Sport Pedagogy and Research. 2015;1(6):30-5.
36. Franco S, Simões V, editors. Participants' Perception and Preference about Body Pump® Instructors' Pedagogical Feedback. 11th Annual Congress of the European College of Sport Science; 2006; Lausanne - Switzerland.
37. Chelladurai P, Riemer HA. Measurement of Leadership in Sport. In: Duda JL, editor. Advances in Sport and Exercise Psychology. Morgantown, WV: Fitness Information Technology; 1998. p. 227-53.
38. Franco S, Simões V, Castañer M, Rodrigues J, Anguera MT. La Conducta de los Instructores de Fitness: Triangulación entre la Percepción de los Practicantes, Auto-percepción de los Instructores Y Conducta Observada. Revista de Psicología del Deporte. 2013;22(2):321-9.
39. Franco S, Rodrigues J, Castañer M. Comportamento Pedagógico dos Instrutores de Aulas de Grupo de Fitness de Localizada. Fitness & Performance Journal. 2008;7(4):251-63.
40. Simões V. Análise do Feedback Pedagógico em Instrutores Estagiários e Experientes na Atividade de Localizada. Comportamentos de Feedback Observados, Auto-perceção dos Instrutores e Preferências dos Praticantes [Tese de Doutoramento]. Vila Real: Universidade de Trás-os-Montes e Alto Douro; 2013.
41. Dias I. Desenvolvimento e Validação do Sistema de Observação do Clima de Aula, em Aulas de Grupo de Fitness [Dissertação de Mestrado]. Rio Maior: Escola Superior de Desporto de Rio Maior; 2015.
42. Luís T. Desenvolvimento, Validação e Aplicação Piloto do Sistema de Obsrvação da Instrução do
Instrutor de Fitness em Aulas de Grupo de Pilates (SOIIF-Pilates) [Dissertação de Mestrado]. Rio Maior: Escola Superior de Desporto de Rio Maior; 2017.
43. Alves S, Rodrigues J, Balcells MC, Foguet OC, Sequeira P, Carvalhinho L, et al. Validação e Desenvolvimento de um Sistema de Observação da Comunicação Cinésica do Instrutor de Fitness. Motricidade. 2014;10(1):77-87.
44. Alves S, Rodrigues J, Balcells MC, Foguet OC, Sequeira P, Carvalhinho L, et al. Sistema de Observação da Comunicação Proxémica do Instrutor de Fitness (SOPROX-Fitness): Desenvolvimento, Validação e Estudo Piloto. Revista Iberoamericana de Psicología del Ejercicio y el Deporte. 2013;8(2):281-99.
45. Campos F, Simões V, Franco S. A Qualidade em Atividades de Grupo de Fitness: Construção e Validação do Questionário "Qualidade do Instrutor de Fitness - Atividades de Grupo" (QIF-AG). Revista Psicologia. 2016;30(1):37-48.
46. Franco S, Simões V, Alves S, Moutão J, Cid L, Rodrigues J, editors. Development of the Questionnaire Instructors’ Pedagogical Behavior in Group Fitness Classes. XII ENSSEE Forum; 2013; Groningen, Holand.
47. Simões V, Rodrigues J, Alves S, Franco S. Validação do Questionário de Feedback de Instrutores de Fitness em Aulas de Grupo. Revista da UIIPS. 2013;1(1):227.
48. Batrakoulis A, Rieger T. European Barometer on the Top Future Trends in Education, Training and Certification of the Exercise Professionals. Journal for Physical Education and Sport Science. 2014;1(1):10-26.
49. Franco S, Simões V. Lazer e Qualidade de Vida: Formação de Técnicos de Fitness. In: Resende R, Albuquerque A, Gomes AR, editors. Formação e Saberes em Desporto e Educação Física. Lisboa: Visão e Contextos; 2015. p. 477-508.
50. Simões V, Santos-Rocha R. Communication: Giving and Gaining Feedback. In: Santos-Rocha R,

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
38
Rieger T, Jiménez A, editors. EuropeActive’s Essentials of Fitness Instructiors. Champaing, IL: Human Kinetics; 2015. p. 9-13.
51. Simões V, Santos-Rocha R. Body Awareness and Exercise Technique. In: Rieger T, Naclerio F, Jiménez A, Moody J, editors. EuropeActive's Foundations for Exercise Professionals. Champaign, Il: Human Kinetics; 2015. p. 191-8.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
39
4 - ORIGINAL RESEARCH: The transtheoretical model of
behaviour change and strategies for fitness professionals to
increase exercise behaviour [Jan Middelkamp]
Jan Middelkamp9
9Behavioural Science Institute, Radboud University, Montessorilaan 3,
Postbox 9104, 6500 HE, Nijmegen, the Netherlands.
E-mail: [email protected]
Abstract: The transtheoretical model of behaviour change (TTM) is often used to understand changes
in health-related behaviour, like exercise. This model also provides a practical framework for tailor-made
interventions, using four core constructs. The purpose of this paper is to apply this integrative model
towards exercise and provide strategies to be used by fitness professionals to increase exercise
behaviour of their clients or members, ultimately to maximise their health and fitness levels.
Key-words: Stages of change, adherence, health
9 Jan Middelkamp is a PhD researcher at the Radboud University in The Netherlands with a special interest in exercise
behaviour change. He lectures in motivation, health behaviour change, personal training and member retention. Jan is a board member of EuropeActive, Development Director at HDD Group and CEO of BlackBoxPublishers. More info: www.janmiddelkamp.com.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
40
Introduction
It is well documented that physical activity (PA) and exercise are beneficial for
health. This holds for individuals as well as for the population in general [1,2]. This
article focuses on exercise only, defined as planned, structured, repetitive bodily
movements with the intention to improve or maintain (physical) fitness or health
[3]. In the health and fitness sector, clients or members predominantly exercise for
health benefits [4]. Several studies demonstrate that exercise behaviour, meaning
the adoption of new behaviour and the maintenance of existing behaviour
(adherence), is problematic [5]. According to the International, Health, Racquet
and Sportsclub Association [6], approximately 151 million individuals exercise in
fitness facilities worldwide. In regards to exercising in a fitness setting, three kinds
of behaviour are relevant. First, an individual has to enter the facility, denoted as
attendance behaviour. Second, the individual has to attend the programme,
labelled as programme attendance. Third, the person needs to exercise according
to certain standards or minimums in terms of frequency, duration and intensity, in
short exercise behaviour. Research on attendance and exercise behaviour in health
and fitness shows strong indications that the frequencies are low. Middelkamp et al.
[7] reported low amounts of exercise sessions, analysing a database of 259,000 ex-
members with an average of 1.1 sessions per month over 24-months, including a
mix of individual and group exercise behaviour. Health effects based on these
frequencies will be marginal at best. In regards to types of exercises, a Dutch study
[8] reports that most males (60%) and females (45%) combine individual and
group exercises, but 31% of the females only participate in group exercise
programmes. The study also reports that most individuals participate in two or
more types of programmes; about 50% participate in at least one group exercise
programme and 23% participate only in group exercise classes with an instructor. A
core task of fitness professionals is to support and increase all three kinds of
behaviour, to ultimately maximise the effects of exercise towards the health and
fitness levels of clients and members.
Transtheoretical Model of Behaviour Change
To systematically study and understand exercise behaviour, but also to provide
practical strategies, several social-cognitive models have been put forward. The

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
41
transtheoretical model (TTM) is frequently used to study different kinds of health
behaviours, including smoking, physical activity and exercise. In different
populations and settings, the existence of significant relationships between the TTM
and exercise behaviour have been demonstrated [9-11]. To increase exercise
behaviour, an in-depth understanding of the development of this specific behaviour
and its change over time is needed, which makes the TTM useful as a theoretical
model. The TTM model was originally developed by observing smokers that wanted
to change their behaviour without professional intervention, the so-called self-
changers. The model describes four key variables: stages of change; decisional
balance; self-efficacy and processes of change. The stages of change contain five
main stages to cease an unhealthy or adopt a healthy behaviour (like exercise), or
six stages if the termination/relapse stage is also included [12]. The stages are
presented in table 5.
Table 5 - Stages of change.
Stage Name Description
1 Pre-
contemplation People who aren’t currently not thinking of changing their behaviour. In short: I WON’T and I CAN’T stage.
2 Contemplation People who aren’t currently changing their behaviour, but do intent to change in the next six months. In short: I MIGHT stage.
3 Preparation People who are preparing to change their behaviour within the next 30 days. In short: I WILL stage.
4 Action People who made a change in their behaviour, but have changed recently (up to six months but no longer). In short: I AM stage.
5 Maintenance People who have changed for some time, at least six months. The behaviour has become a reasonably stable characteristic. In short: I HAVE stage.
6 Relapse On the one hand, people can maintain their behaviour, on the other hand, they can relapse into the previous behaviour and return to the earlier stages.
The decisional balance is the second construct of the TTM, and contains two main
scales of Pros and Cons for changing behaviour. There are four dimensions for Pros:
useful benefits for the self; useful benefits for others; self-approval; approval of
others. There are also four dimensions for Cons: useful losses for the self; useful
losses for others; self-disapproval; disapproval of others. The Pros and Cons are
important for influencing persons in an early stage (pre-contemplation –
preparation) to the action stage.
The third construct is self-efficacy [13]. In short, self-efficacy is a person’s belief in

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
42
capabilities to overcome personal, social and environmental barriers to exercise.
Self-efficacy is commonly split and measured in two aspects and scales: Barrier
self-efficacy is the confidence to overcome barriers to exercise; Temptation is
characterised as the negative impulses to revert back to previous behaviours.
According to self-efficacy theory, two important factors can influence the confidence
to adopt and maintain exercise behaviour. The first is efficacy expectations, that is
one’s belief about their own competence. The second factor is outcome
expectations, one’s belief in regards to the perceived result or outcomes of exercise
behaviour. According to self-efficacy theory, human behaviour is strongly
influenced by self-regulation [14]. The self-regulative mechanisms operate through
three subfunctions; Self-monitoring of one’s behaviour on determinants and
consequences; Judgement of one’s behaviour in relation to personal standards and
circumstances; Affective self-reaction. To increase self-efficacy, exercisers should
be first supported in selecting the right exercises to increase efficacy expectations.
Second, they need guidance in managing outcome expectations, for example by
setting and tracking relevant goals.
The fourth construct measures ten processes of change, which can be divided into
five cognitive processes and five behavioural processes. The five cognitive
processes are: consciousness raising (e.g., looking for information); dramatic relief
(e.g., emotional aspects of change); environmental reevaluation (e.g., assessment
of how inactivity affects society); self-reevaluation (e.g., assessment of personal
values) and social liberation (e.g., awareness, availability and acceptance of active
lifestyles in society). The five behavioural processes are: counter conditioning (e.g.,
substituting physical activity for sedentary leisure choices); helping relationship
(e.g., using social support during change); reinforcement management (e.g., self-
reward for change); self-liberation (e.g., commitment and self-efficacy beliefs
about change); stimulus control (e.g., managing situations that prompt inactivity or
activity) [15,16].
Spencer et al. [11] reviewed 150 studies using the TTM. A total of 31 stage-
matched intervention studies were reviewed and 25 studies were shown to be
successful in motivating participants towards higher stages and increased amounts

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
43
of exercise. Towards the health and fitness sector, Middelkamp et al. [17] executed
a systematic review on exercise behaviour in fitness clubs. A small amount of
studies used constructs of the TTM. For example, Nigg et al. [18] tested the
decisional balance sheet (DBS). The experimental group received a phone call and
were asked to think systematically and record the expected gains and losses of
exercising in a fitness centre. Members reported twice as many Pros as Cons. Pros
were: good equipment/facilities and social interaction. Cons were: crowded
conditions and lack of equipment. Attendance declined from the 4th week baseline
to the 8th week in control and placebo group, but less change in the experimental
group. DBS was effective to keep attendance up [19]. Annesi [19] tested the effect
of a multiple component behaviour change treatment package (for 36 weeks),
partly based on the constructs of self-efficacy and processes of change. The
package included strategies like relapse prevention, self-reinforcement, and
contracting. All studies (US, Great Britain and Italy) showed a significantly higher
attendance (13-30%) and less drop-out (30-39%) for the treatment group [19].
This coach-approach system was also tested in Annesi [20,21], Annesi and Unruh
[22], and Annesi et al. [23], and proved again that adherence was positively
influenced by the intervention. Cox et al. [24] compared home versus fitness centre
based exercise for 18 months, using the stages of change constructs. The centre
based group had higher adherence than the home based group (97, 94, 81%
versus 87, 76, 61%) at respectively 6, 12 and 18 months. The levels of drop-out
range from 3 to 39%. Levesque et al. [25] studied how learned resourcefulness is
related to spontaneous process of change in 6 months, at adult members (n=104)
in the preparation stage of the TTM. Learned resourcefulness are regulatory skills
that enable a person to self-control his/her behaviour. Persons with stronger self-
regulatory capacity use more processes of change over time. They try harder in
attempting to maintain exercise involvement. Middelkamp et al. (2016) tested two
self-regulation interventions to increase self-efficacy and group exercise behaviour.
In total 122 participants (Mage 42.02 yr.; SD 12.29; 67% females) were recruited
and randomly assigned to one control and two experimental groups. The control
group was limited to participate in one virtual group exercise programme only
(group 1). The first experimental group was able to self-set their activities and
participate in multiple group exercise programmes (group 2). The second
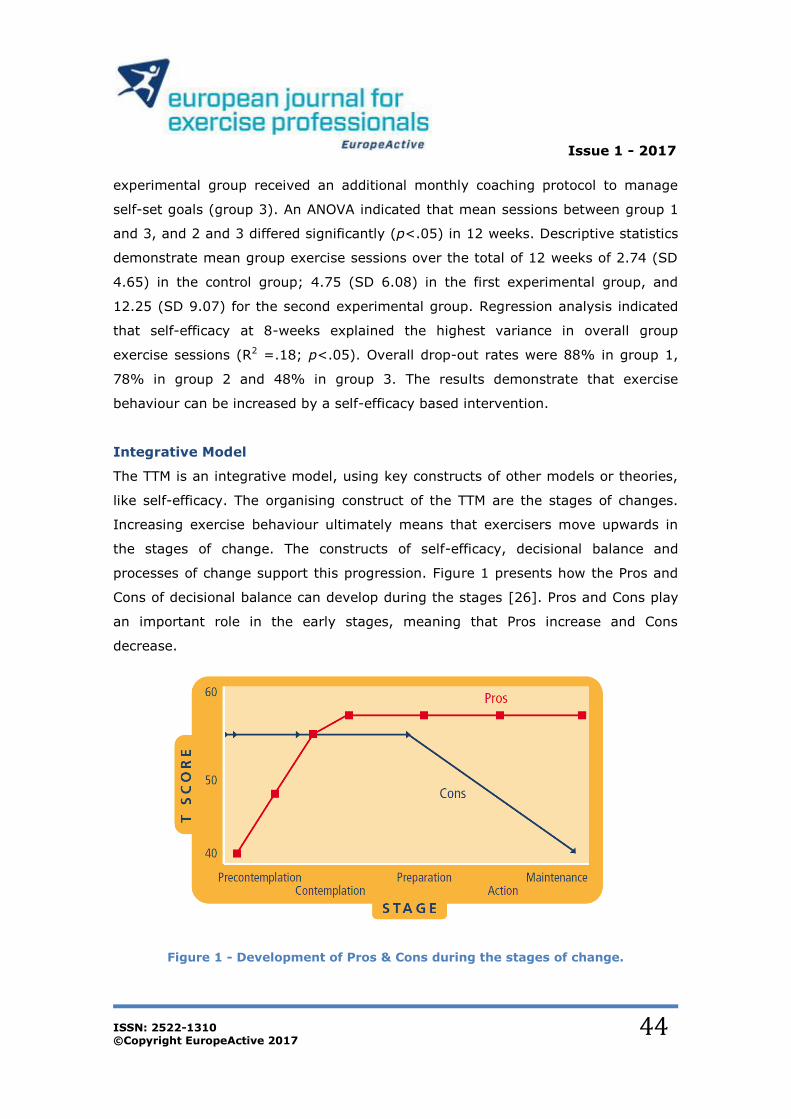
Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
44
experimental group received an additional monthly coaching protocol to manage
self-set goals (group 3). An ANOVA indicated that mean sessions between group 1
and 3, and 2 and 3 differed significantly (p<.05) in 12 weeks. Descriptive statistics
demonstrate mean group exercise sessions over the total of 12 weeks of 2.74 (SD
4.65) in the control group; 4.75 (SD 6.08) in the first experimental group, and
12.25 (SD 9.07) for the second experimental group. Regression analysis indicated
that self-efficacy at 8-weeks explained the highest variance in overall group
exercise sessions (R2 =.18; p<.05). Overall drop-out rates were 88% in group 1,
78% in group 2 and 48% in group 3. The results demonstrate that exercise
behaviour can be increased by a self-efficacy based intervention.
Integrative Model
The TTM is an integrative model, using key constructs of other models or theories,
like self-efficacy. The organising construct of the TTM are the stages of changes.
Increasing exercise behaviour ultimately means that exercisers move upwards in
the stages of change. The constructs of self-efficacy, decisional balance and
processes of change support this progression. Figure 1 presents how the Pros and
Cons of decisional balance can develop during the stages [26]. Pros and Cons play
an important role in the early stages, meaning that Pros increase and Cons
decrease.
Figure 1 - Development of Pros & Cons during the stages of change.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
45
For self-efficacy, the same type of development can be presented for barrier self-
efficacy and temptation to not exercise. The last will decrease moving over the
stages of change, this first will increase because exercisers gain more and more
strategies to overcome barriers.
Figure 2 - Development of Self-Efficacy during the stages of change.
Fallon et al. [27] report several differences between men and women. Compared to
men, women reported significantly less barriers-efficacy, greater pros of exercise,
and greater use of behavioural and experiential processes of change. For the men,
affect temptation was the only significant correlate of action/maintenance, while
barriers efficacy, environmental evaluation, and affect temptation were associated
with maintenance/termination. For the women, environmental re-evaluation and
social liberation were associated with action/maintenance, while barriers-efficacy
was the only construct correlated with maintenance/termination.
Practical applications
The TTM implicates strongly that behaviour change strategies should address the
specific stage of a client or member. It is of no use to provide a pre-contemplator
with self-efficacy driven exercise goals. Keep in mind that defining the stages of

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
46
change of a single person should be done per type of health behaviour. In table 6,
health-related behaviours like physical activity, exercise, smoking and sitting, are
summarised and by example connected to a stage of change for an imaginary
person. In the case of this person, let's name him Jan, it is clear that he is
preparing to start an exercise programme. So strategies to support Jan’s exercise
behaviour could be related to this stage. When it comes to his sitting behaviour, he
is not considering any change, which can be damaging for his health if he is sitting
for many hours a day. The result is that a different approach is needed to change
this type of behaviour.
Table 6 - Combinations between type of health behaviour and stages of change
[28]
As discussed, self-efficacy is one of the strongest and most tested constructs of the
TTM with a large amount of studies demonstrating positive effects on increasing
exercise behaviour. There are four sources for an individual’s self-efficacy. These
are (in order of effectiveness): Past experiences in performing specific behaviours;
Vicarious experiences (watching others successfully perform behaviours); Verbal
persuasion (being told that one is capable); Experiences of physiological arousal.
Self-efficacy can be increased by implementing simple strategies in an exercise
programme of a client or member. The same strategies can be used within a
nutritional or physical activity programme, if applied to a specific stage. Clients
should be interviewed about past experiences and choose a starting activity where
they feel confident with. Add new activities later when their confidence has
increased. Give examples of other clients that specific behaviour can be done,

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
47
preferably other that are similar to the client. Within a specific behaviour
alternatives and options to progress the work-out or regress the work-out should
be provided. Also, educate clients on the expected outcomes and positives of their
(exercise) behaviour. Be very specific in the outcome and what to expect and
supply clients with self-monitoring systems so they can track how they are doing.
The processes of change provide a list of strategies to increase exercise behaviour.
The cognitive processes are most effective in the early stages of change. For
example a pre-contemplator can be moved towards a contemplator by
consciousness raising, like providing information and dramatic relief, increasing the
emotional aspects of (not) changing. The five behavioural strategies are used most
in the later stages of change, for example to adhere to an exercise programme.
Strategies as helping relationship, meaning using social support during change, and
reinforcement management should be implemented during the action and
maintenance stage of an exercise programme.
Conclusion
The health and fitness sector has been growing globally since the eighties, offering
exercise programmes to hundreds of millions of members worldwide. It seems
positive that so many start an exercise programme in a type of fitness facility, but
exercise adherence is low and drop-out rates are high. People are paying to not to
go to the gym [29]. In general, researchers show a lack of interest in this
population and specific setting. Even when studies on other populations can be
applied to exercise behaviour in fitness clubs, specific research in this context is
needed to develop tailor-made strategies and programmes to increase exercise
behaviour and ultimately the health and fitness levels of members. The
transtheoretical model of behaviour change offers a practical framework for this but
needs additional research to improve the effectiveness of programmes to support
the mission of EuropeActive: More people, more active, more often.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
48
References
1. American College of Sports Medicine (2010). ACSM’s guidelines for exercise testing and prescription. American College of Sports Medicine. 8th revised edition. Williams & Wilkins.
2. Dishman, R.K., Heath G.W., & Lee, I-M. (2013) Physical activity epidemiology. 2nd Edition. Human Kinetics Publishers, Champaign USA.
3. Buckworth J., Dishman, R.K., O’Conner, P.J., & Tomporowski, P.D. (2013). Exercise Psychology, 2nd Edition. Human Kinetics, Champaign, USA.
4. Baart de la Faille, M., Middelkamp, J., & Steenbergen, J. (2012). The state of research in the global fitness industry. BlackBox Publishers, the Netherlands.
5. Berger, B.G., Pargman, D., & Weinberg, R.S. (2002). Foundations of exercise psychology. Morgantown, WV: Fitness Information Technology.
6. IHRSA (2016). The IHRSA global report. Boston, USA. 7. Middelkamp, J., Van Rooijen, M. and Steenbergen, B. (2016) Attendance behaviour of ex-members
in fitness clubs: A retrospective study applying the stages of change. Perceptual and Motor Skills, 122 (1), 350 – 359.
8. Hover P., S. Hakkers and Breedveld, K. (2012) Trendrapport fitnessbranche 2012. Mulier Instituut, Den Bosch & Arko Sportsmedia, Nieuwegein.
9. Fallon, E.A., Hausenblas, H.A., & Nigg, C.R. (2005). The transtheoretical model and exercise adherence: examining construct associations in later stages of change. Psychology of Sport and Exercise, 6(6), 629-641.
10. Marshall, S. J., & Biddle, S. J. H. (2001). The transtheoretical model of behaviour change: A meta-analysis of application to physical activity and exercise. Annals of Behavioural Medicine, 23, 229-291.
11. Spencer, L., Adams, T. B., Malone, S., Roy, L., & Yost, E. (2006). Applying the transtheoretical model to exercise: a systematic and comprehensive review of the literature. Health promotion practice, 7(4), 428-443.
12. Prochaska, J., & Marcus, B. (1994). The transtheoretical model: applications to exercise. Dishman R.K. ed. (1994) Advances in exercise adherence. Human Kinetics, Illinois, 161 - 180.
13. Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman. 14. Bandura, A. (1991) Social cognitive theory of self-regulation. Organizational behaviour and human
decision processes, 50, 248 – 287. 15. Dishman, R. K., Jackson, A. S., & Bray, M. S. (2010). Validity of processes of change in physical
activity among college students in the TIGER study. Annals of Behavioural Medicine, 40(2), 164-175.
16. Reed, G.R. (2001). Adherence to exercise and the transtheoretical model of behaviour change. In: Bull, S. (Ed.) (2001) Adherence issues in sport and exercise, 19 – 45.
17. Middelkamp, J. and Steenbergen, B. (2015) The transtheoretical model and exercise behaviour of members in fitness clubs: Systematic review. Journal of Fitness Research, 4, 2, August 2015, 43 – 54.
18. Nigg, C.R., Courneya, K.S., & Estabrooks, P.A. (1997). Maintaining attendance at a fitness center: an application of the decision balance sheet. Behavioural medicine, 23: 130 – 137.
19. Annesi, J.J. (2003). Effects of a Cognitive Behavioural Treatment Package on Exercise Attendance and Drop-Out in Fitness Centers. European Journal of Sport Science, 3 (2): 1 - 16.
20. Annesi, J.J. (2004b). Relationship of social cognitive theory factors to exercise maintenance in
adults. Perceptual and Motor Skills, 99: 142-148. 21. Annesi, J.J. (2007). Effects of computer feedback and behavioural support protocol on dropout from
a newly initiated exercise programme. Perceptual and Motor Skills, 105: 55 – 66. 22. Annesi, J.J., & Unruh, J.L. (2007). Effects of the coach approach intervention on drop-out rates
among adults initiating exercise programmes at nine YMCA’s over three years. Perceptual and Motor Skills, 104: 459 – 466.
23. Annesi J.J., Unruh, J.L., Marti, C.N., Gorjala, S., & Tennant, G. (2011). Effects of the coach approach intervention on adherence to exercise in obese women: assessing mediation of social cognitive theory factors. Research Quarterly for Exercise and Sport, 82 (1): 99 – 108.
24. Cox, K.L., Burke, V., Gorely, T.J., Beilin, L.J., & Puddey, B. (2003). Controlled comparison of retention and adherence in home- versus centre-initiated exercise interventions in woman ages 40-65 years: the SWEAT study (sedentary woman exercise adherence trail). Preventive Medicine, 36: 17 - 29.
25. Levesque, L., Gauvin, L., & Desharnais, R. (2003). Maintaining exercise involvement: the role of learned resourcefulness in process of change. Psychology of Sport and Exercise, 4: 237 – 253.
26. Velicer, W. F, Prochaska, J. O., Fava, J. L., Norman, G. J., & Redding, C. A. (1998). Smoking cessation and stress management: Applications of the Transtheoretical Model of behavior change. Homeostasis, 38, 216-233.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
49
27. Fallon, E.A., Hausenblas, H.A., & Nigg, C.R. (2005). The transtheoretical model and exercise adherence: examining construct associations in later stages of change. Psychology of Sport and Exercise, 6(6), 629-641.
28. Middelkamp, J. (Ed) (2015). EuropeActive’s Essentials of Motivation and Behaviour Change. EuropeActive, Brussels, BlackBoxPublishers, The Netherlands.
29. DellaVigna, S. & Malmendier, U. (2006). Paying not to go to the gym. The American Economic Review, 96: 604 – 719.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
50
5 - ORIGINAL RESEARCH: Health Promotion in Commercial
Fitness Gyms. An analysis of organizational culture as an
organization-specific premise for decision-making. [Thomas
Rieger & Michael Pfleger]
Thomas Rieger10*
Michael Pfleger11
10 & 11 Business and Information Technology School (BiTS), Staatlich anerkannte
private Hochschule, Reiterweg 26b, 58636 Iserlohn, Germany
* Contact person for this article. E-mail: [email protected]
Abstract: Commercial fitness gyms often consider themselves as professional healthcare
organizations and strive for co-operations with stakeholders of the healthcare system. For gym
managers the decision to include exercise programmes into their portfolio of services is of vital
importance. This article analyses whether the implementation of health-oriented exercise programmes in
commercial fitness gyms, particularly against the background of the existing corporate culture, is
feasible. First, the most important characteristics of a corporate culture are described from a theoretical
perspective. Subsequently, the results of an empirical analysis are presented. They indicate that the
integration of specific exercise programme services can be classified as economically reasonable. Fitness
gyms have shed their idealistic identity and changed into market-oriented enterprises.
Key-words: gym, health promotion
10
Thomas Rieger was the Chairman of the Standards Council of EuropeActive (2012-2015). He holds a Doctoral
Degree in Social Sciences with a specialization in Sport Science (German PhD-equivalent) from the University of
Tübingen and a Master Degree in Public Health. In 2007 he was appointed as a Professor of Sport Management at the
Business and Information Technology School – BiTS in Iserlohn, Germany. At BiTS University he is Vice-Dean of the
Bachelor Programme Sport & Event Management and the Master Programme International Sport & Event Management.
He served as Visiting Professor at the Real Madrid Graduate School and the European University Cyprus in Nicosia.
Before entering academia in 2006, he gained more than six years of work experience in the fitness industry, especially
in the fields of fitness marketing and quality management. 11
Michael Pfleger is a Master degree student of the Sport Management at the Business and Information Technology School – BiTS in Iserlohn, Germany.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
51
Introduction In the last three decades commercial fitness gyms have become a central element
of the German sport system. According to the annually published statistics of
Deloitte nine million people hold a membership in a commercial fitness gym
(Deloitte & EuropeActive, 2016). Between 2000 and 2006 the fitness sector had to
overcome a critical situation because of a declining number of members, though
since 2007 the numbers have again steadily increased. Commercial fitness gyms
are market-driven organizations with the need to open themselves for changes in
their environment, to reflect decisions permanently and to adapt strategies for
ensuring their economical existence. The increasing number of gyms led to
competitive situations and to a professionalization of programs and services with
the purpose to achieve differentiation. One effect was that the independent, owner-
managed gyms lost market share for the benefit of fitness gym chains. In addition,
services of health promotion have been successively included into the range. The
qualitative and health-oriented optimization of gym equipment and the expansion
of an intra-industry market for study programs in exercise and health sciences are
indicators for a prioritization. Health and health promotion have become core
components of the product policy of fitness gyms. Furthermore, it has to be
mentioned, that beside the focusing on exercise, approaches of quality
management have been integrated into the organizational structure not only to
maintain and improve the operational efficiency but also for the successful
implementation of exercise programmes (Eigenmann, 2004; Rieger, 2007).
Currently the question whether these programmes fulfil the scientific quality
requirements of exercise programmes (Bouchard, Blair & Haskell, 2006; Brehm,
1997; 1998) are mostly unacknowledged, because the primary organizational
purpose of a commercial gym is not to improve the health status of its customers
by providing scientific based exercise programs or a qualitative sports medical
coaching, but rather to maximize profit.
At this point one question becomes relevant: Under which premises does a
commercial fitness gym include a health promotion orientation or, even better,
does it offer programs with a health promotion orientation or not? This article deals
with the decision whether to implement health-oriented exercise programs or not.
Taking into consideration, that „decisions are incidents, that occur in a certain

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
52
moment and with their appearance already disappear“ (Luhmann, 1988, p. 168,
author’s translation), it gets obvious, that a decision does not describe a process, it
only determines the moment to differentiate the pre form the post. In order to
answer the main question of this article, it is necessary to focus on the rules, which
influence a decision, namely the organizational decision programmes (e.g., the
organizational culture) (Luhmann, 2000). Accordingly, it has to be assumed that
commercial fitness gyms differ from organizations of the healthcare system,
because of their economic orientation.
The present article tries to give answers to the question under which premises
health-oriented exercise programmes are implemented. Therefore, the current
state of research will be illuminated. Afterwards a theoretical approach for the
characterization of organizational decision programmes will be deduced. Within a
qualitative empirical study in the region of East Westphalia/Germany owners of
commercial fitness gyms have been interviewed. Against the background of the
theoretical approach and the related empirical results implications regarding the
feasibility of implementation of health-oriented exercise programmes are
formulated.
State of Research
The current state of research about the commercial fitness gym as a specific type of
organization reveals a lack of publications. Most of the literature makes the
motivational structure of gym customers a subject of discussion (Schubert, 1998;
Heinemann & Schubert, 1990; Kosinski & Schubert, 1989; Janssen, Wegner &
Beyer, 1989). An analysis of the importance of exercise programmes was only
accomplished with regard to these motivational structures. Several authors could
identify a higher importance of health-related compared to other motives (Mrazek,
1988; Trillitzsch, 2004). The study of organizational structures was only taken up
by some publications (Dreßler, 2003; Rampf, 1998; Sack & Hennrich, 1989;
Dietrich, Heinemann & Schubert, 1990). A detailed characterization of
organizational decision programmes in commercial fitness gyms has been left out of

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
53
consideration. In this context the sports club12 research can rely on results with
more solid evidence. Sports clubs have changed only marginally throughout the last
years because of their tendency to an organizational closing (Baur & Braun, 2003;
Emrich, 2005; Emrich, Pitsch & Papathanassiou, 2001 and others). Even these
publications only deliver a minor contribution for the explanation of organizational
decision programmes in sports organizations. Thiel and Meier (2004) submitted a
remarkable publication, which characterizes the sports club as an immunological
organization based on the organizational theoretical approach of Niklas Luhmann
(2000). During its existence the sports club has learned to neutralize environmental
influences like value changes or changes in the sport demand.
In summary, the current state of research is deficient. That is primarily because of
the lacking research interest in sport science towards the fitness sector. Especially
a missing theoretical approach to explain organizational decision-making obstructs
answering the question, why commercial fitness gyms offer health-oriented
exercise programs.
In the next step the main theoretical aspects of sports club research (Thiel & Meier,
2004; Thiel et al., 2006; Thiel & Mayer, 2010) should be deduced and afterwards
be transferred to the commercial fitness gym as a different type of organization in
the sport system.
Aspects of Organizational Theory
Organisations permanently make decisions. With regard to the main question it is
necessary to analyse the reasons and premises for decisions in gyms. The basis for
such a ‘decision-oriented’ consideration of organisations is issued by Luhmann’s
sociological management approach. Thus, organisations construct and reconstruct
themselves by the communication of decisions (Luhmann, 2000). A cluster of
decisions arises from these decisions. Within this cluster every decision has a
meaning for another decision, in other words, the organisation deals with decisions
about decisions (Luhmann, 2000). Therefore, Luhmann introduces the term
12
In the German sport system the term (sports) club always refers to voluntary (non-profit) sports organizations with
significant differences to economic enterprises (Thiel & Mayer, 2009).

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
54
decision premises. These premises are basic decisions, build the structure of an
organisation and provide an orientation for upcoming decisions. Two categories of
premises have to be distinguished: the decidable decision premises and the non-
decidable decision premises.
The first category is empirically observable and differentiated into (1) the decision
programmes (Entscheidungsprogramme), „which define the objectives of the
organization and the methods used to achieve them“ (Thiel & Mayer, 2010, p. 85,
author’s translation), (2) the communication channels and (3) the human
resources. The non-decidable premises can be described as informal values and
traditions, which are not scrutinized by the members of the organisation. Luhmann
uses the term organizational culture (2000), which fills a major role for analysing
the main task of this paper. A complete analysis of the decision premises would
exceed the scope of this paper. So the next step is to focus on the emergence and
impact of organizational culture in commercial fitness gyms. From this point on it is
possible to comprehend the decision process for the implementation of health-
oriented exercise programmes.
The Organizational Culture as a part of the Social System
Before approaching the term organizational culture, a brief introduction of the
concept of organizational learning must be prepended to ensure a better
understanding of the functions of organizational culture.
Several sociological publications, which define learning as an adjustment process
based on precise goals, identified two basic functions of organizational learning.
1. A member of the organization learns to accomplish actions by referring to the
goals and rules of the organization (Argyris & Schön, 1978).
2. The organizational rules should be scrutinized by reflection. This type of
organizational learning also implies that the organization does not learn
directly by observing the relationship to its environment. Because of its
autopoetic and self-referential orientation the organization has the ability to
create the importance of irritations in its environment by itself (Baecker,
1999; Luhmann, 2000; Willke 1998). Changes in the environment are only

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
55
perceived, when they seem to be relevant for the organization. Nevertheless,
the parameters to evaluate this relevance are created by the organization. If
the organization sees itself forced to change structures, this happens on the
basis of internal developed criteria. Substantial structural changes can be the
result, because the organization differentiates a dynamic system of self-
reflection, which is permanently in search of necessities to adjust.
Out of these two functions of organizational learning arises a third one. The
determination on specific premises leads inevitably to a permanent reflection of
decisions (Luhmann, 2000; Thiel & Meier, 2004), which initiates an organizational
hang-up and a restriction in the ability to act. Organizations need an orientation,
which allows them to ensure the approval of decisions without reflecting
permanently. This task is succeeded by the organizational culture (Luhmann,
2000). The culture is not called into question by the organization, it is composed of
several non-decidable decision premises like traditions, common values and general
accepted informal rules (Thiel & Meier, 2004).
In its development organizational culture is marked by contingency, because it
emerges in its own system and based on the system’s operations (Thiel et al.,
2006). Within the organization it is not contingent, but rather understood as an
implicitness, which is accepted by everyone (Luhmann, 2000). The non-decidable
decision premises work secretly and they participate unnoticeably in all decision
processes. Moreover, they promote the community spirit within the organization.
Organizational culture emerges spontaneously and is a „redundant communication“
(Luhmann, 2000, p. 243, author’s translation). In order to ensure that decisions are
accepted, the organizational culture has furthermore the task to reduce
uncertainty, as it generates intimacy with its informal rules, provides stability for
the system and enables to distinguish from other systems (Luhmann, 2000; Thiel
et al., 2006). The concealment and informality of organizational culture influence
the capability to react flexibly to environmental changes much clearer than the
decidable decision premises. This does not mean, that culture is not adaptable, but
it is “more stable than the decidable decision premises” (Thiel et al., 2006, p. 31,
author’s translation). Especially in organization with poorly defined decidable

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
56
decision premises, the organizational culture gains importance when it comes to
evaluate environmental changes. To put it simple in terms: porous and non-
stringent decidable decision premises, namely decision programs, communication
channels and human resources are combined with a stable and dominant
organizational culture, which is very slow and of limited adaptability (Walgenbach,
1999). In contrast, clear decision premises are rather combined with a sub-stable
culture, which is more adaptable and able to respond more flexible to changes in
the environment of the organization.
Referred to Kieser a change of organizational culture requires the formulation of
guiding principles, since this makes contours of the organizational culture visible
(Kieser, 1999). To recognize informal premises can interfere the stability of the
organization, because guiding principles are directly related to the interests,
intentions and conflicts of the organizational members (Luhmann, 2000). In this
context, the organizational culture creates the possibility of a comprehensive
organizational change, which simultaneously questions the organizational structure
and leads to a disorientation that “can only be compensated by decisions
successively” (Thiel et al., 2006, p. 32, author’s translation).
The introduced theoretical approach should be transferred to the commercial fitness
gym as a specific organizational type. As already mentioned, commercial fitness
gyms are economic enterprises and act on the basis of the premises of the
economic system with the main goal to maximize profit (Rieger, 2007; Thiel,
1997). Commercial fitness gyms have, like all economic enterprises, a clear
recognizable target structure, which can be differentiated in main goals and
subgoals. This reveals a distinction to voluntary sports clubs. Their target structure
does not show a comparable system, subgoals are difficult to identify. In
commercial fitness gyms explicit guidelines for communication channels prevail,
which were built up on power and hierarchy. While a sports club manager needs a
democratic legitimation for implementing to programmes or hire people (Thiel et
al., 2006), the gym manager can enforce his ideas against employees will. The
communication channels comprise positions, which are filled up with full-time
employees with a professional knowledge. In voluntary sports clubs the recruitment
process is often influenced by private relationship between its members. A fitness

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
57
instructor needs expertise to fulfil his tasks appropriately. All these characteristics
show that commercial fitness gyms have clear defined decidable decision premises
(decision programs, communication channels, human resources). At this point it
can be assumed that commercial fitness gyms are thoroughly adaptable especially
by regarding the organizational culture in combination with the distinct decision
programmes, communication channels and human resources. The premises for
changes of the organizational culture are favourable. Regarding the history of the
commercial fitness market obvious changes in the mission statements have taken
place. Starting with the 80’s the commercial fitness market was primarily
dominated by performance-oriented weight training with a ‘No Pain-No Gain-
Mentality’. During the last fifteen years the mission statements of commercial
fitness gyms have significantly changed in favour of health-oriented statements
(Rieger, 2007; Zarotis et al., 2003). The main reasons for this change are the
diversified market situations. Health-oriented goals play a major part in the motive
structure of gym customers. This key information is selected by the organization
and supports the decision-making process. Commercial fitness gyms are as
economic enterprises directly affected by market influences. It has to be assumed
that it is vital for commercial fitness gyms to react on the motive-related irritations
from the surroundings with a reflection or even a adaption of mission statements,
because a customer orientation gets more and more important as a result of the
intensive competitive situation on the fitness market (Covell et al. 2007; Rieger,
2007; Trillitzsch, 2004). This market orientation implies an adaptable character of
the organizational culture. Furthermore, the risks, which are connected with an
organizational change, are small in economic enterprises, because in commercial
organizations “positions (Stellen) have the responsibility for the maintenance of the
system” (Thiel et al., 2006, p. 33, author’s translation). Each and every day holder
of positions make a contribution for the attainment of the primary organization’s
purpose in the decision-making framework (Japp, 1992).
At this point it is has to be assumed that the organizational culture does not hinder
an organizational change. It is more the decidable decision premises, which are
opposed to a change, especially if it works against the primary organizational
purpose: the maximization of profit. Health-oriented exercise programmes are also
affected. Their implementation is a subject to very tight limits, if they are classified

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
58
as problematic from an economical point of view.
The Implementation of a Health Promotion Orientation
Against the background of the current results commercial fitness gyms are
dynamic, flexible and innovative organizations. Health promotion orientation seems
to be implementable, if it supports the organizational purpose. The organizational
culture appears to be more adaptable than in non-profit-organizations.
In preparation for the empirical analysis the theoretical results should be
summarized relating to Thiel et al. (2006) and be transferred to the decision
problem in commercial fitness gyms whether to implement programmes with a
health promotion orientation or not.
First, it is necessary to place the concrete decision for or against health promotion
programs in the centre of consideration. As decisions are not made independently,
a selection of information takes place, which helps to make the right decision in
relation to the organizational purpose. An orientation towards information like
market developments or demander’s needs is only realizable on the basis of
decision premises.
As an economic organization a commercial fitness gym is marked by organizational
knowledge and a clear defined system of objectives. All decisions derive from the
pressure for economic efficiency. One mentionable example is the realization of
current fitness trends in the product policy, particularly for the group training
offers.13 Programmes, trends and ideas will be connectable in the organization as
long as they make economically sense. Commercial fitness gyms have developed
detailed and fixed rules to secure organizational knowledge. This indicates a major
importance of decision programmes for economic enterprises and hence also for
commercial fitness gyms.
13
Trends in group training are subject to a short product life cycle, so that the returns are also limited to a short period
of time.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
59
As mentioned before, the decision-making structure of commercial fitness gyms is
also influenced by the organizational culture. Due to its concealment it only appears
empirically observable, if the self-conception is scrutinized.
The implementation of exercise programmes, especially by taking quality
management aspects into consideration, is a manifest intervention for the
organization. With regard to the old-fashioned ‘no pain-no gain’-orientation and the
necessity to earn money, the decision whether to implement or not leads to a
reflection of organizational culture and thus to a discussion about self-conception.
The implementation does not end with the decision, if pro or contra health
promotion, because such decisions initiate long-term processes, which could be
undone. For example, the satisfaction of customers is a key aspect. A permanent
dissatisfaction must entail an intervention. Hence, it is possible that specific
exercise programme will be included or excluded.
Derivation of Research Questions
Organizational culture always moves into the foreground, when serious decisions in
organizations – like the implementation of health-oriented exercise programmes –
have to be made. The characterization of decision-making structures in order to
organizational cultural aspects has to be underlined empirically. Therefore, the
made assumptions have to be operationalized. The following questions can be
derived:
Are there characteristics or developments with a special significance?
Which kind of traditions can be identified?
Have there been any changes in the product policy since the opening?
Is the economical development satisfying?
Why are health-oriented exercise programmes offered?
Which significance has health-oriented exercise programmes?
Methodological approach
The aim of the empirical study was not to reproduce a representative illustration of
exercise program offers in commercial fitness gyms, rather than to deeply

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
60
illuminate the organizational cultural premises for the implementation of health
promotion orientation in the form of exercise programs.
For the study in the region East Westphalia/Germany a qualitative empirical design
has been developed, composed of expert interviews and a documentary analysis.
Apart from questions concerning developed values and traditions, purpose and
conditional programmes, personal recruitment and communication channels have
mainly been analysed.
The size of the analysed fitness gyms is between 400 and 1.800 square meters. All
of them have an equipped gym floor, a group training area and a spa. Furthermore,
they offer exercise programmes in cooperation with different health insurances in
the framework of § 20 of the German social security code.
The empirical design consciously relies on a qualitative approach, because it was
necessary to take a ‘deeper look’ into the organizations. It is not possible to ensure
the realization of this requirement with quantitative methods. In total, eleven
owners and managers of commercial fitness gyms have been interviewed (table 7).
All interviews were recorded on a tape and afterwards a transcript was written. The
analysis of information brochures, workout schedules and advertising brochures
completed the empirical design.
Table 7 - Interview Study – Overview
Interview Study
Owners/Managers of Commercial Fitness Gyms
11 Interviews 651 Interview Minutes
(10,85 Interview Hours)
Minimal Length 41 mins Maximal Length 76 mins
Average 59 mins
Qualitative Evaluation
In the beginning of the research study the knowledge about organizational
sociological premises for the implementation of health-oriented exercise
programmes and its actual dissemination in commercial fitness gyms was low and
the need for transparency and information was high. Methods of the qualitative
evaluation research were used to find out the organization-specific reasons if and
why owners and responsible managers decide for or against such an

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
61
implementation.
Qualitative studies do not aim for a representative status, but rather seek for a
detailed acquisition of the subject. A complete survey would only allow a superficial
description of the organizational structure.
Document Analysis
Considering the amount of already existing material like market statistics,
information and advertising brochures, training schedules and anamnesis the
document analysis was integrated into the research design. It supplements the
expert interviews, because of its non-reactive character (Mayring, 2002). The
documents have been collected, analysed and evaluated.
The evaluation of the empirical data was accomplished by using the qualitative
content analysis by Mayring (2003).
Results
It was problematic to illustrate an organizational culture empirically. This is chiefly
due to the fact, that the culture does not appear openly to the outside and works
invisibly (Thiel et al., 2006). Therefore, it was not possible to fall back on a proven
empirical instrument. This deficit was compensated through creating an information
basis about traditions, corporate history and fundamental values with the aim to
illuminate the self-conception and then to derive essential characteristics about the
organizational culture.
Self-Conception of Commercial Fitness Gyms
The commercial fitness gyms chosen for the research had different firm ages. The
oldest provider started in 1977 and the youngest in 2000. Reflecting the different
developments in the histories of the examined providers, it became obvious, that a
rethinking process had taken place, centred on entrepreneurial thinking:
“Formerly, when I started with my gym, I was a sportsman, who had a
gym as a part-time work. And nowadays it is the other way, now I am

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
62
the person, who manages everything and besides I exercise”
(Interviewee 10, p. 7 of transcript, author’s translation).
For the clarification of possible changes in the self-conception interviewees were
asked about the reasons, why they decided for a self-employment in the
commercial fitness market. The majority of respondents referred to the high
identification potential of fitness activities and relativized the necessity of a
professional corporate management during the pioneering days of the commercial
fitness sector. Considering the motives to become self-employed, interviewee No. 7
said:
“Because I am very interested in fitness and I do training. And because I
totally support fitness ... I would not like to sell unhealthy products“
(Interviewee 7, p. 8 of transcript, author’s translation).
A professionalization of operational and sales processes was not relevant in the
past, because “we just opened the gym door and the people came” (Interviewee 9,
p. 2 of transcript, author’s translation). Tendencies toward professionalization in the
commercial fitness industry made a contribution to overcome old and to develop
new mission statements in the related organizations and thus initiated changes in
the self-conception. The importance of commercial interests moves to the
foreground and is directly related to the developments of the market and the
general economic circumstances:
“Right now I think differently, today I do it to earn money ... because I
bear a big risk“ (Interviewee 1, p. 9 of transcript, author’s translation).
Interviewer: “Are you satisfied with the development of your
business?“
Interviewee No. 3: “It could be better. The market situation is a
disaster. Well, when we started ten years ago, we had the biggest gym
here in East-Westphalia and … we were so new, all the other gyms were
hardcore bodybuilding gyms … and afterwards they shot up like
mushrooms … Within one kilometer there are meanwhile seven gyms.“

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
63
Interviewer: „The competitive situation is critical?“
Interviewee No. 3: „It is catastrophic” (Interviewee 3, p. 6 of
transcript, author’s translation).
All corporate histories of the analysed gyms were marked by one specific
characteristic. Radical market-related changes led to so far not necessary adaptions
in strategic marketing, because “you have to make more serious efforts, more
marketing, more advertising campaigns, you need more innovative ideas to even
make the people come to the gym” (Interviewee 9, p. 10 of transcript, author’s
translation). Main reason for these adaptions was mostly the dramatic development
of the cost situation, which should be compensated by focusing on sales activities:
“Because of the costs, which occurred for example through the state you
can recognize that you need nearly fifty members more per year to
generate the same profit and that frightens me” (Interviewee 8, p. 12 of
transcript, author’s translation).
These reactions to influences indicate a change in the self-conception. Due to the
empirical material a development from idealistic to service-oriented organizations
has taken place. Evidences can be found in numerous interview sections and
documents:
“Of course you have to balance, what the prospective customer wants.
For somebody how wants to take part in a group workout or to train his
endurance, it is not useful to offer a preventive back training. You can
offer, but you have to listen carefully, what the people want. You must
be customer-oriented in that moment” (Interviewee 7, p. 2 of transcript,
author’s translation).
“How did you find about us? Why do you start with exercising? Which
wishes do you have, which exercise goals do you want to achieve?
Which body parts do you want to train? What do you think how long you
have to exercise to achieve your goals?” (Anamnestic Questionnaire
Gym 2, p. 1, author’s translation).

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
64
Aspects of customer orientation become more and more important, but are not
internalized by all organizations:
Interviewer: “A prospective consumer subscribes a member. What
comes next?”
Interviewee 4: “Health check consisting of body fat measurement, blood
pressure measurement, mobility test, endurance test, a complete
anamnesis … including health problems, sport-related experience, goals,
possible training frequency, surgeries, chronic diseases like
osteoporosis, rheumatism … acute symptoms” (Interviewee 4, p. 12 of
transcript, author’s translation).
A comprehensive training guidance and assistance at the beginning of a gym
membership is an indication of professionalism, but this does not necessarily mean
customer orientation as well, because the quantity and quality of this process
should be related to customers’ needs. During the interviews it became apparent,
that the product orientation overlaps the customer orientation. This attitude is
latently based on existing idealistic influences and is represented in the
understanding of quality:
„Well, at least we are committed to fitness with high standard, that
simply means quality of guidance and assistance. People do not come
here just for fun, we accomplish a complete health check, which is also
offered by other gyms, but the important question is always: What is
behind? How much know-how is behind that” (Interviewee 4, p. 5 of
transcript, author’s translation).
Summarizing the results for the self-conception of commercial fitness gyms it is
obvious, that a professionalization process has taken place, which is accompanied
by a change of self-conception. They understand themselves as qualitative sport
service suppliers. The decipherment of the term quality occurs differently. While
some suppliers equate quality with product orientation, others realized the
necessity of customer orientation and set up their processes accordingly. In the
opinion of the interviewed managers professionalism and quality are directly

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
65
connected to the implementation of exercising programs. How far this appreciation
has been strengthened in the organizations should be shown in the following.
Organizational Culture and Health Promotion
The empirical results revealed a high willingness to change the range of offered
services. This seems to indicate minor barriers for the implementation of exercising
programmes with a health promotion orientation. The majority of respondents see
economic advantages in relation to exercising programmes and services:
„In the past people mainly joined a fitness gym with the motive to build
muscles. Things have changed dramatically. People go to a fitness gym
to stay healthy, to strengthen their back, to improve their motor
function and their endurance“ (Interviewee 6, p. 1 of transcript, author’s
translation).
Advantages of a specialization in exercising result from the
„activities of the health insurances, who permanently push that topic
into the foreground, it becomes more and more important in people’s
perception. And the grants ... which are offered by the insurances are
very attractive for the members“ (Interviewee 6, p. 1 of transcript,
author’s translation).
These prejudices necessarily result in a more health-oriented supply, because there
is a durable necessity for the supplier, to orientate himself according to the
demanders’ requirements. The necessity is even existential according to this
statement:
“I believe that if we did not have these health promoting offers: Would
we still be there? Probably not. Therefore it is clear according to the
market position, also the realm of interests, but mostly the market
position. We have to position ourselves in that scope and in our case
that is especially the health sector. In other gyms, they just got fitness
and strength training, nothing concerned with health” (Interviewee 3, p.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
66
14 of transcript, author’s translation).
Within the theoretical considerations of this article, it was already mentioned that
decision programmes, communication channels and the staff take a commanding
appointment. Therefore, it is possible to implement programmes which help to
achieve the primary organizational purpose. Furthermore, it was possible to
ascertain a transformation towards professionalization of the management in the
last subchapter. In what way does a strength training oriented culture affect the
necessity to differentiate health offers? The values, according to how a gym was
controlled and supplied his products, haven’t been marked with health-related
issues in the earlier years, because
“twenty years ago, one left the roots of bodybuilding and it was all
about beauty and gaining muscles…about a complete new kind of sport
in general” (Interviewee 11, p.1 of transcript, author’s translation).
This change is also recognizable because of the change and the restructuring of
technical equipment:
“Well, concerning the equipment you can say that at the beginning there
was an upright bike, but no courses. It was quite small at the beginning,
but over the years, the cardio area was remarkably expanded and
professionalized. Meanwhile, we own more than 40 pieces of cardio
equipment” (Interviewee 10, p. 5 of transcript, author’s translation).
The organizational culture is expressed intensely, if, for instance, conflicts
concerning the implementation of innovative programmes occur or not occur. There
is no controversy arising at the explanation of the empirical material; a health
oriented reorientation was conflict-free completed. The commercial attractiveness is
too dominant:
“Primarily it is of course the commercial aspect, we started to question
ourselves, what we can still do with our grounds? We have got a lot of
customers…and we believe that we are able to attach even more customers
because of the health oriented sector of sports and fitness” (Interviewee 6.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
67
p. 7 of transcript, author’s translation).
Demand satisfactory innovations are connectable without internal conflicts.
Organizational culture does not develop a defense mechanism in order to prevent
such an implementation.
But in what case does such a defense mechanism get promoted? At all times, if the
commercial traceability of certain supplies or structures is questioned because of
indirectly caused impacts (Thiel et al. 2006, p. 41). An Important achievement of
the empirical investigation was the fact, that health promoting exercise
programmes frequently go hand in hand with the necessity of orienting towards
quality.
“In my opinion it will be further important to provide quality in the
fitness sector. The members and new members should say: Oh yeah,
right here we are treated like human beings. There is a certain quality”
(Interviewee 5, p. 24 of transcript, author’s translation).
An investment in quality does not mean to underestimate the investments
according to the declarations of the operators; especially if it is about certification
of offers by external institutions or associations:
“Each seal is not recognized by everybody. If it was about that, you
were ought to own a lot of seals and that is a matter of money. It is
very expensive and it has to be re-examined every year. And every year
you have to pay it again” (Interviewee 3, p. 12 of transcript, author’s
translation).
Within a difficult business situation, the question arises, to what extent,
organizational culture is impeding the continuation of expensive programmes. As a
result of cost reduction, it would not be possible to fulfill the quality requirements,
which health programmes are ought to have, “because if you reduce the costs,
quality is suffering as well” (Interviewee 1, p. 8 of transcript, author’s translation).
Similar arguments can be found in the following statements:
“Like in every company, you would act then and emphasize different

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
68
aspects that would be more interesting under an economical view”
(Interviewee 7, p. 15 of transcript, author’s translation)
Question: “Would you release cost intensive staff?”
Interviewee 6: “Sure, we already did that in the last years. As I told
you, we now have got only one certainly employed and
four temporary employed people in the gym”
(Interviewee 6, p. 14 of transcript, author’s translation).
Organizational culture operates in stages of economical problems. Commercial
conditioned incisions in quality of health promoting offers can be completed without
conflicts, although the suppliers act as quality-oriented exercise service providers in
the external image.14
Conclusion
Decision-making processes in commercial gyms are influenced by their
organizational culture. Models of mutability and resistance depend on organizational
culture to a certain extent. This is the case by regarding the question if and to what
extent decision-making processes can be kicked off, which are not fitting to the
self-image of an organization, but are important for change processes.
The decision for expansion of the health-oriented service spectrum follows a
previous modification. As a result of intensification of competitive situations, such
strategic options gradually got access to the facilities that were no longer idealistic
marked, but were distinguished by a strict economical character. In this context,
this can be named as a pressure of professionalization. According to the empirical
material, we can determine a transformation from idealism to market orientation.
Not every changing process necessarily has to go hand in hand with a change in
self-understanding. A specialization in the health sector leads to a modification of
the spectrum of supply, communication and in the personal structure, because a
health promoting programme is oriented towards the fitness demanders. Therefore,
no organizational change has to be done. Because of their merchantability and the
14
One supplier even changed his corporate slogan from “Where fitness is fun” into “Where health is fun”.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
69
public acceptance, health promoting offers refer to the identity of commercial
gyms. If gyms experience economic trouble despite professionalized health
orientation, conflicts would appear. The maintenance of a necessary level of quality
requires enormous financial efforts and money that is probably not available to that
extent. Expensive health programmes as profit generating products are inevitably
questioned and other options, such as discount strategies become connectable.
References
1. Baur, J. & Braun, S. (2003). (Eds.). Integrationsleistungen von Sportvereinen als Freiwilligenorganisationen. Aachen: Meyer & Meyer.
2. Bouchard, C., Blair, S. & Haskell, W. (2006). Physical Activity and Health. Champaign: Human Kinetics.
3. Brehm, W. (1997). Qualitäten im Gesundheitssport. In H.-J. Schulke, J. von Troschke & A. Hoffmann (Eds.), Gesundheitssport und Public Health (Schriftenreihe der ‚Deutschen Koordinierungsstelle für Gesundheitswissenschaften’, 7, pp. 46-59). Freiburg: Deutsche Koordinierungsstelle für Gesundheitswissenschaften.
4. Brehm, W. (1998). Qualität und deren Sicherung im Gesundheitssport. In A. Rütten (Eds.), Public Health und Sport (pp. 181-202). Stuttgart: Naglschmid.
5. Covell, D., Walker, S., Siciliano, J. & Hess, P. (2007). Managing Sports Organizations (2nd ed.). Burlington: Butterworth-Heinemann.
6. Deloitte & EuropeActive (2016). European Health & Fitness Market Report. Düsseldorf: Deloitte. 7. Dietrich, K., Heinemann, K. & Schubert, M. (1990). Kommerzielle Sportanbieter. Schorndorf:
Hofmann. 8. Dreßler, W. (2003). Angebot und Nutzerstrukturen bei kommerziellen Fitnessstudios – eine
soziologisch-empirische Untersuchung in Fitnessstudios und Sportvereinen in der Stadt Viersen. Retrieved June 15, 2010 from http://docserv.uni-duesseldorf.de/servlets/DerivateServlet/Derivate-2542/542.pdf
9. Eigenmann, P. (2004). Gütesiegel und Qualitätslabel – unerlässlich oder nutzlos? Fitness Tribune, 16 (3), 90-91.
10. Emrich, E. (2005). Organisationstheoretische Besonderheiten des Sports. In C. Breuer & A. Thiel (Eds.), Handbuch Sportmanagement (pp. 95-113). Schorndorf: Hofmann.
11. Emrich, E., Pitsch, W. & Papathanassiou, V. (2001). Die Sportvereine. Ein Versuch auf empirischer
Grundlage. Schorndorf: Hofmann. 12. Heinemann, K. & Schubert, M. (1990). Haben Fitnessstudios eine Zukunft? In H.G. Ilker & M.
Ramme (Eds.), Fitnessstudio im Verein (pp. 22-47). Hamburg: Czwalina. 13. Janssen, J.P., Wegner, M. & Beyer, H. (1989). Einstellungen und Interessen zum Sport bei
Mitgliedern von Sportvereinen und Fitness-Centern. In H. Eberspächer & D. Hackfort (Eds.), Entwicklungsfelder der Sportpsychologie (pp. 293-298). Köln: bps-Verlag.
14. Japp, K.P. (1992). Selbstverstärkungseffekte riskanter Entscheidungen. Zur Unterscheidung von Rationalität und Risiko. Zeitschrift für Soziologie, 21 (1), 31-48.
15. Kieser, A. (1999). Konstruktivistische Ansätze. In A. Kieser (Hrsg.), Organisationstheorien (3. Aufl., S. 287-318). Stuttgart, Berlin, Köln: Kohlhammer.
16. Kosinski, T. & Schubert, M. (1989). Kommerzielle Sportanbieter. In K. Dietrich & K. Heinemann (Eds.), Der nicht-sportliche Sport (pp. 139-149). Schorndorf: Hofmann.
17. Luhmann, N. (1988). Organisationen. In W. Küpper & G. Ortmann (Eds.), Mikropolitik, Rationalität, Macht und Spiele in Organisationen (pp. 165-185). Opladen: Leske & Budrich.
18. Luhmann, N. (2000). Organisation und Entscheidung. Opladen: Westdeutscher Verlag. 19. Mayring, P. (2002). Einführung in die qualitative Sozialforschung (5th ed). Weinheim: Beltz. 20. Mrazek, J. (1988). Fitness-Studio und Sportverein als konkurrierende Modelle. Brennpunkte der
Sportwissenschaft, 2 (2), 189-203. 21. Rampf, J. (1998). Drop Out und Bindung im Fitnesssport. Hamburg: Czwalina. 22. Rieger, T. (2007). Qualitätsmanagement der Gesundheitsförderung bei kommerziellen
Fitnesssportanbietern – Voraussetzungen und Barrieren einer Implementierung. Hamburg: Verlag Dr. Kovac.
23. Sack, H.G. & Hennrich, R. (1989). Kommerzielle Sporteinrichtungen in Berlin (West) – Angebote,

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
70
Nutzung, Stellenwert. Berlin: Institut für Sportwissenschaft der Freien Universität Berlin. 24. Schubert, M. (1998). Zur Nachfragestruktur in kommerziellen Fitnessanlagen. Ergebnisse einer
empirischen Untersuchung. Hamburg: SSV-Verlag. 25. Thiel, A. & Mayer, J. (2009). Characteristics of Voluntary Sports Club Management: a Sociological
Perspective. European Sport Management Quarterly, 9 (1), 81-98. 26. Thiel, A. & Meier, H. (2004). Überleben durch Abwehr – Zur Lernfähigkeit des Sportvereins. Sport
und Gesellschaft, 1, 103-124. 27. Thiel, A. (1997). Steuerung im organisierten Sport. Ansätze und Perspektiven. Stuttgart:
Naglschmid. 28. Trillitzsch, M. (2004). Die Entwicklung des kommerziellen Sportanbietermarkts in Ostdeutschland –
Eine Untersuchung aus modernisierungs- und transformationstheoretischer Perspektive. Hamburg: Verlag Dr. Kovac.
29. Walgenbach, P. (1999). Institutionalistische Ansätze in der Organisationstheorie. In A. Kieser (Ed.), Organisationstheorien (pp. 319-353). Stuttgart, Berlin, Köln: Kohlhammer (3. Aufl.).
30. Zarotis, G.F., Athanailidis, I., Tosunidis, A., Katsagolis, A. & Lagerström, D. (2003). Geschichte und Zukunft des Fitness-Sport. Gesundheitssport und Sporttherapie, 19, 15-18.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
71
6 - ORIGINAL RESEARCH: How exercising women feel about
their bodies and behave in fitness club environment? [Simona
Pajaujiene]
Simona Pajaujiene15
15Lithuanian Sports University. Lithuania, ActiveTraining – Training provider,
Lithuania. EuropeActive – Professional Standards Committee.
E-mail: [email protected]
Abstract: Girls and women receive constant messages from their social (including fitness)
environment that a thin physique is very attractive. Given increasing public health concerns regarding
low rates of physical activity and prevalence of unhealthy eating and exercising habits, research is
needed to better understand the psychosocial factors which influence exercise participation or resistance
to exercise. The aim of the study was to reveal how exercising women feel and behave in fitness clubs
environment. The research has suggested that women are negatively impacted by the constant pressure
of cultural messages that imply that the female body is a public domain for all evaluate and to
“consume”. Many women were dissatisfied with body weight and chose leisure physical activity for the
weight reduction and figure improvement reasons. The obligatory exercising is featured by the women in
fitness clubs. A large part of participants exercise despite illness or injury for fear to miss training
session. More than half of women dramatically worried about their figures and even feared of other
people opinions about it. These emotional state and behavior can lead to unpleasant experiences during
exercise in fitness environment and decrease the adherence rates. Understanding the factors which
foster negative emotions and unhealthy behaviours of women exercising in fitness centres is important
for health educators and exercise professionals.
Key-words: body image, women, fitness environment, weight loss, exercise
15
Simona Pajaujien, 1970, Kaunas, Lithuania. She has been involved in fitness training, exercise for health and fitness education for over 25 years and currently works as trainer, group fitness instructor, educator, speaker, author and technical expert. She is a lecturer and coordinator for several study programmes at the Lithuanian Sports University since 2004. Research interest: Health Education; Body Image in Sport and Leisure Physical Activity; Weight Control and Exercising Behaviour. She is a program director and founder of accredited vocational training school - ActiveTraining. Member of Professional Standards Committee – EuropeActive. Qualifications: BSc in Sport Sciences (1995); MSc in Public Health – Health and Fitness (2004); PhD in Social Science – Sports Science and Education (2012). More info: ResearchGate LinkedIn

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
72
Introduction
With the prevalence of body cult in the Western society, more and more people feel
pressure to conform to social expectations. Media constantly is bombarding with
the messages how to be fit (thin or muscular), nice and forever young. Therefore,
for many people leisure sports become means to acquire a desired body. In other
words, in consumer society Health becomes an alibi for improving Appearance [1].
The global pandemic of obesity is unquestionable truth with evidence [2], but in
addition another great concern is huge dissatisfaction with own bodies, depression,
anxiety, low self-esteem, unhealthy weight lose behavior, disordered eating, etc.
[3].
There is a big increase of leisure sports facilities across the Europe and especially in
health and fitness sector [4]. Paradoxically, but the increase in facilities that offer
spaces and services related to physical exercise and sports activities was
accompanied by a significant increase in obesity and a sedentary lifestyle [5].
Research suggests that 50% of persons starting an exercise program will drop out
within the first 6 months [6]. A person with low self-worth (i.e., self-doubt,
insecure, negative self-talk) and poor body image is more likely to be an exercise
dropout [7]. Therefore, given increasing public health concerns regarding low rates
of physical activity and prevalence of unhealthy eating habits, research is needed to
better understand the psychosocial factors which influence exercise participation or
resistance to exercise.
So the questions could be raised: Do we know how people feel in the fitness
environment? What are their expectations and behavior? Can exercise professionals
do some harm to customers putting too much emphasis on body and appearance?
Fitness clubs create an atmosphere in which the appearance is in the spotlight. As
usual the fitness environment contains a large number of clearly objectifying
features for people: multiple full-length mirrors, posters that idealize the body, the
opportunity for direct comparison with nice looking fitness instructors and other
participants, tight and revealing (lycra) exercise clothing, etc. People exercising in
fitness centres are observed to raise significant requirements for their appearance,
and sometimes have inadequate body weight perception [8]. Critical comments

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
73
from teacher or trainer can be one of the most patent risk factors for developing
eating disorders [9]. A substantial body of evidence demonstrates that the
excessive emphasis on fitness, incorrect behaviour of trainers, and the environment
of fitness clubs may promote a number of negative consequences. The pursuit of
physical perfection can lead to pathological behavior and poor psychological state
(figure 3).
Figure 3 - Hypothetical links between fitness environment, the pursuit of physical
perfection and negative outcomes.
The researches show that psychological factors play a crucial role in adherence to
physical activity, exercise and fitness [7, 10]. Fitness environment may promote
negative emotions towards own body, and compensatory behaviours after missed
workout session, which can become one of the risk factors of psychological health.
Studies show that exercisers’ body image is an important factor associated with
wellbeing, exercise motivation and specific exercise–related behaviour [11].
Although appearance improvement is the strong driving force for the health and
fitness industry, we lack the millions of men and women in exercise sector. If our
goal is to make Europe more active, we should discuss what could be barriers and
obstacles for that. The analysis of factors which might influence exercise adherence
is an important issue for physical activity promotion.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
74
The aim of the study is to reveal how women involved in recreational physical
activity feel and behave in fitness clubs environment and identify the links between
the fitness environment and the attitude and behaviour of exercising women.
Methods
Participants
The study sample consisted of 287 Lithuanian women involved in recreational
physical activity in fitness clubs. The sample was selected using a random cluster
sampling approach, i.e. selecting one group of exercising women from each club.
The mean age of the sample was 29.4 years (SD=9). Most of the women were
exercising for figure improvement reason (39.7%), 3-4 times a week (63.1%) for
more than 2 years (46.7%). 39% of women were engaged only in aerobics groups,
33.1% - in GYM, 27.9% combined both types of sports.
Instrument
The attitude of participating women to behavior related to weight loss was
evaluated according to our 41-item questionnaire consisting of variables as weight-
related body image (accuracy of perception of body weight, attitude towards value
of slimness, weight control concerns, current attempts to lose weight, emotions
related to weight control), exercise motivation and obligatory motivation to
exercise, instructor’s encouragement to go on a diet. Internal consistency of the
questionnaire was satisfactory (Cronbach α was 0.7). Test-retest reliability was 0.8
after a 2-week interval of retesting.
Results
Mean BMI of the sample was 21.8±2.9 kg/m² (16.4-36.5 kg/m²). The majority of
the women were normal weight (n=222, 77.4%), 13 (4.5%) were underweight, 52
(18%) - overweight. Despite the fact that majority had normal body weight as
much as 217 (64.4%) women expressed weight dissatisfaction. The majority of
body weight dissatisfied women were in the overweight group, however even
59.9% of women with normal BMI were dissatisfied with body weight too

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
75
(χ²=32.936, df=2, p=0.000). Perhaps this is why most of the women were
exercising for figure improvement reason (39.7%) and 75.3% sought to reduce
their body weight. The most satisfied with body weight were underweight women,
but even 10% of them desired to lose a few kilograms (figure 4).
Figure 4 - Distribution of desirable body weight among BMI groups (χ2=228.3;
df=12, p=0.000).
A significant number of women admitted that slimness and physical attractiveness
are very important life factors, which can determine their career and relationships.
In addition, many women (57.8%) dramatically worried about their figures and
even feared of other people opinions about it. Slimness as a value was very
relevant among overweight and body weight dissatisfied women (p<0.001). These
women also expressed significantly more anxiety and depressive mood about their
figure and weight control when joined fitness club. It is important to highlight that
exercise motivation to improve figure were significantly related with all mentioned
feeling and attitudes (table 8).
Logistic regression analysis confirmed that women with the highest BMI most of all
associated physical attractiveness with body weight. They 2.5 times more as others
confirmed the value of body weight on attractiveness (95% CI: 1.09-5.93) and
even four times as often tended to admit that their achievements in life would have
been greater if they had been thinner (95% CI: 1.97-9.76). Reasons for exercise
were also associated with the drive to lose weight. Women who started exercising
5
33.3
100
10
70.8
61.1
70
22.7
5.6 20
1.5
<18.5 18.5-24.9 24.9-29.9 >29.9
%
Want to gain some weight
Satisfied with body weight
Want to lose a few kg
Wish to lose 10 kg

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
76
for other than health reasons, twice as often admitted that they had obsessive
thoughts about weight control (95% CI: 1.11-3,.), more than twice as often felt
guilty about weight gain (95% CI: 1.43-4.89).
Table 8 - Women`s opinion about value of slimness in life, attitude to their body
and emotional expression in fitness environment by BMI, body weight satisfaction
and motivation groups (%).
Variables
N (%)
Conviction that physica
l
attra
ctiv
eness
depends
on
body w
eig
ht
Conviction that gener
al s
ucc
ess in
life
dep
ends on slim
nes
s
Anxie
ty, depre
ssiv
e m
oods
and
fears
conce
rnin
g o
thers
opin
ions
about th
e fig
ure
Obse
ssio
n w
ith w
eig
ht co
ntrol
when jo
ined fitness
tra
inin
g
The
imag
es in m
irrors
cause
neg
ativ
e em
otio
ns re
gar
ding their
bodies
Com
par
ed their bodies to
the
bodies of o
ther
exe
rcising w
om
en,
and fe
lt th
emse
lves infe
rior
Avo
ids cloth
ing e
mphas
ising their
body
shap
e during sports
%
60.3 44.1 57.8 45.6 90.6 47 29.3
BMI
Underweight
Normal
Overweight
13 (4.5)
222 (77.4)
52 (18)
61.5
55
82.7*
7.7
37.8
80.4**
30.8
55.9
74.5**
15.4
45.5
54.9**
69.2
90.5
96.1*
15.4
41.9
75**
7.7
26.1
48.1**
Attitude to the body weight
Body satisfied
Body dissatisfied
104 (36.2)
183 (63.8)
47.1
67.8**
14.4
61**
36.5
70.3*
21.2
59.9*
76.9
98.4**
18.3
62.8**
15.4
37.2**
Reasons for exercise
Enjoyment
Figure improvement
Health and fitness
78 (27.2)
114 (39.7)
95 (33.1)
47.4
75.4**
52.6
34.6
54.4*
39.4
44.9
74.6**
48.9
28.2
71.1**
29.8
85.9
98.2**
85.1
44.9
61.4**
30.5
17.9
40.4*
25.3
* p<0.05; ** p<0.001
The participants were asked to assess how they feel in a fitness environment.
Results showed that the images in mirrors cause negative emotions for the majority
(90.6%) of women regarding their bodies, 47% compared their bodies to the
bodies of other participants, and felt themselves inferior, therefore, one-third of
women (29.3%) avoids clothing emphasizing their body shape during sports. These
emotions were significantly more expressed among women with higher BMI,

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
77
dissatisfied with own body weight, and exercising for figure improvement reason
(table 8). Interesting, but age was not related to these feelings (p>0.05).
The study revealed that 15.5% of women for weight loss reason reported using
unhealthy weight reduction behaviour (starvation, smoke, use laxatives, diuretics,
diet pills, vomiting, etc.), which is the most evidence in group of dissatisfied with
their body weight women comparing with satisfied participants (81.4% versus
18.6%; χ2=6.03; df=1, p=0.014). This unhealthy practice was also related to
exercise motivation: more women exercising for figure improvement reason
demonstrated this behaviour comparing with women exercising for enjoyment and
health reasons (accordingly 21.9%, 14.9% and 7.9%; χ2=7.57, df=2, p=0.023).
BMI and age were not related to unhealthy behavior (p>0.05).
Dieting is quite widespread among in fitness activity involved women. Our study
found that nearly half of participants (42.7%) practiced frequent and constant
dieting, 41.8% - admitted overeating behavior followed by negative emotion and
feelings of guilt. 8% of women experienced binge eating followed by compensatory
behaviors ( a symptom of bulimia nervosa).
We considered the role of fitness instructor as the most significant factor of fitness
environment. 65.5% of women admitted that instructor is continuously explaining
how to reduce the amount of body fat, and 23% of women were proposed by the
trainer to go on a diet and to use slimming food supplements. Logistic regression
analysis confirmed that instructor`s recommendation to go on a diet and advised
slimming food supplements has a significant influence on physically active
women`s desire to lose weight: they twice as often reported frequent and constant
dieting (95% CI: 1.21-4.26), twice as often displayed overeating behaviour (95%
CI: 1.08-4.08).
In our study large part of women experienced different characteristics related to
the concern and obligatory exercising behaviour. Concern about body image forced
to exercise 87% of women and this emotion was more expressed in groups of
overweight, body dissatisfied, and women exercising for figure improvement

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
78
reason. Fear that without exercising they will gain weight expressed half of the
women (50.9%). The most women with this fear were in dissatisfied with body
weight (p<0.001) and figure improvement (p<0.001) groups. Exercising despite
illness or injury to fear to miss training session confirmed 35.7% of women. It was
significantly more popular among women with normal BMI (p<0.05). After missed
training session 43.6% of participants feel guilty and other depressive feelings.
Surprisingly, but it was more expressed in underweight women group (p<0.05).
These feelings also were more common for body dissatisfied (p<0.05) and
exercising for figure improvement (p<0.001) women (table 9).
Table 9 - Women`s concerns and behaviors in view of obligatory exercising by BMI,
body weight satisfaction, motivation and instructor’s influence groups (%).
Variables
Conce
rn a
bout body
imag
e fo
rce
to e
xerc
ise
Fear
s th
at w
ithout
exer
cising the
body
weight will
gain
Exe
rcising d
espite
illness
or inju
ry fo
r fe
ar
to m
iss training ses
sion
After
a m
isse
d tra
ining
sess
ion fe
el g
uilty,
anxiety
, dep
ress
ion
Com
pen
sato
ry
beh
aviours
after
misse
d
training
%
87.1 50.9 35.7 43.6 40
BMI
Underweight
Normal
Overweight
84.6
85.1
96.2*
30.8
50
59.6
7.7
39.4*
26.9
69.2*
45.5
28.8
38.5
40.1
40.4
Reasons for exercise
Enjoyment
Figure improvement
Health and fitness
75.6
97.4**
84.2
41
65.8**
41.1
33.3
31.6
42.6
42.3
68.4**
53.7
38.5
47.4
32.6
Attitude to the body weight
Body satisfied
Body dissatisfied
77.9
92.3*
37.5
58.5**
42.7
31.7
44.2
63.4*
26.9
47.5**
Women received instructor’s encouragement for
diet and supplements
Yes
No
89.4
86.4
71.2**
44.8
30.3
37.3
68.2*
52.9
54.5*
35.7
* p<0.05; ** p<0.001

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
79
40% of exercising women reported that after a missed training session they take
compensatory actions. The most popular compensatory behaviours after missed
training were limiting food consumption (16.7%) and exercising more intensively
and longer during the next workout (23.3%). BMI, exercise motivation, body
weight evaluation, age were not significantly related to compensatory strategy.
However, the women with the highest BMI “punish” themselves by limiting food,
whereas women with normal BMI exercise for longer periods, and more intensively
during the next workout session (χ=17,86; df=6; p=0.007). Instructor’s
encouragement to go on a diet and use slimming supplements was also related to
the women’s concern and obligatory exercising behaviour. Women with instructor
influence significantly more often expressed the fear that without exercising body
weight will gain (p<0.001), feelings of guilt, depression after a missed training
(p<0.05) and compensatory actions after missed training (p<0.05).
Discussion
Our research has suggested that women are negatively impacted by the constant
pressure of cultural messages that imply that the female body is a public domain
for all evaluate and to “consume”. Many women (even with normal BMI) were
dissatisfied with body weight and chose leisure physical activity for the weight
reduction reasons. More than half of women dramatically worried about their
figures and even feared of other people opinions about it. This emotional state can
lead to unpleasant experiences during exercise in a fitness environment.
Truth be told, many persons are so ashamed of the way they look that they
don’t even want to be seen in public exercising. Because cultural standards for
the feminine beauty are impossible to realize fully, women, who internalize them,
feel shame. This shame is not simply negative feelings about the body, but about
the self [12]. In our study the most negative emotions and the biggest influence of
fitness environment felt overweight women. These results are similar to others
studies where was confirmed that overweight / obese people suffer from
psychosocial stress caused by social pressure to lose weight, have low self-esteem,
are often dieting, are more likely to get depression compared to their peers with

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
80
normal weight [8, 12-13].
Motivation to exercise was very important factor in our research. It was revealed
that women with figure improvement motivation have the most negative attitude to
their body, emotional expression (concern, anxiety, fear, depressive mood) and
compensatory behaviour. Other studies also confirm that exercising for weight
control, body tone, and attractiveness has been associated with increased negative
feelings and outcomes as body dissatisfaction, eating disorders, and lower body
esteem [14]. Thus, exercising motivation related to body shape
improvement can be one of the precursors of problematic body image. It
should be noted that body image concerns are associated with extrinsic exercise
goals particularly with exercising for appearance improvement [14-15]. Self-
determination theory [16], suggests that in exercise domain people pursuing health
and social engagement goals will be more persistent and experience greater well-
being than those pursuing attractiveness or social recognition goals.
The results of our research contribute that part of women in fitness clubs use
unhealthy weight control methods, have overeating and body dissatisfaction
problems. The combination of these factors can lead to overweight, obesity or even
eating disorders [17]. Although many countries have obesity problems, most
attempts to lose weight and go on a diet are made by people of normal weight. The
study revealed that women’s ambition to reduce weight was mostly related not with
the current body weight, but with the belief that they weigh too much. Unhealthy
weight loss behaviors were the most prevalent in body dissatisfied and exercising
for appearance improving women’s group.
The role of the trainer is very important for exercising participants. Instructor`s
recommendation to go on a diet and advised slimming food supplements has a
significant influence on physically active women`s desire to lose weight. The use of
various supplements has become a meaningful part of the fitness culture.
Exercisers’ body image concerns, especially extreme weight and shape controlling
behaviors, were associated with the use of so-called “appearance and performance
enhancing drugs” [18]. Many fitness clubs additionally profit from the sale of food

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
81
supplements, so in this way, trainers are encouraged to be active sellers.
It was revealed that the obligatory exercising is featured by our women in fitness
clubs. A large part of women exercise despite illness or injury for fear to miss a
training session. What does it mean? Researches point out that the time spent
exercising within the fitness centre environment was more highly related to body
image and eating disorders than time spent exercising outside of the fitness centre
environment [14]. Thus, a problematic question remains relevant: is the weight
loss behavior among physically active women induced by the fitness environment
or do they join fitness clubs already being dissatisfied with their body weight? It
should be noted that the usual fitness environment raises the positive emotions and
long-term internal motivation not for everybody. If we want to attract more people
to be more active we have to realize that many people are obese, dissatisfied with
their bodies and with sensitive emotional experiences associated with their bodies.
Weight loss should not always be the primary goal of fitness training. In the most
cases the goal is the overall health – wellbeing, life quality and chronic disease
prevention. The benefits of physical activity are huge [19] and therefore, they
should not be narrowed to the body weight control or figure improvement.
The overview of the study suggests that Lithuanians still do not give adequate
priority for physical activity. Furthermore, they have a wrong imagination about
weight control and exercising behavior. It is also a lack of experience, skills and
knowledge about the health promotion through physical activity and healthy
lifestyle. It is clear that recognition of fitness sector requires a systematic,
multistage and cross-sectional approach to promoting behavioral change, a new
understanding of what it means to be "fit "and what to expect from the trainer as
well as fitness services, promote the political, social, and environmental changes.
Necessary dialogue across different stakeholder communities about the way in
which exercise professionals might be better to meet growing societal need and
expectations place upon them.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
82
Conclusions
Fitness environment may promote negative emotions towards own body, unhealthy
exercising and weight loss behavior among women. The biggest influence of fitness
environment felt overweight women. The strongest predictors of weight loss
behavior among women exercising in fitness clubs were: body dissatisfaction,
exercise motivation for appearance reason, instructor`s encouragement to go on a
diet and use slimming supplements.
Practical applications
The training environment affects the behaviour of women, and their attitude
to their bodies. Fitness centers should avoid an intensive demonstration of
lean and/or muscular body images and control other factors (i.e., mirrored
walls, advertising) which might foster external motivation in fitness
exercisers of both genders.
Health educators and exercise promoters should make more efforts
changing perceptions of competence by shifting focus from body weight
control to overall feelings of interest and enjoyment. They have client focus
on his/her personal accomplishments and not compare herself/himself to
others.
Educators, coaches, teachers should stop the negative messages about the
bodies and identify the individuality and uniqueness.
Body weight does not reflect the physical condition and physical fitness, thus
unreasonable weight control can cause various health problems.
It is recommended to avoid too frequent and public weighing procedures
and criticism related to body weight and shape. Comments made and
attitudes displayed can have an impact on a person's body image and
attitude towards exercise and eating.
It is important to direct the basic information about nutrition and weight
control for all participants, not just for persons who are overweight.
Educators should focus on the client education on the many health and
lifestyle benefits of exercise, not on weight, and avoid to provide
unsubstantiated information.
Exercise professionals should be more responsible and consider the

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
83
behaviour of women weight loss, preventing the sports of turning into
excessive exercising or addiction.
Is important to note that negative self-esteem or body dissatisfaction does
not develop healthy weight control behaviours, but rather predicts such
behaviour, which can lead to the risk of obesity, eating disorders and lower
health in general.
References
1. Maquire, J. S. (2001). Fit and flexible: The fitness industry, personal trainers and emotional service labour. Journal of Sport and Social, 18, 379–402.
2. Dumith, S. C., Ramires, V. V., Souza, M. A., et al. (2010). Overweight / obesity and physical fitness among children and adolescents. Journal of Physical Activity and Health, 7, 641–648.
3. Sanchez-Carracedo, D., Neumark-Sztainer, D, Lopez-Guimera, G. (2012). Integrated prevention of obesity and eating disorders: barriers, developments and opportunities. Public Health Nutrition, 15(12):2295-309.
4. EuropeActive & Deloitte (2016). European Health and Fitness Market Report 2016. Duesseldorf: Deloitte.
5. Swift, L.D., Johannsen, N.M., Lavie, C.J., et al. (2014). The Role of Exercise and Physical Activity in Weight Loss and Maintenance. Obesity and Obesity Paradox in Cardiovascular Diseases. Progress in Cardiovascular Diseases, 56 (4):441–447.
6. Wilson, K., Brookfield, D. (2009). Effect of goal setting on motivation and adherence in a six-week exercise program. International Journal of Sport and Exercise Physiology, 6, 89-100.
7. Huberty, J.L., Ransdell, L.B., Sigman, C., Flohr, J.A., Schult, B., Grosshans, O., and Durrant, L. (2008). Explaining long-term exercise adherence in women who complete a structured exercise program. Research Quarterly for Exercise and Sport, 79(3), 374-384.
8. Pajaujienė, S. (2009). Kaip sveikatingumo klubų aplinkoje jaučiasi ir elgiasi laisvalaikiu sportuojančios moterys? Sporto mokslas, 4 (58), 62–69.
9. Jacobi, C., Fittig, E., Bryson, S.W., Wilfley, D., et al. (2011). Who is really at risk? Identifying risk factors for subthreshold and full syndrome eating disorders in a high-risk sample. Psychological Medicine, 41, 1939-1949.
10. Trost, S.G., Owen, N., Bauman, A.E., Sallis, J.F., Brown, W. (2002). Correlates of adults participation in physical activity: review and update. Medicine & Science in Sports & Exercise,
34(12):1996–2001. 11. Melbye, L., Tenenbaum, G., Eklund, R. (2008). Self-Objectification and Exercise Behaviors: The
Mediating Role of Social Physique Anxiety. Journal of Applied Biobehavioral Research, 12, 196–220. 12. Jankauskiene, R., Pajaujiene, S. (2011). Disordered eating attitudes and body shame among
athletes, exercisers and sedentary female college students. The Journal of Sports Medicine and Physical Fitness, 2, 52 (1), 92–101.
13. Babio, N., Arija, V., Sancho, C., Canals, J. (2008). Factors associated with the body dissatisfaction in non-clinical adolescents at risk of eating disorders. Journal of Public Health, 16, 107–115.
14. Prichard, I., Tiggeman, M. (2008). Relations among exercise type, self-objectification, and body image in the fitness centre environment: The role of reason for exercise. Psychology of Sport and Exercise, 9 (6), 855–866.
15. LePage, M. L., Crowther, J. H. (2010). The effects of exercise on body satisfaction and affect. Body image, 7(2), 124-130.
16. Deci, E. L., Ryan, R. M. (2008). Self-determination theory: A macrotheory of human motivation, development, and health. Canadian psychology / Psychologie Canadienne, 49(3), 182.
17. Haines, J., Neumark-Sztainer, D. (2006). Prevention of obesity and eating disorders: a consideration of shared risk factors. Health Education Research, 21, 770–782.
18. Hildebrandt, T., Alfano, L., Langenbucher, J. W. (2010). Body image disturbance in 1000 male appearance and performance enhancing drug users. Journal of Psychiatric Research, 44(13), 841-846.
19. Booth, F. W., Roberts, C. K., Laye, M. J. (2012). Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology, 2:1143-1211.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
84
7 - ORIGINAL RESEARCH: Step-Exercise as a mean of bone
health improvement [Rita Santos Rocha]
Rita Santos Rocha16
16IPS-ESDRM - Polytechnic Institute of Santarém - Sport Sciences School of Rio
Maior, Portugal. UL-FMH-CIPER - University of Lisbon - Faculty of Human Kinetics -
Interdisciplinary Centre for the Study of Human Performance, Portugal.
EuropeActive – Professional Standards Committee
E-mail: [email protected]
Abstract: Physical exercise has been found to be effective in the prevention of osteoporosis,
especially those activities that include impact loading. Activities such as walking, jogging and stair
climbing, introduce stress to the skeleton through ground reaction forces (GRF). The analysis of GRF
helps to understand the magnitude and pattern of loading experienced by the body while in contact with
the ground. The purposes were to analyse the peak-GRF and loading-rate produced by Step-Exercise in
18 skilled females; and to investigate the effect of stepping-rate and step-pattern. Step-Exercise seems
to produce greater loading than walking and at increased stepping-rates its loading could be compared
to those obtained during comfortable running. Loading can be effectively controlled by varying stepping-
rate and step-patterns during classes. Controlled stepping exercise appears relatively safe with respect
to the magnitude of loading regarding bone health.
Key-words: step, bone health, ground reaction forces
16
Rita Santos-Rocha, 1971, Lisbon, Portugal. Associate Professor at ESDRM-IPS. She has been teaching subjects
such as Physical Activity and Public Health; Exercise Testing and Prescription; and Exercise Biomechanics, since 1998.
Fitness training provider since 1995. Researcher at CIPER-FMH-UL with participation in research projects in the fields
of Active Pregnancy, Active School, Active Ageing, and Biomechanics. Member of the Scientific Committee of the
Gymnastics Federation of Portugal (since 2006). Member of the Professional Standards Committee – EuropeActive
(since 2011). BSc in Sport Sciences (1996); MSc in Exercise & Health (2000); PhD in Human Movement – Health &
Fitness (2006). Past occupations: fitness instructor, group gymnastics trainer and physical education teacher. List of
publications in ORCID | ResearchGate

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
85
Introduction
Exercise and bone health
Recreational Exercise aiming to improve or maintain health and fitness refers to a
group of physical activities performed by a large number of participants worldwide,
regardless of age and physical or health status [1]. The main objectives of these
physical activities are to provide healthy mechanical and metabolic stimuli as well
as improve adherence. Exercise professionals must provide effective sessions
according to established principles of training and use several tools [1,2]. Besides
its cardiovascular benefits, the structure of exercise sessions and exercise
prescription, concerning rate and magnitude of skeletal loading, can improve the
osteogenic potential of physical activity [3,4].
Exercise Prescription concerns in a sequence of procedures aiming to adapt the
stimuli of the different forms and modes of Exercise to participant’s goals and
needs, using the information of health and fitness assessment, respecting the main
roles of Exercise and the safety of participants [5,6]. In what is concerned to
health-related cardiovascular Exercise, plenty of well-documented references can
be found in the literature [5,6]. Those include the metabolic expenditure of several
forms of physical activity and the step-by-step case studies developed in order to
adapt the metabolic calculations to meet participants’ goals of losing weight or
improving cardiorespiratory fitness.
To give a figurative example, considering that a person is running for 30 min at a
comfortable speed, this type of exercise could be considered a stimulus that can be
translated into an “aerobic effort whose intensity is about 60% of the maximal
oxygen uptake, which is consuming a certain amount of calories”, or into a
“mechanical effort of which vertical component of the ground reaction force is about
1600 Newton or about two times the person’s body weight, and it has been applied
to 1500 times on each foot”. In the first case, we are referring to the specific
effects of this exercise on the cardiorespiratory system and body composition. In
the second case, we are referring to the specific benefits of this exercise on the
musculoskeletal system and bone health.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
86
Regarding bone health, bone mineral density, osteoporosis and osteoporotic
fractures have become one of the major health problems in Western countries [7].
As explained by Beck [8], normal physiological loading causes a range of
deformation reactions (strains) in bone, including compression, tension, shear,
torsion, and vibration. Bone exhibits an intrinsic ability to adapt to alterations in
chronic loading to withstand future loads of the same nature (Wolff’s Law).
Adaptation of bone to loading changes occurs via increased modelling and/or
remodelling.
Physical exercise has been found to be effective in the prevention of osteoporosis,
especially those activities that include impact loading [9-13] and progressive
resistance training [14]. Physical activity, particularly weight-bearing exercise, is
thought to provide the mechanical stimuli or "loading" important for the
maintenance and improvement of bone health, whereas it is well-established that
physical inactivity has been implicated in bone loss and its associated health costs.
High-intensity resistance training has the added benefit of influencing multiple risk
factors for osteoporosis including improved strength and balance and increased
muscle mass in older adults [14]. Moreover, the regular participation of young
people (18-22 years) in weight-bearing exercise might be beneficial for accruing
peak bone mass and optimizing bone structure [15].
The load-bearing capacity of bone reflects both its material properties, such as
density and modulus, and the spatial distribution of bone tissue. These features of
bone strength are all developed and maintained in part by forces applied to the
bone during daily activities and exercise, i.e., functional loading through physical
activity exerts a positive influence on bone mass [16]. Lifestyle choices are
attributed to 40% to 60% of adult peak bone mass, and there is strong evidence
for the benefits of physical activity and calcium intake on bone mass accretion [17].
Hinton et al. [18] concluded that 12 months of resistance training or jump training
increased bone mineral density (BMD) of the whole body and lumbar spine, while
resistance training also increased hip BMD, in moderately active, osteopenic men

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
87
(mean age of 44 years). Kemmler et al. [19] concluded that changes of exercise
levels directly or indirectly caused by occupational factors during young adulthood
significantly affected generation and/or maintenance of peak bone mass. Moreover,
physical activity in youth could reduce the burden of fragility fractures since
Exercise-associated bone trait benefits are found long term after retirement from
sports together with a lower fracture risk [20].
Exercise and ground reaction forces
The major biological effects of forces include changes in the development of
biological tissue and transportation of nutrients through the human body [21]. The
effects of biomechanical loading applied on the Musculoskeletal System can be
either biopositives or bionegatives. Regular exposure to moderately high
magnitudes of force is desirable within certain levels, because mechanical stress
will induce adaptation of biological structures, however the same forces might
produce undesirable effects such as discomfort, pain and injury, especially when
forces are too repetitive in a period of time [22,23]. Load repetition generally does
not result in injury during normal activity, although it has been suggested that
repeated impacts such as the collision of the foot with the ground during
locomotion can result in microtrauma [24]. In Sports and Exercise Biomechanics,
two areas of research are of major interest: 1) the quantification or estimation of
the mechanical load acting on the biological structures; and 2) the study of
biological effects of locally acting forces on living tissue; effects such as growth and
development or overload and injuries [25].
Kohrt et al. [26] defined that activities such as walking, jogging and stair climbing,
involves a group of exercises that introduce stress to the skeleton through ground
reaction forces (GRF); and activities such as weight lifting and rowing constitute a
group of exercises that introduce stress to the skeleton through joint reaction
forces (JRF). Both the GRF and the JRF exercise programmes resulted in significant
and similar increases in BMD of the whole body. Nikander et al. [12] performed
research with 255 premenopausal female athletes and referred that the loadings
that arise from high impacts or impacts from atypical loading directions seem to be
effective. Also, the authors reported that high-impact loading (e.g., volleyball) and

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
88
odd-impact loading (e.g., step aerobics and soccer) activities were associated with
the highest BMD of the femoral neck and bone strength (index Z) when compared
to high-magnitude loading (e.g., weightlifting), low-impact loading (e.g.,
orienteering and cross-country skiing), and non-impact loading (e.g., swimming
and cycling) activities. Jämsä et al. [13] studied for the first time the association
between the intensity of physical activity and proximal femur BMD, using a long-
term quantification of daily activity based on the vertical component of the
acceleration. It appears that strength and overall fitness can be improved at any
age through a carefully planned exercise programme.
Understanding the magnitude of loading is important for exercise prescription and
to design rehabilitation programmes. The vertical peak-GRF allows characterizing
movement in terms of biomechanical loading. It has been suggested that there is
an optimal amount of loading that healthy individuals should maintain and that
loading above a certain limit might be related to the risk of injury [27]. High
skeletal loading intensity has been defined as peak-GRF of greater than 4 times
body weight (BW), moderate intensity as 2-4 BW, and low intensity as GRF less
than 2-BW, and a minimum osteogenic effect was related to 1-2 BW [4,10,27]. The
magnitude of GRF has also been associated, although never verified, with the high
incidence of lower extremities injuries in fitness instructors [28]. Nevertheless, the
human body has a number of mechanisms by which load is attenuated. On one
hand, the body has structures such as fat pads on the plantar surface of the foot,
cartilage in the joints and bone, and soft tissues surrounding the bone. On the
other hand, there are also particular motions of the segments that attenuate shock.
In the lower extremity, these include knee flexion, subtalar pronation, and ankle
dorsiflexion [24].
Step-Exercise and osteogenic potential
Step-Exercise, described in a previous study [29], involves a large number of
loading cycles during each session, which might help to meet the recommendation
of 10,000 steps a day [30], and there are several evidence-based studies on its
cardiovascular benefits [31-35]. When Step-ReebokTM programme was created in
1994, its proponents claimed that GRF were similar to those of walking [36]. Miller
Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
89
[22] reported that GRF in walking has a maximum value of 1-1.2 BW, and in
running, can achieve 3-5 BW. However, the intensity of the workout depends on
the adaptations of stepping-rate (125-150 beats-per-minute – bpm); and on
selecting the types of movements included in a more or less complex choreography
(e.g., propulsive movements). Usually a Step Exercise class is performed with a
mean (±sd) stepping rate of 135±5 bpm, involving a mean (±sd) number of
loading cycles of 4194.1±1055.2, ranging from 1874 to 7250 [29]. A major concern
is how to control the intensity of the workout, maintaining safe and effective levels
of mechanical load, since the GRF of a Step session depends on the type and
number of movements performed [29].
Several authors referred that Step-Exercise seems to induce greater loading than
walking, and at increased stepping-rates its impact loading could be compared to
those obtained during comfortable running and high impact aerobics, but with a
lower risk of injury [37-47]. Most of these studies reported the effects of vertical
peak-GRF during the descending-phase of basic-step, and only a few references
reported the internal loading during Step-Exercise [38,48].
Moreover, one may be interested in the magnitude or in how fast the force is
increasing or decreasing. The loading-rate describes this behaviour. The
quantification of the initial part of the vertical GRF curve may be effectively
characterized by the loading-rate, due to the absence of an impact peak in certain
cases. It is often assumed that the loading-rate is associated with the development
of movement-related injuries [21].
Purposes
To investigate the differences that exist between four stepping-rate conditions
(125/130/135/140-bpm) and ascending and descending-phases of four step-
patterns (basic-step/knee-lift/run-step/knee-hop) in the vertical-1st-peak (FZ) and
in the vertical-1st-peak loading-rate (LR-FZ), in Step-Exercise. We hypothesized
that Step-Exercise is low to moderate activity, and the step-patterns with
propulsion should present higher load than non-propulsive movements, and loading
increases with faster stepping-rate.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
90
Methods
Eighteen female (mean±sd age 29.1±6.8 years; body mass 58.9±6.4 kg; height
1.66±0.06 m) with no history of lower limb trauma or disease, volunteered to
participate in the study. These women were experienced fitness instructors who
were graduate in sport sciences and possessed at least 3 years of teaching
experience. They were led through a sequence of 8 stepping tasks: right-basic-
step, right-knee-lift, left-basic-step, left-knee-lift, right-run-step, right-knee-hop,
left-run-step, left-knee-hop. This sequence ensured a mechanical balance between
both lower limbs. No arm movements were added and participants wore similar
shoes. Verbal instruction was provided during the tests. Music was used to maintain
cadence. All experimental trials were conducted in a “crescent cadence” order.
These procedures were adopted so the result would reflect typical class conditions.
Body weight was measured using a force-platform. The subjects were allowed to
familiarize to each speed before data collection, and was given approximately 60-
90s of rest between trials so as to reduce the potential effects of fatigue. Further
description of the procedures can be found in Santos-Rocha et al. [47].
The stepping-up movements were performed on a 17 cm height force-platform
(AMTI) (substituting the step-bench) and on a force-platform (Kistler) on ground
level for stepping-down [46]. The software Acqknowledge-3.7.3. (BIOPAC) was
used to collect GRF at 1000-Hz and process data. Data were smoothed with a
Hamming low pass digital filter of 8-Hz. Peak values were collected and normalized
to BW in Excel (Microsoft). Loading-rate (N/s) was calculated (loading-rate=peak-
force-N/time-to-peak-s) and normalized to BW/s (figure 5).

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
91
Figure 5 - Identification of the peak of the vertical ground reaction force, and the calculation of the loading rate regarding the descending phase of a basic step at
130 bpm, of one of the subjects.
Using SPSS (Statistical Package for the Social Sciences) the vertical-1st peak (FZ) in
BW and the vertical-1st peak loading-rate (LR-FZ) in BW/s were analysed
statistically. Descriptive statistics are reported and a one-way ANOVA for repeated
measures (RM) was used to determine whether there were significant differences
between the conditions of stepping-rate and step-patterns, resulting in two within-
subjects factors. Prior to performing RM, Kolmogorov-Smirnov normality test and
Mauchly’s test of sphericity were conducted. In the cases sphericity was not
assumed the Huynh-Feldt correction was used. The pairwise comparisons with the
Bonferroni confidence interval adjustments were used to identify where differences
could be found. The level of statistical significance was set at p≤.05.
Results
Figure 6 represents the identification of the movements studied, and shows the
phases of reception during which the peak values were collected. The results
showed that during stepping at different cadences the vertical GRF curves were
very regular and repetitive among subjects, despite different interval time among
conditions. We observed the absence of impact peaks in the movements analysed.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
92
Figure 6 - Vertical components of the ground reaction force of one representative subject at 140 beats per minute. The arrows identify the phases during which the
peak values were collected within the sequence of the 8 Step movements using the
vertical component of the ground reaction force, during the ascending (AMTI Fz) and descending (FZ) phases of the movements: black arrows show basic-step; grey
arrows show knee-lift; black dashed arrows show run-step; and grey dashed
arrows show knee-hop.
Table 10 shows the descriptive statistics of FZ and LR-FZ. Table 11 shows the
results of ANOVA-RM and Bonferroni pairwise comparisons of the parameters
analysed, as well as the summary of the confirmation of the hypothesis. The test of
within-subjects effects has shown no interaction between step-pattern and
stepping-rate in LR-FZ (descending-phase). There was interaction between
conditions in relation to: FZ (ascending-phase, p=0.001; descending-phase,
p=0.011) and LR-FZ (ascending-phase, p=0.002).
0.00000 3.33525 6.67050 10.00575seconds
0.00
144.97
289.94
434.91
N
AM
TI_
Fx
0.00
436.00
872.01
1308.01
N
AM
TI_
Fz
0.00
495.81
991.61
1487.42
NFZ
-315.19
-157.59
0.00
157.59
NFX
Right
Basic
Step
Right
Run
Step
Left
Basic
Step
Left
Run
Step
Right
Knee
Lift
Left
Knee
Lift
Right
Knee
Hop
Left
Knee
Hop
GRFGRF
0.00000 3.33525 6.67050 10.00575seconds
0.00
144.97
289.94
434.91
N
AM
TI_
Fx
0.00
436.00
872.01
1308.01
N
AM
TI_
Fz
0.00
495.81
991.61
1487.42
NFZ
-315.19
-157.59
0.00
157.59
NFX
Right
Basic
Step
Right
Run
Step
Left
Basic
Step
Left
Run
Step
Right
Knee
Lift
Left
Knee
Lift
Right
Knee
Hop
Left
Knee
Hop
GRFGRF
0.00000 3.33525 6.67050 10.00575seconds
0.00
144.97
289.94
434.91
N
AM
TI_
Fx
0.00
436.00
872.01
1308.01
N
AM
TI_
Fz
0.00
495.81
991.61
1487.42
NFZ
-315.19
-157.59
0.00
157.59
NFX
Right
Basic
Step
Right
Run
Step
Left
Basic
Step
Left
Run
Step
Right
Knee
Lift
Left
Knee
Lift
Right
Knee
Hop
Left
Knee
Hop
GRFGRF

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
93
Table 10 - Descriptive statistics of the peak vertical ground reaction force (FZ) normalized to body weight (BW) and of the loading rate of the peak vertical ground
reaction force normalized to body weight per second (BW/s), during ascending phase and descending phase of four Step-patterns (basic-step, knee-lift, run-step
and knee-hop) performed at four stepping-rates (125, 130, 135 and 140 bpm).
BASIC-STEP KNEE-LIFT RUN-STEP KNEE-HOP
BPM 125 130 135 140 125 130 135 140 125 130 135 140 125 130 135 140
ASCENDING PHASE – PEAK FZ GRF (BW)
Mean 1.2 1.2 1.2 1.2 1.3 1.2 1.3 1.3 2.1 2.2 2.2 2.3 1.8 1.8 1.8 1.8
sd 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.2 0.3 0.3 0.2 0.2 0.2 0.2 0.2
Min 1.0 1.0 1.0 1.0 1.0 1.1 1.1 1.0 1.7 1.5 1.6 1.9 1.5 1.5 1.5 1.5
Max 1.4 1.4 1.5 1.5 1.6 1.5 1.5 1.6 2.6 3.0 3.1 2.7 2.1 2.2 2.2 2.2
Range 0.4 0.5 0.4 0.5 0.6 0.5 0.4 0.6 0.9 1.5 1.5 0.9 0.6 0.8 0.7 0.7
DESCENDING PHASE – PEAK FZ GRF (BW)
Mean 1.7 1.7 1.7 1.7 1.7 1.7 1.7 1.8 1.7 1.7 1.8 1.8 1.6 1.6 1.6 1.6
sd 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.3 0.2 0.2 0.3 0.2 0.2 0.2 0.3 0.3
Min 1.3 1.3 1.3 1.2 1.2 1.3 1.3 1.3 1.4 1.3 1.4 1.4 1.2 1.2 1.1 1.1
Max 2.1 2.1 2.1 2.2 2.0 2.3 2.1 2.3 2.2 2.4 2.3 2.3 2.0 2.2 2.0 2.1
Range 0.7 0.8 0.8 1.0 0.8 1.0 0.8 1.0 0.8 1.1 0.9 1.0 0.8 1.0 1.0 1.0
ASCENDING PHASE – LOADING RATE PEAK FZ (BW/s)
Mean 5.8 5.9 6.0 6.3 4.9 5.1 5.1 5.5 8.7 9.0 9.2 10.2 6.5 6.8 6.6 7.2
sd 0.9 1.0 1.2 1.3 0.8 0.7 0.6 0.6 2.1 2.0 1.8 1.5 1.0 1.3 1.1 1.0
Min 4.0 3.9 4.1 4.1 3.5 3.9 4.1 4.4 5.4 4.8 5.7 6.8 4.5 4.8 4.9 5.3
Max 7.3 8.2 8.9 9.3 6.4 7.2 7.4 6.9 14.1 13.5 13.1 13.1 8.4 10.4 9.7 9.1
Range 3.3 4.3 4.7 5.2 3.0 3.3 3.4 2.5 8.7 8.7 7.4 6.3 3.8 5.6 4.8 3.8
DESCENDING PHASE – LOADING RATE PEAK FZ (BW/s)
Mean 8.1 8.2 8.5 8.5 7.4 7.9 8.3 8.5 7.8 8.3 8.5 8.5 7.4 7.5 7.8 7.7
sd 1.4 1.3 1.8 1.6 1.1 1.6 1.7 1.7 1.3 1.7 1.6 1.3 1.2 1.8 1.7 1.5
Min 4.9 5.9 6.3 5.8 4.7 4.5 5.8 5.1 4.7 6.2 5.2 6.3 4.4 4.8 4.8 5.4
Max 10.9 11.1 12.8 12.5 9.4 13.5 15.6 13.1 10.4 12.8 12.1 11.9 10.7 13.2 12.3 11.0
Range 6.0 5.2 6.5 6.7 4.8 9.0 9.7 8.0 5.6 6.7 6.9 5.6 6.3 8.4 7.5 5.6

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
94
Table 11 - Summary of the results of the statistical analysis (ANOVA repeated measures) performed with vertical peak ground reaction forces (FZ) parameters.
Significantly statistical differences (p≤0.050) were found among the following conditions of stepping-rate and step-pattern.
STEPPING-RATE STEP-PATTERN
Peak FZ ascending phase
ANOVA-RM F(3,105)=12.652 (p=0.000) All (p≤0.013); except 125-130 bpm; except 135-140 bpm Increases as stepping-rate increases Hypothesis confirmed
F(2.086,73.005)=441.251 (p=0.000) All (p=0.000) Greater values in run-step Hypothesis confirmed
Peak FZ descending phase
F(3,105)=5.901 (p=0.001) 125-135 bpm (p=0.001); 125-140 bpm (p=0.015) Increases as stepping-rate increases Hypothesis confirmed
F(2.200,77.000)=14.301 (p=0.000) basic-hop (p=0.000); knee lift-hop (p=0.003); run-hop (p=0.000) Hypothesis not confirmed
Loading rate FZ ascending phase
F(3,105)=17.838 (p=0.000)
125-140 bpm (p=0.000); 130-140 bpm (p=0.000); 135-140 bpm (p=0.000) Increases as stepping-rate increases Hypothesis confirmed
F(2.398,83.925)=147.162 (p=0.000) All (p=0.000) Greater values in run-step Hypothesis confirmed
Loading rate FZ descending phase
F(2.715,95.041)=8.432 (p=0.000) 125-135 bpm (p=0.000); 125-140 bpm (p=0.000) Increases as stepping-rate increases Hypothesis confirmed
F(3,105)=8.770 (p=0.000) basic-hop (p=0.000); run-hop (p=0.003) Hypothesis not confirmed
Discussion
The GRF may provide a surrogate measure of the strain experienced by bone on a
variety of loading activities such as Step movements [47]. The analysis of GRF has
shown that higher loads occur during the reception on the step-bench (in
propulsion movements: run-step and knee-hop) and during the reception on the
ground (in non-propulsion movements: basic-step and knee-lift). The results of FZ
in basic-step (descending-phase) were greater than those reported by other
authors that used slower cadences (120-bpm) [37,38,42] but are in line with those
obtained by Teriet and Finch [40]. In knee-lift (descending-phase) the results were
greater than those reported by Farrington and Dyson [37] that used slower
cadences (120-bpm). The results in both phases are in line with those obtained by
Panda [49]. In run-step the mean FZ was 2.3-BW (ascending-phase) and 1.8-BW
(descending-phase). Tagen and Zebas [50] reported 2.5-BW during ascending-
phase of run (126-bpm). The results of FZ in knee-hop (ascending-phase) are in
line with those reported by Machado and Abrantes [45] that also used slower
cadences (120-bpm). The results for both phases of all movements performed at

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
95
130 and 140-bpm were around 0.1-0.2 smaller than those obtained in our previous
studies using pressure insoles [46]. Therefore, Step-Exercise seems to produce
greater loading than walking and at increased stepping-rates its loading could be
compared to those obtained during comfortable running [22].
The results obtained for vertical peak-forces suggest that Step-Exercise is a low to
moderate activity, depending on the inclusion of non-propulsion or propulsion, and
stepping-rate (with experienced participants). Teriet and Finch [40] suggested that
the faster loading and unloading-rates of the musculature due to the faster
stepping-rates (122 to 130-bpm) caused less control of the movement, resulting in
a 4% increase in the FZ and therefore, the use of faster tempos in a beginning level
class could be a source of elevated risk for potential injury. Our results support the
conclusion of Scharff-Olson et al. [41] that experience with Step-Exercise may
afford an ability to make uniform and force-absorbing adjustments in FZ at
increased speeds.
The time of peak FZ, ranged 0.20-0.28s (ascending-phase) and 0.21-0.22s
(descending-phase). The interval time decreased with stepping-rate, meaning that
the same movement has to be performed in the same form but with less time. This
is reflected by the increase in loading-rate. Loading-rate was associated to 77 BW/s
in running speed at 3m/s [22]. In the present study, the mean LR-FZ increased
with stepping-rate, and the greatest value was found in ascending-phase of run-
step. In descending-phase it increased significantly with stepping-rate. The larger
peaks and loading-rates indicate a loss of shock absorbing capacity. This might
increase their susceptibility to lower extremity overuse injuries.
The results indicate that lower extremity external loading can be effectively
controlled by varying stepping-rate during Step classes, and by choosing
movements mechanically similar to those analysed in the present study. As an
example, the run-step clearly induced greater forces and loading-rate, which might
be more related to injury.
These findings indicate the relative contributions of stepping-rate and different

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
96
choreographic movements to the external forces experienced during Step-Exercise.
Further research is needed focusing other step-patterns in order to select those
that are more appropriate to be included in Exercise and Rehabilitation
programmes. The present investigation provides biomechanical data that may be
used as a basis for comparison with patients, older adults and beginners that
participate in Step classes. However, the present results are based on a sample of
18 experienced and physically active instructors, thus, both kinematics [51] and
force characteristics of the tasks may be different if participants with less
experience in Step are involved, and establishing norms for other populations
requires understanding other factors that affect GRF.
Implications for practice
Our results showed that increasing step frequency leads to an increase in the
mechanical load, which appears to be supported by adaptations of the movement
technique which might be related with the increasing GRF. However, if technique
adaptations occur, especially in the knee joint, together with greater GRF and
moments of force and decreased time for contact and force transfer, the stepping-
rate, being one of the most important determinants of exercise intensity,
particularly above 135-bpm, should be chosen carefully in classes, having always in
consideration the participants’ experience in this activity.
The results contribute to understanding how skilled participants deal with the
increase of the external load during Step-Exercise. Skilled participants appear to
control the increase of stepping-rate by means of knee and ankle adaptations.
These joints might be at greater risk of injury in the case of overuse, especially the
knee joint. In order to prevent injury, proper instruction should be provided in
relation to foot placement on the step-bench and on the ground, as well as
information concerning knee flexion. Our results indicate that lower extremity
external loading can be effectively controlled by varying stepping-rate during Step
classes and selecting step-patterns. The results are also relevant to determine
which movements and cadences can be recommended to be included in
rehabilitation or sports programmes where walking and running are prescribed.
Assuming that walking or running are “safe” activities to be included in exercise

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
97
programmes, oriented stepping exercise appear relatively safe with respect to the
magnitude of loading.
Conclusion
Step-Exercise is performed using music that sets movement cadence which
involves the repetition of exercises that induce peak-GRF of low magnitude
moderate activity (1-2.5 BW), depending on step-patterns included, but of high
frequency (3750-4050 loading cycles during a 30-min session), depending on the
stepping-rate, using music speed at 125/135-bpm, that may be recommended for
bone health improvement.
References
1. Santos-Rocha R, Rieger T, Jimenez A (Eds.) (2015). Europe Active’s Essentials of Fitness Instruction. Europe Active. Campaign: Human Kinetics. ISBN Print: ISBN 978-1-4504-2379-3. E-book: ISBN 978-1-4925-0591-4
2. Rieger T, Naclerio F, Jiménez A, Moody J (Eds.). (2015). Europe Active’s Foundations for Exercise Professionals. Europe Active. Campaign: Human Kinetics.
3. Cullen DM, Smith RT, Akhter MP (2001). Bone-loading response varies with strain magnitude and cycle number. Journal of Applied Physiology, 91, 1971-1976.
4. Turner CH & Robling AG (2003). Designing exercise regimens to increase bone strength. Exercise & Sport Science Reviews, 31(1), 45-50.
5. ACSM (2013). ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription (7th ed.). Baltimore: Williams & Wilkins.
6. ACSM (2014). ACSM’s Guidelines for Exercise Testing and Prescription (9th ed.). Baltimore: Williams & Wilkins.
7. Cummings SR & Melton LJ (2002). Epidemiology and Outcomes of Osteoporotic Fractures. Lancet, 359 (pp 1761-1767).
8. Beck BR (2000). American College of Sports Medicine "Current Comment", Stress Fractures, February 2000, www.acsm.org.
9. Wallace BA & Cumming RG (2000). Systematic Review of Randomized Trials of the Effect of Exercise on Bone Mass in Pre- and Postmenopausal Women. Calcified Tissue International, 67 (pp 10-18).
10. Witzke KA & Snow CM (2000). Effects of plyometric jump training on bone mass in adolescent girls. Medicine & Science in Sports & Exercise, 32, 1051-1057.
11. Bauer JJ, Fuchs RK, Smith GA, Snow CM (2001). Quantifying Force Magnitude and Loading Rate From Drop Landings That Induce Osteogenesis. Journal of Applied Biomechanics, 17 (pp 142-152).
12. Nikander R, Sievanen H, Heinonen A, Kannus P (2005). Femoral Neck Structure in Adult Female Athletes Subjected to Different Loading Modalities. Journal of Bone & Mineral Research, 20(3), (pp 520-528).
13. Jämsä, T; Vainionpää, A; Korpelainen, R; Vihriälä, E & Leppäluoto, J (2006). Effect of Daily Physical Activity on Proximal Femur. Clinical Biomechanics, 21 (pp 1-7).
14. Layne JE & Nelson ME (1999). The Effects of Progressive Resistance Training on Bone Density: A Review. Medicine & Science in Sports & Exercise, 31(1), (pp 25-30).
15. Yung PS, Lai YM, Tung PY, Tsui HT, Wong CK, Hung VW, Qin L (2005). Effects of Weight Bearing and Non-weight Bearing Exercises on Bone Properties Using Calcaneal Quantitative Ultrasound. British Journal of Sports Medicine, 39(8), (pp 547-551).
16. ACSM (1995). American College of Sports Medicine Position Stand. Osteoporosis and Exercise. Medicine & Science in Sports & Exercise, 27(4), (pp i-vii).
17. Weaver CM (2005). Parallels between nutrition and physical activity: research questions in development of peak bone mass. Res Q Exerc Sport. 2015 Jun;86(2):103-6. doi: 10.1080/02701367.2015.1030810.
18. Hinton PS, Nigh P, Thyfault J (2015). Effectiveness of resistance training or jumping-exercise to

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
98
increase bone mineral density in men with low bone mass: A 12-month randomized, clinical trial. Bone. 2015 Oct;79:203-12. doi: 10.1016/j.bone.2015.06.008. Epub 2015 Jun 16.
19. Kemmler W, Bebenek M, von Stengel S, Bauer J (2015). Peak-bone-mass development in young adults: effects of study program related levels of occupational and leisure time physical activity and exercise. A prospective 5-year study. Osteoporos Int. 2015 Feb;26(2):653-62. doi: 10.1007/s00198-014-2918-8. Epub 2014 Oct 7.
20. Tveit M, Rosengren BE, Nilsson JÅ, Karlsson MK (2015). Exercise in youth: High bone mass, large bone size, and low fracture risk in old age. Scand J Med Sci Sports. 2015 Aug;25(4):453-61. doi: 10.1111/sms.12305. Epub 2014 Aug 11.
21. Nigg BM (2000). Forces acting in and on human body. In: Nigg, B.M. et al. (editors), Biomechanics and Biology of Movement. Champaign, IL: Human Kinetics, Ch 14.
22. Miller DI (1990). Ground reaction forces in distance running. In: Cavanagh, P.R. (editor), Biomechanics of Distance Running. Champaign, IL: Human Kinetics, Ch 8.
23. Nigg BM, Cole GK, Brüggemann GP (1995). Impact forces during heel-toe running. Journal of Applied Biomechanics, 11, 407-432.
24. Hamill, J & Caldwell, GE (2001). Mechanical load on the Body. In Hauber, M (Ed), ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription (4th ed). Baltimore: Williams & Wilkins, (Ch 11).
25. Brüggemann, GP (2005). Mechanical Loading of Biological Structures and Tissue Response. In Rodrigues, H; Cerrolaza, M; Doblaré, M; Ambrósio, J & Viceconti, M (Eds), Proceedings of the ICCB 2005 – II International Conference on Computational Bioengineering (volumes 1 & 2), (pp 25-26).
26. Kohrt, WM; Ehsani, AA & Birge, SJ Jr. (1997). Effects of Exercise Involving Predominantly Either Joint-Reaction or Ground-Reaction Forces on Bone Mineral Density in Older Women. Journal of Bone Mineral Research, 12(8), (pp 1253-1261).
27. Shaw, J.M., Witzke, K.A. & Winters, K.M. (2001). Exercise for skeletal health and osteoporosis prevention. In: Hauber, M. (editor), ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription (4th ed). Baltimore: Williams and Wilkins, Ch 34.
28. Rousanoglou, E.N. & Boudolos, K.D. (2005). Ground reaction forces and heart rate profile of aerobic dance instructors during a low and high impact exercise programme. Journal of Sports Medicine and Physical Fitness, 45(2), 162-170.
29. Santos-Rocha, R., Oliveira, C. & Veloso, A. (2006). Osteogenic index of Step-Exercise depending on choreographic movements, session duration and stepping-rate. British Journal of Sports Medicine, 40, 860-866 (published online 18 Aug 2006; DOI: 10.1136/bjsm.2006.029413).
30. Wilde, BE; Sidman CL & Corbin, CB (2001). A 10,000-step count as a physical target for sedentary women. Research Quarterly in Exercise and Sport, 72(4), (pp 411-414).
31. Stanforth, D., Stanforth, P.R. & Velasquez, K.S. (1993) Aerobic requirement of bench stepping. International Journal of Sports Medicine, 14(3), 129-133.
32. Scharff-Olson, M., Williford, H.N., Blessing, D.L. & Brown, J.A. (1996). The physiological effects of bench/Step-Exercise. Sports Medicine, 21(3), 164-175.
33. Kin Ilser, A., Kosar, S.N. & Korkusuz, F. (2001). Effects of step aerobics and aerobic dancing on serum lipids and lipoproteins. Journal of Sports Medicine and Physical Fitness, 41(3), 380-385.
34. Kraemer, W.J., Keuning, M., Ratamess, N.A., Volek, J.S., McCormick, M., Bush, J.A., Nindl, B.C., Gordon, S.E., Mazzetti, S.A., Newton, R.U., Gómez, A.L., Wickham, R.B., Rubin, M.R. & Hakkinen, K. (2001). Resistance training combined with bench-step aerobics enhances women’s health profile. Medicine & Science in Sports & Exercise, 33(2), 259-269.
35. Ohta M, Eguchi Y, Inoue T, Honda T, Morita Y, Konno Y, Yamato H, Kumashiro M. Effects of bench step exercise intervention on work ability in terms of cardiovascular risk factors and oxidative stress: a randomized controlled study. Int J Occup Saf Ergon. 2015;21(2):141-9. doi: 10.1080/10803548.2015.1029293. PubMed PMID: 26323772.
36. Reebok University Press (1994). Introduction to Step Reebok. Stoughton: Reebok International, Ltd.
37. Farrington, T. & Dyson, R. (1995). Ground reaction forces during step aerobics. Journal of Human Movement Studies, 29, 89-98.
38. Bezner, S.A., Chinworth, S.A., Drewlinger, D.M., Kern, J.C., Rast, P.D., Robinson, R.E. & Wilkerson, J.D. (1996). Step aerobics: a kinematic and kinetic analysis. In: Wilkerson, J.D. et al. (editors), Proceedings of the XV International Symposium on Biomechanics in Sports. Denton, Texas: Texas Women’s University Press, 252-254.
39. Hecko, K. & Finch, A. (1996). Effects of prolonged bench stepping on impact forces. In: Abrantes, J. (editor), Proceedings of the XIV International Symposium on Biomechanics in Sports. Lisbon: Edições FMH, 464-466.
40. Teriet, C.R. & Finch, A.E. (1997). Effects of varied music tempos and volumes on vertical impact forces produced in step aerobics. In: Wilkerson, J.D. et al. (editors), XV International Symposium on Biomechanics in Sports. Denton, Texas: Texas Women’s University Press, 148.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
99
41. Scharff-Olson, M., Williford, H.N., Blessing, D.L., Moses, R. & Wang, T. (1997). Vertical impact forces during bench-step aerobics: exercise rate and experience. Perceptual Motor Skills, 84, 267-274.
42. Maybury, M.C. & Waterfield, J. (1997). An investigation into the relationship between step height and ground reaction forces in Step-Exercise: a pilot study. British Journal of Sports Medicine, 31, 109-113.
43. Wieczorek, S.A., Duarte, M. & Amadio, A.C. (1997). Estudo da força reação do solo no movimento básico de “step” (in Portuguese). Revista Paulista de Educação Física, São Paulo, 11(2), 103-115.
44. Williford, H.N., Richards, L.A., Scharff-Olson, M., Brown, J., Blessing, D. & Duey, W.J. (1998). Bench stepping and running in women. Changes in fitness and injury status. Journal of Sports Medicine and Physical Fitness, 38(3), 221-226.
45. Machado, M.L. & Abrantes, J. (1998). Basic-step vs. power step: peak values of vertical GRF analysis. In: Hartmut et al. (editors), Proceedings of the XVI International Symposium on Biomechanics in Sports. Universitatverlag Konstanz Gmbh, 514-517.
46. Santos-Rocha, R. & Veloso, A. (2007). Comparative study of plantar pressure during Step-Exercise in different floor conditions. Journal of Applied Biomechanics, 23, 158-164.
47. Santos-Rocha, R, Veloso, A & Machado, ML (2009). Analysis of ground reaction forces in step-exercise depending on step-pattern and stepping-rate. Journal of Strength and Conditioning Research. 23(1), January 2009, 209-224. DOI: 10.1519/JSC.0b013e3181889119.
48. Santos-Rocha, R, Veloso, A, Machado, ML, Valamatos, MJ & Ferreira, C (2009). Peak ground and joint reaction forces in step-exercise depending on step-pattern and stepping-rate. The Open Sports Sciences Journal. 2, 10-21. DOI: 10.2174/1875399X00902010010
49. Panda, M.D.J. (2003). Estudo Dinâmico dos Principais Passos do Step Training. Master thesis (Portuguese). Brasil: Centro de Educação Física, Fisioterapia e Desportos - Universidade do Estado de Santa Catarina (not published).
50. Tagen, L.S. & Zebas, C.J. (1996). Ground reaction forces of three propulsive movements in step aerobics. Medicine & Science in Sports & Exercise, 28 (5), abstract 155.
51. Santos-Rocha, R, Veloso, A, Valamatos, MJ, Machado, ML & André, HI (2009). Analysis of kinematics of the lower limb during step-exercise. Perceptual and Motor Skills. 109, 3, 851-869. DOI: 10.2466/pms.109.3.851-869

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
100
8 - PRACTICE UPDATE: How can we motivate the "unsocial"
children in Fitness classes? [Eljona Spaho]
Eljona Spaho17
17Fitness Advisor and Personal Trainer at Charlottehaven Fitness. Group Fitness
Instructor at Fitness World in Copenhagen, Denmark.
E-mail: [email protected]
Abstract: Nowadays teaching people becomes more and more challenging. In my classes I encounter
difficult people that is why I sat down many days read different scientific articles and books and by
combining the theoretical approaches with my many years work experience I came up to a solution
which helps me a lot in my work. Now I want to share it with all the other teachers.
When we teach we should consider that people are different, considering their resources and
backgrounds. In order to tackle the difficult ones we should try to understand their resources and
backgrounds and instead of thinking of them as a problem, we should try to find a solution that requires
collaboration and adaptation to their current resources and backgrounds. In this article, I apply this
approach when we encounter difficult children/members in fitness classes, but it can be applied in any
teaching situation.
Key-words: motivation, children, fitness
17
Eljona Spaho has a Master's Degree in International Business from Copenhagen Business School and is a Group Fitness Instructor, Personal Trainer and Fitness Nutritionist certified in USA and Denmark. Have been working since 2010 in fitness industry, teaching people of all ages. Furthermore have 2 years’ experience with teaching students at the University.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
101
Introduction
My focus with this article is how to include the children with antisocial behaviors, in
fitness classes, where they don’t disturb the teaching, and even behave good and
have good results in their training. The postmodern society focuses on the
individual and on how individuals can contribute to family, community and work.
We see suddenly for schools or other institutions that mediate different knowledge
and skills to the children that the challenge is no longer only the academic
difficulties but the social ones18. Antisocial children signal the risk for future
difficulties; both for the individual and for society as a whole such as poor
adaptation to working life, family problems, high risk of school dropout etc.,19
therefore, we play as instructors a very important role, not only to teach fitness but
also to raise children with interpersonal skills.
I teach fitness in a class where Joanne is a child 10 years old. She is not focused in
the class; she does not listen and destroys the teaching for the others. My
colleagues informed me that she was just a difficult child, and was tackled by
criticizing her and trying to convince her to attend the class without disturbing. This
approach was energy consuming and not very helpful because every time she
stopped for a while, she started again and again. I decided to study more closely
this issue and come up with new solutions that I will show through this article.
How can we motivate the "unsocial" children/members in fitness
classes?
In order to answer this question, I will focus on the problematic questions below
that support the overall theme's subject.
Problematic questions:
How can we motivate the children/members from their perspective?
What should we do as teacher/instructors to motivate the
children/members?
How can we involve the parents?
18
Positive behavior and supportive learning environment in school, A. Arnesen, T. Ogden, M.A. Sørlie, 2008, 13 19
Positive behavior and supportive learning environment in school, A. Arnesen, T. Ogden, M.A. Sørlie, 2008, 15

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
102
How can we adopt our teaching method?
How can we motivate the children/student/member?
I will try to answer this by focusing on a student/child's perspective.
There is a too large spread between individual' abilities and there are children who
are being distracted and restless. There is said of an "MTV generation" who learned
to zap between channels for what is interesting and a "Nintendo generation" who
choose faster and switch to something else if the contents are not catchy. Each
person is unique. We all have the same basic systems-features, yet we are all
different. Our differences are due to genetic conditions, different ways of thinking,
different talents, etc. Because we are different, it is important to maintain a high
degree of freedom in learning situations20.
In my work as a fitness teacher with the "unsocial" child/member I thought to
tackle Joanne in a different way, not to criticize her. I began to think about how I
could turn all the waste of energy on my side, from trying all the time to convince
her to participate in the education process, to find a way that could benefit us all.
In order to do that I considered different theories and other possible solutions.
I thought one cause of her not following the teaching could be because her skills
are higher or lower than the challenge of teaching, she is exposed.
Csikszentmihalyi21 has created a model that illustrates how learning is considered in
relation to the skills and the challenge of teaching (figure 7). The optimal learning
and wellbeing occurs when there is a balance between children's skills and training
challenge. Not optimum learning and well-being occurs when the challenge is
greater or less than the skill.
I will suppose that the child’s skills are greater than the challenges of fitness
teaching she was exposed. In order to examine the child’s skills, I used the
Activity Triangle Model22 (figure 8).
20
Play, learning and creativity, why happy children learn more, H. H. Knoop, 2002, 71 21
Play, learning and creativity, why happy children learn more, H. H. Knoop, 2002, 48 22
Focus, Journal of Sports Science, 1 February 2009, 33 rd ed., page 21

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
103
Csikszentmihalyi model
High Anxiety
Challenge Flow-Optimal
learning
and well-being
Low
Boredom
0
Low Competence High
Figure 7 - Flow-The natural balance between challenges and skills

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
104
Repeat
Control the skill gained
Experiment Competition
Examine the skills Use the skills
Figure 8 - Activity Triangle
After I had examined the child's skills, I made the exercises a little more difficult in
order the challenge to live up to her already gained skills. When making a program
the teacher must take into account the skills of the children/members in order to
provide them the right challenges. For example, if there is a wide disparity in the
children/members skills the teacher should not make many competitive exercises
but try to find some exercises where everyone can participate. When working with
children is very important to consider their resources and ideas23.
In conclusion, each person is unique. The teacher/instructor must take into account
the children's skills. To ensure that all children/members must attend classes and
get an optimal learning and well-being the challenge must be adapted to the skills.
It is important to turn the negative energy caused by the mismatch of skill with
challenge into something positive and constructive, so the children/members get
something out of the teaching.
23
Intervention in school, J. N. Murphy and B. L. Duncan, 2008, 51
Activity
Triangle

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
105
What should we do as teachers/instructors to motivate the
children/members?
Do you thrive as a fitness instructor with your work? Often it is difficult to work with
unfocused and troubled children, and there are too many differences between the
individual children's abilities in relation to fitness learning. The fitness teacher
maybe thrives by working with his interest, but to work with the children is very
demanding. The relationship teacher/student is a mutual relationship. It is the
student's job to be open to the teacher's teaching but he or she must also show
interest in the teaching. Therefore, the teacher/instructor must be inspiring. When
working with children it is particularly important that the teacher/instructor is
aware of its resources and ideas. What characterizes the skilled and well-liked
teacher is that he is motivated, dedicated, inspiring, captivating, brave,
experimental, is in control and has empathy, is professional competent, has a
positive and pleasing personality, shows interest, etc. The teacher/instructor should
show personal dynamism and charisma. These has partly to do with body language,
use of voice, enthusiasm, eye contact and the distance and location relative to the
student or students when teaching. The teacher/instructor must be responsive and
open to suggestions and requests. This will allow the students/members to have far
more influence and probably feel more freedom and interest24.
The teacher can also use the PALS (Possitive, Attidude, Learning, Support)
model25 that focuses on positive behavior, supportive learning environment and
interaction. The teacher/instructor must make sure to get positive personal contact
with every student/member during a lesson.
The "unsocial" child/member had experienced only criticism from the other
teachers/instructors. I was wondering how I could get a positive contact with her,
that she saw me as a teacher/instructor who likes her and think positively about
her. After I adjusted the challenge of teaching, I saw that she participated in class
and was no longer disturbing because she was occupied in doing the exercises that
matched her skills. I started to say in front of the class how good she did the
exercises. She was very happy because before she had experienced only criticism
from the previous teachers/instructors.
24
Focus, Journal of Sports Science, 1 January 2004, 28th ed., page 29
25 Positive behavior and supportive learning environment in school, A. Arnesen, T. Ogden, M.A. Sørlie, 2008, 15

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
106
In conclusion, the teacher/instructor plays an important role in motivating the
children. If we as teachers/instructors work to find ways to solve student issues in a
positive and constructive way this benefits both the children and the
teacher/instructor.
How can we involve the parents?
The teacher/instructor must be professional, friendly, reliable and have a good
conversation with the parents. Whether you are parent or teacher, you both want
the best for the child. There is a distinction between primary and secondary
socialization. The primary socialization occurs in the family. The secondary takes
place in school. Therefore, it is important to investigate the role of families in the
socialization26.
I was wandering if the "unsocial" child’s behavior had also something to do with the
upbringing. According to Ericsson's Socialization Stages Model27 the child goes
through some development stages (table 12).
Table 12 - Ericsson’s Socialization Stages Model
Life stage / age of
the child Challenge - what needs to be learned
Infant Basic trust over distrust. The child must learn to feel safe, it's nice to be here in the world
2-3 years old Independence over doubt. The child must experience a self-esteem that they have the
right to demand while respecting others
4-5 years old Initiative over blame. The child must learn to act with determination and at the same time
learn that cannot handle everything
6-12 years old Ability over inferiority. The child must learn to complete tasks and resist the feeling of
inferiority when the task is too severe
After I spoke with the parents of the "unsocial" child, I understood that the parents
had not been able to raise their child as good as possible in the 2-3 years’ phase
"the child should experience such esteem that it has the right to require respect
and to respect others". Therefore, I told the parents to work with their child and
teach her at home "to respect others".
26
Parental cooperation, C. Højholt, 2005, 102 27
Life in Denmark, B. Jakobsen and O. Outzen, 2004, 17

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
107
The school/gym environment is different than at home where the small community
can be better organized. The child at school/gym must learn to be part of an
environment that is different from home environment. When one thinks about
school/gym environment one think of it primarily as a learning institution, but
parents see it also as an environment where their children learn to interact socially.
They want their children to learn to work together, resolve conflicts together in
other words to be part of a community. Therefore, the parents should collaborate
with the teachers to help each other in educating social children28.
In conclusion, the parents should collaborate with the teachers. Parents play an
important role in the motivation of children and together with the
teachers/instructors should educate social children.
How can we adopt our teaching method?
It has been much research into learning principles. We can distinguish between four
different types of learning processes: habituation, classical conditioning, operant
conditioning and complex learning29.
Habituation is the learning process through which we learn, is the "habit", a habit
that we no longer need to use mental energy/attention to it. Habituation is often
the reason why we are bored as monotonous repetitions will stimulate us less and
less. In order not to make teaching monotonous and in particular to stimulate the
"unsocial" children the teacher can try to vary the elements of teaching as shown at
the Activity Circle30 (figure 9).
28
Collaboration on children’s development, C. Højholt, 123-125 29
Play, learning and creativity, why happy children learn more, Hans Henrik Knoop, 2002, page 61-64 30
Focus, Journal of Sports Science, 2 May 2005, 29th edition, page 11

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
108
Figure 9 - Activity Circle
The teacher can use various tools to make the same exercise interesting, change
the participants, etc.
Classical conditioning is the learning process through which we learn that a
stimulus follows another. We can connect different experiences, i.e., develop phobic
reactions if we don't like the experience. If the child/student has a bad experience
with fitness every time he hears the word fitness, he will become irritated or
develop phobic reactions such as become nauseous. If we keep only criticizing the
"unsocial" child/student/member, there will come a time when she will associate
fitness with a negative experience, which may result in that she will stop coming to
classes. On the other hand, the school is interested in increasing participation,
therefore it should be a positive experience to go to fitness.
Operant conditioning is a learning process where we learn that an active action
causes a certain consistency. For example, if the children are praised for helping
with teaching, the greater the likelihood that they participate more actively in the
class in the future. We are attracted to situations where we have experiences
where we do well. In order to provide positive experiences to the "unsocial" child I
Rules Focus Participants
Action Activity’s Circle Time
Tools Space

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
109
should praise her when she does something good also in front of the parents, which
will result in more active participation in class next time.
Complex learning is the most advanced form. The following criteria are very
important in this learning process:
The new knowledge should preferably contribute to the person's overall set
of competencies.
Children/members should feel that what they learn gives them more
freedom by giving them new opportunities.
The new teaching should preferably not be too hard to learn. This includes:
Be careful not to overwhelm children/members with a lot of teaching.
Should not be too strong contrast to the person's already established ways
of thinking-meet the child/member where it is and let this be the starting
point for its learning.
The new exercises should be preferably easy to demonstrate and
communicate.
The new exercises should preferably be something that the person wants to
share with others.
Considering all this theoretical background I try to create a positive experience and
in a constructive way with the "unsocial" child/member. I allow her to help me
during the teaching for example by using her as a model during exercises
presented in front of the class. By providing all these positive experiences at the
end, we will have a child/member changed from "unsocial" to a highly motivated
child who on her own initiative helps the teacher and tells proudly about it to her
parents.
In conclusion, the fitness teacher/instructor must ensure that teaching does not
become monotonous and boring. Furthermore, the teaching should be fun, so the
children/students/members associate it with an exciting and fun experience. Fitness
teachers must praise the children/student/member when they do well, by doing so
they will attract them to participate more actively in class in the future.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
110
Discussion
I wrote this article to figure out how to motivate the "unsocial"
children/students/members to the fitness classes and I came up to these
conclusions and practical recommendations.
In your daily teaching work when you encounter the “unsocial” ones consider that
each person is unique, according to their skills. This is the reason why in order to
get an optimal learning and well-being the challenge must be adapted to the skills.
By doing so we turn the negative situations caused by the mismatch of skill with
challenge into positive and constructive situations, where the children/members
learn and behave well. For example, if you have a child/student/member who
considers the exercises boring because her skills are higher than the level of fitness
exercises she is exposed, you can give her extra challenges and she will stop
disrupting the teaching because the challenges will be the same as her level of
skills.
You as teachers/instructors play an important role in motivating the children by
being positive and constructive rather than criticizing and arguing with the children.
You as parents should collaborate with the teachers to educate social children; if
you work together, you will support each other. It is not enough, if only the teacher
tries to educate your child and at home, he still keeps being “unsocial”.
Furthermore, if the parents of the children do not collaborate with the teacher, the
teacher cannot decipher the children's behavior. Through conversation with the
parents, the teacher finds out which phase of appropriate upbringing he/she is
missing, where the parents should especially focus on to correct at the home
environment.
The fitness teacher/instructor must ensure that teaching does not become
monotonous and boring but fun, so the children/students/members associate it with
an exciting and fun experience. Fitness teachers must praise the
children/students/members when they do well, by doing so they will attract them to

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
111
participate more actively in class in the future, it helps changing their behavior and
way of being in class and the manner in which they participate in teaching. If we
experience the child is inactive and not participates and even annoys the other
children for example by being aggressive and teasing, if we implement the new
teaching tools, the fitness classes will alter, and the children/members will
participate actively and their behavior will change positively.
Overall Conclusion
As an overall conclusion and recommendation, I can say that the "unsocial"
children/members can be motivated by taking into account their social and fitness
skills. By increasing the cooperation between the teachers/instructors and parents
and adopting the teaching to the individual child/student/member. Not criticize but
tackle them positively and in a constructive way.
References
1. Arnesen, Anne; Ogden, Terje; Sørlie, Mari-Anne; Klausen, Honoré M. Positiv adfærd og støttende læringsmiljø i skolen (Positive behavior and supportive learning environment in school).; 2008. 13, 15 p. ISBN-13: 9788772812588
2. Fokus (Focus), Journal of Sports Science, 1 February 2009, 33d edition 3. Fokus (Focus), Journal of Sports Science, 1 January 2004, 28th edition 4. Fokus (Focus), Journal of Sports Science, 2 May 2005, 29th edition 5. Højholt, Charlotte. Højholt Ch and other editors. Forældresamarbejde: forskning i fællesskab
(Parental cooperation: research in community), 2005. 102 p. ISBN 87-7706-470-4 6. Højholt, Charlotte. Samarbejde om børns udvikling (Collaboration on children's development),
2001. 123-125 p. ISBN-13: 9788700486881 7. Jakobsen, Benny and Outzen, Ove. Liv i Danmark (Life in Denmark).; 2004. 17 p. ISBN 978-87-
7970-105-2 8. Knoop, Hans Henrik. Leg, læring og kreativitet : hvorfor glade børn lærer mere (Play, learning and
creativity, why happy children learn more), 2002. 48, 61-64, 71 p. ISBN 9788711437025 9. Murphy, John N. and Duncan, Barry L. Intervention i skolen (Intervention in school), 2008. 51 p.

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
112
European Journal for Exercise Professionals – INSTRUCTIONS
FOR AUTHORS AND SUBMISSION PROCESS
Journal’s format and frequency:
The European Journal for Exercise Professionals is an on-going peer-reviewed
online journal which publishes articles on important trends and developments in the
fitness industry and related fields. Each volume will include a set of articles written
in English, which were published in EREPS website during the previous year.
The Journal publishes short articles (up to 3000 words) related to original research,
review papers, expert opinion, technical notes, practice updates, and ethical and
legal commentaries. Articles will provide evidence-based information that is of
immediate use to practitioners. Each article includes a 150-250 words abstract,
with open access to general public. This abstract is also in English but there is the
option of including another abstract written in the author(s) native language(s).
Instructions for authors:
Title (up to 20 words): verdana, 12 pts, 1.5 spaces, justified, bold case
(e.g., The Fitness Sector gets a new publication)
Type of article: original research, review papers, expert opinion, technical
notes, practice updates, ethical and legal commentary
Author(s) name(s): verdana, 10 pts, 1.5 spaces, justified, bold case (e.g.,
Maria Smith)
Affiliation(s): Health Club (…), University (…)
Country(ies)
Contact(s): e-mail address
Key-words (up to 6)
Second language abstract (if applicable): (yes/no), which one?
Main text (up to 3000 words): verdana, 10 pts, 1.5 spaces, justified
Sections: introduction, objectives, methods, discussion, practical
applications / background, discussion, implications for practice

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
113
References in text using [number]
Original figures (up to six)
Tables (up to two)
References (Vancouver style), e.g., Smith M, The Fitness Sector gets a new
publication. EuropeActive’s Journal for Exercise Professionals, 2016, vol 1
Short resumé of authors (up to 100 words)
Submission Process:
Manuscripts must be submitted in a word file, as an attachment to the e-mail:
[email protected]. If the Editors find that the submitted manuscript
is of sufficient quality and falls within the scope of the European Journal for
Exercise Professionals, they will assign the manuscript to a minimum of one and
a maximum of two peer-reviewers.
The reviewers submit their reports on the manuscripts along with their
recommendation of one of the following actions to the Editors:
Publish Unaltered
Consider after Minor Changes
Consider after Major Changes
Reject
After reviewers submit their reports, the Editors can make one of the following
editorial recommendations:
Publish Unaltered - the manuscript is accepted for publication
Consider after Minor/Major Changes - the authors are notified to revise their
manuscripts and submit a final copy of their manuscript with the required
changes suggested by the reviewers. The Editors review the revised
manuscript after the changes have been made by the authors. Once the
Editors agree with the final manuscript, it is accepted for publication
Reject - the Editors can reject any manuscript because of inappropriateness
of its subject, lack of quality, or if two of the reviewers recommend rejecting
the manuscript
Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
114
Article Processing Charges:
The European Journal for Exercise Professionals is an Open Access journal for
EREPS members. The abstract of the article is open for general public. Publishing
an article is free for the authors. Each year volume will be freely available for
download.
Please, submit your manuscript in a word file, as an attachment to this e-mail
address: [email protected]

Issue 1 - 2017
ISSN: 2522-1310 ©Copyright EuropeActive 2017
115
OTHER PUBLICATIONS BY EUROPEACTIVE