Embed Size (px)
Citation preview
CLINICAL TECHNICAL NOTE
Isometric knee extension force measured using ahandheld dynamometer with and withoutbelt-stabilization
Richard W Bohannon, PT, DPT, EdD, NCS, FAPTA, FAFA, FASNR,1 Jeffrey Kindig, SPT,BS,2 Gregory Sabo, SPT, BS,2 Allison E Duni, SPT, BS,2 and Peter Cram, SPT, BA2
1Professor, Physical Therapy Program, Department of Kinesiology, NEAG School of Education,University of Connecticut, Storrs, CT, USA2Graduate Student, Physical Therapy Program, Department of Kinesiology, NEAG School of Education,University of Connecticut, Storrs, CT, USA
ABSTRACT
Although evidence suggests that tester strength limits the magnitude of isometric force that can be measuredusing a handheld dynamometer (HHD), previous studies have not investigated the actual limits of force magni-tude that can be measured by trained testers when a belt is or is not used to stabilize the dynamometer.Therefore, the primary aims of this study were to determine: 1) the magnitude of knee extension forces thatcould be measured with a HHD with and without belt-stabilization and 2) the relationship between tester charac-teristics and knee extension strength measured with and without belt-stabilization. The characteristics of 20trained testers (10 men, 10 women) were determined. Thereafter, they measured isometric knee extensionstrength using the MicroFET HHD with and without belt-stabilization. Paired t-tests were used to compare maxi-mal knee extension forces under two conditions. Pearson product–moment correlations were calculated to deter-mine the relationship between tester characteristics and knee extension forces measured under the twoconditions. Knee extension forces (Newtons) measured using the HHD without belt-stabilization (470.6 ±179.8) were significantly lower (t =−7.968, p < 0.001) than those measured with belt-stabilization (866.9 ±131.7). Pearson correlations between tester characteristics and knee extension forces measured with no belt-stabilization were all statistically significant ( p≤ 0.002); however, the correlations were not statistically significantunder the belt-stabilization condition. The forces that can be measured with a HHD are higher than thosesuggested by previous researchers. By rectifying limitations imposed by tester strength, use of a belt allowsvery high knee extension forces to be measured.
INTRODUCTION
Handheld dynamometry is well established as a pro-cedure for measuring muscle strength (Bohannon,2006). Nevertheless, inadequate tester strength hasbeen identified as a potential threat to the validityof measurements obtained with a handheld dynam-ometer (HHD) (Wikholm and Bohannon, 1991).
As a consequence, numerous investigators havecautioned against using the procedure to measureforces generated by the lower limbs (Agre et al,1987) or forces in excess of certain limits (Becket al, 1999; Beenakker, van der Hoeven, Fock, andMaurits, 2001 Brinkmann, 1994; Martin et al,2006; Mulroy, Lassen, Chambers, and Perry, 1997;Nollet and Beelen, 1999; Roebroeck, Harlaar, andLankhorst, 1998; van der Hoeven, Fock, andMaurits, 2001; Van der Ploeg, Fidler, and Ooster-huis, 1991; Visser et al, 2003; Wadsworth et al,1992; Wikholm and Bohannon, 1991). Other inves-tigators have sought to ameliorate the issue of testerstrength by using belt-stabilization of the
Address correspondence to Richard W Bohannon, Physical TherapyProgram, Department of Kinesiology, NEAG School of Education,University of Connecticut, Storrs, CT, USA. E-mail: [email protected]
Accepted for publication 18 October 2011
Physiotherapy Theory and Practice, 28(7):562–567, 2012Copyright © Informa Healthcare USA, Inc.ISSN: 0959-3985 print/1532-5040 onlineDOI: 10.3109/09593985.2011.640385
562
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
9/14
For
pers
onal
use
onl
y.

dynamometer (Bohannon et al, 2011; Katoh andYamasaki, 2009a; Katoh and Yamasaki, 2009b;Katoh, Isozaki, Sakanoue, and Miyahara, 2010;Katoh, Isozaki, Sakanoue, and Miyahara, 2011).Although numerous researchers have noted thattesters are limited in the magnitude of forces theycan measure with a HHD (Table 1), the actual mag-nitude of forces that can be measured by trainedtesters has not been delineated experimentally.Moreover, it is unclear how the forces obtainedwith a HHD not stabilized by a belt compare
with those obtained with a HHD stabilized by abelt. The relationship of tester characteristics (mostnotably strength) and forces measured with a HHDhas received only limited attention (Mulroy,Lassen, Chambers, and Perry, 1997; Wadsworthet al, 1992). Therefore, the primary purpose ofthis study was to describe and compare the magni-tude of knee extension forces measured with aHHD, both with and without belt-stabilization.The secondary purpose was to determine therelationships between tester characteristics and knee
TABLE 1 Findings of studies addressing the limitations of handheld dynamometry (HHD) for measuring muscle strength.
Study Participants Findings
Beck et al (1999) Patients with amyotrophiclateral sclerosis
When forces exceed 196 N, HHD tends to underestimate actualforce relative to those obtained with a fixed force gauge.HHD recommended only in cases of “clinically evidentweakness” and when forces do not surpass 196 N
32 men, 11 womenAge (range): 29–77 years
Beenakker, van der Hoeven,Fock, and Maurits (2001)
Normal children Upper limit of HHD estimated to be 500 N139 boys, 131 girlsAge (range): 4–16 years
Brinkmann (1994) Patients with neuromusculardisease
Compared with a fixed force gauge, HHDmay only be reliable up to147 N of force
9 men, 12 womenAge (mean): 39–72 years
Martin et al (2006) Healthy individuals Compared with an isokinetic dynamometer, HHD underestimatedknee extension torque an average 14.5 Nm. Differences were“increasingly more apparent” with stronger participants. Strengthof the tester “relative to the participant is an importantconsideration, particularly when measuring larger muscle groupssuch as the quadriceps femoris”
9 men, 11 womenAge (range): 61–81 years
Mulroy, Lassen, Chambers,and Perry (1997)
Patients with post-poliosyndrome
Women, whose push forces were significantly less than men’s, alsoobtained significantly lower knee extension force measurementsthan men (166.8 vs. 341.6 N)7 men, 12 women
Age (mean): 56.8 yearsNollet and Beelen (1999) Patients with post-polio
syndromeComparing knee extension forces measured with a fixed force gauge
to those obtained with HHD, a good correlation was obtainedonly up to 200 N. The authors estimated that the upper limit forreliable HHD testing is 160 N
16 men, 33 womenAge (mean): 45.8 years
Roebroeck, Harlaar, andLankhorst (1998)
Healthy adults Limited force of a therapist is a problem in testing relatively strongmuscle groups such as the knee extensors30 men, 28 women
Age (range): 13–77 yearsvan der Ploeg, Fidler, and
Oosterhuis (1991)Healthy adults “Measuring the knee extensors could not be done carefully beyond
160 N” Measuring values higher than 250 N is not clinicallyuseful because “the patient will not have many complaints orfunctional restrictions”
50 men, 50 womenAge (range): 20–60 years
Visser et al (2003) Patients with progressive lowermotor neuron syndrome
Compared with a fixed force gauge, HHD underestimated forcesbeyond 250 N, “probably due to limited strength of the tester”
11 men, 8 womenAge (range): 37–71 years
Wadsworth et al (1992) Healthy individuals Women testers had difficulty with dynamometer stabilization whentesting knee extension and elbow flexion strength. The mean kneeextension torque measured by women (97.6 N) was less than thatmeasured by men (118.3 N)
1 man, 1 womanAge 24 years
Wikholm and Bohannon(1991)
Healthy adults Beyond 120N, tester strength becomes an important determinant ofthe magnitude and reliability of measured forces5 men, 22 women
Age (mean): 31 years
Physiotherapy Theory and Practice 563
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
9/14
For
pers
onal
use
onl
y.
extension forces measured with and without belt-stabilization.
METHODS
This descriptive and explicatory study was approvedby the Institutional Review Board of the Universityof Connecticut. All participants (testers), who wereentry-level physical therapy students, providedwritten informed consent. All 20 (10 women, 10men) were trained in use of the HHD, with andwithout belt-stabilization, by the same instructor. Fur-thermore, they participated in a review training sessionprior to performing tests for this study. Before doingany testing, selected tester characteristics were deter-mined. Specifically, tester heights and masses weremeasured. Thereafter, a sense of the participants’strength was obtained by: 1) measuring theirmaximal push force with a periodically calibratedMicroFET2 HHD (Hoggan Health Industries, WestJordan, UT, USA), while they assumed a positionsimilar to that used in testing (Figure 1) and 2)measuring their right (dominant) grip force with aperiodically calibrated Jamar hand dynamometer(AllegroMedical, Bolingbrook, IL, USA).
All testing was against the efforts of two males (23years) who were selected because of their ability togenerate forces likely to challenge a tester. Both wereengaged in weight-training regimens. Neither
reported any previous or current lower extremityinjury. Each was over 1.7 m in height and had abody mass of over 80 kg. Their grip strengths weremore than 125 N above the average of men of theirage (Bohannon et al, 2006).
FIGURE 1 Photograph showing the measurement of a tester’smaximum push force with a HHD.
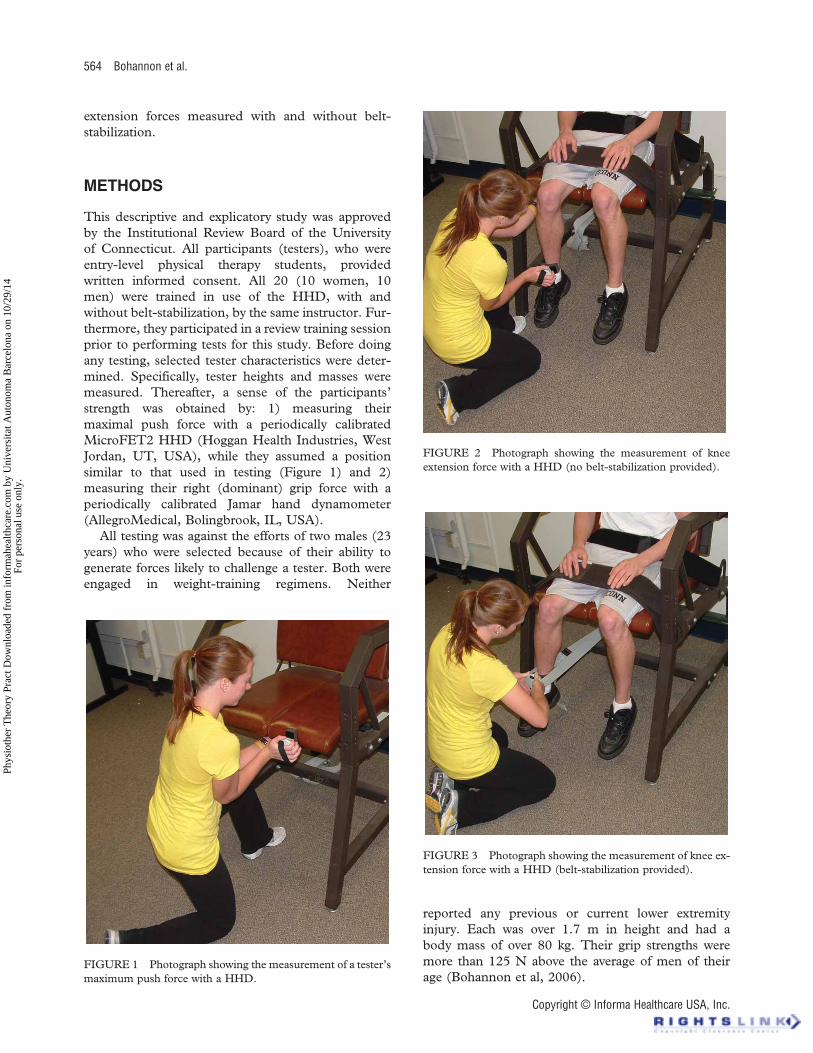
FIGURE 2 Photograph showing the measurement of kneeextension force with a HHD (no belt-stabilization provided).
FIGURE 3 Photograph showing the measurement of knee ex-tension force with a HHD (belt-stabilization provided).
564 Bohannon et al.
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
9/14
For
pers
onal
use
onl
y.
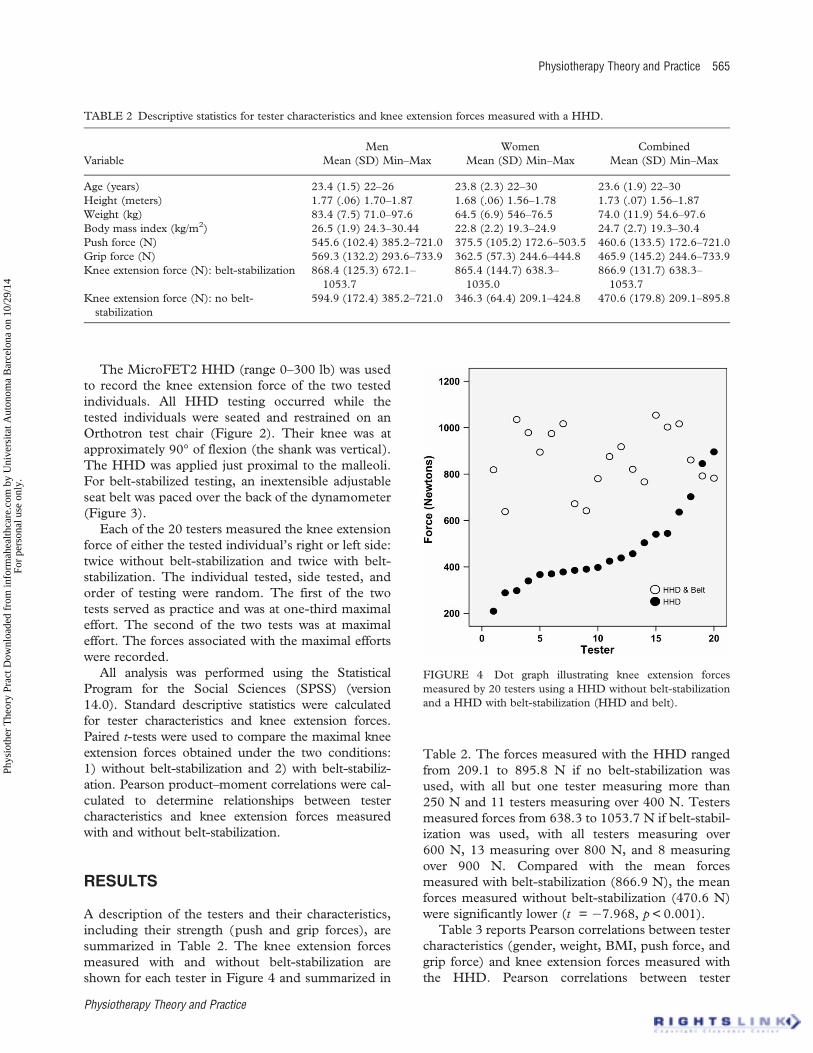
The MicroFET2 HHD (range 0–300 lb) was usedto record the knee extension force of the two testedindividuals. All HHD testing occurred while thetested individuals were seated and restrained on anOrthotron test chair (Figure 2). Their knee was atapproximately 90° of flexion (the shank was vertical).The HHD was applied just proximal to the malleoli.For belt-stabilized testing, an inextensible adjustableseat belt was paced over the back of the dynamometer(Figure 3).
Each of the 20 testers measured the knee extensionforce of either the tested individual’s right or left side:twice without belt-stabilization and twice with belt-stabilization. The individual tested, side tested, andorder of testing were random. The first of the twotests served as practice and was at one-third maximaleffort. The second of the two tests was at maximaleffort. The forces associated with the maximal effortswere recorded.
All analysis was performed using the StatisticalProgram for the Social Sciences (SPSS) (version14.0). Standard descriptive statistics were calculatedfor tester characteristics and knee extension forces.Paired t-tests were used to compare the maximal kneeextension forces obtained under the two conditions:1) without belt-stabilization and 2) with belt-stabiliz-ation. Pearson product–moment correlations were cal-culated to determine relationships between testercharacteristics and knee extension forces measuredwith and without belt-stabilization.
RESULTS
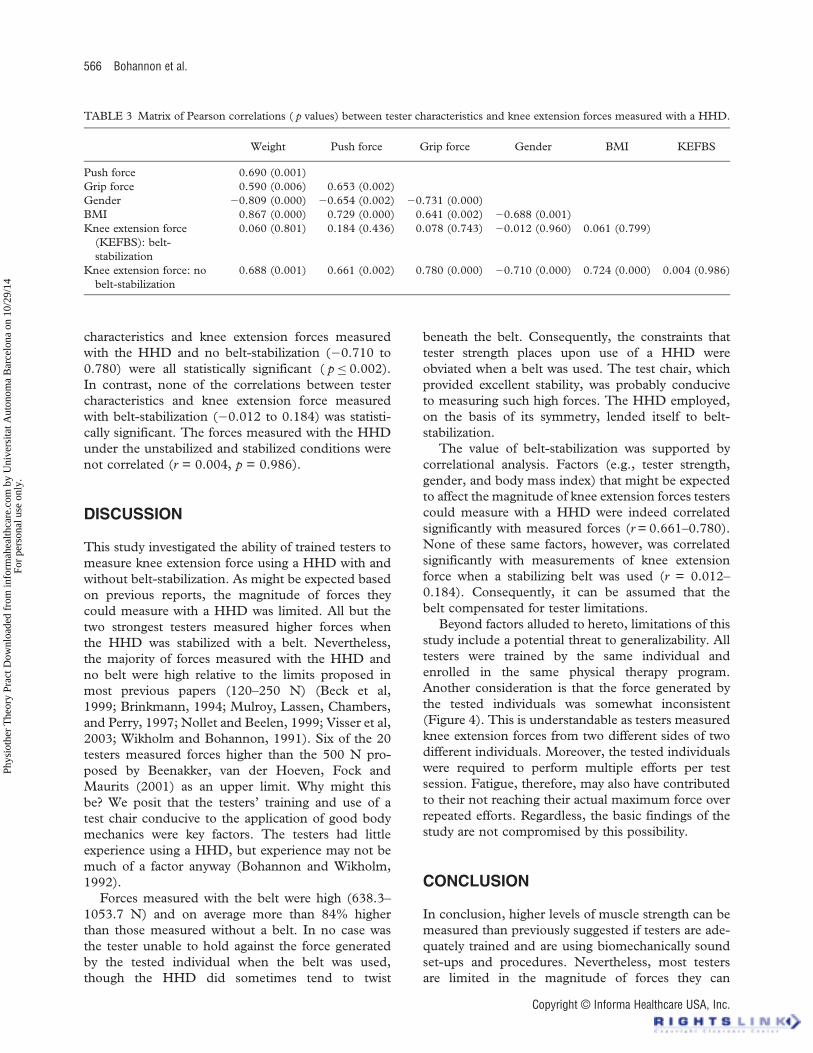
A description of the testers and their characteristics,including their strength (push and grip forces), aresummarized in Table 2. The knee extension forcesmeasured with and without belt-stabilization areshown for each tester in Figure 4 and summarized in
Table 2. The forces measured with the HHD rangedfrom 209.1 to 895.8 N if no belt-stabilization wasused, with all but one tester measuring more than250 N and 11 testers measuring over 400 N. Testersmeasured forces from 638.3 to 1053.7 N if belt-stabil-ization was used, with all testers measuring over600 N, 13 measuring over 800 N, and 8 measuringover 900 N. Compared with the mean forcesmeasured with belt-stabilization (866.9 N), the meanforces measured without belt-stabilization (470.6 N)were significantly lower (t = −7.968, p < 0.001).
Table 3 reports Pearson correlations between testercharacteristics (gender, weight, BMI, push force, andgrip force) and knee extension forces measured withthe HHD. Pearson correlations between tester
TABLE 2 Descriptive statistics for tester characteristics and knee extension forces measured with a HHD.
VariableMen Women Combined
Mean (SD) Min–Max Mean (SD) Min–Max Mean (SD) Min–Max
Age (years) 23.4 (1.5) 22–26 23.8 (2.3) 22–30 23.6 (1.9) 22–30Height (meters) 1.77 (.06) 1.70–1.87 1.68 (.06) 1.56–1.78 1.73 (.07) 1.56–1.87Weight (kg) 83.4 (7.5) 71.0–97.6 64.5 (6.9) 546–76.5 74.0 (11.9) 54.6–97.6Body mass index (kg/m2) 26.5 (1.9) 24.3–30.44 22.8 (2.2) 19.3–24.9 24.7 (2.7) 19.3–30.4Push force (N) 545.6 (102.4) 385.2–721.0 375.5 (105.2) 172.6–503.5 460.6 (133.5) 172.6–721.0Grip force (N) 569.3 (132.2) 293.6–733.9 362.5 (57.3) 244.6–444.8 465.9 (145.2) 244.6–733.9Knee extension force (N): belt-stabilization 868.4 (125.3) 672.1–
1053.7865.4 (144.7) 638.3–1035.0
866.9 (131.7) 638.3–1053.7
Knee extension force (N): no belt-stabilization
594.9 (172.4) 385.2–721.0 346.3 (64.4) 209.1–424.8 470.6 (179.8) 209.1–895.8
FIGURE 4 Dot graph illustrating knee extension forcesmeasured by 20 testers using a HHD without belt-stabilizationand a HHD with belt-stabilization (HHD and belt).
Physiotherapy Theory and Practice 565
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
9/14
For
pers
onal
use
onl
y.
characteristics and knee extension forces measuredwith the HHD and no belt-stabilization (−0.710 to0.780) were all statistically significant ( p≤ 0.002).In contrast, none of the correlations between testercharacteristics and knee extension force measuredwith belt-stabilization (−0.012 to 0.184) was statisti-cally significant. The forces measured with the HHDunder the unstabilized and stabilized conditions werenot correlated (r = 0.004, p = 0.986).
DISCUSSION
This study investigated the ability of trained testers tomeasure knee extension force using a HHD with andwithout belt-stabilization. As might be expected basedon previous reports, the magnitude of forces theycould measure with a HHD was limited. All but thetwo strongest testers measured higher forces whenthe HHD was stabilized with a belt. Nevertheless,the majority of forces measured with the HHD andno belt were high relative to the limits proposed inmost previous papers (120–250 N) (Beck et al,1999; Brinkmann, 1994; Mulroy, Lassen, Chambers,and Perry, 1997; Nollet and Beelen, 1999; Visser et al,2003; Wikholm and Bohannon, 1991). Six of the 20testers measured forces higher than the 500 N pro-posed by Beenakker, van der Hoeven, Fock andMaurits (2001) as an upper limit. Why might thisbe? We posit that the testers’ training and use of atest chair conducive to the application of good bodymechanics were key factors. The testers had littleexperience using a HHD, but experience may not bemuch of a factor anyway (Bohannon and Wikholm,1992).
Forces measured with the belt were high (638.3–1053.7 N) and on average more than 84% higherthan those measured without a belt. In no case wasthe tester unable to hold against the force generatedby the tested individual when the belt was used,though the HHD did sometimes tend to twist
beneath the belt. Consequently, the constraints thattester strength places upon use of a HHD wereobviated when a belt was used. The test chair, whichprovided excellent stability, was probably conduciveto measuring such high forces. The HHD employed,on the basis of its symmetry, lended itself to belt-stabilization.
The value of belt-stabilization was supported bycorrelational analysis. Factors (e.g., tester strength,gender, and body mass index) that might be expectedto affect the magnitude of knee extension forces testerscould measure with a HHD were indeed correlatedsignificantly with measured forces (r = 0.661–0.780).None of these same factors, however, was correlatedsignificantly with measurements of knee extensionforce when a stabilizing belt was used (r = 0.012–0.184). Consequently, it can be assumed that thebelt compensated for tester limitations.
Beyond factors alluded to hereto, limitations of thisstudy include a potential threat to generalizability. Alltesters were trained by the same individual andenrolled in the same physical therapy program.Another consideration is that the force generated bythe tested individuals was somewhat inconsistent(Figure 4). This is understandable as testers measuredknee extension forces from two different sides of twodifferent individuals. Moreover, the tested individualswere required to perform multiple efforts per testsession. Fatigue, therefore, may also have contributedto their not reaching their actual maximum force overrepeated efforts. Regardless, the basic findings of thestudy are not compromised by this possibility.
CONCLUSION
In conclusion, higher levels of muscle strength can bemeasured than previously suggested if testers are ade-quately trained and are using biomechanically soundset-ups and procedures. Nevertheless, most testersare limited in the magnitude of forces they can
TABLE 3 Matrix of Pearson correlations ( p values) between tester characteristics and knee extension forces measured with a HHD.
Weight Push force Grip force Gender BMI KEFBS
Push force 0.690 (0.001)Grip force 0.590 (0.006) 0.653 (0.002)Gender −0.809 (0.000) −0.654 (0.002) −0.731 (0.000)BMI 0.867 (0.000) 0.729 (0.000) 0.641 (0.002) −0.688 (0.001)Knee extension force
(KEFBS): belt-stabilization
0.060 (0.801) 0.184 (0.436) 0.078 (0.743) −0.012 (0.960) 0.061 (0.799)
Knee extension force: nobelt-stabilization
0.688 (0.001) 0.661 (0.002) 0.780 (0.000) −0.710 (0.000) 0.724 (0.000) 0.004 (0.986)
566 Bohannon et al.
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
9/14
For
pers
onal
use
onl
y.
legitimately measure. Belt-stabilizing testing can over-come these limitations even among tested individualswho are very strong. Consequently, belt-stabilizedtesting is recommended if valid measurements ofknee extension force are to be obtained from strongindividuals.
Declaration of interest: The authors report noconflicts of interest. The authors alone are responsiblefor the content and the writing of the paper.
REFERENCES
Agre JC, Magness JL, Hull SZ, Wright KC, Baxter TL, Patterson R,Stradel L 1987 Strength testing with a portable dynamometer:Reliability for upper and lower extremities. Archives of PhysicalMedicine and Rehabilitation 68: 454–458
Beck M, Giess R, Wurffel W, Magnus T, Ochs F, Toyka K 1999Comparison of maximal voluntary isometric contraction andDrachman’s hand-held dynamometry in evaluating patientswith amyotrophic lateral sclerosis. Muscle and Nerve 22:1265–1270
Beenakker EAC, van der Hoeven JH, Fock JM, Maurits NM 2001Reference values of maximum isometric muscle force obtainedin 270 children aged 4–16 years by hand-held dynamometry.Neuromuscular Disorders 11: 441–446
Bohannon RW 2006 Hand-held dynamometry: Adoption1900–2005. Perceptual and Motor Skills 103: 3–4
Bohannon RW, Bubela DJ, Wang Y-C, Magasi SR, Gershon RC2011 Adequacy of belt-stabilized testing of knee extensionstrength. Journal of Strength and Conditioning Research 25:1963–1967
Bohannon RW, Peolsson A, Massy-Westropp N, Desrosiers J,Bear-Lehman JB 2006 Reference values for adult grip strengthmeasured with a Jamar dynamometer: A descriptive meta-analysis. Physiotherapy 92: 11–15
Bohannon RW, Wikholm J 1992 Measurement of knee extensionforce obtained by two examiners of substantially different experi-ence with a hand-held dynamometer. Isokinetics and ExerciseScience 2: 5–8
Brinkmann JR 1994 Comparison of a hand-held and fixed dynam-ometer in measuring strength of patients with neuromusculardisease. Journal of Orthopaedic and Sports Physical Therapy19: 100–104
Katoh M, Isozaki K, Sakanoue N, Miyahara T 2010 Reliability ofisometric knee extension muscle strength measurement using a
hand-held dynamometer with a belt: A study of test–retestreliability in healthy elderly subjects. Journal of PhysicalTherapy Science 22: 359–363
Katoh M, Isozaki K, Sakanoue N, Miyahara T 2011 Reliability ofisometric knee extension muscle strength measurement using ahand-held dynamometer and a belt: Study of hemiplegicpatients. Journal of Physical Therapy Science 23: 25–28
Katoh M, Yamasaki H 2009a. Comparison of reliability of isometricleg muscle strength measurements made using a hand-helddynamometer with and without a restraining belt. Journal ofPhysical Therapy Science 21: 37–42
Katoh M, Yamasaki H 2009b. Test–retest reliability of isometric legmuscle strength measurements made using a hand-helddynamometer restrained by a belt: Comparisons during andbetween sessions. Journal of Physical Therapy Science 21:239–243
Martin HJ, Yule V, Syddall HE, Dennison EM, Cooper C, SayerAA 2006 Is hand-held dynamometry useful for the measurementof quadriceps strength in older people? A comparison withthe gold standard Biodex dynamometry. Gerontology 52:154–159
Mulroy SJ, Lassen KD, Chambers SH, Perry J 1997 The ability ofmale and female clinicians to effectively test knee extensionstrength using manual muscle testing. Journal of Orthopaedicand Sports Physical Therapy 26: 192–199
Nollet F, Beelen A 1999 Strength assessment in postpolio syn-drome: Validity of a hand-held dynamometer in detectingchange. Archives of Physical Medicine and Rehabilitation 80:1316–1323
RoebroeckME, Harlaar J, Lankhorst GJ 1998 Reliability assessmentof isometric knee extension measurements with a computer-assisted hand-held dynamometer. Archives of Physical Medicineand Rehabilitation 79: 442–448
Van der Ploeg RJO, Fidler V, Oosterhuis HJGH 1991 Hand-heldmyometry: Reference values. Journal of Neurology Neurosur-gery and Psychiatry 54: 244–247
Visser J, Mans E, de Visser M, van den Berg-Vos RM, Franssen H,de Jong JMBV, van den Berg LH, Wokke JHJ, de Haan RJ 2003Comparison of maximal voluntary isometric contraction andhand-held dynamometry in measuring muscle strength ofpatients with progressive lower motor neuron syndrome. Neuro-muscular Disorders 13: 744–750
Wadsworth CT, Nielsen DH, Corcoran DS, Phillips CE, SannesTL 1992 Interrater reliability of hand-held dynamometry:Effects of rater gender, body weight, and grip strength.Journal of Orthopaedic and Sports Physical Therapy 16:74–81
Wikholm JB, Bohannon RW 1991 Hand-held dynamometermeasurements: Tester strength makes a difference. Journal ofOrthopaedic and Sports Physical Therapy 13: 191–198
Physiotherapy Theory and Practice 567
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsita
t Aut
onom
a B
arce
lona
on
10/2
9/14
For
pers
onal
use
onl
y.





























