Embed Size (px)
Citation preview

Isolated tuberculosis of the vastus lateralis muscle: A case report
VIVEK TRIKHA, MANISH KUMAR VARSHNEY & SHISHIR RASTOGI
From the Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi, India
AbstractTuberculosis is 1 of the most deadly diseases in the world. With an increase in the incidence of HIV worldwide, tubercularinfections at unusual sites are being reported. Skeletal muscle tuberculosis without bony involvement is an extremely rarepresentation of tuberculosis. A case of isolated tuberculosis of the vastus lateralis muscle without any evident primary focusin a 30-y-old immunocompetent female is presented.
Introduction
Tuberculosis remains a feared disease of mankind
even in the 21st century. Musculoskeletal tubercu-
losis accounts for nearly 3% of all cases of
tuberculosis [1]. Tuberculosis of skeletal muscle
without coexisting skeletal lesion is extremely rare
with only few cases existing in English literature
[2�/8]. Most of these cases have been reported in
patients in an immunocompromized state or having
chronic illness. We report a rare case of tuberculosis
of the vastus lateralis muscle in an immunocompe-
tent female without any primary or contiguous
source of infection or any history of antibiotic
therapy.
Case report
A 30-y-old female presented with progressively
increasing swelling in the lateral aspect of distal right
thigh for the previous 4 months along with pain for
the last week. There was no history of trauma,
injection/ inoculation at the local site, intravenous
drug abuse or any blood transfusion. On examina-
tion a tender, firm mass of the size of small lemon
fixed to the underlying muscle of the distal lateral
thigh was found. There was no local redness or
warmth. The movements at knee and hip were full
with painful terminal flexion at the knee joint. No
associated inguinal lymphadenopathy or discharging
sinus was noted. There was no history of any
infectious condition or previous antibiotic therapy
in the previous 6 months. Her past medical and
surgical history was non-contributory with no family
history of tuberculosis or any history of contact.
CBC was normal with ESR being 24 mm/1st hour.
Radiographs of chest, knee joint including femur and
tibia were normal. Ultrasound revealed an oval
hypoechoic mass seen on lateral aspect of distal
left thigh with homogenous internal architecture
with associated adjacent muscle heterogenecity and
oedema (Figure 1), which was suggestive of infective
abscess or a parasitic cyst. Magnetic resonance
imaging (MRI) with multiple pulse sequences of
T1 and T2 relaxation demonstrated soft tissue
intensity lesion and areas of liquefaction and necrosis
on a localized area of lower thigh in the region of the
lower part of the vastus lateralis muscle without any
osseous or joint involvement. The size of lesion was
approx. 48 mm x 34 mm (Figure 2).
Drainage of the abscess was performed and the
tissue obtained was sent for bacterial, fungal and
AFB staining along with examination for parasite,
which all reported negative. The histopathological
examination revealed the presence of necrotizing
epithelioid granulomas compatible with tuberculo-
sis. The radiometric AFB culture report for tuber-
cular pathogen was positive. Myco-3 DNA PCR
identified the species to be Mycobacterium tubercu-
losis . The patient was started on standard multi-
drug anti-tubercular therapy (ATT) with 4 drugs
(EHRZ) for an initial 3 months followed by 2 drugs
(RH) alone for next 9 months. The swelling
disappeared after drainage and there was no pain
at the local site. Two years later, the patient remains
asymptomatic with pain-free full movements at the
knee.
Discussion
Tuberculosis has staged a remarkable comeback
today following HIV infected cases. Around 8.8
million new cases of tuberculosis were diagnosed
in 2003 and there were 1.7 million deaths making
it 1 of the largest killers [9]. Unusual presentations
of tuberculosis are being increasingly diagnosed in
both immunocompromized and immunocompetent
hosts. Soft tissue infection, defined as the involve-
Correspondence: V. Trikha, L-381, Sarita Vihar, New Delhi 110076, India. Tel: �/91 11 26951052. E-mail: [email protected]
304 Case Reports
(Received 19 August 2005; accepted 22 August 2005)
ISSN 0036-5548 print/ISSN 1651-1980 online # 2006 Taylor & Francis
DOI: 10.1080/00365540500353267
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B G
iess
en o
n 11
/01/
14Fo
r pe
rson
al u
se o
nly.

ment of tenosynovium, bursa, muscle or deep fascia,
is an uncommon form of musculoskeletal tuber-
culosis [6]. It is usually associated with immunosup-
pressed patients.
There are very few reports in the English literature
of primary muscular tuberculosis without any in-
volvement of bone or in immunocompetent patients,
and its manifestations may mimic malignant or other
inflammatory diseases, leading to a faulty diagnosis
[2�/8]. Petter [10] recorded only 1 case of primary
muscular tuberculosis in over 6000 cases of all types
of tuberculosis giving an incidence of 0.015%.
Hence, as such isolated primary skeletal tuberculosis
without any associated involvement of the adjacent
bone or viscera is considered only a diagnosis of
exclusion over a soft tissue tumour or a pyogenic
abscess.
It is of interest to note that most of the reported
cases of extra-osseous muscular tuberculosis have
been reported adjacent to the joints or bursae
[2,6,7,10] or in immunocompromized individuals
[10,11]. The natural history of muscles primarily
involved in the disease process remains elusive [12];
however, extension from adjacent joint, bone, bur-
sae, tenosynovium and even direct inoculation have
all been proposed [2]. The primary focus subse-
quently heals leaving the evident infection in the
muscle. The exact cause of the tuberculous abscess
in our case remains unclear. The involvement of the
vastus lateralis in the presented case could be
ascribed to haematogenous spread or by extension
from nearby bursae. Haematogenous spread may
seem likely, as the prevalence of tuberculosis is fairly
high in our region, with nearly 40% of the total
population being infected with tubercle bacilli in
1 form or another. However, primary haematogen-
ous spread to muscles is an unlikely proposition
owing to previously presented reasons [12]. The
possibility of the infection arising in the adjacent
bursae around the knee and then becoming localized
to the vastus lateralis muscle hence appears to be the
more likely cause. This gains credence in the
presence of nearly 13 bursae around the knee
joint and absence of any adjacent skeletal involve-
ment or previous history of pulmonary or other
form of tuberculosis, or any history of trauma or
direct inoculation.
In the present world, an atypical presentation of
tuberculosis is on the increase. The ongoing pan-
demic of HIV/AIDS further contributes to the ever-
increasing incidence of this disease. The once
forbidden tissues/organs for tuberculosis are no
longer immune from the vagaries of atypical tuber-
culosis. All physicians should have adequate knowl-
edge of tuberculosis and awareness of its atypical
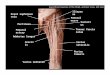
Figure 2. MRI shows altered signal intensity in soft tissue in
lateral aspect of the lower part of the left femur, involving the
vastus lateralis muscle. These appear hyperintense on T2/STIR
and hypointense on T1W images. A few areas of liquefactive
necrosis are also seen within the lesion. No osseous involvement is
seen. Visualized parts of lower femur/patella, upper tibia are
normal
Figure 1. Ultrasound of the distal thigh reveals a hypoechoic
region in the lateral muscle group of the thigh with homogenous
internal architecture. The possibilities of infective lesion or
parasitic cyst can be made on the ultrasound.
Case Reports 305
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B G
iess
en o
n 11
/01/
14Fo
r pe
rson
al u
se o
nly.

presentations to ensure proper management of such
patients.
References
[1] Enarson DA, Fujii M, Nakielna EM, Grzybowski S. Bone
and joint tuberculosis: a continuing problem. Can Med
Assoc J 1979;/120:/139�/45.
[2] Abdelwahab IF, Kenan S. Tuberculous abscess of the
brachialis and biceps brachii muscles without osseous
involvement. A case report. J Bone Joint Surg Am 1998;/80:/
1521�/4.
[3] Abu-Salem OT. Tuberculous abscesses of the quadriceps
femoris muscle without osseous involvement. East Mediterr
Health J 2000;/6:/1136�/8.
[4] Bakshi G, Satish R, Shetty SV, Anjana J. Primary skeletal
muscle tuberculosis. Orthopedics 2003;/26:/327�/8.
[5] Haycock JB, Noble TC. Four cases of syringe-transmitted
tuberculosis. Tubercle 1961;/42:/25�/7.
[6] Puttick MPE, Stein HB, Chan RMT, Elwood RK, How AR,
Reid GD. Soft tissue tuberculosis: a series of 11 cases.
J Rheumatol 1995;/22:/1321�/5.
[7] Seber S, Kose N. Tuberculous abscess of the brachialis and
biceps brachii muscles without osseous involvement. A case
report. J Bone Joint Surg Am 1999;/81:/1788.
[8] Trikha V, Gupta V. Isolated tuberculous abscess in biceps
brachii muscle of a young male. J Infect 2002;/44:/265�/6.
[9] Global tuberculosis control: surveillance, planning, finan-
cing. WHO report 2005. Geneva, World Health Organiza-
tion (WHO/HTM/TB/2005.349)
[10] Petter CK. Some thoughts on tuberculosis of fascia and
muscle. Lancet 1937;/57:/156�/9.
[11] Wang JY, Lee LN, Hsueh PR, Shih JY, Chang YL, Yang PC,
Lu KT. Tuberculous myositis: a rare but existing clinical
entity. Rheumatology 2003;/42:/836�/40.
[12] Gahlaut DS, Nath K, Sikka KK, Singh KN, Samuel KC.
Generalized skeletal muscle tuberculosis. J Indian Med
Assoc 1973;/61:/92�/4.
Severe disseminated tuberculosis in a 4-month-old infant initiallypresenting with multiform cutaneous lesions
NIKOS SPYRIDIS1,2, HELENI GEORGOULI2, THEANO TSOUKATOU2, IRINI SAKOU2,
MARIA TSOLIA2, NIKOS MIRIOKEFALITAKIS2 & PANAYIOTIS SPYRIDIS2
From the 1Department of General Paediatrics, St Thomas’ Hospital, London, UK, and 2Second Department of Paediatrics of
the University of Athens, TB Clinic for Children, Aglaia Kyriakou Children’s Hospital, Athens, Greece
AbstractA 4-month-old female infant presented with 1 month history of horizontal nystagmus and discrete multiform skin lesions.The patient was initially diagnosed with congenital nystagmus and staphylococcal skin infection not responding toantimicrobial agents. The development of severe systemic symptoms led to extensive investigations and the diagnosis ofdisseminated tuberculosis. Mycobacterium tuberculosis (MTB) was isolated from the skin and cerebrospinal fluid. Thepatient was treated with isoniazid, rifampicin, pyrizinamide, streptomycin and dexamethasone. Skin lesions resolvedcompletely but severe neurological deficits persisted.
Case report
A 4-month old female infant born in Athens
of Sudanese parents presented with a 1- month
history of horizontal nystagmus and multiform skin
lesions involving the entire body. She was born at 40
weeks gestation after an uncomplicated pregnancy,
labour and delivery. The baby had not received
any vaccination and no other significant past medical
or family history was noted. Skin lesions were
initially popular, then vesicular with serous fluid
production and were diagnosed as staphylococcal
skin infection by the local hospital. She was also
seen by a paediatric ophthalmologist who considered
the nystagmus to be congenital and a follow-
up appointment was offered. Two weeks after
the initiation of anti-staphylococcal treatment no
significant improvement was noticed and a second
course was given. The development of more
systemic symptoms led to the referral to our
clinic.
Correspondence: N. Spyridis, 46 St Petersburgh Place, London W2 4LD, UK. Tel: �/00 44 2072290898. E-mail: [email protected]
306 Case Reports
(Received 10 July 2005; accepted 9 August 2005)
ISSN 0036-5548 print/ISSN 1651-1980 online # 2006 Taylor & Francis
DOI: 10.1080/00365540500361310
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
B G
iess
en o
n 11
/01/
14Fo
r pe
rson
al u
se o
nly.