Embed Size (px)
Citation preview

Remote monitoring and“Tele-orthodontics”: Concept, scopeand applications
Ismaeel Hansa, Steven J. Semaan, Nikhilesh R. Vaid, and Donald J. FergusonResidentCollege, Unipean UniverUniversity NGold Coast,College, DubaFloor, Office 3
Correspo
© 20181073-87https://d
470
Tele-orthodontics is a broad term that encompasses remote provision of
orthodontic care, advice, or treatment via information technology. The Pur-
poses of the article were two-fold: (1) to review the rather new concept,
applications and scope of teleorthodontics, and (2) to present preliminary
results of a study with and without Dental MonitoringTM (DM) usage on
appointment efficiency, patient perspectives and patient demographics. The
sample was comprised of 74 consecutively treated Invisalign� patients using
DMTM and 85 consecutively completed Invisalign� patients. An online ques-
tionnaire was given to the DMTM group to assess the patients’ perspective
on the ease of use and benefit to treatment experience using a 5-point Likert
scale. Also requested was a list of 5 benefits and problems while using
DMTM. Independent t-tests were used to determine any inter-group differen-
ces in, number of appointments and age; a chi-square test was used for dif-
ferences between genders. Significance was set at P� 0.05. Mean number of
appointments was significantly lower by 1.68 appointments for DM com-
pared to control (P< 0.001). Age averaged 3.2 years younger for the DM
group (P< 0.05). More males used DM than the control group (31.6% vs
16.7%, P< 0.05, respectively). The mean Likert scale rating for “ease of use”
was 4.31 out of 5.0, while benefit to treatment experience rating was 4.4.
The most oft-mentioned perceived benefits were “better communication”
(47 times), “increased convenience” (44 times), “reduced number of appoint-
ments” (40 times), and “ease of use” (38 times). The most oft-mentioned
problems were related to the “difficulty of taking scans” (27 times) and
“reduced communication” (12 times). Preliminary study results suggest the
number of appointments may be reduced with Dental Monitoring. In addi-
tion, there was a positive patient perception on the use of DM. (Semin
Orthod 2018; 24:470–481) © 2018 Elsevier Inc. All rights reserved.
Introduction
T ele-orthodontics is a broad term that encom-passes remote provision of orthodontic care,
advice, or treatment through the medium of
, Advanced Orthodontic Program, European Universityted Arab Emirates; Department of Orthodontics, Euro-sity College, Dubai, UAE; Department of Orthodontics,evada Las Vegas, USA; Orthodontist Private Practice,Australia; Orthodontic Department, European Universityi Healthcare City, UAE, Ibn Sina Building, BlockD, 3rd02, Dubai PO Box 53382, United Arab Emirates.nding author. E-mail: [email protected]
Elsevier Inc. All rights reserved.46/12/1801-$30.00/0oi.org/10.1053/j.sodo.2018.10.011
Seminars in Orthodontics, Vol 24
information technology, rather than direct personalcontact. A simple and relevant example is an ortho-dontist seeking advice from colleagues by sharingdigital records and communicating over the Inter-net. Less commonly, tele-orthodontic consults andtreatments have been reported in conjunction withgeneral dentists in order to facilitate orthodontictreatment.1,2 In the early to mid-2000s, promisingresults were achieved by orthodontists supervisinggeneral dental practitioners in real time to provideorthodontic services to patients with limited accessto orthodontic care.1,3 Simple remote monitoringof patients during the retention period has alsobeen performed with patients sending pictures
, No 4, 2018: pp 470�481

Remote monitoring and tele-orthodontics 471
instead of travelling for in-office visits. The applica-tion of the “tele-orthodontics” concept however hasbeen limited thus far.
An important premise for the development ofthe prescription appliances, customized appli-ance systems and clear aligner therapy (CAT),has been reduced chair-side time and lesser in-office visits.4�7 Efficiency is an important “buzz-word” in orthodontic practice management lex-icons.8�10 One of the pitfalls of traditionalorthodontics is the treating of patients based onestimates of a patient’s response to treatment.Generally, patients are required to have in-officevisits (or aligner changes) at preset intervals,which are average time frames applied to allpatients and not necessarily the ideal time-framespecific to the individual patient and treatmentrequirements. With the advent of tele-orthodon-tics, and more specifically remote monitoring,the scheduling of in-office visits can be personal-ized per patient, creating a supposedly more effi-cient workflow. This not only maximizesprofitability by reducing chair time, but alsoimproves patient convenience.
An important “application” (app) that facili-tates this technology is Dental MonitoringTM
(DM), which allows patients to accurately cap-ture their occlusion using a smart phone. Sincepeople are increasingly using smart phones and“apps” on them, orthodontic applications onthese platforms have also correspondinglyincreased.4,11 Scans made by a patient using asmart phone (photos or videos) are analyzed byDM and viewed by the orthodontist who is thenable to provide real-time monitoring of thepatient's treatment remotely. This is could beespecially important in areas with limited accessto orthodontic care. Similarly, those who travelfrequently or have busy schedules can benefittremendously from remote monitoring. Otherperceived advantages include earlier diagnoses,closer management through remote monitoring,savings in time and transportation costs andincreased convenience for patients.12 Remotepatient monitoring may also reduce overall treat-ment time via early interception of problemssuch as non-tracking aligners, debonded brack-ets or broken appliances, allowing for such prob-lems to be addressed promptly.
Tele-orthodontics may be used for all applian-ces, ranging from phase-1 devices to traditionalappliances to CAT, but may be more appropriate
in customized appliances that require less fre-quent in-office adjustments. The convenience ofreduced appointments may however be replacedby the inconvenience of submitting weekly scans,which can become frustrating or tedious as thescans sent may be rejected and require retaking.In addition, there may be a loss of rapport withthe orthodontist due to the diminished contacttime. Prior consent and training is necessary forthe patient before the start of treatment toensure better understanding and cooperation.
How Dental MonitoringTM works?
DMTM is a software-based program that allowspractitioners to remotely monitor patients’ treat-ment progress. It consists of three integratedplatforms: a mobile app for the patient, a pat-ented movement tracking algorithm and a web-based Doctor Dashboard where updates of thepatients’ progress are received (Fig. 1).
Mobile app: The DMTM app is currently avail-able for Android and iOS operating systems. Theapp guides the patient through the process oftaking the pictures with the dedicated cheekretractor on a schedule suggested by DMTM andrefined by the doctor according to the treatmentneeds (Fig. 2). The app allows the patient toreview their past photos, observe their treatmentprogress, practice in the demo mode, andreceive notifications from their doctor.
Patented movement tracking algorithm: Ini-tially, the 3D model of a patient’s dentition isuploaded to the Doctor Dashboard. This 3Dmodel serves as the initial reference point fortooth position. When the patient submits theirphoto exams, the pictures are uploaded to theservers and verified to ensure suitable quality tobe processed by the DMTM algorithm. Thereaf-ter, the algorithm is able to calculate individualtooth movements in all planes of space (Fig. 3).There is a claimed precision of less than 0.1 mmof movement and less than 0.5° for tip andtorque.13
Online Doctor Dashboard: The Doctor Dash-board is completely web-based and does notrequire additional software. After the analysis bythe algorithm is complete, the results arechecked by a team of DMTM doctors and arethen presented on the web-based Dashboard inthe form of graphs, photos and a 3D visualizationof current tooth position (called 3D Matching).

Figure 1. Dental Monitoring consists of three integrated platforms: a mobile application for the patient, a pat-ented movement tracking algorithm, and a web-based Doctor Dashboard.
472 Hansa et al
The orthodontist is notified immediately whennew results are available, or if any alerts or objec-tives have been detected, and can then commu-nicate with the patient through the app. Theclinician can set parameters to receive alerts in
Figure 2. Use of the Dental Monitoring mobile app, in add
circumstances that require attention, such asnon-tracking aligners, broken appliances or oralhygiene problems. Similarly, notifications can beset for specific objectives such as 2 mm overjet orclass I canines (Fig. 4).
ition to the calibrated cheek retractor, to take pictures.

Figure 3. Visualization of individual tooth movements in all planes of space, with a claimed accuracy of 0.1 mmlinearly, and 0.5° of tip and torque.
Figure 4. Alerts and notifications on the Doctor Dashboard.
Remote monitoring and tele-orthodontics 473

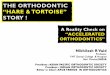
Fig. 5. The activity graph shows the overall movement of teeth in treatment or post-treatment stability.
474 Hansa et al
The activity graph helps to evaluate the activityof treatment or post-treatment stability (Fig. 5). Itallows the doctor to identify exactly how muchthe teeth have moved since the last photo exam.This can help determine when an archwire or analigner needs to be changed allowing for custom-ized treatment based on the patient’s individualbiological response. 3D Matching allows the doc-tor to visualize and replay tooth movement as anupdated 3D model of the teeth is created withevery photo exam taken by the patient. All photostaken by the patient with the DMTM applicationand the dedicated cheek retractor are availableon the Dashboard. Clinicians can easily comparethem with similar photos at different dates to visu-alize changes.
DMTM now provides four tiers of monitoring,varying in their uses and monthly costs, as follows:
Pre-treatment monitoring: Allows for anunlimited duration and can be used while wait-ing for tooth eruption or while using a phase-1device. The default frequency of photo exams isone photo every two months but is modifiableupon request.
Treatment monitoring: Allows for unlimitedtreatment duration and can monitor all types oftreatment including conventional, customizedvestibular or lingual appliances and CAT. Thedefault frequency of photo exams, modifiableupon request, is once a week for aligners and
one every two weeks for the other treatmenttypes. Treatment monitoring includes post treat-ment monitoring for two years.
Post treatment monitoring: Allows for 2-yearsto monitor post treatment stability. The defaultfrequency of photo exams changes with time i.e.a photo every week for the first month, onephoto per month for the next 6 months andthen one photo every 2 months for the remain-der of post treatment monitoring.
DM GoLiveTM: DM GoLiveTM is a patentedalgorithm supervised by the DMTM clinical teamthat detects non-tracking aligners.14 As opposedto fixed aligner changes, the patient receives aweekly “GO” or “NO-GO” notification from theDMTM app indicating whether they should moveto the next aligner or remain in the current one.The doctor is informed whenever a “NO-GO”
notification is sent, identifying the individualteeth that are not tracking as well as other unde-sirable situations such as poor oral hygiene; thedoctor can override NO-GO at any stage. Itshould be noted that DM GoLiveTM does nottrack individual tooth movement for 3D match-ing as do the other options.
Patient perception of DM - a pilot study
Preliminary data obtained from a private practicein the Gold Coast, Australia, has provided some

Remote monitoring and tele-orthodontics 475
insight into Dental Monitoring GoLiveTM and itsclinical applications. Claims of the company indi-cate shorter treatment times, reduced number ofappointments, reduced number of refinementsand increased communication. Unfortunately,there is currently no evidence-based data on theuse of DMTM or remote monitoring in general.Hence, the objective of this preliminary pilotstudy was to investigate the efficacy of DMTM andremote monitoring by determining if DMGoLiveTM reduces the number of appointmentsrequired compared to a control. Secondaryobjectives were to compare the demographicsbetween the two groups and to assess thepatients’ perspectives on using DMTM duringtreatment. The null hypotheses were as follows:There is no difference in the number of appoint-ments nor demographics between the DMTM
group and the control. The study was carried outindependently by the authors without any finan-cial assistance or funding from a third party thatcan constitute a conflict of interest.
The sample from a private practice in theGold Coast, Australia, comprised of 79 consecu-tively treated patients using DMTM in conjunc-tion with Invisalign� (experimental DMTM
group) and 94 consecutively completed patientsusing only Invisalign� (control group). Patientswere given the option of utilizing DMTM afterbeing informed about its pros and cons and weretreated at no additional cost if they chose to usethe app. After exclusions due to inadequaterecords, partial fixed appliances and auxiliaryappliances, five patients were excluded in theDMTM group (n = 74) and nine patients in thecontrol group (n = 85), resulting in a total samplesize of 159 subjects.
Since DMTM is a recent application, only threepatients had completed treatment in the experi-mental group, (mean treatment time was200.2§ 75.2 days) at the time of evaluation. Inorder to match the groups, we capped the
Table 1. Results of independent t-tests comparing Dentapatients for age, gender distribution, treatment length andity significance; n represents sample size; M:F represents m
n Age (in years) Genders (
DM 79 24.5§ 11.2 25:54Control 84 27.7§ 10.5 14:70P signif. P< 0.05 P< 0.05
control group to the initial 210 days (approxi-mately 7 months) of treatment, i.e. a mean of208.3§ 7.9 days. An independent student t-testshowed no significant difference between thetwo groups (P = 0.36). An online questionnairewas then given only to the DMTM group to assessthe patients’ perspective on the ease of use andperceived benefit to treatment on a 5-point Lik-ert scale.15 They were also requested to list fivebenefits and five problems experienced whileusing DMTM. The questions were open ended toavoid the bias of preselected options. 70 patients(94.6%) responded to the questionnaire.
Independent t-tests were used to determineany inter-group differences in number ofappointments and age; a chi-square test was usedfor differences between genders. Significancewas set at P� 0.05.
Mean numbers of appointments were signifi-cantly lower by 1.68(P< 0.001) for DMTM
(3.07§ 1.8) compared to the control (4.75§ 1.6)over the evaluated treatment period. Age aver-aged 3.2 years younger for the DMTM group(24.5§ 11.8) than the control (27.7§ 10.5,P< 0.05). Moreover, gender distribution was sig-nificantly different (P< 0.05) with the DMTM
group comprising of 31.6% male and 68.4%female while the control group comprised of16.7% male and 83.3% female (Table 1).
Questionnaire results showed that 86%responded use of the DMTM app was “easy” or“very easy” to use, 7% regarded ease of DMTM
use as “moderate”, while 7% also regarded theDMTM app as “difficult” or “very difficult” to use.The mean Likert scale rating was 4.31 out of 5.0(Fig. 6); 84% indicated that DMTM was “benefi-cial” or “very beneficial” to their treatment expe-rience with a mean rating of 4.4, 10% indicatedDMTM was of moderate benefit to their treat-ment, while 6% indicated that it was not benefi-cial (Fig. 7). The most oft-mentioned benefitperceived by patients using DMTM was “better
l Monitoring (DM) and control groups of Invisalign�
number of appointments. P signif. represents probabil-ale-to-female ratio.
M:F) Treatment length No. of appointments
200.2§ 75.2 3.06§ 1.8208.3§ 7.9 4.75§ 1.6P> 0.05 P< 0.001

Figure 6. Questionnaire results of when asked to rate the ease of use of DM on a 5-point Likert scale. The meanrating was 4.31.
476 Hansa et al
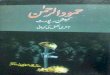
communication” (mentioned 47 times) followedby “increased convenience” (44 times), “reducednumber of appointments” (40 times) and “easeof use” (mentioned 38 times) (Fig. 8). The mostoft-mentioned problem identified by DMTM
patients was related to the “difficulty of takingscans” with 27 mentions; the others being “none”(16 times) and “reduced communication” (12times) (Fig. 9).
Figure 7. Questionnaire results of when asked to rate the bert scale. The mean rating was 4.4.
If were to critically analyze these responses,there was a reduction in mean number ofappointments (1.68) for the DMTM group com-pared to control after approximately 7 months oftreatment, a reduction of approximately 35%.Extrapolation of these findings to an overalltreatment time scale of 24 months would suggesta reduction of 5.8 appointments for DMTM
usage. Clearly, a study with completed patients in
enefit of DM on treatment experience on a 5-point Lik-

Figure 8. Questionnaire results of an open-ended question when asked to rank 5 benefits of using DM.
Remote monitoring and tele-orthodontics 477
both groups would be needed in order to verifythis projection. In addition, an assessment oftreatment outcomes would be needed in ordercompare the efficacy between the two therapies.
Figure 9. Questionnaire results of an open-ended qu
In this study, patients were given the choice touse DMTM at no additional cost, reducing con-founding factors. There was a significant differ-ence in the ages of the DMTM (24.5§ 11.8) and
estion when asked to rank 5 problems using DM.

478 Hansa et al
control (27.7§ 10.5, P< 0.05) groups. While theDMTM group was younger than the control by3.2 years, this difference was likely not clinicallyimportant but nevertheless hints at the trend foryounger patients being more inclined towardusing DMTM and being more comfortable withnew technology. The gender distribution wasalso significantly different (P< 0.05) with theDMTM group comprising of 31.6% male and68.4% female, and the control group comprisingof only 16.7% male and 83.3% female. Thisresult was interesting and suggested that maleswere more likely to use DMTM than females.Perhaps males were more enthusiastic aboutreducing the number of in-office visits andpreferred the greater convenience that DMTM
offered in contrast with direct communicationwith the orthodontist. However, these resultsshould be interpreted with caution as thepatients were from a single practice and maynot represent the demographics in other areasaround the world.
The questionnaire results suggest patientsadapt well to DMTM usage; 86% of DMTM usersresponded that the app was “easy” or “very easy”to use with a mean rating of 4.31. While DMTM
app was easy to use for a majority of patients inthe present study, this finding is not consistentwith 3.0 and 3.3-star app ratings on the AppleApp Store (5 reviews) and Google Play Store(48 reviews), respectively. The majority of DMTM
users (84%) responded that DMTM was “benefi-cial or “very beneficial” to their treatment expe-rience with a mean rating of 4.4. Theimplication being that DMTM met their expecta-tions of reducing in-office visits and increasingconvenience. Again, this finding is not consis-tent with 3.0 and 3.3-star app ratings on theApp Store (5 reviews) and Play Store (48reviews), respectively.
The most frequently mentioned benefits per-ceived by patients using DMTM were “better com-munication” (mentioned 47 times), “increasedconvenience” (44 mentions) and “reduced num-ber of appointments” (40 mentions). Better com-munication via the app was achieved withprompt, same day responses from the DMTM
team or the orthodontist after scans were sent.Whilst “increased convenience” and “reducednumber of appointments” could have beengrouped together, most patients indicated thesebenefits separately and were hence grouped as
such. Increased convenience included responsessuch as: “can be performed at home”, “do notneed to take off from work” and “can be donewhile on holiday”. An unexpected benefit ofDMTM was the patient's ability to see their treat-ment progress (21 mentions). The app allowsthe patient to view their previous scans, encour-aging and motivating them by showing theirprogress since treatment began. The problemidentified by patients most frequently was “diffi-culty of taking scans” with 27 mentions; this find-ing is in agreement with reviews on the PlayStore. The most commonly reported problemson the Play Store were related to software prob-lems and problems and difficulties in takingscans. In the present study, 12 mentions weremade of “reduced communication”, which wassurprising as “better communication” was men-tioned 47 times as a benefit of DMTM. This con-tradiction could be due to software problemsand/or their expectation of what communica-tion entails and how much the patient expectsfrom DMTM and the orthodontist. Surprisingly,one patient mentioned he preferred to see theorthodontist rather than use the app. This lownumber may be because all patients were giventhe option of using DMTM prior to treatment andthose who preferred in-office visits, likely decidedto not use DMTM.
Under the conditions of the present prelimi-nary study, the null hypotheses were rejectedand the conclusions reached were as follows:
� The DMTM group had reduced number ofappointments (3.07) compared with the con-trol group (4.75), with a difference of 1.68appointments after 7 months of evaluation.
� Extrapolation of this finding over the courseof an average 24-month treatment periodwould result in 5.8 fewer appointments for aDMTM sample- however this should be inter-preted with caution.
� The DMTM group was significantly youngerthan the control group, with ages of 24.5 and27.7 years, respectively.
� The DMTM group had almost double the per-centage of males (31.6%) than the controlgroup (16.7%).
� DMTM users indicated the app was easy to usewith 86% of the sample indicating it was“easy” or “very easy” with a mean rating of4.31 out of 5.0.

Remote monitoring and tele-orthodontics 479
� DMTM was perceived as beneficial to the treat-ment experience of the patients with 84% indi-cating that DMTM was “beneficial” or “verybeneficial” with a mean rating of 4.4 out of 5.0.
� The most frequently mentioned benefitsperceived by patients using DMTM were“better communication” (mentioned 47times), “increased convenience” (44 men-tions) and “reduced number of appoint-ments” (40 mentions).
� The most common problem perceived bypatients using DMTM was related to the “diffi-culty of taking scans” with 27 mentions.
While the preliminary results suggest thatnumber of appointments may be reduced withDental MonitoringTM, further studies should beperformed to evaluate overall active treatmenttime, treatment outcomes and refinement differ-ences in order to judge efficacy of DMTM usage.
Future implications
With the exponential incorporation of technol-ogy, the practice of orthodontics has consider-ably changed. The goal of tele-orthodontics is toreduce patient’s office visits while maintainingregular monitoring, without compromisingresults. Moreover, tele-orthodontics may be use-ful for remote consultations, which could be per-formed across the world without the patientpotentially stepping into the office. Comprehen-sive patient records would still require in-officevisits; however, it does open new channels fororthodontic consultations and second opinions.
Technological advances come with a dark sideas well.16 Reducing the number of face-to-faceappointments diminishes the rapport betweendoctor and patient. This traditional relationshipmay be reduced or lost, and with that, possiblytrust as well. The doctor �patient relationshiphas traditionally been much more than transac-tional.17 Dunbar12 reported in a pilot study that70% of subjects felt that the face-to-face aspect ofthe consultation was extremely important andthe majority preferred this over the exclusive useof tele-orthodontic technology. New legal issueswill also play a role with patient confidentialitypotentially being at risk due to records beingcommunicated over the internet.18 Patient com-plaints of malpractice may also increase if
patients do not receive an acceptable level ofcare or if practitioners do not maintain the levelof healthcare expected.
Tele-orthodontics has already gained somenotoriety in the USA by converting “patients” into“consumers” due to the “direct-to-consumer”approach from several companies; a trend thatmay, regrettably, be expected to continue in thefuture. These companies offer clear aligner treat-ment at a much cheaper rate than orthodontistsand market directly to the “consumer”. Kel-leher,19 a prosthodontist, has aptly described thisphenomenon as the “Uberization of orthodon-tics”. This new trend has come as a result of pro-spective patients looking for cheaper andaesthetic alternatives to traditional orthodontics,and service providers reducing care to a “com-modity”.20 A qualified dentist or orthodontist han-dles each case remotely, however no recordsother than casts/intra oral scans are made. Theextent of communication between the “con-sumer” and the “treating” doctor is also in ques-tion, which is especially problematic if treatmentgoes awry or outcomes are deemed unacceptable.
The opinion piece of Ackerman and Burris21
has been sufficiently rebutted numerous timesafter it was published,22�25 and although it wasnot the intention of this article to respond, it mustbe expanded upon as the current state of affairsof tele-orthodontics. According to Ackerman andBurris,21 the future of orthodontics is going theway of the airline industry, i.e. patients simplywish to go “from point A to B” and will skimp onthe “experience”, basing the decision to obtainorthodontic treatment primarily on cost and con-venience. Although this opinion piece continuesthe disturbing trend of renaming patients as con-sumers, they make a point that the new genera-tion of patients may indeed have differentpriorities and expectations. However, the airlineindustry example cannot simply be extrapolatedto the healthcare sector. The end result of ortho-dontics is not so definite as the destination of anairplane, and the orthodontist is not a travelagent.24 Furthermore, the potential for causingharm becomes a serious sequalae if the patient isnot diagnosed or treated appropriately. Access tocare cannot be held up as a slogan, whilst at thesame time placing patients at risk of harm. Unfor-tunately, companies whose primary aim is profit,do not hold themselves to the ethical principle of

480 Hansa et al
non-maleficence, embodied by the phrase “pri-mum non nocere” (first, do no harm).26 It ismind-boggling that over 30 years after an ortho-dontist was found guilty for causing a temporo-mandibular joint disorder (TMD), the same legalsystem is allowing poorly supervised orthodontictreatment. Wertheimer27 suggests that orthodont-ists themselves are somewhat to blame for this situ-ation, citing lack of the pursuit for excellentleading to subpar treatment which becomesundifferentiable to non-specialist orthodontics.He comments on the commoditization of ortho-dontics, suggesting that marketing, profits, prac-tice efficiency and increasing patient numbers,while being worthy goals by themselves, havebeen prioritized at the expense of evidence-based,patient-centric treatment. In order to combat this“direct to consumer” trend, orthodontists may beinclined to treat patients in a limited manner at areduced fee that meets the patient’s expectationsand demands; however, this would continue themarch to mediocrity and sub-par treatment.
The orthodontic community at this point hasan inherent distrust in tele-orthodontics and itspotential to not only reduce their patient base,but also cause harm to patients. However, out-side the USA where regulations of healthcareservices have different protocols, orthodontistsmay be more enthusiastic about the potential oftele-orthodontics. The key to the future of tele-orthodontics would be in balancing the benefitsof in-office visits and direct patient-doctor rela-tionships with the convenience and reducedcosts of remote monitoring, on an individualpatient-to-patient basis, while maintaining anexcellent standard of care.
References1. Berndt J, Leone P, King G. Using teledentistry to provide
interceptive orthodontic services to disadvantaged chil-dren. Am J Orthod Dentofac Orthop. 2008;134(5):700–706.http://dx.doi.org/10.1016/j.ajodo.2007.12.023.
2. Mandall NA, O’Brien KD, Brady J, Worthington HV, HarveyL. Teledentistry for screening new patient orthodontic refer-rals. Part 1: a randomised controlled trial. Br Dent J. 2005;199(10):659–662. http://dx.doi.org/10.1038/sj.bdj.4812930.
3. Stephens C, Cook J, Mullings C. Orthodontic referrals viaTeleDent Southwest. Dent Clin North Am. 2002;46(3):507–520. http://dx.doi.org/10.1016/S0011-8532(02)00010-1.
4. Vaid N. Up in the air: orthodontic technology unplugged!.APOS Trends Orthod. 2017;7(1):1–5. http://dx.doi.org/10.4103/2321-1407.199178.
5. Weber D, Koroluk L, Phillips C, Nguyen T, Proffit W.Clinical effectiveness and efficiency of customized vs. con-ventional preadjusted bracket systems. Jco. 2013;XLVII(4):261–266.
6. Rossini G, Parrini S, Castroflorio T, Deregibus A, DebernardiCL. Efficacy of clear aligners in controlling orthodontic toothmovement: a systematic review. Angle Orthod. 2015;85(5):881–889. http://dx.doi.org/10.2319/061614-436.1.
7. Brown MW, Koroluk L, Ko C-C, Zhang K, Chen M,Nguyen T. Effectiveness and efficiency of a CAD/CAMorthodontic bracket system. Am J Orthod DentofacOrthop. 2015;148(6):1067–1074. http://dx.doi.org/10.1016/J.AJODO.2015.07.029.
8. Vaid NR. Mind your business!: global orthodontic practicepatterns and management protocols: lessons, strategies,and some crystal gazing!. Semin Orthod. 2016;22(4):239–243. http://dx.doi.org/10.1053/J.SODO.2016.08.001.
9. Meghna V, Nikhilesh V, Dhaval F, Meetali S. Integrating“experience economy” into orthodontic practice manage-ment: a current perspective on internal marketing. SeminOrthod. 2016;22(4):301–309. http://dx.doi.org/10.1053/J.SODO.2016.08.011.
1.0. Sondhi A. A management manifesto: Standard Operat-ing Protocols and the application of checklists for ortho-dontic practices. Semin Orthod. 2016;22(4):262–269.http://dx.doi.org/10.1053/J.SODO.2016.08.005.
11. Gupta G, Vaid N. The world of orthodontic apps. APOSTrends Orthod. 2017;7(2):73–79. http://dx.doi.org/10.4103/2321-1407.202608.
12. Dunbar AC, Bearn D, McIntyre G. The influence of usingdigital diagnostic information on orthodontic treatmentplanning - a pilot study. J Healthc Eng. 2014;5(4):411–427.http://dx.doi.org/10.1260/2040-2295.5.4.411.
13. How dental monitoring works - dental monitoring;Accessed 18 June 2018. https://dental-monitoring.com/how-dental-monitoring-works/.
14. DM GoLive - the world’s first dynamic aligner tracking sys-tem - dental monitoring; Accessed 17 June 2018. https://dental-monitoring.com/dm-golive-worlds-first-dynamic-aligner-tracking-system/.
15. Likert R. A technique for the measurement of attitudes. 1932.16. Vaid NA. “Place for everything,” and “everything in its place ee.
APOS Trends Orthod. 2017;7(2):61. http://dx.doi.org/10.4103/2321-1407.202607.
17. Lipp MJ, Riolo C, Riolo M, Farkas J, Liu T, Cisneros GJ.Showing you care: an empathetic approach todoctor�patient communication. Semin Orthod. 2016;22(2):88–94. http://dx.doi.org/10.1053/J.SODO.2016.04.002.
18. Kotantoula G, Haisraeli-Shalish M, Jerrold L. Teleortho-dontics. Am J Orthod Dentofac Orthop. 2017;151(1):219–221. http://dx.doi.org/10.1016/j.ajodo.2016.10.012.
19. Kelleher M. The ‘Uberization of orthodontics’¡ or how lowcan you go? 2016;(September):606�607. doi:10.12968/denu.2016.43.7.606.
20. Vaid N. Commoditizing orthodontics: being as good as yourdumbest competitor? APOS Trends Orthod. 2016;6(3):121–122. http://dx.doi.org/10.4103/2321-1407.183154.
21. Ackerman M, Burris B. The way it was, the way it ought tobe, the way it is, and the way it will be. Am J Orthod DentofacOrthop. 2018;153(2):165–166. http://dx.doi.org/10.1016/j.ajodo.2017.09.010.

Remote monitoring and tele-orthodontics 481
22. Spencer GW. What we have to offer. Am J Orthod Dento-fac Orthop. 2018;154(1):8–9. http://dx.doi.org/10.1016/j.ajodo.2018.05.005.
23. Hughes J. The way it really is. Am J Orthod DentofacOrthop. 2018;154(1):5–6. http://dx.doi.org/10.1016/j.ajodo.2018.04.002.
24. Rigsby O. Thoghts. About “the way it was...”. Am J OrthodDentofac Orthop. 2018;154(1):4–5. http://dx.doi.org/10.1016/j.ajodo.2018.04.001.
25. Frazier MC. The sky is not the limit!. Am J Orthod DentofacOrthop. 2018;154(1):6–8. http://dx.doi.org/10.1016/j.ajodo.2018.04.016.
26. Gillon R. Medical ethics: four principles plus attention toscope; BMJ. 1994;309(6948):184. http://www.bmj.com/content/309/6948/184.abstract.
27. Wertheimer M. Pursuit of excellence: a forgotten quest?APOS Trends Orthod. 2018;8(1):10. http://dx.doi.org/10.4103/apos.apos_3_18.