Embed Size (px)
Citation preview

American Journal of Transplantation 2006; 6: 967–975Blackwell Munksgaard
C© 2006 The AuthorsJournal compilation C© 2006 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2006.01299.x
Islets Transplanted Intraportally into the Liverare Stimulated to Insulin and Glucagon ReleaseExclusively through the Hepatic Artery
J. Laua,∗, L. Janssona and P.-O. Carlssona,b
Departments of aMedical Cell Biology and bMedicalSciences, Uppsala University, SE-751 23,Uppsala, Sweden∗Corresponding author: Joey Lau,[email protected]
Not much is known about the physiology of intrapor-tally transplanted islets. One reason for this is thatit is difficult to study such islets, since they are scat-tered throughout the liver. We employed a perfusiontechnique to characterize the functional properties ofsyngeneic intrahepatic 1-month-old islet grafts, andcompared them to islets transplanted beneath the kid-ney capsule, as well as native islets. The cellular com-position of the islet grafts was also examined. Glu-cose and arginine administered through the hepaticartery, but not through the portal vein, induced in-sulin release from the intraportally implanted islets.Moreover, arginine, only when administered throughthe hepatic artery, induced glucagon release from thesame islets. The first phase of glucose-stimulated in-sulin release from both islets transplanted to the liverand kidney was delayed, and less prominent whencompared to the pancreas. Intraportally transplantedislets contained fewer glucagon-positive cells thanislets transplanted to the kidney and native islets. Ourfindings demonstrate that intraportally transplantedislets respond with insulin and glucagon to secreta-gogues, but only when stimulated through the hepaticartery. Whether intrahepatic islets may sense othersubstances than glucose or arginine occurring in highconcentrations in the portal vein following intestinaluptake remains to be studied.
Key words: Engraftment, graft function, hepaticartery, islets, liver perfusion
Received 11 October 2005, revised and accepted forpublication 25 January 2006
Introduction
Pancreatic islet transplantation is a tempting strategy to
treat patients with type 1 diabetes, since if successful it
could provide a cure for the disease. The “Edmonton pro-
tocol” for islet transplantation changed the immunosup-
pressive protocol toward less b-cytotoxic agents in combi-
nation with the use of freshly isolated islets for transplan-
tation and infusion of islets from 2 to 4 donors. By these
means a 1-year insulin independence rate of 80% was ob-
tained (1, 2). However, recent long-term observations show
that also when applying this protocol there is a continuous
decline in function of islet transplants. Very few patients re-
main insulin-independent beyond 4 years after transplanta-
tion (3), which contrasts to the results for whole pancreas
transplants (4, 5). Since the histocompatibility barrier, the
underlying autoimmune disease, and the immunosuppres-
sive agents used are the same for both procedures, this
puts focus on issues that are related to the adaptation of
the implanted islets in their new microenvironment, the
liver.
The liver provides several site-specific challenges for long-
term engraftment of transplanted islets, for instance be-
cause of its inherently low oxygenation (6, 7) and its func-
tion as the major detoxification site for substances occur-
ring in the portal vein following intestinal uptake. There
are also reports on alterations in islet function after intra-
portal islet transplantation, such as a defective glucagon
response to hypoglycemia (8, 9) and a defective glucose-
stimulated insulin release in murine islets retrieved from
the liver (10). Moreover, one experimental study in rat
has indicated an impaired long-term function of intrapor-
tally transplanted islets when compared to islets implanted
to the kidney (11). In view of these combined observa-
tions, we decided to study in more detail the insulin and
glucagon release from intraportally transplanted islets in
response to different stimuli by applying a technique with
liver perfusion ex vivo in the rat. We also aimed to inves-
tigate the changes in cellular composition of intraportally
transplanted islets, and whether hormone release from in-
traportally transplanted islets is affected by the stimuli ad-
ministered through either the portal vein or hepatic artery.
Materials and Methods
AnimalsInbred male Wistar-Furth rats weighing approximately 300 g were pur-
chased from Scanbur (Sollentuna, Sweden). The animals had free access
to pelleted food and water. All experiments were approved by the animal
ethics committee for Uppsala University.
967
Lau et al.
Islet isolation, culture and transplantationPancreatic islets were isolated from Wistar-Furth rats by collagenase diges-
tion (12), and cultured in groups of 150 islets for 3–4 days in 5 mL of culture
medium consisting of RPMI 1640 (Sigma-Aldrich, St. Louis, MO) supple-
mented with L-glutamine (Sigma-Aldrich) and 10% (vol/vol) fetal calf serum
(Sigma-Aldrich). Culture medium was changed every second day.
At transplantation, groups of 200 islets were packed in a butterfly needle
(25G) and infused via the portal vein into the liver, or packed in a brak-
ing pipette and implanted beneath the left renal capsule, of syngeneic
pentobarbital-anesthetized (60 mg/kg i.p.; Apoteket, Goteborg, Sweden)
Wistar-Furth rats. The transplanted islet volume was estimated to as a mean
2.53 lL by measurements of islet volume packed in the braking pipette be-
fore transplantation.
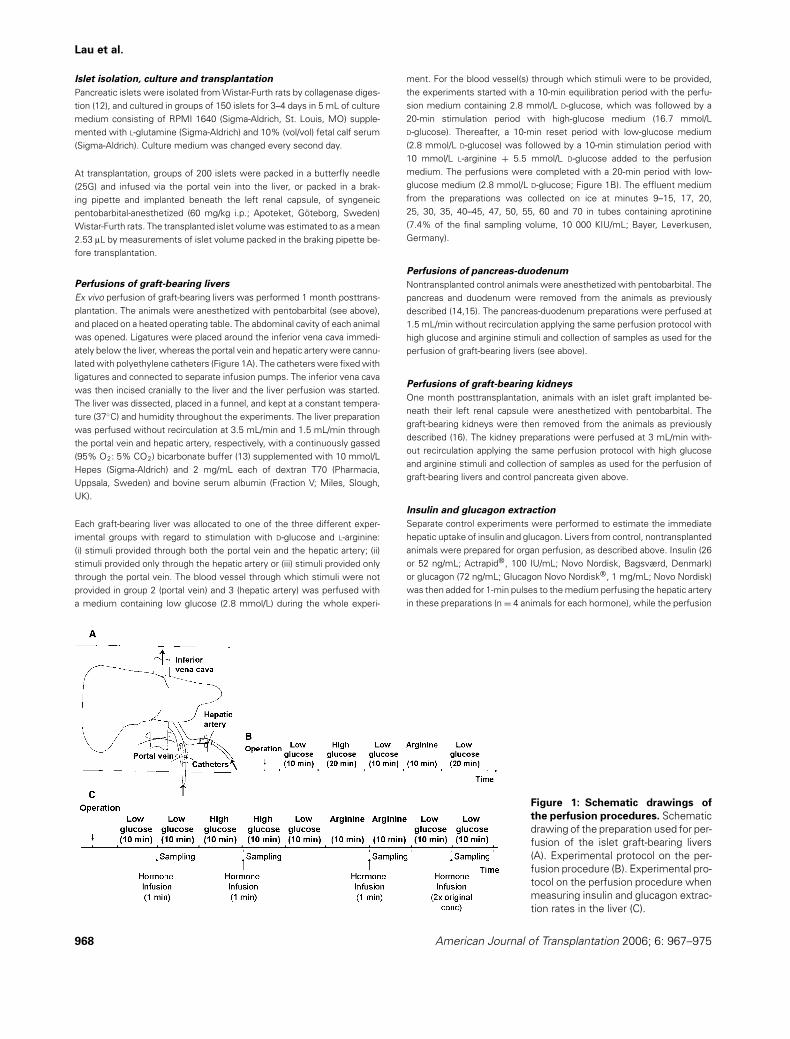
Perfusions of graft-bearing liversEx vivo perfusion of graft-bearing livers was performed 1 month posttrans-
plantation. The animals were anesthetized with pentobarbital (see above),
and placed on a heated operating table. The abdominal cavity of each animal
was opened. Ligatures were placed around the inferior vena cava immedi-
ately below the liver, whereas the portal vein and hepatic artery were cannu-
lated with polyethylene catheters (Figure 1A). The catheters were fixed with
ligatures and connected to separate infusion pumps. The inferior vena cava
was then incised cranially to the liver and the liver perfusion was started.
The liver was dissected, placed in a funnel, and kept at a constant tempera-
ture (37◦C) and humidity throughout the experiments. The liver preparation
was perfused without recirculation at 3.5 mL/min and 1.5 mL/min through
the portal vein and hepatic artery, respectively, with a continuously gassed
(95% O2: 5% CO2) bicarbonate buffer (13) supplemented with 10 mmol/L
Hepes (Sigma-Aldrich) and 2 mg/mL each of dextran T70 (Pharmacia,
Uppsala, Sweden) and bovine serum albumin (Fraction V; Miles, Slough,
UK).
Each graft-bearing liver was allocated to one of the three different exper-
imental groups with regard to stimulation with D-glucose and L-arginine:
(i) stimuli provided through both the portal vein and the hepatic artery; (ii)
stimuli provided only through the hepatic artery or (iii) stimuli provided only
through the portal vein. The blood vessel through which stimuli were not
provided in group 2 (portal vein) and 3 (hepatic artery) was perfused with
a medium containing low glucose (2.8 mmol/L) during the whole experi-
Figure 1: Schematic drawings ofthe perfusion procedures. Schematic
drawing of the preparation used for per-
fusion of the islet graft-bearing livers
(A). Experimental protocol on the per-
fusion procedure (B). Experimental pro-
tocol on the perfusion procedure when
measuring insulin and glucagon extrac-
tion rates in the liver (C).
ment. For the blood vessel(s) through which stimuli were to be provided,
the experiments started with a 10-min equilibration period with the perfu-
sion medium containing 2.8 mmol/L D-glucose, which was followed by a
20-min stimulation period with high-glucose medium (16.7 mmol/L
D-glucose). Thereafter, a 10-min reset period with low-glucose medium
(2.8 mmol/L D-glucose) was followed by a 10-min stimulation period with
10 mmol/L L-arginine + 5.5 mmol/L D-glucose added to the perfusion
medium. The perfusions were completed with a 20-min period with low-
glucose medium (2.8 mmol/L D-glucose; Figure 1B). The effluent medium
from the preparations was collected on ice at minutes 9–15, 17, 20,
25, 30, 35, 40–45, 47, 50, 55, 60 and 70 in tubes containing aprotinine
(7.4% of the final sampling volume, 10 000 KIU/mL; Bayer, Leverkusen,
Germany).
Perfusions of pancreas-duodenumNontransplanted control animals were anesthetized with pentobarbital. The
pancreas and duodenum were removed from the animals as previously
described (14,15). The pancreas-duodenum preparations were perfused at
1.5 mL/min without recirculation applying the same perfusion protocol with
high glucose and arginine stimuli and collection of samples as used for the
perfusion of graft-bearing livers (see above).
Perfusions of graft-bearing kidneysOne month posttransplantation, animals with an islet graft implanted be-
neath their left renal capsule were anesthetized with pentobarbital. The
graft-bearing kidneys were then removed from the animals as previously
described (16). The kidney preparations were perfused at 3 mL/min with-
out recirculation applying the same perfusion protocol with high glucose
and arginine stimuli and collection of samples as used for the perfusion of
graft-bearing livers and control pancreata given above.
Insulin and glucagon extractionSeparate control experiments were performed to estimate the immediate
hepatic uptake of insulin and glucagon. Livers from control, nontransplanted
animals were prepared for organ perfusion, as described above. Insulin (26
or 52 ng/mL; Actrapid®, 100 IU/mL; Novo Nordisk, Bagsværd, Denmark)
or glucagon (72 ng/mL; Glucagon Novo Nordisk®, 1 mg/mL; Novo Nordisk)
was then added for 1-min pulses to the medium perfusing the hepatic artery
in these preparations (n = 4 animals for each hormone), while the perfusion
968 American Journal of Transplantation 2006; 6: 967–975

Perfusion of Islet Graft-Bearing Livers
medium contained a low glucose (2.8 mmol/L), a high glucose concentration
(16.7 mmol/L) or arginine (Figure 1C). In each case, the perfusion medium
had been unchanged for 10 min prior to insulin or glucagon infusion. Follow-
ing each infusion, the contents of the perfusion medium were unchanged
for at least another 10 min, while the effluent from the incised caval vein
was collected on ice in tubes prefilled with aprotinin (7.4% of the final sam-
pling volume, 10 000 KIU/mL). Moreover, there was a 10-min wash-out
period between stimulation with high glucose and arginine. The insulin and
glucagon concentrations used for these control experiments were chosen
to mimic the physiological concentrations of insulin and glucagon in the
liver.
Hormone measurementsThe effluents from the different perfusions of pancreata or graft-bearing
organs were analyzed for insulin concentrations by a rat insulin ELISA
(Mercodia, Uppsala, Sweden). Glucagon measurements in the samples
were carried out using rat glucagon RIA kits (Linco Research, St. Louis,
MO). The mass insulin and glucagon responses to stimuli were calculated
by planimetry (17).
In order to detect glucagon concentrations in the effluents from the livers
containing an islet graft, the samples were concentrated with Centricon
YM-3 tubes (membrane cutoff 3 000 Da; Millipore, Billerica, MA) approxi-
mately 5–6 times. The exact magnitude of concentration was determined
for each sample by weighing it before and after centrifugation.
Insulin and glucagon concentrations in samples obtained from the con-
trol experiments where insulin and glucagon were infused into the hepatic
Figure 2: Insulin release in effluent medium collected from perfused native Wistar-Furth pancreas (A), islet graft-bearing kidneys(B) and islet graft-bearing livers of Wistar-Furth rats (C, D and E). Each graft-bearing liver was allocated to one of three different
experimental groups, where stimuli to insulin release were provided through both the portal vein and the hepatic artery (experimental
group 1; C) only through the hepatic artery; (experimental group 2; D), or only through the portal vein (experimental group 3; E). After
10 min equilibration period with a perfusion medium containing 2.8 mmol/L D-glucose, insulin secretion was stimulated by a 20-min period
with 16.7 mmol/L D-glucose followed by a 10 min reset period with 2.8 mmol/L D-glucose. Thereafter, insulin secretion was stimulated
with a perfusion medium containing 10 mmol/L L-arginine + 5.5 mmol/L D-glucose followed by 20 min with 2.8 mmol/L D-glucose. The
blood vessel through which stimuli were not provided in the perfusion of graft-bearing livers, i.e. portal vein in group 2 and hepatic artery
in group 3, was perfused with low-glucose medium (2.8 mmol/L D-glucose). All values are given as means ± SEM for 5–7 animals in each
group.
artery were analyzed by a human insulin ELISA (Mercodia) and a glucagon
RIA kit (Linco Research), respectively.
Morphological studiesSeparate graft-bearing kidneys/livers and control pancreata were removed,
fixed in 10% (vol/vol) formalin, embedded in paraffin and sectioned at 5 lm.
To determine the percentage of b-cells and a-cells in the different sam-
ples, sections of native or transplanted islets were stained with insulin
(ICN Biomedicals, Aurora, OH) and glucagon (Novo Nordisk). These sec-
tions were then examined using a point-counting method (18), where the
number of intersections overlapping insulin- and glucagon-positive cells, re-
spectively, was counted in a light microscope. A total of 121–726 points
were counted in each pancreas or islet graft. The volume of the islets in
the native pancreata was evaluated as previously described (19). Briefly,
each pancreata of 9 separate animals was weighed, cut into 45–48 pieces
and placed between object slides. Following visualization of the islets by a
freeze-thawing technique (20), the percentage of islet volume was deter-
mined by point-counting (18). A total of 5000–5700 points were counted in
each pancreas. The total islet volume in a Wistar-Furth pancreas could then
be estimated to 12.4 ± 0.6 lL.
Statistical analysisAll values are given as means ± SEM. Multiple comparisons for normally
distributed data were performed using ANOVA and the Bonferroni post-hoc
test, whereas nonparametric values were compared using nonparametric
ANOVA and Dunn’s test. For all comparisons, a p-value < 0.05 was consid-
ered to be statistically significant.
American Journal of Transplantation 2006; 6: 967–975 969

Lau et al.
Results
Insulin releaseA biphasic insulin response to high glucose (16.7 mmol/L;
Figure 2A) was consistently seen from perfused pancre-
ata. A rapid and prominent first peak was followed by a
sustained second phase of insulin release. The incremen-
tal value for the first phase was in average of 150% higher
than the mean plateau values during the second phase.
Similarly to the response to high glucose, two prominent
peaks of insulin release were discerned when arginine was
added to the perfusate. From perfused graft-bearing kid-
neys, there was a first and second phase of insulin release,
as from the control pancreata, in response to 16.7 mmol/L
D-glucose (Figure 2B). However, the first phase of insulin
release from these renal subcapsular grafts was delayed
when compared to the control pancreata with a mean incre-
mental value of 3 min instead of 1 min after introduction of
the high glucose in the perfusion medium (p < 0.05, non-
parametric ANOVA). Moreover, the incremental value for
the first phase of insulin release from these grafts was only
approximately 50% higher than the insulin release values
during the second phase, which is a weaker first-phase re-
sponse than that seen in the pancreata (p < 0.05, ANOVA).
The renal subcapsular grafts responded to arginine with a
prominent first peak followed by a smaller second peak of
insulin release.
In the first experimental group with perfusion of graft-
bearing livers, stimuli to insulin secretion were provided
simultaneously through both the hepatic artery and the
portal vein. Introduction of a high-glucose concentration
(16.7 mmol/L) in the perfusion medium elicited insulin re-
lease (Figure 2C), but as for the renal subcapsular grafts,
the response was delayed with an incremental value oc-
curring 2 min later when compared to control pancre-
ata (p < 0.05, nonparametric ANOVA). Moreover, the
first peak of insulin release from the graft-bearing livers
could barely be separated from the second phase of in-
sulin release, and constituted, as for the renal subcapsu-
lar grafts, a weaker first-phase response than that seen in
the pancreata (p < 0.05, ANOVA). However, a prominent
insulin release response from the intraportally implanted
islets was recorded when the islets were challenged with
arginine.
Also when stimuli to insulin release (high glucose or argi-
nine) were provided only through the hepatic artery into
graft-bearing livers (experimental group 2), there was a pro-
nounced insulin secretion (Figure 2D). The insulin release
in this setting was similar in magnitude to that seen when
stimuli to insulin release were provided through both the
hepatic artery and portal vein. The first phase of insulin
release in response to high glucose tended to be slightly
more prominent than when both blood vessels were per-
fused with high glucose stimuli, but only ∼20% higher than
the plateau values during the second phase.
Figure 3: Glucagon response (as area under curve, AUC) to10 mmol/L L-arginine + 5.5 mmol/L D-glucose from nativeislets, and 1-month-old renal subcapsular or intraportal isletgrafts consisting of 200 islets. All values are given as means
± SEM for 2–8 animals in each group. ∗Denotes p < 0.05 when
compared to native islets, and †p < 0.05 when compared to renal
subcapsular islet grafts. All comparisons were made using ANOVA
and Bonferroni’s post hoc test.
No insulin response at all could be detected when stimuli
to insulin release were administered only through the por-
tal vein (experimental group 3; Figure 2E). In this setting,
the insulin release remained at basal levels throughout the
whole perfusion.
Glucagon releaseWhen the control pancreata were perfused, there was a
rapid and transient peak of glucagon release (mean incre-
mental value 904 ± 403 pg/min) during the first 3 min
of perfusion with the high glucose (16.7 mmol/L) perfu-
sion medium. Moreover, when the perfusion medium con-
tained arginine, a distinct and sustained glucagon release
was elicited from the preparations (Figure 3). Glucagon
concentrations in the effluents during other parts of the
perfusion were below the detection level of the assay
(20 pg/mL).
Also from perfused graft-bearing kidneys, there was
a glucagon response during perfusion with arginine
(Figure 3). Glucagon concentrations in the effluents dur-
ing other parts of the perfusion were below the detection
level of the assay.
When graft-bearing livers were perfused, we could at first
not detect glucagon concentrations in the effluents, even
in response to arginine, in any of the three experimental
groups. However, following concentration of our samples
5–6 times, there was a rapid and transient peak of glucagon
release in response to a high (16.7 mmol/L) glucose con-
centration (mean incremental value 28.9 ± 2.5 and 35.3 ±8.3 pg/min for experimental groups 1 and 2, respectively)
970 American Journal of Transplantation 2006; 6: 967–975

Perfusion of Islet Graft-Bearing Livers
in the effluents of our liver preparations, as in the efflu-
ents from the control pancreata. Likewise, glucagon re-
lease was increased when the perfusion medium was sup-
plemented with arginine (Figure 3). Quite in contrast, there
was no glucagon release at all in response to these stim-
uli in experimental group 3, i.e. when high glucose and
arginine were supplemented to the medium perfusing the
portal vein.
Insulin and glucagon extraction rates in liverIrrespective of whether insulin was administered into
the hepatic artery during perfusion with low glucose
(2.8 mmol/L), high glucose (16.7 mmol/L) or arginine
supplemented medium, 43.6 ± 3.8% (n = 4 animals) of
infused insulin was extracted in the liver. In comparison,
the glucagon extraction rate in the liver was 67.5 ± 5.1%
(n = 4).
Cellular composition of transplanted isletsIn the pancreas of Wistar-Furth rats, 75–80% of all
islet cells were b-cells (Figure 4A,B) and ∼20% a-cells
(Figure 5A, B). Islets transplanted beneath the renal cap-
sule had a decreased fraction of b-cells compared to control
islets (Figure 4A, C), whereas for intraportally transplanted
islets there was only a tendency to a decrease in b-cell
number (Figure 4A, D). In contrast, the fraction of a-cells
was markedly decreased in the intraportally transplanted
islets (Figure 5A, D), but not in the islets grafted to the kid-
ney (Figure 5A, C). Moreover, when comparing the fraction
of a-cells at the different implantation sites, intraportally
transplanted islets had much less glucagon-positive cells
than islets transplanted beneath the renal capsule.
Figure 4: Comparisonbetween native andtransplanted islets. (A)
Percentage insulin-positive
cells in native Wistar-Furth
rat islets, and 1-month-old
syngeneic renal subcap-
sular or intraportal islet
grafts. All values are given
as means ± SEM for
4–5 experiments in each
group. ∗Denotes p < 0.05
when compared to native
pancreatic islets as eval-
uated by nonparametric
ANOVA and Dunn’s test.
(B–D) Micrographs of a
native rat islet (B), renal
subcapsular islet graft (C)
and intraportal islet graft
(D) stained for insulin.
Scale bar 10 lm in B and
D, and 20 lm in C.
Discussion
When pancreatic islets are implanted intraportally they dis-
perse throughout the liver and become lodged deep in dis-
tal tributaries of the portal vein. It has therefore been en-
visaged that islet endocrine cells are chronically exposed
to substances occurring in the portal vein. The present
study shows that only nutrients present in the hepatic
artery could elicit insulin and glucagon release from trans-
planted islets 1 month posttransplantation, whereas nutri-
ents administered through the portal vein had no effects on
islet hormonal release. The latter finding suggests that not
even the endocrine cells located in the islet periphery were
reached by stimuli in the portal vein. We did not investigate
to what extent other substances, e.g. immunosuppressive
drugs, occurring in high concentrations in the portal vein fol-
lowing intestinal uptake could affect islet cells through the
portal vein route. Since both glucose and arginine have a
very high capacity for diffusion in tissues, we think that our
findings are also applicable to other substances following
engraftment. It is possible that the high concentrations of
immunosuppressive drugs occurring in portal blood exert
detrimental effects on islets cells in the immediate post-
transplantation period (21, 22).
Since nutrients in the vicinity of the transplanted islets,
i.e. administered through the portal vein, did not affect
islet hormonal release, it is likely that nutrient sensing
of the islet a- and b-cells in the islet transplants occurs
only through the newly formed vascularity. There have
previously been contradictory reports whether intraportally
transplanted islets become revascularized by tributaries
American Journal of Transplantation 2006; 6: 967–975 971

Lau et al.
Figure 5: Comparisonbetween native andtransplanted islets. (A)
Percentage glucagon-
positive cells in native
Wistar-Furth rat islets, and
1-month-old syngeneic
renal subcapsular or intra-
portal islet grafts. All values
are given as means ± SEM
for 4–7 experiments in
each group. ∗Denotes p <
0.05 when compared to
native pancreatic islets,
and †p < 0.05 when com-
pared to renal subcapsular
islet grafts. All compar-
isons were evaluated by
nonparametric ANOVA and
Dunn’s test. (B–D) Micro-
graphs of a native rat islet
(B), renal subcapsular islet
graft (C) and intraportal
islet graft (D) stained for
glucagon. Scale bar 10 lm
in B, and 20 lm in C–D.
both from the portal vein and the hepatic artery (23), or
mainly by tributaries from the hepatic artery (24). Our data
are consistent with the latter report.
There are some previous studies concerning perfusion
of graft-bearing livers (25–27). Those only concluded that
a biphasic insulin release from intraportally transplanted
islets does occur in response to glucose, but did not com-
pare the response either to native islets or islets implanted
to other organs. In the present study, both islets implanted
to the kidney and intraportally into the liver had a delayed
and decreased first phase of insulin release in response to
glucose when compared to native islets. The decreased
first-phase response, compared to the native pancreas,
may be related to a lower islet mass transplanted and ul-
timately engrafted in the liver. Although we corrected the
first-phase response for the number of islets transplanted,
it is unknown how many islet survive in the ectopic environ-
ment, and the lower first-phase response may simply rep-
resent a lower functional islet mass. It may also reflect dis-
turbances in the secretory machinery of the transplanted
b-cells, as previously indicated in in vitro studies of islets re-
trieved from the renal subcapsular (28) and intraportal site
(10). Alternatively, it may reflect a vascular dysfunction of
the transplanted islets due to their lower vascular density
(29, 30) and blood perfusion (6). In line with this, we have
recently observed that improvements in the blood perfu-
sion of islet renal subcapsular grafts are associated with an
enhanced first phase of glucose-stimulated insulin release
(31).
Since the liver is a major target organ for insulin, some of
the insulin secreted by intraportally transplanted islets is
metabolized within the organ before entering the systemic
circulation. This makes the comparison of the response of
insulin from intraportally transplanted islets to that of islets
implanted at other implantation sites difficult. In order to
estimate the fraction of insulin metabolized in the liver al-
ready during the first passage, we injected insulin into the
hepatic artery of control liver preparations during perfusion.
We found that approximately 55% of injected insulin could
be retrieved in the effluents from the caval vein, irrespec-
tive of whether insulin was injected during perfusion with
buffer containing the low or high glucose concentration or
arginine. These estimations are also consistent with previ-
ous observations on the insulin extraction rate in liver (32–
34). If compensating for the immediate hepatic uptake of
some of the secreted insulin from intraportally transplanted
islets with this factor when performing the comparison to
insulin release from islets in the renal subcapsular site,
these two implantation sites seemed to have a similar in-
sulin response (cf. Figure 6A, B). Following measurements
of islet mass in a Wistar-Furth pancreas, as well as of the
transplanted islet mass, it could also be estimated that the
insulin response from the islet transplants was 26–47% of
the expected for an optimal graft with this number of islets.
However, the insulin response from the transplanted islets
in our perfusion experiments seemed still quite prominent,
which contrasts to previous findings on retrieved intrapor-
tally transplanted islets investigated in vitro. Such islets
showed a much lower insulin content and insulin release
972 American Journal of Transplantation 2006; 6: 967–975

Perfusion of Islet Graft-Bearing Livers
Figure 6: Insulin mass response (as area under curve, AUC) to 16.7 mmol/L D-glucose (A) and 10 mmol/L L-arginine + 5.5 mmol/LD-glucose (B), and glucagon mass response to 10 mmol/L L-arginine + 5.5 mmol/L D-glucose (C), for native Wistar-Furth ratislets and 1-month-old syngeneic renal subcapsular or intraportal islet grafts. For intraportal islet grafts, nutrient stimuli were
infused through both hepatic artery and portal vein. Measured values in the effluents are shown in solid bars. Hatched bars for the islet
transplants denote recalculated values from those shown in solid bars when correcting for differences in islet mass to the pancreas and
also for the immediate hormone uptake by the liver parenchyma in the graft-bearing liver perfusions. The calculations were based on the
assumption of an islet mass of 12.4 lL in the pancreas of Wistar-Furth rats, a transplanted islet mass of 2.53 lL and immediate extraction
rates of 43.6% and 67.5% for insulin and glucagon secreted from the intraportal islet grafts, respectively. All values are given as means ±SEM.
than islets isolated from the pancreas, and also had a dis-
turbed glucose oxidation rate (10). It is possible that this
discrepancy may be explained by that the employed perfu-
sion technique enabled us to study the insulin release from
all transplanted b-cells in the liver, and that it is rather small
or fragmented islets that remain functional after transplan-
tation instead of larger, easily retrievable islets.
The reason for the decreased b-cell fraction in the renal
subcapsular islet grafts is unknown (35). It may, however,
be envisaged that the preferential location of rodent b-cells
to the islet core may predispose them more than other islet
cells to hypoxic injury in the immediate posttransplantation
period (35,36).
As also previously described (8, 9, 37), both renal subcap-
sular islet transplants and intraportal islet grafts responded
similarly to native islets with glucagon release in response
to arginine stimulation. Consistent with previous studies
(38, 39), we observed a high clearance of glucagon by
the liver (65–70%), which underlines the importance of
the liver as a major target organ for glucagon. The lower
size of the glucagon response from the intraportally trans-
planted islets compared to the renal subcapsular grafts
seemed mainly to be explained by this high-clearance rate
(Figure 6C). However, the intraportal islet grafts also con-
tained a decreased fraction of a-cells, both when compared
to native islets and islets implanted to the renal subcapsu-
lar site. Since intraportally transplanted islets do not seem
to sense nutrient stimuli in portal blood, but only those oc-
curring in the hepatic artery, downregulation of glucagon
production induced by higher concentrations of islet hor-
mones such as glucagon in portal than in systemic blood is
unlikely to provide an explanation. Instead, the decrease in
a-cells may be due to the factors associated with the hep-
atic environment per se, or be a result of the intraportal
transplantation procedure.
We consistently recorded a transient peak of glucagon re-
lease in both the effluents of graft-bearing livers and con-
trol pancreata in response to high glucose in the perfusate.
The reason for this seemingly paradoxal glucagon release is
obscure, but a previous study has suggested that a pulse
of glucagon secretion from a-cells may occur after high-
glucose stimulation (40). We could not detect a similar re-
sponse from the renal subcapsular grafts, which may be
explained by the detection limit of the assay (20 pg/mL),
since these samples were not concentrated.
We did not record an increased glucagon release from
either native islets in the control pancreata or the trans-
planted islets during organ perfusion with buffer containing
a low-glucose concentration (2.8 mmol/L). These results
are consistent with previous data on perfused rat pancre-
ata (41, 42) and renal subcapsular grafts (37), and may be
explained by that glucagon release following switching to
low glucose is delayed for at least 10 min in several set-
tings, including pancreas perfusions in rat (9, 43, 44).
The present findings that intraportally transplanted islets
respond with insulin and glucagon release to secreta-
gogues only when stimulated through the hepatic artery
mean that the high concentrations of nutrients in the por-
tal vein following intestinal uptake do not reach such islets.
Further studies on changes in islet physiology following in-
traportal islet transplantation may provide us with impor-
tant clues to the site-specific challenges faced by these
islets, and ultimately strategies on how to counter-act
these to improve islet graft function.
Acknowledgments
The technical assistance of Birgitta Bodin, Astrid Nordin and Eva Tornelius
is gratefully acknowledged.
American Journal of Transplantation 2006; 6: 967–975 973

Lau et al.
This study was supported by grants from the Juvenile Diabetes Re-
search Foundation, the Swedish Research Council (72XD-15043, 72X-109),
EFSD/Novo Nordisk Research Program, the Swedish Diabetes Foundation,
the Swedish Juvenile Diabetes Fund, the Ake Wiberg Foundation, the Aner
Foundation and the Family Ernfors Fund.
References
1. Shapiro AM, Lakey JR, Ryan EA et al. Islet transplantation in seven
patients with type 1 diabetes mellitus using a glucocorticoid-free
immunosuppressive regimen. N Engl J Med 2000; 343: 230–238.
2. Ryan EA, Lakey JR, Paty BW et al. Successful islet transplantation:
Continued insulin reserve provides long-term glycemic control.
Diabetes 2002; 51: 2148–2157.
3. Ryan EA, Paty BW, Senior PA et al. Five-year follow-up after clinical
islet transplantation. Diabetes 2005; 54: 2060–2069.
4. Gruessner AC, Sutherland DE. Pancreas transplant outcomes for
United States (US) and non-US cases as reported to the United
Network for Organ Sharing (UNOS) and the International Pancreas
Transplant Registry (IPTR) as of May 2003. Clin Transplant 2003:
21–51.
5. Humar A, Kandaswamy R, Granger D, Gruessner RW, Gruessner
AC, Sutherland DE. Decreased surgical risks of pancreas trans-
plantation in the modern era. Ann Surg 2000; 231: 269–275.
6. Carlsson PO, Palm F, Andersson A, Liss P. Markedly decreased
oxygen tension in transplanted rat pancreatic islets irrespective of
the implantation site. Diabetes 2001; 50: 489–495.
7. Arteel GE, Thurman RG, Yates JM, Raleigh JA. Evidence that hy-
poxia markers detect oxygen gradients in liver: Pimonidazole and
retrograde perfusion of rat liver. Br J Cancer 1995; 72: 889–895.
8. Gupta V, Wahoff DC, Rooney DP et al. The defective glucagon
response from transplanted intrahepatic pancreatic islets during
hypoglycemia is transplantation site-determined. Diabetes 1997;
46: 28–33.
9. Paty BW, Ryan EA, Shapiro AM, Lakey JR, Robertson RP. In-
trahepatic islet transplantation in type 1 diabetic patients does
not restore hypoglycemic hormonal counterregulation or symp-
tom recognition after insulin independence. Diabetes 2002; 51:
3428–3434.
10. Mattsson G, Jansson L, Nordin A, Andersson A, Carlsson PO.
Evidence of functional impairment of syngeneically transplanted
mouse pancreatic islets retrieved from the liver. Diabetes 2004;
53: 948–954.
11. Hiller WF, Klempnauer J, Luck R, Steiniger B. Progressive de-
terioration of endocrine function after intraportal but not kidney
subcapsular rat islet transplantation. Diabetes 1991; 40: 134–140.
12. Andersson A. Isolated mouse pancreatic islets in culture: Effects
of serum and different culture media on the insulin production of
the islets. Diabetologia 1978; 14: 397–404.
13. Krebs HA, Henseleit. K. Untersuchungen uber die Harnstoffbil-
dung im Tierkorper. Hoppe-Seyler’s Z Physiol Chem 1932; 210:
33–66.
14. Loubatieres A, Mariani MM, Ribes G, de Malbosc H, Chapal J.
Experimental study of a new especially active hypoglycemic sul-
fonamide, HB-419 or Glibenclamide. Diabetologia 1969; 5: 1–10.
15. Jansson L. Flow distribution between the endocrine and exocrine
parts of the isolated rat pancreas during perfusion in vitro with
different glucose concentrations. Acta Physiol Scand 1986; 126:
533–538.
16. Korsgren O, Jansson L, Andersson A. Effects of hyperglycemia
on function of isolated mouse pancreatic islets transplanted under
kidney capsule. Diabetes 1989; 38: 510–515.
17. Korsgren O, Jansson L, Sandler S, Andersson A. Hyperglycemia-
induced B cell toxicity. The fate of pancreatic islets transplanted
into diabetic mice is dependent on their genetic background. J
Clin Invest 1990; 86: 2161–2168.
18. Weibel ER. Stereological methods. Practical Methods for Biologi-
cal Morphometry, Vol.1. San Francisco: Academic Press; 1979.
19. Carlsson PO, Andersson A, Jansson L. Pancreatic islet blood flow
in normal and obese-hyperglycemic (ob/ob) mice. Am J Physiol
1996; 271 (6 Pt 1): E990–E995.
20. Jansson L, Hellerstrom C. A rapid method of visualizing the pan-
creatic islets for studies of islet capillary blood flow using non-
radioactive microspheres. Acta Physiol Scand 1981; 113: 371–
374.
21. Desai NM, Goss JA, Deng S et al. Elevated portal vein drug lev-
els of sirolimus and tacrolimus in islet transplant recipients: Local
immunosuppression or islet toxicity? Transplantation 2003; 76:
1623–1625.
22. Shapiro AM, Gallant HL, Hao EG et al. The portal immunosuppres-
sive storm: Relevance to islet transplantation? Ther Drug Monit
2005; 27: 35–37.
23. Griffith RC, Scharp DW, Hartman BK, Ballinger WF, Lacy PE. A
morphologic study of intrahepatic portal-vein islet isografts. Dia-
betes 1977; 26: 201–214.
24. Andersson A, Korsgren O, Jansson L. Intraportally transplanted
pancreatic islets revascularized from hepatic arterial system. Dia-
betes 1989; 38 (Suppl 1): 192–195.
25. Bromme HJ, Hahn HJ, Blech W. Biphasic release of insulin from
islets of Langerhans after their transplantation into the liver of rats.
Horm Metab Res 1988; 20: 138–140.
26. Porksen N, Munn S, Ferguson D, O’Brien T, Veldhuis J, Butler
P. Coordinate pulsatile insulin secretion by chronic intraportally
transplanted islets in the isolated perfused rat liver. J Clin Invest
1994; 94: 219–227.
27. Gardemann A, Strulik H, Jungermann K. A portal-arterial glucose
concentration gradient as a signal for an insulin-dependent net
glucose uptake in perfused rat liver. FEBS Lett 1986; 202: 255–
259.
28. Shi CL, Taljedal IB. Dynamics of glucose-induced insulin release
from mouse islets transplanted under the kidney capsule. Trans-
plantation 1996; 62: 1312–1318.
29. Mattsson G, Jansson L, Carlsson PO. Decreased vascular density
in mouse pancreatic islets after transplantation. Diabetes 2002;
51: 1362–1366.
30. Carlsson PO, Palm F, Mattsson G. Low revascularization of exper-
imentally transplanted human pancreatic islets. J Clin Endocrinol
Metab 2002; 87: 5418–5423.
31. Kampf C, Lau T, Olsson R, Leung PS, Carlsson PO. Angiotensin II
type 1 receptor inhibition markedly improves the blood perfusion,
oxygen tension and first phase of glucose-stimulated insulin se-
cretion in revascularised syngeneic mouse islet grafts. Diabetolo-
gia 2005; 48: 1159–1167.
32. Ferrannini E, Wahren J, Faber OK, Felig P, Binder C, DeFronzo RA.
Splanchnic and renal metabolism of insulin in human subjects: A
dose-response study. Am J Physiol 1983; 244: E517–E527.
33. Ciampelli M, Fulghesu AM, Cucinelli F et al. Heterogeneity in beta
cell activity, hepatic insulin clearance and peripheral insulin sen-
sitivity in women with polycystic ovary syndrome. Hum Reprod
1997; 12: 1897–1901.
34. Svedberg J, Stromblad G, Wirth A, Smith U, Bjorntorp P. Fatty
acids in the portal vein of the rat regulate hepatic insulin clearance.
J Clin Invest 1991; 88: 2054–2058.
35. Davalli AM, Scaglia L, Zangen DH, Hollister J, Bonner-Weir S, Weir
GC. Vulnerability of islets in the immediate posttransplantation pe-
riod. Dynamic changes in structure and function. Diabetes 1996;
45: 1161–1167.
974 American Journal of Transplantation 2006; 6: 967–975

Perfusion of Islet Graft-Bearing Livers
36. Carlsson PO, Liss P, Andersson A, Jansson L. Measurements of
oxygen tension in native and transplanted rat pancreatic islets.
Diabetes 1998; 47: 1027–1032.
37. Abdel-Halim SM, Ostenson CG, Andersson A, Jansson L,
Efendic S. A defective stimulus-secretion coupling rather than glu-
cotoxicity mediates the impaired insulin secretion in the mildly
diabetic F1 hybrids of GK-Wistar rats. Diabetes 1995; 44: 1280–
1284.
38. Hildebrandt W, Blech W, Kohnert KD. Kinetic studies on
hepatic handling of glucagon using the model of non-
recirculating perfused rat livers. Horm Metab Res 1991; 23: 410–
413.
39. Ikeda T, Terasawa H, Ishimura M et al. Hepatic extraction and
hepatic action of insulin, glucagon, and epinephrine in bivascularly
perfused rat liver. Jpn J Physiol 1993; 43: 371–378.
40. Gromada J, Rorsman P. New insights into the regulation of
glucagon secretion by glucagon-like peptide-1. Horm Metab Res
2004; 36: 822–829.
41. Leclercq-Meyer V, Malaisse WJ. Dual mode of action of glucose
pentaacetates on hormonal secretion from the isolated perfused
rat pancreas. Am J Physiol 1998; 275 (4 Pt 1): E610–E617.
42. Efanova IB, Zaitsev SV, Efanov AM et al. Effects of imidazoline
derivative RX871024 on insulin, glucagon, and somatostatin se-
cretion from isolated perfused rat pancreas. Biochem Biophys Res
Commun 1998; 252: 162–165.
43. Silvestre RA, Rodriguez-Gallardo J, Egido EM, Marco J. Interrela-
tionship among insulin, glucagon and somatostatin secretory re-
sponses to exendin-4 in the perfused rat pancreas. Eur J Pharma-
col 2003; 469: 195–200.
44. Zhou H, Tran PO, Yang S et al. Regulation of alpha-cell function by
the beta-cell during hypoglycemia in Wistar rats: The “switch-off”
hypothesis. Diabetes 2004; 53: 1482–1487.
American Journal of Transplantation 2006; 6: 967–975 975





























