Embed Size (px)
Citation preview

Isla Ogilvie1, Antoine El Khoury2,3, Yadong Cui2, Erik Dasbach2, John D. Grabenstein2, Mireille Goetghebeur1
1BioMedCom Consultants inc., Montreal, Quebec, Canada; 2Merck & Co., Pennsylvania, USA; 3University of Arkansas for Medical Sciences, Arkansas, USA
Acknowledgements
The authors wish to thank Philippe de Wals MD, PhD, from Laval University, Quebec City, Québec, Canada for his expert validation of the analysis of relevance and validity of economic evaluations included in this review as well as for his suggestions and comments on the manuscript. We would also like to thank Lonny Erickson PhD and Randy Levitt PhD from BioMedCom for their contributions to the analysis of the literature as well as Donna Rindress from BioMedCom for her suggestions and comments. This study was funded by Merck & co.
Conclusion This review identified 11 economic evaluations comparing PPV-23 vaccination with
no vaccination
The majority of studies reported that vaccination of over 65 year olds with PPV-23 was a cost-effective (less than US$50,000 per LYG or per QALY), and in some cases a cost-saving, strategy for the prevention of IPD
Studies that specifically included pneumococcal pneumonia reported lower cost-effectiveness ratios, compared to those studies limited to IPD
Structured assessment revealed that the relevance and strength of the studies was limited by data available on vaccine effectiveness, and by data on incidence and case-fatality rates of IPD and pneumonia
While PPV-23 is known to offer protective efficacy against IPD the precise level of efficacy is unclear especially in elderly and high risk groups
This gap in the available efficacy data affected the relevance and strengths of all studies examined.
The relevance and strength of economic evaluations was also affected by the variability of IPD incidence rates reported in different countries, which partly explains the large variability in ICERs
Limitations of this study
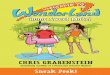
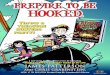
The comparison of ICERs across countries is challenging given different settings, study design, strength of the study, currency and outcomes. Although ICERs have been standardized to a single currency and year and plotted on the same graph (Figure 2), comparison across countries may not be feasible because of the variation in purchasing power across these nations
The subjective nature of assessing the relevance and strength of a study; an instrument promoting transparent critical analysis and reporting of studies was combined with a deliberative process and expert validation
All but one of the economic analyses reviewed utilized incidence rates and serotype distributions measured before the introduction of PCV-7, 29 and therefore the studies may not reflect the current context.
Further economic evaluations may be warranted based on new data on vaccine efficacy and the epidemiology of IPD in adult populations
AimThe objective of this study was to conduct a structured and systematic review of the recent literature on the economic evaluations of pneumococcal polysaccharide vaccination in adults.
Introduction Pneumococcal disease (PD) due to S. pneumoniae includes both non-invasive
infections—such as community acquired pneumonia (CAP), otitis media, and other upper respiratory tract infections—,and invasive disease (IPD), and is a major cause of morbidity and mortality in adults, leading to substantial clinical and economic burden worldwide1
The US Active Bacterial Core Surveillance program reported an incidence for IPD of 43.3 per 100,000 children under 1 year of age and 39.6 per 100,000 for the population aged over 65 years in 2007;2 the incidence of CAP is also higher among the elderly population than for other age groups3-6
An invasive infection such as IPD poses significant demands on healthcare resources because it generally leads to hospital admission; one Canadian study estimated that the economic burden was 2004 US$500,000 per 100,000 persons of the Canadian population7
Currently a 23-valent pneumococcal polysaccharide vaccine (PPV-23) is widely used for the prevention of pneumococcal infections;8 PPV-23 is indicated
primarily for the immunization of adults, and children with chronic diseases9
The most recent Cochrane Review of randomized clinical trials (RCT) concluded that PPV-23 is protective against IPD in healthy adults from high-income countries, but evidence is equivocal for its effectiveness against IPD in patients with chronic illness;10 efficacy findings from observational studies concluded that PPV-23 provides protective efficacy for IPD in immunocompetent adults, including those over 55 years of age10
Previous reviews of the cost-effectiveness of PPV-23 reported that vaccination was cost effective;11,12 however, to our knowledge, no systematic review of the literature on the cost-effectiveness of PPV-23 has yet been done
Cost-Effectiveness of Pneumococcal Polysaccharide Vaccination in Adults: A Systematic Review of Conclusions and Assumptions
References 1 Butler JC. Epidemiology of pneumococcal disease The pneumococcus. Washington, DC: 2004. p. 148-68.
2 Centers for Disease Control and Prevention. Active Bacterial Core Surveillance (ABCs) report emerging infections program network Streptococcus pneumoniae, 2007-provisional. 2008. www.cdc.gov/ncidod/dbmd/abcs/survreports/SPNEUMO_2007_provisional.pdf. (Accessed 3 Sep 2008).
3 Ruiz-Gonzalez A, Falguera M, Nogues A, Rubio-Caballero M. Is Streptococcus pneumoniae the leading cause of pneumonia of unknown etiology? A microbiologic study of lung aspirates in consecutive patients with community-acquired pneumonia. Am J Med. 1999;106(4):385-90.
4 Nelson JC, Jackson M, Yu O, Whitney CG, Bounds L, Bittner R, et al. Impact of the introduction of pneumococcal conjugate vaccine on rates of community acquired pneumonia in children and adults. Vaccine. 2008;
5 Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44 Suppl 2:S27-S72
6 Brown PD, Lerner SA. Community-acquired pneumonia. Lancet. 1998;352(9136):1295-302.
7 Morrow A, De Wals P, Petit G, Guay M, Erickson LJ. The burden of pneumococcal disease in the Canadian population before routine use of the seven-valent pneumococcal conjugate vaccine. Can J Infect Dis Med Microbial. 2007;18(2):121-7.
8 Makela PH, Butler JC. History of immunization Pneumococcal Vaccines: the impact of conjugate vaccine. Washington, DC: 2008. p. 19-27.
9 De Graeve D, Beutels P. Economic aspects of pneumococcal pneumonia: a review of the literature. Pharmacoeconomics. 2004;22(11):719-40.
10 Moberley SA, Holden J, Tatham DP, Andrews RM. Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2008;(1):CD000422
11 Beutels P, Postma MJ. Economic evaluations of adult pneumococcal vaccination strategies. Expert Rev Pharmacoeconomics Outcomes Res. 2001;1(1):47-58.
12 Postma MJ, Heijnen ML, Beutels P, Jager JC. Pharmacoeconomics of elderly vaccination against invasive pneumococcal infections: cost-effectiveness analyses and implications for The Netherlands. Expert Rev Vaccines. 2003;2(4):477-82.
13 Goetghebeur M, Wagner M, Khoury H, Levitt R, Erickson LJ, and Rindress D. Evidence and value: impact on decisionmaking – the EVIDEM framework and potential applications. BMC Health Services Research 2008;8:270
14 Evers SM, Ament AJ, Colombo GL, Konradsen HB, Reinert RR, Sauerland D, et al. Cost-effectiveness of pneumococcal vaccination for prevention of invasive pneumococcal disease in the elderly: an update for 10 Western European countries. Eur J Clin Microbiol Infect Dis. 2007;26(8):531-40.
15 Ament A, Baltussen R, Duru G, Rigaud-Bully C, De Graeve D, Ortqvist A, et al. Cost-effectiveness of pneumococcal vaccination of older people: a study in 5 western European countries. Clin Infect Dis. 2000;31(2):444-50.
16 Merito M, Giorgi RP, Mantovani J, Curtale F, Borgia P, Guasticchi G. Cost-effectiveness of vaccinating for invasive pneumococcal disease in the elderly in the Lazio region of Italy. Vaccine. 2007;25(3):458-65.
17 De Graeve D, Lombaert G, Goossens H. Cost-effectiveness analysis of pneumococcal vaccination of adults and elderly persons in Belgium. Pharmacoeconomics. 2000;17(6):591-601.
18 Smith KJ, Zimmerman RK, Lin CJ, Nowalk MP, Ko FS, McEllistrem MC, et al. Alternative strategies for adult pneumococcal polysaccharide vaccination: A cost-effectiveness analysis. Vaccine. 2008;26(11):1420-31.
19 Parsons HK, Tomlin K, Metcalf SC, Brazier JE, Dockrell DH. The economic cost of invasive pneumococcal disease and the potential for reduction by vaccination in an adult population in South Yorkshire. QJM. 2006;99(5):348-9.
20 Postma MJ, Heijnen ML, Jager JC. Cost-effectiveness analysis of pneumococcal vaccination for elderly individuals in The Netherlands. Pharmacoeconomics. 2001;19(2):215-22.
21 Mangtani P, Roberts JA, Hall AJ, Cutts FT. An economic analysis of a pneumococcal vaccine programme in people aged over 64 years in a developed country setting. Int J Epidemiol. 2005;34(3):565-74.
22 Melegaro A, Edmunds WJ. The 23-valent pneumococcal polysaccharide vaccine. Part II. A cost-effectiveness analysis for invasive disease in the elderly in England and Wales. Eur J Epidemiol. 2004;19(4):365-75.
23 Sisk JE, Whang W, Butler JC, Sneller VP, Whitney CG. Cost-effectiveness of vaccination against invasive pneumococcal disease among people 50 through 64 years of age: role of comorbid conditions and race. Ann Intern Med. 2003;138(12):960-8.
24 Sisk JE, Moskowitz AJ, Whang W, Lin JD, Fedson DS, McBean AM, et al. Cost-effectiveness of vaccination against pneumococcal bacteremia among elderly people. JAMA. 1997;278(16):1333-9.
25 Hicks LA, Harrison LH, Flannery B, Hadler JL, Schaffner W, Craig AS, et al. Incidence of pneumococcal disease due to non-pneumococcal conjugate vaccine (PCV7) serotypes in the United States during the era of widespread PCV7 vaccination, 1998-2004. J Infect Dis. 2007;196(9):1346-54.
26 Plans P. [Cost-effectiveness of 23-valent antipneumococcical vaccination in Catalonia (Spain)]. Gac Sanit. 2002;16(5):392-400.
27 Shapiro ED, Berg AT, Austrian R, Schroeder D, Parcells V, Margolis A, et al. The protective efficacy of polyvalent pneumococcal polysaccharide vaccine. N Engl J Med. 1991;325(21):1453-60.
28 Butler JC, Breiman RF, Campbell JF, Lipman HB, Broome CV, Facklam RR. Pneumococcal polysaccharide vaccine efficacy. An evaluation of current recommendations. JAMA. 1993;270(15):1826-31.
29 Sims RV, Steinmann WC, McConville JH, King LR, Zwick WC, Schwartz JS. The clinical effectiveness of pneumococcal vaccine in the elderly. Ann Intern Med. 1988;108(5):653-7.
30 Farr BM, Johnston BL, Cobb DK, Fisch MJ, Germanson TP, Adal KA, et al. Preventing pneumococcal bacteremia in patients at risk. Results of a matched case-control study. Arch Intern Med. 1995;155(21):2336-40.
31 Melegaro A, Edmunds WJ. The 23-valent pneumococcal polysaccharide vaccine. Part I. Efficacy of PPV in the elderly: a comparison of meta-analyses. Eur J Epidemiol. 2004;19(4):353-63.
32 Mangtani P, Cutts F, Hall AJ. Efficacy of polysaccharide pneumococcal vaccine in adults in more developed countries: the state of the evidence. Lancet Infect Dis. 2003;3(2):71-8..
MethodsLiterature search
An extensive literature search was conducted to identify articles published from 1997 to 2007 pertaining to the economic evaluation of the PPV-23 vaccine against pneumococcal disease in the adult population.
Comparative analysis of economic evaluations
The impact of setting, design and model parameters on cost-effectiveness ratios were explored in a comparative analysis of the economic studies identified
To provide an overview of the selected studies, the data was systematically extracted: type of economic analysis; time horizon; perspective; setting; study cohort base-year currency; costs (including vaccination costs; hospitalization costs; medication
costs; physician visits, and indirect costs such as productivity); discount rate; data sources for incidence and mortality of pneumococcal disease; vaccine-efficacy assumptions; cost-effectiveness ratios and results of sensitivity analysis.
The funding source of each study was also considered
All costs were standardized to 2007 US$ using the consumer price index and the appropriate exchange rate for 2007
Assessment of relevance and strengths of the economic evaluations
The relevance and strengths of each study was assessed using a semi-quantitative instrument designed to explore economic evaluations, developed as part of the EVIDEM framework13
It allows analysis and reporting of the relevance and strengths of an economic evaluation in a structured fashion by prompting systematic consideration of the following 11 dimensions: target population, intervention and setting, comparator, perspective and costs outcome measures, parameter estimates and sources, time horizon, discount rate, event pathway/model, sensitivity analysis, and conclusions
Transparent reporting for each dimension of the instrument was combined with a three-step deliberative process to reach a consensus on potential limitations in relevance and strength of studies. Firstly, an evaluator analyzed each study and provided comments for each dimension All evaluations were then reviewed by a second investigator Comments were validated by an independent expert
Although the EVIDEM instrument can be used to assign a score for each study based on a quantitative assessment, we opted to adapt the instrument by using only the qualitative evaluation component of it, and to focus our analysis on the relevance, strength and limitations of the assumptions and conclusions of the studies
Results A literature search recovered 31 cost-effectiveness studies pertaining to the
use of PPV-23 for the prevention of pneumococcal disease in adults
Eleven studies comparing the cost-effectiveness of PPV-23 vaccination with no vaccination were included in this analysis14-24
Comparative analysis of economic evaluationsCost-effectiveness ratios from the studies were compared by disease; age group; country; and perspective (societal or healthcare); the majority reported that vaccination was cost-effective (< $50,000 per life-year gained [LYG] or per quality-adjusted life-year [QALY] gained) for the prevention of IPD in adults
Impact of indication on cost-effectiveness All but one of the studies evaluated the cost-effectiveness of PPV-23 for the
prevention of IPD only, in the base-case analysis; incremental cost-effectiveness ratios (ICERs) ranged from $9,810 to $26,160 per LYG and from -$9.08 (cost-saving) to $53,955 per QALY.
For studies examining pneumococcal pneumonia, cost-effectiveness ranged from -$221 per LYG (cost-saving) to $30.4 per LYG and from cost-saving to $3,379 per QALY17,21
Cost-effectiveness by country Two related European studies compared cost-effectiveness from country to
country;14,15 other studies were from Belgium,17 Italy,16 the Netherlands,20 the UK19,21,22 and the US23,24
Cost-effectiveness for the ≥ 65 years old population varied from country to country but was below $50,000 per LYG or per QALY in most cases
Impact of perspective and costs on cost-effectivenessMost studies used a healthcare perspective, excluding indirect costs; one study used a societal perspective (including lost productivity) and estimated a base-case ICER of $10,999 per LYG for the vaccination of ≥ 65 year olds21
Figure 1: Literature search and study inclusion
Cost-effectiveness of vaccination with PPV-23 in the post-7-valent pneumococcal conjugate vaccine (PCV-7) era The introduction of PCV-7 has been associated with a marked decrease in disease
incidence caused by PCV-7 serotypes in the elderly population as well as among infants25
Only one study used incidence data from the post-PCV-7 era (2003–2004) and reported that the cost-effectiveness of vaccinating over 65 year olds with PPV-23 was $3,714.52 per QALY18
Cost-effectiveness, effect of age and comorbidities Most studies investigated the cost-effectiveness of PPV-23 vaccine against IPD in
≥ 65 year olds; in general, vaccination was cost-effective for this age group, and cost-saving in one US study24
Base-case values ranged from $9,810 to $34,375 per LYG,16,20 and from -$9.08 per QALY (cost-saving) to a cost of $53,955 per QALY15
Critical parameters Sensitivity analysis was performed in 10 of the studies; vaccine efficacy was a
critical parameter in most studies and accounted for the largest variation in cost-effectiveness values in 4 studies14,15,20,24
Incidence rates of IPD and pneumococcal pneumonia were also a major source of variability in cost-effectiveness results for many studies, as were case-fatality rates 14-17,20-24,26
Relevance and strengths of the economic evaluationsStructured assessment of the relevance and strengths of studies, using the EVIDEM instrument, revealed that most studies most studies used relevant patient populations, outcomes, and perspectives; all studies compared vaccination with PPV-23 to no vaccination
Vaccine efficacy assumptions Structured assessment showed that the efficacy and effectiveness data for PPV-23
vaccination against IPD available to these studies limited the strength and relevance of most of the studies
Efficacy estimates for vaccine-related types of bacteremic pneumococcal disease varied between studies, from 22%–75%21,27
Three studies assumed that vaccine efficacy against pneumococcal pneumonia was the same as for IPD,15,17,21 this affected the strength of their economic analyses
Most studies used a duration of protection of the vaccine of between 5 and 6.5 years based on Shapiro et al, 1991 which found that vaccine efficacy fell with time since vaccination;27
Epidemiological assumptions for IPD and pneumococcal pneumonia Structured assessment also revealed that data sources for the incidence of IPD and
case-fatality due to IPD also affect relevance and strengths
Studies used IPD incidence data from a variety of sources including public-health surveillance; ICD-9 codes for pneumococcal-related hospitalizations; local clinical microbiology laboratory data; and data from published sources
There was substantial variation in the input values used for incidence rates of IPD; from 20.5 to 50 cases per 100,000 population for 65 to 74 year olds
This variation in input values accounts for much of the variation in cost-effectiveness ratios between and within studies
Case-fatality rates were also obtained from a range of data sources including public-health surveillance, hospital-registration data, and international literature
The range of case-fatality rates used by these studies was large, ranging from 4.65%–30% for the 65 to 74 year old age group
-5,000
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
55,000
Co
st
eff
ecti
ven
ess (
2007 U
S$ p
er
QA
LY
)
Evers, 2007
Ament, 2000
Smith, 2008
Sisk, 1997
Sisk, 2003 (50-60 year olds)
Be
lgiu
m
Be
lgiu
m
Den
ma
rk
En
gla
nd/W
ale
s
Fra
nce
Ge
rma
ny
Italy
Neth
erl
an
ds
Sco
tland
Sp
ain
US
Sp
ain
Fra
nce
Sco
tland
Sw
ed
en
Sw
ed
en
US
US
(no
n-b
lack
s)
US
(bla
cks)
2007 US$ 50,000
-5,000
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
55,000
Co
st
eff
ecti
ven
ess (
2007 U
S$ p
er
QA
LY
)
Evers, 2007
Ament, 2000
Smith, 2008
Sisk, 1997
Sisk, 2003 (50-60 year olds)
Be
lgiu
m
Be
lgiu
m
Den
ma
rk
En
gla
nd/W
ale
s
Fra
nce
Ge
rma
ny
Italy
Neth
erl
an
ds
Sco
tland
Sp
ain
US
Sp
ain
Fra
nce
Sco
tland
Sw
ed
en
Sw
ed
en
US
US
(no
n-b
lack
s)
US
(bla
cks)
Be
lgiu
m
Be
lgiu
m
Den
ma
rk
En
gla
nd/W
ale
s
Fra
nce
Ge
rma
ny
Italy
Neth
erl
an
ds
Sco
tland
Sp
ain
US
Sp
ain
Fra
nce
Sco
tland
Sw
ed
en
Sw
ed
en
US
US
(no
n-b
lack
s)
US
(bla
cks)
2007 US$ 50,000
2a) Base-case cost-effectiveness per quality adjusted life year (QALY)
Figure 2: Cost-effectiveness of vaccinating adults (≥ 65 years of age unless otherwise indicated) against IPD with the 23-valent pneumococcal polysaccharide vaccine
Study Population/setting Protective efficacy (%: 95% CI) Studies using data
Efficacy Duration of protection
Shapiro, 199127
US
Case-control study; N=1054 patients with IPD confirmed by isolation of vaccine serotype S. pneumoniae: 1054 controls were matched by age, underlying illness, and site of hospitalization; Median age: 67.6 years; age range 18-99 years
Aggregate protective efficacy of PPV-23 against serotypes in the vaccine in immunocompetent patients by age group and time since vaccinationAge (years) Time since vaccination: Protective efficacy (%: 95% CI)
<3 years 3–5 years >5 years<55 93 (82–97) 89 (74–96) 85 (62–94)55-64 88 (70–95) 82 (57–93) 75 (38–90)65-74 80 (51–92) 71 (30–88) 58 (-2–83)75-84 67 (20–87) 53 (-15–81) 32 (-67–72)≥ 85 46 (-31–78) 22 (-90–68) -13 (-174–54)
14-18, 20,23,24
14-18, 22-24
Protective efficacy (%: 95% CI) Duration of protection (%: 95% CI)
Butler, 199328
USIndirect cohort study; N=2837 persons with IPD confirmed by isolation of S. pneumoniae; Median age 57 years for vaccinated; 50 years for unvaccinated)
Efficacy for immunocompetent patients stratified by ageAge Protective efficacy (%: 95%CI)Overall 60% (30%-77%)65-74 years 70% (30%–87%) ≥ 75 years 78% (54%–89%)
Vaccine efficacy and time since vaccination†
Interval Protective efficacy (%: 95%CI)<2 years 51% (22%–69%)2-4 years 54% (28%–70%)5-8 years 71% (24%–89%)≥ 9 years 80% (16%–95%)
17 19,21
Sims, 198829
USCase-control study; 85 patients with pneumococcal bacteremia; 152 matched controls
Efficacy against IPDAll: 81%
n/a 17
Farr, 199530
USMulticenter, case-control study; 244 controls and 122 patients hospitalized for IPD; aged ≥ 55 years
Efficacy against IPDAll: 70% (37%– 86%)
n/a 17
Melegaro, 200431
International
Meta-analysis of efficacy studies for PPV-23 against pneumonia and IPD in the elderly (≥ 65 years old)
Efficacy against IPD (≥ 65 years old)All: 65% (-49%–92%)
n/a 22
Mangtani, 200332
International
Systematic review of RCTs and observational studies on the efficacy of PPV-23 against IPD
Efficacy against IPD (≥ 65 years old): RCTs: 30%–47%Observational studies: 47%–81%
Non-bacteremic pneumonia/IPD: 37.5%
n/a 21
CI: confidence interval; IPD: invasive pneumococcal disease; PPV-23 pneumococcal polysaccharide vaccine -23 serotypes†Matched analysis of vaccinated and unvaccinated patients; all ages ‡High risk patients were defined as those with COPD, bronchogenic carcinoma and other chronic conditions
Table 1: Sources of vaccine efficacy data
Revaccination
Revaccination with PPV-23 is currently recommended in many European countries, but is not recommended routinely in the US
Revaccination was included in two UK cost-effectiveness studies,21,22 and in the two multicounty European studies,14,15 as well as in one US study18
2b) Base-Case cost-effectiveness per life year gained (LYG)
Literature search: Abstracts identified 31 studies
Possible studies identified 13 studies
Excluded: Only total costs reported 1 studyPPV-23 costs assessed with another intervention 1 study
Excluded: not relevant/no cost data 18 studies
Studies included in analysis: 11 studies
Ita
ly
Net
her
land
s
UK
UK
UK
(M
in I
CE
R)
UK
(M
ax I
CE
R)
2007 US$ 50,000










![EXCLUDED MINORS AND THE RIBBON GRAPHS OF …By considering graphs in orientable surfaces of higher genus, Dasbach, Futer, Kalfagianni, Lin and Stoltzfus in [8] (see also Turaev [24])](https://img.pdfslide.us/doc/110x75/5fc5993dcfaacc342948c02e/excluded-minors-and-the-ribbon-graphs-of-by-considering-graphs-in-orientable-surfaces.jpg)







![(joint with Oliver T. Dasbach) Matilde N. Lal´ınmlalin/mpi2show.pdf · A ∈ MgC[t,t−1] the right-hand side is 2m(det(A)). (joint with Oliver T. Dasbach) Matilde N. Lal´ın (UBS-PIMS,](https://img.pdfslide.us/doc/110x75/5f30c5378b2f64420e02cc6f/joint-with-oliver-t-dasbach-matilde-n-laln-mlalinmpi2showpdf-a-a-mgctta1.jpg)