Embed Size (px)
Citation preview

Is Your Organization a HRO?
(High Reliability Organization)
How can you tell? If not, why Not ?
David EiblingUniversity of Pittsburgh, VA Pittsburgh
CRNA Conference April 11, 2014

What is a “High Reliability Organization” ?
Work groups that function in high stress environments– Highly Complex– Tightly Coupled– High levels of Uncertainty– High Production Pressure
And – have fewer adverse events than expected
Seemingly exempt from “Normal Accidents”

“Normal” AccidentsClassic research by Perrow, Sagan and
othersStudied accidents that occured during
“normal” operations– Nuclear power, Petro-chemical plants
Accident rate and impact modified by numerous factors
“Accidents are Inevitable in complex andtightly coupled systems”Sagan 1993

From NASA PPT

Examples of HROs
Navy carrier operationsSpace Shuttle flights
– Despite two catastrophic crashesCommercial aviation
There is a science!

Deciphering the “R: in HROs
Research dates back to 1980’sOrganizational Theory researchers
– LaPorte, Rochlin, Roberts, Weick, Schulman
– Why do Organizations do what they do?Extensive literature
– Academics tend to be in schools of business and public policy
Science just starting to be recognized in medicine

Characteristics of
High Reliability Organizations
Preoccupation with Failure– What could happen?
Reluctance to Simplify– Always more complex than seems
Sensitivity to Operations– What are we doing?
Commitment to Resilience– What will stop the chain of error?
Deference to expertise– Not always apparent who has it

Where is Healthcare? Medical Error 8th most
common cause of death in US– Recent paper suggests is
3rd most common* Chances of ADE range
from 2 -7 /100 Everyone has a story
*James Journ Pat Safety 2013
Doesn’t seem very reliable

Lets go back 40 Years to
1973
George Foreman knocks out Joe FrazierHoward Cosell shouts “Down goes Frazier,Down goes Frazier, Down goes Frazier”
Yon Kippur warOPEC cuts off oil

1973
Henry Kissinger wins Nobel Peace Prize
Watergate Hearings begin
Rose Mary Woods accidentally erases the tape

1973
Pioneer 10 sends back first close-up pictures of Jupiter Monica Lewinski
is born

1973Emergency Rooms are
just rooms –
Eibling begins his internship at Wilford Hall, San Antonio
Tx

A tale of multiple errors
18 Y/O man falls/jumps from 3rd floor barracks– Chest trauma
Transported to Wilford Hall USAF Med Center
On-call surgeon (Eibling) paged STAT– mid – July 1973

A tale of multiple errors
Patient combative, pale, tachypneic
Unable to obtain vital signsObvious contusion over
lateral thoraxReduced breath soundsPaged Thoracic surgery STAT#14 angio placed in hand

A tale of multiple errors
IV lost immediatelyChief of Cardiac surg arrivesMultiple attempts to restart IV
– Saphenous cut-down attemptedPatient codesPatient diesAutopsy demonstrates lung
laceration & hemothorax – no liver/spleen lac

A tale of multiple errors
Morbidity and Mortality Conference one week later
Focus on Eibling’s actions/lack thereof– Why didn’t you restrain patient?– Why didn’t you place antecubital line?– Why didn’t you place chest tube?– Why did you wait so long to intubate?– Why didn’t you call for help?

We couldn’t imagine that . .
The system could be improved Dedicated Emergency Medicine
physicians would improve outcomes Trauma teams should take group call
– Rapid response teams should train together– That Resuscitation training and ATLS would
save lives That fixing the intern wouldn’t solve
the problem That our system was not “highly
reliable”

20 Years Later “Error in Medicine”
JAMA 1994

Error in MedicineLucian Leape JAMA 1994
Landmark Paper tying Concepts of Human Error (by Reason) to Medical Error
Amazingly pertinent even today Emphasized extent of problem
– Harvard Medical Practice study 1991 Quoted Schimmel’s 1964 report
– Prospective analysis of 1014 medicine patients at Yale-New Haven Hospital
Emphasized value of voluntary reporting “at the bedside by the caregivers themselves”

To Err is Human
Institute of Medicine 1999
Emphasized role of human error in poor outcomes
Estimated Medical Error Results in 44,000 - 98,000 deaths yearly in US(Actual figures much greater)
Emphasized necessity of studying errors
The title tells it all . . . .
Humans are Imperfect – we must design systems that take such imperfections into account

Are we there Yet?Consensus is no substantial improvement since 1999 To Err is Human

Pre-procedure checklists
Time out
Marking sites
Medication safety
Learning from mistakes
Root Cause Analysis
Using Checklists
Patient Safety Goals
Team huddles
Hand off communication tool
Bar coding
CPRS Alerts
Simplification
Standardization
Avoid reliance on memory
Hand hygiene focus
Progress has been made –But has been incremental – not Transformational*
*Anesthesia may be exception to the rule

“There is nothing New Under the Sun”
“Human Error in medicine, and the adverse events that may follow, are problems of psychology and engineering, not of medicine”John Senders, Chapter 9 Human Error in Medicine

WHY so little Improvement ?
Maybe this story will help explain it . . . . . . . .

Who is to Blame?The Patient – 2013
60 y/o smoker with 2 cm pleomorphic adenoma On VA disability for PTSD, tinnitus, hearing loss, diabetes
(HbA1c 9.9) Additional co-morbidities: hypertension, hyperlipidemia, prior
gastric bypass for morbid obesity, prior CABG, known OSA, known ETOH abuse history
Multiple medications managed by non-VA primary care doctor (“shared care”)– Patient not aware of medications/doses “my wife manages my
medications” Preop eval by IMPACT clinic
– Med list in CPRS reviewed– Some meds from VA, some from outside pharmacy– Wife not present for IMPACT, no information from non-VA PCP

Who is to Blame?The Case
Uneventful Parotidectomy– Post-op hypertension to systolic >200
Urgent medicine consult – HTN - likely multifactorial given anxiety w/o SSRI, pain, ?OSA, CKD and likely under-treated HTN at baseline with
goal BP ~130/80. on metoprolol currently as outpatient only which is less than ideal. allergy to Ace/ARB documented and with GFR ~30 HCTZ likely to be less effective. Would recommend starting 2.5 mg of amlodipine now, restarting his SSRI at home dose, continuing Metoprolol and treating pain PRN. prn hydralazine or clonidine as needed for SBP>180. Would recheck Chem8 in AM.
Small hematoma opened prior to DC– Discharged on prior medication regimen– New BP med missed in discharge orders (communication
failure? slip?) In dictated DC summary, not on nursing DC note
ER 2 days later admitted 6 days post op for additional management with uncontrolled hypertension– Med consultant discovered prior (non-VA PCP) dosing of
metoprolol as well as missing ACEI/diuretic combo not reflected in any available med list

Who is to Blame?Context
“Shared care” – Care coordinated with VA and non-VA PCP– Exception rather than rule (most frequent example is
anticoagulation)– Extensive templated notes 1 yr and 6 months previously
– “Medications reconciled”– No data from outside PCP in most cases
VA med co-pay $9.00 per month per med (NSC). Generic meds at Wallmart $4.00 per month or $10.00 for 3 months. ($68 per med per year)– What would YOU do?– Relies on human to enter/update non-VA meds
Medication Recognition?

Assigning Blame Medication reconciliation known problem
– Failure to “reconcile” at discharge well known issue– No single time-linked display of medications across
continuum of care Previously reported to internal system- 3 work
groups have addressed– Pharmacy work group developed single combined list
of all meds (multiple problems such as duplicates)– Engineering group – formal study instituted by
Patient Safety group concluded that with constraints of information system best solution is to assign dedicated pharmacist to inpatient med-rec
Level 3 Peer review level assigned to attending for all medication reconciliation errors
What do you think has happened?
“It will be evident to anyone who has read the foregoing pages, that the history of the problem of error does not bear witness to a steady and well defined progress, from initial perplexity, through stages of ever increasing light, up to a final and triumphant solution. Perhaps it was hardly to be expected in the case of a question so baffling in itself, so open to evasions, and so dependent on others of
positive interest. The same difficulties keep coming back under slightly difficult forms, the same postulates and general distinctions, the same ambiguities and incoherences; til one begins to wonder whether after all it is possible to give a rational and philosophic account of this irrational product of the mind”
Keller The problem of error from Plato to Kant 1934

And just this Monday . . . .
Finding med list from “Spoke” Hospitals(Don’t appear in CPRS Meds Tab)
Click here
But this only lists meds from VA PharmacyHere’s how you find the rest of them

To find all meds from spokes you need to go to “Health Summary”(near bottom of list)
ClarksburgEriePittsburgh
Click to open Clarksburg Health Summary

Now this list opens in Health Summary(partial list – too long for slide)
Click on Medication Reconciliation

Now click on the specific site health summary “Med Rec”
Non-VA Meds NOT in Pharm Tab
AsprinAtorvastatinBudesonideCelecoxibDutasteride (twice)LansoprazoleLatanoprost (twice)Levothyroxine Metformin MetasoneLodrane D herbal??PatanaseOlopatadinePioglitazoneRamiprilTerazosin
What would an HRO Do?
Preoccupation with Failure Reluctance to Simplify Sensitivity to Operations Commitment to Resilience Deference to expertise
Can we use an event as a “biopsy” ?
What would an HRO Do?
Preoccupation with Failure– Constantly asking “why do we have so many med rec errors?” – Med rec failures would demand high level attention– Leadership would feel responsible and insist on a solution
Reluctance to Simplify– How does the system work, anyway?– What are the areas of linkage that contribute to failure?– What are the “little failures” that combine to cause catastrophe?– What is the context we work in - ie the larger systems such as
medication labeling, cost issues, etc– Why don’t we understand all of the components and links?

What would an HRO Do?
Sensitivity to Operations– What is really happening?– Who at the front line is using work-arounds?– What are these work-arounds and why are they necessary?– Who knows what is really happening and is ready to talk about it?
Commitment to Resilience– Where is the resilience in our system?– Where is resilience missing?– Are there areas of tight linkage that impair resilience?– How can we help our front line people stop the chain of error?

Humans are Source of System Resiliency and Adaptability
How many times each day do:– You– Your fellow practitioners– Your colleagues in other
specialties– Your OR nurses
Use a “Work-around” to solve some problem?
Studying Work-arounds is recognized as key to understanding human-system incompatabilities
Fix the system, not the human

What would an HRO Do?
Deference to expertise (Internal)– Who knows what is going on?
Is it the nurse? Resident? Pharmacist? Patient?
– Who might have ideas on how to reduce the likelihood of failure?
– Will we heed their observations and recommendations?– Are they willing to speak up?
“The greatest obstacle to discovery was not ignorance – it was the illusion of knowledge”Daniel Boorstin

How to Find out what “Sharp End” Practitioners Know ?
“Knowledge is more than information”
Challenge is to capture knowledge
Theme of the “Just Culture” movement
Overall, healthcare has done poorly– 2012 Safety Attitudes
survey - 40% not talking Involves more than
merely “Reporting”

What would an HRO Do?
– Deference to expertise (External)
– Are we the first to encounter this failure?– Has this been studied before and where are the reports?– What are others doing?– Are we willing to invest the time and resources to attend
meetings and study the literature when it exists?
“Education is learning that you didn’t even know what you didn’t know”Daniel Boorstin

Science of Error Not a new topic
– Cognitive psychologists Human Error
– James Reason Cambridge Press 1990
– Precipitated by major accidents of the 70’s
Attempted to answer the question– Why do we do what we
do? Leape tied Medical error
to Reason’s work

Triggers
Deflected Error
Accident
Defenses
Adapted from Reason 1990
The famous Swiss-cheese illustration
An HRO knows where the holes are – and worries about the ones it doesn’t know about

Slip versus MistakeAfter Reason
Slip is an error due to failure of execution– 1 Qt oil in Radiator– Occurs at the “Sharp End” of a
system Mistake is a fundamental
error in judgment– Often occurs at the “Blunt End”
of a system Slips are often due to
mistakes in system design

Human Error “Natural consequence” of human
adaptation to environmental stimulation
Focusing attentionRecognizing patterns“Filling in the blanks”Sequencing events
The same strategies we use to manage information overload !

Knowledge and error flow from the same mental sources, only success can tell the one from the other.”
Ernst Mach 1905

Human Error – the Scapegoat
Human Error serves valuable role for organizations
Blaming the human “absolves” organization from blame– Reduces work required to
understand event– Eliminates need to either
seek or alter underlying source(s)
Concept integrated into culture of medicine
“Any RCA that concludes “Human Error” was the cause has fundamentally failed” (Richard Cook Christopher Nemeth)
“If we design our way into difficulty we can design our way out.”(John Thakara)
AE’s nearly always more complex than appear initially
Organizations often restricted by regulatory forces, competing national goals, etc.
“Fish can’t see water”
VA examples legendary– Software issues
Medication recognition
– Patient photo in record

Physical Environment
Nurse
Pharmacy
Patient
Information System
Arm Band
In X-ray
location
Correct armband?
workload
How to print?
location
Pain needsDisease process
Out of bed
Family visitingworkflow
labeling
Medication ordering
Competing tasks
Interruptions
Log in tasks
Doctor
Competing tasks take nurse awayWard lay-out
Equipment fit in room?
Usability
Compatibility with EHR
Competing tasks
System reliability
Error checking
BCMA – An example of complexity

A Constant Theme
“The judgment that this was human error simply produces too many Institutional Benefits”
“By attributing my colleague’s accident to his inattention or stupidity, though, I make it possible to believe that the accident has no relevance for me”
Dekker

A Tale of Two Stories*
The Front line story versus the investigation– Focus on individual actions– Focus on retraining– Backward vs Forward looking
“Hindsight Biasis”
First and Second order Problem Solving***Cook, Woods 1997**Tucker and Edmundson

First Order Problem Solving
Worker compensates for system deficiencies– Classic “work-arounds”– The “Spackle Resident”– The system never is changed
Failure recognized as human failure– Unreliable, inattentive, etc.
Solution is by changing Human or role in process

Second Order Problem Solving:
Assume human actions result of something (or many things)
Begin by assuming assessments and actions of humans are predictable– Seek to understand roles of context and
competing goals as decision architects– Role of cognitive psychology
Much more challenging– Incongruent with prominent themes of
medicine

Hindsight Bias ¾ of all AEs “Human Error” Attribution easy when
outcome known Causal attribution relies on
social/psychological constructs– Previous learning– Context– Decision architects
Difficulties in “tracing back”
David WoodsMay be impossible to understand decision-making processes that led to AE

4 Reasons to Blame Individual
1. People are available to blame
2. People were there (maybe even lots of people)
3. Human performance in complex systems usually very good – (humans compensating for system) hence AEs are rare
4. Knowledge of outcomes when tracing backwards leads to incorrect assumptions regarding cognitive processes (outcome drives diagnosis)

Finding Out What HappenedWho does it right?
The Aviation Industry
Why?

Incentive for US Aviation Safety Reporting SystemWhy the emphasis on preventing aircraft accidents?
Public Visibility of aircraft accidentsCosts
– Economic costs of single event– Lives lost per event
The pilot is first at the scene!Our congressmen fly too

The Aviation Safety Reporting SystemHow does it work?
No-fault reporting of errors– No repercussions for pilot if reported in 10
days De-identified after verification of facts Reviewed by panel of retired pilots Specific recommendations for system
changes– Changes mandated by regulation– Disseminated to entire industry
Follow-up to verify compliance Establishes a culture of safety

Aviation Safety Reporting Systemwww.asrs.arc.nasa.gov
Note – NASA – Not FAA

How does it work?The Aviation Industry:
Accepts that Errors Happen Works to understand:
– Why? When? Where? “Even the little ones!” Begins by Reporting
– No Fault – “Everyone has expertise” Looks for root cause(s)
– Defective system – not defective people Fixes the system – not the individual Follow-ups to confirm fix has been
implemented

History of Human Factors Early years of aviation
checkered history Aircraft reliability
improved during WWII
Post-war introduction of jets did not go well
Began to realize cause not the airframe – but the pilot
Human Error
“If we design our way into difficulty we can design our way out.”(John Thakara)

Human Factors EngineeringA “new” applied science
Military began to realize aircraft too difficult to fly
G-forces, dehydration New technology
Pressure suits, etc. Cockpit controls Too much to remember
– Wheels-up landing Instrumentation
– Autopilot programing AA 965 Dec 21, 1995 Cali
Columbia
Teamwork Eastern Flight 401
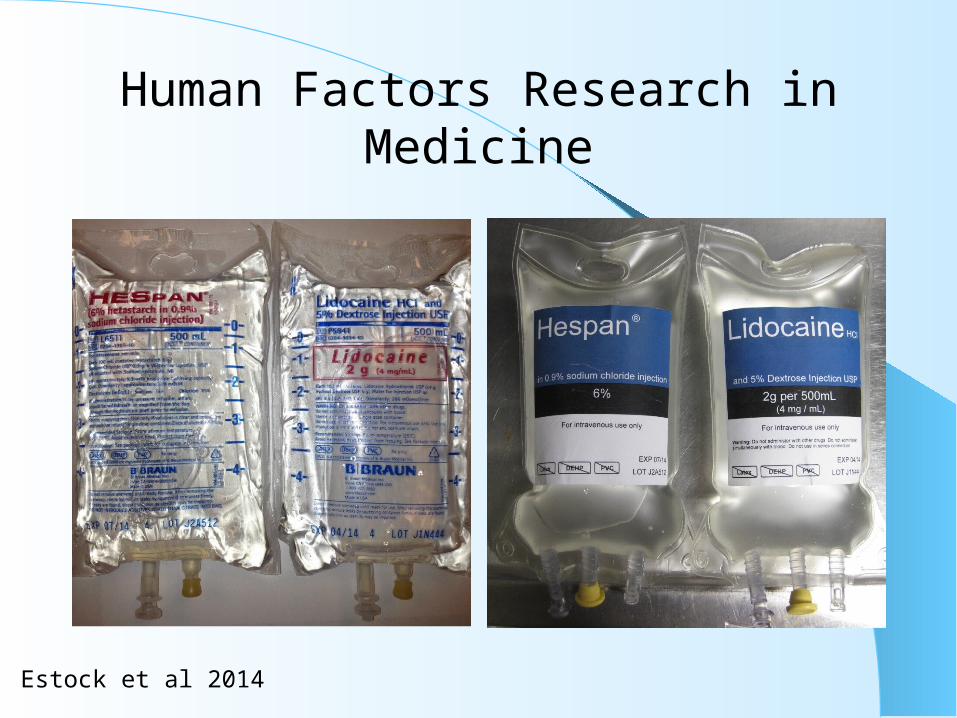
Human Factors Research in Medicine
Estock et al 2014

Some actions ARE blameworthyJust Culture in the Aviation Industry
Available fromhttp://204.108.6.79/products/documents/roadmap%20to%20a%20just%20culture.pdf
Global Aviation Information Network
“a no-blame culture is neither feasible nor desirable”Reason 1997
There are some rules you would never break
How do we define the line between acceptable and unacceptable behavior ?

“Just Culture”
“A just culture recognizes that competent professionals make mistakes and acknowledges that even competent professionals will develop unhealthy norms (shortcuts, routine rule violations), but has zero tolerance for reckless behavior.”(AHRQ website)
There is a “line in the sand” between driving 75 in a 65 MPH zone versus 75 down Fifth Ave
“Who draws the line is the most critical question”Dekker 2012

Culture of SafetyWhat is it we are talking about?
Patient Safety is first priority– Controversial
Leadership leads safety initiatives
Employees believe safety top priority for leadership
Employees empowered to speak up
Employees expect changes will be made to correct threats to safety
Measured by “Patient Safety Attitudes Survey”
Distributed and collated by AHRQ
Data published in February
Overall poor results
Most healthcare workers in US work in systems that address mistakes with name-shame-blame

Leadership is Key
“The most important question in establishing a Just Culture is Who gets to decide what is acceptable”
Dekker

So, What is Our Responsibility?
Recognize that most adverse events are due to latent errors
Highlight these latent errors in our hospitals, clinics, and offices
Educate leadership to the fundamentals of a culture of safety
Accept Responsibility for the Systems of care in which we care for our patients.

We can help our organizations become
HROsBegin by Reporting
Recognize that as front end staff YOU have expertise
Speak up and encourage others to report
Participate in analyses of failures– Look for the “second Story”
Don’t accept the Status Quo

High Reliability Organizations
consistently demonstrate a: Preoccupation with Failure
– What could happen?
Reluctance to Simplify– Always more complex than seems
Sensitivity to Operations– What are we doing?
Commitment to Resilience– What will stop the chain of error?
Deference to expertise– Not always apparent who has it
We CanShow the Way





























