Embed Size (px)
Citation preview

Journal of Affective Disorders 122 (2010) 267–272
Contents lists available at ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Research report
Is subclinical anxiety an endophenotype for bipolar I patients? A study froma Costa Rican sample
Javier Contreras a,b,⁎, Elizabeth Hare a, Adriana Pacheco b,Michael Escamilla a, Henriette Raventos b
a Psychiatric Genetics Research Center, Department of Psychiatry, University of Texas Health Science Center at San Antonio, San Antonio, Texas, USAb Centro de Investigación en Biologia Celular y Molecular, University of Costa Rica, San Jose, Costa Rica
a r t i c l e i n f o
⁎ Corresponding author. Centro de InvestigaciónMolecular, University of Costa Rica, San Jose, Costa R3187; fax: +506 2511 3190.
E-mail addresses: [email protected],[email protected] (J. Contreras).
0165-0327/$ – see front matter © 2009 Elsevier B.V.doi:10.1016/j.jad.2009.07.017
a b s t r a c t
Article history:Received 18 March 2009Received in revised form 20 July 2009Accepted 21 July 2009Available online 4 September 2009
Background: Although genetic influences on bipolar I disorder are well established, localizationof genes that predispose to the illness has been difficult. Some genes predisposing to bipolar Idisorder may be transmitted without expression of the categorical clinical phenotype. Onestrategy to overcome this obstacle is the use of quantitative endophenotypes, as has been donefor other medical disorders.Methods: We analyzed 30 bipolar I extended families (300 subjects, average family size 10.34members, range: 2–31) and 20 unrelated healthy controls from a Costa Rican sample.Heritability and genetic correlation of the state and trait scale from the Anxiety State and TraitInventory was computed by using the general linear model (SOLAR package software). We alsoassessed variation of both scores among groups (patients, relatives and controls) and testedindependence of affection status.Results: Heritability for state is 0.45 (SE=0.11, p=0.0000001) and for trait is 0.89 (SE=0.06,p=6.22e−29). Genetic correlation for state and trait is 0.29, (SE=0.12, p=0.038–3.19e−8).Bipolar I patients showed the highest trait score (F=12.17 [5,24], p=0.002), (bipolar IpatientsN relatives with other pathologies, Nhealthy relativesNunrelated healthy controls) withnormal distribution in healthy individuals and no difference regarding depression and maniacurrent status, (F=0.230, df=1, p=0.632 and F=1.401, df=1, p=0.238, respectively),contrary to the state score.Limitations: Confounding factors such as comorbid disorders could affect the interaction ofsubclinical anxiety with mania. Due to our limited budget we were not able to re-evaluate thesubjects and conduct a test retest to assess the STAI reliability and mood state independence ofanxiety traits over different times. Further research is needed to evaluate if anxiety traits arespecially related to bipolar I disorder in comparison with other traits such as anger, attention orresponse inhibition deficit, pathological impulsivity or low self-directedness.Conclusions: Anxiety state and trait are heritable and share some genetic factors but only traitshowed normal distribution in healthy subjects, mood current status independence andsignificant liability for bipolar I disorder. A stair-step distribution of trait anxiety scores in thefamily members and controls based on their genetic proximity to affected individuals anddiagnostic status suggests that trait anxiety could be an endophenotype in these bipolar I families.
© 2009 Elsevier B.V. All rights reserved.
Keywords:Bipolar disorderEndophenotypeGeneticsFamily studiesSubclinical anxiety
en Biologia Celular yica. Tel.: +506 2511
All rights reserved.
1. Introduction
Estimatesof theprevalenceof bipolar I disorder have rangedfrom 0.8% to 1.6% of the general population (Berns andNemeroff, 2003). The disorder is primarily defined by a history

268 J. Contreras et al. / Journal of Affective Disorders 122 (2010) 267–272
of a manic episode, although many patients experience bothmanic and depressive episodes. Many bipolar I patients showanxiety symptoms that can be very disabling in the case ofbipolar disorder. Anxiety symptoms are caused by an interac-tion of biopsychosocial factors, including genetic vulnerability,stress, or trauma which produce clinically significant syn-dromes in part through by the action of norepinephrine andserotonin (Schinka et al., 2004; Sen et al., 2004; Unschuld et al.,2007). High commorbidity rates for anxiety have beendocumented in bipolar I disorder (MacKinnon et al., 2002;Chen andDilsaver, 1995;McElroy et al., 2001; Feske et al., 2000;Keck et al., 1998); however, subclinical levels of anxiety havealso been associated with bipolar I patients who did not meetcriteria for a categorical Diagnostic and Statistical Manual ofMental Disorders (DSM-IV) anxiety disorder (Mantere et al.,2008). These individuals have poor outcomewith longer, morefrequent, and more difficult to treat mood episodes, are lessresponsive to lithium therapy, have earlier onset of symptomsand have greater functional impairment (McElroy et al., 2001).
Candidate gene association studies on the comorbidity ofthese two disorders have been controversial and replicationof findings has always been difficult (Rotondo et al., 2002). Todate, most genetic research has focused on the categoricalclassification and few have assessed anxiety as a quantitativephenotype (Wozniak et al., 2002).
Imprecision of psychiatric phenotyping might explain thefailure of genetic research to identify genes that contribute tosusceptibility of these two disorders where subjective assess-ments form the basis of both clinical and research diagnoses(Bearden et al., 2004). This lack of objective markers has, inturn, promoted substantial disagreements about the specificcriteria to define diagnostic categories, and the interpreta-tion of results from genetic studies. The need for a newapproach to psychiatric genetics has led to the introductionof the concept of endophenotypes (internal phenotypes thatlie intermediate between the gene and the disease itself)(Gottesman and Shields, 1973). It is assumed that genesinvolved in endophenotypic variation are likely to representmore elementary phenomena than those involved in com-plex psychiatric diagnostic entities. It is also used inter-changeably with the term ‘intermediate trait,’ describing aheritable quantitative phenotype believed to be closer in thechain of causality to the genes underlying the disease(Bearden and Freimer, 2006).
Many candidate endophenotypes for bipolar I disorder(e.g. neurocognitive functions, behavioral traits, sleep abnor-malities) have been proposed (Gottesman and Gould, 2003;Hasler et al., 2006). To our knowledge, no study has assessedanxiety traits in bipolar I extended pedigrees.
To determine whether quantitative anxiety symptom-atology is a candidate endophenotype for bipolar I disorder,we tested heritability of the state scale (measurement of thelevel of anxiety the individual is currently experiencing thatmay be expected to change over time) and trait scale(measurement of the general level of anxiety experiencedover the lifetime) from the Anxiety State and Trait Inventory(STAI) in a sample of extended pedigrees from the CentralValley of Costa Rica. We will demonstrate that patients andtheir relatives show higher scores on the measures, andestablish genetic correlation between the measure andaffection status.
2. Methods
2.1. Participants
Subjects were originally recruited for a multi-site bipolarsibling pair study (Genetics of Bipolar disorder in LatinoPopulations NIMH 1 R01 MH069856-01A2). The study wasexplained to each subject and written informed consent wasobtained. This study was reviewed and approved by theInstitutional Review Boards of the University of Costa Ricaand the University of Texas (UTHSCSA).
The sample was composed of 30 extended families (300subjects, average family size 10.34 members, range: 2–31)and 20 unrelated healthy controls. Each family had at leastone member diagnosed with bipolar disorder type I.
2.2. Diagnostic assessment
The subjects were diagnosed based on the diagnosticcriteria of DSM-IV through a best estimation process (Leckmanet al., 1982), utilizing clinical information obtained from theDiagnostic Interview for Genetic Studies (Nurnberger et al.,1994), a Family Interview for Genetic Studies (Maxwell, 1992)and psychiatric records. Final diagnoses were determinedthrough a consensus process where two independent psychia-trists reviewed all available information, arrived at indepen-dent diagnoses and, if there were differences, reached aconsensus diagnoses. The Lifetime Dimensions of PsychosisScale (LDPS) was used to capture affective and psychoticsymptomsover the lifetimeanda consensusprocess of twobestestimators per case was utilized as well.
2.3. Anxiety assessment
Subclinical anxiety was assessed by means of the STAI tomeasure anxiety scores in each individual. The STAI is a self-rated instrument that contains two 20-item scales (4 responsechoices per item, higher scores indicate higher anxiety)(Spielberger et al., 1983). One scale measures state anxiety(i.e. the extent to which respondents experience anxietysymptoms at the time ofmeasurement) (Vigneau and Cormier,2008). The second scale measures trait anxiety (i.e. the extentto which respondents generally experience anxiety symp-toms). This instrument has been validated in Spanish (Rodrigoand Lusiardo, 1988).
The instrument was applied within the same monthperiod after the psychiatric interview in 285 subjects, while35 individuals were assessed with the STAI at a different time(later than a month after psychiatric interview) due toavailability of the participants.
2.4. Statistical analysis
General linear model (GLM) techniques were used to testendophenotype criteria (e.g. heritability, sensitivity to theillness, genetic correlation). Heritability was assessed withvariance component methods by using the SOLAR packagesoftware. Genetic correlation was also computed for thescales of the STAI (state and trait) and quantifiable maniasymptoms score from the M-1 item (duration×severity) ofthe LDPS. Models were analyzed with cofactors age, sex, the

Table 1STAI score by group.
Variable BPI (n=30) RELs+ (n=40) RELs− (n=230) CON (n=20)
Trait mean (SD) 37.13 (12.07) 33.10 (10.80) 30.72 (9.46) 21.95 (7.04)State mean (SD) 23.23 (12.02) 23.49 (10.09) 20.87 (9.65) 21.45 (7.49)
Abbreviations: BPI = Bipolar disorder type I. RELs+ = Relatives with other psychiatric disorders. RELs− =Healthy relatives. CON = Unrelated healthy controls.
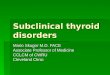
Fig. 1. Trait score by group.
269J. Contreras et al. / Journal of Affective Disorders 122 (2010) 267–272
square of age, and interactions between age and sex, to allowfor different age effects in males and females and non-linearchange with age. Bivariate analyses provide genetic andenvironmental correlations as a means of examining howthese traits vary together. Such analyses allowed us to askwhether scores on anxiety correlated with each other andwith mania in the bipolar I subjects because they areinfluenced by the same genes.
To test association of anxiety traits with the illness, weexamined multiple dependent, independent and covariatevariables (e.g. age, gender). We tested the anxiety scores ofbipolar I individuals and their relatives to determine whetherthey differed from scores in controls, suggesting an underly-ing genetic correlation between anxiety score and bipolar Idisorder. This hypothesis was tested through GLM methodsmodeling anxiety scores as function of genetic proximity toan affected individual (bipolar I disorderNrelatives with otherpsychiatric illness (different than bipolar I disorder)NhealthyrelativesNhealthy unrelated controls). All calculations wereadjusted for age and gender by using the Statistical Packagefor the Social Sciences (SPSS) Software v.15.
3. Results
3.1. Sample characteristics
Of the 300 subjects from extended pedigrees, 63 hadbipolar disorder type I, 79 major depressive disorder, 23specific phobia, 15 panic disorder, 7 schizoaffective disorder,7 psychosis not otherwise specified, 4 social phobia, 4 bipolardisorder type II, 3 obsessive compulsive disorder, 1 general-ized anxiety disorder and 101 had no axis I disorder. One-hundred and seventy-four (54%) were females and theaverage age of the whole sample was 39.3 (SD=16.2).
Only 46 individuals (14.37% of the total sample)met criteriafor a DSM-IV categorical anxiety diagnosis. In contrast, out ofthe 274 subjectswithno categorical anxiety diagnosis after bestestimation diagnostic process, 72 (26%) were over percentile75 (37 points) of the trait scale.
The average dimensional index of lifetime mania (M-1severity×duration of the LDPS)was 2.55. The average anxietystate score was 21.46 (SD=7.5) out of a maximum of 60 andthe average trait score was 31.07 (SD=8.1) out of amaximum of 60.
3.2. Heritability analysis
In the present study, the heritability for anxiety state was0.45 (SE=0.11, p=0.0000001) and for anxiety trait is 0.89(SE=0.06, p=6.22e−29). The interaction between age and
sexwas significant only for state (although the two individualcovariates were not statistically significant). The computedgenetic correlation for anxiety state and trait is 0.29,(SE=0.12, p: correlation is different from zero=0.038 andp: correlation is different from one=3.19e−8).
3.3. Sensitivity to liability for bipolar I disorder
As seen in Table 1 and Fig. 1, bipolar I patients showedsignificantly higher anxiety trait scores than their relativesand healthy controls (F=12.17 [5,24], p=0.002), (bipolar IpatientsNrelatives with other pathologies, Nhealthy relati-vesNunrelated healthy controls). State score did not show anysignificant difference between groups (F=1.18, p=0.32).
To confirm the overall difference between groups on traitanxiety scores we assessed the difference between eachgroup by conducting the post-hoc pairwise comparisons test.Since variances of trait mean were unequal (Levene'sstatistic=2.45, df=3, p=0.06), Dunnett C test was used.As seen in Table 2, mean differences between each groupremained statistically significant.
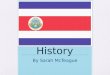
As shown in Fig. 2, we found a normal distribution for traitscores in the healthy subjects (healthy relatives and healthyunrelated controls) but not for the state scores.

Table 2Pairwise differences for trait anxiety between groups (post-hoc comparisonpairwise test).
(I) Group (J) Group Mean difference (95%CI) SE (p)
BPI RELs+ 6.53 (0.34, 12.72) 2331 (0.03)RELs− 7.90 (2.90, 12.90) 1884 (0.0001)CON 16.65 (9.21, 24.09) 2801 (0.0001)
RELs+ BPI −6.53 (−12.72, −0.34) 2331 (0.03)RELs− 1.37 (−3.00, 5.74) 1645 (1.0)CON 10.12 (3.10, 17.15) 2646 (0.001)
RELs− BPI −7.90 (−12.90, −2.90) 1884 (0.0001)RELs+ −1.37 (−5.74, 3.00) 1645 (1.0)CON 8.75 (2.75, 14.76) 2262 (0.001)
CON BPI −16.65 (−24.09, −9.21) 2801 (0.0001)RELs+ −10.12 (−17.15, −3.10) 2646 (0.001)RELs− −8.75 (−14.76, −2.75) 2262 (0.001)
Abbreviations: BPI = Bipolar disorder type I. RELs+ = Relatives with otherpsychiatric disorders. RELs− = Healthy relatives. CON = Unrelated healthycontrols. SE = Standard error.Dunnett C for unequal n's and variances was utilized as a post-hoc test tocompare specific groups.Significant mean differences are in bold.
Fig. 2. Trait score distribution in healthy subjects.
270 J. Contreras et al. / Journal of Affective Disorders 122 (2010) 267–272
The trait score was correlated with lifetime mania (LDPS M-1duration×severity) r=0.21(p≤0.0001) after controlling forage contrary to lifetime depression (LDPS DE-1 duration×se-verity) r=0.06 (p=0.26). The state score does not showcorrelation with mania.
Of the 285 subjects (90% of the whole sample) evaluated atthe same time (during a month period after psychiatricevaluation), 27 (9%) met criteria for a current depressivesyndrome (five or more depressive symptoms within the lasttwo weeks of psychiatric assessment) and 11 (3%) for a currentmanic syndrome (elated mood+three or more manic symp-toms or irritability+four or more manic symptoms within thelast week of psychiatric evaluation). The 27 subjects who weredepressed during the time of assessment and had a meananxiety trait score of 31.26 (SD=10.95) compared to 30.32(SD=9.62) in the non-depressed group. The eleven individuals
had mania during the time of assessment had an anxiety traitscore of 27.0 (SD=7.34) in contrast to 30.54 (SD=9.80) in thenon-manic group. We found no significant differences in thetrait scores regarding current mood status (currently depressedor currently manic), (F=0.230, df=1, p=0.632) and(F=1.401, df=1, p=0.238) respectively.
4. Discussion
Quantitative measures of anxiety represent a window intothe genetically influenced biological processes underlyingbipolar I disorder and can facilitate the identification of someof its susceptibility genes.
With the current categorical diagnostic system, anxietysymptoms are often under-diagnosed. In our sample, morethan one quarter of patients with high trait anxiety scores(above percentile 75) did not receive any anxiety diagnosisafter best estimation diagnostic process. The main reason isthat many individuals who endorse anxiety do not meet allcriteria for a full blown anxiety disorder. This finding stronglyencourages the use of anxiety quantitative measures inpsychiatric genetics research.
Regarding trait anxiety, individuals with bipolar I disordershowed the highest scores followed by relatives with otherpsychiatric disorders, healthy relatives and healthy unrelatedcontrols. These results are similar to previous publications.For instance, Vázquez et al. (2008) found that healthyrelatives of bipolar patients exhibited higher scores on theanxious temperament subscale of the TEMPS-A than controls.In a study by Evans et al. (2005) unaffected relatives ofbipolar patients and controls showed differences on thehyperthymic scale and on the first extracted factor, anxious/reactive of the TEMPS-A and TCI-125. All of the aboveevidence is consistent with temperament and personalityanxiety related traits having a genetic basis rather than beingsecondary to full-blown bipolar disorder.
A positive significant correlation was also found betweentrait scores and quantitative lifetime mania whereas nocorrelation was observed between anxiety trait scores andlifetime depression. This finding reflects what is frequently seenin clinical practice, when bipolar I patients' complain of anxietysymptoms even if they do not have a specific anxiety disorderaccording to the current diagnostic classification. Likewise,many healthy relatives of bipolar I patients endorse anxietysymptoms sometimes perceived as personality anxiety relatedtraits.
We found significant heritability for quantitative anxietymeasures in a set of multiplex, multigenerational familiesaffected by bipolar I disorder, suggesting that some of thevariations in the traits are affected by genetic factors. Eventhough both scales (state and trait) showed significantheritability, state was less heritable and it was affected bythe interaction between age and sex whereas trait score wasmore stable within the sample. Consequently, lifetimemeasurement seems to be more useful to capture quantita-tive anxiety symptoms in this population while currentquantitative anxiety is more affected by other variants. Wealso found genetic correlation significantly different fromzero between these scores suggesting that they are influencedby some of the same genes. Based on these results, weconclude that both measures (state and trait score) are

271J. Contreras et al. / Journal of Affective Disorders 122 (2010) 267–272
heritable and share some genetic factors (overlapping geneticinfluences) in this Costa Rican sample.
We found a stair-step distribution of trait anxiety scores inthe family members and controls based on their geneticproximity to affected individuals and diagnostic status. Thisencourages our research focus of studying trait anxiety as anendophenotype in this population of families with bipolar Idisorder.
From the two STAI scales, only anxiety trait showednormal distribution in healthy subjects (healthy relatives andhealthy unrelated matched controls), current mood statusindependence and significant liability for bipolar I disordernot only per groups but also as a continuum quantitativevariable (lifetime mania). All of this evidence allows us topostulate anxiety trait as an intermediate phenotype forbipolar I disorder in this Costa Rican sample.
It is worth noting that in liability threshold model analyses,significant results are difficult to obtain when working withdichotomous traits. In our study we used continuous traits(state scale, trait scale and quantitative lifetime mania) thatallowed us to reach significant results. Another strength of thiswork is provided by the study design; besides bipolar I patientswe assessed individuals without overt symptom expression(healthy relatives) but with high genetic risk for bipolar Idisorder and healthy unrelated controls. The diagnosis of eachsubjectwasobtained thru the best-estimateprocedurewhich isconsidered the current standard in many psychiatric geneticresearch studies (Contreras et al., 2009). All participants werefromanenvironmentally and genetically homogeneous samplereducing etiological heterogeneity and confusing interactionsof genes and environment.
Some methodological differences between our work andtwo recent publications that we cited above can be found. Inthe Argentinean study, Vázquez et al. (2008) used the MoodDisorder Questionnaire to rule out bipolarity and a best-estimate procedure was not mentioned as being done. In astudy with a larger sample of 85 BP families and 63 controlsconducted by Evans et al. (2005), bipolar I and bipolar IIsubjects from San Diego, Vancouver, and Cincinnati wereplaced in the same group. Their controls were recruitedthrough advertisements (for participation in sleep studiesand other studies at the UCSD Mental Health Clinical), whichmay have introduced an ascertainment bias. They did notassess mood state at the time of completing the questionnairewhich could affect subjects' rating.
Some limitations of our work need to be taken intoconsideration. Confounding factors such as substance abuse,medical illness and medication history could affect theinteraction of measured anxiety with mania. Due to ourlimited budget we were not able to re-evaluate the subjectsand conduct a test retest to assess the instrument reliabilityand mood state independence of anxiety traits over differenttimes. Such a test is necessary to ensure that this scale can beused as a measurable trait and to better understand, if it doesvary with time, the relationship of the anxiety trait to othercore symptoms of bipolar I disorder (i.e. depression, mania,psychosis). Additional assessment needs to be done toidentify how many patients with high anxiety score havebeen treated and to evaluate current functioning and effect ofmedication on clinical course. Our findings raise severalquestions that with our available data we were not able to
answer. It is crucial to know if anxiety traits are speciallyrelated to bipolar I disorder in comparison with other traitssuch as anger (frequently associated with bipolar II andbipolar family history), attention or response inhibitiondeficit, pathological impulsivity or other character dimen-sions such as low self-directedness (ability to adapt one'sbehaviors to achieve chosen goals). All of these issues will beaddressed in our future research project in addition toidentification of regions containing genes specific for thesequantitative measures by means of Quantitative Trait Locilinkage and association analyses. This will improve ourunderstanding of the pathophysiology of affective andanxiety disorders in the Costa Rican population.
The relevance of our work can be summarized as follows:(1) Quantitative anxiety measures as an endophenotype mayfacilitate the identification of genes which predisposeindividuals to develop bipolar I disorder. (2) Confirmationof this result will aid researchers to understand the essentialpathophysiology underlying bipolar spectrum disorders.(3) If this trait is proven to be an endophenotype, it will beof help in diagnosing and treating bipolar I patients in a morereliable and biologically valid manner than our currentclassification allows. This will also have direct epidemiolog-ical implication on public health policies. (4) As for otherbipolar endophenotypes, anxiety traits can be modeled inanimal research. Several genetic, pharmacological, andbehavioral animal models have long been used to establishanimal anxiety-like phenotypes, as well as to assess theirmemory, learning, and other cognitive functions (Ennaceur etal., 2006; Kalueff and Murphy, 2007; Waikar and Craske,1997; Wang et al., 2007; Yokoyama et al., 2009). Specifically,chronic icv oxytocin has been used to attenuate the high levelof trait anxiety in rats (Slattery and Neumann, 2009). Someinnate fear responses may also underlie the type of elevatedanxiety levels found in the subjects with bipolar I disorderdescribed in this paper. High anxiety levels as we found inCosta Rican bipolar I patients.
Role of funding sourceFinancial support for this study was provided by Fogarty (TW006152)
training grant and NIMH 1 R01 MH069856-01A2 grant. SOLAR is supportedby NIMH grant MH59490 (J. Blangero).
Conflict of interestNone of the authors has financial disclosers.
Acknowledgments
Financial support for this study was provided by Fogarty(TW006152) training grant and NIMH 1 R01 MH069856-01A2 grant. SOLAR is supported by MH59490 (J. Blangero).The authorswish to thank Evelyn Duran, MD,Marcela Barguil,MA and Lara Mora, MA for assistance in data collection, LuisSantos BA and Joseph Peters BA for coordination and datamanagement, and Mercedes Ramirez, MD, Salvador Con-treras, MD, Juan Zavala MD, and Lorena Jimenez, MD forassistance in best estimation. None of the authors hasfinancial disclosers and portions of these data were presentedat the World Congress of Biological Psychiatry (Paris, 2009)where Dr. Javier Contreras received the Young InvestigatorBest Poster Award. We are also grateful to the families whohave made this research possible.

272 J. Contreras et al. / Journal of Affective Disorders 122 (2010) 267–272
References
Bearden, C.E., Freimer, N.B., 2006. Endophenotypes for psychiatric disorders:ready for primetime? Trends Genet. 22 (6), 306–313.
Bearden, C.E., Reus, V.I., Freimer, N.B., 2004. Why genetic investigation ofpsychiatric disorders is so difficult? Curr. Opin. Genet. Dev. 14 (3), 280–286.
Berns, G.S., Nemeroff, C.B., 2003. The neurology of bipolar disorder. Am. J.Med. Genet. C. (Semin. Med. Genet.) 123C, 76–84.
Chen, Y.W., Dilsaver, S.C., 1995. Comorbidity of panic disorder in bipolarillness: evidence from the Epidemiologic Catchment Area Survey. Am. J.Psychiatry. 152 (2), 280–282.
Contreras, J., Dassori, A., Medina, R., Raventós, H., Ontiveros, A., Nicolini, H.,Munoz, R., Escamilla, M., 2009. Diagnosis of schizophrenia in Latinopopulations: a comparison of direct interview and consensus basedmulti-source methods. J. Nerv. Ment. Dis. 197 (7), 530–535.
Ennaceur, A., Michalikova, S., Chazot, P.L., 2006. Models of anxiety: responsesof rats to novelty in an open space and an enclosed space. Behav. Brain.Res. 171 (1), 26–49.
Evans, L., Akiskal, H.S., Keck Jr., P.E., McElroy, S.L., Sadovnick, A.D., Remick, R.A.,Kelsoe, J.R., 2005. Familiality of temperament in bipolar disorder: supportfor a genetic spectrum. J. Affect. Disord. 85 (1–2), 153–168.
Feske, U., Frank, E., Mallinger, A.G., Houck, P.R., Fagiolini, A., Grochocinski, V.J.,Kupfer, D.J., 2000. Anxiety as a correlate of response to the acutetreatment of bipolar I disorder. Am. J. Psychiatry. 157, 956–962.
Gottesman, I.I., Gould, T.D., 2003. The endophenotype concept in psychiatry:etymology and strategic intentions. Am. J. Psychiatry. 160, 636–645.
Gottesman, I.I., Shields, J., 1973. Genetic theorizing and schizophrenia. Br. J.Psychiatry. 122, 15–30.
Hasler, G., Drevets, W., Gould, T., Gottesman, I., Manji, H., 2006. Towardconstructing an endophenotype strategy for bipolar disorders. Biol.Psychiatry. 60 (2), 93–105.
Kalueff, A.V., Murphy, D.L., 2007. The importance of cognitive phenotypes inexperimental modeling of animal anxiety and depression. Neural, Plast.
Keck Jr, P.E., McElroy, S.L., Strakowski, S.M., West, S.A., Sax, K.W., Hawkins, J.M.,Bourne,M.L., Haggard, P., 1998. 12-month outcomeof patientswith bipolardisorder following hospitalization for a manic or mixed episode. Am. J.Psychiatry. 155, 646–652.
Leckman, J., Sholomskas, D., Thompson,W., Belanger, A., Weissman, M., 1982.Best estimate of lifetime psychiatric diagnosis: a methodological study.Arch. Gen. Psychiatry. 39, 879–883.
MacKinnon, D.F., Zandi, P.P., Cooper, J., Potash, J.B., Simpson, S.G., Gershon, E.,Nurnberger, J., Reich, T., DePaulo, J.R., 2002. Comorbid bipolar disorderand panic disorder in families with a high prevalence of bipolar disorder.Am. J. Psychiatry. 159, 30–35.
Mantere, O., Suominen, K., Valtonen, H.M., Arvilommi, P., Isometsä, E., 2008.Only half of bipolar I and II patients report prodromal symptoms.J. Affect. Disord. 111 (2–3), 366–371.
Maxwell, M., 1992. Manual for the FIGS. Intramural Research Program,National Institute of Mental Health, Wasington, DC.
McElroy, S.L., Altshuler, L.L., Suppes, T., Keck Jr., P.E., Frye, M.A., Denicoff, K.D.,Nolen,W.A., Kupka, R.W., Leverich, G.S., Rochussen, J.R., Rush,A.J., Post, R.M.,2001. Axis I psychiatric comorbidity and its relationship to historical illnessvariables in 288 patients with bipolar disorder. Am. J. Psychiatry. 158,420–426.
Nurnberger Jr., J.I., Blehar, M.C., Kaufmann, C.A., York-Cooler, C., Simpson, S.G.,Harkavy-Friedman, J., Severe, J.B., Malaspina, D., Reich, T., 1994. Diagnosticinterview for genetic studies. Rationale, unique features, and training.NIMH Genetics Initiative. Arch. Gen. Psychiatry. 51, 849–859.
Rodrigo, G., Lusiardo, M., 1988. Note on the reliability and concurrent validityof the Spanish version of the State–Trait Anxiety Inventory. Percept. Mot.Skills. 67 (3), 926.
Rotondo, A., Mazzanti, C., Dell'Osso, L., Rucci, P., Sullivan, P., Bouanani, S.,Gonnelli, C., Goldman,D., Cassano,G.B., 2002.Catechol o-methyltransferase,serotonin transporter, and tryptophanhydroxylase genepolymorphisms inbipolar disorder patients with and without comorbid panic disorder. Am. J.Psychiatry. 159 (1), 23–29.
Schinka, J.A., Busch, R.M., Robichaux-Keene, N., 2004. A meta-analysis ofthe association between the serotonin transporter gene polymorphism(5-HTTLPR) and trait anxiety. Mol. Psychiatry. 9, 197–202.
Sen, S., Burmeister, M., Ghosh, D., 2004. Meta-analysis of the associationbetween a serotonin transporter promoter polymorphism (5-HTTLPR)and anxiety-related personality traits. Am. J. Med. Genet. 127B, 85–89.
Slattery, D.A., Neumann, I.D., 2009. Chronic icv oxytocin attenuates thepathological high anxiety state in female high anxiety-related behaviourrats. Neuropharmacology.
Spielberger, C.D., Gorsuch, R.L., Lushene, R., Vagg, P.R., Jacobs, G.A., 1983.Manual for the State–Trait Anxiety Inventory (Form Y). ConsultingPsychologists Press, Palo Alto, CA.
Unschuld, P.G., Ising, M., Erhardt, A., Lucae, S., Kloiber, S., Kohli, M., Salyakina, D.,Welt, T., Kern,N., Lieb, R., Uhr,M., Binder, E.B.,Müller-Myhsok, B.,Holsboer, F.,Keck, M.E., 2007. Polymorphisms in the serotonin receptor gene HTR2A areassociated with quantitative traits in panic disorder. Am. J. Med. Genet. B.Neuropsychiatr. Genet. 144 (4), 424–429.
Vázquez, G.H., Kahn, C., Schiavo, C.E., Goldchluk, A., Herbst, L., Piccione, M.,Saidman,N., Ruggeri, H., Silva,A., Leal, J., Bonetto, G.G., Zaratiegui, R., Padilla,E., Vilapriño, J.J., Calvó,M., Guerrero, G., Strejilevich, S.A., Cetkovich-Bakmas,M.G., Akiskal, K.K., Akiskal, H.S., 2008. Bipolar disorders and affectivetemperaments: a national family study testing the “endophenotype” and“subaffective” theses using the TEMPS-A Buenos Aires. J. Affect. Disord. 108(1–2), 25–32.
Vigneau, F., Cormier, S., 2008. The factor structure of the State–Trait AnxietyInventory: an alternative view. J. Pers. Assess. 90 (3), 280–285.
Waikar, S.V., Craske, M.G., 1997. Cognitive correlates of anxious and depressivesymptomatology: an examination of the Helplessness/Hopelessnessmodel. J. Anxiety. Disord. 11 (1), 1–16.
Wang, D., Noda, Y., Tsunekawa, H., Zhou, Y., Miyazaki, M., Senzaki, K.,Nabeshima, T., 2007. Behavioural and neurochemical features of olfactorybulbectomized rats resembling depression with comorbid anxiety. Behav.Brain. Res. 178 (2), 262–273.
Wozniak, J., Biederman, J., Monuteaux, M.C., Richards, J., Faraone, S.V., 2002.Parsing the comorbidity between bipolar disorder and anxiety disorders: afamilial risk analysis. J. Child. Adolesc. Psychopharmacol. 12 (2), 101–111.
Yokoyama, F., Yamauchi, M., Oyama, M., Okuma, K., Onozawa, K., Nagayama, T.,Shinei, R., Ishikawa, M., Sato, Y., Kakui, N., 2009. Anxiolytic-like profiles ofhistamineH3 receptor agonists in animalmodels of anxiety: a comparativestudy with antidepressants and benzodiazepine anxiolytic. Psychophar-macology. (Berl). 205 (2), 177–187.