Embed Size (px)
Citation preview

European Journal of Endocrinology (2011) 164 169–178 ISSN 0804-4643
CLINICAL STUDY
Is it possible to avoid hypopituitarism after irradiation ofpituitary adenomas by the Leksell gamma knife?Josef Marek, Jana Jezkova, Vaclav Hana, Michal Krsek, L’ubomıra Bandurova, Ladislav Pecen1, Vilibald Vladyka2
and Roman Liscak2
Third Department of Medicine, First Medical Faculty, Charles University, U nemocnice 1, 128 02 Praha 2, Czech Republic, 1Institute of Informatics of theCzech Academy of Science, Pod Vodarenskou vezı 2, 182 07 Praha 8, Czech Republic and 2Department of Stereotactic and Radiation Neurosurgery, HospitalNa Homolce, Roentgenova 2, 150 30 Praha 5, Czech Republic
(Correspondence should be addressed to J Jezkova; Email: [email protected])
q 2011 European Society of E
Abstract
Objective: Radiation therapy is one of the treatment options for pituitary adenomas. The most commonside effect associated with Leksell gamma knife (LGK) irradiation is the development ofhypopituitarism. The aim of this study was to verify that hypopituitarism does not develop if themaximum mean dose to pituitary is kept under 15 Gy and to evaluate the influence of maximum distalinfundibulum dose on the development of hypopituitarism.Design and methods: We followed the incidence of hypopituitarism in 85 patients irradiated with LGKin 1993–2003. The patients were divided in two subgroups: the first subgroup followed prospectively(45 patients), irradiated with a mean dose to pituitary !15 Gy; the second subgroup followedretrospectively 1993–2001 and prospectively 2001–2009 (40 patients), irradiated with a mean doseto pituitary O15 Gy. Serum TSH, free thyroxine, testosterone or 17b-oestradiol, IGF1, prolactin andcortisol levels were evaluated before and every 6 months after LGK irradiation.Results: Hypopituitarism after LGK irradiation developed only in 1 out of 45 (2.2%) patients irradiatedwith a mean dose to pituitary !15 Gy, in contrast to 72.5% patients irradiated with a mean dose topituitary O15 Gy. The radiation dose to the distal infundibulum was found as an independent factor ofhypopituitarism with calculated maximum safe dose of 17 Gy.Conclusion: Keeping the mean radiation dose to pituitary under 15 Gy and the dose to the distalinfundibulum under 17 Gy prevents the development of hypopituitarism following LGK irradiation.
European Journal of Endocrinology 164 169–178
Introduction
Treatment of pituitary adenomas is a complex issue,involving neurosurgical, pharmacological and radiationtreatment modalities. The success rates of neurosurgicaltreatment vary from 10 to 90% depending on the typeof adenoma (1–6). Medical treatment often has to becontinued lifelong and does not always control thegrowth and hormonal secretions of adenomas. Radi-ation therapy is typically used when both previousmethods have failed.
Conventional fractionated radiotherapy has achievedgood results but only after a long latency and withconsiderable post-radiation morbidity. The main adverseeffect is hypopituitarism, which is reported in 50–80%of patients followed up 10 years after conventionalirradiation (7–9). Other less frequent side effects ofconventional radiotherapy are optic neuropathy, radio-necrosis, radiation-induced cerebral tumours andvascular injury (10–14).
Radiosurgery primarily involves stereotactic irradi-ation with the Leksell gamma knife (LGK), or,
ndocrinology
alternatively, with a stereotactic linear accelerator.The hormonal normalization after LGK treatmenttakes several years but is considered to be faster thanwith conventional radiotherapy. Stereotactic radiosur-gery with the LGK is supposed to decrease the incidenceof side effects because of its highly consistent dosedelivery, which is associated with less irradiation outsidethe targeted volume. Optic neuropathy is reported in 1%of patients who were irradiated by the LGK (15, 16),and the risk of damage to cranial nerves in thecavernous sinus is !1%. Moreover, these cranialneuropathies are often temporary (16). Radionecrosisin the hypothalamic and temporal regions related toLGK irradiation was described in !1% of patients aswell. However, the majority of these patients underwentconventional fractionated radiation prior to LGKirradiation (16). As far as vascular injury is concerned,symptomatic carotid artery stenosis was reported inonly two cases (17). Up until now, radiation-inducedneoplasm has not been reported.
However, LGK irradiation was reported not toeliminate the incidence of hypopituitarism. Published
DOI: 10.1530/EJE-10-0733
Online version via www.eje-online.org

170 J Marek and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
data vary widely, ranging from 0 to 40% (18–20).Similarly, among our first patients treated with the LGK,38.2% of them developed hypopituitarism (21). Conse-quently, in our previously published study, we analysedfactors leading to this unfavourable outcome andevaluated the radiation tolerance of functioning sellarstructures after LGK irradiation (22). This retrospectivestudy demonstrated that the mean dose to the pituitarygland surrounding the adenoma is the most importantfactor causing the development of hypopituitarism.The radiation dose of 15 Gy was determined as themaximum safe limit of the mean radiation dose to thepituitary gland. Another factor, which influencedthe development of hypopituitarism, was the maximaldose to the distal infundibulum. However, the fullcharacterization of this relationship was not defined.Pretreatment factors such as the previous neurosurgery,previous partial pituitary deficiency and the tumourvolume were demonstrated to play less important rolein the development of hypopituitarism.
On the basis of our previous report, the aim of thisstudy was to verify that hypopituitarism does notdevelop if the maximum mean dose to the healthypituitary is kept under 15 Gy and to evaluate if themaximum dose to distal infundibulum influences thedevelopment of hypopituitarism in a prospectivelyprolonged study.
Subjects and methods
We followed a group of 85 patients (54 females and31 males, aged 16–74 years, mean age 45.14G16.13years) with pituitary adenomas, treated with the LGK atthe Department of Stereotactic and Radiation Neuro-surgery at the Na Homolce Hospital in Prague, CzechRepublic. The follow-up period was 60–192 months(meanGS.D., 100.9G39.9 months; median 84months).
LGK irradiation was indicated as I) secondary therapyafter incomplete surgery; II) primary therapy i) inpatients contraindicated for surgery or ii) in patientsrefusing surgery. The group of 85 patients was dividedin two subgroups according to the mean dose ofradiation to the pituitary tissue surrounding theadenoma. The first subgroup (group I) consisted of 45patients who were irradiated with a mean dose to thepituitary of !15 Gy. The second subgroup (group II)consisted of 40 patients who were irradiated with amean dose to the pituitary of more than 15 Gy. Thepatients underwent LGK irradiation between 1993 and2003. For the retrospective part of the study, all patientswere included, in whom the radiation doses to thepituitary and pituitary stalk were measured (all patientsfrom group II and six patients from group I), and for theprospective part of the study, all new patients withpituitary adenomas irradiated between September 2001and September 2003 (39 patients from group I).
www.eje-online.org
In group I, there were 28 females and 17 males aged16–72 years (mean 48.6G15.9 years); 21 patients withacromegaly, 10 patients with prolactinomas, 5 patientswith Cushing’s disease and 9 patients with functionlessadenomas. Twenty-two (48.9%) patients underwentneurosurgical operations prior to LGK irradiation.None of the patients underwent the fractionatedradiotherapy prior to LGK irradiation. The follow-upperiod in group I ranged from 60 to 192 months(meanGS.D., 77.8G23.7 months; median 73 months).
In group II, there were 26 females and 14 males aged17–74 years (mean 41.2G15.6 years); 23 patientswith acromegaly, 8 patients with prolactinomas, 6patients with Cushing’s disease, 1 patient with Nelson’ssyndrome and 2 patients with functionless adenomas.Twenty-five (62.5%) patients underwent neurosurgicaloperations prior to LGK irradiation. None of the patientsunderwent the fractionated radiotherapy prior to LGKirradiation. The follow-up period in group II rangedfrom 60 to 192 months (meanGS.D., 126.9G38.6months; median 135 months).
None of the patients in both groups had surgery orradiation therapy after LGK radiation.
Radiosurgery was performed using an LGK model B(Elekta Instrument AB, Stockholm, Sweden). Stereo-tactic imaging was performed by magnetic resonanceimaging (MRI; Magnetom Expert 1T, Siemens, Erlangen,Germany), using classical native turbo spin-echo (TSE)sequences in T2-weighted (4100/99) and T1-weighted(500/15) axial and coronary cuts of 3 mm thickness,before and after contrast. In some patients, images wereobtained by dynamic TSE T1-weighted (395/12)sequence. The accuracy of our MRI targeting wasevaluated in a separate study (23). Irradiation wasdesigned using GammaPlan 5.11 (Elekta InstrumentAB). However, in the first year of LGK therapy (1993), adifferent planning system was used (Kula, ElektaInstrument AB). Pituitary radiosurgery planning is acomplex procedure because a highly conformal doseplan is needed to spare any remaining normal pituitarygland as well as the optic pathway. The examples ofpituitary radiosurgery planning are showed in Figs 1and 2. Of the 85 patients, 6 were treated according to theplanning system Kula, by which it was impossible tocalculate the accurate dose to all specific structures.In the case of these six patients, the radiosurgeryplanning was later reconstructed into the systemGammaPlan, which enabled accurate calculation. Datapertaining to the radiosurgical target volume andradiation doses to the pituitary adenoma, healthypituitary and distal infundibulum are summarized inTable 1. Between both groups of patients, there was nosignificant difference in the radiosurgical target volume(non-significant P levels in Wilcoxon and ANOVA tests(majority of distribution of results also shows moderateviolation of normality assumptions; therefore, boththese tests were used)). There were found significantdifferences in radiation doses to the pituitary adenoma

S
R 8 Gy
8 Gy
35 Gy
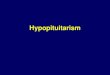
Figure 1 Fifty years old women with Cushing’s disease. The targettumour volume was 1600 mm3. The tumour received a margin doseof 35 Gy at the 50% isodose line. The maximum dose to the opticpathway was 7.6 Gy. The volume of hypophysis (*) was 205.3 mm3,the minimum dose to hypophysis was 3 Gy, the maximum dosewas 29.1 Gy, the mean dose was 7.8G4.2 Gy and the integral dosewas 1.6 mJ. S
R8 Gy
15 Gy
8 Gy
Figure 2 Seventy-two years old men with the functionless pituitaryadenoma, who underwent one previous neurosurgery operationbefore LGK irradiation. The target tumour volume was 2800 mm3.The tumour received a margin dose of 15 Gy at the 50% isodoseline. The maximum dose to the optic pathway was 8.0 Gy. Thevolume of hypophysis (*) was 124.8 mm3, the minimum dose to thehypophysis was 6.4 Gy, the maximum dose was 19.0 Gy, the meandose was 12.3G1.9 Gy and the integral dose was 1.5 mJ.
Hypopituitarism after LGK irradiation 171EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
(both functionless and secretory adenomas). Bothmaximal (Wilcoxon P!0.004 and ANOVA P!0.013)and margin (Wilcoxon P!0.022 and ANOVAP!0.012) doses were higher in the group II incomparison with the group I. When comparing thepatients only with hormone-secreting adenomas, therewere found no significant differences in the radiosurgicaltarget volume (group I 1636 mm3 versus group II1655 mm3) and margin dose (group I 33.4 Gy versusgroup II 35.5 Gy) between both groups of patients. Thedifference was only in maximal dose (group I 64.5 Gyversus group II 67.8 Gy; Wilcoxon P!0.036 andANOVA P!0.19 (NS)). The dose to the optic pathwaywas kept !8 Gy, and the dose to the brain stem was kept!14 Gy.
The regular hormonal follow-up was carried out at asingle centre (Third Department of Medicine, First Schoolof Medicine, Charles University, Prague, Czech Republic).The tests were carried out every 6 months in order toestablish the normalization of hormonal overproductionand the possible pituitary deficits after irradiation.
To evaluate the success of treatment of the differentpituitary adenomas, the following criteria of hormonalnormalization were followed: i) in acromegaly patients,normal IGF1 according to sex and age; ii) inprolactinoma patients, prolactin (PRL) !619 mIU/l innon-pregnant women, PRL !430 mIU/l in postmeno-pausal women and PRL !375 mIU/l in men; iii) in
patients with Cushing’s disease, an 0800 h plasmacortisol and 24-h free urinary cortisol in the normalrange, and either suppressibility of plasma cortisol afteran overnight dexamethasone (1 mg) suppression testwith 0800 h cortisol level below 84 nmol/l or the res-titution of circadian variability of plasma cortisol levels.
The activity of the pituitary–thyroid axis wasdetermined by measuring peripheral levels of freethyroxine (fT4). In order to exclude a diagnosis ofincident primary hypothyroidism, TSH level wasmeasured. Activity of the pituitary–adrenocortical axiswas monitored by measuring the levels of morningplasma cortisol (between 0800 and 0900 h). Cortisollevels O450 nmol/l at this time excluded adrenalinsufficiency, while a level !150 nmol/l was diagnosticof hypocortisolism. In all patients with morning plasmacortisol levels between 150 and 450 nmol/l, themeasurements of cortisol levels in response to insulin-induced hypoglycaemia (0.1–0.2 IU/kg insulin humanrapid as i.v. bolus; samples drawn at 0, 30, 60 and90 min) were performed. If cortisol level rose to500 nmol/l, hypocortisolism was excluded. The activityof the pituitary–gonadal axis was measured in men bydetermining plasma testosterone levels and in womenby measuring serum levels of 17b-oestradiol, andassessed by the presence of regular menstrual bleeding.
www.eje-online.org

Table 1 Radiosurgical target volume and radiation doses.
Range Average Median
Group I: the mean dose to the pituitary !15 GyTarget tumour volume (cm3) 0.034–11.2 1.819 0.961Radiation doses (Gy)
Adenoma – maximum dose 30–80 60 65Adenoma – margin dose 15–42 31 35Mean dose to the pituitary 4–14.9 11.4 12.5Dose to the distal infundibulum 1.9–21.7 9.4 9.0
Group II: the mean dose to the pituitary O15 GyTarget tumour volume (cm3) 0.24–6.7 1.782 1.065Radiation doses (Gy)
Adenoma – maximum dose 40–80 67 70Adenoma – margin dose 20–49 35 35Mean dose to the pituitary 15.4–63 33.1 30.8Dose to the distal infundibulum 10.2–67.0 28.6 28.0
172 J Marek and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
The gonadotrophic deficiency was not evaluated in 28women older than 45 years, because of the impossibilityto decide whether the deficiency is caused by irradiationor whether it is the consequence of the naturalmenopause, and in 21 men over 50 years, because inthem the testosterone levels can irregularly decrease asthe consequence of andropause. As IGF1 level is not areliable criterion for diagnosis of GH deficiency (24) andthe determination of GH levels following provocativetesting was not carried out, the activity of somatotropicaxis was not evaluated. The development of diabetesinsipidus was not observed after LGK irradiation.
All hormonal levels were measured by commercialkits: GH and IGF1 by IRMA kits (Immunotech,Marseille, France); PRL by chemiluminescence analysis(ADVIA Centaur Bayer); plasma cortisol and urinaryfree cortisol by RIA kit (Immunotech); testosterone andoestradiol by chemiluminescence analysis (ArchitectAbbott); TSH and fT4 by chemiluminescence analysis(Centaur Bayer).
Table 2 Development of hypopituitarism in individual axes.
Axis
Number ofaxes with
replacementtherapy
Number ofaxes withoutreplacement
therapy
Number (%) ofpatients devel-oping a new
deficiency afterirradiation
Mean dose to the pituitary !15 GyThyroid 9 36 0 (0%)Adrenal 1 44 0 (0%)Gonadala 32 13 1 (7.7%)
Mean dose to the pituitary O15 GyThyroid 4 36 21 (58.3%)Adrenal 8 32 13 (40.6%)Gonadala 25 15 8 (53.3%)
aGonadal axis was evaluated in women only up to 45 years and in men onlyup to 50 years of age.
Statistical analysis
Descriptive statistics for numerical data (meanGS.D.,median) and categorical data (absolute and relativefrequencies) are presented. Inferential statisticalanalysis was done by means of the Cox proportionalhazard regression model and logistic regression model;comparison of groups was done by means of ANOVAand Wilcoxon Rank Sum tests. Some of the variableswere logarithmically transformed to normalize distri-bution of results for the purpose of statistical testing. Foran estimation of time to an event (development ofhypopituitarism in total and in individual axes), theproduct limit method (also called the Kaplan–Meiermethod) was used; this is one variant of a non-parametric estimation. Mutual relationship betweennumerical parameters was investigated via correlationanalysis done by means of Spearman rank correlationcoefficient.
www.eje-online.org
Results
Hypopituitarism after LGK irradiation did not develop in97.8% (95% confidence interval (CI) (93.5; 100.0)) ofpatients in group I: the patients irradiated with a meandose to the pituitary of !15 Gy. In contrast, hypopitui-tarism after LGK irradiation did not develop in only27.5% (95% CI (13.6; 41.3)) of patients in group II: thepatients irradiated with a mean dose to the pituitaryof O15 Gy.
In group I, the pituitary–thyroid axis was evaluatedin 36 patients and the pituitary–adrenocortical axis in44 patients who received no corresponding replacementtherapies before irradiation. Neither thyroid noradrenocortical deficiency developed after LGK irradi-ation. The pituitary–gonadal axis was evaluated in only13 patients, who were not replaced by sex hormonesand fulfilled age criterion (women up to 45 years andmen up to 50 years of age). Gonadal deficiency wasdeveloped by one patient (7.7%) 12 months afterirradiation (Table 2). This patient had undergone twoprevious pituitary surgeries and had already hadcentral hypothyroidism before he was irradiated.

Table 3 Development of hypopituitarism related to previous pituitary deficiency before LGK irradiation.
Number (%)of patients
Number (%) of patientsdeveloping a new defici-ency after irradiation
Number (%) of patientswithout a new deficiency
after irradiation
Mean dose to the pituitary !15 GyPatients receiving replacementtherapy before LGK treatment
11 (24.4%) 1 (9.1%) 10 (90.9%)
Patients without replacementtherapy before LGK treatment
34 (75.6%) 0 (0%) 34 (100%)
Mean dose to the pituitary O15 GyPatients receiving replacementtherapy before LGK treatment
15 (37.5%) 14 (93.3%) 1 (6.7%)
Patients without replacementtherapy before LGK treatment
25 (62.5%) 15 (60%) 10 (40%)
There were no statistically significant differences between both groups in the number of patients with and without replacementtherapy before LGK treatment.
Hypopituitarism after LGK irradiation 173EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
In group II, 29 patients (72.5%) developed hypo-pituitarism in at least one axis 10–126 months (meanGS.D., 41.9G30.6 months; median 33 months) afterirradiation. The pituitary–thyroid axis was evaluatedin 36 patients, who were not replaced with T4 afterirradiation. Twenty-one patients (58.3%) experiencedsubnormal serum fT4 levels following LGK irradiation.The pituitary–adrenal axis was studied in 32 patients,who were not replaced by hydrocortisone after irradi-ation. Thirteen of them (40.6%) developed cortisoldeficiency after irradiation. The pituitary–gonadal axiswas evaluated in 15 patients, who were not replaced bysex hormones and fulfilled age criterion. Eight of thesepatients (53.3%) developed sex hormone deficiency(Table 2). In summary, new pituitary deficiencydeveloped at least one pituitary axis in 93.3% ofpatients already receiving replacement therapy toanother axis before LGK irradiation and in 60% ofpatients without replacement therapy before LGKirradiation (Table 3). The development of hypopituitar-ism was observed in 88.0% of patients with previousneurosurgery before LGK irradiation and in 46.7% of
Table 4 Development of hypopituitarism related to previous n
Number (%)of patients
Mean dose to the pituitary !15 GyPatients with previous neurosurgerybefore LGK treatment
22 (48.9%)
Patients without previous neurosurgerybefore LGK treatment
23 (51.1%)
Mean dose to the pituitary O15 GyPatients with previous neurosurgerybefore LGK treatment
25 (62.5%)
Patients without previous neurosurgerybefore LGK treatment
15 (37.5%)
There were no statistically significant differences between both groupsbefore LGK treatment.
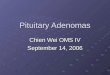
patients without previous neurosurgery before LGKirradiation (Table 4). The mean dose to the pituitary(dose !15 vs O15 Gy) was statistically significant forthe development of hypopituitarism in a group of 47patients with previous neurosurgery (P!0.0001) andin a group of 38 patients without previous neuro-surgery (P!0.0003). Similarly, the mean dose to thepituitary (dose !15 vs O15 Gy) was statisticallysignificant for the development of hypopituitarism in agroup of 26 patients receiving replacement therapybefore LGK irradiation (P!0.0001) and in a group of59 patients without replacement therapy (P!0.0001).Percentage of patients without the development ofhypopituitarism according to the Kaplan–Meier curve ingroup II (the patients irradiated with a mean dose tothe pituitary of more than 15 Gy) is shown in Fig. 3.The hypopituitarism developed only in one out of allpatients irradiated with a mean dose to the pituitaryof !15 Gy during the follow-up of 5 years and in 5, 40and 55% of patients irradiated with a mean dose to thepituitary of more than 15 Gy within 1, 3 and 5 yearsafter LGK irradiation.
eurosurgical treatment before LGK irradiation.
Number (%) of patientsdeveloping a new defici-ency after irradiation
Number (%) of patientswithout a new deficiency
after irradiation
1 (4.5%) 21 (95.5%)
0 (0%) 23 (100%)
22 (88.0%) 3 (12.0%)
7 (46.7%) 8 (53.3%)
in the number of patients with and without previous neurosurgery
www.eje-online.org

0 1 2 3 4 5 6 7
Time in years
8 9 10 11 12
100
90.0
80.0
70.0
60.0
50.0
Per
cent
age
of p
atie
nts
with
out h
ypop
ituita
rism
40.0
30.0
20.0
10.0
0.0
Figure 3 Percentage of patients without the development ofhypopituitarism (Kaplan–Meier estimate) in group II: the patientsirradiated with a mean dose to the pituitary of more than 15 Gy.
Table 5 Prognostic factors for the development of hypopituitarism.
Prognostic factors
Multivariate Coxregression model(stepwise selection)
P value
Univariate Coxregression
model P value
Tumour volume NS NSAdenoma – maximum dose NS NSAdenoma – margin dose NS NSMean dose to the pituitary 0.0411 !0.0001Dose to the distal
infundibulum0.0268 !0.0001
Previous neurosurgerybefore LGK treatment
NS NS
Replacement therapybefore LGK treatment
NS NS
NS, non-significant.
174 J Marek and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
Between group I and group II, the significantdifferences were demonstrated in the mean doseto the pituitary (Wilcoxon P!0.0001 and ANOVAP!0.0001) and the dose to the distal infundibulum(Wilcoxon P!0.0001 and ANOVA P!0.0001). Accor-ding to the univariate and multivariate analyses, boththe mean dose to the pituitary and the dose to the distalinfundibulum are the most important and independentfactors for the development of hypopituitarism. Statisti-cal significance of other factors has not been proved(Table 5). Correlation analysis according to Spearmenrank correlation coefficient demonstrated that the doseto the distal infundibulum correlates with the meandose to the pituitary; this correlation is more expressedin patients irradiated with a mean dose to the pituitaryof more than 15 Gy (rs 0.63) than in patients irradiatedwith a mean dose to the pituitary of !15 Gy (rs 0.35).
The threshold level of the mean dose to the pituitaryand the maximum dose to the distal infundibulum forthe development of hypopituitarism was evaluatedaccording to the Cox model. The threshold levels of18.2 Gy for the mean dose to the pituitary and16.8 Gy for the maximum dose to the distal infundibu-lum were found.
When comparing both groups of patients accordingto the success of the treatment, hormonal normalizationwas achieved in 42.8% of acromegaly patients, 50% ofprolactinoma patients, 80% of patients with Cushing’sdisease in the group I and in 65.2% of acromegalypatients, 37.5% of prolactinoma patients and 83.3% ofpatients with Cushing’s disease in the group II at thetime of 5 years after LGK irradiation. All differences inhormonal normalization between both groups were notfound to be significant (non-significant P levels in c2-test). In the group of acromegaly patients, the effect ofLGK irradiation depended on the baseline hormonalactivity of adenoma; the less active adenomas werenormalized earlier (Wilcoxon P!0.0074 and Kruskal–Wallis P!0.0047).
Growth of the adenoma after LGK irradiation was notobserved in any of the groups.
www.eje-online.org
Discussion
Radiation therapy is one of the treatment optionsfor pituitary adenomas, which is used especiallywhen neurosurgical treatment and pharmacologicaltreatment have failed. Radiation treatment (bothconventional fractionated irradiation and radiosurgery)is reported to be associated with the developmentof side effects, especially with the development ofhypopituitarism.
With regard to the development of hypopituitarismafter conventional radiotherapy, the total absorbed doseto the hypothalamo–pituitary axis is the major factordetermining the risk and speed of radiation-inducedhypopituitarism (25). The incidence of hypopituitarismincreases with time after irradiation (13, 25). It hasbeen observed that the somatotrophic axis is the mostradiosensitive one, followed by the gonadal, adreno-cortical and TSH axes. Furthermore, the more thepituitary function is disturbed prior to conventionalradiotherapy, the greater the incidence of hypopitui-tarism. The incidence of hypopituitarism varies indifferent published studies and is reported to rise up to80% 10 years after conventional radiotherapy (7, 9).
A high number of pituitary deficiencies are reportedeven in recent studies of fractionated stereotacticradiotherapy (FSRT). Schalin-Jantti et al. (26) referredthe development of new hypopituitarism in 40% ofpatients during a mean follow-up of 5.25 years;Roug et al. (27) reported the development of hypopitui-tarism in 29% of patients with a median of 48 monthsafter FSRT.
Data regarding the incidence of hypopituitarismfollowing LGK irradiation differ in published studies aswell (Table 6). Possible explanations for the differentincidence of hypopituitarism following LGK irradiationinclude different lengths of follow-up after irradiation,different sizes of adenomas, previous damage ofpituitary and above all different radiation doses.
Our patients with pituitary adenomas were treatedwith an LGK model B (Elekta Instrument AB). It is an

Table
6O
verv
iew
of
the
develo
pm
ent
of
hypopituitarism
after
LG
Kirra
dia
tion.
Study
Numberof
patients
NFA
a/SA
b
Targettumour
volume
(mm
3)
Maxim
al
dose
(Gy)
Margin
dose
(Gy)
Follow-up
(month
s)
Tim
eto
the
developmentof
hypopituitarism
(month
s)
Percentageof
patients
developing
hypopituitarism
(29)
25
0/2
5(G
H,
pro
lactin
and
AC
TH
)M
ean
1340G
830
(75–
3360)
Mean
28G
6(1
2–35)
Mean
20
(6–36)
Range
12–24
16
(30)
16
0/1
6(G
H)
Mean
50
Mean
25
Mean
16.8
(6–31.2
)0
(31)
65
22/4
3(G
H,
pro
lactin
and
AC
TH
)M
ean
48.5
Mean
25.4
(15–36)
Mean
25.5
(3–54)
1.5
(32)
37
0/3
7(p
rola
ctin,
GH
and
AC
TH
)M
ean
900
(100–2600)
Mean
54.8
(35–80)
Mean
28.7
(18–40)
Mean
26.9
0
(33)
73
31/4
2(p
rola
ctin,
GH
and
AC
TH
)M
ean
4400
(475–18
475)
Mean
31.6
(18.3
–45.5
)M
ean
28.9G
21.5
19.2
(34)
43
0/4
3(A
CT
H)
Mean
47
(12–60)
Media
n20
(3.6
–30)
Media
n44
(18–113)
Mean
21
(8–35)
16
(28)
17
0/1
7(G
H)
Mean
25
(20–40)
Mean
58.8
0
(20)
92
61/3
1(p
rola
ctin,
GH
and
AC
TH
)M
ean
3800
(200–14
600)
Mean
15
(8.5
–35.5
)M
ean
55.2G
28.8
Media
n18
40
(19)
30
30/0
Media
n1700
(100–9100)
Media
n29.1
(16.4
–40.0
)M
edia
n16.0
(11.1
–20.0
)M
edia
n57.7
(27.8
–86.1
)10
(18)
42
42/0
Mean
32G
8(2
0–70)
Mean
16.2G
4(1
0–34)
Mean
31.2
(6–102)
0
(17)
43
0/4
3(p
rola
ctin,
GH
and
AC
TH
)M
edia
n4300
(400–17
000)
Media
n40
(30–60)
Media
n20
(14.4
–30)
Media
n36
(12–108)
16
(35)
33
33/0
Media
n5000
(1000–11
700)
Media
n36
(30–40)
Media
n16
(12–40)
Media
n43
(16–106)
Media
n24
(19–48)
28
(36)
30
0/3
0(G
H)
Media
n1430
(200–3700)
Media
n20
(15–35)
Media
n46
(9–96)
Range
24–72
6.7
(37)
78
56/2
2(p
rola
ctin,
GH
and
AC
TH
)M
edia
n2300
(100–27
400)
Media
n30
(20–32)
Media
n15
(14–16)
Media
n36
(9–100)
4
(38)
54
54/0
Mean
2300
(600–7800)
Mean
33.2G
0.7
(24–42)
Mean
16.6G
0.4
(12–21)
Mean
41.1G
3.1
9.3
(39)
82
0/8
2(G
H)
Media
n25
(12–40)
Mean
49.5
(6–108)
Range
12–84
17.1
(21)
96
0/9
6(G
H)
Media
n1350
(93.6
–12
700)
Media
n70
(26–80)
Media
n35
(10–42)
Media
n54
(12–120)
Media
n30
(6–72)
38.2
(40)
37
0/3
7(G
H)
Mean
49.5
(25–70)
Mean
29.3
(2.8
–85.6
)R
ange
18–78
8.1
(41)
100
100/0
Mean
4800
(600–27
000)
41.5
(10–70)
Mean
18.5
(5–25)
Mean
47.9
(6–127)
Mean
26
(8–107)
19.7
(42)
28
0/2
8(P
RL)
Media
n3400
(200–21
000)
Mean
43.1
(10–62.5
)M
ean
18.9
(0.3
–25)
Media
n52
(15–122)
Mean
44
(33–51)
29
(43)
46
0/4
6(G
H)
Media
n3300
(500–18
000)
Media
n43.5
(30–60)
Media
n21.5
(14.4
–30)
Media
n63
(22–168)
Media
n32
(12–120)
33
(44)
90
0/9
0(A
CT
H)
Mean
49
(18–60)
Mean
23
(8–30)
Media
n45
(12–132)
Mean
16
(4–36)
22
(45)
62
62/0
Media
n4000
(800–12
900)
Media
n34.5
Media
n16
(11–20)
Media
n64
(23–161)
Media
n24
27
(46)
40
0/4
0(A
CT
H)
Media
n521
(94–4300)
Media
n29.5
(15–40)
Media
n48
(12–120)
Range
12–96
15
(47)
35
0/3
5(P
RL)
Media
n980
(34–13
200)
Media
n70
(40–80)
Media
n34
(20–49)
Media
n66
(18–138)
Media
n54
(31–103)
14.3
aN
on-f
unctionaladenom
as.
bH
orm
one-s
ecre
ting
adenom
as.
Hypopituitarism after LGK irradiation 175EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
www.eje-online.org

176 J Marek and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
optimal tool for radiosurgery in the sellar region thanksto the distribution of radioactive Cobalt-60 sources inspace, which allows a steep decline of isodoses at themargin. In spite of this tool, we recorded a highincidence of hypopituitarism in our first patients treatedby LGK. This fact led us to analyse factors inducing thedevelopment of hypopituitarism. In our previouslypublished study (22), according to the statisticalanalysis (univariate and multivariate methods) of thepotential risk factors responsible for radiation-inducedhypopituitarism, it was found that the most importantfactor is the mean dose to the pituitary gland. Whenthis dose did not exceed 15 Gy, no impairment ofthyroid or gonadal function was observed, rising to18 Gy for adrenocortical function. The cumulativerisk of adrenocortical deficiency development wascalculated at 85% after 90 months when the meandose on the healthy pituitary exceeded 20 Gy. Similarly,when the dose was 17 Gy (or more) on healthypituitary, the cumulative risk of hypogonadism was60%, and of hypothyreosis was 85% (also calculated forthe period of 90 months). On the basis of this analysis, aradiation dose of 15 Gy was determined as themaximum safe limit of the mean radiation dose to thepituitary gland.
In our group of patients, hypopituitarism developed inonly one (2.2%) patient among those irradiated with amean dose to the pituitary of !15 Gy in contrast to 29(72.5%) of the patients irradiated with a mean dose tothe pituitary of more than 15 Gy. The follow-up periodfor patients irradiated with a mean dose to the pituitaryof !15 Gy was shorter than the follow-up period for agroup of patients irradiated with a mean dose to thepituitary of more than 15 Gy (follow-up median 73 vs135 months). However, when comparing both sub-groups of followed patients at the same time point of5 years after LGK irradiation, it was found thathypopituitarism developed in only 1 (2.2%) patientamong those irradiated with a mean dose to thepituitary of !15 Gy and in 22 (55.0%) patientsamong those irradiated with a mean dose to thepituitary of more than 15 Gy.
In this study, for the entire group of 85 patients,the radiation dose of 18.2 Gy was calculated as themaximum safe limit of the mean radiation dose to thepituitary gland. As mentioned above, in our previouslypublished study (22), it was found that hypothyreosisor hypogonadism did not develop, when the mean doseto the pituitary gland did not exceed 15 Gy, rising to18 Gy for adrenocortical deficiency. With regard to theresults of both observations, we recommend keepingthe mean dose to pituitary gland under 15 Gy.
Information about the mean dose to the pituitaryis also given in the study by Ikeda et al. (28). In theirstudy, 17 acromegalic patients irradiated with LGKafter transsphenoidal surgery were followed. The doseto the pituitary did not exceed 10 Gy, and themean follow-up was 4.9 years. Of 17 patients,
www.eje-online.org
3 exhibited panhypopituitarism before LGK irradiation.Hypopituitarism was not observed in any of the14 remaining patients.
Data referring to the development of hypopituitarismrelated to previous partial pituitary deficiency andneurosurgery before LGK irradiation support theimportance of keeping the mean radiation dose to thepituitary gland under 15 Gy. In patients receiving somereplacement therapy before LGK irradiation, a newdeficiency developed in only one of patients irradiatedwith a mean dose to the pituitary of !15 Gy incomparison with 93.3% of patients irradiated with amean dose to the pituitary of O15 Gy. Similarly, inpatients undergoing neurosurgery before LGK irradi-ation, a new deficiency developed in only one of patientsirradiated with a mean dose to the pituitary of !15 Gyin comparison with 88.0% of patients irradiated with amean dose to the pituitary of O15 Gy.
In our previous study, it was confirmed that themaximum dose to the distal infundibulum plays asimilarly important role in the development of hypopi-tuitarism. Results proved that the maximum dose to thedistal infundibulum is an independent factor for thedevelopment of hypopituitarism. This dose should bekept under 17 Gy. In the study published by Feigl et al.(20), it was demonstrated that the dose to the pituitarystalk was significantly higher in patients with deterio-ration of pituitary function as compared with those inwhom function remained unchanged.
When comparing the success of hormonal normal-ization, there were no significant differences bet-ween both groups of patients. In agreement with ourpreviously published data relating to acromegalypatients, the effect of the LGK therapy depends on thebaseline hormonal activity of the adenoma – the lessactive adenomas are normalised earlier (21).
Hypopituitarism is the most common side effectassociated with LGK irradiation. Our study provesthat keeping the mean radiation dose to the pituitarygland under 15 Gy and the infundibulum dose to levels!17 Gy prevents the development of hypopituitarismfollowing LGK irradiation. It is known that hypopitui-tarism can develop many years after irradiation. Weobserved the results of a mean dose to the pituitaryof up to 15 Gy and the maximum dose to the distalinfundibulum of up 17 Gy for 5 years. Future long-termstudies will be necessary to confirm that they remainmaximum safe doses to avoid hypopituitarism. Theabsence of investigation of GH axis after LGK irradiationis another limitation of our study.
In conclusion, to avoid hypopituitarism, the meanradiation dose to the pituitary tissue surrounding theadenoma should be !15 Gy, and the maximum dose todistal infundibulum should be !17 Gy. These limitsshould become a rule when irradiating pituitaryadenomas, similar to the dose rules of 8 Gy for theoptical tract or 12–14 Gy for brain stem.

Hypopituitarism after LGK irradiation 177EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
Declaration of interest
The authors declare that there is no conflict of interest that could beperceived as prejudicing the impartiality of the research reported.
Funding
This work was supported by an institutional grant from the Ministry ofEducation of the Czech Republic (MSM 002 162 0807).
References
1 Hardy J. Transsphenoidal microsurgery of prolactinomas. InSecretory Tumors of the Pituitary Gland, pp 73–81. Eds PM Black,NT Zervas, EC Ridgway & JB Martin, New York: Raven Press,1984.
2 Fahlbusch R & Buchfelder M. Present status of neurosurgery inthe treatment of prolactinomas. Neurosurgical Review 1985 8195–205. (doi:10.1007/BF01815444)
3 Freda PU, Sharon L, Wardlaw SL & Post KD. Long-termendocrinological follow-up evaluation in 115 patients whounderwent transsphenoidal surgery for acromegaly. Journal ofNeurosurgery 1998 89 353–358. (doi:10.3171/jns.1998.89.3.0353)
4 Swearingen B, Biller BMK, Barker FG, Katznelson L, Grinspoon S,Klibanski A & Zervas NT. Long-term mortality after transsphenoi-dal surgery for Cushing’s disease. Annals of Internal Medicine 1999130 821–824.
5 Kreutzer J, Vance ML, Lopes MB & Laws ER Jr. Surgicalmanagement of GH- secreting pituitary adenomas: an outcomestudy using modern remission criteria. Journal of ClinicalEndocrinology and Metabolism 2001 86 4072–4077. (doi:10.1210/jc.86.9.4072)
6 Jane JA Jr & Laws ER. The surgical management of pituitaryadenomas in a series of 3,093 patients. Journal of the AmericanCollege of Surgeons 2001 193 650–659. (doi:10.1016/S1072-7515(01)01101-2)
7 Barrande G, Pittino-Lungo M, Coste J, Ponvert D, Bertagna X,Luton JP & Bertherat J. Hormonal and metabolic effects ofradiotherapy in acromegaly: long-term results in 128 patientsfollowed in a single center. Journal of Clinical Endocrinology andMetabolism 2000 85 3779–3785. (doi:10.1210/jc.85.10.3779)
8 Biermasz NR, van Dulken H & Roelfsema F. Postoperativeradiotherapy in acromegaly is effective in reducing GH concen-tration to safe levels. Clinical Endocrinology 2000 53 321–327.(doi:10.1046/j.1365-2265.2000.01095.x)
9 Minniti G, Jaffrain-Rea M, Osti M, Esposito V, Santoro A, Solda F,Gargiulo P, Tamburrano G & Enrici RM. The long-term efficacy ofconventional radiotherapy in patients with GH-secreting pituitaryadenomas. Clinical Endocrinology 2005 62 210–216. (doi:10.1111/j.1365-2265.2005.02199.x)
10 Flickinger JC, Nelson PB, Taylor FH & Robinson A. Incidence ofcerebral infarction after radiotherapy for pituitary adenoma.Cancer 1989 63 2404–2408. (doi:10.1002/1097-0142(19890615)63:12!2404::AID-CNCR2820631205O3.0.CO;2-3)
11 Fukamachi A, Wakao T & Akai J. Brain stem necrosis afterirradiation of pituitary adenoma. Surgical Neurology 1982 18343–350. (doi:10.1016/0090-3019(82)90146-X)
12 Bowen J & Paulsen CA. Stroke after pituitary irradiation. Stroke1992 23 908–911.
13 Brada M, Rajan B, Traish D, Ashley S, Holmes-Sellors J & Uttley D.The long-term efficacy of conservative surgery and radiotherapy inthe control of pituitary adenomas. Clinical Endocrinology 1993 38571–578. (doi:10.1111/j.1365-2265.1993.tb02137.x)
14 Fisher BJ, Gaspar LE & Noone B. Radiation therapy of pituitaryadenoma: delayed sequelae. Radiology 1993 187 843–846.
15 Liscak R, Vladyka V, Marek J, Simonova G & Vymazal J. Gammaknife radiosurgery for endocrine-inactive pituitary adenomas. ActaNeurochirurgica 2007 149 999–1006. (doi:10.1007/s00701-007-1253-7)
16 Sheehan JP, Niranjan A, Sheehan JM, Jane JA, Laws ER,Kondziolka D, Flickinger J, Landolt AM, Loeffler JS &Lunsford LD. Stereotactic radiosurgery for pituitary adenomas:an intermediate review of its safety, efficacy, and role in theneurosurgical treatment armamentarium. Journal of Neurosurgery2005 102 678–691. (doi:10.3171/jns.2005.102.4.0678)
17 Pollock BE, Nippoldt TB, Stafford SL, Foote RL & Abboud ChF.Results of stereotactic radiosurgery in patients with hormone-producing pituitary adenomas: factors associated with endocrinenormalization. Journal of Neurosurgery 2002 97 525–530.(doi:10.3171/jns.2002.97.3.0525)
18 Sheehan JP, Kondziolka D, Flickinger J & Lunsford LD. Radiosurgeryfor residual or recurrent nonfunctioning pituitary adenoma.Journal of Neurosurgery 2002 97 (Supplement 5) 408–414.(doi:10.3171/jns.2002.97.supplement5.0408)
19 Wowra B & Stummer W. Efficacy of gamma knife radiosurgery fornonfunctioning pituitary adenomas: a quantitative follow up withmagnetic resonance imaging-based volumetric analysis. Journal ofNeurosurgery 2002 97 (Supplement 5) 429–432. (doi:10.3171/jns.2002.97.supplement5.0429)
20 Feigl GCh, Bonelli ChM, Berghold A & Mokry M. Effects of gammaknife radiosurgery of pituitary adenomas on pituitary function.Journal of Neurosurgery 2002 97 (Supplement 5) 415–421.
21 Jezkova J, Marek J, Hana V, Krsek M, Weiss V, Vladyka V, Liscak R,Vymazal J & Pecen L. Gamma knife radiosurgery for acromegaly –long-term experience. Clinical Endocrinology 2006 64 588–595.(doi:10.1111/j.1365-2265.2006.02513.x)
22 Vladyka V, Liscak R, Novotny J Jr, Marek J & Jezkova J. Radiationtolerance of functioning pituitary tissue in gamma knife surgeryfor pituitary adenomas. Neurosurgery 2003 52 309–317. (doi:10.1227/01.NEU.0000043709.53906.31)
23 Novotny J Jr, Novotny J, Vymazal J, Liscak R & Vladyka V.Assessment of the accuracy of stereotactic target localizationusing magnetic resonance imaging: phantom study. Journal ofRadiosurgery 1998 1 99–111. (doi:10.1023/B:JORA.0000010893.37324.87)
24 Abs R, Bengtsson BA, Hernberg-Stahl E, Monson JP, Tauber JP,Wilton P & Wuster Ch. GH replacement in 1034 growthhormone deficient hypopituitary adults: demographic and clinicalcharacteristics, dosing and safety. Clinical Endocrinology 1999 50703–713. (doi:10.1046/j.1365-2265.1999.00695.x)
25 Littley MD, Shalet SM & Beardwell CG. Hypopituitarism followingexternal beam radiotherapy for pituitary tumours in adults.Quarterly Journal of Medicine 1989 70 145–160.
26 Schalin-Jantti C, Valanne L, Tenhunen M, Setala K, Paetau A,Sane T & Kouri M. Outcome of fractionated stereotactic radio-therapy in patients with pituitary adenomas resistant toconventional treatment: a 5.25-year follow-up study. ClinicalEndocrinology 2010 73 72–77.
27 Roug S, Rasmussen AK, Juhler M, Kosteljanetz M, Poulsgaard L,Heeboll H, Roed H & Feldt-Rasmussen U. Fractionated stereo-tactic radiotherapy in patients with acromegaly: an interimsingle-centre audit. European Journal of Endocrinology 2010 162685–694. (doi:10.1530/EJE-09-1045)
28 Ikeda H, Jokura H & Yoshimoto T. Transsphenoidal surgery andadjuvant gamma knife treatment for growth hormone-secretingpituitary adenoma. Journal of Neurosurgery 2001 95 285–291.(doi:10.3171/jns.2001.95.2.0285)
29 Morange-Ramos I, Regis J, Dufour H, Andrieu JM, Grisoli F,Jaquet P & Peragut JC. Short-term endocrinological resultsafter gamma knife surgery of pituitary adenoma. Stereotactic andFunctional Neurosurgery 1998 70 (Supplement 1) 127–138.(doi:10.1159/000056415)
30 Landolt AM, Haller D, Lomax N, Scheib S, Schubiger O, Siegfried J& Wellis G. Stereotactic radiosurgery for recurrent surgically
www.eje-online.org

178 J Marek and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2011) 164
treated acromegaly: comparison with fractionated radiotherapy.Journal of Neurosurgery 1998 88 1002–1008. (doi:10.3171/jns.1998.88.6.1002)
31 Lim YL, Leem W, Kim TS, Rhee BA & Kim GK. Four years’experience in the treatment of pituitary adenomas with gammaknife radiosurgery. Stereotactic and Functional Neurosurgery 199870 (Supplement 1) 95–109. (doi:10.1159/000056412)
32 Kim SH, Huh R, Chang JW, Park YG & Chung SS. Gamma kniferadiosurgery for functioning pituitary adenomas. Stereotactic andFunctional Neurosurgery 1999 72 (Supplement 1) 101–110.(doi:10.1159/000056445)
33 Mokry M, Ramschak-Schwarzer S, Simbrunner J, Ganz JC &Pendl G. A six year experience with the postoperative radiosurgicalmanagement of pituitary adenomas. Stereotactic and FunctionalNeurosurgery 1999 72 (Supplement 1) 88–100. (doi:10.1159/000056444)
34 Sheehan JM, Vance ML, Sheehan JP, Ellegala DB & Laws ER Jr.Radiosurgery for Cushing’s disease after failed transsphenoidalsurgery. Journal of Neurosurgery 2000 93 738–742. (doi:10.3171/jns.2000.93.5.0738)
35 Pollock BE & Carpenter PC. Stereotactic radiosurgery as analternative to fractionated radiotherapy for patients with recur-rent or residual nonfunctioning pituitary adenomas. Neurosurgery2003 53 1086–1094. (doi:10.1227/01.NEU.0000088661.81189.66)
36 Attanasio R, Epaminonda P, Motti E, Giugni E, Ventrella L, Cozzi R,Farabola M, Loli P, Beck-Peccoz P & Arosio M. Gamma-kniferadiosurgery in acromegaly: a 4-year follow-up study. Journal ofClinical Endocrinology and Metabolism 2003 88 3105–3112.(doi:10.1210/jc.2002-021663)
37 Petrovich Z, Yu C, Gianotta SL, Zee CS & Apuzzo ML. Gammaknife radiosurgery for pituitary adenoma: early results. Neuro-surgery 2003 53 51–59. (doi:10.1227/01.NEU.0000068702.00330.47)
38 Losa M, Valle M, Mortini P, Franzin A, da Passano CF, Cenzato M,Bianchi S, Picozzi P & Giovanelli M. Gamma knife surgery fortreatment of residual nonfunctioning pituitary adenomas aftersurgical debulking. Journal of Neurosurgery 2004 100 438–444.(doi:10.3171/jns.2004.100.3.0438)
39 Castinetti F, Taieb D, Kuhn JM, Chanson P, Tamura M, Jaquet P,Conte-Devolx B, Regis J, Dufour H & Brue T. Outcome of gamma
www.eje-online.org
knife radiosurgery in 82 patients with acromegaly: correlationwith initial hypersecretion. Journal of Clinical Endocrinology andMetabolism 2005 90 4483–4488. (doi:10.1210/jc.2005-0311)
40 Landolt AM, Lomax N, Scheib SG & Girard J. Gamma knifesurgery after fractionated radiotherapy for acromegaly. Journal ofNeurosurgery 2006 105 31–36. (doi:10.3171/sup.2006.105.7.31)
41 Mingione V, Yen ChP, Vance ML, Steiner M, Sheehan J, Laws E &Steiner L. Gamma knife surgery in the treatment of nonsecretarypituitary macroadenoma. Journal of Neurosurgery 2006 104876–883. (doi:10.3171/jns.2006.104.6.876)
42 Pouratian N, Sheehan J, Jagannathan J, Laws ER, Steiner L &Vance ML. Gamma knife radiosurgery for medically and surgicallyrefractory prolactinomas. Neurosurgery 2006 59 255–264.(doi:10.1227/01.NEU.0000223445.22938.BD)
43 Pollock BE, Jacob JT, Brown PD & Nippoldt TB. Radiosurgery forgrowth hormone-producing pituitary adenomas: factors associ-ated with biochemical remission. Journal of Neurosurgery 2007106 833–838. (doi:10.3171/jns.2007.106.5.833)
44 Jagannathan J, Sheehan JP, Pouratian N, Laws ER, Steiner L &Vance ML. Gamma knife surgery for Cushing’s disease. Journal ofNeurosurgery 2007 106 980–987. (doi:10.3171/jns.2007.106.6.980)
45 Pollock BE, Cochran J, Natt N, Brown PD, Erickson D, Link MJ,Garces YI, Foote LR, Stafford SL & Schomberg PJ. Gamma kniferadiosurgery for patients with nonfunctioning pituitary adeno-mas: results from a 15-year experience. International Journal ofRadiation Oncology, Biology, Physics 2008 70 1325–1329.(doi:10.1016/j.ijrobp.2007.08.018)
46 Castinetti F, Nagai M, Dfour H, Kuhn JM, Morange I, Jaquet P,Conte-Devolx B, Regis J & Brue T. Gamma knife radiosurgery is asuccessful adjunctive treatment in Cushing’s disease. EuropeanJournal of Endocrinology 2007 156 91–98. (doi:10.1530/eje.1.02323)
47 Jezkova J, Hana V, Krsek M, Weiss V, Vladyka V, Liscak R,Vymazal J, Pecen L & Marek J. Use of the Leksell gamma knife in thetreatment of prolactinoma patients. Clinical Endocrinology 200970 732–741. (doi:10.1111/j.1365-2265.2008.03384.x)
Received 13 October 2010
Accepted 11 November 2010