Embed Size (px)
Citation preview

IdM
Opc
Sai
Rmrr
Co
Taftwiwrib
aUtu
FGRCIDU(
PPS
R2
R
0©d
PCOGS Papers www.AJOG.org
s computed tomography a reliable diagnostic modality inetecting placental injuries in the setting of acute trauma?aria Manriquez, MD; Gujjarappa Srinivas, MD; Srigayatri Bollepalli, MD; Lynley Britt, MD; David Drachman, PhD
Ctmpbct
K
BJECTIVE: The objective of this study was to determine whether com-uted tomography (CT) is a reliable method of imaging to assess pla-ental injury after acute trauma during pregnancy.
TUDY DESIGN: This study was a retrospective review of digital CT im-ges and electronically scanned charts of pregnant trauma patients
dentified from the hospital trauma registry list.
ESULTS: Using delivery within 36 hours of trauma as the clinicalarker for the occurrence of placental abruption, positive radiologic
eadings showed 86% sensitivity and 98% specificity. The overall accu-
f acute trauma? Am J Obstet Gynecol 2010;202:611.e1-5.
vurad
etrciatetscrclp
ccrirfAgrwveloping preembryo, e
oi: 10.1016/j.ajog.2010.01.027
ONCLUSION: Given that defined patterns on CT can be identified andhose can be correlated to actual abruption, CT may be a reliableethod for evaluation of placental abruption after maternal trauma, es-
ecially in the face of abdominal trauma. Our results show that CT hasoth good sensitivity and specificity identifying abruption and should beonsidered for use in the management in the pregnant patient afterrauma.
ey words: computed tomography, placental abruption, trauma in
acy was 96%. pregnancyite this article as: Manriquez M, Srinivas G, Bollepalli S, et al. Is computed tomography a reliable diagnostic modality in detecting placental injuries in the setting
pdwbttcsicrttctaag
MTpiopMAoa
oc
rauma has been reported to affectbetween 3% and 8% of pregnancies
nd is known to increase maternal andetal morbidity and mortality.1,2 Placen-al abruption is present in up to 40% ofomen with severe maternal trauma and
s clinically evident in 1-5% of womenith minor trauma.3 When placental ab-
uption occurs in the face of trauma dur-ng pregnancy, fetal and maternal life cane compromised.Early and accurate diagnosis is imper-
tive for fetal and maternal resuscitation.sually evaluation for placenta disrup-
ion from the uterus is accomplished byltrasound imaging; however, in a re-
rom the Departments of Obstetrics andynecology (Drs Manriquez and Britt),adiology (Drs Srinivas and Bollepalli), andlinical Research (Dr Drachman), Maricopa
ntegrated Health System, and theepartment of Obstetrics and Gynecology,niversity of Arizona College of Medicine
Dr Manriquez), Phoenix, AZ.
resented at the 76th Annual Meeting of theacific Coast Obstetrical and Gynecologicalociety, La Jolla, CA, Sept. 30-Oct. 4, 2009.
eceived Sept. 15, 2009; revised Nov. 14,009; accepted Jan. 15, 2010.
eprints not available from the authors.
002-9378/$36.002010 Mosby, Inc. All rights reserved.
iew of the literature, the sensitivity forltrasound in diagnosing abruption iseported to be anywhere between 24%nd 50%. Consequently, a negative scanoes not rule out placental abruption.4
In early abruption, which would gen-rally be the time of evaluation afterrauma, it was found that the area of ab-uption was hyperechoic to isoechoicompared with the placenta.5 Depend-ng on the age of the abruption, theppearance on ultrasound can vary be-ween hyperechoic, isoechoic, hypo-choic, or sonolucent, which may add tohe difficulty in diagnosis in the traumaetting. Computed tomography (CT) isommonly used to diagnose nonobstet-ic injuries in traumas, although con-erns regarding radiation exposure haveimited this practice in the pregnantatient.The American College of Obstetri-
ians and Gynecologists guidelines dis-ourage the use of multiple diagnosticadiology examinations while recogniz-ng a cumulative amount of less than 5ad has not been associated with adverseetal effects.6 Moreover, according to themerican College of Radiology, no sin-le diagnostic X-ray procedure results inadiation exposure to a degree thatould threaten the well-being of the de-
mbryo, or fetus. l
JUNE 2010 Americ
When CT is used in the evaluation of aregnant trauma patient, the chest, ab-omen, and pelvis may be scanned safelyith a low-exposure technique, com-ined with nonionic iodinated con-rast.7,8 Recognizing that CT imaging ofhe abdomen and pelvis is used with in-reasing frequency, we undertook atudy to determine whether CT imagings a reliable method in diagnosing pla-ental abruption after trauma. In aecent study of CT evaluation of placen-al abruption, the authors found thatrue placental abruptions were large,ontiguous, and retroplacental. The au-hors also noted that full-thicknessreas of low enhancement that formcute angles with myometrium sug-ested abruption.9
ATERIALS AND METHODShis study was a retrospective study ofregnant trauma patients. After receiv-
ng institutional review board approvaln Oct. 8, 2008, a list of pregnant traumaatients from the trauma registry ataricopa Medical Center in Phoenix,
Z, was obtained. We focused our studyn patients who had abdominal CT im-ging during an 18 month period.
A board-certified experienced radiol-gist (G.S.) with no knowledge of thelinical course reviewed the CT images,
ooking for placental disruption, identi-an Journal of Obstetrics & Gynecology 611.e1

fitatwat
pobhlpdro
imtsch
2easA
wccwoof
tsgdcpatsW
RTacawaotbmctdcw
7ipto(h5acfpruhas
ChC
M
PCOGS Papers www.AJOG.org
6
ed by separation of the placenta fromhe uterus, retroplacental hematoma,nd decreased percent enhancement ofhe placenta after trauma. Independentlyithout seeing the CT scan or its report,
n obstetrician (M.M., L.B.) reviewedhe electronically scanned charts of these
FIGURE 1CT scan at 37 weeks’ gestational a
T scan of 37 weeks’ gestational age shows pancement representing nonperfused placenta. TT, computed tomography.
anriquez. CT to diagnose placental injuries in acute traum
TABLE 1CT interpretation results
Variable
CT readingsfor abruption Total
Negative Positive Negative
Delivered..................................................................................................
No 53 1 54..................................................................................................
Yes 1 6 7...........................................................................................................
Total 54 7 61...........................................................................................................
CT, computed tomography.
Manriquez. CT to diagnose placental injuries inacute trauma. Am J Obstet Gynecol 2010.
11.e2 American Journal of Obstetrics & Gynecolo
atients to evaluate for clinical evidencef abruption, using markers of vaginalleeding, uterine pain, abnormal fetaleart rate tracings, contractions, and de-
ivery. Those patients who had any of thereviously listed markers that requiredelivery were considered potential ab-uption, abruption then being validatedn examination of placenta at delivery.The data were collected and recorded
ndependently and then submitted to aember of the research department who
hen merged the data. Given the retro-pective nature of this study, the clini-ians actually caring for the patients didave access to the CT scan and its report.Between May 2006 and November
008, 61 pregnant trauma patients werevaluated by abdominal or pelvic CT im-ging (GE 16 slice detector; GE, Wauke-ha, WI) at Maricopa Medical Center.ll patients had intravenous contrast
rior placenta with large area of decreased en-lack arrow points to a retroplacental hematoma.
J Obstet Gynecol 2010.
t
gy JUNE 2010
ith iopamidol, a nonionic iodine-basedontrast medium that is safety rated asategory B. A low-exposure techniqueas not implemented because the intentf scan was not focused to a specific areaf interest but a full abdomen to assessor internal injury.
The data collected were analyzed usinghe kappa coefficient, thus allowing mea-ure of association between the radiolo-ist’s judgments and the clinical courseefining abruption but correcting forhance agreement. With respect toower analysis, if the CT images are nott all useful in detecting placentalrauma, then we would expect that sen-itivity and specificity to be 50% each.
e took this as the null hypothesis.
ESULTShe cause of trauma was motor vehicleccident except in 4 cases of assault and 2ases of pedestrian vehicle accident. Thege range of our patient was 16-40 yearsith 49 of the 61 patients being under the
ge of 30 years. Delivery within 36 hoursf trauma was used as the standard forhe occurrence of placental trauma, thiseing validated by postdelivery com-ents in the patients’ record of the pla-
enta for clots or pathology reports iden-ifying abruption. Of the patients whoelivered, all were victims of motor vehi-le accidents: 4 were restrained and 3ere not.Fifty-four patients did not deliver anddid deliver; 6 of these 7 had positive
nterpretations (Table 1). Positive inter-retations were retroplacental hema-oma (Figure 1), separation of placenta,r decreased placental enhancementFigure 2). We classified placental en-ancement in 3 categories, greater than0% enhancement was considered nobruption, 25-50% enhancement wasonsidered equivocal, and less than 25%ocal enhancement was the marker forlacental abruption. The CT image rep-esenting the largest area of placenta wassed in determining percentage of en-ancement; this was typically of 1 slice,nd a combination of axial, coronal, andagittal views were used.
The 1 patient with a negative interpre-
ge
ostehe b
a. Am
ation had a 25-50% enhancement (Fig-

uptstahlvdtcohsrclo
pcs9w(hfstps5t
CTtrsacadnoi
cnitntt
BC
M
www.AJOG.org PCOGS Papers
re 3), and she delivered after 36 hours inreterm labor. Noteworthy, the opera-ive note for this patient identified amall less than 10% abruption defined byhe amount of clot covering the placentat the time of delivery. The patient whoad a positive interpretation without de-
ivery was the result of a severe motorehicle accident and was discharged un-elivered at 7 weeks’ gestation. The pa-ient was instructed to follow up with ourlinic, but she was lost to follow-up. An-ther patient who had a severe motor ve-icle accident in the first trimester didhow CT signs of abruption by both aetroplacental clot and less than 25% fo-al enhancement. Her hospital stay wasengthy, and she ultimately spontane-usly aborted during her hospitalization.Using this information, the CT inter-
retations showed 86% sensitivity with aonfidence interval of 81-91% and 98%pecificity with a confidence interval of2-100%. The overall accuracy was 96%ith a confidence interval of 90-100%
Table 2). With our sample size of 61, weave 99% statistical power to detect a dif-
erence of 36% for sensitivity (the ob-erved value of 86% minus 50% underhe null hypothesis) and 99% statisticalower to detect a difference of 48% inpecificity (the observed value of 98% vs0% under the null hypothesis), both athe 95% level of confidence.
OMMENThe principal findings of our study were
hat CT imaging correctly identified ab-uption in cases with significant clinicaligns and gross placental pathology ofbruption. Often patients who have in-urred trauma receive CT imaging of thebdomen to evaluate for internal organamage. To date, at our institution, it hasot been the protocol to make judgmentf whether the placenta show signs of
njury.Many of the dictated reports reviewed
ommented only on the fact that a preg-ancy or fetus was seen on scan. Ideally,
f an abdominal or pelvic CT scan isaken for any reason in a trauma preg-ancy, the protocol would be to evaluate
he placenta for signs of trauma. Of note,
he position of the placenta, anterior orFIGURE 2Transverse and sagittal CT views of 34 weeks’ gestation
lack arrow identifies �25% enhancement, and white star identifies a retroplacental hematoma.T, computed tomography.
anriquez. CT to diagnose placental injuries in acute trauma. Am J Obstet Gynecol 2010.
JUNE 2010 American Journal of Obstetrics & Gynecology 611.e3
pnt
v
shibw
trwscul
idnthcwMett
astcitCta
oprgtfioccrfoncIagrt
R1C2
TaaC
M
PCOGS Papers www.AJOG.org
6
osterior, did not show a statistically sig-ificant difference on having abruption;
his has been also previously reported.10
The strength of this retrospective re-iew of CT images and clinical signs or
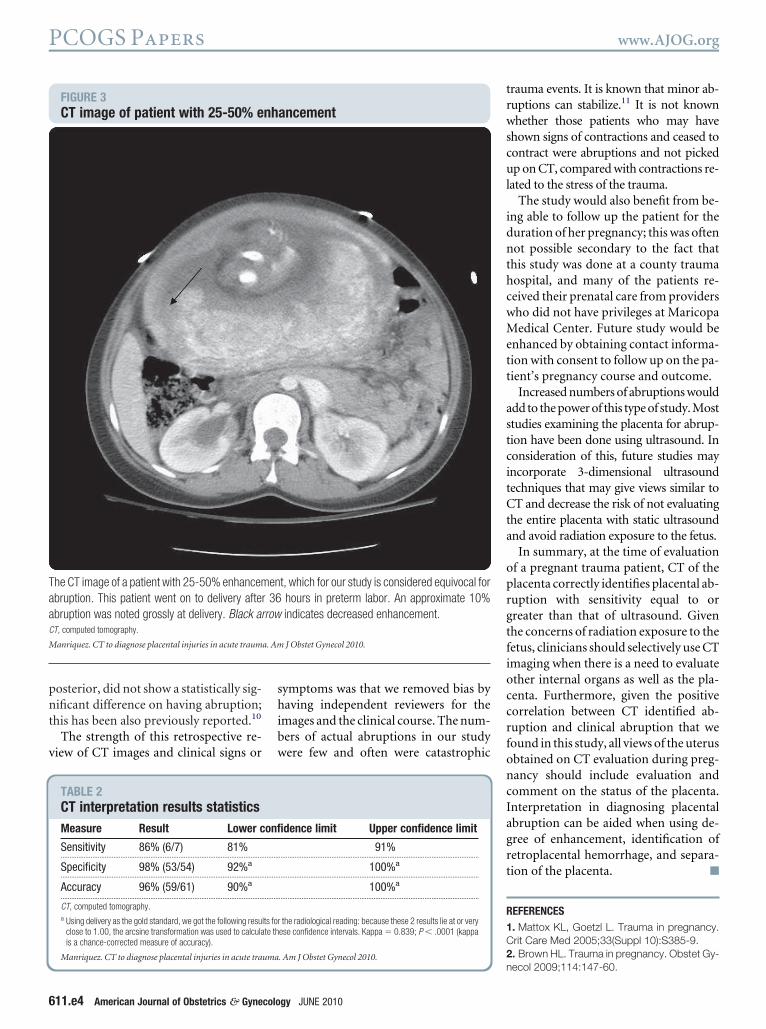
FIGURE 3CT image of patient with 25-50% e
he CT image of a patient with 25-50% enhancembruption. This patient went on to delivery afterbruption was noted grossly at delivery. Black arT, computed tomography.
anriquez. CT to diagnose placental injuries in acute traum
TABLE 2CT interpretation results statisticsMeasure Result Lower c
Sensitivity 86% (6/7) 81%...................................................................................................................
Specificity 98% (53/54) 92%a
...................................................................................................................
Accuracy 96% (59/61) 90%a
...................................................................................................................
CT, computed tomography.a Using delivery as the gold standard, we got the following resu
close to 1.00, the arcsine transformation was used to calculais a chance-corrected measure of accuracy).
Manriquez. CT to diagnose placental injuries in acute trauma
11.e4 American Journal of Obstetrics & Gynecolo
ymptoms was that we removed bias byaving independent reviewers for the
mages and the clinical course. The num-ers of actual abruptions in our studyere few and often were catastrophic
ancement
t, which for our study is considered equivocal forhours in preterm labor. An approximate 10%indicates decreased enhancement.
J Obstet Gynecol 2010.
dence limit Upper confidence limit
91%..................................................................................................................
100%a
..................................................................................................................
100%a
..................................................................................................................
the radiological reading: because these 2 results lie at or veryese confidence intervals. Kappa � 0.839; P � .0001 (kappa
n. Am J Obstet Gynecol 2010.
gy JUNE 2010
rauma events. It is known that minor ab-uptions can stabilize.11 It is not knownhether those patients who may have
hown signs of contractions and ceased toontract were abruptions and not pickedp on CT, compared with contractions re-
ated to the stress of the trauma.The study would also benefit from be-
ng able to follow up the patient for theuration of her pregnancy; this was oftenot possible secondary to the fact that
his study was done at a county traumaospital, and many of the patients re-eived their prenatal care from providersho did not have privileges at Maricopaedical Center. Future study would be
nhanced by obtaining contact informa-ion with consent to follow up on the pa-ient’s pregnancy course and outcome.
Increased numbers of abruptions woulddd to the power of this type of study. Mosttudies examining the placenta for abrup-ion have been done using ultrasound. Inonsideration of this, future studies mayncorporate 3-dimensional ultrasoundechniques that may give views similar toT and decrease the risk of not evaluating
he entire placenta with static ultrasoundnd avoid radiation exposure to the fetus.
In summary, at the time of evaluationf a pregnant trauma patient, CT of thelacenta correctly identifies placental ab-uption with sensitivity equal to orreater than that of ultrasound. Givenhe concerns of radiation exposure to theetus, clinicians should selectively use CTmaging when there is a need to evaluatether internal organs as well as the pla-enta. Furthermore, given the positiveorrelation between CT identified ab-uption and clinical abruption that weound in this study, all views of the uterusbtained on CT evaluation during preg-ancy should include evaluation andomment on the status of the placenta.nterpretation in diagnosing placentalbruption can be aided when using de-ree of enhancement, identification ofetroplacental hemorrhage, and separa-ion of the placenta. f
EFERENCES. Mattox KL, Goetzl L. Trauma in pregnancy.rit Care Med 2005;33(Suppl 10):S385-9.. Brown HL. Trauma in pregnancy. Obstet Gy-
nh
en36
row
a. Am
onfi
.........
.........
.........
lts forte th
ecol 2009;114:147-60.

3sO4pa5Shw
6pO7m18aa
9ot1tt31B
www.AJOG.org PCOGS Papers
. Pearlman MD, Viano D. Automobile crashimulation with first pregnant test dummy. Am Jbstet Gynecol 1996;175(4 Pt 1):977-81.. Glantz C, Purnell L. Clinical utility of sonogra-hy in the diagnosis and treatment of placentalbruption. J Ultrasound Med 2002;21:837-40.. Nyberg DA, Mack L, Benedetti TJ, Cyr DR,chuman WP. Placental abruption and placentalemorrhage: correlation of sonographic findings
ith fetal outcome. Radiology 1987;164:357-61. 2. Guidelines for diagnostic imaging duringregnancy. ACOG committee opinion no. 299.bstet Gynecol 2004;104:647-51.. Moore MM, Shearer DR. Fetal dose esti-ates for CT pelvimetry. Radiology 1989;71:265-67.. Atwell T, Lteif A. Neonatal thyroid functionfter administration of IV iodinated contrastgent to 21 pregnant patients. Am J Retroen
008;191:268-71. 1JUNE 2010 Americ
. Wei SH, Helmy M, Cohen AJ. CT evaluationf placental abruption in pregnant trauma pa-ients. Emerg Radiol 2009;16:365-73.0. Nagayama C, Suzuki S. Influence of placen-al position on outcome in patients with placen-al abruption. J Nippon Med Sch 2006;73:51-3.1. Pearlman MD, Tintinalli JE, Lorenz RP.lunt trauma during pregnancy. N Engl J Med
991;323:1609-13.an Journal of Obstetrics & Gynecology 611.e5





























