Embed Size (px)
Citation preview

Is a Brief Behavioral Activation Intervention Effective in Reducing Depressive
Symptoms?.Jennifer Funderburk, Ph.D.1,2,3
Collaborative Family Healthcare AssociationOctober 5th, 2012 Austin, Texas
1 Clinical Research Psychologist, Center for Integrated Healthcare, Syracuse VAMC
2 Department of Psychiatry, University of Rochester3 Department of Psychology, Syracuse University
Jennifer Funderburk does not have any relevant financial relationships during the past 12 months.
The views expressed in this article are those of the authors and do not reflect the official policy of the Veterans’
Affairs’ departmentor other departments of the U.S. government.
Thanks to Robyn Fielder, M.S. & Spiro Tzeztsis, M.D. who are instrumental in helping to obtain the data presented in
this presentation as an example. Thanks to Dev Crasta for helping me to
organize the information.
Understand the fundamental components of a clinical case study/series research design
Describe our application of the design to the implementation of a brief behavioral activation intervention for depressive symptoms
Discuss how this approach can provide preliminary data on interventions providers are using regularly within primary care
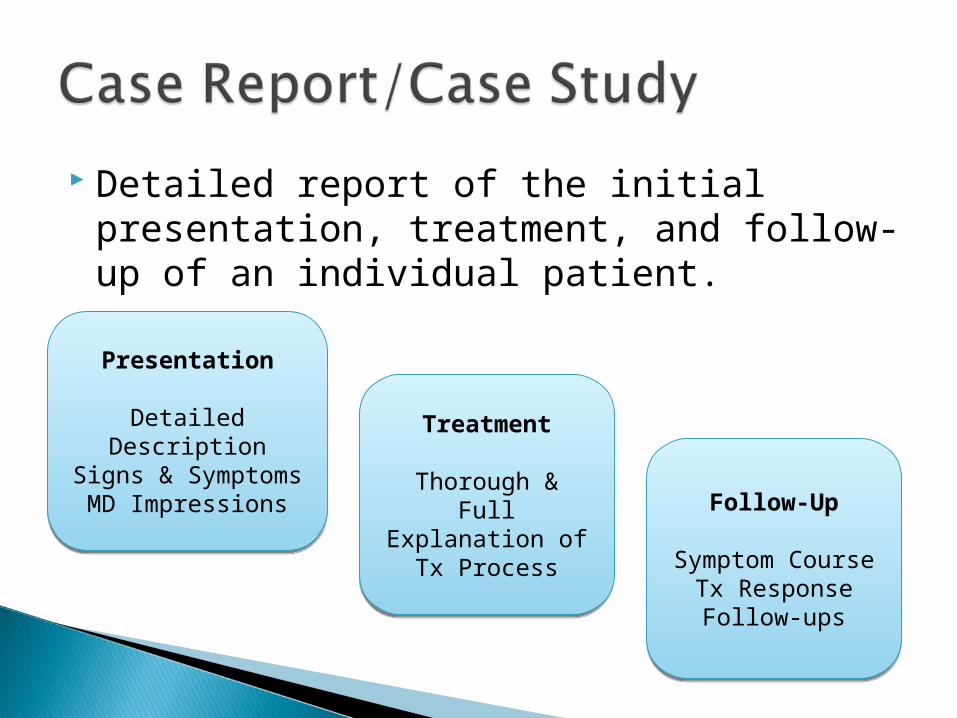
Detailed report of the initial presentation, treatment, and follow-up of an individual patient.
Presentation
Detailed Description
Signs & SymptomsMD Impressions
Presentation
Detailed Description
Signs & SymptomsMD Impressions
Treatment
Thorough & Full Explanation of
Tx Process
Treatment
Thorough & Full Explanation of
Tx Process
Follow-Up
Symptom CourseTx ResponseFollow-ups
Follow-Up
Symptom CourseTx ResponseFollow-ups
Case Report
Case Report
Case Report
Case Report Case Report
Case Report
A study describing the outcomes of multiple patients who were given a similar treatment.
Patients
DemographicsSelect Diagnoses
Patients
DemographicsSelect Diagnoses
Common Treatment
Shared Features&
Individualized Adaptations
Common Treatment
Shared Features&
Individualized Adaptations
Outcomes
% Positive Change
# Adverse Events
Follow-ups
Outcomes
% Positive Change
# Adverse Events
Follow-ups
Decide on clear criteria ◦Examples: Treatment used Condition shows up in chart Symptoms above a certain threshold Demographic Characteristic (e.g.,
Gender; Age)
Decide on a clear definitions of outcomes.◦Examples: Patient drops below a certain symptom
threshold Symptoms drop a measurable amount Patient experiences ANY symptom reduction ABSENCE of negative outcomes or
complications Measurable restoration of patient functioning

Best Practice: Do this prospectively so you can make sure you collect all the data you would like to have
Consider talking to your IRB if you plan on sharing this information through publication in the future
However, you may already have the data already
ELECTRONIC MEDICAL RECORD/CHART REVIEW
Quick and Simple Systematic Method for Evaluating Clinical
Experience Provides a Way to Evaluate Things as a
Clinician Without Funding Provides a Way to Evaluate Things
Diffucult to Evaluate Other Ways

Selection criteria and outcome definitions must be used consistently.
Keep track of relevant treatment differences for each patient.
Remember, the results suggest implications but are not conclusive. This is not a way to determine cause and effect and a limitation is that the findings may not generalize.
CONSIDER MULTIPLE ASSESSMENTS PRIOR TO INTERVENTION AND AT FOLLOW-UP

Depressive symptoms especially common in college students◦High Risk for Suicide
Evidence mixed for antidepressants in:◦Sub-threshold depressive symptoms◦Suicide management
Brief Behavioral Activation (BA)◦Effective in a wide range of populations◦Easily implemented in Primary Care
Syracuse University Health Clinic◦Serves Syracuse University (total
enrollment approx. 20,000)◦ E9,464 patients per semester, E146
patients per day◦2 physicians, 7 nurse practitioners, 4 per
diem practitioners Integrated Behavioral Healthcare (IBHC)
◦Regular screening◦Behavioral Health Providers

BHPs encouraged to use BA with patients reporting depression because:◦ Research demonstrating its effectiveness in reducing
depressive symptoms (Cuijpers, van Straten & Warmerdam, 2007; Mazzucchelli, Kane & Rees, 2009)
All BHPs received additional training and supervision by the first author ◦ Lejuez et al. (2011) manual as a guide
Modifications needed to adjust to brief sessions was necessary◦ Education about depression and the link between
thoughts, behaviors, and mood◦ The importance of increasing pleasurable activities
All charts reviewed for patients in:◦Aug. 2009 –May 2010◦Aug. 2010– Dec. 2010
Charts selected if:◦Presented with depressive
symptoms(n=102)◦Behavioral Activation discussed in 1st
Session (n=42)◦Came back for a second session (n=14)
and a second PHQ-9 score was recorded 11 charts met criteria
Patient Characteristics◦8 Female◦8 White◦Age 19-27 (M= 20.9)◦3 Upperclass; 2 Graduate
Presentation◦Reason for Referral to BHP: Depression/Positive PHQ-9 screen (8) Depression and Sleep (2) Depression and Anxiety (1)
◦Diagnosis on Encounter: Major Depressive Disorder: unspecified (1),
mild (2), moderate (1) Depressive Disorder N.O.S. (2) Adjustment Reaction (2) No Diagnosis (3)
◦PHQ-9: Mean=12.82; SD= 3.55◦5 marked suicidal screening item on
PHQ-9 as greater than 0 3 indicated experiencing thoughts of
death/hurting oneself several days 2 indicated experiencing thoughts of
death/hurting oneself more than ½ the days in the past 2 weeks
At All Sessions◦ BA was used◦ BHP provided educational info about
depression◦ Additional educational materials were provided
Avg. 13 days (SD=6.99) --session 1 & 2 Extra Components
◦ 3 Referred for extra treatment (long-term psychotherapy, medication management)
◦ 2 were seen for a 3rd session, no PHQ-9 data though
◦ Other interventions were also given depending on problem complexity (e.g., stimulus control for sleep problems)

Intake◦ 5 marked suicidal screening item on PHQ-9 as
greater than 0 3 indicated experiencing thoughts of death/hurting
oneself several days 2 indicated experiencing thoughts of death/hurting
oneself more than ½ the days in the past 2 weeks 2nd Session
◦ Only one individual continued to report suicidal ideation and it was maintained at the level of experiencing thoughts several days across the past 2 weeks

Disadvantages◦No way to determine cause/effect
relationships◦Hard to generalize◦Possible biases in data collection and
interpretation Advantages
◦Makes some studies possible◦Easier to implement◦Rich data◦Good way to examine innovative ideas
Lejuez, C., Hopko, D.R., Acierno, R., Daughters, S., and Sherry, L. (2011). Revised Treatment Manual Ten Year Revision of the Brief Behavioral Activation Treatment for Depression. Behavioral Modification, 35, 111-161. DOI: 10.1177/0145445510390929





























