Embed Size (px)
Citation preview

Iron-Deficiency Anemiaof Gastrointestinal Origin
T. S. Dharmarajan, D. Lourdusamy, and C. S. Pitchumoni
ContentsBackground, Definitions, and Prevalence of Anemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Consequences of Anemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Etiology of Anemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Basics of Ferrokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Distribution of Iron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Absorption of Iron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Role of Hepcidin and Ferroportin in Iron Homeostasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Iron Deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Insufficient Dietary Intake . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Gastrointestinal Absorption Defect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Gastrointestinal Blood Loss . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Miscellaneous Causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Evaluation of Iron Deficiency and Related Anemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
T. S. Dharmarajan (*)Albert Einstein College of Medicine, Yeshiva University,Bronx, NY, USA
Montefiore Medical Center (Wakefield Campus), Bronx,NY, USA
N. Y. Medical College, Valhalla, NY, USAe-mail: [email protected]
D. LourdusamyGeriatrics, Montefiore Medical Center, Bronx, NY, USAe-mail: [email protected]
C. S. PitchumoniN. Y. Medical College, Valhalla, NY, USA
Robert Wood Johnson School of Medicine, RutgersUniversity, New Brunswick, NJ, USA
St. Peter’s University Hospital, New Brunswick, NJ, USAe-mail: [email protected]
© Springer Nature Switzerland AG 2020C. S. Pitchumoni, T. S. Dharmarajan (eds.), Geriatric Gastroenterology,https://doi.org/10.1007/978-3-319-90761-1_24-1
1

Diagnostic Markers of Iron Deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Red Blood Cell (RBC) Indices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Serum Indices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Oral Iron Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Duration of Iron Therapy and Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Parenteral Iron Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Key Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
AbstractAnemia, defined as hemoglobin (Hgb) below13 g/dl in males and below 12 g/dl in females,is common in the geriatric population. A thirdof anemia in the old results from nutritionaldeficiency, of which iron deficiency is a majorcontributor. Iron deficiency seldom if everresults from dietary inadequacies in Westernsociety; iron deficiency suggests blood loss,typically of gastrointestinal (or genitourinary)origin, in the geriatric population. Anemia ofiron deficiency always warrants evaluation foran etiology and entails gastrointestinal evalua-tion. After addressing the etiology of iron defi-ciency, iron replacement therapy is provided.Oral iron is adequate in most cases, although itis associated with adverse effects and may leadto nonadherence. In such cases several optionsare available for parenteral iron administration.The chapter discusses the many gastrointesti-nal causes of iron-deficiency anemia and theapproach for evaluation and management.
KeywordsAnemia · Anemia in older adults · Anemia ofgastrointestinal origin · Anemia of irondeficiency · Evaluation of iron-deficiencyanemia in older adults · Iron replacementtherapy · Oral iron therapy · Intravenous irontherapy · Dietary sources of iron · Etiology ofiron deficiency
Background, Definitions,and Prevalence of Anemia
Anemia is increasingly recognized as a serioushealth problem, especially in older adults, as itrelates to morbidity, disability, and mortality(Le 2016; Penninx et al. 2004; Caro et al. 2001;Komajda et al. 2006; Cesari et al. 2004; Groenveldet al. 2008; Culleton et al. 2006; Dharmarajan et al.2008). Although definitions of anemia are incon-sistent, the widely accepted definition is based onthe World Health Organization (WHO) scientificgroup from 1968 (World Health Organization andScientific Group on Nutritional Anaemias 1968).Anemia is defined by a hemoglobin (Hgb) con-centration<13 g/dl in the adult male and<12 g/dlin the adult female. Additional definitions forlower limits of Hgb concentration differ from theWHO definition based on age, race, and gender(Beutler and Waalen 2006). The overall preva-lence of anemia in the US population >65 yearsis 11–12 % based on the National Health andNutritional Examination Survey (NHANES III)(Guralnik et al. 2004). The global prevalence ofanemia in individuals over 60 years is even higheras estimated by WHO data (1993–2005),approaching 23.9% (McLean et al. 2009). In insti-tutionalized residents, the prevalence of anemia ishigher and between 48% and 60% (Artz et al.2004; Landi et al. 2007; Robinson et al. 2007).Prevalence of anemia increases with agefairly consistently, going up to 20–26% of US
2 T. S. Dharmarajan et al.

population over 85 years of age (Guralnik et al.2004; Beghé et al. 2004; Salive et al. 1992; DenElzen et al. 2009; den Elzen et al. 2008). Patternsof geriatric anemia in countries such as Indiareveal that iron deficiency accounts for nearly aquarter of cases and is the common cause, readilytreatable (Sharma et al. 2019) (Tables 1, 2, and 3).
This chapter will detail the gastrointestinalbasis for iron deficiency and related anemia inthe geriatric population.
Consequences of Anemia
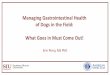
Anemia of any cause in the older population isassociated with consequences. Though mortalityremains the most dreaded consequence, impairedquality of life and organ dysfunction are typicaland common. Anemia is often asymptomaticand discovered incidentally on laboratory testing(Lanier et al. 2018). Studies suggest that evenmilder forms of anemia are associated withdecreased physical and mental functioningleading to impairment in mobility with a predis-position to falls and a decline in cognitive perfor-mance (Penninx et al. 2003; Peters et al. 2008;Winchester et al. 2018). Decline in quality of lifefrom anemia-associated morbidities may even
result in institutionalization. Although anemiahas an association with increased mortality(Groenveld et al. 2008), it is difficult to ascertainif anemia is an independent predictor in thisregard (Fig. 1).
Etiology of Anemia
NHANES III data shows that more than a third ofanemia in age group >65 years (34.3%) relatesto nutrient deficiency of iron, folate, B12, ora combination (Le 2016; Dharmarajan et al.2008; Guralnik et al. 2004). Among the nutri-tional causes of anemia, iron deficiency formsthe major component (>16.6%). Renal insuffi-ciency and anemia of chronic inflammation(ACI) account for 32.2%, while in the remaining33.6%, the cause remains unclear (Table 4)(Fig. 2). Though geographical differences in theetiology of anemia exist, iron deficiency is a sig-nificant contributor to anemia globally, affectingmore than two billion people worldwide (McLeanet al. 2009; Kassebaum et al. 2014).
Our focus will be specifically on iron defi-ciency and related anemia; other nutrient deficien-cies causing anemia are covered elsewhere inthis text.
Table 1 Lower limits ofHgb concentration in olderadults (Beutler and Waalen2006)
Race and sex Hemoglobin (g/dl)
White men >60 years 13.2
White women >50 years 12.2
Black men >60 years 12.7
Black women >50 years 11.5
Table 2 Definitions of anemia
GenderWorld Health Organization(WHO) Hemoglobin (g/dl)
National Kidney Foundation(NKF) Hemoglobin (g/dl)
European Best Practice Guideline(EBPG) Hemoglobin (g/dl)
Male <13 <12 <13.5
Female <12 <11 <11.5
Table 3 Global prevalence of anemia, WHO data (1993–2005)
Populationgroup
Prevalence of anemia Population affected
Percentage%
95% confidence interval(CI)
Number(millions)
95% confidence interval(CI)
Age >60 years 23.9 18.3–29.4 164 126–202
Total population 24.8 22.9–26.7 1,620 1,500–1,740
Iron-Deficiency Anemia of Gastrointestinal Origin 3

Basics of Ferrokinetics
Iron is a critical nutrient for biologic functions anda vital component of hemoglobin, myoglobin,and cytochrome enzymes. Iron homeostasis ismaintained by three key processes: absorption,storage, and recycling. Iron absorption is tightlycontrolled by hepcidin, a circulating peptide
hormone synthesized in the liver. Iron breakdownfrom senescent red blood cells (RBCs) is recycledefficiently by macrophages of the reticuloendo-thelial system (RES) and is circulated by transfer-rin, to be subsequently reused for erythropoiesis.The role of RES in iron metabolism is thus two-fold, recycling and storage. The spleen, liver,and bone marrow are key organs in the RES.
Predisposes to ventricular hypertrophy, heart failure
Predisposes to dementia, depression
Renal dysfunction Poorer intestinal mucosal
health and malabsorption
Gait instability, falls, fractures
Association with fatigue, weakness
Muscle weakness and weaker grip strength
Hospitalizationsand higher costs
ANEMIA
Anemia: Associations and Consequences (Ref.4-8)
Fig. 1 Anemia: Associations and consequences (Komajda et al. 2006; Cesari et al. 2004; Groenveld et al. 2008; Culletonet al. 2006; Dharmarajan et al. 2008)
Table 4 Distribution of types of anemia in older adults (age >65 years) in the USA based on NHANES III, data Phase2 (1991–1994) (Guralnik et al. 2004)
Etiology of anemia Number affected Distribution percentage %
Iron only 467,000 16.6
Folate only 181,000 6.4
B12 only 166,000 5.9
Folate and B12 56,000 2.0
Iron with folate or B12 or both 95,000 3.4
Renal insufficiency only 230,000 8.2
Anemia of chronic inflammation, no renal insufficiency 554,000 19.7
Anemia of chronic inflammation and renal insufficiency 120,000 4.3
Idiopathic 945,000 33.6
Total 2,814,000 100%
4 T. S. Dharmarajan et al.

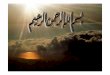
Iron is stored intracellularly in the form of ferritin,a cytosolic protein. Excess iron is depositedas hemosiderin (Trumbo et al. 2001; Waldvogel-
Abramowski et al. 2014; Knutson and Wessling-Resnick 2003) (Fig. 3).
Fig. 2 Anemia and recognized etiology. (Based on NHANES III data, 1988–1994. (Guralnik et al. 2004))
Ferrokinetics
Transferrin
Average Total body Iron ~ 3500 - 4000 mg
Liver ~ 1000 mg
Diet 15 -20 mg/dDuodenum 1-3 mg absorptionLosses 1-3 mg/d
Bone marrow ~ 300 mg
Heart, skeletal muscle, cytochrome enzymes: 400 mg
Macrophages (RES) ~ 600 mg RBCs ~ 2000 mg
Fig. 3 Ferrokinetics
Iron-Deficiency Anemia of Gastrointestinal Origin 5

Distribution of Iron
About two-thirds of the total body iron is presentin erythrocytes as hemoglobin. The average maletotal body iron is around 4,000 mg, of which2,500 mg is in erythrocytes and bone marrow;about 1,000 mg is in intracellular storageform in macrophages of RES and hepatic paren-chymal cells. The remaining iron is distributedbetween myoglobin (skeletal muscle and heart),cytochrome enzymes, and other ferroproteins(Trumbo et al. 2001; Waldvogel-Abramowskiet al. 2014). About 1–2 mg of iron is lost physio-logically daily through desquamation from thegastrointestinal tract and skin. The body mustabsorb roughly the same amount of iron everyday to maintain equilibrium. Adult plasma con-tains only 3–4 mg of iron bound to transferrin,serving as a vehicle between the RES and bonemarrow.Most of the circulating iron is contributedby the RES, while liver parenchyma and absorbediron from the gut contribute a small portion(Knutson and Wessling-Resnick 2003).
Absorption of Iron
Iron absorption occurs predominantly in the duo-denum and upper jejunum (Fuqua et al. 2012).A typical Western or European diet containsabout 15–25 mg iron available for absorption perday. In developing countries, where fortificationis inconsistent, the daily intake is likely lower.Only about 5–18% (~1–3 mg per day) of iron isabsorbed from the gastrointestinal (GI) tract.Absorption is strictly regulated by hepcidin (dis-cussion follows). Heme iron is derived from ani-mal sources such as meat, fish, or poultry, whilenon-heme iron (inorganic iron) is found in bothvegetable and animal sources. Heme protein fromanimal sources is acted upon by gastric acid andproteolytic enzymes thereby releasing the hemefrom proteins. Gastric acidity stabilizes the iron inthe reduced ferrous form (Fe++), which is morebioavailable than the oxidized ferric (Fe+++)form. Ascorbic acid aids in non-heme iron absorp-tion, (Teucher et al. 2004) while some plant-derived components including phytates, tannates,and phosphates (from whole grains and beans)
hinder its absorption by forming complexes withinorganic iron. Ferrous iron is absorbed at thebrush border cells with the transporter divalentmetal ion transporter 1 (DMT-1). Ferric reductaseactivity and duodenal cytochrome B at the levelof brush border of enterocytes also facilitatethe conversion from ferrous to ferric form(McKie et al. 2001). Heme iron is more readilyabsorbed by a different mechanism, although notwell elucidated; this is independent of gastricpH. To summarize, dietary iron is availableas more bioavailable heme or less bioavailableinorganic iron, absorbed at the brush border inferrous form (Fe++). A mixed western diet(including vegetables, meat, and fruits) wouldhave a balance of inhibitors and facilitators ofiron absorption so that the net absorption isfavorable.
Role of Hepcidin and Ferroportinin Iron Homeostasis
Hepcidin meticulously regulates iron absorption.Understanding the molecular mechanism ofhepcidin has improved significantly in the lasttwo decades. Hepcidin functions by blockingabsorption from the GI tract and release frommacrophages and hepatic parenchyma (Hentzeet al. 2010; Ganz 2011). Hepcidin regulates thisaction by an interaction with the iron proteinferroportin. Ferroportin is an iron export proteinexpressed in the basolateral membrane ofenterocytes, hepatocytes, and macrophages ofRES. Hepcidin blocks the absorption of iron bybinding to ferroportin, causing internalization anddegradation of ferroportin (Nemeth et al. 2004; DeDomenico et al. 2007). Hepcidin expression isincreased in response to iron overload and inflam-mation, while it is decreased in response to iron-deficient states and hypoxia. Classic examplesinclude hereditary hemochromatosis, caused bydownregulation (decreased) of hepcidin produc-tion or activity, leading to iron absorption andoverload. On the other hand, chronic inflamma-tion is characterized by upregulation of hepcidinactivity leading to functional iron deficiency withinability to absorb iron and release iron fromstores.
6 T. S. Dharmarajan et al.

Iron Deficiency
With regard to the mechanics of iron deficiency,this chapter will focus solely on the gastrointesti-nal basis for iron loss. Causes of iron deficiencysuch as gynecological blood loss in females mayapply to a given individual, but will not bediscussed here. It should be noted that early stagesof iron deficiency may not manifest with anemia.An individual can become iron deficient from anyof the following circumstances:
1. Insufficient dietary intake2. Gastrointestinal malabsorption3. Blood loss from GI tract4. Miscellaneous causes
Insufficient Dietary Intake
Insufficient dietary intake of iron is never thelikely or common basis for IDA in Western soci-ety; rather iron deficiency is more likely frommalabsorption or blood loss. On the other hand,nutritional causes of iron deficiency apply todeveloping countries where food fortification isnot uniformly enforced and intestinal parasiteinfestations are common. Daily iron requirementto replace the daily physiological losses amountsto 1–2 mg daily. Recommended dietary allowance(RDA) for iron is 8 mg/day for males >19 yearsand females over 51 years (Trumbo et al. 2001).Menstruating and pregnant women require higherintake.
Meat, fish, and poultry have high iron contentwith better bioavailability. Fortified cereals areone of the richest sources of iron in developedcountries. Major sources of non-heme ironinclude vegetables, beans, and fortified grainproducts. Table 5 lists the common food sourcesand their approximate high, moderate, or low ironcontent.
One is unlikely to develop dietary irondeficiency while consuming a balanced diet.Inadequate dietary iron intake can however beencountered in older individuals with cognitivedeficits, inadequate dietary supervision, and die-tary fads. Socioeconomic factors may well be
contributory. A balanced should not result iniron deficiency, unless there is coexisting bloodloss or a malabsorption disorder. In summary, irondeficiency in the older adult necessitates evalua-tion as to the cause.
Gastrointestinal Absorption Defect
Absorption of iron from the gastrointestinal tractmay result from primary defects in intestinalabsorption (e.g., celiac disease) or following gas-trointestinal surgery. Iron deficiency and relatedanemia secondary to malabsorption are generallyunderestimated requiring a high index ofsuspicion.
Celiac DiseaseCeliac disease is an autoimmune disease witha genetic predisposition where the ingestion ofgluten causes injury to the small intestine; whileit is classically identified in younger adults, thedisorder is not uncommon in the old. The mucosalinflammation and villous atrophy in celiac diseaseresult in loss of small intestinal absorptive surface.About 19–34% of new cases of celiac disease areidentified in people over 60 years and up to 25%noted in the seventh decade in developed coun-tries (Rubio-Tapia et al. 2012; Freeman 1995;Lurie et al. 2008; Rashtak and Murray 2009).Clinical presentation may be asymptomatic orsubtle with bloating or mild diarrhea. Lack ofawareness among health-care professionals inconjunction with variable presentations makesthis a diagnostic challenge in the geriatric agegroup. Presence of other autoimmune diseasesshould raise suspicion for the disorder. Nutrientdeficiencies including iron, folic acid, calcium,B12, D, and other fat-soluble vitamins heightenthe suspicion particularly in the presence of anintact gut and absence of bacterial overgrowthsyndrome. Celiac disease is detailed in anotherchapter.
Anemia is common in celiac disease, occurringin up to 60–80% of older people with the disorder(Rubio-Tapia et al. 2012; Rashtak and Murray2009). Iron deficiency results from malabsorp-tion; however, anemia may be multifactorial
Iron-Deficiency Anemia of Gastrointestinal Origin 7

from coexisting vitamin B12 or folate deficiency.Classic features of iron deficiency may be lackingif iron deficiency coexists with B12 and/or folatedeficiency; the blood smear may be atypical insuch cases.
Primary care physicians and geriatricians havea role to consider the possibility of celiacdisease in those with iron deficiency. Serologicaltesting includes anti-endomysial (EMA) and anti-tissue transglutaminase (TTG) autoantibodies.
However, the gold standard for diagnosis isintestinal biopsy, facilitated by referral to thegastroenterologist.
Other Causes of MalabsorptionWith increasing incidence of obesity worldwide,bariatric surgery is on the rise. Though bariatricsurgery is commonly performed in youngeradults, one frequently encounters older adultswho have undergone prior bariatric surgery.
Table 5 Common food sources and approximate iron content. (Source: United States Department of Agriculture(USDA))
mg/serving % daily value
Food with high iron content
Breakfast cereals, fortified with 100% of the DV for iron, 1 serving 18 100
Oysters, eastern, cooked with moist heat, 3 ounces 8 44
White beans, canned, 1 cup 8 44
Chocolate, dark, 45–69% cacao solids, 3 ounces 7 39
Beef liver, pan fried, 3 ounces 5 28
Food with moderate to low iron content
Lentils, boiled and drained, ½ cup 3 17
Spinach, boiled and drained, ½ cup 3 17
Tofu, firm, ½ cup 3 17
Kidney beans, canned, ½ cup 2 11
Sardines, Atlantic, canned in oil, drained solids with bone, 3 ounces 2 11
Chickpeas, boiled and drained, ½ cup 2 11
Tomatoes, canned, stewed, ½ cup 2 11
Potato, baked, flesh and skin, one medium potato 2 11
Cashew nuts, oil roasted, 1 ounce (18 nuts) 2 11
Green peas, boiled, ½ cup 1 6
Chicken, roasted, meat and skin, 3 ounces 1 6
Rice, white, long grain, enriched, parboiled, drained, ½ cup 1 6
Bread, whole wheat, one slice 1 6
Bread, white, one slice 1 6
Raisins, seedless, ¼ cup 1 6
Spaghetti, whole wheat, cooked, 1 cup 1 6
Tuna, light, canned in water, 3 ounces 1 6
Turkey, roasted, breast meat and skin, 3 ounces 1 6
Nuts, pistachio, dry roasted, 1 ounce (49 nuts) 1 6
Broccoli, boiled and drained, ½ cup 1 6
Egg, hard boiled, one large 1 6
Rice, brown, long or medium grain, cooked, 1 cup 1 6
Food with no iron content
Cheese, cheddar, 1.5 ounces 0 0
Cantaloupe, diced, ½ cup 0 0
Mushrooms, white, sliced and stir-fried, ½ cup 0 0
Cheese, cottage, 2% milk fat, ½ cup 0 0
Milk, 1 cup 0 0
8 T. S. Dharmarajan et al.

We can speculate that this number is on theincrease in the geriatric population. In the USA,an estimated 228,000 bariatric procedures wereperformed in 2017 with a consistent increasein the number of procedures every year since2011 (Estimate of Bariatric Surgery Numbers,2011–2017 | American Society for Metabolicand Bariatric Surgery 2019). Among the proce-dures, sleeve gastrectomy and Roux-en-Y gastricbypass (RYGB) were the two most commonlyperformed (75–80%). RYGB involves creationof a small gastric pouch which is connectedto the jejunum, whereas in sleeve gastrectomy,a longitudinal resection of the stomach isperformed without any intestinal diversion.Of note, iron is absorbed largely in the duodenumand proximal jejunum.
Evaluation of iron status in patients undergo-ing bariatric surgery is crucial. Preoperativeiron status can influence the postoperative ironstatus and outcomes. Obese individuals mayhave underlying iron deficiency, which mayworsen following bariatric surgery, warrantingan evaluation before and after bariatric surgery.In a study there was a progressive increase in iron-deficiency anemia to 72.4% at 24 months postRoux-en-Y gastric bypass (de Cleva et al. 2019).Post-bariatric surgery, iron deficiency results frommultiple reasons. Iron absorption is affectedby a decline in gastric acid secretion, bypassof the primary sites of absorption, small intestinalbacterial overgrowth (SIBO), reduced food intakeor intolerance, and nonadherence to dietary rec-ommendations (Saltzman and Philip 2013).
SIBO is characterized by overgrowthof colonic-type bacteria in the small intestine,an entity that escapes diagnosis given the vaguepresentation. SIBO occurs in those with a predis-position to intestinal stasis such as gastrointestinalsurgery leading to structural abnormalities (stric-tures and blind loops), gastroparesis, motilitydisorders (autonomic neuropathy, scleroderma,etc.), diverticulosis, and long-term use of protonpump inhibitors (detailed in another chapter).
Gastrointestinal Blood Loss
Gastrointestinal bleeding is the most commoncause of bleeding-related IDA in older adults.Occult GI blood loss should be ruled out in anygeriatric patient presenting with IDA. The list ofmedications the patient is on and the comorbidityshould be taken into account. Antiplatelet agents,anticoagulants, and NSAIDs are often causativefactors for GI bleeding and influence the persis-tence of bleeding and prognosis. Beta blockersmay blunt the tachycardia response to GI bloodloss and anemia. Multiple comorbidities such ascardiac or renal disease influence the outcome ofbleeding and increase the risk of interventions.
Subtle, chronic, or occult GI blood loss canpresent as IDA, first noticed by a primary provideror geriatrician. Common causes of upper andlower GI bleed in the old are listed below (Kaplanet al. 2001; Tang et al. 2018; Strate 2005;Longstreth 1997; Ríos et al. 2005). The incidenceof LGIB increases with age, (Longstreth 1997) asa consequence of increased prevalence of colonicdiverticula, ischemia, vascular telangiectasia, andneoplasms (Kaplan et al. 2001; Ríos et al. 2005).Angiodysplasia and aortic stenosis are highlyprevalent in the elderly and often coexist (Moheeet al. 2013). VonWillebrand factor (VWF) defectsarising from shear in vasculature from the stenoticaortic valve may contribute to bleeding (Soranet al. 2002). Though controversies exist in thisregard, it is worth noting this association in olderadults, especially in cases of obscure bleed. GIbleeding in geriatric individuals incurs longerinpatient stays and greater health-care costswhen compared to younger individuals (Comayand Marshall 2002).
Gastric antral vascular ectasia (GAVE), thoughrare, accounts for up to 4% of non-variceal upperGI bleeding; while the pathophysiology is notclear, the disorder must be differentiated fromportal hypertensive gastropathy. GAVE does notrespond to measures to reduce portal pressure.
Iron-Deficiency Anemia of Gastrointestinal Origin 9

Table 6 lists the common causes of upper andlower GI bleeding in the geriatric age group.Endoscopic ablation is the treatment of choice(Selinger and Ang 2008). Linear gastric erosion,associated with large diaphragmatic hernia andchronic blood loss anemia, is a result of trauma;the gastric erosions are located on the crests ofmucosal fold at or near the diaphragm (Cameronand Higgins 1986). A large diaphragmatic herniawithout the lesions may be an occult cause ofIDA.
IDA may be the only presenting sign of occultGI bleeding in an individual with a neoplasm.Cognitive status may limit history taking in theold, compounded by the absence of an availablecaregiver. Most cases of occult bleeding in thosewith good functional and cognitive status benefitfrom referral to a gastroenterologist in anticipa-tion of interventional procedures. Decision forintervention is multidisciplinary and should bemade following discussion with the patientand/or caregiver (if warranted), primary care phy-sician, and gastroenterologist.
Miscellaneous Causes
Gastritis-induced achlorhydria is hypothesized tobe an independent cause of IDA (Batesh et al.2015). Helicobacter pylori (H. pylori) and iron-deficiency anemia are prevalent worldwide; datais equivocal on the benefit ofH. pylori eradicationand benefit for IDA. In a meta-analysis of 16 ran-domized controlled trials totaling 956 patients, thedata suggested that treatment of H. pylori infec-tion could be effective in improving iron statusand related anemia, especially when the anemia
is moderate or severe (Yuan et al. 2010). Anothermeta-analysis suggested that an associationbetween IDA and H. pylori and that eradicationof H. pylori can improve hemoglobin andserum ferritin levels, although not significantly(Qu et al. 2010).
Iron-deficiency anemia is associated with sev-eral GI conditions including inflammatory boweldisorders and also liver disorders (Stein et al.2016). Several factors may be contributoryincluding blood loss, malabsorption, and inflam-mation; IDA is a comorbid disorder commonly inpatients with GI and liver disease (Stein et al.2016). Anemia is considered the most prevalentextraintestinal complication of inflammatorybowel disease (IBD) (Stein et al. 2010). Anemiais common in IBD and influences outcomesincluding hospitalizations and quality of life; ane-mia results from several causes including bloodloss and inflammation; treatment involves use ofiron supplements, although oral iron may exacer-bate the disease due to the adverse effects, pro-mpting consideration for intravenous iron (Steinet al. 2010).
Evaluation of Iron Deficiencyand Related Anemia
As previously emphasized, IDA in the old war-rants a search for a GI etiology for bleedingor malabsorption. A significant number of consul-tations requested of gastroenterologists aredirected toward evaluating anemia, in particulariron-deficiency anemia (Zhu et al. 2010). The keyis to identify the etiology of anemia and treat theunderlying cause where possible. In older adults,
Table 6 Common causes of upper and lower GI bleed in elderly
Upper GI bleed Lower GI bleed
Peptic ulcer Diverticular bleed
Esophageal and gastric varices Angiodysplasia
Gastric malignancy Neoplasm
Portal gastropathy Ischemia
Gastric antral vascular ectasia Hemorrhoids and other anorectal disorders
Dieulafoy’s lesion Post polypectomy
Mallory Weiss tear Radiation proctitis
Aorto-enteric fistula Rectal varices
Linear gastric erosions Inflammatory bowel disease and colitis (infectious, ischemic, antibiotic associated)
10 T. S. Dharmarajan et al.

anemia is common, occurring in one study intwo-thirds of subjects over geriatric patients,with the anemia primarily due to iron deficiencyin 65% (Geisel et al. 2014). The practice ofreplacing iron losses alone without searching fora cause must be discouraged.
Age by itself is not a contraindication for fur-ther evaluation, including GI procedures. TheBritish Society of Gastroenterology has publishedstepwise guidelines in defining IDA, the investi-gations involved, and management (Goddardet al. 2011). The guidelines suggest upper andlower GI investigations in all postmenopausalfemale and all male patients with IDA, unlessthere is a confirmed history on non-GI bloodloss. All patients are to be screened for celiacdisease, based on the guideline; if the screen ispositive, in those over age 50 years with anemia,lower GI evaluation should still be considered(Goddard et al. 2011). Fecal occult blood testingis of no benefit in the diagnosis of IDA based onthe guidelines; rectal examination is seldom con-tributory in the absence of rectal bleeding andtenesmus and can be done along with colonos-copy (Goddard et al. 2011).
Evaluation should begin with obtaining afocused history including review of medications.Barriers may exist in this regard in those withcognitive impairment, depression, and psychiatricdisorders. Clinical features of anemia may besubtle or asymptomatic; physical activity andprior functional status of patients help interpretmanifestations such as decreased exercise toler-ance and easy fatigability. Orthostatic hypoten-sion could be an indicator of significant bloodloss. Subtle symptoms include irritability, delir-ium, or worsening cognition. Underlying organdysfunction may be exacerbated, as in heart fail-ure, chronic obstructive lung disease, or kidneydisease (Fig. 1).
Diagnostic Markers of Iron Deficiency
Diagnosis of iron deficiency and IDA may not bestraightforward in older people with coexistingillnesses that alter the red cell indices, makinglaboratory diagnosis of IDA challenging. Bone
marrow biopsy which is the gold standard diag-nostic tool for iron deficiency is seldom usedin practice today, as it has limited practical appli-cability because of its invasiveness.
Red Blood Cell (RBC) Indices
Chronic iron deficiency is manifested by micro-cytic, hypochromic RBCs on peripheral bloodsmear, which reflect low mean corpuscularvolume (MCV) and low mean corpuscular hemo-globin concentration (MCHC), respectively.In early stages of iron deficiency, red cells maybe normocytic, as is the case with acute bloodloss. In many older adults, iron deficiency maycoexist with B12 or folate deficiency which willrender the above parameters less reliable.
Serum Indices
FerritinSerum ferritin is a commonly used marker for irondeficiency. Though ferritin is an indicator of intra-cellular iron storage, small quantities of ferritinare secreted into the serum (Cohen et al. 2010) andcorrelate with iron stores (Walters et al. 1973).Serum ferritin levels below 18–20 mcg/L are areliable index of depleted iron stores (Lipschitzet al. 2010;Wawer et al. 2018). Ferritin is a markerof inflammatory state (Kell and Pretorius 2014).Acute and chronic infections, inflammatorydisorders such as rheumatoid arthritis and inflam-matory bowel disease, and liver disease are asso-ciated with elevate serum ferritin levels. Duringhospitalizations, ferritin is typically elevated as anacute phase reactant. In light of these facts, anormal ferritin level does not necessarily rule outiron deficiency in the old. Higher cutoff levels offerritin (50 mcg/dl) will improve the diagnosticsensitivity (Joosten et al. 1991).
Serum Iron, Transferrin Saturation,Transferrin Iron-Binding CapacitySerum iron levels are low in iron deficiency.However, low serum iron is not specific for irondeficiency as it is also low in anemia of chronic
Iron-Deficiency Anemia of Gastrointestinal Origin 11

disease (ACD). Transferrin synthesis isupregulated in iron-deficient states. Transferriniron-binding capacity (TIBC) is the sumof unbound iron-binding capacity and plasmairon. Normal range for TIBC is 255–450 μg/dL.TIBC is typically increased in iron deficiency;increased TIBC is a specific marker of irondeficiency. Transferrin saturation is the ratio ofserum iron to TIBC. Normally transferrin isone-third saturated with iron; a range of 25–45%is considered normal. In iron deficiency, transfer-rin saturation is <20%.
Table 7 provides a comparison of iron-deficiency anemia and ACD.
Management
The first step is to address the cause of iron defi-ciency where possible. Examples include treat-ment of peptic ulcer disease and avoidanceof the use of NSAIDs in cases of upper GIbleeding, where applicable. Replacement of iron(or supplements such as B12 or folic acid)is subsequent step and not the sole treatment strat-egy. In general, while counseling regarding nutri-tious diets is good practice, correction of irondeficiency through use of iron rich foods is likelyto be inefficient in the long run. Use of oral orparenteral iron is the preferred means to correctiron deficiency.
Referral to a gastroenterologist may be indi-cated for most cases to delineate a cause foriron deficiency and offer appropriate treatmentfor the underlying cause. In older adults, anesophagogastroduodenoscopy and colonoscopyshould be initiated to identify a bleeding cause;CT colonography can replace colonoscopy
(Joosten 2018). In addition, obscure GI bleed(e.g., angiodysplasia or other small bowel bleed-ing source) may warrant the use of video capsuleendoscopy (Sealock et al. 2018). In a cohort, smallbowel capsule endoscopy diagnosed clinicallyrelevant findings in the setting of IDA in almosthalf the patients, with the diagnostic yield higherin those older than 60 years (Xavier et al. 2018).While testing for Helicobacter pylori isrecommended for evaluation of unexplainedIDA, the evidence supporting this recommenda-tion is scant in older adults without peptic ulcerdisease or significant upper GI source of bloodloss (John et al. 2018). However, often, geriatri-cians and primary care physicians may needto manage this aspect especially when gastroin-testinal procedures are not readily accessible oravailable.
Oral Iron Therapy
Oral iron is a safe, inexpensive, and efficientmethod of iron replacement. It has remained thefrontline standard despite evidence that it ispoorly tolerated (Auerbach and Spivak 2019).Older adults may complain of intolerance to oraliron, relating to gastrointestinal adverse effectssuch as metallic taste, nausea, flatulence, consti-pation, diarrhea, epigastric distress, and vomiting.In addition, some people on oral iron supplementsexperience anxiety from black or tarry stools.These factors can contribute to nonadherence totherapy. Alternate day dosing of oral iron has beenshown to be effective (Auerbach and Schrier2017) and associated with fewer gastrointestinalside effects. In fact, multiple daily dosing of oraliron has shown a paradoxical effect on iron
Table 7 Iron indices
Indices Iron-deficiency anemia Anemia of chronic disease
Serum iron Decreased Decreased
Transferrin Increased Decreased or normal
TIBC Increased Decreased or normal
Transferrin saturation Decreased Decreased
Ferritin Decreased Increased
Transferrin receptor status High Low
12 T. S. Dharmarajan et al.

absorption (Moretti et al. 2015). In a randomizedcontrol study done in octogenarians, a daily dos-ing of 15, 50, and 150 mg elemental iron wasshown to be equally effective in increasing hemo-globin concentration in a 2-month period, withsignificantly lower side effects in the low-dosegroup (Rimon et al. 2005). A 325 mg ferroussulfate tablet contains 65 mg of elemental iron,of which approximately 25 mg is absorbed. Iron isbest absorbed in a mildly acidic medium. PPIs andother acid reducing agents decrease oral ironabsorption. Practical approaches to improve oraliron absorption are helpful in those who tolerateoral iron. In general, iron should not be given withfood containing phytates, tannates, phosphates,and calcium. Co-administration of oral iron withorange juice or vitamin C on an empty stomachmay be ideal to enhance absorption. Once-a-dayoral iron is the current recommendation in contrastto the twice- or thrice-daily oral iron therapy in thepast; in those intolerant to oral iron, even a singledose thrice weekly helps and will minimizeadverse effects. Iron therapy has been largelyunderutilized, because of missing the diagnosisof iron deficiency, complex schedules, andadverse effects (Busti et al. 2019). Table 8 listsexamples of oral iron preparations.
Duration of Iron Therapy and Response
Duration of iron therapy and response depends onvarious factors; these include correction of under-lying etiology and adherence with the regimen.All available oral preparations are equally effec-tive and do not influence the response to therapy.Typically, reticulocytosis is the earliest observed
response, occurring in 7–10 days. Subjective feel-ing of well-being may occur in the first few daysor weeks of therapy. Hemoglobin concentrationis expected to increase in several weeks, atabout 1–2 g/dl increase in 3–4 weeks of therapy.Duration of the therapy should be titrated toresponse. Lack of response to oral iron therapy(after confirming adherence and correct modeof administration) warrants re-evaluation for anetiology, including ongoing blood loss, coexistingchronic inflammatory conditions that retard oraliron absorption, and exclusion of disorders suchas celiac disease.
Parenteral Iron Therapy
The most common indication for intravenous irontherapy is intolerance to oral therapy or failure toabsorb iron. In those with chronic inflammatorydisorders that interfere with iron absorption, intra-venous (IV) iron is the preferred method toreplace iron. In cases of malabsorption includingceliac disease, bacterial overgrowth, or followingbariatric surgery, IV iron therapy is logical.Although the potential GI adverse effects of oraliron are not an issue with intravenous iron therapy,one may encounter minor allergic or infusion-related reactions including fever, urticaria, arthral-gia, and myalgia in a small number of cases andanaphylactic reactions rarely. High molecularweight (HMW) dextran, the initially marketedform of IV iron, was associated with significantadverse events including life-threatening anaphy-laxis and is currently obsolete. Rare instanceswhen HMW dextran is substituted as a lessercost generic counterpart are not unheard
Table 8 Forms of oral iron
DrugElemental iron (mg iron/mg of tablet or per mlliquid)
Common dosage inpreparation
Ferrous sulfate 20–30% 325 mg tablet220 mg/5 ml oral elixir75 mg/ml oral solution
Ferrous fumarate 33% 324 or 325 mg
Ferrous gluconate 10–14% 240 mg, 324 mg, 325 mg
Polysaccharide-iron complex(PIC)
Variable with manufacturer Various preparationsavailable
Iron-Deficiency Anemia of Gastrointestinal Origin 13

of. The adverse events with low molecular weight(LMW) dextran and the more commonly usediron sucrose and ferric gluconate are muchlower (Moniem and Bhandari 2007; Critchleyand Dundar 2007; Chertow et al. 2004).Premedication with drugs prior to IV iron admin-istration is not routinely recommended, assome side effects from the former can be mis-interpreted as adverse effects due to the latter.Antihistamines as premedication cause hypoten-sion, dizziness, irritability, flushing, and wheez-ing. Administration guidelines vary with eachpreparation; review of manufacturer instructionsis suggested. Test dosing may be required withsome preparations. Overall, most currently avail-able formulations of IV therapy are safe. Formsof IV iron are listed in Table 9. While the route ofiron supplementation is less important in termsof raising the hemoglobin levels, it is importantto offer iron in some form; perhaps iron storesare raised more effectively with intravenousiron (Bager and Dahlerup 2014). Intravenousiron is used when oral iron is not tolerated(Goddard et al. 2011).
In summary, iron-deficiency anemia resultsfrom a cause, typically blood loss; in the geriatricpopulation, it is likely to be GI blood loss ormalabsorption of iron. Although the disorder iscommon and treatable, management presentschallenges. In a study by the British GeriatricsSociety to ascertain how older adults with
potential IDA are managed, a third indicated thatthey would accept hemoglobin levels <10 g/dlwithout further investigation, and a quarter statedthat they only occasionally or never check ferritinlevels; only 30% would sometimes or always useparenteral iron when oral supplements were nottolerated (Donaldson et al. 2019). The findingssuggest a high level of variation in clinical prac-tice and low level of knowledge in managing IDAin the older population. Guidelines offer a lucid,succinct approach to manage iron-deficiency ane-mia (Goddard et al. 2011).
Key Points
• Iron deficiency is a common cause of anemia inolder adults.
• Iron-deficiency anemia warrants evaluation;dietary iron deficiency is seldom the cause.
• Occult GI blood loss should be alwaysexcluded as an initial step.
• Clinical symptoms of iron deficiency may besubtle in the old especially in those physicallyinactive.
• Referral to a gastroenterologist for endoscopicprocedures and delineation of etiology forblood loss is generally recommended in apatient with iron deficiency.
• Awareness of malabsorptive disorders furtherhelps improve diagnostic yield; celiac disease
Table 9 Forms of IV iron
DrugCommonbrand
Elemental ironconcentration (mg/ml) Dosing and additional comments
Iron sucrose Venofer 20 Several doses of 200–300 mg
Ferric carboxymaltose
Injectafer,Ferinject
50 For weight>50 kg, two doses of 750 mg, 7 or moredays apartFor weight <50 kg, two doses of 15 mg/kg given7 or more days apart
Ferric gluconate Ferrlecit 12.5 Multiple doses of 125 to 187.5 mg
Ferumoxytol Feraheme 30 Two doses of 510 mg (given 3 to 8 days apart) orsingle dose of 1020 mgRadiologist should be notified if MRI is plannedwithin 3 months of administration
Iron dextran (lowmolecular weight)
INFeD 50 Multiple doses of 100 mg or single dose of 1000 mgAdd: needs test dose
Iron isomaltoside Monomer 100 500 mg dose up to three doses given over 1 week orsingle dose of 20 mg/kg
14 T. S. Dharmarajan et al.

and inflammatory bowel dose may be encoun-tered in the old for the first time.
• After addressing the cause, one may consideroral iron therapy as an initial step; the dosagefor oral iron is once daily. In those intolerant oforal iron, alternate day dosing is efficient andmay improve adherence with therapy.
• In situations when oral iron is associated withadverse effects and not tolerated, intravenousiron therapy is a reasonable next step.
References
Artz AS, Fergusson D, Drinka PJ, Gerald M,Gravenstein S, Lechich A, et al. Prevalence ofanemia in skilled-nursing home residents. ArchGerontol Geriatr. 2004. https://doi.org/10.1016/j.archger.2004.03.006.
Auerbach M, Schrier S. Treatment of iron deficiency isgetting trendy. Lancet Haematol. 2017. https://doi.org/10.1016/S2352-3026(17)30194-1.
Auerbach M, Spivak J. Treatment of iron deficiency in theelderly: a new paradigm. Clin Geriatr Med. 2019.https://doi.org/10.1016/j.cger.2019.03.003.
Bager P, Dahlerup JF. Randomised clinical trial: oralvs. intravenous iron after upper gastrointestinalhaemorrhage – a placebo-controlled study. AlimentPharmacol Ther. 2014;39(2):176–87.
Batesh AL, Santa Ana CA, Cole JA, Fordtran JS. Is achlor-hydria a cause of iron deficiency anemia? Am J ClinNutr. 2015;102(1):9–19.
Beghé C,Wilson A, Ershler WB. Prevalence and outcomesof anemia in geriatrics: a systematic review of theliterature. Am J Med. 2004. https://doi.org/10.1016/j.amjmed.2003.12.009.
Beutler E, Waalen J. The definition of anemia: what is thelower limit of normal of the blood hemoglobin concen-tration? Blood. 2006. https://doi.org/10.1182/blood-2005-07-3046.
Busti, F., Marchi, G., Lira Zidanes, A., Castagna, A. &Girelli, D. Treatment options for anemia in the elderly.Transfus Apher Sci. (2019). https://doi.org/10.1016/j.transci.2019.06.018.
Cameron AJ, Higgins JA. Linear gastric erosion. A lesionassociated with large diaphragmatic hernia andchronic blood loss anemia. Gastroenterology.1986;91(2):338–42.
Caro JJ, Salas M, Ward A, Goss G. Anemia as an indepen-dent prognostic factor for survival in patients withcancer: a systematic, quantitative review. Cancer.2001. https://doi.org/10.1002/1097-0142(20010615)91:12<2214::AID-CNCR1251>3.0.CO;2-P.
Cesari M, Penninx BWJH, Lauretani F, Russo CR,Carter C, Bandinelli S, et al. Hemoglobin levels andskeletal muscle: results from the InCHIANTI study.
J Gerontol Ser A Biol Sci Med Sci. 2004. https://doi.org/10.1093/gerona/59.3.m249.
Chertow GM, Mason PD, Vaage-Nilsen O, AhlménJ. On the relative safety of parenteral iron formulations.Nephrol Dial Transplant. 2004. https://doi.org/10.1093/ndt/gfh185.
Cohen LA, Gutierrez L,Weiss A, Leichtmann-BardoogoY,Zhang DL, Crooks DR, et al. Serum ferritin is derivedprimarily from macrophages through a nonclassicalsecretory pathway. Blood. 2010. https://doi.org/10.1182/blood-2009-11-253815.
Comay D, Marshall JK. Resource utilization for acutelower gastrointestinal hemorrhage: the Ontario GIbleed study. Can J Gastroenterol. 2002. https://doi.org/10.1155/2002/156592.
Critchley J, Dundar Y. Adverse events associated withintravenous iron infusion (low-molecular-weightiron dextran and iron sucrose): a systematic review.Transfus Altern Transfus Med. 2007. https://doi.org/10.1111/j.1778-428x.2007.00042.x.
Culleton BF, Manns BJ, Zhang J, Tonelli M, Klarenbach S,Hemmelgarn BR. Impact of anemia on hospitalizationand mortality in older adults. Blood. 2006. https://doi.org/10.1182/blood-2005-10-4308.
de Cleva R, Cardia L, Riccioppo D, Kawamoto M,Kanashiro N, Santo MA. Anemia before and afterRoux-en-Y gastric bypass: prevalence and evolutionon long-term follow-up. Obes Surg. 2019. https://doi.org/10.1007/s11695-019-03920-6.
De Domenico I, Ward DM, Langelier C, Vaughn MB,Nemeth E, Sundquist WI, et al. The molecularmechanism of hepcidin-mediated ferroportin down-regulation. Mol Biol Cell. 2007. https://doi.org/10.1091/mbc.e07-01-0060.
den ElzenWPJ, Westendorp RGJ, Frölich M, de Ruijter W,Assendelft WJJ, Gussekloo J. Vitamin B12 and folateand the risk of anemia in old age. Arch Intern Med.2008. https://doi.org/10.1001/archinte.168.20.2238.
Den Elzen WPJ, Willems JM, Westendorp RGJ, De CraenAJM, Assendelft WJJ, Gussekloo J. Effect of anemiaand comorbidity on functional status and mortality inold age: results from the Leiden 85-plus study. CMAJ.2009. https://doi.org/10.1503/cmaj.090040.
Dharmarajan TS, Pankratov A, Morris E, Qurashi S,Law G, Phillips S, et al. Anemia: its impact on hospi-talizations and length of hospital stay in nursing homeand community older adults. J Am Med Dir Assoc.2008. https://doi.org/10.1016/j.jamda.2008.02.008.
Donaldson, A. I. C., Soiza, R. L., Hands, K. J.,Witham, M. D. &Myint, P. K. Variability in the clinicalmanagement of iron deficiency anaemia in older adults:results from a sur vey of UK specialists in the care ofolder people. Ther Adv Drug Saf. 2019. https://doi.org/10.1177/2042098619854870.
Estimate of Bariatric Surgery Numbers, 2011–2017 |American Society for Metabolic and Bariatric Surgery.https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers. Accessed 2 Aug 2019.
Iron-Deficiency Anemia of Gastrointestinal Origin 15

Freeman HJ. Clinical spectrum of biopsy defined celiacdisease in the elderly. Can J Gastroenterol. 1995.https://doi.org/10.1155/1995/290893.
Fuqua BK, Vulpe CD, Anderson GJ. Intestinal iron absorp-tion. J Trace Elem Med Biol. 2012. https://doi.org/10.1016/j.jtemb.2012.03.015.
Ganz T. Hepcidin and iron regulation, 10 yearslater. Blood. 2011. https://doi.org/10.1182/blood-2011-01-258467.
Geisel T, Martin J, Schulze B, et al. An etiologicprofile of anemia in 405 geriatric patients. Anemia.2014;2014:932486. https://doi.org/10.1155/2014/932486.
Goddard AF, James MW, McIntyre AS, et al. Guidelinesfor the management or iron deficiency anaemia. Gut.2011;60:1309–16.
Groenveld HF, Januzzi JL, Damman K, vanWijngaarden J,Hillege HL, van Veldhuisen DJ, et al. Anemia andmortality in heart failure patients. A systematic reviewand meta-analysis. J Am Coll Cardiol. 2008. https://doi.org/10.1016/j.jacc.2008.04.061.
Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG,Woodman RC. Prevalence of anemia in persons65 years and older in the United States: evidence for ahigh rate of unexplained anemia. Blood. 2004. https://doi.org/10.1182/blood-2004-05-1812.
Hentze MW, Muckenthaler MU, Galy B, Camaschella C.Two to tango: regulation of mammalian ironmetabolism. Cell. 2010. https://doi.org/10.1016/j.cell.2010.06.028.
John S, Baltodano JD, Mehta N, Mark K, Murthy U.Unexplained iron deficiency anemia: does Helicobacterpylori have a role to play? Gastroenterol Rep. 2018.https://doi.org/10.1093/gastro/goy001.
Joosten E. Iron deficiency anemia in older adults: a review.Geriatr Gerontol Int. 2018. https://doi.org/10.1111/ggi.13194.
Joosten E, Hiele M, Ghoos Y, PelemansW, Boogaerts MA.Diagnosis of iron deficiency anemia in a hospitalizedgeriatric population. Am J Med. 1991. https://doi.org/10.1016/S0002-9343(05)80022-1.
Kaplan RC, Heckbert SR, Koepsell TD, Furberg CD,Polak JF, Schoen RE, et al. Risk factors for hospitalizedgastrointestinal bleeding among older persons. J AmGeriatr Soc. 2001. https://doi.org/10.1046/j.1532-5415.2001.49032.x.
Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK,Johns N, Lozano R, et al. A systematic analysis ofglobal anemia burden from 1990 to 2010. Blood.2014. https://doi.org/10.1182/blood-2013-06-508325.
Kell DB, Pretorius E. Serum ferritin is an important inflam-matory disease marker, as it is mainly a leakage productfrom damaged cells. Metallomics. 2014. https://doi.org/10.1039/c3mt00347g.
Knutson M, Wessling-Resnick M. Iron metabolism in thereticuloendothelial system. Crit Rev Biochem MolBiol. 2003. https://doi.org/10.1080/713609210.
Komajda M, Anker SD, Charlesworth A, Okonko D,Metra M, Di Lenarda A, et al. The impact of new
onset anemia on morbidity and mortality in chronicheart failure: results from COMET. Eur Heart J. 2006.https://doi.org/10.1093/eurheartj/ehl012.
Landi F, Russo A, Danese P, Liperoti R, Barillaro C,Bernabei R, et al. Anemia status, hemoglobin concen-tration, and mortality in nursing home older residents.J Am Med Dir Assoc. 2007. https://doi.org/10.1016/j.jamda.2007.01.028.
Lanier JB, Park JJ, Callahan RC. Anemia in older adults.Am Fam Physician. 2018;98(7):437–42.
Le CHH. The prevalence of anemia and moderate-severeanemia in the US population (NHANES 2003–2012).PLoS One. 2016. https://doi.org/10.1371/journal.pone.0166635.
Lipschitz DA, Cook JD, Finch CA. A clinical evaluation ofserum ferritin as an index of iron stores. N Engl J Med.2010. https://doi.org/10.1056/nejm197405302902201.
Longstreth GF. Epidemiology and outcome of patientshospitalized with acute lower gastrointestinal hemor-rhage: a population-based study. Am J Gastroenterol.1997;92(3):419–24.
Lurie Y, Landau DA, Pfeffer J, Oren R. Celiac diseasediagnosed in the elderly. J Clin Gastroenterol. 2008.https://doi.org/10.1097/01.mcg.0000247995.12087.7b.
McKie AT, Barrow D, Latunde-Dada GO, Rolfs A,Sager G, Mudaly E, et al. An iron-regulated ferricreductase associated with the absorption of dietaryiron. Science (80–). 2001. https://doi.org/10.1126/science.1057206.
McLean E, Cogswell M, Egli I, Wojdyla D, De Benoist B.Worldwide prevalence of anaemia, WHO Vitamin andMineral Nutrition Information System, 1993–2005.Public Health Nutr. 2009. https://doi.org/10.1017/S1368980008002401.
Mohee K, Aldalati O, Dworakowski R, Haboubi H. Aorticstenosis and anemia with an update on approaches tomanaging angiodysplasia in 2018. Cardiol J. 2013.https://doi.org/10.5603/cj.a2018.0068.
Moniem KA, Bhandari S. Tolerability and efficacyof parenteral iron therapy in hemodialysis patients,a comparison of preparations. Transfus AlternTransfus Med. 2007. https://doi.org/10.1111/j.1778-428x.2007.00050.x.
Moretti D, Goede JS, Zeder C, Jiskra M, Chatzinakou V,Tjalsma H, et al. Oral iron supplements increasehepcidin and decrease iron absorption from daily ortwice-daily doses in iron-depleted young women.Blood. 2015. https://doi.org/10.1182/blood-2015-05-642223.
Nemeth E, Tuttle MS, Powelson J, Vaughn MD,Donovan A, Ward DMV, et al. Hepcidin regulatescellular iron efflux by binding to ferroportin and induc-ing its internalization. Science (80–). 2004. https://doi.org/10.1126/science.1104742.
Penninx BWJH, Guralnik JM, Onder G, Ferrucci L,Wallace RB, Pahor M. Anemia and decline in physicalperformance among older persons. Am J Med. 2003.https://doi.org/10.1016/S0002-9343(03)00263-8.
16 T. S. Dharmarajan et al.

Penninx BWJH, Pahor M, Cesari M, Corsi AM,Woodman RC, Bandinelli S, et al. Anemia is associatedwith disability and decreased physical performance andmuscle strength in the elderly. J Am Geriatr Soc. 2004.https://doi.org/10.1111/j.1532-5415.2004.52208.x.
Peters R, Burch L, Warner J, Beckett N, Poulter R, BulpittC. Haemoglobin, anaemia, dementia and cognitivedecline in the elderly, a systematic review. BMCGeriatr. 2008. https://doi.org/10.1186/1471-2318-8-18.
Qu XH, Huang XL, Hiong P, et al. Does Helicobacterpylori infection play a role in iron deficiencyanemia? A meta-analysis. World J Gastroenterol.2010;16(9):886–96.
Rashtak S, Murray JA. Celiac disease in the elderly.Gastroenterol Clin N Am. 2009. https://doi.org/10.1016/j.gtc.2009.06.005.
Rimon E, Kagansky N, Kagansky M, Mechnick L,Mashiah T, Namir M, et al. Are we giving too muchiron? Low-dose iron therapy is effective in octogenar-ians. Am J Med. 2005. https://doi.org/10.1016/j.amjmed.2005.01.065.
Ríos A, Montoya MJ, Rodríguez JM, Serrano A, Molina J,Parrilla P. Acute lower gastrointestinal hemorrhagesin geriatric patients. Dig Dis Sci. 2005. https://doi.org/10.1007/s10620-005-2662-1.
Robinson B, Artz AS, Culleton B, Critchlow C, Sciarra A,Audhya P. Prevalence of anemia in the nursinghome: contribution of chronic kidney disease.J Am Geriatr Soc. 2007. https://doi.org/10.1111/j.1532-5415.2007.01389.x.
Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA,Everhart JE. The prevalence of celiac disease in theUnited States. Am J Gastroenterol. 2012. https://doi.org/10.1038/ajg.2012.219.
Salive ME, Cornoni-Huntley J, Guralnik JM, Phillips CL,Wallace RB, Ostfeld AM, et al. Anemia and hemoglo-bin levels in older persons: relationship with age, gen-der, and health status. J Am Geriatr Soc. 1992. https://doi.org/10.1111/j.1532-5415.1992.tb02017.x.
Saltzman E, Philip Karl J. Nutrient deficiencies after gastricbypass surgery. Annu Rev Nutr. 2013. https://doi.org/10.1146/annurev-nutr-071812-161225.
Sealock RJ, Thrift AP, El-Serag HB, Sellin J. Long-termfollow up of patients with obscure gastrointestinalbleeding examined with video capsule endoscopy.Medicine (United States). 2018. https://doi.org/10.1097/MD.0000000000011429.
Selinger CP, Ang YS. Gastric antral vascular ectasia(GAVE): an update on clinical presentation, pathophys-iology and treatment. Digestion. 2008;77(2):131–7.
Sharma D, Suri V, Pannu A, Attri S, Varma N, Kochhar R,et al. Patterns of geriatric anemia: a hospital-basedobservational study in North India. J Fam MedPrim Care. 2019. https://doi.org/10.4103/jfmpc.jfmpc_450_18.
Soran H, Lewis M,Whorwell PJ. Bleeding angiodysplasia:should we concentrate more on the aortic valve than onthe bowel? Int J Clin Pract. 2002;56(2):155–6.
Stein J, Hartmann F, Dignass AU. Diagnosis and manage-ment of iron deficiency anemia in patients with IBD.Nat Rev Gastroenterol Hepatol. 2010;7(11):599–610.
Stein J, Connor S, Virgin G, et al. Anemia and iron defi-ciency in gastrointestinal and liver conditions. WorldJ Gastroenterol. 2016;22(35):7908–25.
Strate LL. Lower GI bleeding: epidemiology and diagno-sis. Gastroenterol Clin N Am. 2005. https://doi.org/10.1016/j.gtc.2005.08.007.
Tang GH, Hart R, Sholzberg M, Brezden-MasleyC. Iron deficiency anemia in gastric cancer: aCanadian retrospective review. Eur J GastroenterolHepatol. 2018. https://doi.org/10.1097/MEG.0000000000001251.
Teucher B, Olivares M, Cori H. Enhancers of iron absorp-tion: ascorbic acid and other organic acids. Int J VitamNutr Res. 2004. https://doi.org/10.1024/0300-9831.74.6.403.
Trumbo P, Yates AA, Schlicker S, Poos M. Dietary refer-ence intakes: vitamin A, vitamin K, arsenic, boron,chromium, copper, iodine, iron, manganese, molybde-num, nickel, silicon, vanadium, and zinc. J Am DietAssoc. 2001. https://doi.org/10.1016/S0002-8223(01)00078-5.
Waldvogel-Abramowski S, Waeber G, Gassner C,Buser A, Frey BM, Favrat B, et al. Physiology of ironmetabolism. TransfusMed Hemother. 2014. https://doi.org/10.1159/000362888.
Walters GO, Miller FM, Worwood M. Serum ferritin con-centration and iron stores in normal subjects. J ClinPathol. 1973. https://doi.org/10.1136/jcp.26.10.770.
Wawer AA, Jennings A, Fairweather-Tait SJ. Iron status inthe elderly: a review of recent evidence. Mech AgeingDev. 2018. https://doi.org/10.1016/j.mad.2018.07.003.
Winchester LM, Powell J, Lovestone S, Nevado-Holgado AJ. Red blood cell indices and anaemia ascausative factors for cognitive function deficits and forAlzheimer’s disease. Genome Med. 2018. https://doi.org/10.1186/s13073-018-0556-z.
World Health Organization, Scientific Group onNutritional Anaemias. Nutritional anemias. Reportof a WHO scientific group, World Health Organization– technical report series. Geneva: World HealthOrganization; 1968.
Xavier S, Magalhães J, Rosa B, Moreira MJ, Cotter J.Impact of small bowel capsule endoscopy in iron defi-ciency anemia: influence of patient’s age on diagnosticyield. Arq Gastroenterol. 2018. https://doi.org/10.1590/s0004-2803.201800000-61.
Yuan W, Yumin L, Kehu Y, et al. Iron deficiency anemiain Helicobacter pylori infection: meta-analysis of ran-domized controlled trials. Scand J Gastroenterol.2010;45(6):665–76.
Zhu A, Kaneshiro M, Kaunitz JD. Evaluation and treat-ment of iron deficiency anemia: a gastroenterologicalperspective. Dig Dis Sci. 2010;55(3):548–59.
Iron-Deficiency Anemia of Gastrointestinal Origin 17